Embed Size (px)
Citation preview
Evaluating HIV Patient for Liver Transplantation
Marion G. Peters, MD Professor of Medicine
University of California San Francisco USA
Slide 2
ESLD and HIV • Liver disease has become a major cause of death
in people infected with HIV • Prevalence of HCV coinfection is high (30%) • Prevalence of HBV coinfection ~ 10% • Progression to cirrhosis more rapid in HIV patients • End stage liver disease (ESLD) common
Slide 3
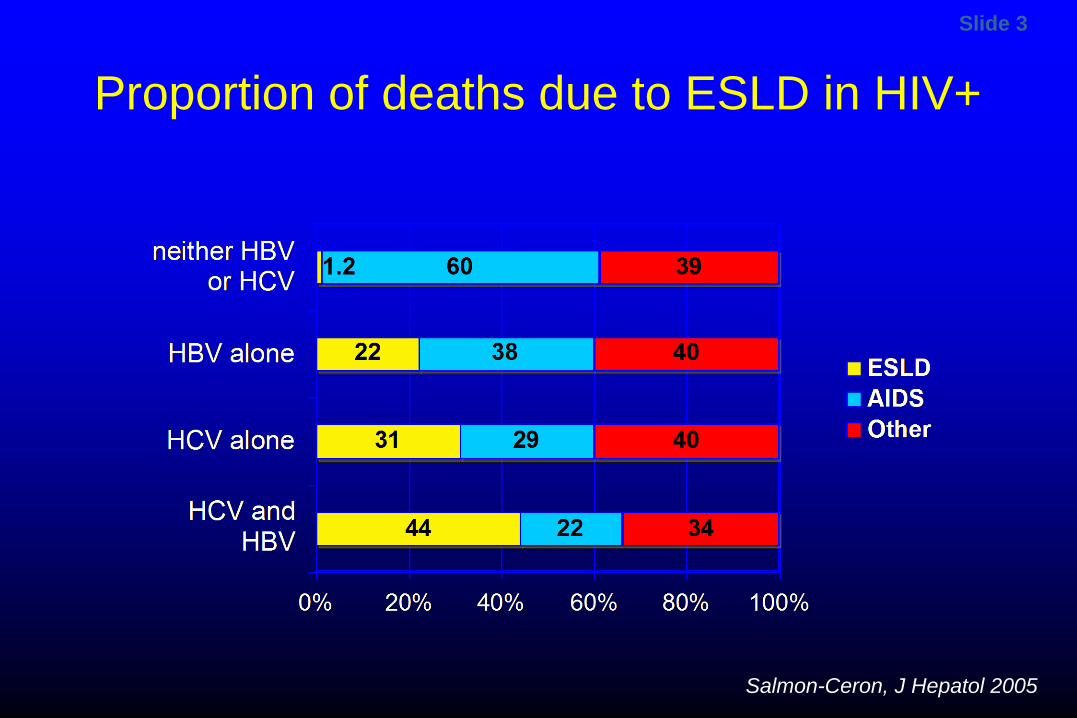
Proportion of deaths due to ESLD in HIV+
Salmon-Ceron, J Hepatol 2005
Slide 4
Complications of cirrhosis in HIV- and non-HIV-infected patients
• Ascites • Gastroesophageal variceal bleeding • Synthetic dysfunction: jaundice, coagulopathy • Spontaneous bacterial peritonitis (SBP) • Hepatic encephalopathy (HE) • Hepatorenal syndrome (HRS) • Hepatocellular carcinoma (HCC)
Cardenas & Gines, J Hepatol, 2005; Bruix J, J Hepatol, 2001
Slide 5
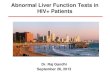
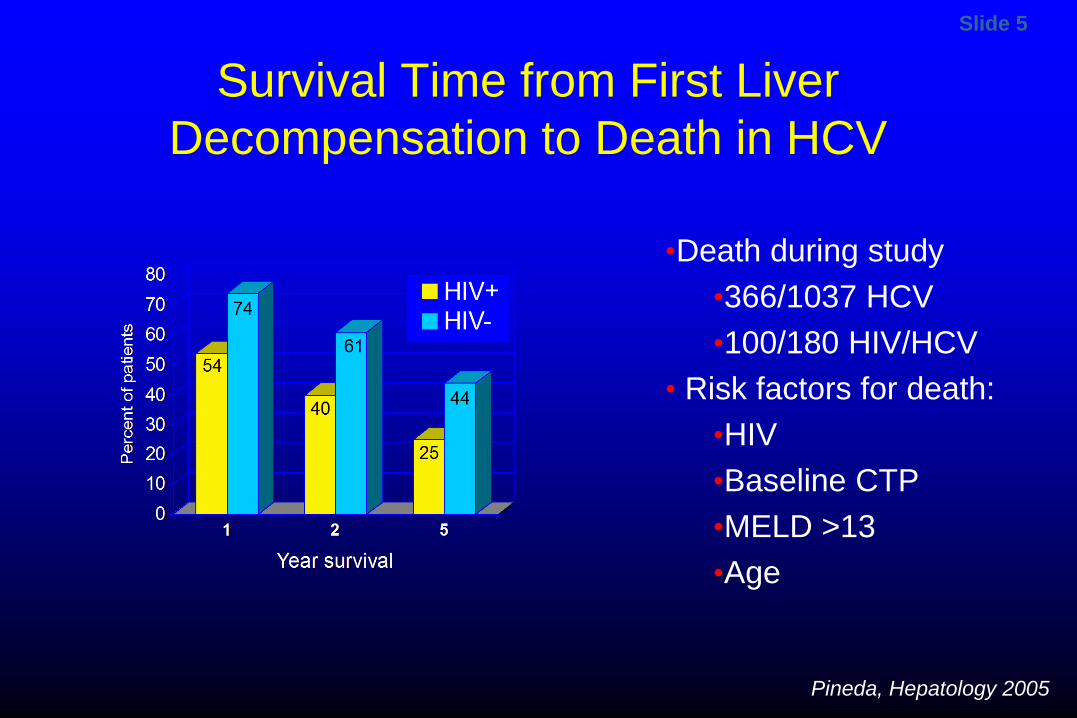
Survival Time from First Liver Decompensation to Death in HCV
Pineda, Hepatology 2005
•Death during study •366/1037 HCV •100/180 HIV/HCV
• Risk factors for death: •HIV •Baseline CTP •MELD >13 •Age
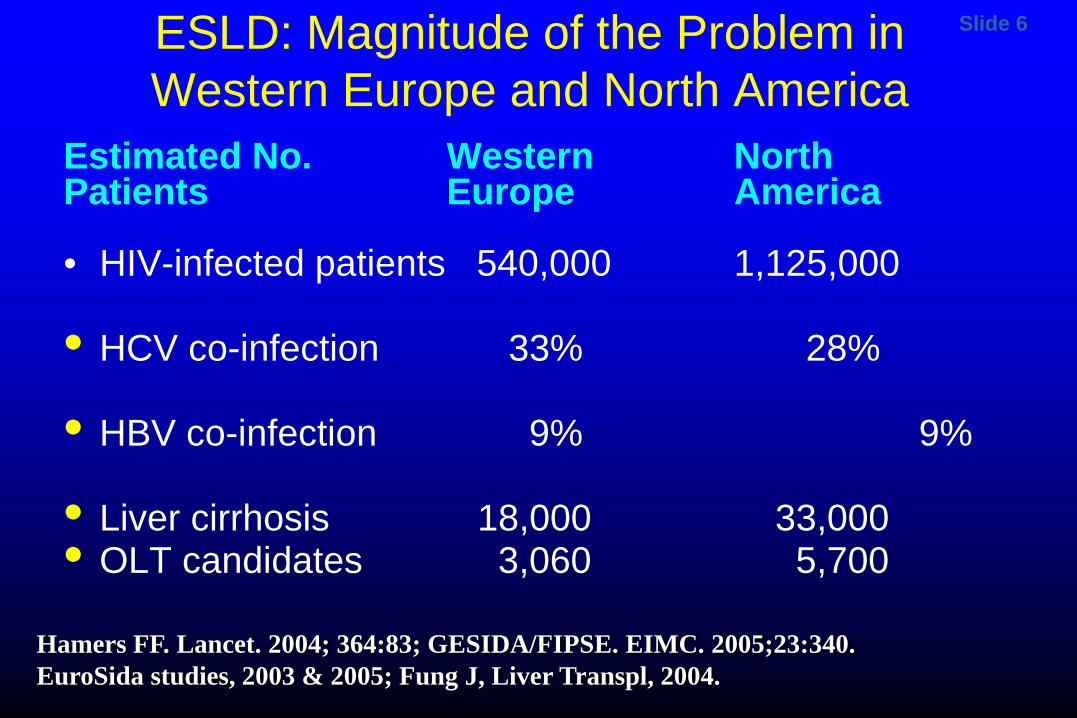
Slide 6 ESLD: Magnitude of the Problem in Western Europe and North America
Estimated No. Western North Patients Europe America • HIV-infected patients 540,000 1,125,000
• HCV co-infection 33% 28%
• HBV co-infection 9% 9%
• Liver cirrhosis 18,000 33,000 • OLT candidates 3,060 5,700
Hamers FF. Lancet. 2004; 364:83; GESIDA/FIPSE. EIMC. 2005;23:340.
EuroSida studies, 2003 & 2005; Fung J, Liver Transpl, 2004.
Slide 7
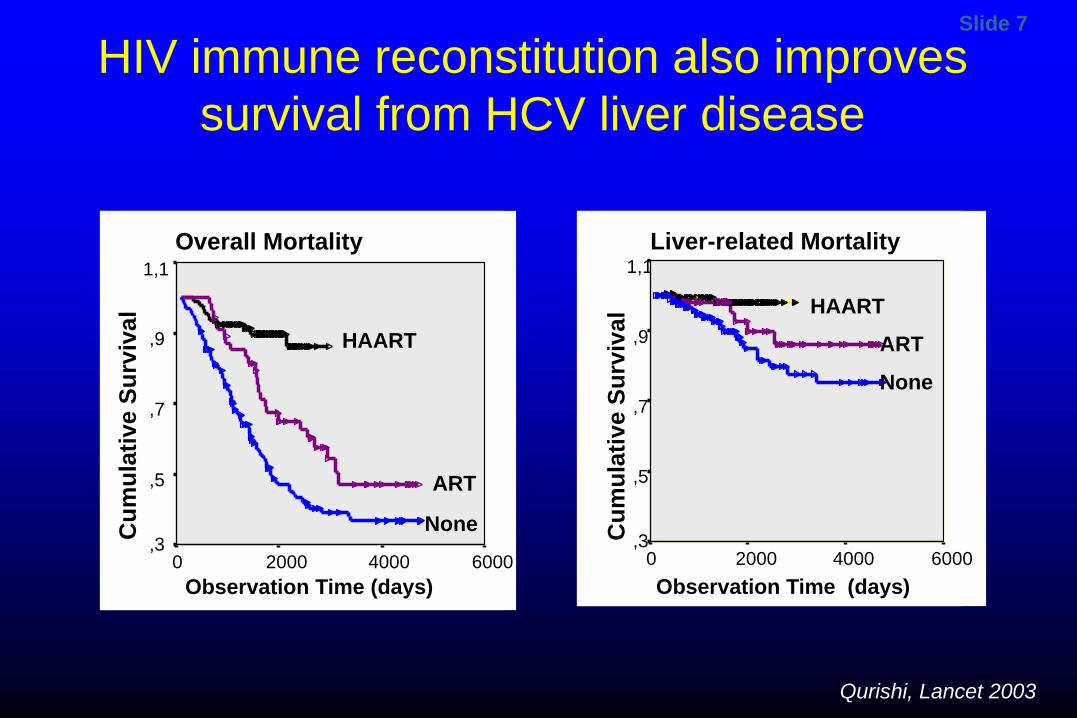
Overall Mortality
Observation Time (days) 6000 4000 2000 0
Cum
ulat
ive
Surv
ival
1,1
,9
,7
,5
,3
Liver-related Mortality
Observation Time (days) 6000 4000 2000 0
Cum
ulat
ive
Surv
ival
1,1
,9
,7
,5
,3
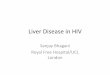
HAART
ART HAART
ART
None
None
HIV immune reconstitution also improves survival from HCV liver disease
Qurishi, Lancet 2003
Slide 8
Management of ESLD Cirrhotics • Upper endoscopy
– Varices or portal gastropathy, non selective beta blockers • Ascites: diuretics, paracentesis, TIPS, SBP
prophylaxis • Evaluate for HCC
– Liver imaging, alpha fetoprotein q 6-12 monthly • If decompensated
– Refer for possible transplant • Do not treat decompensated HCV with IFN
Slide 9
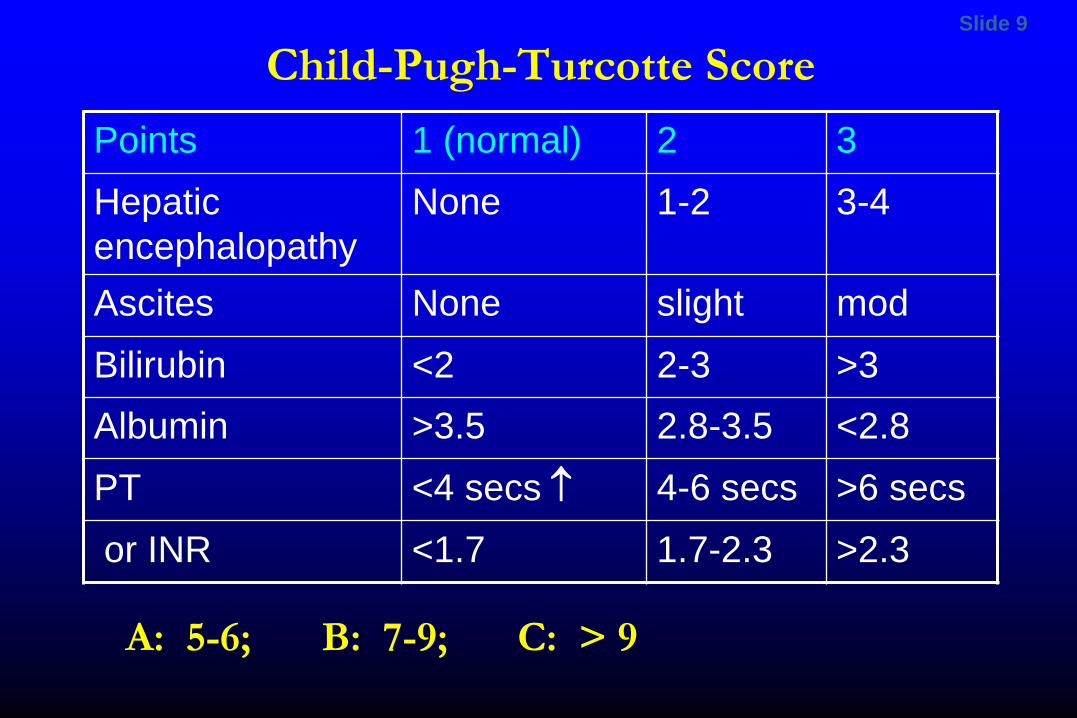
Child-Pugh-Turcotte Score Points 1 (normal) 2 3 Hepatic encephalopathy
None 1-2 3-4
Ascites None slight mod Bilirubin <2 2-3 >3 Albumin >3.5 2.8-3.5 <2.8 PT <4 secs ↑ 4-6 secs >6 secs
or INR <1.7 1.7-2.3 >2.3
A: 5-6; B: 7-9; C: > 9
Slide 10
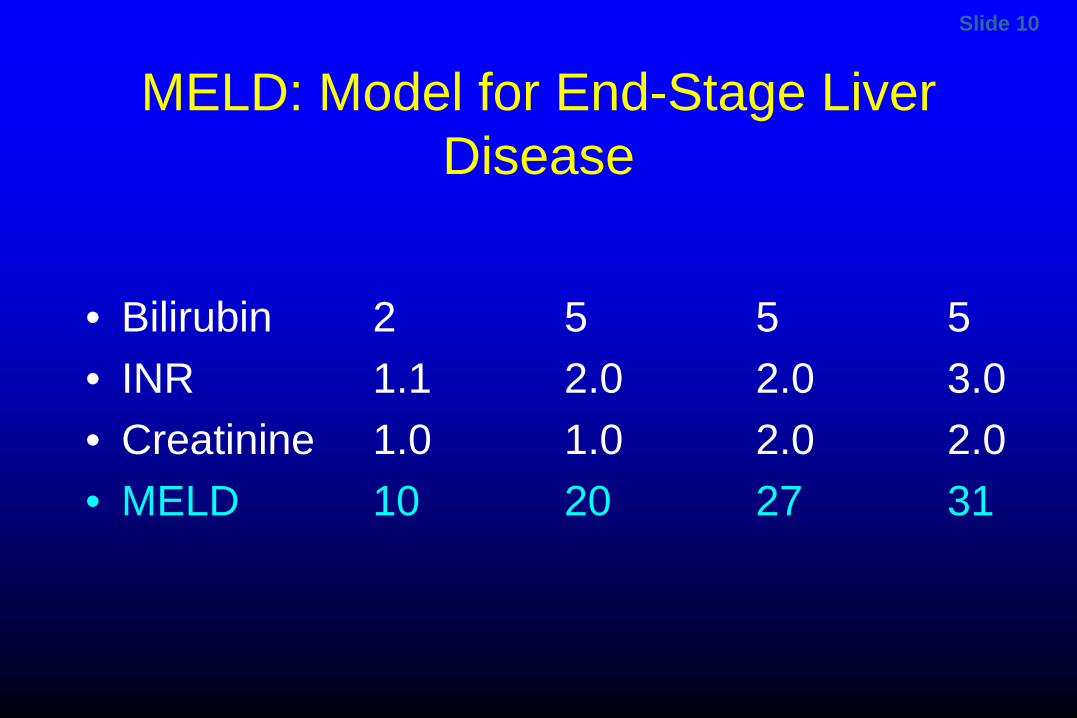
MELD: Model for End-Stage Liver Disease
• Bilirubin 2 5 5 5 • INR 1.1 2.0 2.0 3.0 • Creatinine 1.0 1.0 2.0 2.0 • MELD 10 20 27 31
Slide 11
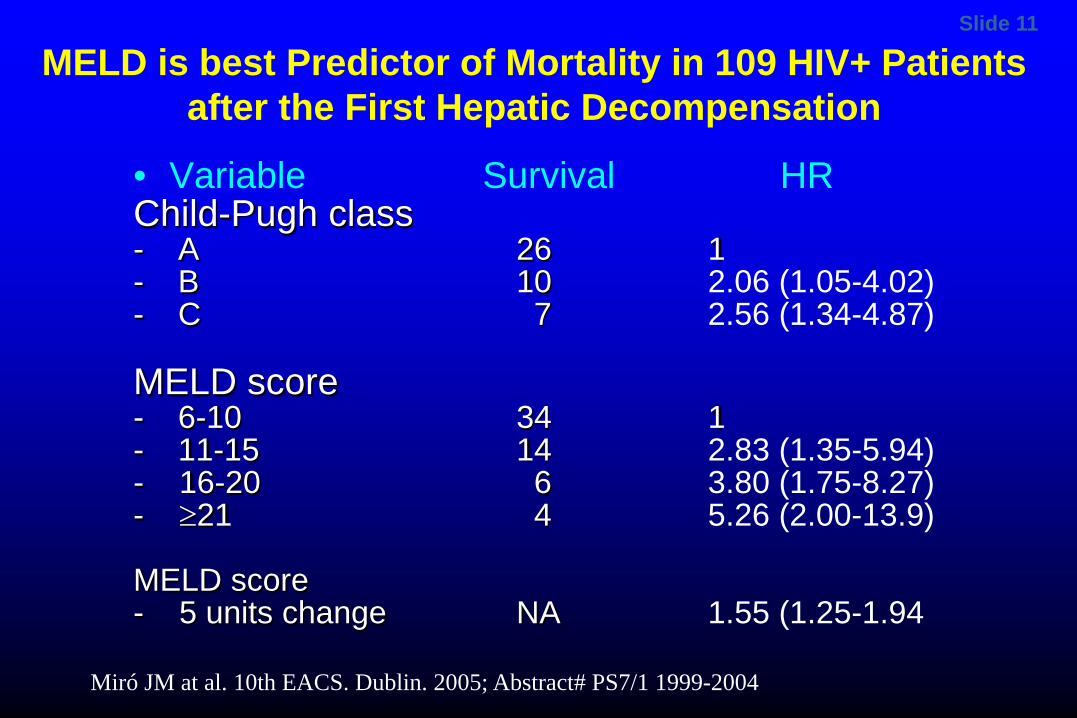
MELD is best Predictor of Mortality in 109 HIV+ Patients after the First Hepatic Decompensation
• Variable Survival HR Child-Pugh class - A 26 1 - B 10 2.06 (1.05-4.02) - C 7 2.56 (1.34-4.87)
MELD score - 6-10 34 1 - 11-15 14 2.83 (1.35-5.94) - 16-20 6 3.80 (1.75-8.27) - ≥21 4 5.26 (2.00-13.9) MELD score - 5 units change NA 1.55 (1.25-1.94 Miró JM at al. 10th EACS. Dublin. 2005; Abstract# PS7/1 1999-2004
Slide 12 OLT in HIV: Why Now? • HAART-associated improvements:
– decreased mortality – decreased incidence of opportunistic infections – decreased hospitalization rates
• Immunosuppressives may have anti-HIV effects – cyclosporine, MMF, rapamycin
• Better prophylaxis for opportunistic infections Patients: CD4+ T-cell count > 100 for liver recipients HIV RNA undetectable or if predicted to suppress OIs excluded PML, cryptosporidiosis and visceral KS
Slide 13
Indications for Liver Transplantation
• Liver decompensation – Development of decompensation (ascites,
variceal hemorrhage, Hepatic encephalopathy) in patients with cirrhosis is associated with a 5y survival of <50% (cf HIV 25%)
• Hepatocellular carcinoma- if small, contained – 3 lesions largest <3 cm – 1 lesion <5 cm
Slide 14
Pre OLT – what can you do?
• Pretransplant monitor for – Varices- yearly if decompensated- beta blockers – Ascites- tap for spontaneous bacterial peritonitis – Ultrasound / CT for HCC
– HCV treatment – HBV antivirals to ensure HBV DNA undetectable
Slide 15
HCV Pre OLT – what can you do? • HCV Pretransplant
– Treat select patients to eradicate HCV if MELD <20 – If HCV RNA positive at OLT then 100% post OLT – Peg IFN- problems with low platelets, WBC, infections – RBV- problems with anemia, renal insufficiency – BOC, TPV with PR- lots of side effects – All oral DAAs ideal here
• Donor – Careful donor selection
Slide 16 The Process- Phase I • How Referred: In patient -FHF • Out patient- hepatologist • Evaluation: Phase I
– Nurse coordinator – Hepatologist – Surgeon – Social Worker, support group – Labs: HBV, HCV, HIV, ABO blood group, MELD – Ultrasound, Doppler
Slide 17
OLT- The Process • Patient referred to hepatologist • Do they need a liver?
– MELD: • Is there a contraindication?
– Severe medical disease – Cancer – Psychosocial
• Does the patient want one?
Slide 18
OLT listing • Need for OLT
– MELD: creatinine, bilirubin, INR – Decompensation: albumin, INR, ascites,
encephalopathy, variceal bleed • Contraindication
– Medical- • AIDS defining illness • cardiac, renal, pulmonary disease, • extrahepatic cancer
– Social, psychiatric
Slide 19 Inclusion Criteria for OLT in HIV-infected patients in USA
• Liver criteria: same as for non HIV-infected • Drug abuse: same as for non HIV-infected • HIV criteria: 1) Clinical: untreatable OI’s: PML, crypto, MDR fungal
infection, Lymphoma, non cutaneous KS 2) Immunological: pre-decomp CD4 cell count greater
than 100 cells/mm3 3) Virological: RNA HIV-1 viral load u/d on ART or, if
detectable, post-OLT suppression predicted
Slide 20
OLT- The Process-2
• Phase I evaluation • Present to selection conference • If approved Phase II
– Cardiac, pulmonary, ca, renal • Sickest patient offered first by MELD • For Live donor, recipient must meet standard
criteria
Slide 21
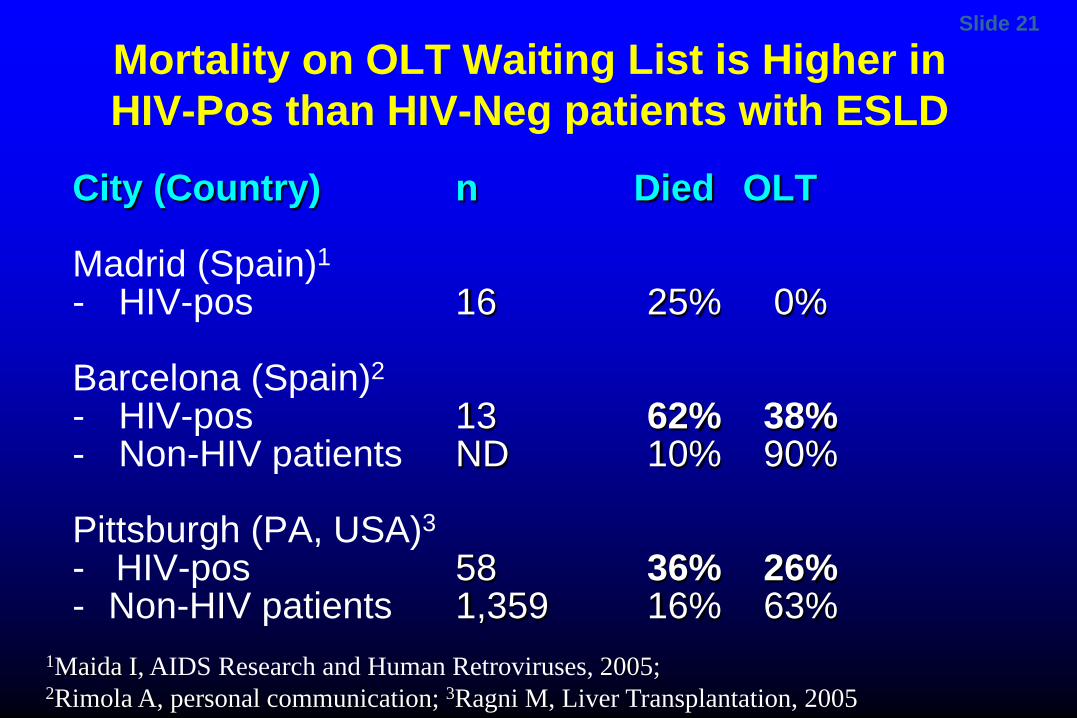
Mortality on OLT Waiting List is Higher in HIV-Pos than HIV-Neg patients with ESLD
City (Country) n Died OLT Madrid (Spain)1
- HIV-pos 16 25% 0% Barcelona (Spain)2
- HIV-pos 13 62% 38% - Non-HIV patients ND 10% 90% Pittsburgh (PA, USA)3
- HIV-pos 58 36% 26% - Non-HIV patients 1,359 16% 63%
1Maida I, AIDS Research and Human Retroviruses, 2005; 2Rimola A, personal communication; 3Ragni M, Liver Transplantation, 2005
Slide 22
HIV and Liver Disease: OLT • Refer for any decompensation:
– ascites, encephalopathy, UGIB – synthetic dysfunction
• Refer early • Many issues confound ability to reach OLT
– Medical, social, geography, insurance • Need to fulfill listing criteria
– Medical – Psychosocial
• Need multidisciplinary approach
Slide 23
Liver Transplantation • MELD • Serum sodium • Underestimated
– chronic encephalopathy – hepatic hydrothorax – hepatopulmonary syndrome – portopulmonary hypertension
Slide 24
Post OLT – what can you do?
• Immunosuppression (IMS) modulation – steroid and calcineurin inhibitor (CNI)
minimization – Avoid T-cell-depleting treatments, acute rejection – control of metabolic problems- BMI, DM – Start Rx prior to significant damage to the
allograft is strongly recommended.
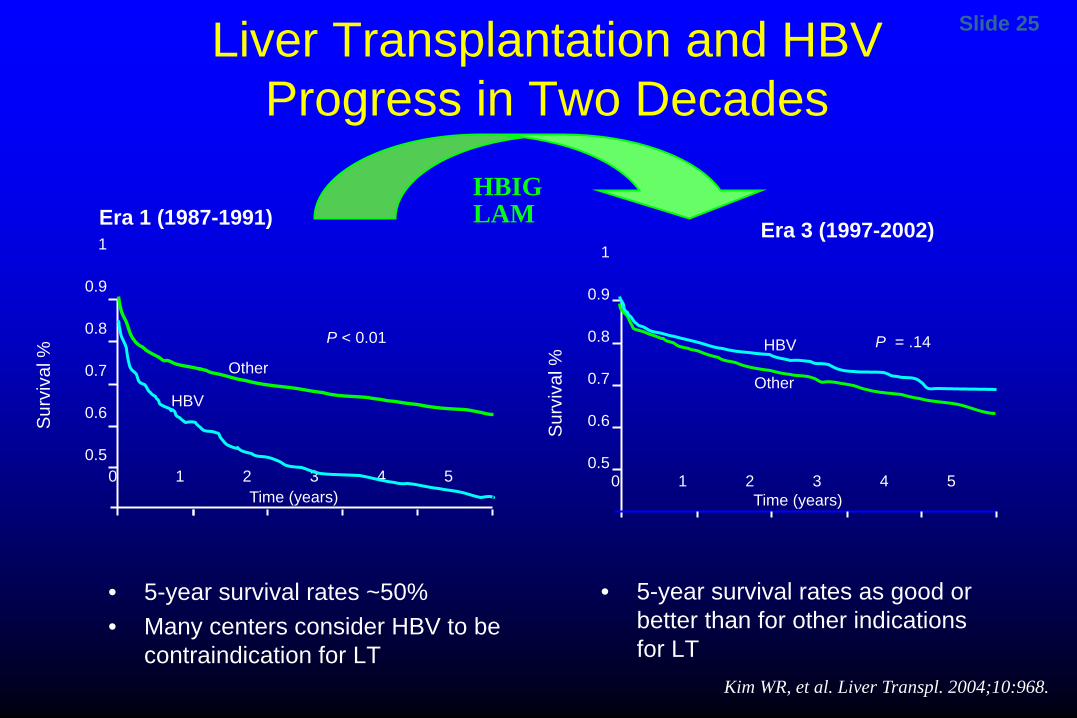
Slide 25
1
0.9
0.8
0.7
0.6
0.5 0 1 2 3 4 5
Surv
ival
%
Era 3 (1997-2002)
Time (years)
P = .14
Other
HBV
1
0.9
0.8
0.7
0.6
0.5 0 1 2 3 4 5
Surv
ival
%
Era 1 (1987-1991)
Time (years)
P < 0.01
Other
HBV
Kim WR, et al. Liver Transpl. 2004;10:968.
Liver Transplantation and HBV Progress in Two Decades
• 5-year survival rates ~50% • Many centers consider HBV to be
contraindication for LT
• 5-year survival rates as good or better than for other indications for LT
HBIG LAM
Slide 26
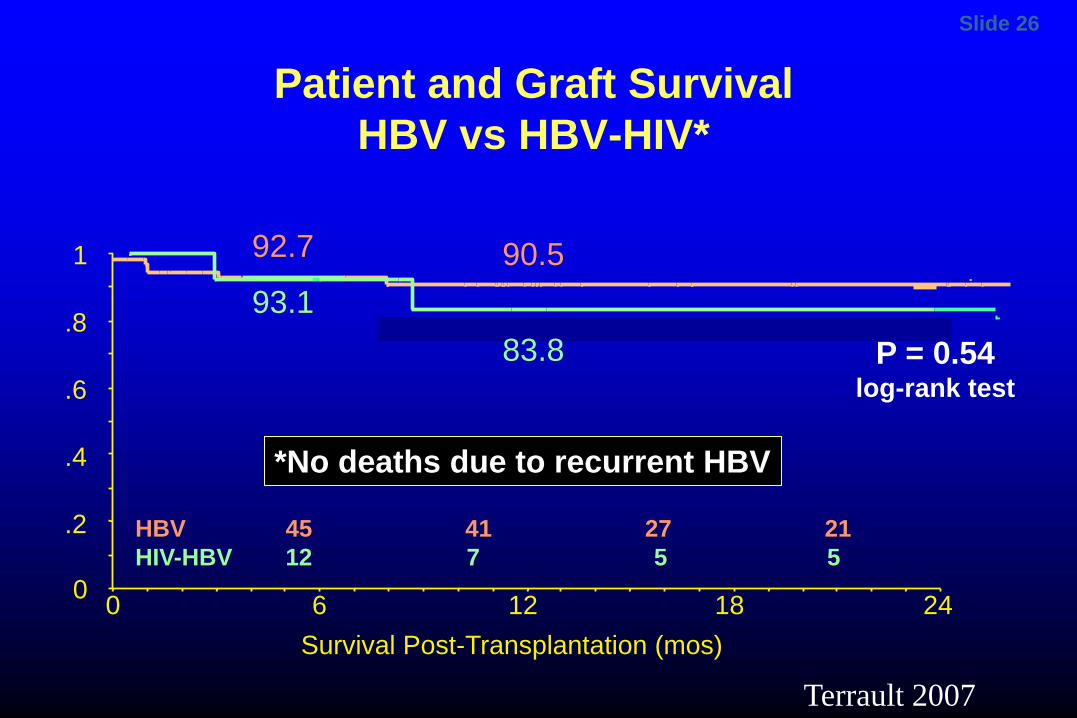
HBV 45 41 27 21 HIV-HBV 12 7 5 5
93.1
92.7
Patient and Graft Survival HBV vs HBV-HIV*
90.5
*No deaths due to recurrent HBV
Survival Post-Transplantation (mos) 24 18 12 6 0
1
.8
.6
.4
.2
0
P = 0.54 log-rank test
83.8
Terrault 2007
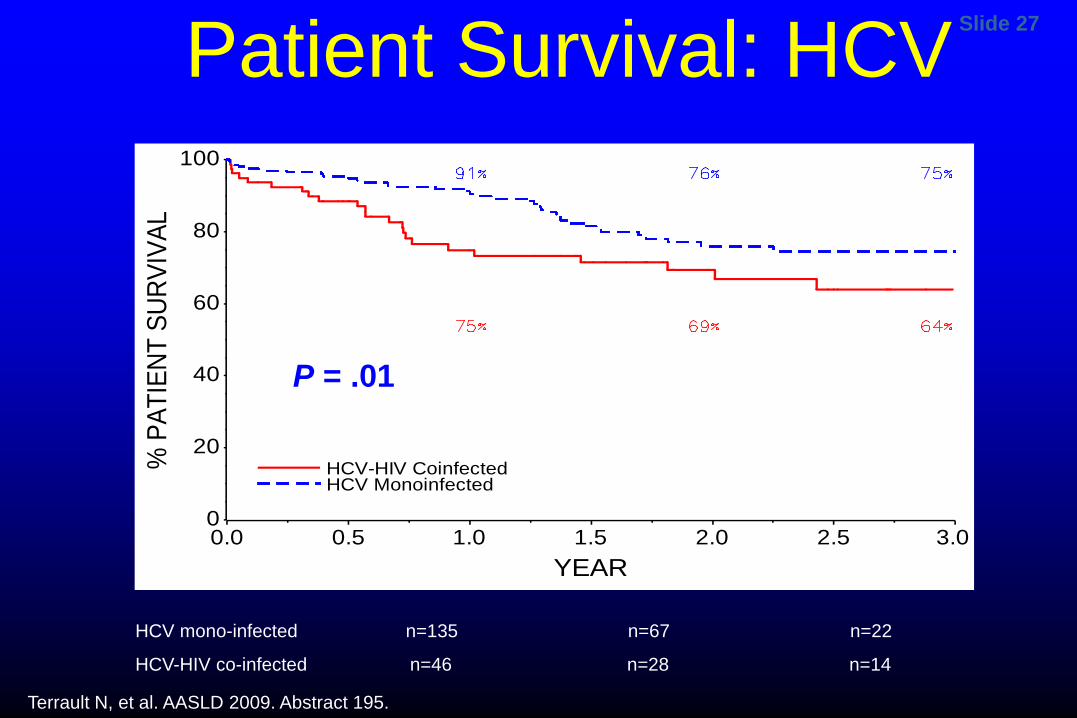
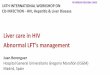
Slide 27 Patient Survival: HCV
P=0.01 P=0.01
HCV mono-infected n=135 n=67 n=22
HCV-HIV co-infected n=46 n=28 n=14
% P
ATIE
NT S
URVI
VAL
0
20
40
60
80
100
YEAR0.0 0.5 1.0 1.5 2.0 2.5 3.0
HCV-HIV CoinfectedHCV Monoinfected
P = .01
Terrault N, et al. AASLD 2009. Abstract 195.
Slide 28
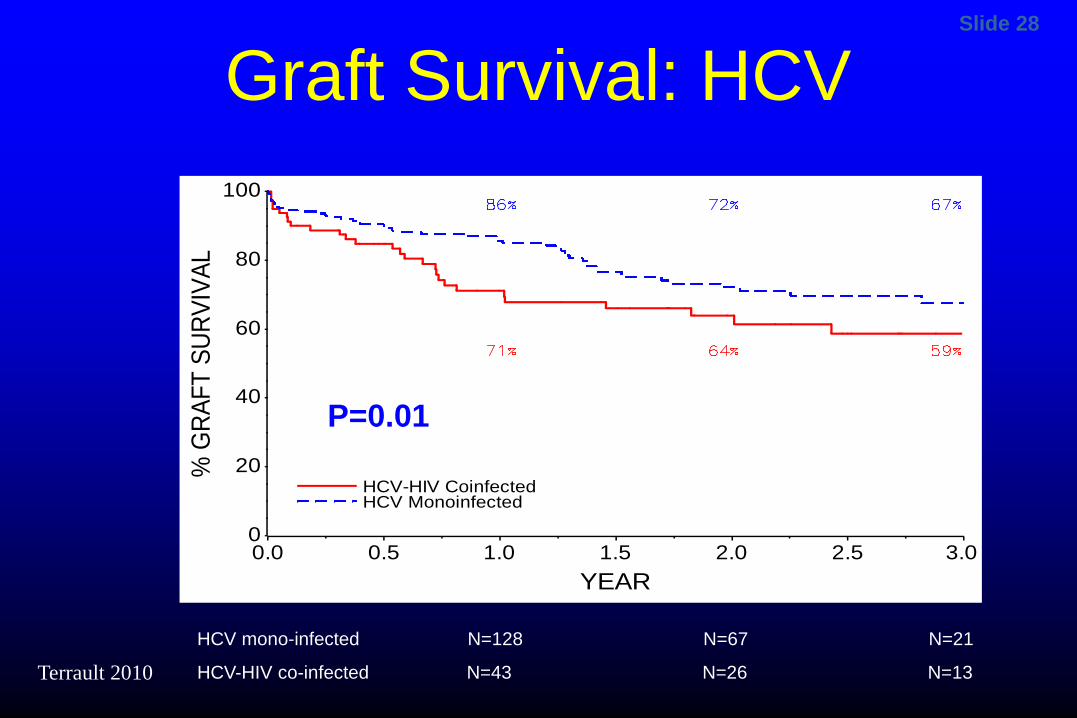
Graft Survival: HCV
P=0.01 % G
RAFT
SUR
VIVA
L
0
20
40
60
80
100
YEAR0.0 0.5 1.0 1.5 2.0 2.5 3.0
HCV-HIV CoinfectedHCV Monoinfected
HCV mono-infected N=128 N=67 N=21
HCV-HIV co-infected N=43 N=26 N=13
P=0.01
Terrault 2010
Slide 29
HIV and Liver Transplantation What Have We Learned?
HBV outcomes excellent and recurrent low level viremia controllable with combination HBIG and antivirals Recurrent HCV a significant problem, with increased risk of
morbidity and mortality some surprising positive outcomes (spontaneous
clearance, higher response to antiviral therapy) HAART regimens including PI require major adjustments in
CNI and sirolimus dosing Treatment with anti-T-cell depleting agents results in
prolonged depletion of CD4 positive cells
Slide 30
HCV outcomes and implications for patient selection
Patient and graft survival in HCV-HIV co-infected transplant recipients are lower but acceptable Not due to HIV-related complications
Outcomes may be improved by: Clearing HCV prior to OLT Restricting to BMI >21; no dual kidney transplant Avoiding use of livers from anti-HCV+ donors Better management of acute rejection
Stock 2011
Slide 31
HCV/HIV and Liver Transplantation Recurrence is universal and disease progression
appears to be more rapid post-transplantation No effective form of prophylactic therapy Antiviral therapy (peg/interferon plus ribavirin
+DAA) some successes Therapies are suboptimal Limited tolerability (higher rate of treatment
discontinuation) All oral DAA clearing HCV will improve outcomes post
OLT Post OLT DAA PI drug drug interactions with CNI
Slide 32
HIV and Liver Transplantation HBV and HCV are the most common causes of
chronic liver disease in HIV-infected persons Most transplant programs HCV>>HBV
Liver disease progression is accelerated in persons with viral hepatitis and HIV coinfection (compared to HIV un-infected persons)
With use of HAART, the number of liver-related deaths is increasing among HIV-infected persons
New DAA therapies should improve HCV outcomes