Embed Size (px)
Citation preview

Lessons learned Integrating PMTCT, HIV Care and ART
Track 1.0 ART Program MeetingSeptember 25, 2007
Dr Lulu Oguda
Senior Medical Officer
Elizabeth Glaser Pediatric AIDS Foundation

EGPAF PMTCT Program ResultsCumulative data, 2000 – June 2007
0
500000
1000000
1500000
2000000
2500000
3000000
3500000
4000000
4500000
Eligiblew omen
Counseled Tested Results HIV+ WomenARV
Infant ARV

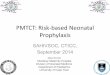
Project HEART: Patient Enrollment1
269,649
226,227
189,820
167,401
134,426117,996
96,37079,706
41,88531,337
15,039
142,249
20,84936,712
45,56157,882 68,536
86,69697,870
117,203
0
50,000
100,000
150,000
200,000
250,000
300,000
Q1-05 Q2-05 Q3-05 Q4-05 Q1-06 Q2-06 Q3-06 Q4-06 Q1-07 Q2-07
Cumulative Number on HIV Care
Cumulative Number on ART
30
36
56
73
92
94
119
144
163
183
1. CUMULATIVE data by June 30, 2007
2. Boxed numbers indicate the number of active sites each quarter

PMTCT and C&T sites: Project HEART Countries
Country #PMTCT sites only
# only C&T sites
# sites with both services
Total # sites
CI 72 36 37 145
Moz 14 4 15 33
SA 19 3 30 52
Tz 285 11 27 323
ZA 148 14 32 194

EGPAF Approach to Integrating PMTCT, HIV Care and ART
• Practice differs across countries• In most instances, HIV +ve pregnant women identified through ANC
and referred for PMTCT.• Number of women identified though HIV Care and the ART clinics
not well documented.• Estimated pregnancy rate in ART clinics in Zambia in 2006 = 4 /per
woman-year.• Pregnant women in HIV Care and on ART sent to nearest health
facility offering ANC• Adaptation of ART and other meds done as appropriate in ART
clinics• SA and CI offer both clinical screening and urine tests for pregnancy
[if clinically indicated] in ART clinics• Preconception care and counseling not routinely offered at the sites• CI, SA and TZ and ZA have established coding system that allow for
linking of mother-infant data from ANC/PMTCT to C&T

PMTCT Addendum A Indicators
Number of (see below) Identified as HIV+ Through PMTCT Enrolled in Care and Treatment Program – Pregnant Women– Pregnant Girls (14 and younger)– Non-Pregnant Women (15 and older)– Adult Men (15 and older)– Female Children (0-14 years old)– Male Children (0-14 years old)Number of (see below) Identified as HIV+ Through PMTCT
Receiving HAART– Pregnant Women (15 and older)– Pregnant Girls (14 and younger)– Non-Pregnant Women (15 and older)– Adult Men (15 and older)– Female Children (0-14 years old)– Male Children (0-14 years old)

Number of HIV+ pregnant women initiating ART : Project HEART countries
[PMTCT Reported Data]
Country 2005 2006 Q1 2007
Cote d’Ivoire 10 111 68
Mozambique 5 195 196
South Africa 64 183 205
Tanzania 43 528 449
Zambia NA 238 1010

Number of HIV-exposed infants initiating Cotrimoxazole prophylaxis at 6 weeks
of age : Project HEART countries [PMTCT Reported Data]
Country 2005 2006 Q1 2007
Cote d’Ivoire 123 203 189
Mozambique 183 1612 878
South Africa 663 337 454
Tanzania 779 942 512
Zambia NA 3040 1523

Number of HIV exposed infants tested for HIV : Project HEART countries
[PMTCT Reported Data]
Country 2005 2006 Q1 2007
Cote d’Ivoire 124 364 154
Mozambique NA 48 28
South Africa 642 1394 1669
Tanzania 209 314 131
Zambia NA 476 871

Number of HIV + infants identifiedProject HEART countries
[PMTCT Reported Data]
Country 2005 2006 Q1 2007
Cote d’Ivoire 19 51 12
Mozambique NA 10 16
South Africa 56 114 261
Tanzania 25 54 20
Zambia NA 131 276

Models of Integrated Service Delivery: Tanzania
• Specific project seeking to expand care and identification for children through increased identification of infants and strengthened linkages between PMTCT and C&T through:– PITC– Training – Active referral of HIV-positive children to CTC– Active follow-up of HIV-exposed children in community for 2y
with CTX prophylaxis• Implementation began in April 2007 at 2 hospitals –
Huruma and Mawenzi• Baseline data gathering and sensitization done• PITC introduced at RCH, general OPD clinics and IPD

Models of Integrated Service Delivery: Tanzania
Quantitative Summary – Huruma & Mawenzi Apr-Jun 2007
#
peds
tested
In PITC
# HIV
expose
#HIV
infected
# in HIV care
#
Mother
tested
#
Mother
positive
# Mother
in HIV
Care
572 36 43 47 22 3 3

Models of Integrated Service Delivery: Swaziland
• KSII PHU – • Initiated as partnership with ICAP and AED• Busiest primary care facility in Manzini. Referral facility
for 15 clinics. One of the 3 initial sites where EGPAF began support for PMTCT in 2004
• Counseling and Testing offered to all and referral to RFM hospital for ART[RFM = Raleigh Fitkin Memorial]
• C&T services began to be offered in Feb 2007. Reasons included:– Referral were ineffective– Self-selection of pregnant women– Change in counselors at the different ART site

Models of Integrated Service Delivery: Swaziland
• KSII first site to provide one-stop shop’ PMTCT service in Swaziland.
• Luyengo clinic introduced the services of a physician-led ART team in PMTCT clinic fortnightly in 2007
• Pigg’s Peak PHU began HIV Care and ART services in 2004 and introduced PMTCT in 2006. ART physician supervises the PMTCT clinic enhancing clinical care

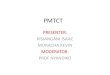
Models of Integrated Service Delivery: Swaziland
Data Summary Jan-June 2007
709
215184
775
18396
1441
14811757 26 21
0
200
400
600
800
1000
1200
1400
1600
Number ofpregnantwomen
testing HIV+
CD4 cellcount done
Individualsstarted onCTX (care)
Pregnantwomen
started onHAART
Data Summary Jan- June 2007
KSII PHU
LUYENGO CLINIC
PIGG'S PEAK PHU

Issues to Address
• Indicators to capture integration between PMTCT, HIV care and ART not well developed.
• ‘Artificial’ divide between services → HIV Care, ART & PMTCT and RH services– Funding streams– Data reporting mechanisms – Emphasis on specialization not realistic where the NO and MO =
GP perform most tasks• History of ANC Care in HIV Care and ART clinics
– Traditionally housed in MCH/RCH unit of the facility– PMTCT generally provided at PHC level, ART at secondary or
tertiary centers– ANC care not provided as part of HIV Care & Treatment
package

Issues to Address
• Host government policies and clinical guidelines– Incomplete guidelines on preconception care, prenatal care in
ART or HIV palliative care clinic.– Unclear until what point PMTCT clinic should provide
longitudinal follow-up of the mother-infant pair
• Infant diagnosis– Dependency on DNA PCR– Presumptive diagnosis and use of Ab tests– Symptomatic infants not routinely offered Ab test– Aggregate number includes infants tested at other sites and
referred for care. – Difficult to ascertain transmission rates from the data available.

Issues to Address
• Different data sources for individual patients – Medical records, Registers etc
• Data source and reporting mechanism may not be at the same site or within the same service
• Linkage of data between HIV-exposed infants in HIV Care and mothers from PMTCT poor due to paucity of data

EGPAF Strategies for Integration
To optimize outcomes for patients 1. Link women and children identified in PMTCT to longitudinal C&T
1. a. Infant and Child Diagnosis2. b. Increase Infant and Child C&T
2. Link women in C&T to PMTCT
1. Increase # women receiving PMTCT from C&T
3. Strengthen Family Focus of C&T and PMTCT
• CoC Task Force established in 2006, framework created• CoC TWG appointed in 2007

EGPAF Strategies for Integration
Proposed Indicators: Care & Treatment
• Number of HIV positive women enrolled in HIV care and/or treatment that were referred from a PMTCT program
• Number of HIV-exposed children less than 2 years old enrolled in HIV care and/or treatment who were referred from a PMTCT program
• Number of HIV-exposed infants in C&T that have received an HIV Test
• Number of women in HIV care and/or treatment newly identified as pregnant and enrolled in ANC providing PMTCT services

EGPAF Strategies for Integration
Proposed Indicators: PMTCT
• Number of HIV positive women referred from PMTCT program and enrolled in HIV care and/or treatment programs
• Number of HIV positive women referred from PMTCT program that have been clinically staged for HIV illness
• Number of HIV positive women referred from PMTCT program that have had a CD4 assessment
• Number of HIV-exposed infants less than 8 weeks old identified by PMTCT program and enrolled in care and/or treatment programs
• Number of HIV-exposed infants identified by PMTCT program initiating Cotrimoxazole prophylaxis

EGPAF Strategies for Integration
Indicator Pilot StudiesPhase I
– October 2007 – Analysis of Data Sources – Mozambique, Zimbabwe
Phase II– Early 2008 – Propose denominators and refine indicators, based on Phase I– Pilot Implementation of refined indicators– 8 Countries 2008
Phase III– Mid 2008 – All EGPAF-Supported Countries