Embed Size (px)
Citation preview

Frameworks for Research
Patricia Liehr and Mary Jane Smith
From Practice to Research
To be introduced to frameworks for research, put yourself in the shoes of Kate and thoughtfully
listen to her story by attending to the message it brings for the practicing nurse wishing to critique,
understand and do research. Kate works in a coronary care unit (CCU). She has worked in this unit for
nearly three years, since she graduated with a baccalaureate degree in nursing. She has grown more
comfortable over time and now believes that she can readily manage whatever comes her way with the
complexities of patient care in the CCU. Recently, she has been observing the pattern of blood pressure
(BP) change when healthcare providers enter a patient’s room. This observation began when Kate
noticed that one of her patients a 62 year old African-American woman who had continuous arterial
monitoring, had dramatic increases in BP, as much as 100%, each time the healthcare team made rounds
in the CCU. Furthermore, this elevated BP persisted after the team left her room and slowly decreased
to reach pre-round levels within the following hour. Conversely, the same patient, when visited by the
nurse manager on her usual daily rounds, engaged calmly in conversation and was often left with lower
BP when the nurse-manager moved on to the next patient. Kate thought about what was happening and
adjusted her work so that she could closely observe the details of this phenomenon over several days.
Team rounds were led by the attending cardiologist and included nurses, pharmacists, social
workers, medical students and nursing students. The nurse-manager’s visit occurred one-on-one. During
team rounds the patient was discussed and occasionally, she was asked to respond to a question about
her history of heart disease or her current experience of chest discomfort. Participants took turns
listening to her heart and students responded to questions related to her case. During the nurse manager
conversation, the patient had the nurse’s attention. In fact, the nurse usually sat and spent time. Kate
noticed that the nurse manager was especially attentive to the patient’s experience. She spent time
talking to the patient about how her day was going, what she was thinking about while lying in bed and
what feelings were surfacing as she began to consider how life would be when she returned home.
Kate decided to talk to the nurse manager about her observation. The nurse manager, Alison,
was pleased that Kate had noticed these BP changes associated with interaction. She told Kate that she,
too, noticed these change during her 8 year experience of working in CCU. Her observation led her to a
theory, which seemed applicable to the observation. As a first year Master’s student Alison learned the

theory, attentively embracing story (Smith & Liehr, 1999; Liehr & Smith, 2000). She was applying the
theory in practice and beginning plans to use the theory to guide her thesis research. Attentively
embracing story proposes that intentional nurse-client dialogue, which engages the human story, enables
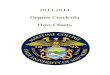
connecting with self-in-relation to create ease (Figure 1). As depicted by the theory model, the central
concept of the theory is intentional dialogue. It is what Kate had first observed when she noticed Alison
interacting with the patient. Alison was there with full attention, following the patient’s lead and
pursuing what mattered most to the patient. Alison seemed to get a lot of information in a short time and
the patient seemed willing to share things, which she wasn’t sharing with other people.
According to the theory, each of the three concepts, intentional dialogue, connecting with self-
in-relation, and creating ease are intricately connected. So, when Kate observed intentional dialogue,
she also observed connecting with self-in-relation as the patient reflected on her experience in the
moment; and, creating ease, when she saw lowered BP as the nurse-manager left the room. Alison and
Kate shared an understanding that there was a relationship between patient-health care provider
interaction and BP. They discussed several possible issues, which might be affecting this relationship.
They identified research questions related to each issue (Table 1). You may be able to think of other
issues, which could generate a research question contributing to understanding of the relationship
between patient-health care provider interaction and BP. The list developed by Kate and Allison only
serves as a reflection of the complexity of the relationship. The list highlights the fact that the
relationship cannot be understood with one study but a series of studies may enhance understanding and
offer suggestions for change. For instance, a thorough understanding may lead to testing of different
approaches for conducting team rounds.
Practice-theory-research links
There are several important aspects of frameworks for research embedded in the story of Kate
and Alison. First, it is important for the reader to notice the links between practice, theory and research.
Each is intricately connected with the other to create the knowledge base for the discipline of Nursing.
(Figure 2). Theory is a set of interrelated concepts, which provides a systematic view of a phenomenon.
Theory guides practice and research; practice enables testing of theory and generates questions for
research; research contributes to theory-building, and selecting practice guidelines. So, what is learned
through practice, theory and research interweaves to create the knowledge fabric of the discipline of
Nursing. From this perspective, each reader is in the process of contributing to the knowledge base of
the discipline. For instance, if you are practicing, you can use focused observation (Liehr, 1992) just as

Kate did, to consider the nuances of situations, which matter to patient health. Kate noticed the change
in BP occurring with interaction and systematically began to pay close attention to the effect of varying
interactions. This inductive process often generates the questions, which are most cogent for enhancing
patient well-being.
Approach to science
Another major theme of the story of Kate and Alison can be found in each nurse’s way of
approaching the phenomenon of the relationship between health care provider-patient interaction and
BP. Each nurse was using a different approach for looking at the situation, but both were systematically
evaluating what was observed. This is the essence of science…systematic collection, analysis and
interpretation of data. Kate was using inductive reasoning, a process of starting with details of
experience and moving to a general picture. Inductive reasoning involves the observation of a particular
set of instances that belong to and can be identified as part of a larger set. (Feldman, 1998). Alison told
Kate that she, too, had begun with inductive reasoning and now was using deductive reasoning, a
process of starting with the general picture, in this case the theory of attentively embracing story, and
moving to a specific direction for practice and research. Deductive reasoning uses two or more related
concepts, that when combined, enable suggestion of relationships between the concepts (Feldman,
1998). Inductive and deductive reasoning are basic to frameworks for research. Inductive reasoning is
the pattern of “figuring out what’s there” from the details of the nursing practice experience. Inductive
reasoning is the foundation for most qualitative inquiry (Chapter 9). Research questions related to the
issue of the meaning of experience for the patient (Table1) can be addressed with the inductive
reasoning of qualitative inquiry. Deductive reasoning begins with a structure, which guides one’s
searching for “what’s there”. All but the last two research questions listed in Table 1 would be
addressed with the deductive reasoning of quantitative inquiry.
Given Alison’s use of deductive reasoning guided by the theory of attentively embracing story, it
can be assumed that she has read and critiqued the literature on theoretical frameworks, and has chosen
attentively embracing story as a theoretical framework to guide her Master’s thesis research. In order for
Kate to move on in her thinking about research to study the way changes in blood pressure are related to
healthcare provider-patient interaction, she needs to become well versed on the importance of
theoretical frameworks. As she reads the literature and reviews research studies, she will critique the
theoretical frameworks guiding those studies. In doing the critiquing of existing frameworks, she will

develop the knowledge and understanding needed to choose an appropriate framework for research. As
a beginning, Kate is reading this chapter, recognizing herself as a critiquer of nursing research.
HELPFUL HINT
Investigators may not always provide a detailed explicit statement of the observation(s) that led them to
their conclusion(s) when using inductive reasoning; likewise, you will not always find a clear picture of
the structure guiding the study when deductive reasoning has been used.
Frameworks as structure for research
Whether evaluating a qualitative or a quantitative study, it is wise to look for the framework,
which guided the study. Generally, when the researcher is using qualitative inquiry and inductive
reasoning methods, the critiquer will find the framework at the end of the manuscript in the discussion
section (See Chapter 9). From the findings of the study, the researcher builds a structure for moving
forward. In the study on bone marrow transplantation in the appendix C (Cohen & Ley, 2000), the
researchers obtained stories about what it was like to have a bone marrow transplant. These stories were
analyzed and the findings were synthesized at the theoretical level. The researchers moved from
particulars of the bone marrow transplant experience to a general structure of concepts, which included
fears, losses, hopes and a sense of transitioning through a life-altering event. These concepts were
described in the context of the subjects’ stories and relevant literature, creating a conceptual structure,
which could be modeled.
A model is a symbolic representation of a set of concepts, which is created to depict
relationships. Figure 1 is the model of attentively embracing story. It represents the nurse-client
connection through the rhythmical symbol labeled intentional dialogue. The model depicts process by
linking the concepts through nurse-client dialogue with arrows, which link to each other. This model
could be the basis for deductive reasoning. An example of a deductive question, which could be derived
from the model, is:
What is the difference in salivary cortisol (an indicator of ease) for cancer patients who engage with
participants (connecting with self-in-relation) in a nurse-led (intentional dialogue) cancer support
group?
HELPFUL HINT
When an investigator has used a deductive approach, the theoretical framework should

be described to substantiate how the research question emerged.
When the researcher is using quantitative inquiry and deductive reasoning methods, the critiquer
will find the framework at the beginning of the paper before a discussion of study methods. In the study
of a model for discharge planning for elders with heart failure in the appendix of this book, Bull,
Hansen and Gross (2000) present a model, which they have derived from a broader evaluation
perspective. Their model, which depicts inputs, process and outputs, is a framework for structuring the
research questions and accompanying hypotheses. The inputs they identify are elder and family-
caregiver characteristics. The process is the partnership model, which proposes that discharge planning
be a collaborative interaction between professionals, patients and family caregivers. The partnership
model is the intervention administered to the experimental group in their research. The outputs or
outcomes they measure are: health status satisfaction, perception of care continuity, difficulties of
managing care and resource use for both the elderly patient and the family caregiver. The researchers
have identified questionnaires or medical record sources, which will bring these outcomes to a
measurable level. Their model and the related literature lead Bull, Hansen and Gross (2000) to
hypothesize that (p.20):
1. scores on perceived health will be different for clients in the intervention and control cohorts;
2. client satisfaction with discharge planning, perceptions of care continuity, preparedness and
difficulties managing care will differ for the intervention and the control cohorts;
3. caregiver’s response to care-giving will be different for the experimental and control cohorts; and,
4. resource use will be different for the control and intervention cohorts.
The researchers have used deductive reasoning to move from their model, which they substantiated with
literature, to the hypotheses (See Chapter 3), or best guesses about what they will find. Their model has
provided a framework to guide their research from theory to hypotheses. They have moved from the
abstract to the concrete, in contrast to Cohen and Ley’s (2000) movement from the concrete experience
of bone marrow transplant to the abstract structure of the concepts.

The ladder of abstraction
The ladder of abstraction is a way for the critiquer to gain a perspective when reading and
thinking about frameworks for research. When critiquing the framework of a study, imagine a ladder
(Figure 3). The highest level on the ladder includes beliefs, assumptions, what is sometimes called the
worldview of the researcher. Although the worldview is not always explicitly stated in a manuscript, it
is there. In the study on outcomes of anger (Mahon, Yarcheski & Yarcheski, 2000) (See appendix B),
the researchers hold beliefs that there is a relationship between mind and body, and that emotions do
indeed influence health. The middle level on the ladder includes the frameworks, theories and concepts
the researcher uses to articulate the problem, purpose and structure for research. Mahon, Yarcheski and
Yarcheski (2000) study the problem of positive and negative outcomes of anger in early adolescents.
The purposes described by the authors were to examine symptom patterns and diminished well-being as
negative outcomes of trait and state anger; and vigor and willingness to change as positive outcomes of
trait and state anger. Using the literature they create frameworks of the positive and negative outcomes
of state and trait anger. These frameworks, which are presented as models, guide their research study
and are based on Spielberger’s theory of anger. The negative outcomes framework depicts relationships
between the concepts of state anger, trait anger, diminished well-being and symptom patterns. The
positive outcomes framework outlines links between state anger, trait anger, vigor and willingness to
change. These frameworks were derived from the literature and constructed by the researchers in order
for them to logically structure their study.
This “middle of the ladder” position of frameworks, theories and concepts moves to a lower
rung where the empirical is located. The empirical is about that which can be observed through the
senses. The empirical includes the variables, which are measured and described in quantitative research
studies and the story that is described in qualitative studies. Table 2 outlines the concepts with their
conceptual definitions and the accompanying variables with their operational definitions from the
Mahon, Yarcheski and Yarcheski (2000) study.
A conceptual definition is much like a dictionary definition, conveying the general meaning of
the concept. However, the conceptual definition goes beyond the general language meaning found in the
dictionary by defining the concept as it is rooted in the theoretical literature. The operational definition

specifies how the concept will be measured….what instruments will be used to capture the variable. In
looking closely at the language used to describe conceptual and operational definitions (Table 2), the
critiquer will notice that operational definitions are lower on the ladder of abstraction than conceptual
definitions. The language of the operational definition is closer to the ground.
HELPFUL HINT
Some reports of research embed conceptual definitions in the literature review. It is wise for the
critiquer to seek and find the conceptual definitions so that the logical fit between the conceptual
and operational definitions can be determined.
The middle of the ladder: Frameworks, theories and concepts
It is important to consider the middle of the ladder of abstraction, where concepts, theories and
frameworks are located. Pretend to look at the middle section through a magnifying glass so that what is
located there can be distinguished and clarified. Concepts, theories and frameworks can be compared to
each other from the perspective of abstraction, concepts being the lowest on the ladder and frameworks
highest. However, some concepts are closer to the ground than others. The same is true for theories and
frameworks. For instance, the concept of pain relief is closer to the ground than the concept of caring.
The idea of varying levels of abstraction within the middle of the ladder will be emphasized in the
section addressing theories but it has relevance for concepts and frameworks as well.
Concepts
A concept is an image or symbolic representation of an abstract idea. Chinn and Kramer (1999)
define a concept as a “complex mental formulation of experience”. Concepts are the major components
of theory and convey the abstract ideas within a theory” (p. 252). Already, the reader has been
introduced to several concepts, such as trait and state anger, well-being and vigor. The concepts of the
theory of attentively embracing story, intentional dialogue, connecting with self-in relation and creating
ease, have been defined and their relationship has been modeled for the reader. Each concept creates a
mental image, which is explained further through the conceptual definition. For instance, pain is a
concept and when it comes to mind, it means something based on experience. The experiential meaning
of the concept is different for the child who had just fallen off a bike, or the elderly person with

rheumatoid arthritis or the doctorally prepared nurse who is studying pain mechanisms using an animal
model. These definitions and associated images of the concept of pain incorporate different experiential
and knowledge components…all with the same label, pain. Therefore, it is important to know the
meaning of the concept for the person. In the case of the critiquer, it is important to know the meaning
that the researcher gives to the concepts in a research study. As outlined in Table 2, Mahon, Yarcheski
and Yarchesi (2000) very clearly defined the concepts of interest in their study.
Theories
A theory is a set of interrelated concepts, which structure a systematic view of phenomena for
the purpose of explaining or predicting. A theory is like a blueprint, a guide for modeling a structure. A
blueprint depicts the elements of a structure and the relation of each element to the other, just as a
theory depicts the concepts, which compose it and the relation of concepts with each other. Chinn and
Kramer (1999) define a theory as an “expression of knowledge….a creative and rigorous structuring of
ideas that project a tentative, purposeful, and systematic view of phenomena.” (p. 258). Theories are
located on the ladder of abstraction relative to their scope. An often-used label in nursing is Grand
Theory, which suggests a broad scope, covering major areas of importance to the discipline. Grand
theories arose at a time when nursing was addressing its nature, mission and goals (Im & Meleis, 1999).
Therefore, it is historically important. However, the importance of grand theory extends beyond history
to have implications for guiding the discipline today and in the future. For the purpose of introducing
the critiquer to theory as a framework for nursing research, grand theory, midrange theory and micro-
range theory will be discussed. As is suggested by the names of these theory categories, grand theories
are highest and micro-range theories are lowest in level of abstraction.
Grand Theory
Theories unique to nursing help the discipline define how it is different from other disciplines.
Nursing theories reflect particular views of person, health, environment and other concepts that
contribute to the development of a body of knowledge specific to nursing’s concerns (Feldman, 1998).
Grand theories are all-inclusive conceptual structures, which tend to include views on person, health
and environment to create a perspective of nursing. This most abstract level of theory has established a
knowledge base for the discipline and is critical for further knowledge development in the discipline.

There are several well-known nursing theorists whose grand theories have served as a basis for
practice and research. Among these theories are Rogers’ (1990; 1992) science of irreducible human
beings; Orem’s (1995) theory of self-care deficit; Neuman’s theory of health as expanding
consciousness (1997); Roy’s adaptation theory (1991); Leininger’s culture care diversity and
universality theory (1996); King’s goal attainment theory (1997); and, Parse’s theory of human
becoming (1997). Each of these grand theories addresses the phenomena of concern to nursing from a
different perspective. For example, Rogers views the person and the environment as energy fields
coextensive with the universe. So, she recognizes the person-environment unity as a mutual process. In
contrast, King (1997) distinguishes the personal system, from the interpersonal and social systems,
focusing on the interaction between the systems, and the interaction of the systems with the
environment. So, for King, person and environment are interacting as separate entities. This is different
than the person-environment mutual process described by Rogers.
If a researcher is using Roger’s theory to guide plans for a study, the research question will
reflect different values than if the researcher is using King. The researcher using Roger’s theory might
study the relationship of therapeutic touch, to other phenomena which reflect a valuing for energy fields
and pattern appreciation, while the one using King might study outcomes related to nurse-patient shared
goals or other phenomena related to interacting systems. It is important for the critiquer to realize that
one grand theory is not better than another. Rather, these varying perspectives allow the nurse-
researcher to select a framework for research, which facilitates movement of concepts of interest down
the ladder of abstraction to the empirical level, where they can be measured as study variables. What is
most important about the use of theoretical frameworks for research is the logical connection of the
theory to the research question and the study design.
Midrange Theory
Mid-range theory is a focused conceptual structure, which synthesizes practice-research into
ideas central to the discipline. Merton (1968), who has been the original source for much of Nursing’s
description of mid-range theory, says that mid-range theory lie between everyday working hypotheses
and all-inclusive grand theories. The critiquer might notice that Merton’s view of the “middle” allows
for a great deal of space…between grand theories and hypotheses. This expansive view of the “middle”
has been noted and efforts have been made to more clearly articulate the middle, as well as distinguish
the characteristics of midrange theory. Liehr and Smith (1999), in a ten year review of nursing literature
using specific criteria, identified 22 midrange theories. Following the suggestion of Lenz (1996), they

considered the scope of the 22 midrange theories and grouped the 22 into high-middle, middle-middle
and low-middle categories using the theory names (Table 3). The critiquer will recognize that the
groupings move from a higher to a lower level of abstraction. Because midrange theories are lower in
level of abstraction than grand theories, they offer a more direct application to research and practice. As
the level of abstraction decreases, translation into practice and research simplifies. In their conclusion,
Liehr and Smith (1999) recommend that nurses thoughtfully construct midrange theory weaving
practice and research threads to create a whole fabric, which is meaningful for the discipline. Hamric,
Spross and Hanson (2000) in their text on advanced nursing practice call midrange theories to the
attention of advanced practice nurses:
“Middle-range theories address the experiences of particular patient populations or a cohort of
people who are dealing with a particular health or illness issue……Because middle range
theories are more specific in what they explain, practitioners often find them more directly
applicable…” (p. 159).
The theory of attentively embracing story, introduced in the beginning of this chapter as one,
which Kate was using to guide her practice and research, is a middle range theory. The theory
was generated from nursing practice and research experience (Smith & Liehr, 1999).
Micro-range theory
Micro-range theory is a linking of concrete concepts into a statement that can be
examined in practice and research. Higgins and Moore (2000) distinguish two levels of micro-
range theory, one of higher level abstraction than the other. Micro-range theory at the higher
level of abstraction, they suggest, is closely related to midrange theory, comprised of a limited
number of concepts and applicable to a narrow issue or event (Higgins & Moore, 2000) The
low-middle theory in Table 3 may fit this category. Hypotheses are an example of low
abstraction micro-range theories. The critiquer will recall that a hypothesis is a best guess or
prediction about what one expects to find. Chinn and Kramer (1999) define a hypothesis as a
“tentative statement of relationship between two or more variables that can be empirically
tested” (p. 254). Higgins and Moore (2000) emphasize the value of micro-range theory, noting
that the “particularlistic approach is invaluable for scientists and practitioners as they work to
describe, organize and test their ideas” (p 181).
As you read this text, you could articulate a micro-range theory at the level of a
hypothesis. In the beginning of the Chapter, Kate formulated a hypothesis about the relationship

between patient-health care provider interaction and blood pressure. Although Kate didn’t label
her idea as a hypothesis, it was a best guess based on observation. If you would take a minute to
think about it, some experience from nursing practice, which has provoked confusion, could be
stated as a hypothesis. A mismatch between what is known or commonly accepted as fact and
what one experiences creates a hypothesis-generating moment. Every nurse has hypothesis-
generating moments. Cultivating these moments requires noticing them, focusing observation to
untangle details, and allowing time for creative thinking and dialogue (Liehr, 1992), leading to
possibilities for creating low level micro-range theory…. or hypotheses.
HELPFUL HINT
The critiquer of research will find mixed messages about levels and placement of theory. While one
author labels a particular theory “grand”, another author will label the same theory “midrange”. The
critiquer can read the theory carefully and place it on the ladder of abstraction. If the theory is at the
more concrete level on the ladder, then it falls into micro-theory.
Frameworks for research
The critical thinking decision path (Figure 4) takes the critiquer through the thinking of a researcher
who is about to begin doing research. It is reasonable for the critiquer to expect to find some but not
all of the phases of decision-making addressed in a research manuscript. Beginning with the view of
the world, the highest rung on the ladder of abstraction, the researcher is inclined to approach a
research problem from a perspective of inductive or deductive reasoning. If going in the direction of
inductive reasoning, the researcher will generally not present a framework before beginning
discussion of the methods. This is not to say that literature will not be reviewed before introducing
methods. As an example, consider the Cohen and Ley (2000) manuscript in Appendix C. The authors
provide a brief overview of the increasing prevalence of bone marrow transplant as a treatment for
cancer and they describe several studies which examined dimensions of life for persons undergoing
transplant. The point of their literature review is to establish a case for doing the research they are
reporting. They do not provide a framework for the study because they are planning an inductive
approach to study the problem. Their intent is to be free of the structures, which may limit what they
learn; and, to be open to the experience of the person who is living through a bone marrow transplant.

Referring back to Figure 4, if one’s view of the world guides deductive reasoning, the researcher
will go in one of two directions; a choice will be made between a conceptual or a theoretical
framework. The critiquer will notice when reading the theory literature that these terms are used
interchangeably (Chinn & Kramer, 1999). However, in this case, each term is being distinguished
from the other on the basis of whether the researcher is creating the structure or whether the structure
has already been created by someone else. Generally, each of these terms refers to a structure, which
will provide guidance for research. If it is a conceptual framework, it is a structure of concepts
and/or theories which are pulled together as a map for the study. If it is a theoretical framework, it
is structure of concepts which exists in the literature, a ready-made map for the study
To better understand these differences, refer to the manuscript by Mahon, Yarcheski and
Yarcheski (2000) in Appendix B. These authors create a conceptual framework for their study
incorporating Spielberger’s anger theory with the four concepts, well-being, symptom patterns, vigor,
and willingness to change. This framework is shared as a model and the critiquer is able to follow the
logic of the study by referring to the conceptual framework. In contrast, the manuscript by LoBiondo-
Wood, Williams and Kouzekanani (2000) (Appendix D) uses a theoretical framework to guide their
research, the Double ABC-X Model of Family Adaptation. Although not a nursing theory, the Model
of Family Adaptation is a tested structure, which some would label a midrange theory. The authors
focus on one piece of the Model, the post-crisis period, which includes the five concepts, pile-up,
existing new resources, coping, perception of stressor and adaptation. Each of these concepts is
presented with clear indication of how it was measured in this sample of mothers of transplant
children. The Double ABC-X Model of Family Adaptation logically guides the choice of variables
and measures. Instead of creating a structure, these authors used a theoretical framework, which
already existed in the literature.
HELPFUL HINT
When researchers use conceptual frameworks to guide their studies, you can expect to find a system of
ideas, synthesized for the purpose of organizing thinking and providing study direction.
From the perspective of the critical thinking decision path outlined in Figure 4, theoretical
frameworks can be grand, midrange or micro-range theories. Whether the researcher is using a
conceptual or theoretical framework, conceptual and then operational definitions will emerge from the

framework. The decision path (Figure 4) moves down the ladder of abstraction from the philosophical
to the empirical level, tracking thinking from the most abstract to the least abstract for the purposes of
planning a research study.
Critiquing the framework
The framework for research provides guidance for the researcher as study questions are fine-
tuned, methods for measuring variables are selected and analyses are planned. Once data are collected
and analyzed, the framework is used as a base of comparison. Did the findings coincide with the
framework? If there were discrepancies, is there a way to explain them using the framework? The
critiquer of research needs to know how to critically appraise a framework for research (Framework
Critiquing Criteria box-end of chapter).
The first question posed is whether a framework is presented. Sometimes, there may be a
structure guiding the research but a diagrammed model is not included in the manuscript. The reader
must then look for the study structure in the narrative description of the study concepts. When the
framework is identified, it is important to consider its relevance for nursing. The framework doesn’t
have to be one created by a nurse but the importance of its content for nursing should be clear. The
question of how the framework depicts a structure congruent with nursing should be addressed. For
instance, although the Double ABC-X Model was not created by a nurse, it is clearly related to nursing
practice with families. Sometimes, frameworks from very different disciplines, such as physics or art,
may be relevant. It is the responsibility of the author to clearly articulate the meaning of the framework
for the study and to link the framework to nursing.
Once the meaning and nursing-relatedness are articulated, the critiquer will be able to determine
whether the framework is appropriate to guide the research. For instance, if a researcher is studying
students’ response to the stress of being in the clinical setting for the first time and presents a framework
of stress related to recovery from chronic illness….something is the matter. This is a blatant mismatch,
which generally won’t occur. However, subtle versions of mismatch will occur. So, the critiquer will
want to look closely at the framework to determine if it is “on target” and the “best fit” for the research
question and proposed study design.
Next, focus on the concepts being studied. Does the reader know which concepts are being
studied, how they are defined and translated into measurable variables? Is there literature to support the
choice of concepts? Concepts should clearly reflect the area of study; for example, using the general
concept of stress when anxiety is more appropriate to the research focus creates difficulties in defining

variables and determining methods of measurement. These issues have to do with the logical
consistency between the framework, the concepts being studied and the methods of measurement. All
along the way, from view of the world to operational definitions (Figure 4), the critiquer is evaluating
fit. Consider once more the paper by LoBiondo-Wood, Williams and Kouzekanani (2000) (Appendix
D). The authors provide a logically consistent link between the Double ABC-X Model of Family
Adaptation; the concepts diagrammed in the post-crisis phase of the model; and, the measures used to
address each concept. Finally, the critiquer will expect to find a discussion of the findings as they relate
to the model. This final point enables evaluation of the framework for use in further research. It may
suggest necessary changes to enhance the relevance of the framework for continuing work. So, it is a
place for letting others know where one will go from here.
Evaluating frameworks for research requires skill, which can only be acquired through repeated
critique and discussion with others who have critiqued the same manuscript. The novice critiquer of
research must be patient as these skills are developed. With continuing education and a broader
knowledge of potential frameworks, one builds a repertoire of knowledge to judge the foundation of a
research study….the framework for research.
nREFERENCES
Bull, MJ, Hanson, HE & Gross, CR: A professional-patient partnership model of discharge
planning with elders, Applied Nursing Research 13:19-28, 2000.
Chinn PL, Kramer MK: Theory and nursing: a systematic approach, ed 5, St Louis, 1999,
Mosby.
Cohen, MZ & Ley, CD: Bone marrow transplantation: The battle for hope in the face of fear.
Oncology Nursing Forum, In press.
Hamric, AB, Spross, JA & Hanson CM:Advanced Nursing Practice, Philadelphia, 2000,
Saunders.
Higgins, PA & Moore, SM: Levels of theoretical thinking in nursing, Nursing Outlook
48(4):179-183, 2000.
Im E. & Meleis AI: Situation-specific theories: Philosophical roots, properties and approach.
Advances in Nursing Science 22(2):11-24, 1999.
King IM: King’s theory of goal attainment in practice, Nursing Science Quarterly 10(4):180-
185, 1997.

Leininger, MM. Culture care theory. Nursing Science Quarterly 9(2):71-78, 1996.
Lenz, E: Middle range theory-Role in research and practice, In Proceedings of the sixth
Rosemary Ellis scholar’s retreat, Nursing science implications for the 21 st century. Cleveland Ohio:
Frances Payne Bolton School of Nursing, Case Western Reserve University, 1996.
Liehr, P: Prelude to research, Nursing Science Quarterly, 5(3):102-103, 1992.
Liehr P. & Smith MJ: Using story to guide nursing practice, International Journal of Human
Caring 4(2):13-18, 2000.
Liehr P. & Smith MJ: Middle range theory: Spinning research and practice to create knowledge
for the new millennium, Advances in Nursing Science 21(4):81-91, 1999.
LoBiondo-Wood, G, Williams, L & Kouzekanani K: Family adaptation to a child’s transplant:
Pretransplant phase, Progress in Transplantation, In press.
Mahon NE., Yarcheski, A & Yarcheski: TJ. Positive and negative outcomes of anger in early
adolescents, Research in Nursing and Health 23:17-24, 2000.
Merton RK: On sociological theories of the middle range. In Social Theory and Social Structure.
New York, 1968, Free Press.
Newman, MA: Evolution of the theory of health as expanding consciousness, Nursing Science
Quarterly 10(1):22-25, 1997.
Orem, DE: Nursing: Concepts of practice, ed 5, St. Louis, 1995, Mosby.
Parse, RR: Transforming research and practice with the human becoming theory, Nursing
Science Quarterly 10(4):171-174, 1997.
Rogers, ME: Nursing: Science of unitary, irreducible human beings: Update 1990. In E. Barrerr
(Ed). Visions of Rogers’ science-based nursing, New York, 1990, National League for Nursing.
Rogers, ME: Nightingale’s notes on nursing: Prelude to the 21st century, In Notes on nursing:
What it is and what it is not. Commemorative Ed. Philadelphia, 1992, Lippincott
Roy C. & Andrews HA: The Roy adaptation model: The definitive statement, Norwalk, 1991,
Appleton & Lange.
Smith, MJ & Liehr, P: Attentively embracing story: A middle range theory with practice and
research implications, Scholarly Inquiry for Nursing Practice 13(3):3-27,1999.

Table 1: Issues affecting BP change and related research questions
Issues Research questions
Number of people in patient’s room Is there a difference in BP for patients in CCU when interacting with one person as compared to interacting with two people or a group of three or more people?
Involvement of patient For the patient in CCU, what is the relationship between BP and the amount of time spent listening to the healthcare team’s discussion of personal qualities during routine rounds?
What is the effect of nurse-patient intentional dialogue on BP within the hour after the dialogue?
Continuing effect of experience on BP over the next hour
What is the BP pattern of patients in CCU from the beginning of routine healthcare rounds until 1 hour after the completion of rounds?
Content of dialogue What is the relationship between issues discussed during intentional dialogue and BP?
Meaning of experience for the patient What is the patient experience of being the object of routine healthcare rounds?
What is the patient experience of sharing what matters with a nurse while in the CCU?
BP: blood pressure
CCU: coronary care unit
Table 2 Concepts and Variables: Conceptual and Operational Definitions
Concept Conceptual Variable OperationalDefinition Definition
Trait anger Disposition of individuals to perceive a wide range of situations as frustrating or annoying, tending to respond to such situations with elevations in state anger. (p. 17)
Trait anger Spielberger Trait anger scale
10 items that assesses how angry one generally feels
State anger Emotional state marked by subjective feelings that vary in intensity from mild annoyance or irritation to intense fury and range (p. 17)
State anger Spielberger State anger scale
10 items that assesses how angry one is feeling right now

General well-being
Holistic, multidimensional construct incorporating mental/psychological, physical and social dimensions (p. 18)
General well-being
Short version of Adolescent General Well-Being questionnaire
39 items that assess the social, physical, and mental dimensions of well-being
Symptompatterns
Physical, psychological and psychosomatic patterns (p.18)
Symptompatterns
Symptom Pattern Scale
17 items that measure physical, psychological and psychosomatic manifestations of psychological distress
Vigor Mood or vigorousness, ebullience and high energy (p. 19)
Vigor-activity
Vigor-activity subscale of the Profile of Moods States
8 item adjective checklist used to measure vigor
Inclination to change
Seeking new and different experiences, readily changing opinions or values in different circumstances, and adapting readily to changes in the environment (p. 19)
Change Change subscale of the Personality Research Form-E
16 true-false items assessing inclination to change
Mahon, Yarcheski & Yarcheski, 2000
Table 3: Middle range theory by level of abstraction
High middle Middle middle Low middleCaring Uncertainty in illness Hazardous secrets and
reluctantly taking chargeFacilitating growth and development
Unpleasant symptoms Affiliated individuation as a mediator of stress
Interpersonal perceptual awareness
Chronic sorrow Women’s anger
Self-transcendence Peaceful end of life Nurse-midwifery careResilience Negotiating partnerships Acute pain managementPsychological adaptation Cultural brokering Balance between analgesia and
side effectsNurse expressed empathy and patient distress
Homelessness-helplessness
Individualized music intervention for agitationChronotherapeutic intervention for post-surgical pain
Liehr & Smith, 1999


Figure 1 Attentively Embracing Story
Connecting with Self-in-Relationpersonal history
reflective awareness
Creating Easere-membering disjointed story moments
flow in the midst of anchoring
Intentional Dialogue
true presencequerying emergence
PersonNurse