Embed Size (px)
Citation preview

LIPIDS AND ATHEROSCLEROSIS
IN FAMILIES

ACKNOWLEDGEMENTS
The studies described in tltis thesis were funded by the Netherlands Heart Foundation and the
Netherlands Prevention Fund. Financial support by the Netherlands Heart Foundation for the
publication of this thesis is gratefully acknowledged. The author also gratefully acknowledges
the contribution of the following organizations to the publication of this thesis: Romeres
Foundation, the Netherlands Institute for Health Sciences, Merck Sharpe & Dolune BV, Pfizer
BV, Parke-Davis BV, Byke Nederland BV, Vpjohn-Nederland.
Cover: Cecile Janssens, HFamily portrait'\ 1995
~edrukt door: Drukkerlj Haveka B.V., Alblasserdam
ISBN 90-9008391-X
© C.S.P.M. Viterwaal, 1995
No part of this book may be reproduced, stored in a retrieval system or transmitted in any other fonn or by any means, without pennission of the author, or, when appropriate, of the publishers of the publications.

LIPIDS AND ATHEROSCLEROSIS IN FAMILIES
Lipiden en atherosclerose in families
PROEFSCHRIFT
Ter verkrijging van de graad van doctor
aan de Erasmus Universiteit Rotterdam
op gezag van de rector magnificlls
Prof. Dr. P.W.C. Akkermans M.A.
en volgens besluit van het College voor Promoties.
De openbare verdediging zal plaatsvinden op
woensdag 7 juni 1995 om 11.45 uur
door
Cunibert Stephan Philip Maria Uiterwaal
geboren te Utrecht

PROMOTIECOMMISSIE
Promotores:
Co-promotor:
Overige leden:
Prof. Dr. D.E. Grobbee
Prof. Dr. A. Hofman
Dr. Ir. J.C.M. Witteman
Prof. Dr. J.C. Birkenhager
Prof.Dr. J. Hess
Prof. Dr. J.F. Koster

CONTENTS
1. Introduction
1.1 Rationale
1.2 Study objectives
1.3 Chapter outline
Appendix
2. Postprandial triglyceride response in young adult men and familial risk for
coronary atherosclerosis
3. Lipoproteins and apolipoproteins in young adult men and women and
risk for coronary atherosclerosis
4. Families and natural history of lipids in childhood:
an 18 year follow-up study
5. General discussion I
6. General discussion II
7. Summary
Samenvatting
nankwoord
About the author
1
2
4
5
6
15
39
5S
73
85
93
96
99
101

Chapter 2
PUBLICATIONS AND MANUSCRIPTS BASED ON THE
STUDIES DESCRIBED IN THIS THESIS
Uiterwaal CSPM, Grobbee DE, Witteman JCM, van Stiphout W AHJ, Krauss XH, Havekes
LM, de Bruijn AM, van Tol A, Hofman A. Postprandial triglyceride response in young adult
men and familial risk of coronary atherosclerosis. Ann Intern Med 1994;121;576-583.
Uiterwaal CSPM, Witteman JCM, Grobbee DE. Triglyceride levels in sons of patients with
coronary artery disease (Re). Ann Intern Med 1995;122:475-6.
Chapter 3
Uiterwaal CSPM, Witteman JCM, van Stiphout W AHJ, Krauss XH, de Bruijn AM, Hofman
A, Grobbee DE. Lipoproteins and apolipoproteins in young adults and risk of coronary
atherosclerosis. Submitted.
Chapter 4
Uiterwaal CSPM, Witteman JCM, de Bruijn AM, Hofman A, Grobbee DE. Families and
natural history of lipids in childhood: an 18 year follow-up study. Submitted.
Chapter 5
Uiterwaal, CSPM, Witteman JCM, Hofman A, Grobbee DE. Pitfalls in the patient-offspring
study. Submitted.

CHAPTER I
INTRODUCTION

1. Introduction
1.l Rationale
In most industrialized countries, age-standardized cardiovascular disease mortality rates have
shown a decreasing trend since the mid seventies (I). However, cardiovascular diseases are
still the most important cause of morbidity and mortality in these countries. About one-half
of the cardiovascular disease mOliality results from coronary heart disease and about one
quarter from cerebrovascular disease. The main underlying process in these diseases is
aUterosclerosis. Symptomatic atherosclerotic cardiovascular disease is predominantly a disease
of the adult population. However, there is increasing evidence to suggest that the
atherosclerotic process begins in childhood. Enos et al. (2) showed that a majority of young
soldiers autopsied during the Korean war had significant atherosclerotic lesions in their
coronary arteries. Subsequently, Holman et al. (3) showed that lesions are present in the aorta
of children. McNamara et al. (4) autopsied American soldiers killed in action in Vietnam and
reported that 45% of them had atherosclerotic lesions, and as much as 5% had severe coronary
atherosclerosis. These and more recent observations (5-10) from autopsy studies clearly
showed the onset of atherosclerotic coronary ariery disease by young adulthood. Similarly,
autopsy studies suggested the presence of potential precursors of atherosclerotic lesions such
as fatty streaks and fibrous plaques, or raised lesions, in the coronary arteries as early as the
second decade of life (3, 11-13). In a recent report from the Bogalusa Heart Study (15),
extensive intimal surface involvement with fatty streaks of the aorta and the coronary arteries
was found in young adults, aged 6 to 30 years. Fibrous plaques were found in both the aorta
and the coronaries. In the coronary arieries higher correlations of fatty streaks with raised
fibrous plaques lesions were found than in the aorta. Pariicularly in the coronary arieries, the
fatty streak lesion is a likely precursor of fibrous plaques (15). The above-mentioned studies
reporting on vessel lesions in children and young adults made use of autopsies for their
assessment. Recently, standardized noninvasive techniques for examining the carotid arteries
of children and young adults have been developed (16), which potentially extends the
possibilities for research on vessel wall characteristics to a more general population of children
and young adults. Ultrasonic examinations in children have indicated that differences in the
elastic properties of carotid arteries in children and young adults are detectable and relate to
various risk factors for atherosclerotic cardiovascular disease and also to parental heart disease
(17).
Cholesterol and cholesterol esters have since long been recognized to be a constituent of
-2-

Chapter I
atherosclerotic lesions (18-21). This has led to the assumption that plasma lipids, and more
in particular plasma low density lipoprotein cholesterol, play an essential role in the process
of atherosclerosis. In non-human primates, cholesterol feeding was shown to be a prerequisite
for the development of major atherosclerosis (22,23), and later studies demonstrated that
chronic diet induced hypercholesterolemia led to fatty streak formation (24,25) similar to the
fatty streaks observed in humans. Epidemiologic and laboratory studies have identified several
risk factors contributing to the high prevalence and incidence of atherosclerotic coronary
artery disease in industrialized countries. Among these risk factors, hypertension,
hypercholesterolemia and smoking were disclosed as conditions independently linked to
atherosclerotic coronary artery disease. The positive relation of semm total cholesterol, as welt
as the inverse association of one of its subfractions, high density lipoprotein cholesterol with
atherosclerosis is now welt established. Similarly, in particular high levels of another
subfraction, low density lipoprotein cholesterol are associated with coronary artery disease
(26-32). In children and young adults, particularly males, aorta fatty streaks were found to be
strongly related to antemortem levels of total cholesterol and low density lipoprotein
cholesterol and coronary artery fatty streaks with levels of triglycerides and very low density
lipoprotein-cholesterol as welt as with systolic and diastolic blood pressure (14).
Apolipoproteins are the protein components of lipoproteins, which are involved in the
stmcture, receptor binding and enzymatic metabolism of these lipoproteins. These
apolipoproteins have been studied in patients with ischaemic heart disease (33,34) as welt as
in their offspring (35), but their relative merit as risk factors for coronary artery disease stitt
has to be elucidated.
It is since 1979 that more attention has been drawn to the possible association botween
atherosclerosis and triglyceride-rich lipoproteins that occur in plasma primarily in the
postprandial or fed state. (36) However, hypotheses about such an association date back much
earlier. Moreton (37) proposed in 1947 that it was because of investigating only casual lipid
concentrations, and primarily in the postabsorptive (fasting) state, that the clue to the
underlying etiology of atherosclerosis had been missed. Much later it was reported that the
renmants of chylomicrons, the principal carriers of dietary (exogenous) cholesterol and fat,
are atherogenic in human adults (36, 38), thus giving support to this theory. There is no
insight yet into the role of triglyceride-rich lipoproteins in the young. The finding of a strong
association between fatty streak involvement in the coronary arteries of young males and
antemortem levels of triglyceride and very low density lipoprotein-cholesterol (14) may be
an indication that triglyceride-rich lipoproteins do playa role.
In view of the process of atherosclerosis beginning in young adulthood it is worthwhile to
-3-

Chapter I
study this process in relation to semm lipids, (apo)lipoproteins and postprandial lipid
metabolism in children and young adults as a means of gaining insight into how these factors
may have contributed to the occurrence of coronary atherosclerosis in their parents. Eventually, this may not only lead to a better understanding of the etiology and the
determinants of atherosclerotic cardiovascular diseases, but also provide a means for the prevention of these diseases.
These considerations form the rationale for investigating lipids, (apo)lipoproteins and lipid
metabolism in the young in relation to disease in their parents, with emphasis on fat intake
and postprandial changes in lipid profiles. In the studies presented in this thesis lipids,
(apo)lipoproteins and postprandial lipids and lipoproteins were investigated in offspring of
parents suffering from clinically manifest and angiographically proven coronary
atherosclerosis. The natural history of lipids and lipoproteins was studied in children and
young adults in relation to parental total serum cholesterol levels.
1.2 Study objectives
A general question that may be asked is whether and how efforts to prevent cardiovascular
diseases should start with children and young adults. Prevention of a chronic disease such as
cardiovascular disease implies knowledge about the relevant risk factors in the young and their
role in the etiology of cardiovascular disease. The objectives of the studies presented in this
thesis were to assess, within the realm of familial cardiovascular disease, the causal relations between coronary artery disease as measured in adults and (apo )lipoprotein levels as measured
in their offspring as a means of studying their role in the occurrence of parental disease. A
furUler objective was to evaluate if cardiovascular risk factor levels show aggregation in
families over time by relating parental risk factor levels and offspring risk factor levels. The
latter should provide evidence for the idea that high risk parents may have offspring with high
risk factor levels, which is important in the concept of such risk factors being causally related
to the life-long process ultimately leading to cardiovascular disease. Familial aggregation of
risk factors over time is also an important premise for shldies relating offspring risk factor levels to parental disease. Thus, in view of the knowledge on both the etiology and ultimately
the prevention of atherogenesis it is important to assess whether levels of plasma lipids and
(apo)lipoproteins measured at a yomlg age are related to heart disease. Similarly, studying
postprandial lipid metabolism may provide new insights into atherogenesis and shed light on
-4-

Chapter J
predictors of heart disease.
1.3 Chapter outline
Chapter 2 describes a patient-offspring study of postpraudial lipid metabolism aud vitamin
A metabolism and their relation with coronary atherosclerosis. In chapter 3 a patient-offspring
study is presented on the relation between lipids aud (apo)lipoproteins in young people aud
coronary artery disease in their parents. Chapter 4 presents the natural history of serum total
cholesterol and lipoprotein-cholesterol levels in a follow-up study of young people in relation
to total cholesterol levels in their parents. General discussion I in chapter 5 focuses on specific
design aspects aud the interpretation of the patient-offspring study. General discussion II in
chapter 6 places the findings of the studies as presented in this thesis in the context of the
considerations in general discussion I.
-5-

Chapter}
Appendix
In this thesis the emphasis is on lipids, (apo)lipoproteins and postprandial lipoproteins as
risk factors for coronary artery disease. In the following, a short overview of lipid metabolism
and in particular lipid transport through plasma will be given.
The lipids that are predominantly found in human plasma are free cholesterol and
cholesterol esters, triglycerides, free fatty acids and phospholipids. Free cholesterol is the
principal form present in most body tissues, in particular as a structural component of cell
membranes. It is a precursor of steroid hormones produced by the adrenal gland and the
ovary. Cholesterol ester is the storage form of cholesterol found in tissues and also the
predominant form found in plasma. Cholesterol is produced by many tissues in the body but
predominantly by the liver and the intestine (newly formed) and is cleared from the body via
the faeces (free cholesterol and bile acids), cell loss (skin) and urine (steroid hormones).
Normally there is a balance between production including dietary intake and loss.
Triglycerides are synthesized from glycerol and free fatty acids in adipose tissue, the liver and
the intestine (from dietary intake). Their main role is to serve as energy supply for muscles.
They are transported through plasma as triglycerides in the core of lipoproteins. Free fatty
acids can also be transported through plasma mostly bound to albumin. Plasma phospholipids
are mainly derived from the liver and small intestine. They are important components of cell
membranes. In plasma lipoproteins they playa major role in keeping water-insoluble lipids
a soluble state.
Plasma lipoproteins are the principal carriers for the transport of lipid molecules. As
triglycerides and cholesterol esters are water-insoluble, the spherical shaped lipoproteins
contain these molecules in their core which is surrounded by a monomolecular surface layer
consisting of the arnphipathic phospholipids and free cholesterol as well as proteins. Ofthese
molecules, the hydrophobic part is directed to the lipid core and the hydrophillic part to the
water phase (plasma), thus making the lipoprotein a water-soluble particle.
Lipoproteins are commonly, and in this thesis, classified according to their density. This
density classification defines to a large extent differences in structure, composition and
metabolism. According to density the following lipoproteins can be distinguished by
increasing density and decreasing size: chylomicrons; VLDL ~ very low density lipoproteins;
IDL ~ intermediate density lipoproteins (also: VLDL remnants); LDL ~ low density
lipoproteins; HDL ~ high density lipoproteins; VHDL ~ very high density lipoproteins (also:
pre-(3 HDL).
Apoproteins are the structural protein components of lipoproteins. They play an important
-6-

Chapter I
role in lipid and lipoprotein metabolism, mainly through their interaction with enzymes and
receptors. They are, like phospholipids, important for the solubility of lipoproteins in water
phases. Specific properties of apoproteins are listed in table 1.1.
Table 1.1. Characteristics and functions of apolipoproteins.
Apoprotein Chromosome Lipoprotein Function
A·I II chylomicron, HOL Structural protein of HOL, activates
LCAT
A·2 HDL Structural protein of HOL
A·4 II chylomicron, VHOL Reverse cholesterol transport?
B·IOO 2 VLDL, IDL, LDL Structural protein of VLOL and HOL,
ligand for LDL receptor
B·48 2 chylomicron Essential for chylomicron fonnation
C·I 19 VLDL,HDL Activator of LCA 1'1
C·2 19 chylomicrons, VLDL, Cofactor of lipoprotein lipase
HDL
C·3 II VLDL,HDL Regulator of lipoprotein lipase
D 3 HDL ?
E 19 chylomicron, VLDL, Ligand for remnant and LOL receptors
IDL, HDL
Lipid transport by lipoproteins can be subdivided into three major pathways: transport of
exogenous (dietary) lipids; transport of endogenous lipids; and reverse cholesterol transport.
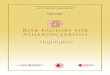
In the following these pathways and s.ome of their interrelations will be discussed. Transport through the plasma of exogenous (dietary-derived fat) is graphically depicted in figure 1.1.
After its digestion in the intestinal lumen, dietary fat is taken up by mucosal cells in the
duodenum and proximal jejunum (figure 1.1). In the enterocytes dietary free fatty acids and
monoglycerides are reesterified to form triglycerides. Phospholipids are synthesized as well.
Part of the dietary cholesterol is esterified to cholesterol ester. Subsequently, these lipids are
combined into chylomicrons. Chylomicrons are the largest and lightest of lipoproteins. Newly
-7-

Chapter J
formed chylomicrons contain apoproteins A-I, A-IV and B48, large quantities of triglyceride
and smaller anlOunts of phospholipid and cholesterol ester. They are transported from the
intestine through the lymphatic system and they enter the circulation via the thoracic duct,
where they acquire the apoproteins C-II and E from HDL.
Intestine Chylomicrons Chylomicron remnants
Liver
> TO E ~ Remnant LPL ~ CE receptor
~
Figure 1.1. Exogenous lipid transport. TO = triglyceride; CE = cholesterol ester; A-I, A-IV, BAS, C-JI and E are apoproleins.
Through the enzyme lipoprotein lipase (LPL), which is found on the luminal surface of
endothelial cells in almost all tissues, and which is activated by the apoprotein C-II,
triglycerides are hydrolized and taken up by the tissues. The remaining chylomicron remnants
are then taken up by the liver via receptors that recognize apoprotein E. Apoprotein E enters
the plasma mainly from the liver. There are three major isoforms namely E2, E3, E4. These
isoforms are coded for by three different alleles that determine six apoprotein E phenotypes:
E21E2, E21E3, E21E4, E31E3, E31E4, E41E4. Lipoprotein remnant clearance from the plasma
is sensitive for apoprotein E polymorphism and is reported to be slower in subjects with
E21E2 phenotypes. lsoforms E3 and E4 interact readily with the LDL receptor while E2 does
not. An LDL receptor related protein in the liver may also bind apoprotein E rich lipoproteins
such as chylomicrons and their remnants. During the delipidation process the apoproteins A
and C, phospholipids and free cholesterol are transferred from chylomicrons to HDL. All
cholesterol esters end up in the chylomicron remnants.
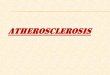
The endogenous pathway (figure 1.2.) encompasses the transport of triglycerides and
cholesterol as synthesized by the liver. These lipids are transported through the plasma by
-8-

Chapter J
liver-derived VLDL to sites of storage and utilization.
Newly formed VLDL contains apoproteins B-IOO, E and C-II, the latter also being
transferred from HDL. Delipidation of VLDL may be compared with that of chylomicrons.
During deli pi dation the VLDL lose apoprotein C-II. Most of the VLDL forms lDL (VLDL
remnants). lDL may subsequently be taken up by the liver through liver receptors recognizing
apoprotein E; or it may lose more triglycerides via the enzyme hepatic triglyceride lipase
(HTGL) and apoprotein E to HDL and be converted into LDL. LDL contains free cholesterol
and cholesterol ester (60 - 70% of total plasma cholesterol) and apoprotein B-IOO as its only
constituent apoprotein. LDL is cleared from the plasma mainly by the liver through the well
established LDL-receptors which recognize apoprotein B-IOO as well as apoprotein E.
Liver
LDL Receptors ------..
~
IDL
VLDL
Figure 1.2. Endogenous lipid transport. TG = triglyceride; CE = cholesterol ester; B-lOO, C-I1 and E are apoproleins. VLDL = very low density lipoprotein; IDL = intermediate density lipoprotein; LDL = low density lipoprotein; LPL = lipoprotein lipase; HTGL = hepatic triglyceride lipase.
This receptor plays an important role in cholesterol homeostasis. Whenever cells have excess
supply via the receptor of free cholesterol molecules they down-regulate the synthesis of LDL
-9-

Chapter J
receptor protein as well as the synthesis and activity of enzymes (HMG-CoA-reductase)
involved in de-novo synthesis of cholesterol.
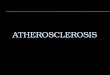
A surplus of cholesterol in extrahepatic cells can be removed by a process called reverse
cholesterol transp0l1 for which a putative scheme is shown in figure 1.3.
HDL plays a key role in reverse cholesterol transport. Newly formed HDL's are precursor
lipoproteins with a discoidal shape, containing phospholipids, free cholesterol and
predominantly apoproteins A-I and A-II, but also apoprotein E. There are two commonly
described sources of HDL. There are nascent HDL of liver and intestinal origin and there are
discoidal lipoproteins (surface material) which are formed during lipolysis of chylomicrons
and VLDL. An additional third putative source is shown in figure 1.3. It is proposed to be
Uver
r~-<f--' CB1l'
LDL Receptor
Related ProteIn ? HDL if LCAT I~ LCAT i
R,<ep<o, \~ __ G G ~ I Extrahepatic cells
LJ ,------I -----<t '--------------'Lll'
HDL, HDL, VHDL
Figure 1.3. Reverse cholesterol transport. TO = triglyceride; CE = cholesterol ester; HDL = high density lipoprotein; VHDL = very high density lipoprotein; LCAT = lecithin cholesleryl acyl transferase; PLTP = phospholipid transfer protein; CETP = cholesterol ester transfer protein.
formed after conversion of HDL3 particles through phospholipid transfer protein (PLTP).
Irrespective of the source of discoidal HDL it is capable of taking up free cholesterol from
extrahepatic cells. This cholesterol is subsequently esterified by the enzyme lecithin
cholesterol acyl transferase (LCAT) which is activated by apoprotein A-I. Through the uptake
-10-

Chapter J
of cholesterol ester the discoidal HDL becomes the spherical HDL3 which may subsequently
be converted into the bigger HDL2 which is more enriched with cholesterol ester. Through
cholesterol ester transfer protein (CETP), the cholesterol esters can then be transferred to
apoprotein B containing lipoproteins and through that route be taken up by the liver. It is not
exactly known which proportion of HDL is subsequently degraded as a particle. The presence
of specific cellular binding sites has been proposed (HDL receptor).
References
Uemura K, Pisa Z. Trends in cardiovascular disease mortality in industrialized countries since
1950. World health statistics quarterly 1988; 41: 155-78.
2 Enos WF, Holmes RH, Beyer 1. Coronary disease among United States soldiers killed in action
in Korea. JAMA 1953;152:1090-3.
3 Holman RL, McGill HC, Strong JP, Geer JC. The natural history of atherosclerosis: The early aortic lesions as seen in New Orleans in the middle of the 20th century. Am J Pathol 1958;34:209~
35.
4 McNamara JJ, Molot MA, Stremple JF et al. Coronary artery disease in combat casualties in
Vietnam. JAMA 1971;216:1185-7.
5 Berenson GS (Ed.). Causation of Cardiovascular Risk Factors in Children: Perspectives on
Cardiovascular Risk in Early Life. New York:Raven Press, 1986. 6 Strong JP, Oalmann MC, Newman WP III, Tracey RE, Malcom GR, Johnson WD, McLahall LH,
Rock WA Jr, Ounnan MA. COrollary heart disease in young black and white males in New Orleans: Community Pathology Study. Am Heart J 1984;108:747-59.
7 Strong JP. Coronary atherosclerosis in soldiers: A clue to the natural history of atherosclerosis in
the young. JAMA 1986;256:2863-6.
8 Newman WP, Freedman DS, Voors AW, Gard PD, Srinivasan SR, Cresanta JL, Williamson GD, Webber LS, Berenson OS. Relation of serum lipoprote'lnlevels and systolic blood pressure to early
atherosclerosis: The Bogalusa Heart Study. New Engl J Med 1986;314:138-44.
9 Tell OS, Tuomilehto J, Epstein FH, Strasser T. Studies of atherosclerosis detemtinants and precursors during childhood and adolescence. Bull WHO 1986;64:595-605.
10 Solberg LA, Strong JP. Risk factors and atherosclerotic lesions: A review of autopsy studies.
Arteriosclerosis 1983;3: 187-98.
II Zeek P. Juvenile arteriosclerosis. Arch Pathol 1930;10:417-66.
12 McGill HC Jr. The geographic pathology of atherosclerosis. Lab Invest 1968;18:463-635.
13 International Atherosclerosis Project. McGill HC Jr (Ed) The Geographic Pathology of
Atherosclerosis. Baltimore: Williams and Wilkins, 1968.
14 Berenson OS, Wattigney WA, Traoy RE, Newman III WP, Srinivasan SR, Webber LS, Dalferes
-11-

Chapter J
ER, Strong JP. Atherosclerosis of the aorta and coronary arteries and cardiovascular risk factors
in persons aged 6 to 30 years and studied at necropsy (TIle Bogalusa Heali Study). Am J Cardiol
1992;70:851-8.
15 McGill HC Jr. The George Lyman Duff Memorial Lecture: Persistent problems in the pathogenesis
of atherosclerosis. Arteriosclerosis 1984;4:443-51.
16 Riley WA, Barnes RW, Schey HM. An approach to the non-invasive periodic assessment of
arterial elasticity in the young. Prev Med 1984;13:169-84.
17 Riley WA, Freedman DS, Higgs NA, Barnes RW, Zinkgraf SA, Berenson GS. Decreased arterial
elasticity associatied with cardiovascular disease risk factors in the young: Bogalusa Heart Study.
Arteriosclerosis 1986;6:378-86.
18 Vogel J. The pathological anatomy of the human body. Philadelphia: Lea and Blanchard,
1847:531-4.
19 Windaus A. Ober den Gehalt normaler und atheromatoser Aorten an Cholesterin und
Cholesterinestern. Z Physiol Chern 1910;67:174-6.
20 Smith EB. The influence of age and atherosclerosis on the chemistry of aortic intima, I. The lipids.
J Atheroscler Res 1965;5:224-46.
21 InsulJ W Jr, Bartsch GE. Cholesterol, triglyceride and phospholipid content of intima, media, and
atherosclerotic fatty streak in human thoracic aorta. J Clin Invest 1966;45:513-23.
22 Strong JP. Atherosclerosis in primates. Introduction and overview. Primates Med 1976;9: 1-15.
23 Greshanl GA. Primates atherosclerosis. Monogr Atheroscler 1976;7:1-95.
24 Faggiotto A. Ross R, Harker L. Studies of hypercholesterolemia in the nonhuman primate. I.
Changes that lead to fatty streak formation, Arteriosclerosis 1984;4:323-40.
25 Faggiotto A, Ross R. Studies of hypercholesterolemia in the nonhuman primate. II. Fatty streak
conversion to fibrous plaque. Arteriosclerosis 1984;4:341-56.
26 Kannel WB, McGee D, Gordon T. A general cardiovascular risk profile: The Framingham Study.
Amer J Cardiol 1976;30:46-52.
27 Dawber TR. The Framingham Study: The Epidemiology of Coronary Heart Disease. Cambridge,
MA: Harvard Univ. Press, 1980.
28 Castelli WP, Abbott RD, McNamara PM. Summary estimates of cholesterol lIsed to predict
coronary heart disease. Circulation 1983j67:730-34.
29 Castelli WP, Garrison RJ, Wilson PWF, Abbott RO, Kalousdian S, Kannel WB. Incidence of
coronary heart disease and lipoprotein cholesterol levels. The Framingham Study. JAMA
1986;256:2835-8.
30 Kannel WB, Castelli WP, Gordon T. Cholesterol in the prediction of atherosclerotic disease: new
perspectives based on the Framingham Study. Ann Intern Med 1979;90:85-91.
31 Martin MJ, Hulley SB, Browner WS. Kuller LH, Wentworth D. Serum cholesterol, blood pressure
and mortality: implications from a cohort of 361662 men. Lancet 1986jii:933-6.
32 Pooling Project Research Group. Relationship of blood pressure, senun cholesterol, smoking habit,
-12-

Chapter I
relative weight and ECG abnormalities to incidence of major coronary events: Final report of the
pooling project. J Chronic Dis 1978;31 :201-306.
33 Avogaro P, Bittolo Bon G, Cazzolato G, Quincy GB. Are apolipoptoteins better discriminators than lipids for atherosclerosis? Lancet 1979;i:901-3.
34 Durrington PN, Ishala M, Hunt L, Arrot S, Bhatnagar D. Apalipaproteins (a), AI, and B and
parental history in men with early onset ischaemic heart disease. Lancet 1988;i:1070-3. 35 Freedman DS, Srinivasan SR, Shear eL, Franklin FA, Webber LS, Berenson GS. The relation of
apolipoproteins A-I and B in children to parental myocardial infarction. N Eng J Med
1986;315:721-6. 36 Zilversmit DB. The George Lyman Duff Memorial Lecture: Atherogenesis: A Postprandial
Phenomenon. Circulation 1979;60:473-85.
37 Moreton JR. Atherosclerosis and Alimentary Hyperlipemia. Science 1947;106: 190-1.
38 Redgrave T. Postprandial remnants and their relations in atherogenesis. In: DeGenlles, Polonovski,
Paoletti, eds. Latent dyslipoproteinemias and atherosclerosis. New York: Raven Press, 1984:9-15.
-13-


CHAPTER 2
POSTPRANDIAL TRIGLYCERIDE RESPONSE IN YOUNG
ADULT MEN AND FAMILIAL RISK FOR CORONARY ATHEROSCLEROSIS

Abstract
2. Postprandial Triglyceride Response in Young
Adult Men and Familial Risk for Coronary Atherosclerosis
In this cross-sectional study, the postprandial handling of a standardized oral lipid load
(mean 397.6 grams), labelled with retinyl palmitate as a marker for chylomicrons and
chylomicron remnants, was studied in 80 sons (mean age, 24.8 years) of patients with
clinically manifest and angiographically proven severe coronary artery disease and in 55 sons
(mean age 23.2 years) of angiographically negative controls. The objective was to determine
whether an increased risk of coronary artery disease in young adults is related to changes in
postprandial lipoprotein metabolism. Patients and controls were obtained from coronary
angiography departments of four central general hospitals in the Netherlands. In both group
of offspring postprandial levels of semm triglycerides, retinyl palmitate, and total cholesterol
were measured during a 12 hour period. Both groups showed a marked rise in semm
triglyceride and retinyl palmitate concentrations after the lipid load, reaching a maximum 4
to 6 hours postprandially. No changes in postprandial total cholesterol concentrations were
observed in either group. In sons of patients with coronary artery disease postprandial
hypertriglyceridemia was prolonged as compared to the sons of controls. Differences between
groups mainly occurred between 6 and 12 hours after the lipid load. Similar results, although
smaller and not statistically significant, were obtained with regard to postprandial retinyl
palmitate, also showing differences mainly after 6 hours. It is concluded that healthy young
sons of fathers with established coronary artery disease have a prolonged postprandial
hypertriglyceridemia. These findings support the hypothesis that postprandial lipoprotein
metabolism plays a role in atherogenesis.
Introduction
Atherosclerosis starts early in life (l, 2). Postprandial lipoprotein metabolism is proposed
to be involved in this process (3). Cholesteryl ester-rich remnants of triglyceride-rich
lipoproteins may directly promote accumulation of cholesterol esters in the arterial wall (4 -
6). Further, it has been reported (7, 8) that the protective effect of increased levels of high
density lipoprotein (HDL) cholesterol levels on the risk for coronary artery disease may not
only be explained by its role in reverse cholesterol transport but also by the relationship
-16-

Chapter 2
between HDL and triglyceride metabolism (9). Plasma triglycerides have an effect on HDL
composition and HDL-cholesterol levels (10); an inverse relationship between HDL, levels
and postprandial triglyceride levels has been shown (II). Levels and composition of HDL
could thus be a reflection of the effectiveness of triglyceride-rich lipoprotein catabolism. A
deranged metabolism of triglyceride-rich lipoproteins in plasma has been reported in familial
dysbetalipoproteinemia (12, 13), a disease associated with premature coronary atherosclerosis.
Studies comparing patients with coronary artery disease and persons without the disease
have shown that differences with respect to postprandial hypertriglyceridemia (14 - 16) and
postprandial retinyl palmitate concentrations (a marker of chylomicrons and their remnants)
are detectable after an oral lipid load (14, 15). These results suggest a delayed clearance of
these lipoproteins in patients with coronary artery disease. Thus, accumulating evidence indicates that postprandial lipemia plays an important role in causing coronary artery disease,
and the implications with respect to treatment and primary prevention are increasingly being
recognized (17).
Postprandial lipoprotein metabolism has not yet been studied in children and young adults
with an increased risk for coronary atherosclerosis. In our study, male offspring of men with
clinical manifestations of angiographically proven coronary atherosclerosis were compared
with the male offspring of men who did not have coronary atherosclerosis (negative results
after angiography). This approach enabled us to study a group of healthy young adults at a
high familial risk for developing clinical manifestations of coronary artery disease later in life.
We assessed whether changes in the triglyceride response to a standardized oral lipid load,
as reported in patients with coronary artery disease, can also be measured in healthy yOWlg
male offspring of such patients.
Methods
Part/clpants
Men with very severe coronary artery disease (patients), defined as more than 70%
occlusion in at least three major coronary vessels were selected from coronary angiography
databases of cardiology departments of the Zuiderziekenbuis Rotterdanl (1988 - 1991), the
University Hospital Rotterdanl (1988 - 1989), the Refaj. Ziekenbuis in Dordrecht (1990 -
1991), and the Antonius Ziekenbuis in Nieuwegein (1992), all hospitals situated in the
Netherlands. Simultaneously, a reference group of men (controls) was selected who at
-17-

Chapter 2
coronary angiography had no or, at most, only minor lesions, defined as 20% stenoses or less in all coronary vessels. Further, participants were selected according to the following
additional criteria: I) age between 45 and 65 years, 2) blood pressure not exceeding 160/100
nun Hg, 3) absence of liver disease, diabetes mellitus, thyroid disease, and renal disease, 4)
first coronary angiography within two years before examination for our study, 5) first
consultation of a physician for cardiac symptoms within 5 years before the examination for
our study.
Eligible participants were sent a letter asking whether they had a son 15 to 30 years of age
and, if so, whether the son was willing to participate in the study. These sons (identified by
their fathers) received a separate letter inviting them to have an oral lipid loading test.
Participants also received a short questionnaire about smoking habits, alcohol intake, physical
activity, and fat intake.
We screened medical files of 629 patients whose coronary angiographic data met the
criteria. Of these patients, 19 had died, 46 had diabetes mellitus, 6 had renal disease, 2 had
thyroid disease, 183 had either no son or sons outside the required age range, 58 could not
be contacted, 17 had no contact with their children, 78 had a cardiac history exceeding 5
years, and 63 could not be invited for other reasons (hospitalization, other serious diseases).
Of 157 families (fathers and sons) who met all the criteria, 55 (either father or son) refused
to participate in the study (response, 65%), leaving 102 fathers and 139 sons. The latter had
oral lipid loading tests. The study protocol was approved by the medical ethics conunittees
of the Zuiderziekenhuis Rotterdam and the University Hospital Rotterdam. Informed consent
forms were obtained from all participants in the study.
Baseline measurements
Fathers were asked to visit the hospital at 9:00 a.m. after fasting for at least 12 hours.
Fathers responded to a questionnaire about the number of first-degree relatives who had had
myocardial infarctions and about the medication use at the time of the examination
(medication was taken to the hospital where the exanlination took place). Systolic blood
pressure and diastolic blood pressure were measured using a random zero sphyg-momanometer (Hawksley, Lancing, United Kingdom). Fasting sernm blood sanlples were drawn by
arltecubital venipuncture for measurement of levels of triglycerides, total cholesterol, low
density lipoprotein (LDL) cholesterol, and HDL cholesterol (and its subfractions HDL, and
HDL,). Height and weight were measured without shoes and without heavy clothing.
-18-

Chapter 2
The sons were invited to come to the hospital, after the same period of fasting, on a separate
day to have an oral lipid loading test. For sons, questionnaires were used to obtain data about
use of medication, fat intake, alcohol intake, and smoking habits, referring to a I-month
period before the examination for this study. Daily total fat intake was calculated from an 81
item semiquantitative food frequency questionnaire by using a computerized food-composition
table (17). In the sons, blood samples were taken by antecubital venipuncture for measurement
of baseline levels of semm triglycerides, total cholesterol, LDL cholesterol, HDL cholesterol
(and its subfractions HDL, and HDL,), apoprotein A-I, apoprotein A-2, apoprotein B, and
retinyl palmitate concentrations. This baseline measurement of lipid levels was taken as the
starting point (10) for the oral lipid loading test. In all of the sons, apolipoprotein E was
phenotyped.
Oral lipid loading lesl
Sons of patients and sons of controls came to the hospital at 7:45 a.m. after an overnight
fasting of 12 hours. Height and weight were measured first to calculate body surface area.
Five minutes after the venipuncture for obtaining baseline lipid levels (at 10), all participants
received a liquid lipid load, which consisted of a mixture of dairy cream (40% fat), egg yolk,
milk powder, and retinyl palmitate (in aqueous solution) (15). Pru1icipants received the lipid
load in a dose based on their individual body surface area (77.5 g fat, 0.5 g cholesterol, and
27.000 IV of retinyl palmitate per square meter of body surface area). The mixture was
conswned within 15 minutes.
The participants received an antecubital venous catheter (Venflon, Viggo AB, Helsingborg,
Sweden), which was kept open during the test period by means of dispensable obturators
(Venflon). Through this catheter, blood samples were drawn at 2 (1,), 4 (t,), 5 (t,), 6 (t,), 7
(1,), 8 (t,), 10 (tlO), and 12 (t,,) hours after starting consumption of the oral lipid load. Total
cholesterol, triglyceride, ruld retinyl palmitate concentrations were determined in serum
isolated from these samples. During the 12-hour period, other sources of calories were
withheld from the participants. Because postprandial exercise has been reported to decrease
postprandial lipemia (19), participants stayed in the hospital and were asked to refrain from
heavy physical activity during the test period.
LaboralDlY analyses
-19-

Chapter 2
Serum total cholesterol levels were measured with an automated enzymatic method (Boehringer Mannheim, Mannheim, Germany) CHaD-PAP reagent kit (20). Levels of HDL
cholesterol and LDL cholesterol were measured by the same method after precipitation. For
HDL cholesterol, the phosphotungstate method according to Burstein (21), with a minor
modification as described by Grove (22), was used. For LDL cholesterol, precipitation was
carried out with polyvinylsulphate (Boehringer Mannheim). Tlu'oughout the entire study
period, results of total cholesterol and HDL cholesterol determinations were within limits of
the quality control program of the World Health Organization Regional Lipid Reference
Centre (Prague, Czechoslovakia). Levels of apoprotein A-I and B were assayed using an
automated immunoturbidimetric method (Kone Diagnostics, Espoo, Finland). Levels of
apoprotein A-2 was determined by radial immunodiffusion against specific antiserum
(Boehringer Mannheim, Germany) according to Cheung and Albers (23), with slight
modifications. All automated analyses were carried out on the Kone Specific Analyzer (Kone
Instruments) using frozen (-20°C) selUm samples. High-density lipoprotein, and HDL,
subfractions in serum were assayed as described by Gidez and colleagues (24), with slight
modifications. High-density lipoprotein, and HDL, subfractions were separated using stepwise
precipitation of apoprotein B containing lipoproteins with heparinelMn" and HDL, with
dextran sulphate. Apolipoprotein E phenotyping was done by isoelectric focusing of
delipidated serum followed by immunoblotting, using apolipoprotein E antiserum as first
antibodies (25). Retinyl palmitate analyses were performed as described previously by Groot
and colleagues (15).
Statistical analysis
Mean ± SDs were calculated for baseline characteristics of all fanlily members. The total
cholesterollHDL cholesterol and LDL cholesterollHDL cholesterol ratios were calculated for
fathers and sons, and the apoprotein A-l/apoprotein B ratio was calculated for sons. Baseline
differences between patients and controls, as well as their respective sons were evaluated using the two group I-test, or the Marm-Whitney U test when appropriate. Differences in
postprandial responses between sons of patients and sons of controls with regard to
triglycerides and retinyl palmitate were evaluated with age-adjusted repeated-measures analysis
to determine if group differences at each postprandial measurement time differed significantly
from group differences at any other measurement time. Subsequently, linear regression analysis was used to compare mean group postprandial responses. Adjustments were made for
-20-

Chapter 2
age, HDL, cholesterol, HDL, cholesterol, apolipoprotein E phenotype, and daily total fat
intake. This was done at each postprandial measurement time (I, to t,,) and for areas under
the curve for several time (2: 2 hour) intervals. In the analyses both individual postprandial
measurements and areas under the curve were evaluated after subtracting the initial individual
values (t,,) for triglycerides and retinyl palmitate from all respective postprandial measure
ments, yielding the net postprandial change.
Results
Two sons of patients did not tolerate the oral lipid load because of gastrointestinal problems
and were excluded from the study. All other participants tolerated the fat load very well and
did not have gastrointestinal symptoms or steatorrhea during or after the tes!.
Two (other than already excluded) participants had baseline triglyceride values of2.52 and
2.45 mmol/L, respectively. The first participant had six measurements of postprandial retinyl
palmitate measurements that were more than 3 to 5 standard deviations above the mean, and
the latter participant had five measurements of postprandial triglyceride measurements that
were more than 3 to 5 standard deviations above the mean. Because of the marked effect of
these outliers on the precision of the results obtained in the group as a whole, these two
participants were excluded from analyses.
Baseline characteristics are given for both groups of fathers and sons in table 2.1. No
statistically significant differences were noted between patients and controls. Sons of patients
were slightly older and had a lower total fat intake. All patients (n~59) had had coronary
angiography for evaluation of symptoms of chest pain. For controls, the indications for
coronary angiography were symptoms of chest pain (n~30), evaluation of cardiac valves
(n~7), suspected cardiomyopathy (n~5), and ventricular septum defect (n~ 1). At the time of
coronary angiography, 19 (32.2%) patients and 11 (25.6%) controls were treated for
hypertension. The average time elapsed between the date of the coronary angiography and
date of the examination was 13.2 ± 0.9 months (mean ± SE) for patients and 13.2 ± 1.1 months for the controls.
Baseline serum measurements after an overnight fast are given for both groups in table 2.2.
As expected, patients had higher serum levels of total cholesterol, LDL cholesterol, and
triglycerides and had higher total cholesterollHDL cholesterol and LDL cholesterollHDL
cholesterol ratios than did controls. Levels of HDL cholesterol and its subfractions tended to
be slightly lower in patients than in controls (Table 2.2). Compared with sons of controls,
-21-

Table 2.1. Baseline cha:racterist:ics of fathers and SODS.
Cha:racterist:ic Fathers
Patients Controls P value (n ~ 59) (n ~ 43)
Age (y) 555 ± 0.8 53.9 ± 12 >02
Height (em) 176.4 ± 0.7 1783 ± 12 0.15
Weight (kg) 79.4 ± 12 79.8 ± 1.6 >02
, Quetelet-index (kgfm') 25.4 ± 03 25.1 ± 0.4 >02 tv ~ Systolic blood pressure (rom Hg) 125.4 ± IS 128.5 ± 2.4 >02
Diastolic blood pressure (rom Hg) 82.6 ± 1.5 823 ± 1.7 >02
Hypertension treatment (%) 322 25.6 >02
Smoking (%) 153 27.9 0.19
Alcohol use (%)
Alcohol intake (gfd)
Total tat intake (gf d)
Values are mean ± SD. where appropriate. P values compare patients and controls.
SODS of
Patients Controls (n~80) (n~5)
24.8 ± 0.6 232 ± 0.6
1832 ± 0.7 183.4 ± 0.9
78.0 ± 12 753 ± 13
232 ± 0.03 22.4 ± 0.03
120.9 ± 1.4 118.1 ± 22
77.6 ± 1.0 75.0 ± 1.8
28.8 31.6
86.3 78.9
11.4 ± 1.7 9.6 ± IS
133.6 ± 9.0 169.8 ± 13.9
P value
0.049
>02
0.19
0.12
0.19
0.10
>02
>02
>02
0.012
9 {l ~ '"

,:, Y'
Table 2.2. Baseline serum measurements in fathers and SODS.
Variable Fathers Sons of
Patients Controls P value Patients Controls P value (n = 59) (n = 43) (n = 80) (n = 55)
Total cholesterol (mg/dL) 2633 ± 5.0 2412 ± 5.9 0.006 200.0 ± 3.7 195.8 ± 45 >02
WL cholesterol (mg/dL) 193.4 ± 4.7 169.6 ± 55 0.002 137.4 ± 3.8 130.8 ± 45 >02
IIDL cholesterol (mg/dL) 42.8 ± 1.4 45.4 ± 1.6 >02 43.4 ± 1.0 45.7 ± 13 0.15
IIDI., cholesterol (mg/dL) 73 ± 0.7 8.6 ± 0.9 >02 7.7 ± 0.5 6.7 ± 0.7 >02
IIDI., cholesterol (mg/dL) 36.0 ± 0.9 36.6 ± l.l >02 35.7 ± 0.8 38.9 ± 1.0 0.016
Triglycerides (romol/L) 2.01 ± 0.12 1.53 ± 0.15 0.015 1.09 ± 0.06 !.I5 ± 0.08 >02
Total cholesterolJHDL cholesterol 6.6 ± 03 5.6 ± 03 0.015 4.8 ± 0.1 4.4 ± 02 0.09
LDL cholesterollHDL cholesterol 4.8 ± 02 3.9 ± 03 0.001 33 ± 0.1 3.0 ± 02 0.10
Apoprotein A-I (mg/dL) ll5.7 ± 2.4 120.1 ± 3.0 >02
Apoprotein A-2 (mg/dL) 43.1 ± 0.9 482 ± l.l 0.001
Apoprotein B (mg/dL) 85.3 ± 2.3 85.6 ± 2.8 >02
Apoprotein A~I/Apoprotein B 1.45 ± 0.05 1.45 ± 0.06 >02
Retinyl palmitate (J<g/dL) 2.8 ± 05 2.4 ± 0.6 >02
Values are mean ± SE, adjusted for age. LDL = Low-density lipoprotein; HDL = High-density lipoprotein. P values compare patients and controls. 9
{l il '"

Chapter 2
sons of patients had a somewhat less favorable lipoprotein and apoprotein profiles (not
statistically significant). Sons of patients had significantly decreased levels of HDL,
cholesterol (p~O.OI6) and apoprotein A-2 (p~O.OOI) when compared with controls. The
frequencies of apolipoprotein E phenotypes did not differ between sons of patients and sons
of controls. Apoprotein E2 alleles were present in 8 sons of controls and 6 sons of patients,
I of whom was of the E2fE2 phenotype. TillS participant was not an outlier with regard either
to baseline lipid profile or postprandial data.
The mean fat load ingested by sons of patients was 399.4 ± 3.2 g (mean ± SE) by and by
sons of controls was 395.1 ± 3.8 g. None of the sons in both groups had previous or current
diseases or received medication known to have an effect on lipoprotein metabolism.
Serum Triglyceride Serum Retinyl Palmitate Serum Total Cholesterol " ,ro '"
'" -" <"" ,ro "' '" '"
f' '\ '\ ~l~
I" '\ Il • '\ ----,/\ '\ 11. '\ ..--a ..--
" • " ~
"- '" '" " • - CAD+sOM(n=SO)
• • -- CAD. WM(Q=S5) ,.
• • , , , . ,. " • I , 6 7 8 " " • I J 6 7 3 " " Time (h) Time (h) 11me(h)
Figure 2.1. Serum lipid levels in young adult men after an oral fat load. Levels of postprandial serum triglyceride (left), retlnyl palmitate (middle), and total cholesterol (right) are mean values adjusted for age. To convert cholesterol levels to mmollL, multiply by 0.02586. CAD "" COrollary artery disease; CAD + and CADrefer to sons whose fathers do and do not have coronary artery disease, respectively.
Figure 2.1 shows age-adjusted mean postprandial curves for levels of triglyceride, retinyl
pahTIitate, and total cholesterol. Figure 2.1 (left panel) shows mean postprandial triglyceride
curves for sons of patients and sons of controls. In both groups, oral lipid loading led to
markedly similar increases in triglyceride concentrations, maximum levels appeared between
4 to 6 hours postprandially. After 12 hours, triglyceride concentrations had decreased below
initial levels. The age-adjusted repeated-measures analysis showed an interaction effect
between group and time (X2~19.2; p~O.OI4), indicating that the two curves were significantly
different from each other.
-24-

Chapter 2
In Figure 2.1 (middle panel) the mean postprandial retinyl palmitate curves are shown.
Retiny! palmitate concentrations increased from virtually zero in both groups to reach maximum concentrations between 5 and 6 hours postprandially. Thereafter, retinyl palmitate concentrations decreased to levels at t" that were approximately tenfold the initial levels at
to. The repeatedMmeasures analysis for these curves indicated no significant difference
(X'~6.42; p~O.60).
In Figure 2.1. (right panel) curves are shown for postprandial total cholesterol responses.
Sons of patients had higher mean total cholesterol levels at to than did sons of controls, and
this difference remained remarkably constant during the lipid loading test, showing no
significant response to the intervention. The age-adjusted difference in mean cholesterol levels
(mean of all cholesterol measurements) was 2.3 ± 5.87 mg/dL (mean ± SE, p~O.70).
A slight difference in age was noted between sons of patients and sons of controls. Age has
been shown to have an effect on postprandial lipoprotein changes (26) and postprandial retinyl
ester response (27), and therefore the differences in postprandial response between sons of
patients and sons of controls were adjusted for age.
Table 2.3 shows the age-adjusted differences between net postprandial changes in
triglyceride and retinyl pahnitate responses between sons of patients and sons of controls.
Triglyceride response differences showed a maximum at t5, and reached significance at times
t" t", and t". With respect to retinyl palmitate, sons of patients and sons of controls showed
a slight difference in response, increasing to a maximum at ts to t6' None of the retinyl
palmitate differences was found to be statistically significant.
In Figure 2.2.A, age-adjusted areas under the curves for 2-hour time intervals are given for
postprandial triglyceride responses in sons of patients and sons of controls. Peak areas for both
groups were found in interval t4 to t6' Differences were mainly found in intervals t6 to tg, tg to t lO, and t" to t". In the latter interval, the triglyceride response of sons of controls
decreased below to (baseline) levels to a greater extent than in sons of patients. Figure 2.2.B
shows total area under the curves for 10-, 8-, 6-, and 4-hour time intervals up to t". For all
intervals, areas under the curve differed significantly between the groups. Figures 2.2.C and
2.2.D show similar data for retinyl palmitate responses in the groups. For 2-hour intervals and
larger intervals, areas under the curves for sons of patients tended to be higher, although
differences did not reach statistical significance.
The results for postprandial retinyl palmitate as well as triglycerides did not materially
change after adjustment for baseline HDL, cholesterol levels, HDL, cholesterol levels, and
apolipoprotein E phenotype. Total fat intake was decreased in sons of patients compared with
sons of controls (p~O.OI2; Table 2.1). Adjustment for this difference in postprandial analyses
-25-

~ 9'
Table 2.3. Postprandial triglyceride and retinyl palmitate responses in sons of patients with coronary artery disease and sons of controls.
Time (Il) Triglycerides (mmol/l) Retinyl palmi""e (pgldL)
Sons of Sons of Difference Sons of Sons of Difference patients controls (95% Cl) patients controls (95% Cl) (n=80) (n=65) (n=80) (n=65)
2 Ll7 ± 0.08 1.04 ± 0.09 0.13 (-0.11 to 037) 353 ± 3.0 353 ± 3.6 0.03 (-9.1 to 92)
4 1.81 ± 0.13 1.64 ± 0.16 0.17 (-024 to 058) 103.9 ± 6.0 101.7 ± 73 23 (-163 to 20.8)
5 1.89 ± 0.15 1.46 ± 0.18 0.43 (-0.02 to 0.88) 122.8 ± 7.4 110.8 ± 9.0 12.0 (-11.0 to 34.9)
6 1.40 ± 0.12 1.06 ± 0.15 034 (-0.03 to 0.72) 124.6 ± 8.1 106.6 ± 9.8 17.9 (-72 to 43.0)
7 0.87 ± 0.10 058 ± 0.13 029 (-0.03 to 0.61) 100.0 ± 72 90.4 ± 8.7 9.6 (-12.6 to 31.8)
8 0.54 ± 0.09 0.19 ± 0.11 035 (0.07 to 0.62) 80.7 ± 6.9 70.6 ± 8.4 10.0 (-11.4 to 31.5)
10 -0.12 ± 0.05 -033 ± 0.06 021 (0.06 to 036) 46.0 ± 4.6 40.0 ± 5.5 6.0 (-8.1 to 20.1)
12 -029 ± 0.04 -0.42 ± 0.05 0.13 (0.01 to 026) 262±23 222 ± 2.7 4.0 (-3.1 to 11.1)
Triglyceride and retinyl palmitate values are mean ± SE, adjusted for age. Age-.adjusted mean differences (values of sons of patients minus values of sons of controls) are given with their corresponding 95% CIs.
Q -§ ~ ..,

Chapter 2
A C 250
4
• 200
~ 3
$150 • 2
1 * .
1 01)100-"-
0 50
·1 0 2·4 4·6 6· , 8 -to 10- 12 2·4 4·6 6·' 8 - 10 10 -12
Time intervals (It) Time illtelVals (h)
B D 12 *
1000 [ II sonS or-patients J 10
t 800-o Sons of controls
~ , $ 600 6
'0 4 • on 400-
~ 2 t "-200
O·
·2 0-2-12 4 -12 6-12 8-12 2-12 4 -12 6 -12 8 -12
Time Intervals (It) Time intervals (h)
Figure 2.2. Age adjusted areas under the curve for levels of postprandial triglyceride and retinyl palmitate. A. Areas under the curve for postprandial triglyceride levels for 2-hour time intervals. B. Areas under the curve for
larger time intervals. C and D. Areas under the curve for postprandial retinyl palmitate. Closed bars ~ sons of
patients with coronary artery disease; open bars"" sons of controls (those without coronary artery disease) . • = p<O.05; t = p<O.Ol.
did not change the results, with adjusted group differences in triglyceride levels at t, of 0.32
mmollL [95% CI, 0.04 to 0.59], at tlO of 0.2 mmollL [95% CI, 0.047 to 0.36], and at t" of
0.1 mmollL [95% CI, 0.002 to 0.26]. All sons were asked whether they had changed their
lifestyles with regard to smoking habits, physical activity, and fat intake since their fathers had
had cardiac examination. None of the group differences was statistically significant. Also, a
similar analysis of sons who reported to live separately from their fathers at the time of
examination (45 sons of patients [56%] and 24 sons of controls [42%] yielded no significant
group differences with respect to lifestyle changes. An analysis of postprandial data in these
groups showed similar results, with sons of patients having higher triglyceride levels at t,
(difference, 0.47 mmollL; 95% CI, -0.018 to 0.95) and t10 (difference, 0.29 mmollL; 95% CI,
-27-

Chapter 2
O.oJ5 to 0.57). When analyses were done for participants with normal levels oftriglycerides
only (serum triglyceride:; 2.28 mmollL), thereby excluding 13 participants, no major changes
in the results were found.
Discussion
Familial aggregation of risk factors for coronary artery disease is well established, and the
offspring of patients with very severe coronary artery disease are at increased risk for this
disease (28, 29). We assessed whether this increased familial risk was related to postprandial
metabolic handling of an oral fat load in healthy young male adults whose fathers had severe
coronary artery disease. Baseline measurements showed that sons of patients and sons of
controls had similar levels of lipids and apolipoproteins, only levels of HDL, cholesterol and
apoprotein A-2 were significantly decreased in sons of patients.
After oral lipid loading, however, prolonged postprandial hypertriglyceridemia was observed
in the sons of patients, amounting to statistically significant group differences of 0.35 mmollL
after 8 hours, 0.21 mmollL after 10 hours, and 0.13 mmollL after 12 hours. Differences in
postprandial triglyceride levels between the groups were mainly observed in the declining part
of the curves, which suggests a delayed clearance of triglyceride from plasma. Data on
postprandial retinyl palmitate responses also suggest similar differences for postprandial
triglyceride levels with regard to the direction of the difference and the postprandial period
in which differences appeared. However, these latter differences were not statistically
significant.
A marked contrast between patients with coronary artery disease and controls with regard
to angiographlc findings was chosen to minimize the chance of misclassification of patients
and also because of the anticipated subtle differences between both groups of offspring.
Considering the efforts asked on a strictly voluntary basis from fathers, and particularly their
offspring, the response rate of 65% in this study is satisfactory. However, it is possible that
postprandial lipoprotein metabolism in these young healthy participants was in some way
differentially related to the response in both groups and, although unlikely, it is possible that
selection mechanisms have affected the findings. Because contraceptive steroids have an effect
on postprandial lipid metabolism in young health women (30), we restricted the study to sons.
Chylomicron metabolism is thought to occur essentially in two successive steps. First, these
particles interact with lipoprotein lipase, an enzyme which is located on capillary endothelial
surfaces of various tissues, including heart, skeletal muscle, and adipose tissue (31). This lipase
catalyses the hydrolysis of triglycerides, and this results in uptake of free fatty acids by tissues
-28-

Chapter 2
(32). Thereafter, resulting chylomicron remnant particles are taken up relatively quickly and
efficiently (33) by parenchymal cells in the liver. The importance of this process, with regard
to atherogenesis, is that any hampering in this course of events might lead to higher plasma
levels of atherogenic triglyceride-rich Iipiproteins and their remnants.
In principle, the oral lipid loading test cannot distinguish between mechanisms involved in
chylomicron entry into and clearance of chylomicrons and their remnants from the circulation.
In our study, no attempt was made to assess differences between intestinal lipid absorption in
the two groups of young adult men. In a study of postprandial lipoprotein metabolism,
Weintraub and colleagues (13) showed that gastrointestinal transit time was similar in normal
participants and participants with different types of hyperlipoproteinemias. Previous studies
(14 - 16) showed that mean triglyceride and mean retinyl palmitate response curves are similar
during the first 4 hours postprandially when comparing patients and controls, which we also
found in our study in sons of such patients. This suggests that differences in fat absorption or
in intestinal secretion, if any, are not likely to explain group differences during the second half
of the test period.
Retinyl pahnitate is a useful marker of the metabolism of intestinally derived triglyceride
rich lipoproteins and their remnants because it is incorporated into the core of these
lipoproteins (34) and retained within them until their irreversible clearance from plasma by
the liver (35). Although a considerable postprandial exchange between lipoproteins of total
retinyl esters has been reported in man (36), little exchange of retinyl pahnitate between
intestinally derived lipoproteins and other lipoproteins has been shown (37, 38). In our study,
retinyl palmitate responses showed considerable interindividual variation in both groups, which
may explain why differences between group responses did not reach statistical significance.
An alternative explanation might be that the postprandial retinyl ester response is greater in
older persons than in YOlmger persons (27), thus making it more difficult to detect group
differences in the young. Further, postprandial hypertriglyceridemia may partly be induced by
endogenous very-low-density lipoprotein and its remnants (39), which do not contain retinyl
palmitate. Finally, significant group differences in retinyl palmitate may emerge after the 12-
hour measuring period used in the present study and, thus, may have been missed (14).
In our study, data were analyzed after subtracting individual fasting triglyceride levels and
retinyl palmitate levels from respective subsequent measurements. Differences in body height
and weight were considered by standardizing the oral lipid load to body surface area as a
function of body height and weight. Possible confounding effects of age, HDL, cholesterol
levels, HDL, cholesterol levels, and apolipoprotein E phenotype were adjusted for in the
analysis. Apolipoprotein E polymorphism has recently been shown to have an effect on
-29-

Chapter 2
postprandial retinyl palmitate concentrations (40). Adjustment for these factors did not
materially change results with regard to group differences.
The hypothesis that postprandial lipoprotein metabolism plays an essential role in
atherogenesis was first postulated by Zilversmit (3). This hypothesis was adressed in recent
studies in humans (14 - 16) in which patients with coronary artery disease were compared with
controls with respect to postprandial lipemia; the study found that patients had higher
postprandial triglyceride and retinyl palmitate responses. In another study, Simons and
colleagues (41) fOlmd that 4 hours postprandially the apoprotein B48/apoprotein BIOO ratio,
used as a relative measure of chylomicrons and chylomicron renlllants in plasma, was higher in patients with coronary artery disease than in controls. In addition, a positive correlation
between the postprandial triglyceride response to an oral lipid load and carotid artery wall
thickness has been reported (42). These studies suggest that prolonged presence oftriglyceride
rich lipoproteins in plasma may indeed playa role in atherogenesis.
The design of our investigation enabled us to examine a group of young adult men at high
familial risk for developing clinical manifestations of coronary artery disease much later in
life. One advantage of the design of this study is that sons of these patients are not exposed
to treatments such as medication that could alter triglyceride metabolism, as might occur when
patients themselves are studied. However, if patients have been given advice about lifestyle,
this may in turn have led to lifestyle changes in their sons. In both groups of sons, most
reported not to have changed their levels of physical activity, smoking behavior, and fat intake
since their fathers were examined for cardiac symptoms; approximately equal proportions reported to eat less fat. Additionally, an analysis of sons living separately from their fathers,
who are assumed to be less influenced by lifestyle advice given to their fathers, yielded similar
results with statistically significant differences in the declining part of the triglyceride curves,
despite the considerably decreased number of participants. Although no major differences were
noted with regard to reported fat intake, daily total fat intake as calculated from the food
frequency questionnaire was significantly decreased in sons of patients compared with sons
of controls. Long- and short-term effects of fat intake on postprandial lipoprotein levels have
been reported (43), but in our study, adjustment for daily total fat intake did not change
postprandial results. Thus, we believe that changes in physical activity, smoking behavior, and
fat intake are not likely to explain the postprandial differences found between both groups of
sons.
Our data show that healthy young sons whose fathers have established coronary artery
disease have prolonged postprandial hypertriglyceridemia. Tltis finding suggests that changes
in postprandial lipid metabolism are associated with familial risk for coronary atherosclerosis.
-30-

Chapter 2
Acknowledgement
The authors thank Ms. Lorette Q.M. Hulsman for assistance with conducting the study, Ms.
Jeannette M. Vergeer-Drop for assistance in laboratory analyses, and the cardiologists Dr. H.J.
Kingma (Antonius Ziekenhuis in Nieuwegein, the Netherlands), Dr. Ph.W. Fels (Refaja
Ziekenhuis in Dordrecht, the Netherlands), and Dr. F.J. ten Cate (University Hospital
Rotterdam, the Netherlands) for helping select the patients. This investigation was supported
by a grant of the Netherlands Heart Foundation.
References
Newman WP, Freeman OS, Voars AW, Gard PO, Srinivasan SR, Cresanta JL, Williamson GO, Webber LS, Berenson GS. Relation of serum lipoprotein levels and systolic blood pressure to early
atherosclerosis: The Bogalusa Heart Study. New Engl J Med 1986;314:138-44.
2 Relationship of atherosclerosis in young men to serum lipoprotein cholesterol concentrations and smoking. A preliminary report from the Pathobiological Detenninants of Atherosclerosis in Youth
(PDAY) research group. JAMA 1990;264:3018-24.
3 Zilversmit DB. Atherosclerosis: A postprandial phenomenon. Circulation 1979;60:473-85. 4 Goldstein JL, Ho YK, Brown MS, Innerarity TL, Mahley RW. Cholesteryl ester accumulation in
macrophages resulting from receptor-mediated uptake and degradation of hypercholesterolemic canine beta-very low density lipoproteins. J BioI Chern 1980;255: 1839-48.
5 Gianturco SH, Lin AH, Hwang SL, Young J, Brown SA, Via DP, Bradley WA. Distinct murine
macrophage receptor pathway for human triglyceride-rich lipoproteins. J Clin Invest 1988;82(5): 1633-43.
6 parthasarathy S, Quinn MT, Schwenke DC, Carew TE, Steinberg D. Oxidative modification of
beta-very low density lipoprotein. Potential role in monocyte recruitment and foam cell fonnation. Arteriosclerosis 1989;9:398-404.
7 Pearson TA, Bulkley BH, Achuff SC, Kwiterovich PO, Gordis L. The association of low levels of HDL cholesterol and arteriographically defined coronary artery disease. Am J Epidemiol 1979;109:285-95.
8 Castelli WP, Garrison RJ, Wilson PWF, Abbott RD, Kalousdian S, Kannel \VB. Incidence of coronary heart disease and lipoprotein cholesterol levels: The Franlingham Study. JAMA 1986;256:2835-8.
9 Davis CE, Gordon D, LaRosa J, Wood PD, Halperin M. Correlations of plasma high density lipoprotein cholesterol levels with other plasma lipid and lipoprotein concentrations. The Lipid
-31-

Chapter 2
Research Clinics Program Prevalence Study. Circulation 1980;62(suppl IV):24-30.
10 Deckelbaum RJ, GranDt E, Oschry Y, Rose L, Eisenberg S. Plasma triglyceride determines
structure, composition in low and high density lipoproteins. Arteriosclerosis 1984;4:22Sw31.
11 Patsch JR, Prasad S, Gotto AM Jr, Patsch W. High density lipoprotein2• Relationship of the plasma
levels of this lipoprotein species to its composition, to the magnitude of postprandial lipemia, and to the activities of lipoprotein lipase and hepatic lipase. J Clin Invest 1987;80:341-7.
12 Hazzard WR, Biemlan EL. Delayed clearance of chylomicron remnants following vitaminwAw
containing oral fat loads in broad-Jl disease (type III hyperlipoproteinemia). Metabolism
1976;25:777-801.
13 Weintraub MS, Eisenberg S, Breslow JL. Different pattems of postprandial lipoprotein metabolism
in normals, type IIa, type III, and type IV hyperlipoproteinemic individuals: Effects of treatment
with cholestyramine and gemfibrozil. J Clin Invesl 1987;79: 1110·9.
14 Simpson HS, Williamson CM, Olivecrona T, Pringle S, Maclean J, Lorimer AR, Bonnefous F,
Bogaievsky Y, Packard eJ, Shepherd J. Postprandial lipemia, fenofibrate and coronary artery
disease. Arteriosclerosis 1990;85: 193w202.
IS Groot PRE, Van Stiphout WAHJ, Krauss XH, Jansen H, Van Tol A, Van Ramshorst E, ChinwOn
S, Hofinan A, Cresswell SR, Havekes L. Postprandial lipoprotein metabolism in nonnolipidemic
men with and without coronary artery disease. Arterioscler Thromb 1991;11:653w62.
16 Patsch JR, Miesenbtsck G, Hopferwieser T, MUhlberger V, Knapp E, Dunn JK, Gotto Am Jr,
Patsch W. Relation of triglyceride metabolism and -coronary artery disease. Studies in the
postprandial slale. Arterioscler TItromb 1992;12: 1336-45.
17 Slyper AH. A fresh look at the atherogenic remnant hypothesis. Lancet 1992;340:289-91.
18 Commissie N.C.V. 's Gravenhage: Voorlichtingsbureau voor de voeding. N.C.V. tabel (Dutch
Computerized Food Composition Table), 1989.
19 Schlierf 0, Dinsenbacher A, Katller H, Kohlmeier M, Haberbosch W. Mitigation of alimentary
lipemia by postprandial exercise: Phenomena and mechanisms. Metabolism 1987;36:726-30.
20 Van Gent eM, Van der Voort HA, de Bruijn AM, Klein F. Cholesterol detemlinations. A
comparative study of methods with special reference to enzymatic procedures. Clin Chim Acta
1977;75:243-51.
21 Burstein M, Scholnick HR, Morfin R. Rapid method for the isolation of lipoproteins from human
semm by precipitalion wilh polyanions. J Lipid Res 1970; II :583-95.
22 Grove TH. Effect of reagent pH on determination of high-density lipoprotein cholesterol by
precipitation with sodium phosphotungstate-magnesiulll. Clin Chim Acta 1979;2S:S60w4.
23 Cheung MC, Albers JJ. The measurement of apolipoprotein Aw 1 and Aw2 levels in men and women
by immunoassay. J Clin Invesl 1977;60:43-50.
24 Gidez LI, Miller GJ, Burstein M, Slagle S, Eder HA. Separation and quantitation of sUbclasses of
human plasma high-density lipoproteins by a simple precipitation procedure. J Lipid Res 1982;23: 1206-23.
-32-

Chapter 2
25 Havekes LM, de Knyff p. Beisiegel U, Havinga J, Smit M, Klasen E. A rapid micromethod for
apolipoprotein E phenotyping directly in serum. J Lipid Res 1987;28:455-63.
26 Cohn JS, McNamara JR, Cohn SD, Ordovas JM, Schaefer EJ. Postprandial plasma lipoprotein
changes in human subjects of different ages. J Lipid Res 1988;29:469-79
27 Krasinsky SD, Cohn JS, Schaefer EJ, Russell RM. Postprandial plasma retillyl ester response is
greater in older subjects compared with younger subjects. Evidence for delayed plasma clearance
of intestinal lipoproteins. J Clin Invest 1990;85:883-92
28 Morrison JA, Kelly K, Horvitz R, Khoury P, Laskarzewski PM, Mellies MJ, Glueck Cl Parent
offspring and sibling lipid and lipoprotein associations during and after sharing household
environments: The Princeton School District Family Study. Metabolism 1982;31: 158-66.
29 Weinberg R, Webber LS, Berenson GS. Hereditary and environmental influence on cardiovascular
risk factors for children. Am J Epidem 1982;116:385-93.
30 Berr F, Eckel RH, Kem F Jr. Contraceptive steroids increase hepatic uptake of chylomicron
remnants in healthy young women. J Lipid Res 1986;27:645-51.
31 Breckenridge we, Little JA, Steiner G, Chow A, Poapst M. Hypertriglyceridemia associated with
deficiency of apolipoprotein C-II. N Engl J Med 1978;298: 1265-73.
32 Redgrave TG. Fonnation of cholesteryl ester-rich particulate lipid during metabolism of
chylomicrons. J Clin Invest 1970;49:465-71.
33 Stalenhoef AFH, Malloy MJ, Kane JP, Havel RJ. Metabolism of apolipoproteins B-48 and B-I00
of triglyceride-rich lipoproteins in nonnal and lipoprotein lipase-deficient humans. Proc Natl Acad
Sci USA 1984;81:1839-43.
34 Goodman DS, Blomstrand B, Werner B, Huang HS, Shiratori T. The intestinal absorption and
metabolism of vitamin A and beta carotene in man. J Clin Invest 1966;45:1615-23.
35 Sherrill BC, Innerarity lL, Mahley RW. Rapid hepatic clearance of the canine lipoproteins
containing only the E apoprotein by a high affinity receptor: Identity with the chylomicron remnant
transport process. J BioI Chern 1980;225:1804-7.
36 Krasinski SO, Cohn JS, Russell RM, Schaefer EJ. Postprandial plasma vitamin A metabolism in
humans: a reassessment of the use of plasma retinyl esters as markers for intestinally derived
chylomicrons and their remnants. Metabolism 1990;39:357~65.
37 Wilson DE, Chan IF, Ball M. Plasma lipoprotein retinoids after vitamin A feeding in nonnalman:
minimal appearance ofretinyl esters among low·density lipoproteins. Metab Clin Exp 1983;32:514-
7.
38 Berr F, Kern F. Plasma clearance ofchylomicrons labelled with retinyl palmitate in healthy human
subjects. J Lipid Res 1984;25:805-12.
39 Cohn JS. McNamara JR, Krasinski SD, Russell RM, Schaefer EJ. Role of triglyceride~rich
lipoproteins from the liver and intestine in the etiology of postprandial peaks in plasma triglyceride
concentration. Metabolism 1989;38:484-90.
40 Boenvinkle E, Brown S, Sharrett AR, Heiss GJ Patsch W. Apolipoprotein E polymorphism
-33-

Chapter 2
influences postprandial retinyl palmitate hut not triglyceride concentrations. Am J Hum Genet
1994;54:341-60.
41 Simons LA, Dwyer T, Simons J, Bernstein L, Mock P, Poonia NS, Balasubramaniam S, Baron D,
Branson J, Morgan J, Roy P. Chylomicrons and chylomicron remnants in coronary artery disease:
a case~control study. Atherosclerosis 1987;65:181-9.
42 Ryu JE, Howard 0, Craven TE, Bond MG, Hagaman AP, Crouse JR. Postprandial triglyceridemia
and carotid arteriosclerosis in middle-aged subjects. Stroke 1992j23:823-8.
43 Weintraub MS, Zedmer R, Brown A, Eisenberg S, Breslow JL. Dietary polyunsaturated fats of the
W-6 and W-3 series reduce postprandial lipoprotein levels. Chronic and acute effects of fat
saturation on postprandial lipoprotein metabolism. J Clin Invest 1988;82:1884-93.
-34-

Chapter 2
In an editorial accompanying the publication of the study described in chapter 2 (I), the
possible explanations for postprandial offspring group differences found in this study were
discussed. These included mechanisms by which the differences could be acquired or genetic,
the latter being either monogenic of polygenic. It was proposed that a monogenic defect may
exist that affects triglyceride metabolism. In that case the postprandial group differences might
be explained by much more marked responses in a few sons who inherited this defect rather
than a general shift of the distribution of responses for the gl'Oup as a whole. In the reaction
described below this possibility was analyzed.
Triglyceride levels in sons of patients with coronary artery disease (Re)
To the editor: We thank Dr. Grundy (l) for his supportive and useful discussion of our
report (2), in which he considers various explanations for the prolonged postprandial
hypertriglyceridemic response in the sons of patients with coronary artery disease. Dr. Grundy
suggests that we examine the possible bimodality of responses in the offspring of patients, a
bimodality that would theoretically emerge if group differences could be attributed to a
heterozygous monogenic defect of triglyceride metabolism in patients. Given this monogenic
hypothesis, a subgroup of patients having the gene would transmit it to 50% of their offspring.
Consequently, a subgroup of sons would have marked postprandial responses, and Dr. Grundy
suggests that these responses may explain the effect that we found.
A classic debate between Platt and Pickering (reviewed in reference 3) on the mode of
transmission of primary hypertension on the basis of the shapes of blood pressure distribution
curves has shown that bimodality, as distinct from left-skewing, in such curves is not easily
proved. Further, a familially acquired abnormality in only a subgroup of families could
theoretically lead to a similar bimodality. This and the relatively small sample size of our
study initially led us not to engage in such an analysis. An alternative approach in unravelling
putative modes of inheritance is segregation analysis, but such an analysis would not be overly
informative in tillS case because of the limited number of siblings in our study. Nevertheless,
we have attempted to address Dr. Grundy's suggestion. Figure 2.3 shows the frequency
distribution of areas under the curve of the triglyceride response for sons of patients 6 to 12
hours after lipid loading. Although not a normal distribution, the mnnber of observations does
not allow definite conclusions on modality. Moreover, if those with a response above the
arrow (n=7) are exluded from the analysis, the difference between offspring groups remains
-35-

Chapter 2
of borderline significance (difference, 0.78 rumol x hJL; 95% CI, -0.015 to 1.574). Thus, it
seems that offspring group differences cannot be fully explained by a subgroup of sons of
patients with markedly high postprandial responses. Although this analysis must be evaluated
with some caution, the monogenic mechanism as the sale explanation for prolonged
postprandial hypertriglyceridemia does not appear to be supp011ed by our data.
c-15 -
r-r-
c- -c-5
- ! c- -c-
o rT I n n Area under curve (t6 - t12)
Figure 2.3, Frequency distribution of area under the curve (l nunol x hIL intervals) for sons of patients with coronary artery disease. t6-t12 '" triglyceride responses 6 to 12 hours after lipid loading. Patients with responses higher than that indicated by the arrow were excluded from the analysis.
-36-

Chapter 2
References
Grundy SM. Triglyceride levels in sons of patients with coronary artery disease [Editorial]. Ann
Intem Med 1994;121:614-5.
2 Uiterwaal CSPM, Grobbee DE, Witteman JCM, van Stiphout WAHJ, Krauss XH, Havekes LM,
de Bruijn AM, van Tol A, Hofman A. Postprandial triglyceride response in young adult men and
familial risk for coronary atherosclerosis. Aim Intem Med 1994;121:576·83.
3 Swales JD, ed. Platt versus Pickering: An episode in recent medical history. London: Keynes Press;
1986.
-37-


CHAPTER 3
LIPOPROTEINS AND APOLIPOPROTEINS IN YOUNG ADULT MEN
AND WOMEN AND RISK FOR CORONARY ATHEROSCLEROSIS

Abstract
3. Lipoproteins and Apolipoproteins in Young Adult Men
and Women and Risk for Coronary Atherosclerosis
Atherosclerotic lesions develop early in life. The role of lipoproteins and apolipoproteins in
the atherosclerotic process at a young age is not completely elucidated. The aim of the present
study was to assess lipoprotein and apolipoprotein levels in young adults in relation to
coronary atherosclerosis in their parents. We studied the offspring of patients who were admitted for diagnostic coronary angiography
in several general hospitals in the Netherlands. From these patients we selected a group of
male patients (n~90), who had severe coronary atherosclerosis at angiography, and a reference
group of male patients (n~62), who had no coronary atherosclerosis at angiography.
Lipoprotein and apolipoprotein levels were determined in 115 sons and 73 daughters of the
patients with severe coronary atherosclerosis. These were compared to levels in 68 sons and
47 daughters of men from the reference group.
Lower levels of HDL, cholesterol and apolipoprotein A2 were found in sons of patients
suffering from severe coronary atherosclerosis. Similar differences were observed in daughters
of such patients without, however, achieving statistical significance. Our findings add to the growing evidence that changes in lipoprotein and apolipoprotein
levels can be detected relatively early in life. It is concluded that the low levels of HDL,
cholesterol and apolipoprotein A2 found in sons of patients with severe coronary sclerosis may
playa role in the development of coronary atherosclerosis.
Introduction
Cholesterol levels and other risk factors in the young are related to atherosclerotic lesions
which may develop early in life (1-4). Total serum cholesterol levels measured in adolescent
men have also been shown to be associated to the occurrence of manifest cardiovascular
disease later in life (5). Less is known, however, about the role of lipoproteins and
apolipoproteins at a young age. One way to study the relation between lipoproteins and
apolipoproteins in relation to coronary artery disease is to examine the offspring of parents
who suffer from coronary atherosclerosis. Coronary heart disease and its risk factors tend to
aggregate in families (6-9). Recent prospective studies have shown that a parental history of
-40-

Chapter 3
myocardial infarction is a risk factor for coronary artery disease, which is independent from classical cardiovascular risk factors (10,11). Thus, there may be other as yet unknown genetic
or acquired risk factor for coronary artery disease. In the present study lipoproteins and apolipoproteins in 188 children of fathers who suffered
from severe clinically manifest and angiographically proven coronary atherosclerosis were compared to levels measured in 115 children of fathers who did not have coronary
atherosclerosis at diagnostic coronary angiography.
Subjects and methods
From 1987 to 1992 two groups of male patients were selected from the coronary
angiography databases of the cardiology departments of the Zuiderziekenhuis in Rotterdanl
(1987 - 1991), the Academic Hospital Dijkzigt in Rotterdam (1988 - 1989), the Refaja
Ziekenhuis in Dordrecht (1990 - 1991), and the Antonius Hospital in Nieuwegein (1992), the
Netherlands. The index group had severe coronary atherosclerosis, defined as more than 70%
stenosis in at least three major coronary vessels at angiography (CAD+ fathers). A reference
group had no or only minor angiographic lesions, defined as 20% stenosis or less in all
coronary vessels (CAD- fathers). Additional criteria for both groups of men were: (I) age
between 45 and 65 years, (2) blood pressure not exceeding 160/100 mmHg, (3) absence of
liver disease, diabetes mellitus, thyroid disease, and renal disease, (4) coronary angiography
within two years preceding examination, (5) first consultation of a physician for cardiac
complaints within five years preceding examination for this study. Eligible subjects were sent
a letter in which they, their children and the mothers of their children were invited to
participate in the study. The average time elapsed since catheterisation to the present
examination was 12.6 ± 6.0 months (mean ± SD) for CAD+ fathers and 13.6 ± 6.4 for CAD
fathers.
Measurements
The fathers, mothers, sons and daughters were asked to come to the hospital at 9.00 a.m.
after fasting for at least 12 hours. Systolic blood pressure (SBP) and diastolic blood pressure
(DBP) were measured using a random zero sphygmomanometer (Hawksley). Fasting senull
blood samples were drawn by antecubital venipuncture for measurement of triglycerides, total
-41-

Chapter 3
cholesterol, low density lipoprotein cholesterol (LDL cholesterol), high density lipoprotein
cholesterol (HDL cholesterol), its subfractions HDL, cholesterol and HDL, cholesterol,
apolipoprotein AI, apolipoprotein A2, and apolipoprotein B. Height and weight were measured
without shoes and heavy clothing. The Quetelet-index was calculated as weight (kg) divided
by the square of height (m').
The fathers answered a questionnaire with questions on the number of first degree relatives
who had suffered from myocardial infarctions and on the use of medication at the time of
exanlination (medication was taken to the hospital). Parents and children answered a
questionnaire referring to a one month period prior to the examination, with questions on use of medication, habitual alcohol intake, coffee intake, and smoking habits. In addition, mothers
and daughters were asked about the use of oral contraceptives, menstrual cycle and
pregnancies. Sons and daughters were also asked about changes in lifestyle (physical activity,
smoking behavior, and fat intake) since their fathers had first been exanlined by a physician
for cardiac complaints. In the first 50 families selected for this study all members were invited
for baseline measurements only. In these families the response rate was 92%. In the next 102
families the sons (80 sons of CAD+ fathers and 57 sons of CAD- fathers) were invited to
come to the hospital on a separate day because of their simultaneous involvement in another
study for which the criteria and conditions were similar to those in the present study. The sons
as well as the daughters from these 102 families underwent the same measurements under the
same conditions as the offspring of the first 50 fanlilies. The protocol of the extended study
required sons from these 102 families to stay in the hospital for 12 hours, and the response
rate was lower (65%) in this group of sons.
Laboratory analysis
Serum total cholesterol was measured with an automated enzymatic method, using the
Boehringer Mammeim (FRG) CHOD-PAP reagent kit (12). HDL and LDL cholesterol were
measured by the same method after precipitation. For HDL cholesterol the phosphotungstate
method according to Burstein (13), with a minor modification as described by Grove (14) was
used. For LDL cholesterol precipitation was carried out with polyvinylsulphate (Boehringer
Mannheim, FRG). Throughout the entire study period the results of both total cholesterol and
HDL cholesterol were within limits of the quality control progranlllle of the WHO Regional
Lipid Reference Centre (prague, Czechoslovakia). Apolipoproteins Al and B were assayed by
an automated immunoturbidimetric method (Kone Diagnostics, Espoo, Finland).
-42-

Chapter 3
Apolipoprotein A2 was determined by radial inununodiffusion against specific antisenun
(Boehringer Mannbeim, FRO) according to Cheung and Albers, with slight modifications (15).
All automated analyses were carried out on the Kone Specific Analyzer (Kone Instruments,
Espoo, Finland) using frozen (-20°C) serum samples. HDL, and HDL, cholesterol subfractions
in serum were assayed as described by Gidez et al. (16) with slight modifications. HDL, and
HDL, cholesterol subfractions were separated using stepwize precipitation of apolipoprotein
B containing lipoproteins with heparin/Mn" in two steps and HDL, with dextran-sulphate.
Statistical methods
Mean values and standard deviations were calculated for all characteristics of the two groups
of fathers, mothers, sons and daughters, separately. Mean group differences in baseline
characteristics were tested with the t-test or MarUl-Whitney U test when appropriate, and the
X' test for proportional data. All further analyses were adjusted for age. Adjusted mean values
for lipoproteins levels in parents and offspring were obtained using linear regression analysis with the (apo)lipoprotein level as the dependent and a group indicator and age as the
independent variables. The associations between (apo)lipoprotein levels in family members
were assessed by linear regression analysis. This analysis included fathers and mothers and the
first sons or daughters taking part in the study. Because of the dependency of measurements
between brothers and between sisters within families, group differences between lipoprotein
values in the offspring were analyzed u,ing a repeated measures analysis of variance where
fathers were considered the sampling units (BMDP, 1990). In this analysis, lipoprotein values
in sons and daughters were considered repeated measures within fathers. In the repeated
measures analysis mean lipoprotein levels were adjusted for age, as well as for a combination of age, height, weight, systolic blood pressure, diastolic blood pressure, smoking, alcohol
intake and in daughters the use of oral contraceptives.
Results
Table 3.1 shows the characteristics of the CAD+ patients and the CAD- reference group, as
well as those of their family members. On average CAD+ patients and their family members
were older. Significant differences were present in a number of characteristics. Fathers of the
CAD- group were taller, the proportion of smoking mothers was higher in the CAD- group,
-43-

Chapter 3
systolic and diastolic blood pressure were on average higher in sons of CAD+ and the
proportions of smokers and users of coffee as well as the Quetelet-index were higher in
daughters of CAD+. After adjustment for age only the group differences in smoking in
mothers and diastolic blood pressure in sons remained significant.
In table 3.2 the mean (apo)lipoprotein levels are given for fathers and mothers from both
groups. There were considerable differences with regard to lipids and apolipoproteins between
the two groups of fathers. CAD+ fathers had higher levels of total and LDL cholesterol, of
triglycerides and of apolipoprotein B and lower levels of HDL cholesterol than CAD- fathers.
Further adjustment for other risk factors did not materially change these results (data not
shown). In the mothers the only difference was a higher triglyceride level in the wives of
CAD+ and a higher apolipoprotein A I after adjustment for other risk factors.
Table 3.3 shows the mean age adjusted lipoprotein and apolipoprotein values for the sons
and the daughters. Sons and daughters of CAD+ fathers on average had adverse lipoprotein
and apolipoprotein levels compared with sons and daughters of CAD- fathers.
Table 3.4 gives the mean differences between the groups of sons and daughters with regard
to lipoprotein and apolipoprotein levels, as analyzed with repeated measures analysis of
variance. Sons of CAD+ fathers had significantly lower levels of HDL, cholesterol and
significantly lower levels of apolipoprotein A2. None of the other group differences was
statistically significant. HDL, cholesterol and apolipoprotein A2 levels were also somewhat
lower in daughters of CAD+ fathers, but none of these as well as other differences were
statistically significant. An additional repeated measures analysis in which all families were
excluded in which either one or both parents and one or more offspring had total cholesterol
levels exceeding 300 mgldl yielded similar results. When all families were excluded in which
one of the parents had a total cholesterol level exceeding 300 mgldl similar results were
observed with significantly lower levels of HDL, cholesterol and apolipoprotein A2 in sons
of CAD+ fathers.
For total cholesterol there were significant associations between levels in fathers and sons
(regression coefficient b=0.38, 95% confidence interval 0.21,0.56), mothers and sons (b=0.47,
95% CI 0.24,0.70), fathers and daughters (b=0.32, 95% CI 0.13,0,51), and mothers and
daughters (b=0.39, 95% CI 0.15,0.63). For LDL cholesterol and apolipoprotein B similar
associations were observed. The strongest associations were found for apolipoprotein Al
between fathers and offspring and in particular sons (b=0.65, 95% CI 0.50,0.80), mothers and
sons (b=0.78, 95% CI 0.60,0.95) and mothers and daughters (b=0.57, 95% CI 0.37,0.76).
Apolipoprotein A I also showed the strongest association between levels in sons and daughters
-44-

Table 3.1. Characterist:ics of CAD+ and CAD- fathers and mothers and offspring.
Variable Fathers Mothers Sons Daughters
CAD+ CAD- CAD+ CAD- CAD+ CAD- CAD+ CAD-(n"'90) (n952) (n"'9l) (n95l) (n=lIS) (n958) (n=73) (-7)
Age (yrs) 56.4 ± 7.6 522 ± 8.1 t 52.5 ± 9.4 492 ± 7.9 * 25.5 ± 6.4 22.5 ± 5.6 t 25.4 ± 83 21.4 ± 7.7 t
Height (em) 175.6 ± 6.0 178.6 ± 7.9 * 1663 ± 6.1 1662 ± 6.4 180.8 ± 9.7 1813 ± 11.3 167.0 ± 7.5 167.6 ± 9.9
Weight (kg) 78.5 ± 8.7 79.8 ± 11.0 72.4 ± 12.5 71.4 ± 103 75.8 ± 12.9 73.8 ± 13.3 63.7 ± lI.5 60.1 ± 14.0
Quetelet-index (kglm') 25.4 ± 2.2 25.0 ± 2.9 262 ± 4.5 25.9 ± 3.9 23.0 ± 2.9 22.3 ± 3.1 22.9 ± 4.0 212 ± 3.8 *
... SBP(mmHg) 127.2 ± 12.8 127.5 ± 16.9 127.0 ± 16.7 125.3 ± 14.8 122.9 ± 13.4 1182 ± 14.5* 113.5 ± 14.5 1\6.0 ± 11.2
'1' DBP (mmHg) 84.1 ± 11.1 82.1 ± 10.3 83.6± 11.1 81.0 ± 8.3 79.4 ± 10.1 73.9 ± 12.7t 74.3 ± !I.O 72.5 ± 8.4
Smoking (%) 18.9 21.0 18.7 36.1 * 33.9 29.4 37.0 19.1 *
Alcohol intllke (gIday) 13.8 ± 13.6 14.1 ± 11.4 6.4 ± 7.7 6.7 ± 8.0 11.6 ± 12.9 93 ± 9.6 4.8 ± 6.0 5.6 ± 6.4
Coffee drinking (%) 98.9 93.5 97.8 98.4 82.6 73.5 753 5L1 t
Post menarche (%) 92.8 84.1
Pregnant at 2.9 7.1 examination (%)
Use of oral 435 452 contraceptives (%)
Values are means ± SD, unless stated otherwise. SBP = systolic blood pressure, DBP = diastolic blood pressure. Q -5 * = p<O.05; t = p<O.OI for differeoces between CAD+ and CAD-. ~ w

Chapter 3
Table 3.2. Lipoproteins and apolipoproteins of CAD+ and CAD· fathers and the respective mothers in both groups,
Variable Fathers Mothers
CAD+ CAD· CAD+ CAD·
(n~O) (n~2) (n~l) (n~61)
Total cholesterol (mmolll) 6.9 ± 0.11 6.3 ± 0.14 + 6.6 ± 0.2 6.6 ± 0.18
LDL cholesterol (mmolll) 5.I±O.l1 4.5 ± 0.13 , 4.6 ± 0.15 4.8 ± 0.19
HDL cholesterol (mOlolll) 1.1 ± 0.03 1.2 ± 0.04 • 1.4 ± 0.03 1.3 ± 0.03
HDL2 cholesterol (mmolll) 0.2 ± 0.01 0.2 ± 0,02 0.4 ± 0.03 0.3 ± 0.02
HDL) cholesterol (nmlolll) 0.9 ± 0.02 0.9 ± 0.02 1.1 ± 0.03 1.0 ± 0.02
Triglycerides (mmolll) 2.09 ± 0.09 1.50 ± 0.12 t 1.48 ± 0.08 1.25 ± 0.06 •
Apolipoprotein AI (mg/dl) 133.5 ± 2.5 135.6 ± 3.8 155.0 ± 3.5 145.2 ± 3.8
Apolipoprotein A2 (mg/dl) 45.3 ± 0.8 46.6 ± 0.8 47.3 ± 0.7 47.1 ± 0.9
Apollpoproteln B (mg/dl) 131.4 ± 3.3 110.2 ± 3.7 I 111.0 ± 3.6 106.0 ± 3.5
Values are means ± SEM, adjusted for age, LDL :=: low density lipoprotein, HDL :=: high density lipoprotein,
• '" p<O.05j ~ :=: p<O.OOI for differences between CAD+ and CAD·.
(b~0.55, 95% CI 0.35,0.74). Between fathers and mothers associations were observed for
HDL, cholesterol (b~0.25, 95% CI 0.12,0.39) and apolipoprotein Al (b~0.43, 95% CI
0.32,0.55). Much weaker or no associations between family members were observed for the
other lipoproteins.
We have attempted to assess the effects of possible changes in lifestyle, possibly advised to
fathers, which may have been passed on to the children. There were no differences between
the two groups of sons with regard to changes in reported smoking behavior, alcohol intake
and fat intake after their fathers had been first examined for cardiac complaints. However,
since this first examination, 39% of daughters of CAD+ fathers reported to have diminished
their fat intake, as opposed to 17% of daughters of CAD· fathers (Yates corrected X' 5.1,
·46·

Chapter 3
Table 3.3, Lipoproteins and apolipoproteins of the offspring of CAD+ and CAD~ fathers.
Variable Sons Daughters
CAD+ CAD- CAD+ CAD-
(n~115) (n~8) (n=l7) (n~73)
Total cholesterol (mmolll) 5.4 ± 0.11 5.0 ± 0.10 5.6 ± 0.14 5.0 ± 0.15
LDL cholesterol (mmolll) 3.7 ± 0.11 3.3 ± 0.10 3.6 ± 0.14 3.1 ± 0.15
HDL cholesterol (mmolll) 1.2 ± 0.02 1.2 ± 0.03 1.5 ± 0.04 1.5 ± 0.04
HDLl cholesterol (mmol/l) 0.2 ± 0,01 0.2 ± 0.02 0.4 ± 0.03 0.4 ± 0.03
HDLJ cholesterol (nmlOlIl) 0.9 ± 0.02 1.0 ± 0.02 1.1 ± 0.02 1.1 ± 0.03
Triglycerides (mmolll) 1.16 ± 0.06 1.13 ± 0.Q7 1.14 ± 6.0 1.04 ± 8.0
Apolipoproteln AI (mg/dl) 126.6 ± 2.5 123.8 ± 2.8 159.6 ± 3.7 151.6 ± 4.3
Apolipoprotein A2 (mg/dl) 44.1 ± 0.6 47.5 ± 1.3 46.6 ± 1.0 48.0 ± 1.0
Apolipoprotein B (mg/dl) 89.4 ± 2.5 83.9 ± 2.5 86.9 ± 2.6 77.8 ± 3.6
Apollpoproteln AI/B 1.6 ± 0.04 1.5 ± 0.06 1.9 ± 0.Q7 2.1 ± 0.09
Values are means ± SEM, adjusted for age,
p~0.02). A repeated measures analysis was performed in which an adjustment was made for
the offspring living either with their parents or on their own. This analysis showed lower
levels of HDL, cholesterol (difference -2.6 mgldl, 95% CI -5.3,0.2) and apolipoprotein A2
(-5.5 mgldl, 95% CI -8.4,-2.5) in sons of CAD+ fathers. Similar results were observed in
daughters of CAD+ fathers who had lower levels of HDL, cholesterol (-4.5 mgldl, 95% CI
-8.2,-0.9) and apolipoprotein A2 (-4.5 mgldl, 95% CI -8.3,-0.7).
-47-

Chapter 3
Table 3.4. Differences in lipoproteins and apolipoproteins of the offspring of CAD+ and CAD· fathers.
Variable Sons Daughters
Adjusted for Difference 95 %C.I. Difference 95% C.I.
Total cholesterol (nunoI/l) age 0.11 [-0.18, OAI) 0.19 [-0_29, 0_68)
age/risk factors· 0.0005 [-0.31, 0.32) 0,28 [-0,22, 0,78)
LDL cholesterol (mmoI/l) age 0,14 [-0,16,0.44) 0_16 [-0,34, 0,66)
age/risk factors 0,09 [-0,23, 0.42) 0,24 [-0,26, 0,74)
HDL cholesterol (nunoI/l) age -0,04 [-0,13, 0,05) -0,005 [-0.13, 0.12)
age/risk factors -0,07 [-0,16,0,02) -0,04 [-0.15,0.06)
HDL2 cholesterol (mmoI/l) age 0,02 [-O.oJ, 0,08) 0,05 [-O.oJ,0,14)
age/ risk factors 0,005 [-0.05, 0,06) 0,06 [-0,01, 0.12)
HDL) cholesterol (mmoI/l) age -0,07 [-0.13,-0,0005) -0,05 [-0.13,0,04)
age/risk factors -0,09 [-0.16,-0,03) -0,07 [-0,15, 0,02)
Trlglycerides (mmolll) age -0,03 [-0.22,0.16) 0,09 [-0,32,0,15)
age/risk factors -0.11 [-0.32,0,09) 0.13 [-0.09, 0,36)
Apolipoprotein Al (mg/dl) age 3,1 [-6,3,12.5) 10,6 [-2,0, 23,3)
age/risk factors -2,8 [-11.7,6,1) 11.9 [-0,7, 24,6)
Apolipoprotein A2 (mgldl) age -5.1 [-7,9,-2.3) -2,7 [-5,9, 0,6)
age/risk factors -4.4 [-7,0,-1.9) -2,1 [-5.3, 1.2)
Apolipoprotein B (mgldl) age 2,1 [-5,1,9,2) 5,7 [-4.5, 15,9)
age/risk factors -0,6 [-7,9,6,7) 8,1 [-1.3, 17.5)
Apolipoprotein AI/B age 0,07 [-0,09,0,22) -0,05 [-0.30,0,20)
age/risk factors 0,007 [-0,14,0,16) -0,08 [-0,31,0.14)
Values are mean differences (values offspring CAD+ fathers· values offspring CAD· fathers) as calculated with repeated measures analysis of variance; 95% C.I.= 95% confidence interval; LDL = low density lipoprotein, HDL
= high density lipoprotein; • = adjusted for risk factors: height, weight, systolic blood pressure, diastolic blood pressure, smoking, alcohol intake, and (daughters) use of oral contraceptives,
-48-

Chapter 3
Discussion
In this study we observed differences in lipoproteins and apolipoproteins between the
offspring of fathers with and without coronary atherosclerosis. Sons and daughters of CAD+
fathers had a less favorable (apo)lipoprotein profile. Sons of patients with coronary artery
disease had lower HDL, cholesterol and apolipoprotein A2 levels. Daughters of such patients
tended to have lower levels of HDL, cholesterol and apolipoprotein A2 as well, but these
differences reached only borderline significance.
Before interpreting these findings some methodologic aspects of the study need to be
discussed. We have assessed lipoprotein and apolipoprotein levels in young healthy adults in
relation to coronary atherosclerosis in their parents. The selection of patients was based on
coronary angiography, which enabled us to relate lipoprotein and apolipoprotein levels directly
to risk of atherosclerosis. Coronary angiographic criteria were severe tluee-vessel disease in CAD+ fathers and virtually no coronary sclerosis in CAD- fathers in order to maximize the
atherosclerotic contrast between these groups. This contrast is reflected in the differences
found between the two groups of fathers with regard to lipoproteins and apolipoproteins,
CAD+ fathers having a less favorable (apo)lipoprotein profile.
Although there may be differences between the two groups of fathers with regard to lifestyle
and medication, important differences, e.g. medication, will not be present in the offspring.
A higher proportion of daughters of CAD+ fathers reported to have changed fat intake after
their fathers had first been exanlined for cardiac complaints, but this was not accompanied by
a change in other aspects of lifestyle, in particular smoking. Thus, the possibility that
differential group changes of lifestyle could explain group differences in lipoproteins and
apolipoproteins, cannot be completely ruled out. However, as it is not likely that changes to
healthier lifestyles affect lipoprotein levels unfavorably, tlllS, if present, results in an
underestimation of the true differences. Support for this was found in the analysis in which
we adjusted for possible differences between offspring living with or separately from their
parents. The latter group is supposedly less affected by lifestyle advise given to the fathers.
This analysis did not materially change the results.
The findings of the pres~nt study are generally in agreement with those in other studies (17)
in that the offspring of patients suffering from coronary artery disease have less favorable
lipid profiles. However, some studies have indicated that apolipoproteins, and particularly the
ratio apolipoprotein Al/apolipoprotein B, measured in offspring of CAD patients are more
strongly related to risk of cardiovascular disease than other (apo)lipoproteins (18-21). In the
present study apolipoprotein B level and the ratio apolipoprotein Allapolipoprotein B were
-49-

Chapter 3
not found to be significantly different between groups. Furthermore, in contrast to earlier
studies, we found that HDL, cholesterol and apolipoprotein A2 levels in offspring of CAD+
fathers and particularly the sons of CAD+ fathers show important differences. Differences in
results between earlier studies and the present study are that (apo)lipoproteins in offspring
were studied in relation to myocardial infarction in the parents (19-21) and not specifically
to atherosclerosis, which may reflect other mechanisms in addition to those leading to
atherosclerosis. Another explanation for these differences may be that in the present study the
offspring was older than in other studies (18-19).
An inverse relation between HDL cholesterol and risk of ischemic heart disease is well
established (22-25). HDL cholesterol has been shown to aggregate within families of patients
with myocardial infarction (26,27) and, recently, HDL cholesterol subfractions and
apolipoprotein Al as well as apolipoprotein A2 have been reported to be strongly and
independently associated with risk of myocardial infarction (28,29). The results of the present
study are in line with these studies and suggest that HDL cholesterol, its subfractions and
related apolipoproteins playa role in atherogenesis early in life. The specific role that the
HDL subfractions HDL, and HDL, play in the inverse relation with ischemic heart disease
still has to be elucidated, although HDL, is thought to be the most important factor in this
respect. In the present study total HDL cholesterol levels are somewhat lower in sons of
CAD+ fathers and not materially different between the two groups of daughters, and HDL,
cholesterol tends to be higher in both the sons and daughters of CAD+ fathers, which is
suggestive of a shift from HDL, to HDL, cholesterol in sons and daughters of CAD+ fathers.
In summary, we have compared lipoprotein and apolipoprotein levels in the offspring of
patients suffering from severe, angiographically proven, coronary atherosclerosis with levels
in offspring of patients with angiographically minimal coronary atherosclerosis. Lower levels
of HDL, cholesterol and apolipoprotein A2 were found in the offspring and particularly in the
sons of patients suffering from severe coronary atherosclerosis. Our findings add to the
growing evidence that changes in lipoprotein and apolipoprotein levels can be detected
relatively early in life. It is concluded that sons of patients with severe coronary sclerosis have
reduced levels of HDL, cholesterol and apolipoprotein A2 and that these reduced levels may
playa role in the development of coronary artery disease.
Acknowledgements
The authors thank Ms. Lorette O.M. Hulsman for assistance in the conduct ofthe study, Ms.
-50-

Chapter 3
Jeannette M. Vergeer-Drop for assistance in laboratory analyses, and the cardiologists Dr. H.J.
Kingma, Antonius Hospital in Nieuwegein, Dr. Ph. W. Fels, Refaja Ziekenhuis in Dordrecht
and Dr. F.!. ten Cate, University Hospital Rotterdanl, The Netherlands for their help in the
selection of patients. Tllis investigation was supported by a grant of the Netherlands
Prevention Fund.
References
Newman WP III, Freedman OS, Voors AW, Gard PO, Srinivasan SR, Cresanta JL, Williamson GS, Webber LS, Berenson GS. Relation of serum lipoprotein levels and systolic blood pressure
to early atherosclerosis: The Bogalusa Heart Study. N Engl J Med 1986;314: 138-44. 2 Freedman OS, Newman WP Ill, Tracy RE, Voors AW, Srinivasan SR, Webber LS, Restrepo C,
Strong JP, Berenson GS. Black/white differences in aortic fatty streaks in adolescence and early
adulthood: The Bogalusa Heart Study. Circulation 1988;77:856-64. 3 Pathobiological Determinants of Atherosclerosis in Youth (POA Y) Research Group. Relationship
of atherosclerosis in young men to serum lipoprotein cholesterol concentrations and smoking.
JAMA 1990;264:3018-24. 4 Berenson GS, Wattigney WA, Tracy RE, Newman WP III, Srinivasan SR, Webber LS, Oalferes
ER, Strong JP. Atherosclerosis of the aorta and coronary arteries and cardiovascular risk factors
in persons aged 6 to 30 years and studied at necropsy: The Bogalusa Heart Study. Am J Cardiol
1992;70:851-8. 5 Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Liang KY, Levine OM. Serum cholesterol in
young men and subsequent cardiovascular disease. N EngJ J Med 1993j328:3l3~8.
6 llissanen AM. Familial aggregation of coronary heart disease in a high incidence area (North Karelia, Finland). Br Heart J 1979;42:294-303.
7 Friedlander Y, Bucher KD, Namboodiri KK, Heiss G, Kark ill, Tyroler HA, Eisenberg S, Stein Y, Rifkind BM. Parent-offspring aggregation of plasma lipids in selected populations in North
America and Israel: The Lipid Research Clinics Prevalence Study. Am J Epidemiol 1987; 126:268-79.
8 Barrett-Connor E, Khaw K-T. Fanlily history of heart attack as an independent predictor of death due to cardiovascular disease. Circulation 1984j69:1065~9.
9 Criqui MH, Barrett-COIlior E, Holdbrook MJ, Austin M, Turner ID. Clustering of cardiovascular
disease risk factors. Prev Med 1980;9:525-33. 10 Colditz GA, Rimm EB, Giovallnucci E, Stampfer MJ, Rosner B, Willett WC. A prospective study
of parental history of myocardial infarction and coronruy artery disease in men. Am J Cardial 1991 ;67:933-8.
11 Myers RH, Kiely DK, Cupples LA, Kannel WB. Parental history is an independent risk factor for
-51-

Chapter 3
coronary artery disease: The Framingham Study. Am Heart J 1990:120:963-9.
12 Van Gent CM, Van der Voort HA, de Bruijn AM, Klein F. Cholesterol detenninations. A
comparative study of methods with special reference to enzymatic procedures. Clin Chim Acta
1977;75:243-51.
13 Burstein M, Scholni~k HR, Morfin R. Rapid method for the isolation of lipoproteins from human
serum by precipitation with polyallions. J Lipid Res 1970; 11 :583-95.
14 Grove TH. Effect of reagent pH on detennination of high-density lipoprotein cholesterol by
precipitation with sodium phosphotungstate-magnesium. Clin Chim Acta 1979;25:560-4.
15 Cheung MC, Albers JJ. The measurement of apolipoprotein A-I and A-2 levels in men and
women by immunoassay. J Clin Invest 1977;60:43-50.
16 Gidez LI, Miller GJ, Burstein M, Slagle S, Eder. HA. Separation and quantitation of subclasses
of human plasma high-density lipoproteins by a simple precipitation procedure. J Lipid Res
1982;23: 1206-23.
17 Lee J, Lauer RM, Clarke WR. Lipoproteins in the progeny of young men with coronary artery
disease: children with increased risk. Pediatrics 1986;78:330-7.
18 Van Stiphout WAHJ, Hofinan A, Kruijssen HACM, Venneeren R, Groot PRE. Is the ratio apo
Blapo A-I an early predictor of coronary atherosclerosis? Atherosclerosis 1986;62: 179-82.
19 Freedman DS, Srinivasan SR, Shear CL, Franklin FA, Webber LS, Berenson GS. The relation of
apolipoproteins A-I and B in children to parental myocardial infarction. N Engl J Med
1986;315:721-6.
20 De Backer 0, Hulstaert F, De Munck K, RosseneuM, Van Parijs L, Dramaix M. Serum lipids and
apoproteins in students whose parents suffered prematurely from a myocardial infarction. Am
Heart J 1986;112:478-84.
21 Widhalm K, Koch S, Pakosta R, Schurz M, Brelldinger M. Serum lipids, lipoproteins and
apolipoproteins in children with and without familial history of premature coronary heart disease.
J Am ColI Nutr 1992:11:32S-3SS.
22 Atherosclerosis Study Group: Optimal resources for primary prevention of atherosclerotic diseases.
Circulation 1984;70: 157 A-20SA.
23 Heiss G, Johnson NJ, Reiland S, Davis CE, Tyroler HA. The epidemiology of plasma' high density
lipoprotein levels. The Lipid Research Clinics Program Prevalence Study. Circulation
1980;62(suppl IV): 116-36.
24 Gordon T, Kannel WB, Castelli WB, Dawber TR. Lipoproteins, cardiovascular disease and death.
The Framingham Study. Arch Intern Med 1981;141:1128-31.
25 Gordon T, Castelli WP, Hjortland MC, Kannel WE, Dawber TR. High density lipoprotein as a
protective factor against coronary heart disease. The Framinghanl Study. Am J Med 1977;62:707-14.
26 Pometta D, Micheli H, Raymond L, Oberhaensli I, Suenram A. Decreased lIDL cholesterol in
prepubertal and pubertal children of CHD patients. Atherosclerosis 1980;36: 10 1-9.
-52-

Chapler 3
27 Pometta D, Suenram A, Sheybani E, Grab E, James R. HDL cholesterol levels in patients with
myocardial infarctions and their families. Atherosclerosis 1986;59:21-9.
28 Buring JE, O'Connor GT, Goldhaber SZ, Rosner B, Herbert PN, Blum CB, Breslow JL,
Heilllekens CH. Decreased HD~ and HDLJ cholesterol, apo A-I and apo A-II, and increased risk
of myocardial infarction. Circulation 1991;85:22-9.
29 Stampfer MJ, Sacks FM, Salvini S, Willett WC, Hennekens CH. A prospective study of
cholesterol, apolipoproteins and risk of myocardial infarction. N Engl J Med 1991;325:373-81.
-53-


CHAPTER 4
FAMILIES AND NATURAL HISTORY OF LIPIDS IN CHILDHOOD:
AN 18 YEAR FOLLOW-UP STUDY

Abstract
4. Families and Natural History of Lipids in Childhood:
an 18 year Follow-up Study
Parental levels of total cholesterol were related to repeated measurements of total cholesterol
and lipoprotein-cholesterol in their offspring in the EPOZ study. In the EPOZ study (1975 -
1978) risk indicators for chronic diseases were studied in families of which the members were
5 years and over who were living in two districts in the Dutch town of Zoetermeer. A sample
of youngsters was subsequently followed up for 18 years (average follow-up: 13.8 years) with
yearly measurements of cardiovascular risk factors. Positive associations were found between
age-adjusted tertiles of parental cholesterol levels and offspring cholesterol and low density
lipoprotein-cholesterol levels, which persisted tlll'oughout childhood and young adulthood.
Offspring with both parents in the upper cholesterol tertile had almost I nl1'll01l1 higher
cholesterol levels compared to offspring with both parents in the lowest tertile. Differences
between offspring of parents with high total cholesterol levels and parents with low levels
were stable with increasing age of the offspring. There was considerable change with age of
offspring cholesterol levels, with a dip around puberty. For high density lipoprotein
cholesterol and its subfractions no relations with parental cholesterol level were found.
In tllis study the aim was to assess parental cholesterol level as a determinant of offspring
lipid level and change in lipid level over time. A strong positive association was shown
between parental cholesterol levels and offspring cholesterol and low density lipoprotein
cholesterol levels. This association was already detectable at a young age and persisted with
increasing age.
Introduction
The natural history of lipids and lipoproteins in children and adolescents (1-5) suggests that
serum lipids and lipoproteins show tracking from childhood into young adulthood, with lipid
and lipoprotein levels remaining at relatively stable ranks within distributions over time. Thus,
lipid and lipoprotein levels measured at a young age may be predictive of adult levels.
Furthermore, in a recent prospective study (6), total cholesterol levels in young men were
shown to be related to coronary heart disease much later in life. Preventive measures might
therefore already be taken in childhood and adolescence. Lipids and lipoproteins tend to
-56-

Chapter 4
aggregate within families (7) and selective cholesterol screening may, among other indications,
be recommended for children having a parent with a high blood cholesterol level (8).
Therefore, it is important to know if offspring of parents with high risk factor levels have
high levels themselves and to what extent these high levels persist throughout childhood and
young adulthood.
In this study the aim is to assess the relation between parental cholesterol level and offspring
lipid levels and change in offspring lipid levels with increasing age.
Methods
Subjects
All residents of ages 5 years and over who were living in two districts in the Dutch town
of Zoetermeer were invited to participate in a study of risk indicators for chronic diseases (Dutch acronym: EPOZ study) (9-11). Zoetermeer is a suburban residential community near
The Hague in The Netherlands, of at that time about 55,000 inhabitants. Between 1975 and
1979, 4,649 persons aged 5 - 19 years took part in the study (82% of those invited). In 1980
and 1981 all migrants moving to Zoetermeer were also asked to participate in the study. From
this total group a random sample of 596 children was selected for annual follow up in a study
of cardiovascular risk factors and its determinants. This paper deals with 483 subjects (81 %),
252 males and 231 females, who took part in the follow up study. The average follow-up
period was 13.8 years (range 3 to 18 years). Data on parents of these 483 subjects were
obtained at the baseline study (1975 - 1981). Complete data were available for 425 fathers and
454 mothers. In 1991, 352 subjects still took part in the follow up study.
Measurements
Both parents and offspring were seen at baseline (1975 - 1981). Subsequently, the offspring
were seen yearly and measurements were performed by one research assistant throughout the
whole follow-up period. At each examination systolic blood pressure (SBP) and diastolic
blood pressure (DBP) were measured using a random zero sphygmomanometer (Hawksley)
as described in detail elsewhere (12). Serum blood samples were drawn by antecubital
venipuncture for measurement of total cholesterol, low density lipoprotein-cholesterol, high
-57-

Chapter 4
density lipoprotein-cholesterol, and its subfractions high density lipoprotein2-cholesterol and
high density lipoprotein3-cholesterol. Height and weight were measured without shoes and
heavy clothing. At each examination, the offspring answered a questionnaire about use of
medication, alcohol intake, coffee consumption and smoking habits. Additionally, daughters
were asked about use of oral contraceptives, menstrual cycle and pregnancies.
Laboratory analysis
Serum total cholesterol at baseline was measured with an automated enzymatic method (13).
During follow-up a modified reagent was used (CHODIP AP High Performance, Boehringer
Mannheim, Germany). In the transition period both reagents have been used simultaneously,
obtaining an excellent correlation (r>0.99). The overall coefficient of variation was 2.5% at
baseline and 2.3% during follow-up. Cholesterol determinations at follow-up were performed
on serum samples stored at -20'C for up to 4 years. Repeated measurements performed by our
laboratory in frozen serum showed no significant changes up to 4 years after sampling
compared to frozen samples measured within one week after venipuncture. The standard
deviation of these duplicate measurements did not exceed 3.0% in all instances and did not
show a significant drift.
High density lipoprotein-cholesterol measurements were started in 1979 and low density
lipoprotein-cholesterol measurements in 1984. High density and low density lipoprotein
cholesterol were measured by the same method after precipitation. For high density
lipoprotein-cholesterol the phosphotungstate method according to Burstein (14), with a minor
modification as described by Grove (15) was used. For low density lipoprotein-cholesterol
precipitation was carried out with polyvinylsulphate (Boehringer Mannheim, FRG). All
measurements were carried out in the laboratory of the Department of Epidemiology &
Biostatistics (Erasmus University Medical School), which participates since 1978 in the lipid
standardization program of the WHO Regional Lipid Reference Centre in Prague (Dr. D.
Grafnetler) and from 1979 in the Dutch National Cholesterol standardization program (KCA
foundation), initiated in analogy to the program of the CDC Lipid Standardization Laboratory
in Atlanta. In addition, during the baseline period quality control was indirectly checked on
the CDC protocol by monthly comparison with cholesterol determination using the Abell
Kendall method (Gaubius Institute TNO, Leiden). Both accuracy and precision of total and
high density lipoprotein-cholesterol measurements were within acceptable limits (CDCfWHO)
over the whole period. All automated analyses were initially carried out on a Technicon Auto
-58-

Chapter 4
Analyzer-II system (Technicon Instruments, Tarrytown, USA) and from 1989 on a Kone
Specific Analyzer (Kone Instruments, Espoo, Finland) using frozen (-20'C) serum samples.
From 1987 high density lipoproteiu2 and high density lipoprotein3-cholesterol subfractions
in serum were assayed as described by Gidez et al. (16) with slight modifications. High
density lipoprotein2 and high density lipoprotein3-cholesterol subfractions were separated
using stepwize precipitation of apolipoprotein B containing lipoproteins with heparinJMn" in
two steps and high density lipoproteiu2 with dextran-sulphate.
Data analysis
The data analysis aimed to assess parental total cholesterol level as a determinant of
offspring lipid level, and change in offspring lipid level over time. Mean values and standard
deviations of baseline characteristics of parents and offspring were calculated. Tertile cut off
values of the age-adjusted serum total cholesterol distributions were obtained for fathers and
mothers separately. Baseline characteristics of sons and daughters were calculated according
to both paternal and maternal tertiles of total cholesterol. In the offspring mean individual
cholesterol and lipoprotein levels in 5 year age intervals were obtained by averaging for each
subject all yearly measurements witllin that category. Thus, values from individual subjects
could contribute to different age categories. Subsequently, mean total cholesterol and
lipoprotein values were calculated according to tertiles of parental total cholesterol level.
Offspring cholesterol levels were analyzed according to total cholesterol levels in fathers and
mothers separately as well the combination of their total cholesterol levels, where both the
father and the mother were in the same gender-specific tertile of their respective total senun
cholesterol distributions. For testing group differences the lowest parental tertile values are
taken as a reference category.
Individual lipid level change with age was determined by calculating slopes of regression
lines through total cholesterol and lipoprotein values in each of the above mentioned 5 year
intervals. Again, subjects could contribute to values calculated for different age-categories.
Differences in change of offspring lipid levels between parental tertiles were tested using
Student's t-test with values in the lowest parental tertile as reference category. Group
comparisons of changes in offspring lipid levels were weighed for the individual number of
lipid measurements within age-categories.
-59-

Chapter 4
Results
Table 4. J shows antropometric characteristics, systolic and diastolic blood pressure and
serum total cholesterol levels of fathers (n=l25) and mothers (n=454). Mean levels are also
given by tertiles of parental total cholesterol levels. The cutoff-points of parental total
cholesterol corresponding to the tertiles were 5.4 nunolll and 6.2 nnuoUI in fathers and 5.2
nUnol/l and 6.0 mmol/l in mothers. In both fathers and mothers, Quetelet-index, and systolic
and diastolic blood pressure were higher in those with higher total cholesterol levels. During
follow-up, familial hypercholesterolemia was diagnosed in one mother and both her sons
taking part in the present investigation. One of the sons started taking symvastatine in 1990
and his later follow-up data were excluded from the analysis.
Baseline characteristics of sons and daughters are shown in table 4.2, according to paternal
tertiles of total cholesterol. Table 4.3 shows the same characteristics by maternal tertiles of
total cholesterol. None of the differences between parental tertiles in table 4.2 and table 4.3
was statistically significant.
In table 4.4 total cholesterol and low density lipoprotein-cholesterol levels in offspring are
shown by parental tertiles of serum total cholesterol levels. Thus, total cholesterol levels in
offspring are given according to level in the father, irrespective of the total cholesterol level
in the mother and vice versa. Total cholesterol and low density lipoprotein-cholesterol levels
in children were strongly related to total cholesterol levels in their parents. For total
cholesterol levels statistically significant differences were present between the highest and the
lowest tertile. The differences persisted in the same direction in all age-categories but the last,
while values in the medium tertile were consistently intermediate between values according
to the lowest and the highest tertile. Differences between offspring total cholesterol levels by
parental tertiles were fairly constant with increasing offspring age. In all tertiles the lowest
offspring cholesterol levels were found in the age groups of 10 - 14 years and 15 - 19 years,
suggesting a dip in cholesterol levels around puberty. Data according to paternal and maternal
tertiles of total cholesterol are essentially similar, although the differences between mean
offspring cholesterol levels by maternal tertiles seemed slightly larger than differences by
paternal tertiles, amounting to more than 0.5 nnuoUI between the highest and lowest tertiles.
The differences between tertiles were already present for the youngest age category and
persisted into adult age-categories. Statistically significant differences in low density
lipoprotein-cholesterol levels were found between the highest and lowest paternal tertile in the
age categories from 15 to 29 years. Numbers on low density lipoprotein cholesterol
measurements in the younger age categories (5 - 9 and 10 - 14 yrs) were too
-60-

'" -,
Table 4.1. CbaracteriStics of fathers and mothers, who took part in the study (1975 - 1981): overall and by age-adjusted tertiles of total cholesterol.
Fathers Mothers
Overall Tertiles total cholesterol Overall Tertiles total cholesterol
Low Medimn High Low Medium High
Number of participants 425 142 141 142 454 150 152 152
Age (yrs) 443 ± 79 44.6 ± 82 44.0 ± 7.7 44.4 ± 72. 415 ± 75 40.6 ± 69 42.1 ± 79 41.8 ± 7.6
Height (em) 176.1 ± 7.0 176.8 ± 7.0 176.1 ± 7.1 1752 ± 6.8 1645 ± 6.1 1645 ± 6.0 164.4 ± 62 164.6 ± 6.1
Weight (kg) 76.4 ± 102 749 ± 10.4 763 ± 10.8 77.9 ± 93 65.6 ± 102 62.8 ± 82 65.7 ± 10.5 682 ± 10.9
Quetelet-index (kgfm'l 24.6 ± 2.8 24.0 ± 3.1 24.5 ± 2.7 25.4 ± 2.5 242± 35 232 ± 2.9 24.3 ± 3.6 252 ± 3.7
Systolic blood pressure 128.2 ± 153 1252 ± 14.4 1282 ± 15.5 131.4 ± 15.3 1252 ± 16.7 120.5 ± 15.6 126.4 ± 16.6 128.8 ± 16.7 (mmHg)
Diastolic blood pressure 792 ± 11.1 77.6 ± 10.4 78.8 ± 11.1 81.3 ± 11.4 792 ± 12.0 75.5 ± 9.8 803 ± 12.2 81.7 ± 12.8 (mmHg)
Total cholesterol 5.9 ± 1.14 4.8 ± 0.5 5.8 ± 02 7.1 ± 0.9 5.7 ± 1.37 4.6 ± 0.5 5.6 ± 02 6.9 ± 1.6 (mmol/l)
range range range range range range 3.4 - 5.4 5.4 - 62 62 - 10.0 2.5 - 52 52 - 6.0 6.0 - 24.1
Values are mean ± SD.
Q -5 ~ ...

Table 4.2. Baseline characteristics of SODS and daughters by tertiles of age-adjusted serum total cholesterol of fathers.
Sons Daughters
Tertiles total cholesterol fathers Tertiles total cholesterol fathers
Low Medium High Low Medium High
Number of participants 68 75 80 74 66 62
Age (yrs) 13.6 ± 0.46 13.1 .:!: 0.49 12.9 ± 0.50 12.5 ± 0.44 13.1 ± 0.50 13.0 ± 0.56
'" Height (em) 159.7 ± 233 156.5 ± 2.73 156.5 ± 2.63 151.2 ± 1.93 152.0 ± 2.26 150.2 ± 2.18 ~
Weight (kg) 47.3 ± 195 45.7 ± 2.08 459 ± 2.17 43.4 ± 1.50 43.6 ± 1.88 43.1 ± 1.87
Quetelet-index (kglm') 17.8 ± 0.29 17.5 ± 0.28 17.8 ± 034 17.9 ± 030 18.0 ± 038 18.2 ± 038
SystOlic blood pressure (mmHg) 103.9 ± 1.45 1033 ± 1.50 103.4 ± 1.57 98.5 ± 1.06 97.8 ± 1.28 97.8 ± 138
Diastolic blood pressure (mmHg) 58.0 ± 096 55.4 ± 098 57.0 ± 092 563 ±092 55.6 ± 0.81 56.0 ± 1.07
Ever smoked (%) 22.4 26.4 23.8 24.8 223 20.3
Current smoking (%) 16.7 20.0 20.5 21.2 20.1 21.2
Use of oral contraceptives (%) 273 23.7 20.1
Values are mean ± SEM.
Q .§ ~ ...

Table 4.3. Baseline characteristics of sons and daughters by tertiles of age-adjusted serum total cholesterol of mothers.
Sons Daughters
Tertiles total cholesterol mothers TertiIes total cholesterol mothers
Low Medium High Low Medium High
Number of participants 81 68 84 69 84 68
Age (yrs) 132 ± 0.48 132 ± 0.52 132 ± 0.46 122 ± 0.48 132 ± 0.45 12.7 ± 0.50
'" Height (em) 158.2 ± 237 1572 ± 2.59 156.5 ± 2.61 149.5 ± 1.99 153.5 ± 2.01 1503 ± 2.13 'f
Weight (kg) 46.7 ± 1.91 463 ± 2.19 46.9 ± 2.05 40.7 ± 1.65 44.6 ± 1.64 42.9 ± 1.74
Quete1et-index (kglm'l 17.7 ± 0.29 17.8 ± 034 18.0 ± 028 17.4 ± 032 18.1 ± 0.34 182 ± 036
Systolic blood pressure (mmHg) 103.9 ± 1.43 104.6 ± 1.61 104.1 ± 1.40 98.5 ± 1.16 97.5 ± 1.13 98.6 ± 121
Diastolic blood pressure (mmHg) 56.6 ± 1.01 57.4 ± 1.02 56.9 ± 0.82 54.7 ± 0.92 563 ± 0.83 55.9 ± 0.94
Ever smoked (%) 20.6 21.0 24.0 24.0 23.1 21.7
Current smoking (%) 19.6 192 18.7 212 21.7 212
Use of oral contraceptives r/o) 24.5 25.5 20.8
Values are mean ± SEM
Q ~ ~ ....

Table 4.4. Total cholesterol and LDL cholesterol in offspring by tertiles of total cholesterol in fathers and in mothers.
Tertiles of total cholesterol in fathers Tertiles of total cholesterol in mothers
A$e Low Medium High Low Medium High
5-9 4.6 ± 0.06 4.6 ± 0.1 5.0 ± 0.09 • 4.6 ± 0.06 4.8 ± 0.10 4.9 ± 0.09 ..
10 - 14 4.5 ± 0.07 4.7 ± 0.07 * 4.8 ± 0.Q7 t 4.6 ± 0.08 4.7 ± 0.06 .. 4.9 ± O.Q71O
Total cholesterol 15 - 19 4.5 ± 0.Q7 4.7 ± 0.06 * 4.8 ± 0.06 t 4.4 ± 0.06 4.6 ± 0.05 * 4.9 ± O.Q71O
'" (mmol/l) 20 - 24 4.9 ± 0.08 5.0 ± 0.Q7 52 ± 0.07 t 4.8 ± 0.06 5.0 ± 0.06 t 53 ±0.081O f'-
25 - 29 5.1 ± 0.09 5.4 ± 0.09 * 5.5 ± 0.09 t 5.0 ± 0.Q7 5.4 ± 0.09 t 5.6 ± 0.10 •
30 - 37 52 ± 0.17 53 ± 0.11 5.6 ± 0.14 5.1 ± 0.14 55 ± 0.14 * 5.6 ± 0.16 ..
15 - 19 2.7 ± 0.12 3.0 ± 0.15 3.0 ± 0.10 * 2.8 ± 0.12 2.9 ± 0.09 3.1 ± 0.14 * LDL cholesterol 20 - 24 3.0 ± 0.09 33 ± 0.11 * 3.4 ± 0.09 t 2.9 ± 0.08 32 ± 0.08" 3.6 ± 0.11 1:
(mmol/l) 25 - 29 32 ± 0.11 3.5 ± 0.10 3.7 ± 0.10 t 3.1 ± 0.09 35 ± 0.10 * 3.7 ± 0.11 1: 30 - 37 3.4 ± 0.18 3.4 ± 0.11 3.4 ± 0.16 33 ± 0.14 3.6 ± 0.15 3.7 ± 0.16 •
Values are mean ± SEM. LDL = low density lipoprotein; * = p<o.05, t = p<o.OI. ::: = p<O.OOl, reference category: lowest parental tertile.
9 {j il ..

Chapter 4
small to allow a meaningful analysis. The direction and magnitude of the differences found
for low density lipoprotein-cholesterol levels were quite similar to those found in total
cholesterol levels and again differences according to maternal tertiles were higher than
according to paternal tertiles.
High dens;ty lipoprotein-cholesterol, high density lipoprotein2-cholesterol and high density
lipoprotein3-cholesterollevels did not show differences by paternal and maternal tertiles nor
were they detectable with increasing age, Pooled levels (over age) for males were: high
density lipoprotein-cholesterol 1.2 ± 0.01 mmoUI (mean ± SEM); high density lipoprotein2-
cholesterol 0.26 ± 0.010 mmoUI and high density lipoprotein3-cholesterol 0.90 ± 0.008
IllIllOUI. Pooled values (over age) for females were 1.4 ± 0.02 ImnoUI; 0.44 ± 0.014 lllIlloUI
and 0.98 ± 0.011 lllIlloUI respectively.
Daughters
t
t
, -5-9 10-14 15-19 20-24 30_ 37
Age (years)
Cholestnol mothers o lo~- 121 Mod",,,, III Hi.h
Sons
5,5
5-9 10-14 15-19 20-24 25-29 30-37
Age (years)
CI\Ol~sterol mothers o Low El Med,"", II High
5,5 -
S 5 o
~ 4.5
"
6
Daughters
t
5-9 10·14 15-19 20·24 25·29 30-37 Age (years)
Choluterol rathers o [-01'0- IZ1 M,dJum II IUgh
Sons
" ~'I"'-~'1"'~ 5·9 10-14 15-19 20·24 25·29 30-}7
Age (years)
Cholesterol fathers o low II] Medium III Hi~h
Figure 4,1. Total cholesterol in daughters and sons by tertiles of total cholesterol in mothers and fathers.
'" = p<O,05, t = p<Q,Ol, t = p<O,QOI, with lowest tertile as reference category,
-65-

Chapter 4
Figure 4.1 shows total cholesterol levels separately in daughters and sons by paternal and
maternal tertiles of total cholesterol. There were no major differences between the gender
specific data and the overall analyses. However, in sons the data were suggestive of u steeper
rise in total cholesterol levels after age 15 in both paternal and maternal tertiles.
In figure 4.2 serum total cholesterol levels in offspring are shown according to tertiles of
total cholesterol in the fathers (upper left), the mothers (upper right), and both
Total ehole5terolln of tip ring by lertile5 of tolal chotesltrol (alhers (3~llmavin8IWngtl)
, t .... ~.- -~ .. ~ ... : .. :
............. " " .. :: .. ' .......
- I'lthellnh1sh~lurti!e - - - Father In m~.jiom Utblt
F'~llnkwtJllutile
"*IO~~~'1S~~~'''~~~-,''~~~-,lO Ag~(yean)
Total cholesterol in offspring by lertilt.!l of tolal cholesterol parents (1 YUI mavinglVtllgU)
---'-r----t --,
.... _--" ................... ... ~ ...
- Bo-thpmntllnblghtolkrlile - - - Bothpmnll!<lm«llutllUrtiIc -- Bothpll.!IIll.!!t~llcrtile
"+IO'-"'-IT,.-~.-,,~~~~,,~~~~lO Age (rl:m)
Total cholesterol In offspring by tertiles of total cholesterol mothers (lyur mMg Ivuagtl)
- Mothtf In hl$.he.llertile - - - MOIhu In oxdlUlIl tertile
Mother In t<:rwe&lutb1e "+,~.-TO~~~.-"~~~~~~
ro " ~ ~ W Age (yean)
Figure 4.2. Serum total cholesterol levels in offspring according to tertlles oftolal cholesterol levels in fathers (upper left), mothers (upper right), and both parents (lower).
fathers and mothers (lower panel). When offspring was analyzed that had both fathers and
mothers in the same gender specific tertile the offspring differences between parental tertiles
increased to almost I mmoUI between the lowest and highest tertile. Again, total cholesterol
levels dipped between 15 and 20 years of age, most clearly for the lowest two tertiles and
showed a gradual increase thereafter.
..66 ..

Offspring - fathers
10· 14 15· 19 20·24 25·29 Age (years)
Offspring - mothers 1,5
I ~
I ~O § ·0,5
o .1.'--,----~---~--___r--
10 - 14 15-19 20-24 25 - 29 Age (years)
Chapter 4
Offspring of fathers in: o Lowtertile III Medium tertile II High tertile
Offspring of mothers in:
o Low teetHe
III Medium tertile II High tertile
Figure 4.3. Change of tolal cholesterol level in offspring by tertiles of palemal (upper panel) and matemal
(lower panel) tolal cholesterol. Bars represent mean 5-year change.
Figure 4,3 show., the age-specific change in total cholesterol in offspring by paternal tertiles
(upper panel) and maternal (lower panel) tertiles of total cholesteroL It shows that in each
-67-

Chapter 4
tertile there is a decrease of total cholesterol levels up to age 15 and a rise in total cholesterol
levels from age 15 to 25. None of the differences in change between parental tertiles was
statistically significant.
Before 1991, there were 131 offspring who terminated their participation in the study.
Separate analyses were performed to evaluate if this group of offspring was differentially
distributed over parental groups. In the fathers there were 44 offspring from the low group
who terminated participation, 35 offspring from the medinm group and 33 from the high
group. These offspring groups showed differences in total cholesterol levels by parental
tertiles for the 5 year age groups which were similar to those found for still participating
subjects. In the age category 15 - 19 years the low paternal group (n=41) had mean total
cholesterol levels of 4.4 ± 0.11 mmoUI, the medium group (n~26): 4.6 ± 0.12 mmoUI, and
the high group (n~26): 4.9 ± 0.15 mmoUI. Similar differences were found when analyzed
according to maternal level.
Discussion
In the present study, we have found a strong positive relation between parental levels of
serum total cholesterol and levels of serum total cholesterol and low density lipoprotein
cholesterol levels in their offspring. Offspring group differences in total cholesterol and low
density lipoprotein-cholesterol were present from childhood and persisted into young
adulthood, while throughout this period these group differences remained rather constant. No
associations between parental total cholesterol levels and offspring high density lipoprotein
cholesterol and its subfractions were found. The association between maternal total cholesterol
levels and offspring total and low density lipoprotein-cholesterol levels appeared slightly more
pronounced than for paternal total cholesterol levels. The largest effects were observed when
cholesterol levels of both parents were taken into account. The association for daughters and
sons did not differ materially.
Before we can interpret these findings some methodological aspects of the study have to be
discussed. The present analyses are based on data obtained in a random sample of youngsters
initially examined in a population survey and subsequently invited for longitudinal follow-up.
It is felt that response rates were high enough to consider this sample representative of the
source population. Loss-to-follow-up would have biased our results if offspring loss-to
follow-up would be differentially (with regard to offspring groups) associated with risk factor
levels. However, there was no evidence from the data for such differentialloss-to-follow-up.
-68-

Chapter 4
During the whole follow-up period laboratory measurements quality was controlled by the
CDCfWHO (total cholesterol and high density lipoprotein-cholesterol) and by KCA (for total
cholesterol measurements) and no drift of measurements over time was observed.
Coronary heart disease tends to aggregate in families (17-19). In two recent prospective
studies it was shown that a parental history of myocardial infarction is an independent risk
factor for coronary artery disease (20,21). A number of cross-sectional studies has shown that
the offspring of patients with cardiovascular disease have less favorable (apo)lipoprotein
profiles as compared to offspring of non-patients (22-25). This familial aggregation of
coronary heart disease may reflect shared genetic factors, shared environmental factors, or both. Coronary heart disease risk factors themselves have also been shown to aggregate within
families (7,26,27). The cross-sectional relation between total cholesterol levels in parents and
offspring total cholesterol and lipoprotein-cholesterol levels throughout childhood and young
adulthood has been reported earlier (28), including in the present cohort (29). Tracking of
lipids at a young age has been demonstrated in a number of studies in general populations of
children and young adults (1-5). In the present study the parent-offspring relation with regard
to cholesterol and lipoprotein-cholesterol levels is further shown to persist longitudinally. This
indicates that the influence of parental cholester levels on cholesterol levels in their offspring
is apparent particularly at a young age and much less thereafter. In general, the origins of
parent-offspring similarity may be genetic, acquired or both. Genetic explanations for familial
similarity among relatives of adverse lipid levels are the genetic dyslipoproteinemias, of which
the autosomal dominant disorders familial hypercholesterolemia, leading to impaired low
density lipoprotein-receptor function and familial combined hyperlipidemia are the most
frequent. Familial hypercholesterolemia was confirmed in one family taking part in the present
study. The finding that there were no significant differences in change with increasing age of
total cholesterol and low density lipoprotein-cholesterol levels between the groups of offspring
suggests that parental cholesterol level, although strongly related to offspring level, is not a
major determinant of change in offspring levels. TillS means that offspring group differences
in total cholesterol and low density lipoprotein-cholesterol by parental levels of total
cholesterol are not only found in cross-sectional analyses but also longitudinally. Thus, on an
individual level, children of high risk parents have on average higher levels of the studied risk
factors than children of low risk parents irrespectivem of their age. The phenomenon of
familial aggregation of cardiovascular risk factors may underlie aggregation of coronary heart
disease and it may further provide a tool for its prevention at an early age.
In conclusion, our longitudinal data show a strong positive association between parental cholesterol levels and the levels of total and low density lipoprotein-cholesterol levels in their
-69-

Chapter 4
offspring.
References
Webber LS, Srinivasan SR, Wattigney WA, Berenson OS. Tracking of serum lipids and
lipoproteins from childhood to adulthood: The Bogalusa Heart Study. Am J Epidemiol
1991; 133:884-99.
2 Lauer RM, Lee J, Clarke WR. Predicting adult cholesterol levels from measurements in childhood
and adolescence: The Muscatine Study. Bull N Y Acad Med 1989;65:1127-42.
3 Porkka KVK, Viikari JSA, Akerblolll HK. Tracking of serum HDL-cholesterol and other lipids
in children and adolescents: The Cardiovascular Risk in Young Finns Study. Prev Med
1991;20:713-24.
4 Vobecky JS, David P, Vobecky J. Dietary habits in relation to tracking of cholesterol level in
young adolescents: a nine-year follow-up. Ann Nutr Metab 1988;32:312-23.
5 Stuhldreher WL, Orchard TJ, Donahue RP, Kuller LH, Gloninger MF, Drash AL. Cholesterol
screening in childhood: sixteen~year Beaver County Lipid Study experience. J Pediatr
1991;119:551-6.
6 Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Linag KY, Levine OM. Serum cholesterol in
young men and subsequent cardiovascular disease. N Engl J Med 1993;328:313-8.
7 Morrison JA, Narnboodiri K, Green P, Martin J, Glueck CJ. Familial aggregation of lipids and
lipoproteins and early identification of dyslipoproteinemia. The Collaborative Lipid Research
Clinics Family Study. JAMA 1983;250:1860-8.
8 National Cholesterol Education Program: Report of the Expert Panel on Blood Cholesterol Levels
in Children and Adolescents. April 1991. Pediatrics 1992;89(suppl.):525-84.
9 Hofman A, Klein F, Valkenburg HA. Natural history of sentm cholesterol in childhood. Artery
1980;8:157-63.
10 Hofman A, Van Laar A, Klein F, Valkenburg HA. Coffee and cholesterol. New Engl J Med
1983;309: 1248-9.
11 Valkenburg HA, Hofman A, Klein F, Gro~stra FN. Een epidemiologisch onderzoek naaT risico~
indicatoren voor hart- en vaatziekten (EPOZ).I. Bloeddruk, serumcholesterolgehalte, Queteletindex
en rookgewoontell in een open bevolking van 5 jaar en ouder. Ned T Geneesk 1980;124: 183-9.
12 Hofman A, Valkenburg HA. Determinants of change in blood pressure during childhood, Am. J
Epidemiol 1983;117:735-43.
13 Van Gent CM, Van def Voort HA, de Bruijn AM, Klein F. Cholesterol determinations. A
comparative study of methods with special reference to enzymatic procedures. Clin Chirn Acta
1977;75:243-51.
-70-

Chapter 4
14 Burstein M, Scholnick HR, Morfin R. Rapid method for the isolation of lipoproteins from human
sefilm by precipitation with polyanions. J Lipid Res 1970;11:583-95.
15 Grove TH. Effect of reagent Ph 011 determination of high~density lipoprotein cholesterol by precipitation with sodium phosphotungstate-magnesium. Clin Chim Acta 1979;25:560~4.
16 Gidez LI, Miller GJ, Burstein M, Slagle S, Eder HA. Separation and quantitation of subclasses
of human plasma high·density lipoproteins by a simple precipitation procedure, J Lipid Res
1982;23: 1206-23.
17 RissanenAM. Familial aggregation of coronary heart disease in a high density area (North Karelia,
Finland). Br Heart J 1979;42:294-303.
18 Friedlander Y, Kark JD, Stein Y. Family history as an independent risk factor for coronary heart
disease. Br Heart J 1985;53:382-7.
19 Barrett~eonnor E, Khaw K-T. Fanlily history of heart attack as an independent predictor of death
due to cardiovascular disease. Circulation 1984;69:1065-9.
20 Colditz GA, Rimm EB, Giovannucci E, Stampfer MJ, Rosner B, Willett we. A prospective study
of parental history of myocardial infarction and coronary artery disease in men. Am J Cardiol
1991 ;67:933-8.
21 Myers RH, Kiely DK, Cupples LA, Kannel WB. Parental history is an independent risk factor for
coronary artery disease: The Framingham Study. Am Heart J 1990;120:963-9
22 Freedman DS, Srinivasan SR, Shear CL, Franklin FA, Webber LS, Berenson GS. The relation of
apolipoproteins A-I and B in children to parental myocardial infarction. N Engl J Med
1986;315:721-6.
23 De Backer 0, Hulstaert F, De Munck K, Rosseneu M, Van Parijs L, Dramaix M. Serum lipids and
apoproteins in students whose parents suffered prematurely from a myocardial infarction. Am
Heart J 1986;112:478-84.
24 Van Stiphout WAHJ, Hofman A, Kruijssen HAeM, Vernleeren R, Groot PHE. Is the ratio apo
B/apo A-I an early predictor of coronary atherosclerosis? Atherosclerosis 1986;62: 179-82.
25 Burke GL, Savage PJ, Sprafka JM, Selby N, Jacobs Jr DR, Perkins LL, Roseman JM, Hughes
GH, Fabsitz RR. Relation of risk factor levels in young adulthood to parental history of disease.
The CARDIA Study. Circulation 1991;84:1176-87.
26 Criqui MH, Barrett-Connor E, Holdbrook MJ, Austin M, Turner JD. Clustering of cardiovascular
disease risk factors. Prev Med 1980;9:525-33.
27 Friedlander Y, Bucher KD, Namboodiri KK, Heiss G, Kark JD, Tyroler HA, Eisenberg S, Stein
Y, Rifkind BM. Parent-offspring aggregation of plasma lipids in selected populations in North
America and Israel. The Lipid Research Clinics Prevalence Study. Am J Epidemiol 1987; 126:268-79.
28 Greenberg RA, Green PP, Roggenkamp K.J, Barrett-CoMor E, Tyroler HA, Heiss O. The
constancy of parent-offspring similarity of total cholesterol throughout childhood and early adult
life. The Lipid Research Clinics Program prevalence study. J Chron Dis 1984;37:833-8.
-71-

Chapter 4
29 Stiphout Van WAHl, Hofrnan A, Bruijn De AM, Valkenburg HA. Distributions and detenninants
of total and high-density lipoprotein cholesterol in Dutch children and young adults. Prey Med
1985; 14: 169-80.
-72-

CHAPTER 5
GENERAL DISCUSSION I

5. General discussion I
Introduction
In the studies described in this thesis the focus is on etiology; lipids and lipoproteins as
putative causal risk factors of atherosclerosis. Conunon to the definitions of causality in
medical science is the notion that exposures antecede health outcomes. As atherosclerosis is a life-long process, a point of departure in the study of causality is to ensure that factors of
interest do indeed antecede atherosclerosis. What are the suitable options in study design that
meet this requirement? Let us examine the example of postprandial lipid metabolism and
coronary artery disease. One option would be to measure postprandial lipids in a group of
children and young adults and follow these subjects until manifest coronary artery disease
occurs in some of them. This cohort design, although valid in itself, would obviously require
a very long study period and large numbers of subjects and thus is rather impractical. Still,
such a study has been performed for the classical cardiovascular risk factor serum total
cholesterol in yOlmg men who were followed for 27 to 42 years (I).
Alternatively, a study may be considered in which postprandial lipid metabolism is
examined in groups of diseased and non-diseased subjects. In general, such a study carmot
exclude the possibility that the process of atherosclerosis itself influenced postprandial lipid
metabolism or that atherosclerotic events and symptoms change behavior, which in turn may
influence postprandial lipid metabolism. There is one exception for which this design could
be used and the time-sequence criterion could unequivocally be met. If, hypothetically, an
unfavorable postprandial lipid metabolism was known to be completely genetically determined
and would express at a young age, studying postprandial lipids in patients with coronary artery
disease would lead to valid results, in the sense that the exposure, unfavorable postprandial
lipid metabolism, precedes the outcome, coronary atherosclerosis, in time. However, as the
genetic contribution and mechanistic pathways to postprandial lipids is not fully understood,
such a study design will not inherently meet the time-sequence criterion.
A valid and efficient alternative is provided by the patient-offspring study as described in
chapters 1 and 2 of this thesis. In the patient-offspring study, risk factors are measured in
offspring of patients with the disease and compared with risk factors measured in offspring
of parents who do not have the disease. Tlus design allows to study the relation between a
risk factor and disease, such as coronary atherosclerosis, where the risk factor is measured in the offspring who have not yet developed coronary atherosclerosis. In the next sections the
essential characteristics of this design are discussed.
-74-

Chapter 5
The patient-offspring study
Design
In general, a study in parents and their offspring may be used to assess the relation between:
1. a risk factor (R) in offspring and the same factor in parents (R-R), or
2. an outcome (D) in offspring and the same outcome in parents (D-D), or
3. a risk factor in offspring and disease in parents: the patient-offspring study
The underlying assumptions in these three types of study are familial aggregation of risk
factors (R-R), of disease (D-D), or both. In the first type of study the assumption is similarity
of risk factor levels in parents and their offspring, in other words familial aggregation of risk
factor levels (R-R). In the second type of study it is expected to find more disease among
offspring if in their parents the disease has occurred, in other words familiar aggregation of
. disease (D-D).
The third type of study will be referred to as the patient-offspring study. In the patient
offspring study the goal is to study risk factors for a disease before the occurrence of the
disease. The study design as described in chapters 1 and 2 of this thesis is depicted in figure
5.1. In these studies, a group of fathers with coronary artery disease and a reference group of
fathers without coronary artery disease was selected, irrespective of the disease status in the
mothers. Levels of putative risk factors were compared between the sons of both groups of
fathers.
Premises
1. Familial aggregation of risk factors
One point of departure in a patient-offspring study is the assumption of familial aggregation
of disease (D-D aggregation). In this paragraph we will examine how this relates to causes
for disease in patients and offspring.
In a multifactorial disease such as coronary artery disease we may distinguish familial risk
factors and non-familial risk factors. The familial risk factors may be genetic factors or
acquired factors that aggregate in families (R-R aggregation). Non-familial risk factors for
-75-

Chapter 5
coronary artery disease are not transmitted from one generation to another. The disease is
Fathers Mothers Fathers Mothers
CAD + CAD-
I I I I I I
Offspring Offspring
R R
Figure 5.1. The patient-offspring study: a risk factor is studied in offspring of parents with and without coronary artery disease (CAD).
caused by: a set of familial risk factors; or a set of non-familial risk factors; or combinations
of familial and non-familial risk factors. Every patient with coronary artery disease has at least
one of these three combinations of risk factors.
In an unselected group of patients with coronary artery disease, some patients will have
familial and non-familial risk factors, other patients will have familial risk factors only and
yet other patients will only have non-familial risk factors. Suppose that we now follow a
group of healthy offspring of patients with coronary artery disease from the present into the
future and select those who developed coronary artery disease. These offspring will not
necessa'ily have the same distribution of causes for coronary artery disease as the total group
of diseased parents. In these offspring we will particularly find familial risk factors, perhaps
in combination with non-familial risk factors. In some of the offspring with coronary artery
disease we will find sets of non-familial risk factors only. A smaller proportion of the
offspring of controls, as compared to offspring of cases, will also develop coronary artery
disease in the future. However, because they have healthy parents, familial risk factors,
-76-

Chapter 5
exclusively or in combination with non-familial risk factors, will be found less frequent in
these diseased offspring of controls than in the diseased offspring of patients. In the diseased
offspring of controls a much larger proportion of disease will be due to sets of non-familial
risk factors. If the familial and non-familial risk factors are not correlated, the percentage of
the nnselecte~ offspring of controls with non-familial risk factors only will be similar to the
percentage of the unselected offspring of cases with non-familial risk factors only. Therefore,
in offspring of patients we will find the familial risk factors to be different from those in
offspring of controls. The non-familial risk factors may be found in both groups of offspring,
but none of these will be differently distributed in offspring of cases compared with controls.
TillS example shows that the patient-offspring study can only detect differences between
offspring groups in risk factors that are familial and not in risk factors that are non-familial.
Familial aggregation of the disease thus is not sufficient as a basis for the patient-offspring
study, the premise is familial aggregation of risk factors.
2. Tracking by parental risk
Given that a risk factor is fanlilial, the patient-offspring study aims to detect differences in
risk factor levels between offspring of patients and offspring of controls. It would facilitate
the patient-offspring study if these risk factor differences between offspring groups can be
detected in a large age range of the offspring. This requires that the risk factor levels are
higher in offspring of patients than in offspring of controls over long periods of time. The
group differences may change in magnitude but should remain over time. The examination
of such 'tracking by parental risk' requires a study as described in chapter 4 of this thesis,
which evaluated whether offspring of high risk parents (based on high cholesterol levels) have
high cholesterol levels over time. Risk factors that do not track by parental risk are much
more difficult to detect in a patient-offspring study.
Quant!fication of the effect
In each of the tluee types of study relating characteristics in parents to characteristics in
their offspring, the parent to offspring transmission has to be considered. In the patient
offspring study, given that the disease is multifactorial, the risk factor under studY'will
probably explain only part, if any, of the occurrence of the disease. The subgroup of parents
with the risk factor will transmit it to a proportion but not to all of their offspring. In the
-77-

Chapter 5
hypothetical situation of a purely Mendelian inheritance of a risk factor the expected
proportion of offspring with the risk factor can be calculated and is it possible to infer the
strength of the Ime risk factor-disease association (2). Also, if the risk factor were completely
acquired it seems unlikely that an environment that has led to high levels of the risk factor
in the parents will in all instances lead to similarly high levels in their offspring.
Consequently, if in the patient-offspring study a relation is found between a risk factor in
offspring and parental disease it will probably always underestimate the strenght of the
OCcurrence relation that one would find in the patients themselves. In other words, the relation
between offspring risk factor levels and parental disease is likely to reflect a dilution or
smaller derivative of the real occurrence relation.
The extent to which a risk factor aggregates in families (R-R) is an indicator of the
underestimation of the occurrence relation. Familial aggregation of disease (D-D) may be
predominantly explained by other familial risk factors than the one under study. Thus, familial
aggregation of the risk factor is more indicative of the magnitude of underestimation than
familial aggregation of disease.
Inference
Except for ecological studies, risk factor and disease status in epidemiologic research are
assessed in the sarne individuals. In the patient-offspring study, however, risk factors and
disease are measured in different individuals; offspring and parents. In this type of study it
is not immediately apparent what the conceptual unit of observation is. In most studies the
increased risk for disease in offspring is taken as the starting point in lipid research (3-7) and,
for instance, hypertension research (see for review 8). Thus, many investigators set out to
relate offspring risk factor levels to increased offspring disease risk. Here, the offspring are
taken as the conceptual units of observation and parental disease is taken as a proxy for
disease in the offspring. This will be referred to as the offspring-perspective. This perspective
is graphically depicted for atherosclerosis in figure 5.2. It shows the hypothetical situation
where there is familial aggregation of atherosclerosis. In the patient-offspring study parents
are selected according to their presence of coronary atherosclerosis and risk factors are
measured in their offspring at some point in time (To). In the cases (upper panel), parents have
high degrees of atherosclerosis. In the controls (lower panel), parents have low degrees of
atherosclerosis. Based on D-D type aggregation, a proportion of the offspring of cases (upper
panel) will at some point in their future develop atherosclerosis. Most of the control offspring
-78-

Chapter 5
(lower panel) will maintain low degrees of atherosclerosis. Suppose that in the offspring
perspective familial as well as nOll-familial risk factors are examined in relation to the proxy
of disease. As shown earlier non-familial risk factors will not be different between offspring
Degree of atherosclerosis based on familial di5casc risk
t
Degree of atherosclerosis based on familial disease risk
t
T,
DO P 0
T,
CAsr,s
Prospective time
---lI>-
CONTROLS
Prospective time
---lI>-
Offspring future
o o
Offspring future
P "" parent
o "" offspring
P = parent
o "" offspring
Figure 5.2. Schematical representation ofthe offspring-perspective to a patient-offspring study. Risk factor levels are indicated by lines within bars.
-79-

Chapter 5
groups even though they may be causally related to the disease.
From the offspring-perspective, however, it is not uncommon that it will be concluded. th~t _
non-familial risk factors are not related to the disease, without considering the alternative
explanation that such risk factors are not familial. An example of such a pitfall is presented
in a landmark report on lipoproteins and apolipoproteins that was published in the New
England Journal of Medicine by Freedman and colleagues (7). In this study on data from the
Bogalusa Heart Study, the authors report on the assessment of lipoprotein-cholesterol levels
and apolipoprotein A-I and B levels in children of fathers who rep0l1ed to have had a
myocardial infarction as compared with children whose fathers did not report such a medical
history. Logistic regression was used to predict on the basis of levels of offspring serum
variables the probability of myocardial infarction in the parents. Because the authors stated
that this study design may provide "relevant information concerning the future risk of
disease", they presumably had the intent to use parental myocardial infarction as a proxy of
offspring disease. No offspring differences were found for lipoprotein-cholesterol fractions.
Adverse levels of apolipoproteins A-I and B were found in offspring of fathers with
myocardial infarctions. It was concluded that apolipoproteins may be more strongly related
to the risk of cardiovascular disease than lipoprotein-cholesterol fractions. However,
apolipoproteins A-I and B could show different levels of familial aggregation than
lipoprotein-cholesterol fractions. Apolipoprotein levels are probably more genetically
determined than lipoprotein-cholesterol levels (9). Differences in familial aggregation between
apolipoproteins and lipoprotein-chOlesterol fractions could provide an alternative explanation.
The question is ifthere is a better approach to the patient-offspring study that will prevent this
type of erroneous inference. We introduce the parent-perspective as a better approach to the patient-offspring study. In
this approach, offspring levels of a risk factor are taken as a proxy for parental levels of this
risk factor when they were of the age of their offspring. Parents are chosen as lmits of
observations, an orientation that we will further refer to as the parent-perspective. The parent
perspective to the patient-offspring study is graphically depicted in figure 5.3. The same
patient-offspring study as depicted in figure 5.2 is performed at To. Now, however, estimates
are made of parental risk factor levels in their past through offspring risk factor levels
measured at To. These estimates are related to parental current disease, with the classical case control study as the paradigm. At To, the cases are parents with high degrees of atherosclerosis
(upper panel). At To, the controls are parents with low levels of atherosclerosis.
Atherosclerosis in both offspring of cases and of controls is still minimal.
From the parent-perspective in the patient-offspring study only familial risk factors will be
-80-

Chapter 5
studied. Non-familial risk factors will not be studied, because they are not a proxy for parental
levels of these risk factors. Information about these non-familial risk factors must be obtained
Degree of atherosclerosis based on familial risk factor
t
Degree of atherosclerosis based on familial risk factor
t
Parents P""
o p
Parents past
CASES
Retrospective time ~
CONTROLS
Retrospective time
~
p:;:;: parent
o = offspring
I,', $
o
T.
P = parent
o :;:;: offspring
DO P 0
Figure 5.3. Schematical representation of the parent-perspective to a patient-offspring study. Risk factor levels are indicated by lines within bars.
-81-

Chapter 5
from other research.
Thus, contrary to the offspring-perspective, the parent-perspective to the patient-offspring
study inherently meets its prior premise, the familial aggregation of the risk factor under
study.
Consideration of familial aggregation of the risk factor is a logical step in the parent
perspective which protects the investigator from the pitfalls of interpretation. Therefore, the
parent-perspective provides a better orientation to the patient-offspring study than the
offspring perspective.
Summary
The time-sequence of risk factors and subsequent disease occurrence is an important criterion for causality. In the patient-offspring study risk factor levels in offspring are related
to disease in their parents and aim to meet the time-sequence criterion. It gives a valid and feasible tool for studying etiological relations between risk factors and a multifactorial disease.
While in the patient-offspring study measurements of risk factors and disease take place at one
point in time it can detect relationships between risk factors and disease that would otherwise
require studies with long follow-up and large numbers of subjects for their assessment.
In tllls chapter we discussed the premises for the patient-offspring study. It was shown that
disease aggregation is not sufficient as a point of departure for the patient-offspring study. A
first premise for the patient-offspring study is that there is familial aggregation of the risk
factor (R-R). If tltis premise of fanlilial aggregation risk factor is not met, the absence of
familial aggregation of a risk factor should be considered as an alternative explanation for a
zero finding. A second premise is that there is 'tracking by parental risk' from young into late
adulthood, which facilitates the possibility for a patient-offspring study to detect offspring
group differences in risk factor levels.
If there is familial aggregation of the risk factor it is not known to what extent risk factors
are transmitted from one generation to the next generation. Therefore, the patient-offspring
study will not provide exact information about the strengths of risk factor - disease
associations. If risk factors differ in familial aggregation, they will differ with respect to the
strenght of association with the disease. This sets limitations to conclusions from the patient
offspring study about which of these risk factors is best suitable for intervention.
The offspring-perspective to the patient-offspring study takes parental disease as a proxy for
offspring future disease. Because the disease-proxy involves a selection of causes, in particular
-82-

Chapter 5
causes involving familial risk factors alone or in combination with non~familial risk factors, this offspring-perspective may lead to wrong inference with respect to non-familial risk
factors. The parent-perspective uses offspring risk factor levels as a proxy for parental risk
factor levels in the past. Because in the parent-perspective it is a logical step to evaluate the
premise of familial aggregation of the risk factor it is considered less vulnerable to erroneous
interpretation of results.
References
Klag MJ, Ford DE, Mead LA, He J, Whelton PK, Liang KY, Levine DM. Serum cholesterol in
young men and subsequent cardiovascular disease. N Engl J Med 1993j328:313~8.
2 Tiret L, Nicaud V, Ehnholm C, Havekes L, Menzel HJ, Ducimetiere P, Cambien F. Inference of the strength of genotype-disease association from studies comparing offspring with and without parental history of disease. Ann Hum Genet 1993j57:141-9.
3 De Backer a, Hulstaert F, De Munck K, Rosseneu M, Van Parijs L, Dramaix M. Serum lipids and apoproteins in students whose parents suffered prematurely from a myocardial infarction. Am
Heartb J 1986;112:478-84.
4 Sveger T, Fex G, Borgfors N. Hyperlipidemia in school children with family histories of
premature coronary heart disease. Acta Paediatr Scand 1987;76:311-5. 5 Durrington PN, Ishola M, HUllt L, Arrol S, Bhatnagar D. ApoJipoproteins (a), AI, and Band
parental history in men with early onset ischaemic heart disease. Lancet 1988;ii:1070-3. 6 Burke OL, Savage PJ, Sprafka JM, Selby N, Jacobs Jr DR, Perkins LL, Roseman JM, Hughes
GH, Fabsitz RR. Relation of risk factor levels in young adulthood to parental history of disease. The CARDIA Study. Circulation 1991;84:1176-87.
7 Freedman DS, Srinivasan SR, Shear CL, Franklin FA, Webber LS, Berenson as. The relation of
apolipoproteins A-I and B in children to parental myocardial infarction. N .Engl J Med 1986;315:721-6.
8 Muldoon MF, Terrell DF, Bunker CH, Manuck SB. Family history studies in hypertension
research. Review of the literature. Am J Hypertens 1993;6:76~88. 9 Ordovas JM, Schaefer EJ, Salem 0, Ward RH, Glueck CJ, Vergani C, Wilson PWF, Karathanasis
SK. Apolipoprotein A-I gene polymorphism associated with premature coronary artery disease and
familial hypoalphalipoproteinemia. N Engt J Med 1986;314:671-7.
-83-


CHAPTER 6
GENERAL DISCUSSION II

6. General discussion II
In general discussion I essential aspects of the patient-offspring study were discussed in
relation to familial aggregation of disease and familial aggregation of risk factors. In this
chapter familial aggregation of cardiovascular disease and its risk factors will be discussed.
Familial aggregation of cardiovascular disease and cardiovascular risk factors
Heart attacks occur more often in certain families, an observation that dates back decades
before the concept of coronary risk factors. Already in the 50's and 60's family history studies
demonstrated that coronary heart disease aggregates in families (1-3), particularly when the
proband had coronary heart disease at a relatively young age (3-5). Where cardiovascular
disease runs in families, the same is true for classical risk factors for cardiovascular disease such as hypertension (6,7), smoking (8), and cholesterol levels as was also shown
longitudinally in chapter 4 of this thesis. Other factors related to coronary artery disease
including diabetes mellitus (9,10), obesity (II) and physical fitness (12) have been reported
to aggregate in families as well. In cardiovascular research a question has been to what extent,
if at all, familial aggregation of coronary heart disease may be attributed to familial
aggregation of the known cardiovascular risk factors. In a number of prospective studies (13-
19), cardiovascular risk profiles were related to the occurrence of cardiovascular disease in
subjects who had family relatives with cardiovascular disease and thus had a positive family
history. Overall, these studies have indicated that familial aggregation of cardiovascular
disease can only partially be attributed to classical cardiovascular risk factors. The question
remains how this may be explained. It may be that members of families in which
cardiovascular disease aggregates have an increased susceptibility to the effects of classical
risk factors. Thus, this increased susceptibility may be an unknown risk factor in itself.
Alternatively, the familial aggregation of cardiovascular disease may be related to other, as
yet unknown, risk factors. Such new risk factors and their relation with fanlilial cardiovascular
disease may be studied with the patient-offspring study. In chapters 2 and 3 the angiographic
patient-offspring study was used to assess relatively unexplored risk factors such as changed
postprandial lipoprotein metabolism and apolipoproteins. Familial aggregation of postprandial
responses to an oral lipid load has, to our knowledge, not been studied. There are, however,
some indications for familial aggregation of an increased triglyceride response to an oral lipid
load in families of probands with coronary heart disease. Familial aggregation of lipids,
cholesterol and its subfractions has been reported in several studies, including determinants
-86-

Chapter 6
of postprandial lipid metabolism such as triglyceride level and high density lipoprotein
cholesterol level (20-25).
Tracking of risk factors
The phenomenon of tracking of a risk factor for a disease concerns the stability of
individual's ranks of the risk factor level within the distribution of this risk factor over time.
In general discussion I it was pointed out that 'tracking by parental risk' is one of the
premises for the patient-offspring study.
A number of longitudinal studies in children and young adults has shown tracking for total
cholesterol and low density lipoprotein cholesterol in childhood and young adulthood, with
weaker levels of tracking for high density lipoprotein cholesterol and triglycerides (26-35).
The apolipoproteins A-I and B were shown to track to a similar extent as high density
lipoprotein cholesterol and low density lipoprotein cholesterol respectively (36). Recently, 3-
. year tracking was shown for high density lipoprotein, and to a lesser extent high density
lipoprotein,-cholesterol (37), high density lipoprotein, being considered a determinant of
postprandial triglyceride metabolism (38). Thus, there is a large body of evidence from
popUlation studies that lipoproteins and apolipoproteins track over time. To our knowledge
there have been no reports actually showing tracking of postprandial lipids and lipoproteins
over time. Repeated measurements of postprandial triglyceride responses suggested some
degree of stability of ranking, although these were performed in small numbers of subjects
and over short time intervals (39,40).
In the study of tracking by parental risk, categories are made of parental risk factor levels
and the ranks of offspring risk factor levels are followed over time according to these parental
categories. Parent-offspring similarity of total cholesterol values throughout childhood and
early adulthood has been shown previously (23,41). The study in chapter 4 on the EPOZ
popUlation describes the yearly follow-up of total cholesterol and lipoprotein-cholesterol levels
in offspring according to tertiles of total cholesterol levels in their parents. It illustrates that
total cholesterol and low density lipoprotein cholesterol values in offspring are related to
parental levels of total cholesterol. There were clear differences between offspring of parents
with high cholesterol levels as compared to parents of low cholesterol values, for both total
cholesterol and low density lipoprotein cholesterol. The differences appear to remain fairly
constant throughout childhood. This is further substantiated by the analysis of chauge of
cholesterol levels during childhood within subjects. Low density lipoprotein-cholesterol and
-87-

Chapter 6
high density lipoprotein-cholesterol were shown to track to a similar extent as their main
constitnent apolipoproteins B and A-I, respectively (45). One might speculate that tracking
by parental risk of these apolipoproteins resembles tracking by parental risk of their
corresponding lipoproteins. For the angiographic patient-offspring stndy on apolipoproteins
and coronary atherosclerosis as described in chapters 2 and 3 of tills thesis more direct
information on tracking by parental risk was available. Studies on the relation between
apolipoprotein levels in offspring and myocardial infarction in their parents indicated tracking
by parental risk of apolipoprotein levels (42-44). There have been no studies on tracking by
parental risk of postprandial lipoproteins. Tracking of postprandial lipid response to an oral
lipid load may be related to the tracking of determinants of this response such as triglyceride
level and high density lipoprotein, (37). However, inference about tracking of this response
by parental risk is speculative.
Summary
In this chapter the familial aggregation of cardiovascular disease and of cardiovascular risk
factors were discussed. Familial aggregation of cardiovascular risk factors within fanlilies and
tracking of such factors by parental risk are the main premises for a patient-offspring study.
Current evidence shows that lipids and lipoproteins are fanlilial, and that they as well as
apolipoproteins show tracking. In previous stndies, tracking by parental risk was demonstrated
for apolipoproteins in offspring of parents with myocardial infarction. For the studies in
chapter 2 and 3 of this thesis the premise of tracking by parental risk was thus met for
apolipoproteins but speculative for postprandial lipoproteins.
References
Gertler MM", White PD. Coronary heart disease in young adults: A multidisciplinary study. Cambridge, Massachusetts: Harvard University Press; 1954.
2 Thomas CB, Cohen BH. The familial occurrence of hypertension and coronary artery disease with
observations concerning obesity and diabetes. Ann Intern Med 1955;42:90-127.
3 Rose G. Familial patterns in ischaemic heart disease. Br J Prey Soc Med 1964;18:75-80.
4 Slack J, Evans KA. The increased risk of death from ischaemic heart disease in first-degree relatives of 121 men and 96 women with ischaemic heart disease. J Med Genet 1966;3:239-57.
5 Rissanen AM. Familial occurrence of coronary heart disease: Effect of age at diagnosis. Am J
-88-

Chapter 6
Cardiol 1979;44:60-6.
6 Clarke WR, Sehrott HG, Bums n, Sing CP, Lauer RM. Aggregation of blood pressure in the
families of children with labile high systolic blood pressure: The Muscatine Study. Am J
Epidemiol 1986;123:67-80.
7 Laskarzewski P, Morrison JA, Horvitz R, Khoury P, Kelly K, Mellies M, Glueck CJ. The
relationship of parental history of myocardial infarction, hypertension, diabetes and stroke to
coronary heart disease risk factors in their adult progeny. Am J Epidemiol 1981;113:290-306.
8 Chesebro rn, Fuster V, Elveback LR, Frye RL. Strong family history and cigarette smoking as
risk factors of coronary artery disease in young adults. Br Heart J 1982;47:78-83.
9 Beaty TIl, Neel N, Fajans SS. Identifying risk factors for diabetes in first degree relatives of non
insulin dependent diabetic patients. Am J Epidemiol 1982;115:380-97.
10 Selby N, Newman B, King M, Friedman GD. Environmental and behavioral detenninants of
fasting plasma glucose in women. Am J Epidemiol 1987;125:979-88.
11 Gam SM. Family-line and socioeconomic factors in fatness and obesity: A matched co-twin
analysis. Nutr Rev 1986;44:381-6.
12 Perusee L, Leblanc C, Tremblay A, Allard C, Theriault G, Landry F, Talbot J, Bouchard C.
Familial aggregation in physical fitness, coronary heart disease risk factors, and pulmonary
function measurements, Prev Med 1987;16:607-15,
13 Sholtz RI, Rosenman RH, Brand RJ. The relationship of reported parental history to the incidence
of coronary heart disease in the Western Collaborative Group Study. Am J Epidemiol
1975;102:350-6.
14 Barrett-Connor E, Khaw K-T. Family history of heart attack as an independent predictor of death
due to cardiovascular disease, Circulation 1984;69: 1 065-9.
15 Colditz GA, Stampfer MJ, Willett WC, Rosner B, Speizer FE, Hennekens CH. A prospective study
of parental history of myocardial infarction and coronary heart disease in women. Am J Epidemiol
1986;123:48-58.
16 Hopkins PN, Williams RR, Kuida H, Stults BM, Hunt SC, Barlow OK, Owen Ash K. Family
history as an independent risk factor for incident coronary artery disease in a high-risk cohort in
Utah. Am J Cardiol 1988;62:703-7.
J 7 Philips AN, Shaper AG, Pocock 8J, Walker M. Parental death from heart disease and the risk of
heart attack. Eur Heart J 1988;9:243-5 I. 18 Colditz GA, Rimm EB, GiOV8IUlUCCi E, Stampfer MJ, Rosner B, Willett WC. A prospective study
of parental history of myocardial infarction and coronary artery disease in men. Am J Cardiol
1991 ;67:933-8.
19 Myers RH, Kiely DK, Cupples LA, Kannel WB. Parental history is an independent risk factor for
coronary artelY disease: The Framingham Sludy. Am Heart J 1990;120:963-9.
20 Schaefer E, Adlersberg D, Steinberg AG. Heredity, environment and serum cholesterol: a study
of 201 healthy families. Circulation 1958;17:537-542.
-89-

Chapter 6
21 Johnson BC, Epstein FH, Kjalsberg MO. Distributions and familial studies of blood pressure and
serum cholesterol level in a total community ~ Tecumseh. Michigan. J Chron Dis 1965;18:147-60.
22 Garrison RJ, Casteli WP, Feinleib M, Kannel WB, Havlik RJ, Padgett SJ, McNamara PM. TIle
association of total cholesterol, triglycerides, and plasma lipoprotein cholesterol levels in first
degree relatives and spouse pairs. Am J Epidemiol 1979; 110:313-21.
23 Tyroler HA, Heiss G, Heyden S, Hames CO. Family follow~up study of senlm cholesterol in
Evans County, Georgia. J Chron Dis 1980;33:323-30.
24 Sosenko JM, Breslow JL, Ellison RC, Miettinen OS. Familial aggregation of total cholesterol, high
density lipoprotein cholesterol and total triglyceride levels in plasma. Am J Epidemiol
1980; 112:656-60. 25 Friedlander Y, Bucher KD, Namboodiri KK, Keiss G, Kark ill. Tyroler HA, Eisenberg S, Stein
Y, Rifkind BM. Parent-offspring aggregation of plasma lipids in selected populations in North
America and Israel. The Lipid Research Clinics Prevalence Study. Am J Epidemiol 1987; 126:268-
79. 26 Lee J, Lauer RM, Clarke WR. Lipoproteins in the progeny of young men with coronary artery
disease: Children with increased risk. Pediatrics 1986;78:330~7.
27 Lauer RM, Lee J, Clarke WR. Factors affecting the relationship between childhood and adult
cholesterol levels: The Muscatine Study. Pediatrics 1988;82:309-18.
28 Clark WR, Schrou HG, Leaverton PE, Connor WE, Lauer RM. Tracking of blood lipids and blood
pressure in school age children: The Muscatine Study. Circulation 1978;58:626-34.
29 Webber LS, Cresanta JL, Voors A W, Berenson OS. Tracking of cardiovascular disease risk factor
variables in school-age children. J Chron Dis 1983;36:647-60.
30 Webber LS, Srinivasan SR, Wattigney WA, Berenson GS. Tracking of serum lipids and
lipoproteins from childhood to adulthood: The Bogalusa Heart Study. Am J Epidemiol
1991;33:884-98.
31 Freedman DS, Shear CL, Srinivasan SR, Webber LS, Berenson GS. Tracking of serum lipids and
lipoproteins in children over an 8-year period: The Bogalusa Heart Study. Prev Med 1985; 14:203-
16.
32 Stuhldreher WL, Orchard TJ, Donue RP, Kuller LH, Gloninger MP, Drash AL. Cholesterol
screening in childhood: Sixteen-year Beaver County Lipid Study experience. J Pediatr
1991; 119:551-6.
33 Laskarzewski P, Morrison JA, deGroot I, Kelly KA, Mellies MJ, Khoury P, Glueck CJ. Lipid and
lipoprotein tracking in 108 children over a four-year period. Pediatrics 1979;64:548-91.
34 Pagnan A, Ambrosio GB, Vincenzi M, Mormino P, Maiolino P, Oerin L, Barbieri E, Cappaletti
F, Dal Palu C. Precursors of atherosclerosis in children: The Cittadella Study. Follow-up and
tracking of total serum cholesterol, triglycerides, and blood glucose. Prev Med 1982; 11 :381-90.
35 Orchard TJ, Donahue RP, Kuller LH, Hodge PN, Drash AL. Cholesterol screening in childhood:
Does it predict adult hypercholesterolemia? The Beaver County Experience. J Pediatr
-90-

Chapter 6
1983;103:687-91.
36 Bao W, Srinivasan SR, Berenson GS. Tracking of serum apolipoproteins A-I and B in children and young adults: The Bogalusa Heart Study. J Clin Epidemiol 1993;46:609-16.
37 Porkka KVK, Viikari JSA, Taimela S, Dahl M, Akerblom HK. Tracking and predictiveness of
serum lipid and lipoprotein measurements in childhood: a 12 year follow-up. The Cardiovascular Risk in Young Finns Study. Am J Epidemiol 1994;140:1096-110.
38 Patsch JR, Prasad S, Gotto AM Jr, Patsch W. High density Iipoprotein2• Relationship of the plasma levels of this lipoprotein species to its composition, to the magnitude of postprandial lipemia, and
to the activities of lipoprotein lipase and hepatic lipase. J Clin Invest 1987;80:341-7.
39 Kashyap ML, Barnhart RL, Srivastava LS, Perisutti G, Allen C, Hogg B, Glueck CJ, Jackson RL. Alimentary lipemia: plasma high-density lipoproteins and apolipoproteins ClI and cm in healthy subjects. Am J Clin Nutr 1983;37:233-43.
40 Cohn JS, McNamara JR, Cohn SO, Ordovas JM, Schaefer EJ. Postprandial plasma lipoprotein
changes in human subjects of different ages. J Lipid Res 1988;29:469-79.
41 Greenberg RA, Green PP, Roggenkamp KJ, Barrett-Connor B, Tyroler HA, Heiss G. TIle
constancy of parent-offspring similarity of total cholesterol throughout childhood and early adult life. The Lipid Research Clinics Program Prevalence Study. 1984j37:833-8.
42 De Backer G, Hulstaert F, De Munck K, Rosseneu M, Van Parijs L, Dramaix M. Serum lipids and
apoproteins in stUdents whose parents suffered prematurely from a myocardial infarction. Am Heart J 1986;112:478-84.
43 Durrington PN, Ishola M, HUllt L, Arrol S, Bhatnagar D. Apolipoproteins (a), AI, and B and
parental history in men with early onset ischaemic heart disease. Lancet 1988jii: 1070-3. 44 Freedman DS, Srinivasan SR, Shear eL, Franklin FA, Webber LS, Berenson OS. The relation of
apolipoproteins A-I and B in children to parental myocardial infarction. N Bngl J Med 1986;315:721-6.
-91-


CHAPTER 7
SUMMARY

7. Summary
Cardiovascular disease is the leading cause of morbidity and mortality in western
industrialized countries. Nunlerous studies have shown that classical risk factors such as
hypertension, high levels of total and low density lipoprotein·cholesterol, low high density
lipoprotein·cholesterol and smoking are related to the occurrence of cardiovascular disease.
The atherosclerotic process starts early in life and from an etiologic and a preventive point
of view it is important to kuow if and to what extent this process and the diseases resulting
from it are related to risk factors measured in the young. Cardiovascular disease aggregates
in families, which implies that healthy relatives of patients with cardiovascular disease have
an increased risk for developing the disease themselves. Current evidence suggests that if in
certain families patient(s) have cardiovascular disease, otherwize healthy relatives of those
patients have an increased risk of the disease, a relation which is seemingly not predominantly
caused by aggregation of classical cardiovascular risk factors. Risk factors for cardiovascular
disease are also kuown to aggregate in families, meaning that there is a resemblance of the
levels of cardiovascular risk factors among fanlily members. A method for assessing the
relation between putative risk factors and cardiovascular disease is to study such factors in
offspring of patients with the disease. The general research question is if this new
cardiovascular risk factor is causally related to the occurrence of the disease in the parents.
Chapter 2 describes a study on postprandial triglyceride metabolism in 80 sons of fathers
with angiographically established coronary sclerosis and in 55 sons of fathers who had at most
only minor coronary atherosclerotic lesions at coronary angiography. Both groups of sons
received an oral lipid load and the subsequent postprandial handling of this lipid load was
studied in their serum for 12 hours after lipid loading. The sons of coronary artery disease
patients had a prolonged postprandial hypertriglyceridemia.
Chapter 3 describes a study on lipoprotein·cholesterollevels and apolipoprotein levels in 188
offspring of fathers with angiographically established severe coronary sclerosis and in 115
offspring of fathers who had at most only minor coronary lesions at coronary angiography.
In this study sons of patients with coronary artery disease had significantly lower mean levels
of high density lipoprotein3-cholesterol and of apolipoprotein A2. Although similar trends for
high density lipoprotein3-cholesterol and apolipoprotein A2 levels were observed in daughters
of patients none of the differences was statistically significant.
Chapter 4 describes an 18-year follow-up study on cardiovascular risk factors in 252 male
and 231 female children and young adults. These subjects were a random sample of
youngsters initially examined in the cross-sectional EPOZ study, a population based study on
risk factors for chronic diseases, conducted in 1975 - 1978 in the Dutch town of Zoetermeer,
-94-

Summary
and who were subsequently invited to take part in the follow-up study. In the initial EPOZ
study, the parents of these subjects were also examined. Total cholesterol levels measured in
the parents were then related to levels and change of levels of total cholesterol and its
lipoprotein-subfractions, which were repeatedly measured on a yearly basis. The results show
a strong cross-sectional as well as longitudinal relationship between parental total cholesterol
levels and levels of total cholesterol and low density lipoprotein-cholesterol throughout
childhood and adolescence. Overall, levels showed an initial tendency to decrease untill about
15 years of age with a rise in levels thereafter. Despite these changes in lipid levels
differences between groups of offspring contrasted by total cholesterol levels in their parents
appeared to be stable, indicating that parental total cholesterol level is not a major determinant
of change of cholesterol and lipoprotein-cholesterol levels during childhood and adolescence.
No offspring group differences were found for high density lipoprotein-cholesterol and its
subfractions.
In chapter 5 some considerations are given for the use of the patient-offspring study (chapter
2 and chapter 3) as a means to study the putative causal relationship between some factor as
measured in offspring, and disease as measured in parents. It is postulated that familial
aggregation of the risk factor as well as tracking by parental risk of the factor in offspring are
premises for the patient-offspring study. An often used approach to the patient-offspring study
is the offspring-perspective which means that offspring of parents with cardiovascular disease
are at increased risk for the disease and risk factors measured in offspring are related to their
increased disease risk. It is shown in chapter 5 that familial aggregation of disease is not
sufficient as a premise for the patient-offspring study. The parent-perspective to the patient
offspring study considers risk factor levels in offspring as an approximation of the level of
the factor in parents when they were of the age of their offspring. Thus, consideration of the
premise of familial aggregation of the risk factor is a logical step in this perspective and,
therefore, the parent-perspective is postulated to be a preferable approach to the patientoffspring study.
In chapter 6, the patient-offspring studies as described in chapters 2 and 3 are discussed in
the context of the current evidence for the relation between cardiovascular risk factors and
familial aggregation of cardiovascular disease. The study as described in chapter 4 is discussed
as being further evidence for familial aggregation of cardiovascular risk factors such as total
cholesterol and low density lipoprotein-cholesterol and as a model to investigate the premises
for the patient-offspring study.
-95-

7. Samenvatting
Hart- en vaatziekten vormen de belangrijkste oorzaak van morbiditeit en mortaliteit in
westerse geindustrialiseerde landen. Vele studies hebben aangetoond dat klassieke
risieofaetoren zoals hypertensie, verhoogde plasma gehalten van totaal en low density
Iipoproteine-eholesterol en roken zijn gerelateerd aan het ontstaan van hart- en vaatziekten.
Het proees van atheroselerose begint vroeg in het leven. Het is daarom van belang vanuit
etiologiseh en preventief oogpunt om na te gaan in hoeverre dit proees en de daaruit
resulterende ziekten samenhangen met risieofaetoren bij jongeren. Hart- en vaatziekten
aggregeren in fanlilies, hetgeen suggereert dat gezonde verwanten van patienten met hart- en
vaatziekten zelf een verhoogd risico hebben op deze ziekten. Ook risicofaetoren voor hart- en
vaatziekten aggregeren in fanlilies, betgeen betekent dat niveau's van deze risieofaetoren in
met elkaar verwante familieleden overeenkomen. Onderzoek laat zien dat gezonde verwanten
van patienten een verhoogd risieo op hart- en vaatziekten hebben, waarbij kan worden
aangetekend dat deze relatie niet uitsluitend kan worden verklaard op basis van familiaire
aggregatie van cardiovasculaire risicofactoren. Een methode om de relatie tussen veronderstelde risieofaetoren en hart- en vaatziekten te
onderzoeken is het bepalen van zulke risieofactoren in nakomelingen Van patienten die Iijden
aan dergelijke ziekten. De algemene onderzoeksvraag is daarbij of er een causaal verband
bestaat tussen deze risieofaetoren en het ontstaan van de ziekten.
Hoofdstuk 2 beschrijft een onderzoek naar het postprandiale triglyeeriden metabolisme in
80 zonen van vaders met angiografisch aangetoonde coronair atherosclerose en in 55 zonen
van vaders die bij angiografie hoogstens minimale eoronairafwijkingen hadden. Beide groepen
zonen kregen een orale vetbelasting toegediend en de postprandiale verwerking daarvan werd
bestudeerd in het bloed gedurende 12 uur na toediening van de vetbelasting. Zonen van vaders
met corooair atherosclerose hadden ten opzichte van zonen uit de controle groep een verlengde postprandiale hypertriglyceridaemie.
Hoofdstuk 3 beschrijft een onderzoek naar niveau's van Iipoproteine-cholesterol en
apoproteinen in 188 nakomelingen van vaders met angiografisch aangetoonde eoronair
atheroselerose en in 115 nakomelingen van vaders met angiografisch hoogstens minimale
eoronaire afwijkingen. Zonen van patienten hadden gemiddeld statistisch significant lagere
waarden van high density Iipoproteine3-eholesterol en van apoproteine A2. Hoewel
vergelijkbare trends voor waarden van high density Iipoproteine3-eholesterol en apoproteine
A2 te zien waren bij doehters van patienten waren de groepsverschillen niet statistiseh
significant.
Hoofdstuk 4 beschrijft een vervolgstudie, uitgevoerd over een periode van 18 jaar, naar
-96-

Samenvafling
cardiovasculaire risicofactoren in 252 mannelijke en 231 vrouwelijke kinderen en jonge
volwassenen. Deze groep kinderen vormde een random sample uit jongeren die zijn
onderzocht in het Epidemiologisch Preventief Onderzoek Zoetermeer (EPOZ). Het EPOZ
onderzoek is een populatie onderzoek naar risicofactoren voor chronische ziekten, dat in de
periode 1975 - 1978 is uitgevoerd in Zoetermeer. Deze groep heeft deelgenomen aan een
vervolgstudie waarbij serom totaal cholesterol gehalten en lipoproteinen-fracties jaarlijks zijn
gemeten. In het EPOZ populatie onderzoek zijn serom totaal cholesterol gehalten tevens
eenmalig gemeten bij de ouders van deze groep kinderen. De gehalten in de ouders zijn
bestudeerd in relatie tot de herhaald gemeten gehalten bij hun kinderen. De resultaten laten
zien dat er een sterk cross-sectioneel en ook longitudinaal verband bestaat tussen ouderlijke
totaal cholesterol gehalten en de totaal cholesterol en low density lipoproteine-cholesterol
gehalten bij kinderen en jonge volwassenen. In aHe groepen kinderen vertoonden de totaal
cholesterol gehalten een daling tot ongeveer het 15e jaar en daarna een stijging. Ondanks deze
veranderingen bleven de verschillen tussen de groepen kinderen, ingedeeld naar cholesterol
niveau's van hun ouders, gelijk. Dit wijst erop dat ouderlijke cholesterol gehalten weI een
belangrijke determinant zijn van de niveau's van totaal cholesterol en low density
lipoproteine-cholesterol tijdens de jeugd, maar niet van de veranderingen hierin in de tijd.
Voor high density lipoproteine-cholesterol en de subfracties daarvan werden geen verschiHen
bij de kinderen waargenomen.
In hoofdstuk 5 worden eakele overwegingen gegeven voor het onderzoeken van patienten
en nakomelingen (patient-offspring onderzoek, hoofdstukken 2 en 3) als methode om het
veronderstelde oorzakelijk verband te bestuderen tussen een risicofactor zoals gemeten in
kinderen en de ziekte zoals gemeten in hun ouders. Besproken wordt dat familie aggregatie
van een risicofactor alsmede "tracking naar ouderlijk risico" van de risicofactor in de kinderen
aannamen zijn voor de patient-offspring studie. Een vaak toegepaste benadering van de
patient-offspring studie is de benadering vanuit de kinderen (offspring-perspective). Dit houdt
in dat kinderen van patienten met cardiovasculaire ziekten zelf een verhoogd fisico op deze
ziekten hebben en risicofactoren, gemeten in de kinderen, worden gerelateerd aan dit
verhoogde ziekte risico. In hoofdstuk 5 wordt gedemonstreerd dat familie aggregatie van
ziekte als aanname niet voldoende is voor de patient-offspring studie. Bij de benadering vanuit
de ouders (parent-perspective) worden niveau's van risicofactoren in kinderen beschouwd als
een schatting van de .niveau's van deze factoren in de ouders toen zij de leeftijd van hun
kinderen hadden. In deze benadering is het een logische stap om rekening te houden met de
aanname van familie aggregatie van de risicofactor. Om deze reden zou in de patient-offspring
studie de benadering vanuit de ouders moeten worden verkozen boven die vanuit de kinderen.
-97-

Samenvalling
In hoofdstuk 6 worden de patient-offspring studies zoals beschreven in de hoofdstukken 2
en 3 geplaatst in het licht van de huidige kennis over de relatie tussen risicofactoren en
familie aggregatie van hart- en vaatziekten. Het in hoofdstuk 4 beschreven onderzoek wordt
besproken als nieuwe aanwijzing voor familie aggregatie van risicofactoren voor hart- en vaatziekten zoals totaal cholesterol en low density lipoproteine-cholesterol geh.lten. Tevens
wordt dit onderzoek beschreven als model om de aannamen voor de patient-offspring studie
te onderzoeken.
-98-

Danl<woord
Bij de totstandkoming van dit proefschrift is een aantal personen van groot belang gewees!.
Prof.dr ruck Grobbee dank ik voor zijn zeer kundige begeleiding. De werkbesprekingen die
ik met hem had zijn nogal eens geeindigd met het vaststellen van een rueuwe planning en het
is met name door zijn stimulans geweest dat dit proefschrift er is. Prof.dr Albert Hofman ben
ik dankbaar voor zijn bijdrage aan de totstandkoming van het onderzoek en zijn voortdurende
enthousiasme. Dr.ir Jacqueline Witteman wit ik drulken voor de dagelijkse begeleiding. De
vele inhoudelijke discussies die ik met haar had zijn voor dit proefschrift als geheel onmisbaar
gewees!. Dr. Willy-Anne van Stiphout ben ik erkentelijk omdat het onderzoek een voorzetting
was in een richting die zij voor een belangrijk deel initieerde. Voor de ziekenhuis gebonden
onderzoeken was samenwerking met velen onontbeerlijk. Dr. Hanno Krauss, cardioloog in het
Zuiderziekenhuis Rotterdam, maakte uitvoering van deze onderzoeken in zijn kliruek en in
andere klirueken mogelijk. Dr. Aad van Tol, biochemicus van de afdeling Biochemie van de
Erasmus Universiteit, dank ik voor zijn inzet bij de vele laboratoriumbepalingen en voor veel
prive onderwijs op het gebied van het lipoproteinen metabolisme. Dr. Louis Havekes,
biochemicus van het TNO Institute for Ageing and Vascular Research in Leiden, dank ik voor
de apo-E phenotyperingen. Ing. Ton de Bruijn en Jeanette Vergeer-Drop dank ik voor de vele
lipiden bepalingen en apoproteinen bepalingen die zij hebben verricht. De cardiologen Dr. F.J.
ten Cate van het Academisch Ziekenhuis Rotterdam, Dr. Ph. W. Fels van het Refaja
Ziekenhuis te Dordrecht en Dr. H.J. Kingma van het Antonius Ziekenhuis te Nieuwegein en
hun staf waren zeer behulpzaam bij het uitbreiden van het onderzoek in hun klinieken. Voor
de praktische uitvoering van de onderzoeken waren twee personen van bijzonder belang.
Vooral dankzij het onverwoestbare goede humeur van Lorette Hulsman bleek het haalbaar om
zoveel jongeren in het onderzoek te betrekken, ze op hun nuchtere maag een enorme
hoeveelheid vet te laten drinken, als eruge maaltijd voor de 12 uur daama, en ze tevens om
het uur bloed te laten afstaan. Ik ben haar bijzonder dankbaar voor haar enorme inzet op vaak
onaantrekkelijke tijden en afgelegen plaatsen. De jarenlange bijdrage van Joke Janssen uit
Zoetermeer aan het EPOZ jaaronderzoek heeft bijgedragen aan een imniddels unieke studie.
Ik dank haar voor de prettige samenwerking op de dinsdagavonden. De afdeling computing
is altijd zeer behulpzaam gewees!. Marcel Eijgermans wit ik met name noemen voor zijn ruet
aflatende steun bij het beschikbaar en analyseerbaar maken van onderzoeksgegevens. Chris
de Ruijter speelde een belangrijke rol in het oplossen van pc-problemen. Mijn ex
kamergenoten Cock van Duijn, Jacqueline Witteman, Erik Buskens en huidige kamergenoot
Amo Hoes en ook aUe andere coUega's van het Instituut Epidemiologie & Biostatistiek dank
ik voor de prettige samenwerking. Marieke Visser dank ik voor haar correctiewerk ten
behoeve van dit proefschrift. Ik ben blij dat Carl Moons en Thorold Uiterwaal mijn
-99-

Samenvattlng
paranymfen zijn. Ed van Beeck, managing director van het Netherlands Institute for Health
Sciences, wi! ik danken voor de wijze waarop hij meehieIp om de combinatie van promoveren
en NIHES onderwijsco5rdinatie uiteindeIijk mogeIijk te maken. Ook het NIHES secretariaat
in de personen van Mariska Drinkwaard, Cilia Kuynders, Soeja de Groot en Marie-Louise Bot
dank ik daarvoor. Dr. Ina Koopman-van Daro, cardioIoog, dank ik voor haar belangrijke
bijdrage. Sien en Iannis Kostoulas dank ik voor de vele nachten die ik bij hun in Rotterdaro
kon doorbrengen. Tenslotte ben ik heel veel dank verschuldigd voor de bijdrage van vele gezinnen aan het onderzoek en voor de bijdrage aan dit proefschrift van mijn eigen gezin,
Maayke, Dirk en Atma.
-100-

About tbe author
Cuoo Uiterwaal was born on March 5, 1955 in Utrecht, The Netherlands. He graduated in
1976 from the Stichting Utrechtse Avondscholen (secondary school) in Utrecht. After a period
of studying psychology he started his medical training in 1979 at the Rijksuoiversiteit Utrecht.
In 1987 he received his medical degree and started research work in the field of cardiac echo
doppler in Nijmegen. In 1988 he started the work as described in this thesis and received a
training in epidemiology at the Department of Epidemiology & Biostatistics of Erasmus
University Rotterdam (head Prof.Dr. A. Hofman). Since 1993 he has been a staff member of
the Netherlands Institute for Health Sciences.
-101-