Embed Size (px)
Citation preview

Letrozole: mechanism of action
in infertility
October 2018

2
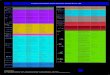
1. Product Information: Letrozole Denk 2.5
Indication Approval Patient type Dosage
Hormone receptor-positive breast cancer
Official Postmenopausal women
Initial dose: 2.5 mg/d orally
Anovulatoryinfertility
Off-label Women in reproductive age with PCOS, endometriosis and infertility conditions
2.5 mg/d for 5 days starting on menstrual cycle day 3Maximum: 7.5 mg/d

3
2. Natural ovarian cycle overview
1. The brain makes GnRH hormone in the hypothalamus.
2. GnRH is released in a special circulation going to the pituitarygland.
3. The pituitary gland releases two hormones FSH and LH.
4. These hormones travel in the blood stream to the ovary causing the ovary to produce an egg (follicle = single egg cell surrounded by multiple supporting cells).
5. The egg travels to the uterus and if fertilized will stay in the uterus OR, if not, the egg is shed and the women will have a normal menstrual period.
Important hormones in the ovarian cycle:- Gonadotropin releasing Hormone (GnRH) → hypothalamus- Lutenizing Hormone (LH) → pituitary gland- Follicle Stimulating Hormone (FSH) → pituitary gland- Estrogen → ovaries- Progesterone → ovaries
Hypothalamus
Pituitary gland
Ovary
Uterus
Estrogen+ Progesterone
GnRH
FSH + LH
Posi
tive
fee
db
ack N
egative feed
back

4
3. Key events in the ovarian cycle (1)
FOLLICULAR PHASE
1. Follicle is stimulated by FSH to develop.
2. The dominant follicle starts to release estrogen.
3. Estrogen has a negative feedback at the pituitary gland → slowing the release of FSH and LH → prevents other follicles growing.
4. Estrogen impact the uterus → increase thickening and vascularization preparing for potential embryo implantation.
OVULATION
1. As the follicle continues to develop, estrogen levels continue to rise.
2. A Positive feedback on hypothalamus → increase release of GnRH → rapid ↑ of FSH and LH release from the pituitary.
3. LH stimulates the developing follicle to release an egg in the ovary (ovulation). The tissue where the egg develops is known as Corpus Luteum.
Adapted from http://ib.bioninja.com.au/standard-level/topic-6-human-physiology/66-hormones-homeostasis-and/menstrual-cycle.html
Menstruation Proliferative Secretory Phases

5
3. Key events in the ovarian cycle (2)
LUTEAL PHASE
1. The Corpus Luteum produces estrogen and progesterone → negative feedback on pituitary and hypothalamus → ↓ production of FSH and LH.
2. Estrogen and progesterone act on the uterus → thicken the endometrial lining in preparation for pregnancy.
MENSTRUATION
1. If fertilization occurs, the developing embryo will implant in the endometrium and release hormones to sustain the Corpus Luteum.
2. If fertilization does not occur, the Corpus Luteum degenerates, levels of estrogens and progesterone ↓ and the endometrial layer is sloughed (menstruation)
Adapted from http://ib.bioninja.com.au/standard-level/topic-6-human-physiology/66-hormones-homeostasis-and/menstrual-cycle.html
Menstruation Proliferative Secretory Phases

6
4. What is PCOS? (1)
ESHRE/ASRM. Hum Reprod 2008;23:462–477.Balen et al., Human Reproduction Update, Vol.22, No.6 pp. 687–708, 2016Teede et al., Fertility and Sterility® Vol. 110, No. 3, August 2018 0015-0282http://www.pcos.org/
Polycystic ovary syndrome (PCOS), or Stein-Leventhal Syndrome, is the most common hormonal, genetic, metabolic and reproductive disorder in women and accounts for 80% of women with anovulatory infertility.
WHAT HAPPENS:• The brain does not produce GnRH in normal
cycles, but in rapidly interrupted manner• Causes LH levels to rise ↑, FSH levels drop ↓• LH causes ovary to produce more
testosterone/androgens• Ovary is unable to produce an egg = ovulation
inhibited
SOME FACTS:• 1-in-10 women are affected by PCOS• 3x increased risk of women with PCOS to develop
diabetes, stroke, heart disease and endometrial cancer
• 2x increased risk of anxiety, depression and drug use
WHAT IT IS:• It is an imbalance of hormones• Ovaries may develop cysts

7
4. What is PCOS? (2)
Balen et al., Human Reproduction Update, Vol.22, No.6 pp. 687–708, 2016Teede et al., Fertility and Sterility® Vol. 110, No. 3, August 2018 0015-0282
PCOS MAIN SYMPTOMSOccur often, but not always
1 Weight gain
2 Irregular Menstrual cycle
3 Unwanted hair growth
PCOS CAUSESCaused by several hormonal disorder
1 Genetic factors
2 Cysts in Ovaries
3 Lack of Hormone levels
4 Anxiety & Depression

5. Assessment and management of OI in PCOS
OI = anovulatory infertility
Balen et al., Human Reproduction Update, Vol.22, No.6 pp. 687–708, 2016
Appropriate assessment and treatment of PCOS are important for helping the patients.

6. Mechanism of action: Clomiphene C
Adapted from Paloma S., J Clin Endocrinol Metab, May 2015, 100(5):1742–1747
*Selective estrogen receptor modulators (SERMs)
3
1. Binding of CC to the estrogen receptor (ERs) in the reproductive system and, more importantly, in the hypothalamus → depletion of receptor concentration.
2. Interference with negative feedback effect of estradiol: Levels of estrogen are falsely perceived as low.
3. GnRH release from pituitary gland more pulsatile.
4. Increased and prolonged secretion of FSH and LH.
5. Ovarian follicle maturation.6. Ovulation induction
2
4
6. Ovulation induction
5
1

7. Mechanism of action: Letrozole Denk
6. Ovulation induction
*Aromatase inhibitor (AIs)
Adapted from Paloma S., J Clin Endocrinol Metab, May 2015, 100(5):1742–1747
3 1. Blockage of the conversion of androgens to estrogens.
2. Acute hypoestrogenic state: Levels of estrogen are low.
3. Hypothalamic-pituitary axis from the estrogenic negative feedback: GnRH release from pituitary gland more pulsatile.
4. Increased and prolonged secretion of FSH and LH.
5. Ovarian follicle maturation → monofollicular growth.
6. Ovulation induction
1
2
4
5

8. Fast facts: Letrozole Denk vs. CC (1)
Mechanism of action Letrozole and CC:

12
8. Fast facts: Letrozole Denk vs. CC (2)
Key facts about Letrozole:
Approved by FDA as one of the first-line adjuvant therapies for estrogen-receptor-positive breast cancer.
Off-label use for anovulatory infertility (2.5 mg daily for 5 days in the early proliferative phase, generally from day 3 of menses).
Controlled and uncontrolled studies have reported ovulation and pregnancyrates of 50-90% and of 10%-40%, respectively.
Aromatase inhibitors (AIs) can be more or equally efficient than CC and with less implications on the safety after prolonged and consecutive treatments. → AIs have short half-lives (ca. 45h) → less adverse effects for estrogentarget tissues (such as endometrium).
Clomiphene citrate (CC - dosage from 150 mg/d) successfully inducesovulation in 60–80% of PCOS patients (cumulative ovulation rate ca. 50%) and live-birth rate of about 30%.

13
9. Clomiphene Citrate resistance
Clomiphene citrate (CC) resistance is defined as failure to ovulate after receiving 150 mg of CC daily for 5 days per cycle, for at least 3 cycles.
CC resistance is common and occurs in approximately 15-40% women with PCOS.
Insulin resistance, hyperandrogenemia and obesity are the major factors involved in CC resistance and prevent the ovary responding to raise FSH levels following CC therapy.
Aromatase inhibitors were originally used to improve pregnancy rate and limit adverse events, especially with CC resistance.
One RTCs on 147 women with CC resistance found that letrozole was better than laparoscopic ovarian surgery for ovulation rate per cycle.
http://pcos-cre.edu.au/wp-content/uploads/2018/02/PCOS-guideline_MASTER_05022018_7-1.pdfHashim HA, www.intechopen.com DOI: 10.5772/27856

10. Metformin Denk: an alternative
Metformin Denk is an insulin-lowering drug and improves insulin action and anovulation → off-label use for ovulation induction.
Metformin treatment alone or in combination with clomiphene was shown not to be superior to clomiphene alone. However, it might be used as an alternative to first –line drugs in specific clinical situations (e.g. contraindication to those agent).
Dosage: 500 mg/d during the main meal and up to 2000 mg/d

15
11. Guidelines recommendations (1)
Abbreviations:EBR- Evidence-based recommendations are made where evidence is sufficient to inform a recommendation made by the guideline development group.CCR - Clinical consensus recommendations are made in the absence of adequate evidence on PCOS. These are informed by evidence in other populations and are made by the guideline development group, using rigorous and transparent processes.CPP - Clinical practice points are made where evidence was not sought and are made where important clinical issues arose from discussion of evidence-based or clinicalconsensus recommendations.
http://pcos-cre.edu.au/wp-content/uploads/2018/02/PCOS-guideline_MASTER_05022018_7-1.pdfTeede et al., Fertility and Sterility® Vol. 110, No. 3, August 2018 0015-0282
2018 update: 1st internationally endorsed and evidence-based guidelines, developed by the Centre for Excellence in PCOS research in partnership with the European Society of Human Reproduction and Embryology (ESHRE) and American Society of Reproductive Medicine (ASRM).
Letrozole

16
11. Guidelines recommendations (2)
2018 update: 1st internationally endorsed and evidence-based guidelines
http://pcos-cre.edu.au/wp-content/uploads/2018/02/PCOS-guideline_MASTER_05022018_7-1.pdfTeede et al., Fertility and Sterility® Vol. 110, No. 3, August 2018 0015-0282
CC/Metformin

17
11. Guidelines recommendations (3)
http://pcos-cre.edu.au/wp-content/uploads/2018/02/PCOS-guideline_MASTER_05022018_7-1.pdfWang et al., BMJ 2017;356:j138 | doi: 10.1136/bmj.j138
2016 following WHO group classification: summary of previous recommendations for the treatment of PCOS.
RCTs/studies: 13 RCTs compared letrozole with CC. 7of these RCTs had a high risk of bias, 2 had a moderate risk of bias and 4 had a low risk of bias. Upon meta-analysis, letrozole was better than clomiphene citrate for ovulation rate per patient, pregnancy rate per patient and live birth rate per patient.

18
12. What else can you do?
Antioxidant supplementation has been shown to improve insulin sensitivity and restore redox balance in women with PCOS‡ → optimal antioxidant intake might improve female fertility and full-term pregnancy outcomes.
‡Sekhon LH. et al., Female Infertility and Antioxidants. Current Women’s Health Reviews (2010), 6, 84-95.
Blister pack
Appearance Shelf life
Pack size
Capsules Shiny capsules 2 years 60 caps
fertilo lady Denk is a well-thought-out food supplement. It is a potent combination of vitamin C, vitamin B6, folate, vitamin B12, iron, zinc, Iodine, Acai berry extract and L-arginine that supports an healthy life style and nutritional habits. It can impact women fertility.
Note: Food supplements do not treat, diagnose or cure diseases. They supplement the normal diet and correct mild nutritional deficits or maintain an adequate intake of certain nutrients. We recommend physicians to choose individual therapies for their patients and weigh possible interactions with the APIs in our products.

DENK PHARMA GmbH & Co. KG | Prinzregentenstrasse 79 | 81675 Munich | www.denkpharma.de | Germany