Embed Size (px)
Citation preview
Liver Transplantation 2012
Marion Peters MD
University of California
San Francisco
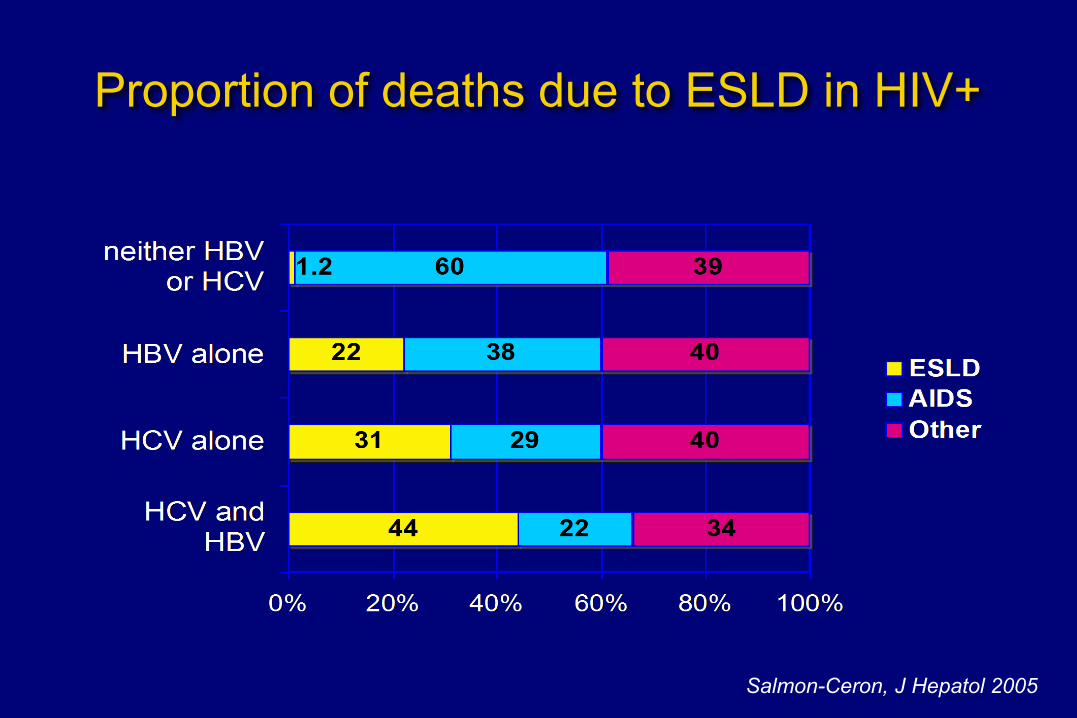
Proportion of deaths due to ESLD in HIV+
Salmon-Ceron, J Hepatol 2005
Indications for Liver Transplantation Development of liver decompensation
Ascites Variceal hemorrhage Hepatic encephalopathy Synthetic dysfunction Hepatocellular carcinoma
HIV patients with decompensated cirrhosis have a median survival of ≈ 1 year
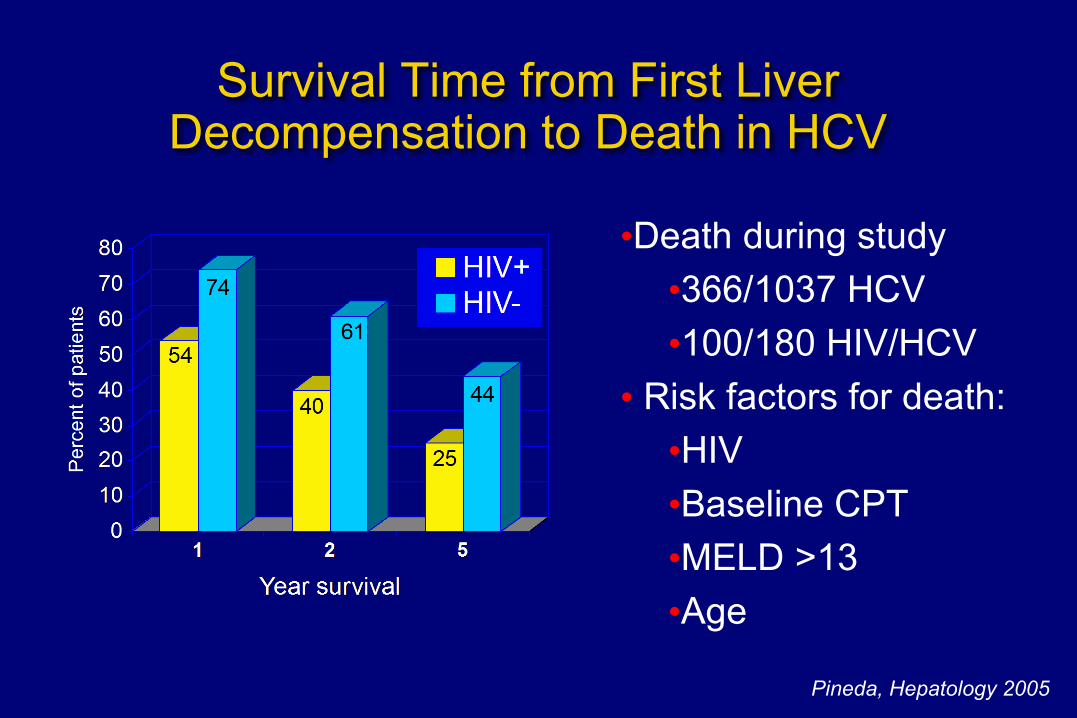
Survival Time from First Liver Decompensation to Death in HCV
Pineda, Hepatology 2005
•Death during study •366/1037 HCV •100/180 HIV/HCV
• Risk factors for death: •HIV •Baseline CPT •MELD >13 •Age
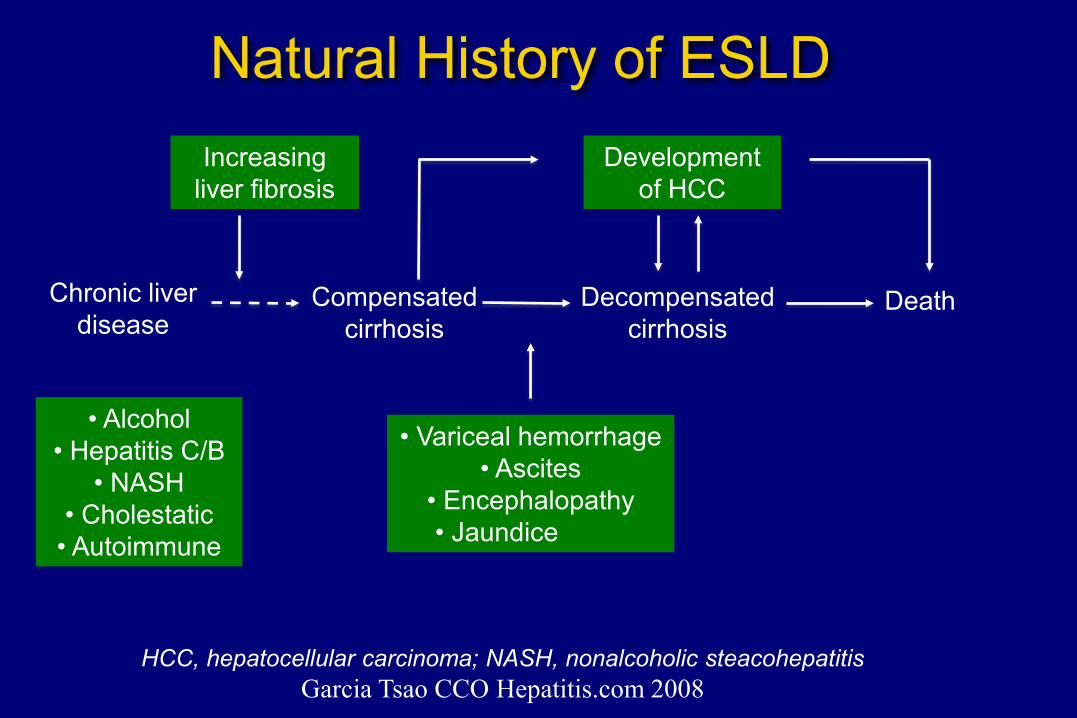
Natural History of ESLD Increasing
liver fibrosis Development
of HCC
Chronic liver disease
Compensated cirrhosis
Decompensated cirrhosis
Death
• Alcohol • Hepatitis C/B
• NASH • Cholestatic
• Autoimmune
• Variceal hemorrhage • Ascites
• Encephalopathy • Jaundice
HCC, hepatocellular carcinoma; NASH, nonalcoholic steacohepatitis Garcia Tsao CCO Hepatitis.com 2008
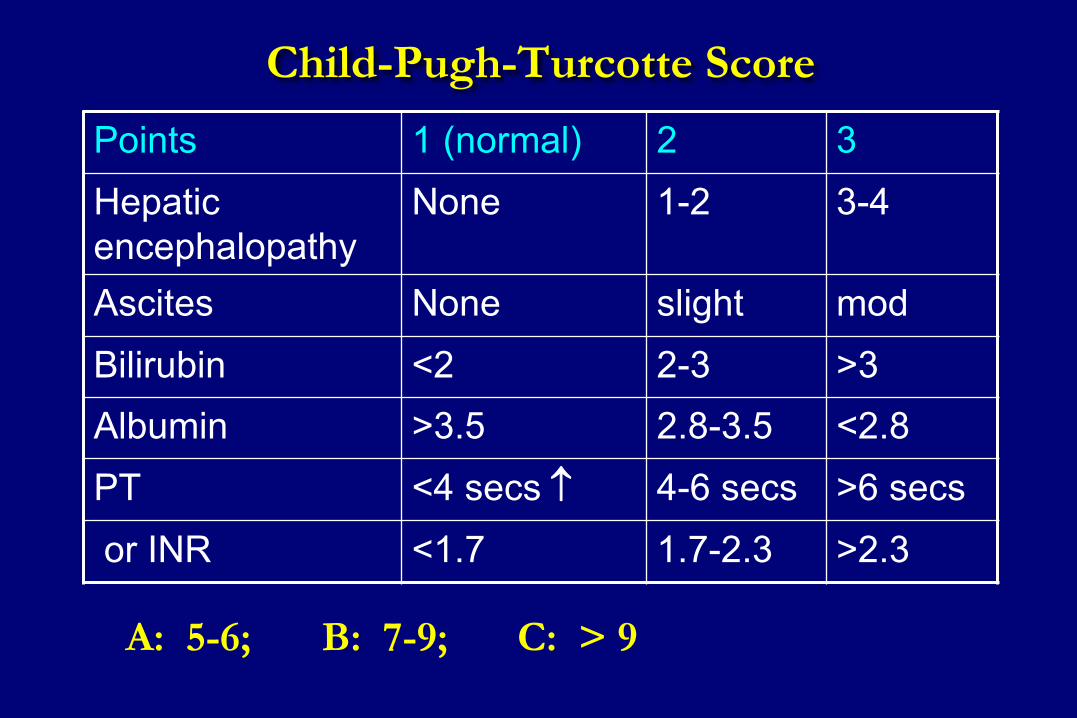
Child-Pugh-Turcotte Score Points 1 (normal) 2 3 Hepatic encephalopathy
None 1-2 3-4
Ascites None slight mod Bilirubin <2 2-3 >3 Albumin >3.5 2.8-3.5 <2.8 PT <4 secs ↑ 4-6 secs >6 secs
or INR <1.7 1.7-2.3 >2.3
A: 5-6; B: 7-9; C: > 9
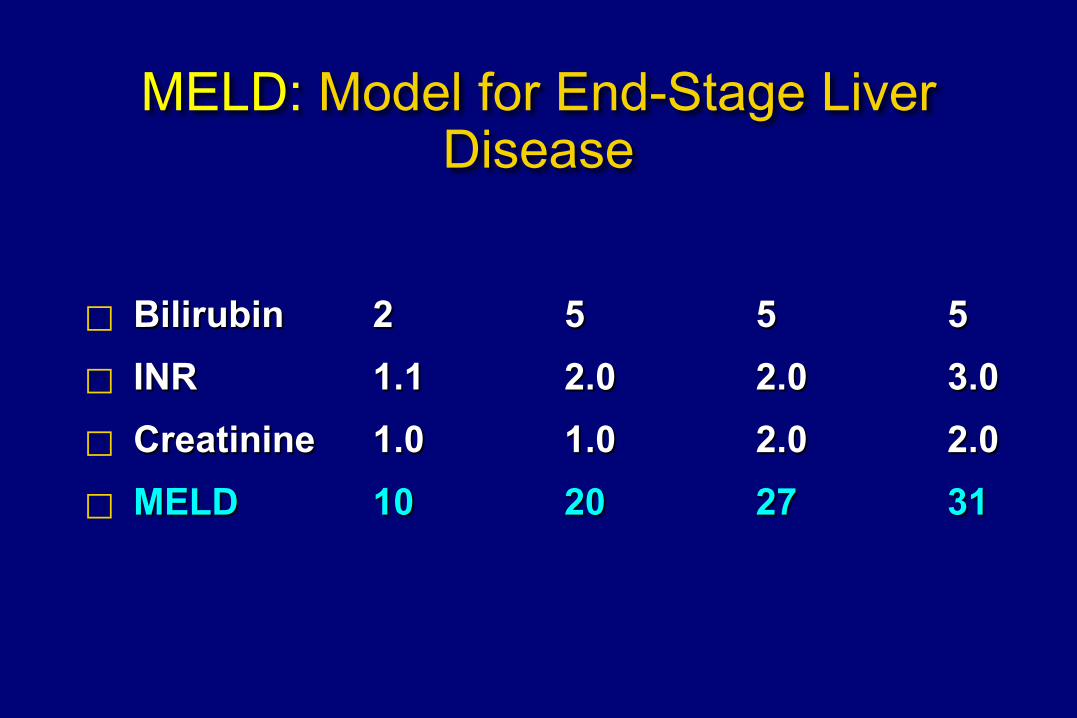
MELD: Model for End-Stage Liver Disease
Bilirubin 2 5 5 5 INR 1.1 2.0 2.0 3.0 Creatinine 1.0 1.0 2.0 2.0 MELD 10 20 27 31
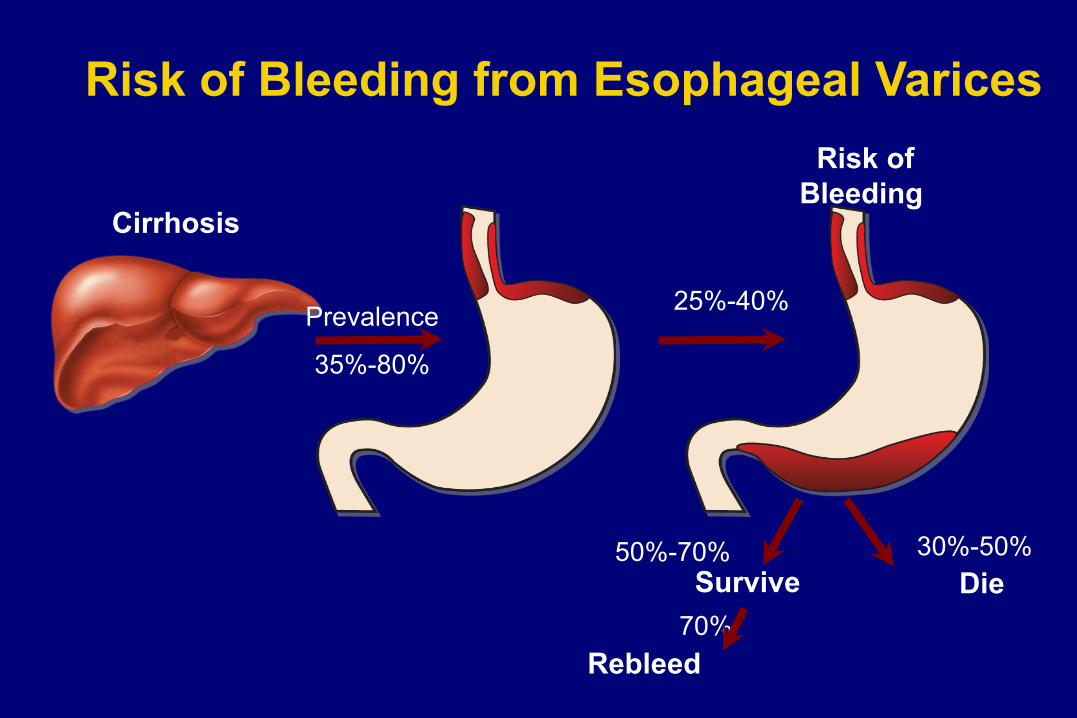
Cirrhosis
Prevalence
35%-80%
25%-40%
Die 30%-50% 50%-70%
Survive
Rebleed 70%
Risk of Bleeding
Risk of Bleeding from Esophageal Varices

Variceal Surveillance
All cirrhotics require Esophagogastroduodenoscopy
Garcia-Tsao G, et al. Hepatology. 2007;46:932-938.
No varices
Repeat endoscopy in 3 years (well
compensated); in 1 year if
decompensated
No beta-blocker prophylaxis
Small varices (< 5 mm), Child B/C
Nonselective Beta-blocker prophylaxis
Medium or large varices
Child Class A, no red wales: beta blockers
Child class B/C, red wales: beta blockers or
band ligation
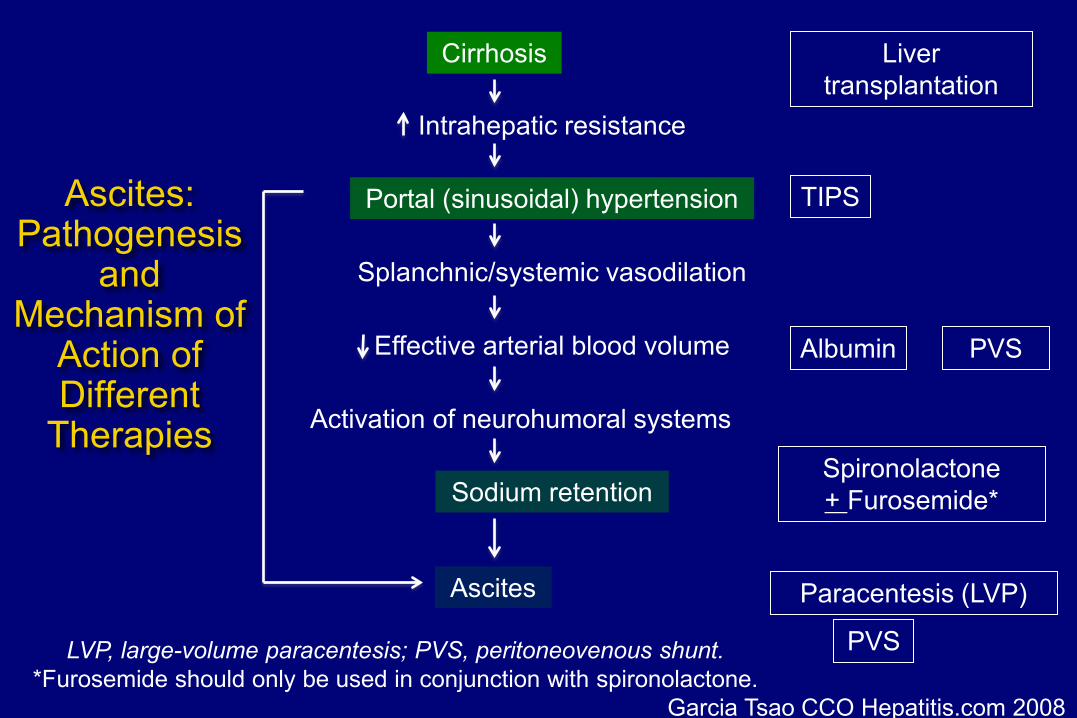
Ascites: Pathogenesis
and Mechanism of
Action of Different
Therapies
Cirrhosis
Intrahepatic resistance
Portal (sinusoidal) hypertension
Splanchnic/systemic vasodilation
Effective arterial blood volume
Activation of neurohumoral systems
Sodium retention
Ascites
Liver transplantation
TIPS
Albumin PVS
Spironolactone + Furosemide*
Paracentesis (LVP)
PVS LVP, large-volume paracentesis; PVS, peritoneovenous shunt. *Furosemide should only be used in conjunction with spironolactone.
Garcia Tsao CCO Hepatitis.com 2008
Treatment of ascites Diuretic-responsive ascites
Sodium restriction Spironolactone (75-100 mg) and furosemide (20-40 mg)
Refractory ascites Large volume paracentesis with 25% albumin (50 cc/L) TIPS- higher OLT free survival, higher PSE TIPS HVP <12 mm Hg Albumin, midodrine and octreotide- vasoconstriction Experimental: clonidine, vasopression 2 R antagonists
Hyponatremia Fluid restriction, vasopression 2R antagonists, midodrine
Hepatorenal syndrome Results from vasodilatation and marked reduction
in effective arterial blood volume leading to renal vasoconstriction
Occurs in patients with refractory ascites and/or hyponatremia.
Type 1 HRS: rapidly progressive renal failure in 2 weeks with a doubling of serum creatinine to a level > 2.5
mg/dL or halving creatinine clearance to < 20 mL/min Prognosis: < 50% survival at 1 month
HRS-contd Type 2 HRS: slowly progressive
increase in serum creatinine level to > 1.5 mg/dL a creatinine clearance of < 40 mL/mi or a urine sodium < 10 mEq/d associated with ascites that is unresponsive to
diuretic medications median survival: ~ 6 months
Spontaneous bacterial peritonitis (SBP)
Most common type of bacterial infection in hospitalized cirrhotic patients
Clinical suspicion: <50%: fever, abdominal pain or tenderness, and
leukocytosis unexplained encephalopathy, jaundice worsening renal failure
Diagnose: tap ascites: WCC>500, PMN > 250 cells/mm3
Place ascites in blood culture bottles
Start treatment immediately before culture results
SBP treatment Cephalosporins Renal dysfunction is main cause of death
prevented by the use of intravenous albumin if serum bilirubin > 4 mg/dL serum creatinine > 1 g/dL or blood urea nitrogen level > 30 mg/dL
Prevent recurrence: ciprofloxacin, TMP/SMX, norfloxacin
Primary prophylaxis: ciprofloxacin weekly if MELD >9
Hepatic Encephalopathy Results from a combination of
Portosystemic shunting failure to metabolize neurotoxic substances Ammonia remains the most important neurotoxic
substance but poorly correlates with stage
Precipitants Infection- especially SBP or UTI HCC Bleeding Electrolyte imbalance Portal vein thrombosis Worsening liver disease
Hepatic Encephalopathy
Treatment aims to reduce production of ammonia from the colon through nonabsorbable disaccharides
lactulose, lactitol, and lactose
nonabsorbable antibiotics neomycin, rifaximin
Protein restriction promotes protein degradation and, if maintained for long periods, worsens nutritional status and decreases muscle mass No longer recommended
OLT in HIV HAART-associated improvements:
decreased mortality decreased incidence of opportunistic infections decreased hospitalization rates
Immunosuppressives may have anti-HIV effects
cyclosporine, MMF, rapamycin Better prophylaxis for opportunistic infections
Data from NIH multicenter study of 125 OLT 150 CRT
Liver Transplantation
MELD Serum sodium Underestimated
chronic encephalopathy hepatic hydrothorax hepatopulmonary syndrome portopulmonary hypertension
1
0.9
0.8
0.7
0.6
0.5 0 1 2 3 4 5
Sur
viva
l %
Era 3 (1997-2002)
Time (years)
P = .14
Other
HBV
1
0.9
0.8
0.7
0.6
0.5 0 1 2 3 4 5
Sur
viva
l %
Era 1 (1987-1991)
Time (years)
P < 0.01
Other
HBV
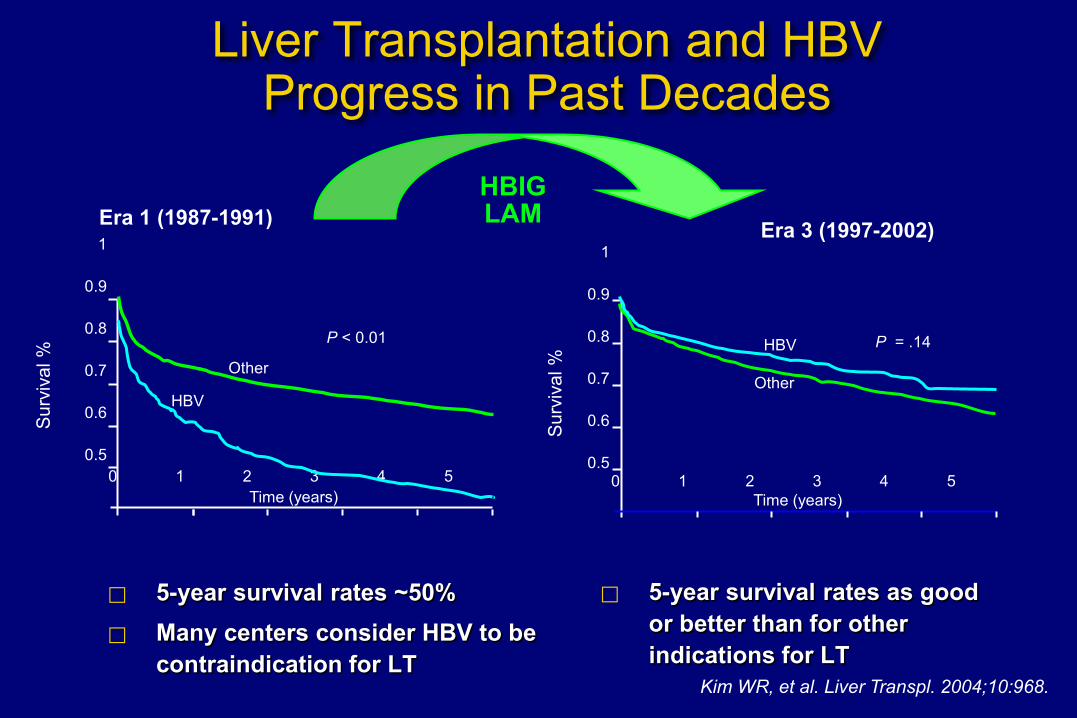
Kim WR, et al. Liver Transpl. 2004;10:968.
Liver Transplantation and HBV Progress in Past Decades
5-year survival rates ~50% Many centers consider HBV to be
contraindication for LT
5-year survival rates as good or better than for other indications for LT
HBIG LAM
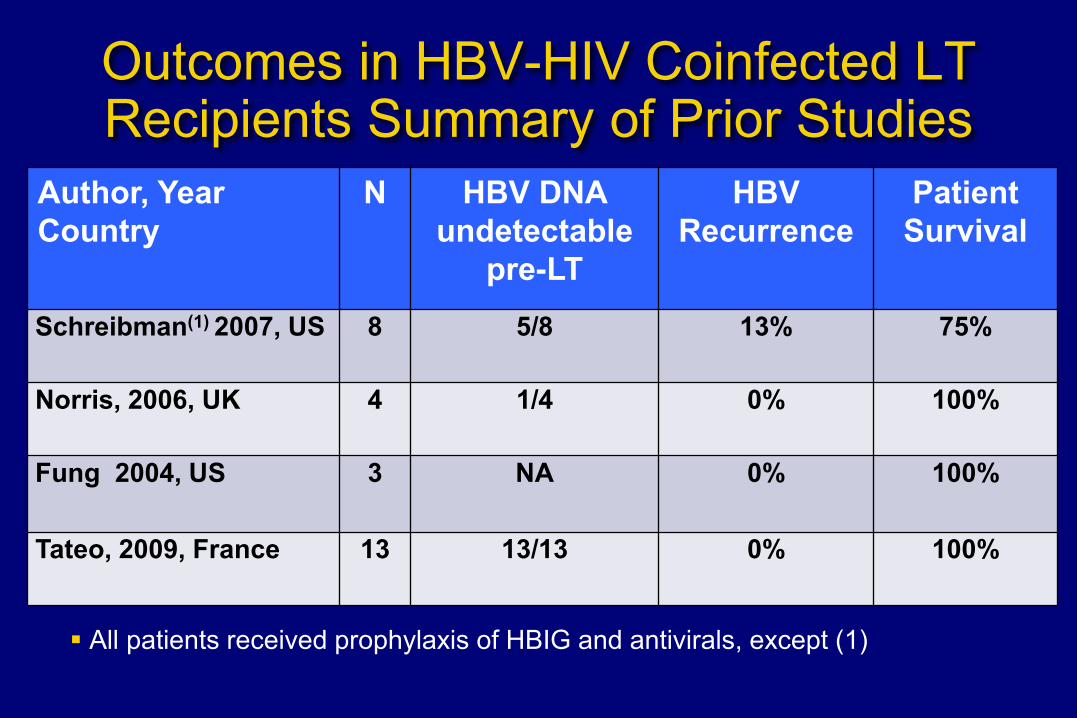
Outcomes in HBV-HIV Coinfected LT Recipients Summary of Prior Studies
Author, Year Country
N HBV DNA undetectable
pre-LT
HBV Recurrence
Patient Survival
Schreibman(1) 2007, US 8 5/8 13% 75%
Norris, 2006, UK 4 1/4 0% 100%
Fung 2004, US 3
NA 0% 100%
Tateo, 2009, France 13 13/13 0% 100%
All patients received prophylaxis of HBIG and antivirals, except (1)
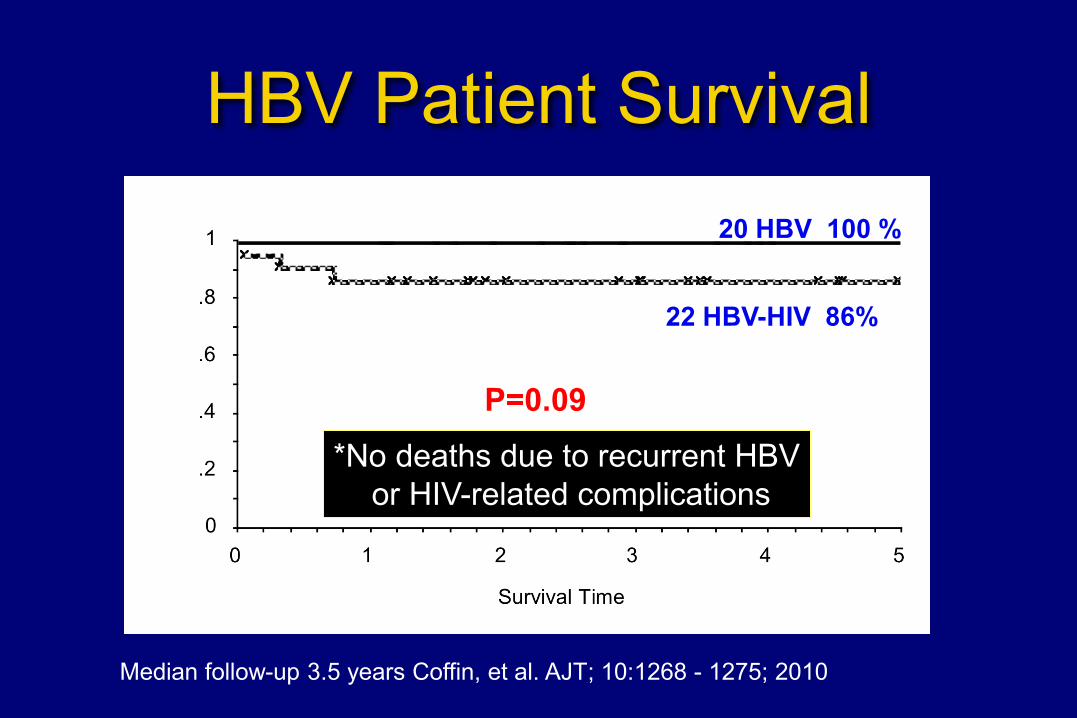
HBV Patient Survival
*No deaths due to recurrent HBV or HIV-related complications
P=0.09
20 HBV 100 %
22 HBV-HIV 86%
Median follow-up 3.5 years Coffin, et al. AJT; 10:1268 - 1275; 2010
HBV Recurrence & Viremia No recurrent HBsAg
No histologic recurrence
53% detectable HBV DNA post-transplant
Mean HBV DNA 108 IU/ml (range 20-790 IU/ml) More frequent in patients with detectable HBV DNA pre-
transplant and those with prior treated acute rejection No persistently detectable HBV DNA
Coffin, et al. AJT; 10:1268 - 1275; 2010
HBV as Indication for LT HBV common in HIV-infected persons 19-fold higher risk of liver-related death in coinfected vs HBV
monoinfected patients 1 Among referred patients Clinically evident LMV-resistance frequent is 67- >90% 2 Survival lower in patients on LMV vs drug combinations
(ADV/TDF + LMV/FTC) at the time of referral
Post-LT, recurrent disease is rapidly progressive without virologic control Higher rates of LAM-r among HIV-HBV infected patients
presenting for LT may increase risk of prophylaxis failure
Thio CL, et al. Lancet. 2002 Terrault NA, et al. Liver Transplant 2007
HCV as Indication for LT HCV is the most common cause of liver-related
mortality in HIV-infected patients
Prior studies in HCV-HIV coinfected transplant recipients indicate:
Higher rates of wait-list mortality Worse post-LT survival More severe recurrent HCV disease Poor response to HCV treatment
Duclos-Vallee JC, Hepatology 2008;47:407–417.
Castells L, Transplantation 2007;83:354–358. Ragni MV, Liver Transpl 2005;11:1425–1430.
Pineda JA, Hepatology 2005;41:779–789.
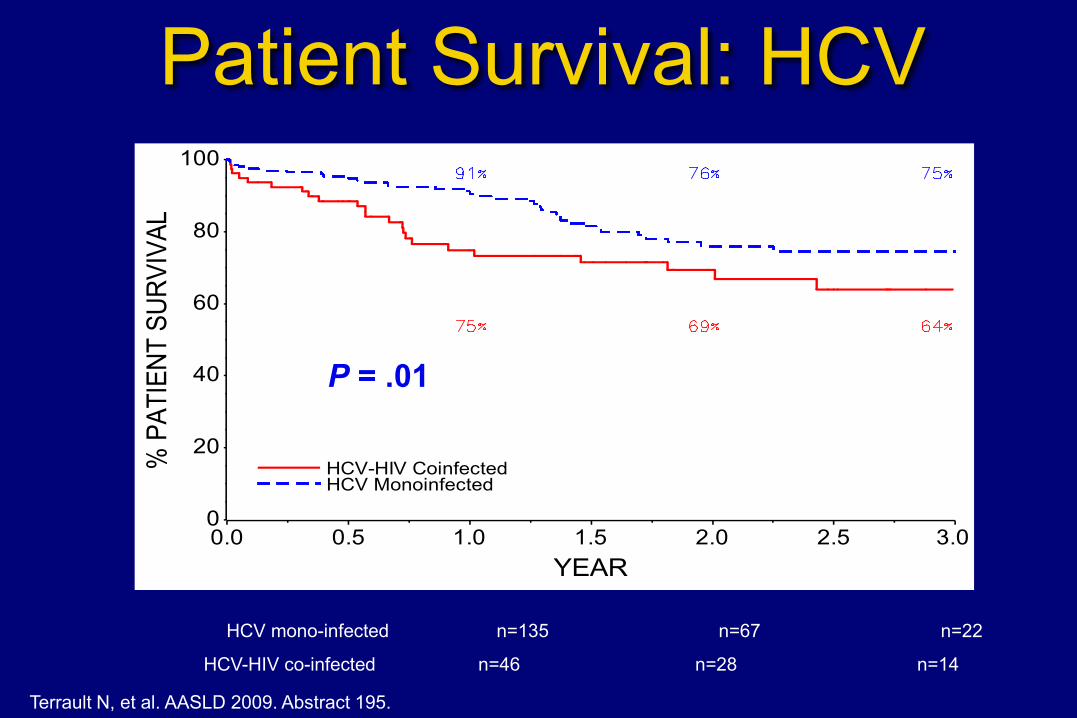
Patient Survival: HCV
P=0.01 P=0.01
HCV mono-infected n=135 n=67 n=22
HCV-HIV co-infected n=46 n=28 n=14
% P
ATIE
NT S
URVI
VAL
0
20
40
60
80
100
YEAR0.0 0.5 1.0 1.5 2.0 2.5 3.0
HCV-HIV CoinfectedHCV Monoinfected
P = .01
Terrault N, et al. AASLD 2009. Abstract 195.
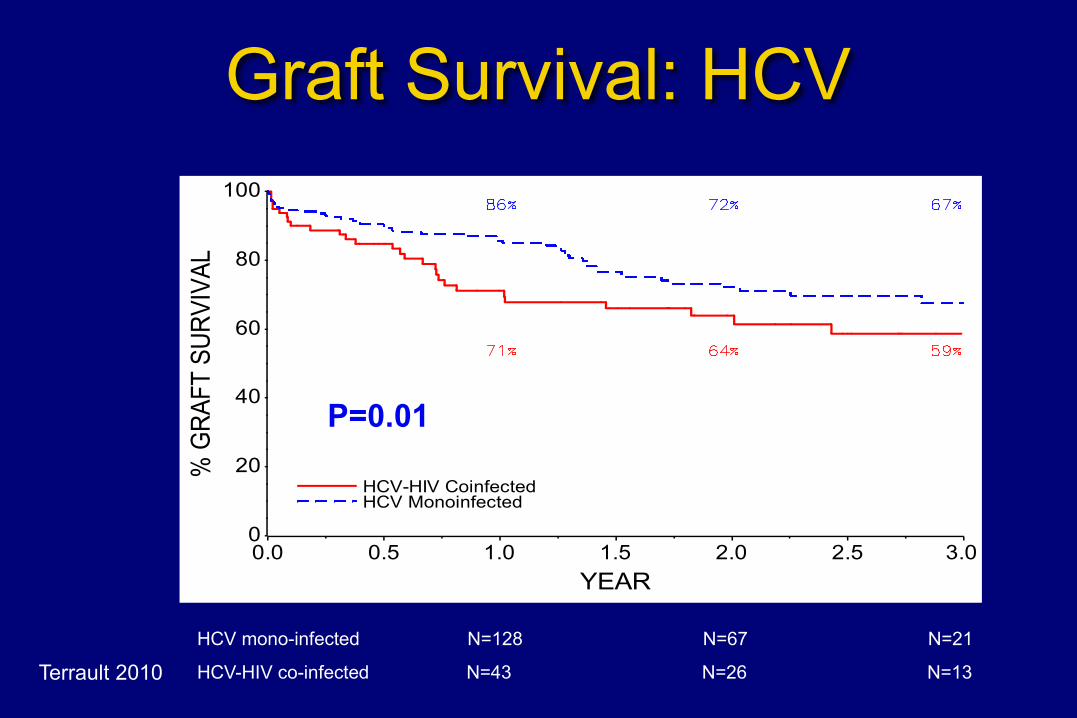
Graft Survival: HCV
P=0.01 % G
RAFT
SUR
VIVA
L
0
20
40
60
80
100
YEAR0.0 0.5 1.0 1.5 2.0 2.5 3.0
HCV-HIV CoinfectedHCV Monoinfected
HCV mono-infected N=128 N=67 N=21
HCV-HIV co-infected N=43 N=26 N=13
P=0.01
Terrault 2010
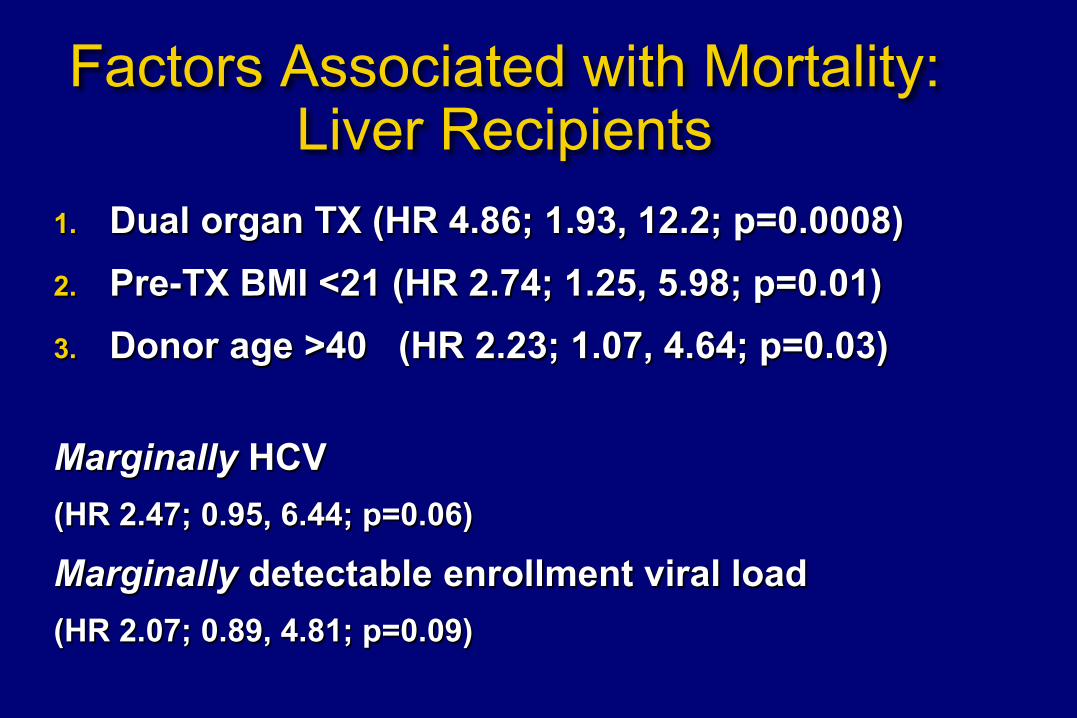
Factors Associated with Mortality: Liver Recipients
1. Dual organ TX (HR 4.86; 1.93, 12.2; p=0.0008) 2. Pre-TX BMI <21 (HR 2.74; 1.25, 5.98; p=0.01) 3. Donor age >40 (HR 2.23; 1.07, 4.64; p=0.03)
Marginally HCV (HR 2.47; 0.95, 6.44; p=0.06)
Marginally detectable enrollment viral load (HR 2.07; 0.89, 4.81; p=0.09)
HCV outcomes and implications for patient selection
Patient and graft survival in HCV-HIV co-infected transplant recipients are lower but acceptable
Not due to HIV-related complications
Outcomes may be improved by:
Restricting to BMI >21; no dual kidney transplant Avoiding use of livers from anti-HCV+ donors
Better management of acute rejection
Stock 2011
HIV and Liver Transplantation What Have We Learned?
HBV outcomes excellent and recurrent low level viremia controllable with combination HBIG and antivirals
Recurrent HCV a significant problem, with increased risk of morbidity and mortality some surprising positive outcomes (spontaneous clearance, higher
response to antiviral therapy)
HAART regimens including PI require major adjustments in CNI and sirolimus dosing
Treatment with anti-T-cell depleting agents results in prolonged depletion of CD4 positive cells
HIV and Liver Transplantation What Have We Learned?
Transplantation is an option for HIV-infected patients with endstage liver disease
Need to consider early at first decompensation
No significant HIV clinical, virologic, immunologic disease progression noted in the immunosuppressed patients
No evidence of impaired graft function due to HIV
Rejection rates unexpectedly high in HCV-infected liver transplant recipients
ESLD and HIV Liver disease has become a major cause of death in
people infected with HIV Prevalence of HCV coinfection is high (30%) Prevalence of HBV coinfection ~ 10% Progression to cirrhosis is rapid in coinfected pt ESLD common Monitor ascites and infection (SBP prophylaxis) EGD for varices, imaging for HCC Consider OLT early