Embed Size (px)
Citation preview
Les HypnotiquesLes Hypnotiques
Luc Barvais, MD PhDLuc Barvais, MD PhD
[email protected]@ulb.ac.be
Thiopental, Etomidate, (Ketamine), Propofol
AIVOC = Anesthésie Intraveineuse Objectif Concentration
Simulation pharmacocinétiqueTIVA TRAINER
ThiopentalThiopental
Barbiturique synthétisé en 1935 ; Hypnotique pur
Forte liposolubilité, lié albumine (85-90% et 100% à pH 7.8)
Métabolisation hépatique (CYT P450) avec clairance basse: 2 à 4 ml/kg/min = coefficient extraction de ± 10% élimination indépendante du flux sang hépatique
Induction: bolus 3 à 7 mg/kg mais ↓ doses avec l’âge.Dose à calculer en fonction poids maigre
ThiopentalThiopental
Effet niveau SNC essentiellement sur récepteur GABA (neurotransmetteur inhibiteur).
↓ consommation O2 cérébrale et ↓ débit sanguin cérébral ↓volume et pression intracanienne
Effets hémodynamiques par effet inotrope – et ↓ précharge
ThiopentalThiopental
Pas d’allergie
Pas douloureux si concentration < 2.5%
Contre indication = porphyrie aigue
Indication 2010: coma barbiturique pré ischémie cérébrale?= 10 mg/kg en 20 minutes suivi perfusion: 1 à 5 mg/kg/heure
EtomidateEtomidate
dérivé imidazolé éthylcarboxylé, sans structure apparentée aux autres anesthésiques
Instable en solution aqueuse =solution à 2%, dans du propylène glycol à 35% ou solution lipidique (Etomidate, Lipuro, B Braun)
Osmolalité élevée douleurs fréquentes lors de l’injection dans des veines de petit calibre.
EtomidateEtomidate
T1/2 varie de 3 à 5 heures (retour lent < Vdss large)
Clairance hépatique > 90% du débit sanguin hépatique
0,2 à 0,3 mg.kg-1 taux plasmatiques entre 300 et 600 ng/ml assurant l’inconscience pendant 5 à 15 minutes, lorsque l’étomidate est le seul hypnotique utilisé
Ampoule= 20 mg / 10 ml
EtomidateEtomidate
Dépression respiratoire < propofol (↓ VC + ↑ FR)Induction peut s’accompagner hoquet et toux (20%)
Myoclonies (50 à 80% si étomidate seul) = perte de l’inhibition des structures sous-corticales sur l’activité motrice extrapyramidale
Inhibition enzyme 11 hydroxylase intervenant dans la synthèse du cortisol et de l’aldostérone au niveau de la corticosurrénale persistant jusque à 24h.
EtomidateEtomidate
Hypnosédatif intraveineux d’action rapide et brève
Provoque moins de dépression cardiovasculaire et respiratoire que ses analogues
Dépourvu d’effet analgésique
Indiqué chez le patient atopique
Diminue PIC et consommation cérébrale en oxygène
Choix raisonnable pour intubation milieu extrahospitalier
Inhibe la synthèse de corticoïdes et donc déconseillé en perfusion continue
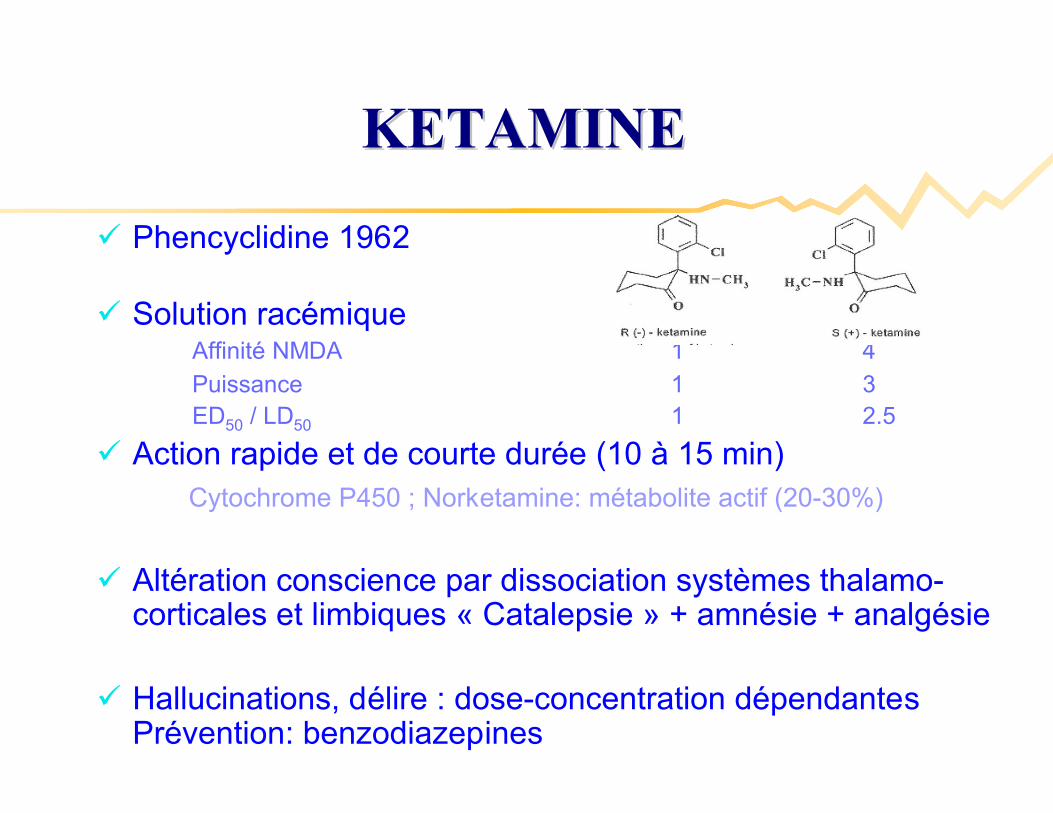
Phencyclidine 1962
Solution racémiqueAffinité NMDA 1 4
Puissance 1 3ED50 / LD50 1 2.5
Action rapide et de courte durée (10 à 15 min)Cytochrome P450 ; Norketamine: métabolite actif (20-30%)
Altération conscience par dissociation systèmes thalamo-corticales et limbiques « Catalepsie » + amnésie + analgésie
Hallucinations, délire : dose-concentration dépendantesPrévention: benzodiazepines
KETAMINEKETAMINE
KETAMINE: mKETAMINE: méécanismes dcanismes d’’actionaction
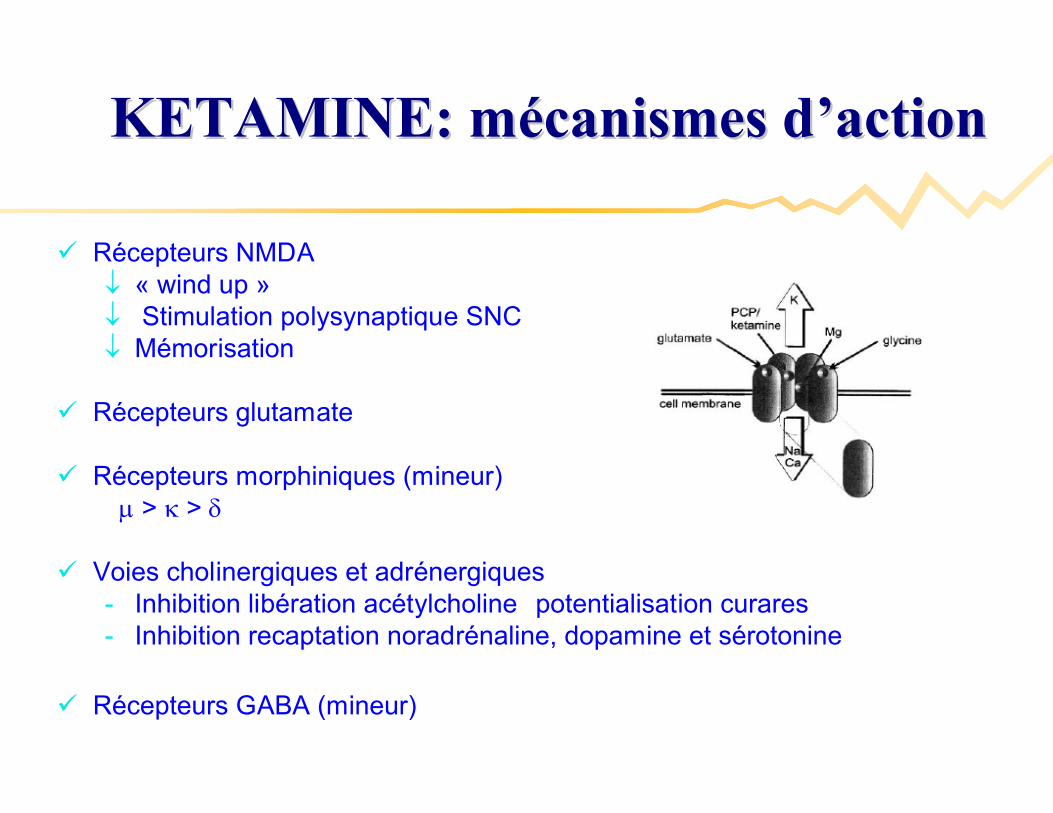
Récepteurs NMDA « wind up » Stimulation polysynaptique SNC Mémorisation
Récepteurs glutamate
Récepteurs morphiniques (mineur) > >
Voies cholinergiques et adrénergiques- Inhibition libération acétylcholine potentialisation curares- Inhibition recaptation noradrénaline, dopamine et sérotonine
Récepteurs GABA (mineur)
KETAMINE : mode administrationKETAMINE : mode administration
Anesthésie IV- Induction 1-2mg.kg-1
- Maintenance 10 – 90 g.kg-1.min-1
- AIVOC analgésique 0.2 – 0.5 g.ml-1 (Biais: 20%)- AIVOC hypnotique 0.6 – 1.3 g.ml-1
Anesthésie IM5 -10 mg.kg-1 ; durée ± 30-45 min ; Biodisponibilité 90%
Anesthésie IR 8-15 mg.kg-1 Biodisponibilité 25%
PHARMACOLOGIE KETAMINEPHARMACOLOGIE KETAMINE
Dépression de la fonction du myocarde S(-) > S(+)
Stimulation système sympathique: adrénergique- Tachycardie- Hypertension, débit cardiaque, ou = RVP, PVC, ou= PAP et RVPulm
- débit coronaire consommation O2
- Prévention avec BZD et 2-agonistes
Stabilité hémodynamique en chirurgie et cathétérismes cardiaques en pédiatrie
PROPOFOLPROPOFOL
2,6-di-isopropylphénol
1ère administration chez l’homme en 1977 en BelgiquDevenu (crémophor)
Peu soluble dans l’eau solvant lipidique à base de Soja
Devenu agent d’induction de référence
Agent de sédation pour endoscopie, USI, …
Douleur injection!!
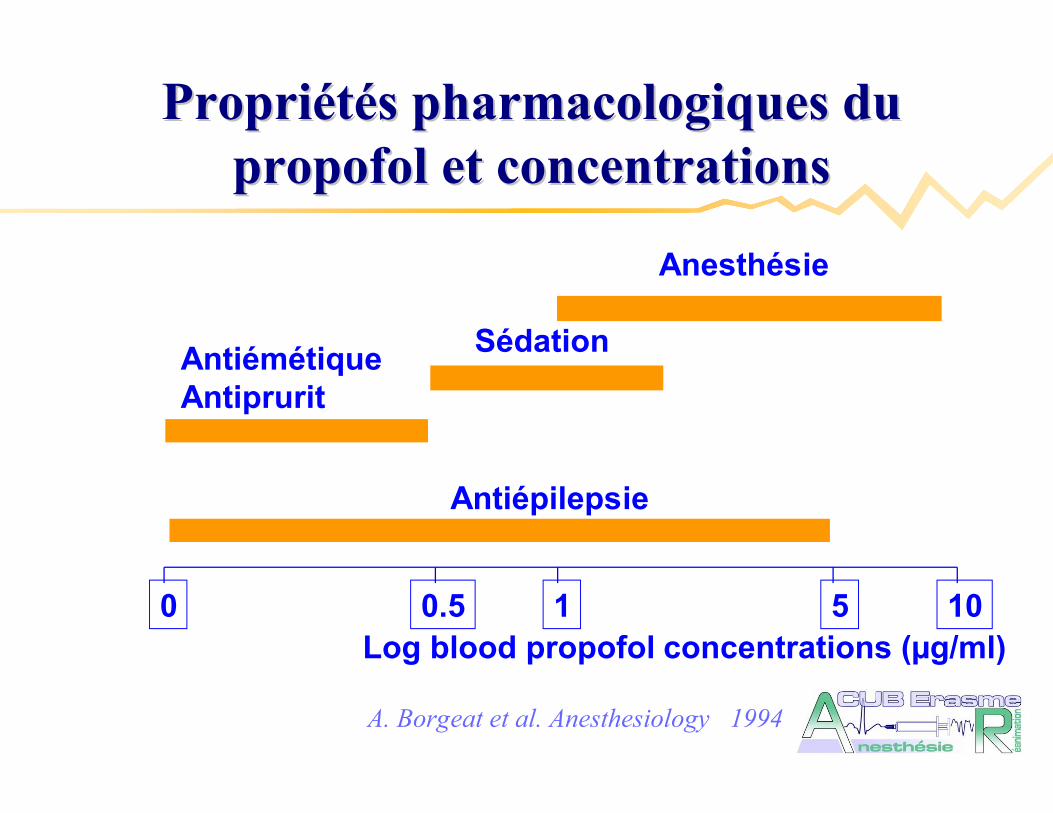
PropriPropriééttéés pharmacologiques dus pharmacologiques dupropofol et concentrations propofol et concentrations
0 0.5 1 5 10
Antiépilepsie
AntiémétiqueAntiprurit
Sédation
Anesthésie
Log blood propofol concentrations (µg/ml)
A. Borgeat et al. Anesthesiology 1994
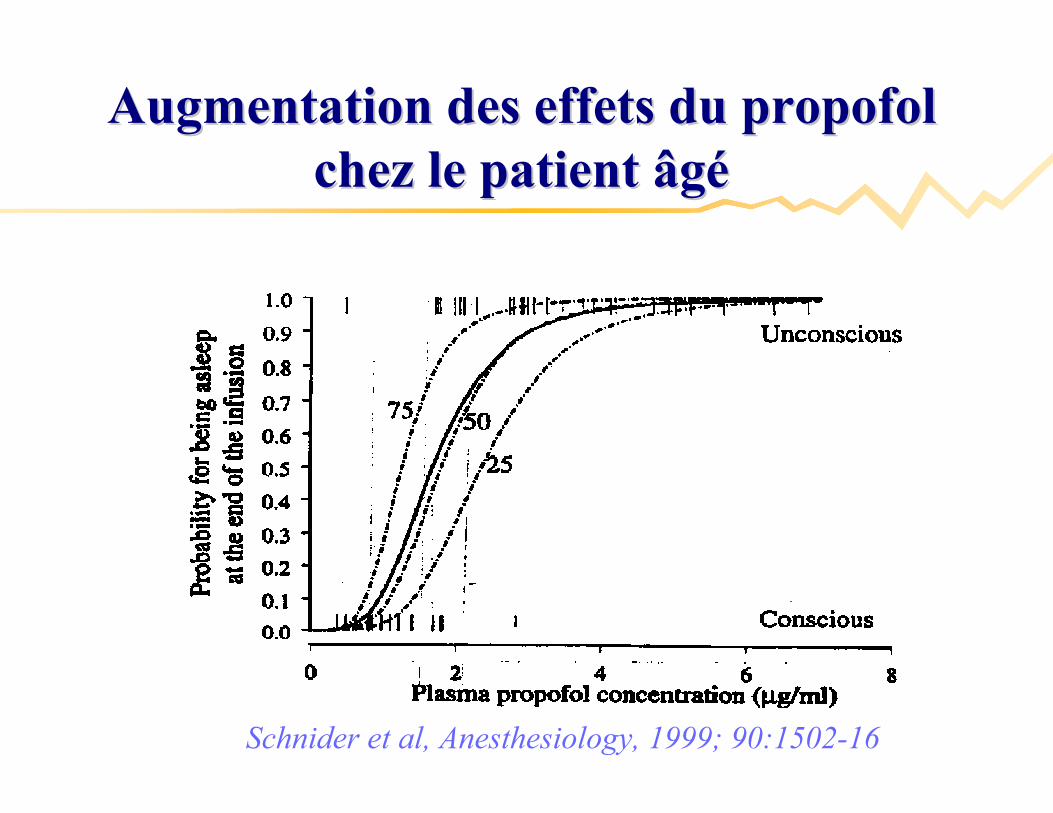
Augmentation des effets du propofol Augmentation des effets du propofol chez le patient âgchez le patient âgéé
Schnider et al, Anesthesiology, 1999; 90:1502-16
Plasma TCI : 1 to 12 µg/ml stable during 30 min
41 patients: - Group 1: 20-39 yr- Group 2: 40-59 yr- Group 3: 60-69 yr- Group 4: 70-85 yr
Kazama et al, Anesthesiology, 1999; 90: 1517Kazama et al, Anesthesiology, 1999; 90: 1517--2727
Comparison of the effect site keos of propofol for Comparison of the effect site keos of propofol for BISBIS and and blood pressure in elderly and younger patientsblood pressure in elderly and younger patients
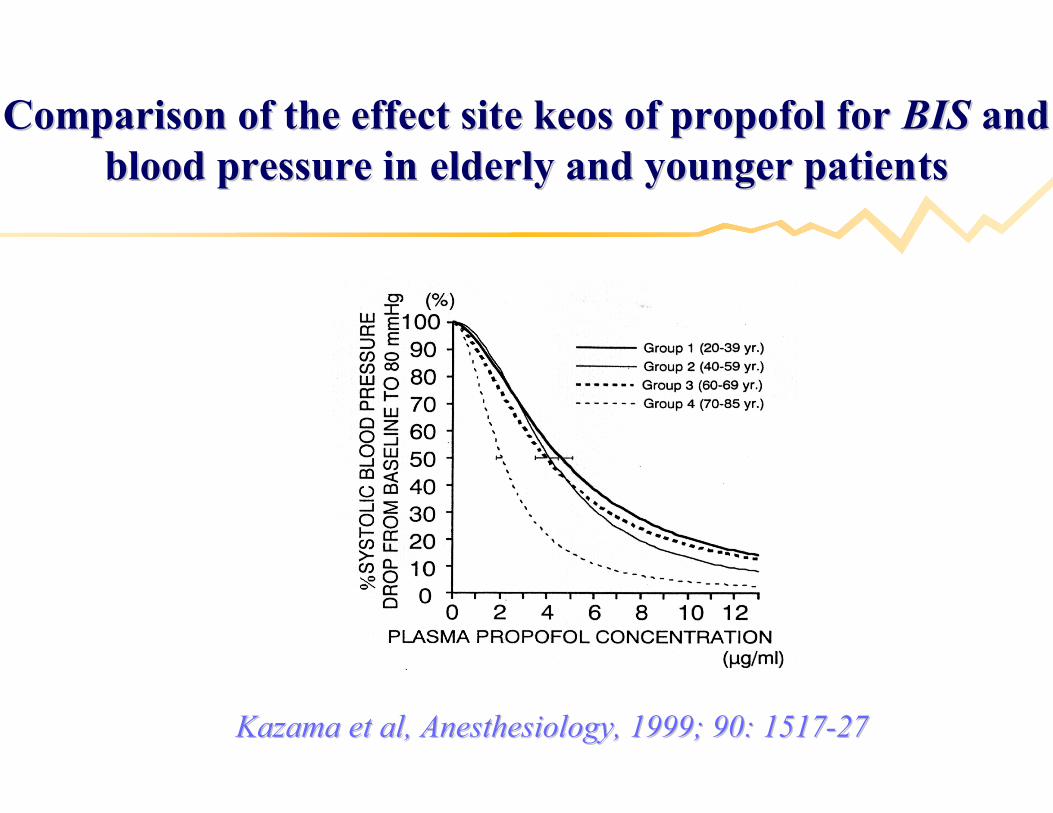
Kazama et al, Anesthesiology, 1999; 90: 1517Kazama et al, Anesthesiology, 1999; 90: 1517--2727
Comparison of the effect site keos of propofol for Comparison of the effect site keos of propofol for BISBIS and and blood pressure in elderly and younger patientsblood pressure in elderly and younger patients
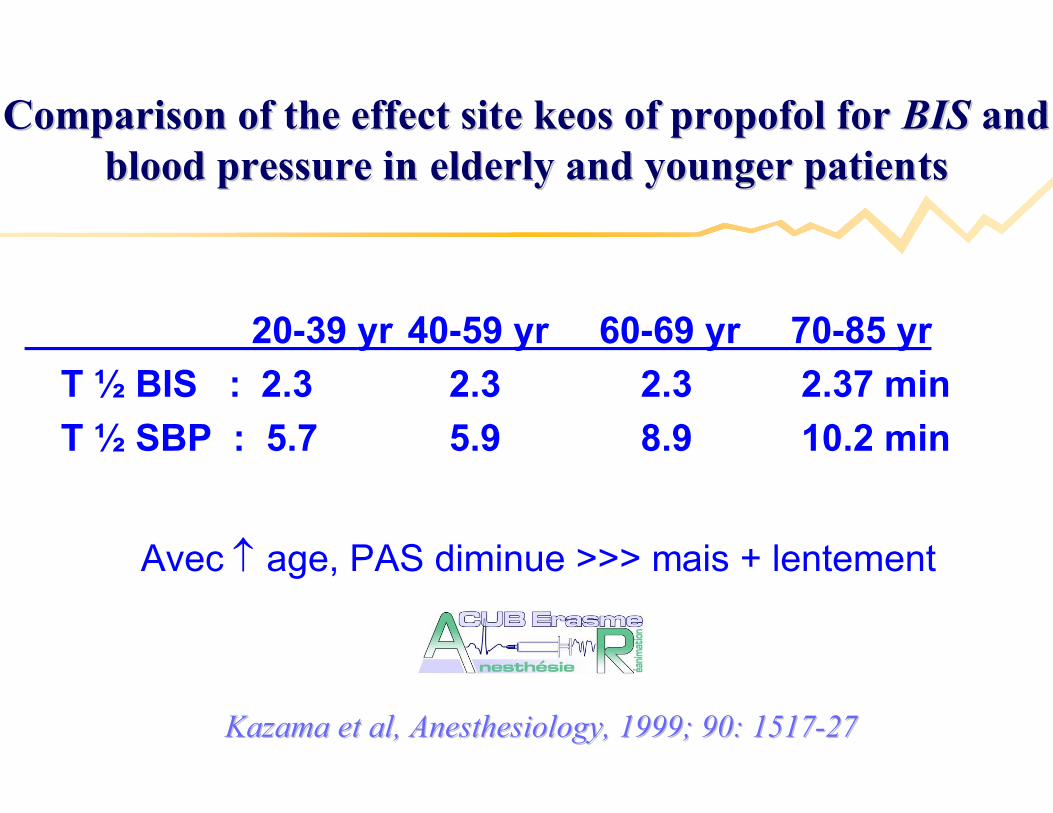
20-39 yr 40-59 yr 60-69 yr 70-85 yr
T ½ BIS : 2.3 2.3 2.3 2.37 min
T ½ SBP : 5.7 5.9 8.9 10.2 min
Avec age, PAS diminue >>> mais + lentement
Kazama et al, Anesthesiology, 1999; 90: 1517Kazama et al, Anesthesiology, 1999; 90: 1517--2727
Comparison of the effect site keos of propofol for Comparison of the effect site keos of propofol for BISBIS and and blood pressure in elderly and younger patientsblood pressure in elderly and younger patients

DDéébut but actionaction
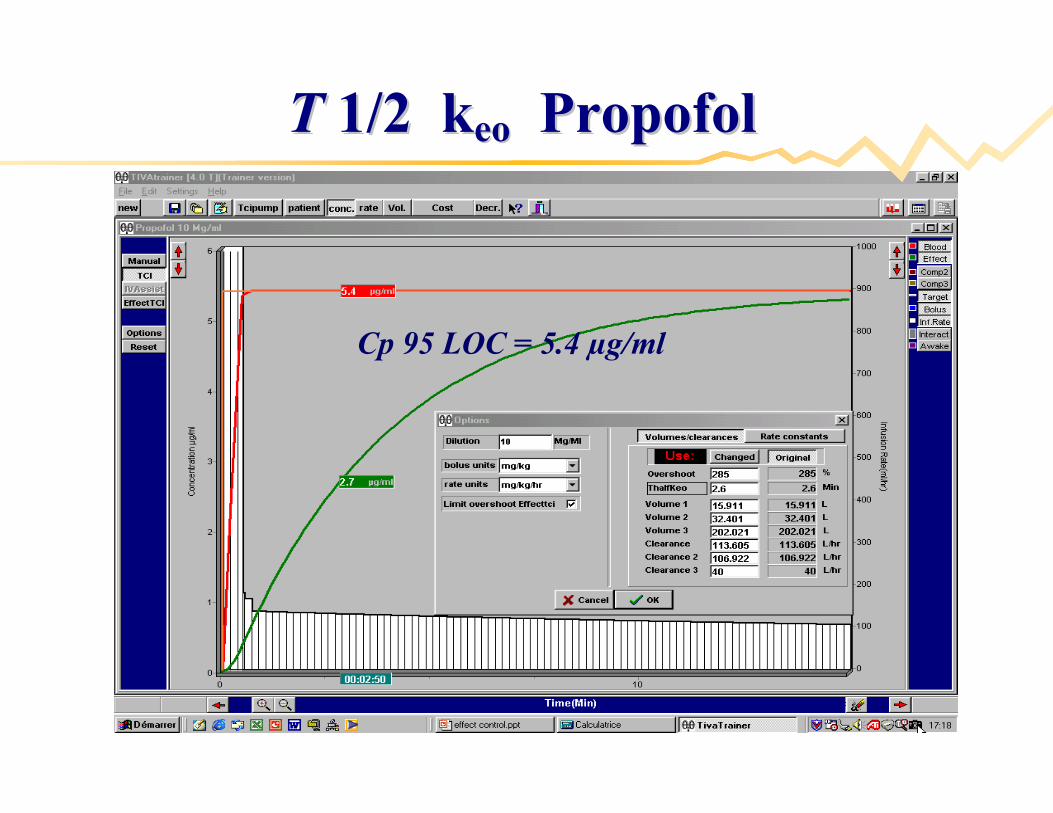
TT 1/2 k1/2 keo eo PropofolPropofol
Cp 95 LOC = 5.4 µg/ml
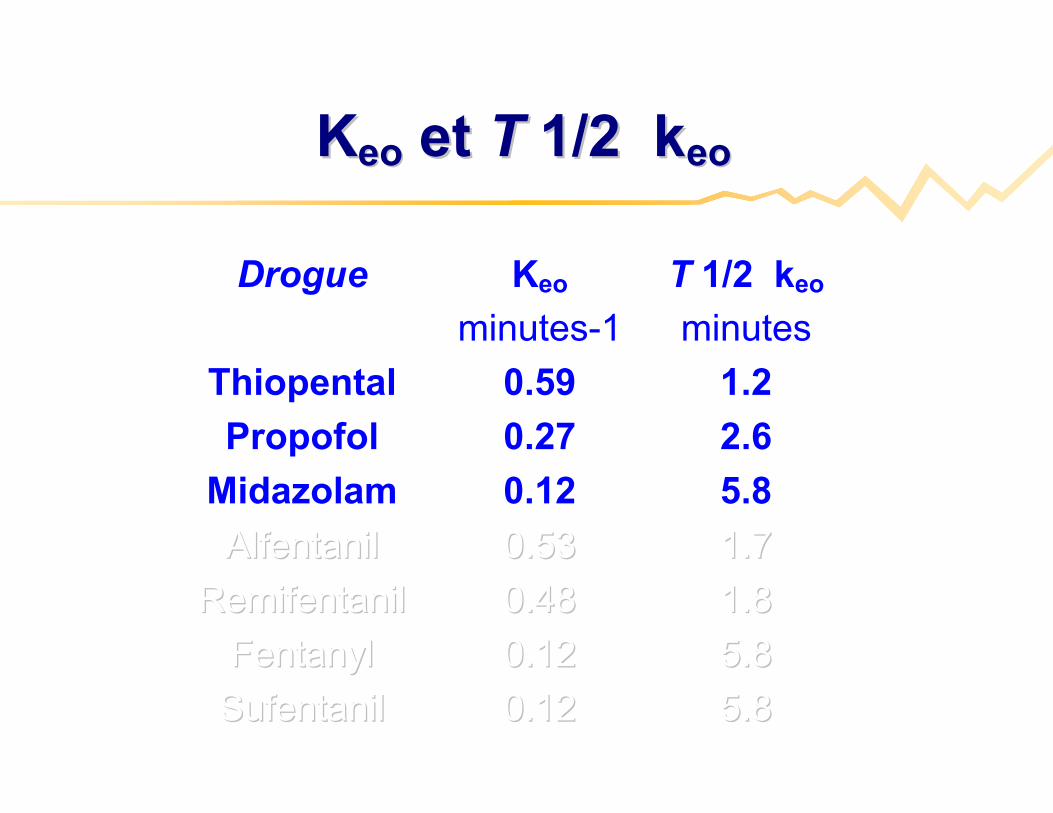
Drogue Keo
minutes-1
T 1/2 keo
minutes
Thiopental 0.59 1.2
Propofol 0.27 2.6
Midazolam 0.12 5.8
AlfentanilAlfentanil 0.530.53 1.71.7
RemifentanilRemifentanil 0.480.48 1.81.8
FentanylFentanyl 0.120.12 5.85.8
SufentanilSufentanil 0.120.12 5.85.8
KKeoeo et et TT 1/2 k1/2 keo eo
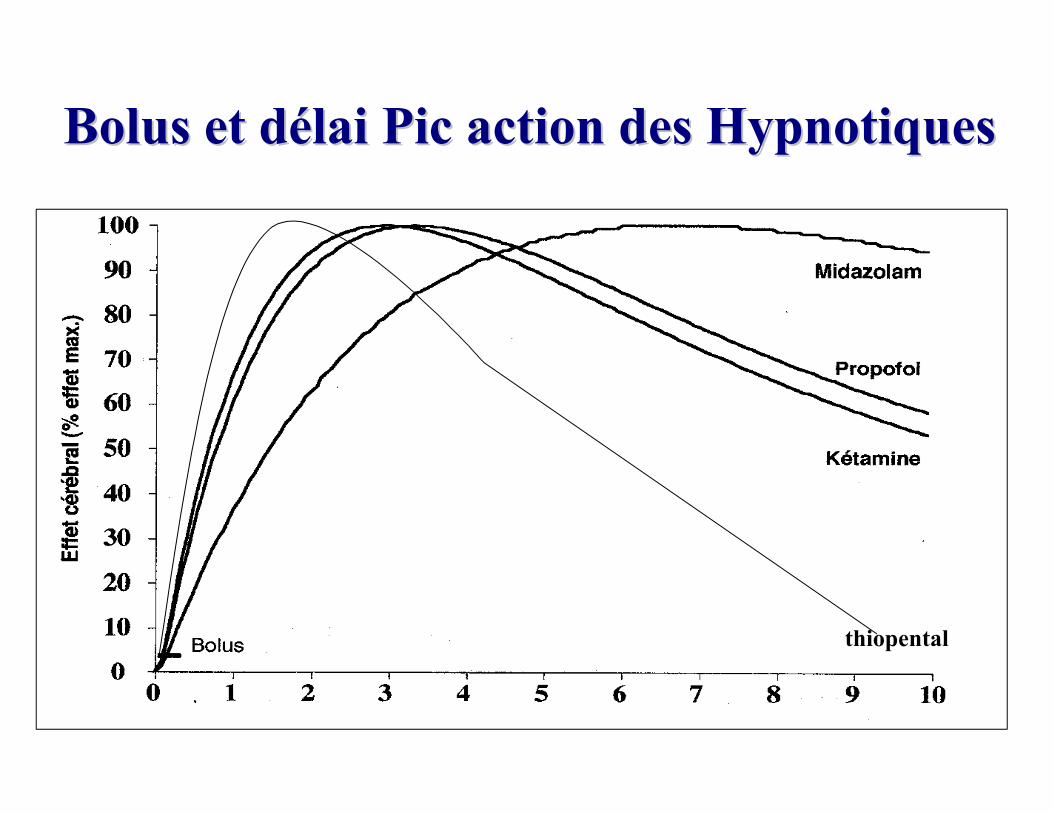
Bolus et dBolus et déélai Pic action des Hypnotiqueslai Pic action des Hypnotiques
thiopental
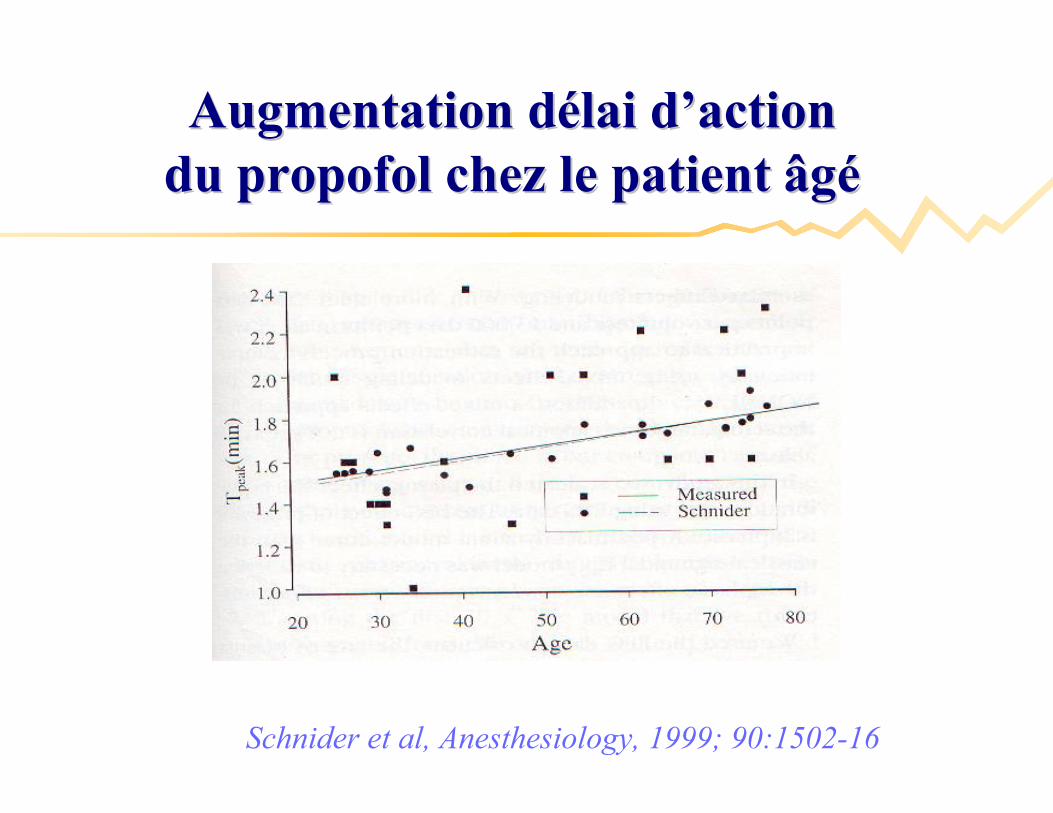
Schnider et al, Anesthesiology, 1999; 90:1502-16
Augmentation dAugmentation déélai dlai d’’actionactiondu propofol chez le patient âgdu propofol chez le patient âgéé

DurDuréée e actionaction
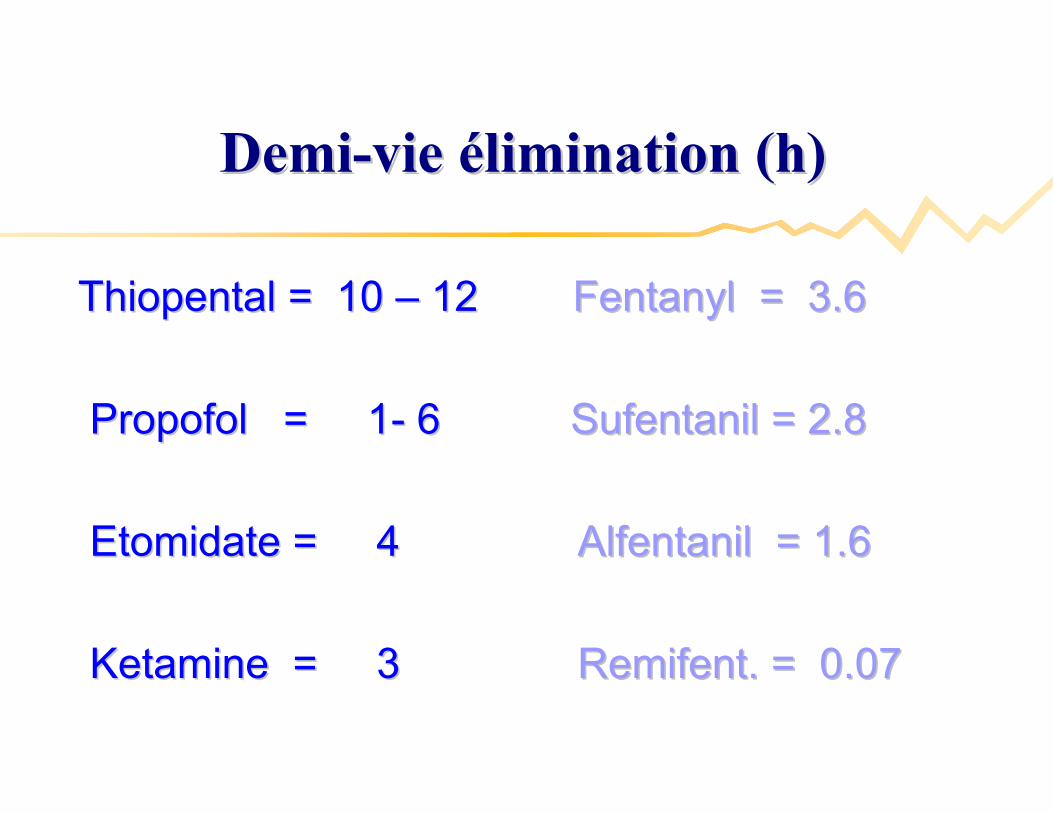
DemiDemi--vie vie éélimination (h)limination (h)
Thiopental = 10 Thiopental = 10 –– 12 12 Fentanyl = 3.6Fentanyl = 3.6
Propofol = 1Propofol = 1-- 6 6 Sufentanil = 2.8Sufentanil = 2.8
Etomidate = 4 Etomidate = 4 Alfentanil = 1.6 Alfentanil = 1.6
Ketamine = 3 Ketamine = 3 Remifent. = 0.07Remifent. = 0.07
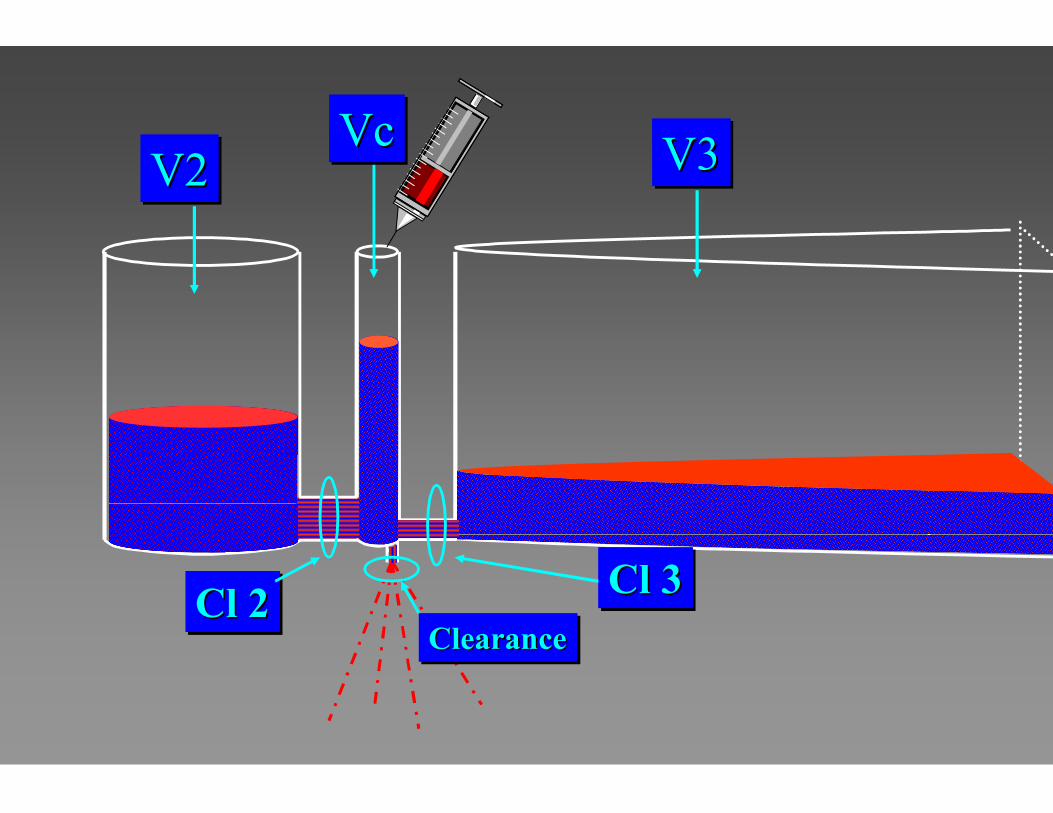
Cl 2Cl 2Cl 2 Cl 3Cl 3Cl 3ClearanceClearanceClearance
V2V2V2 V3V3V3VcVcVc
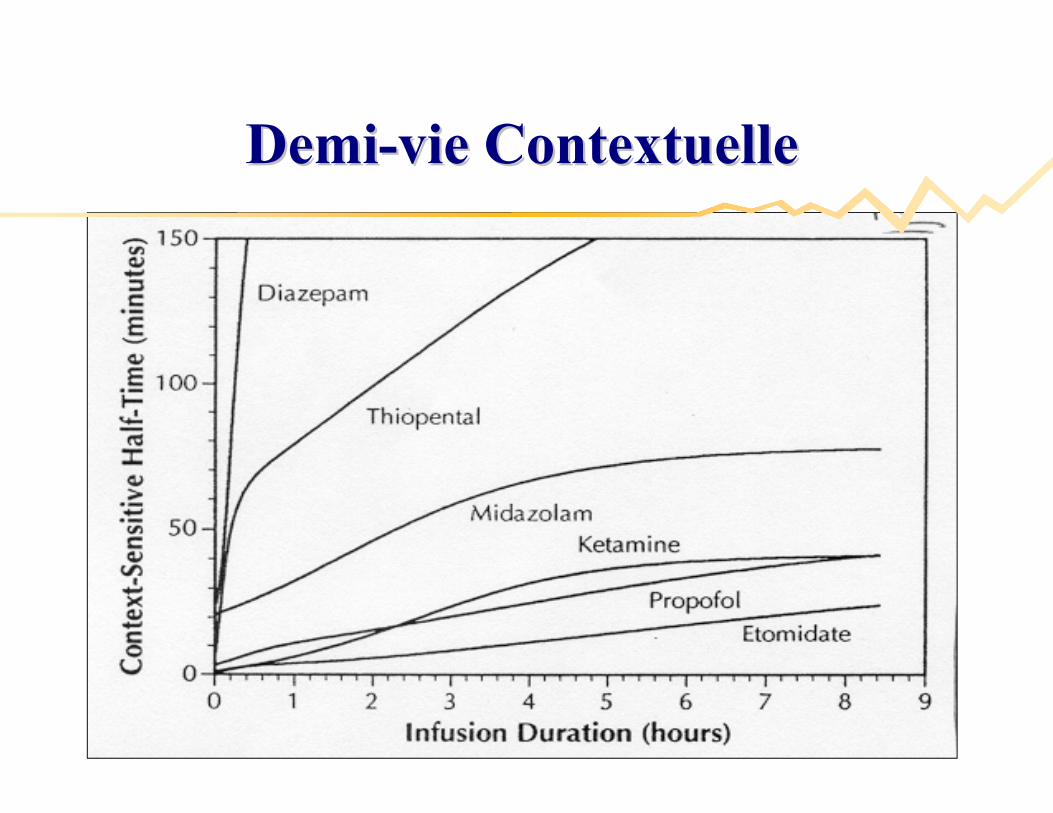
DemiDemi--vie Contextuellevie Contextuelle
AIVOC ou TCIAIVOC ou TCI
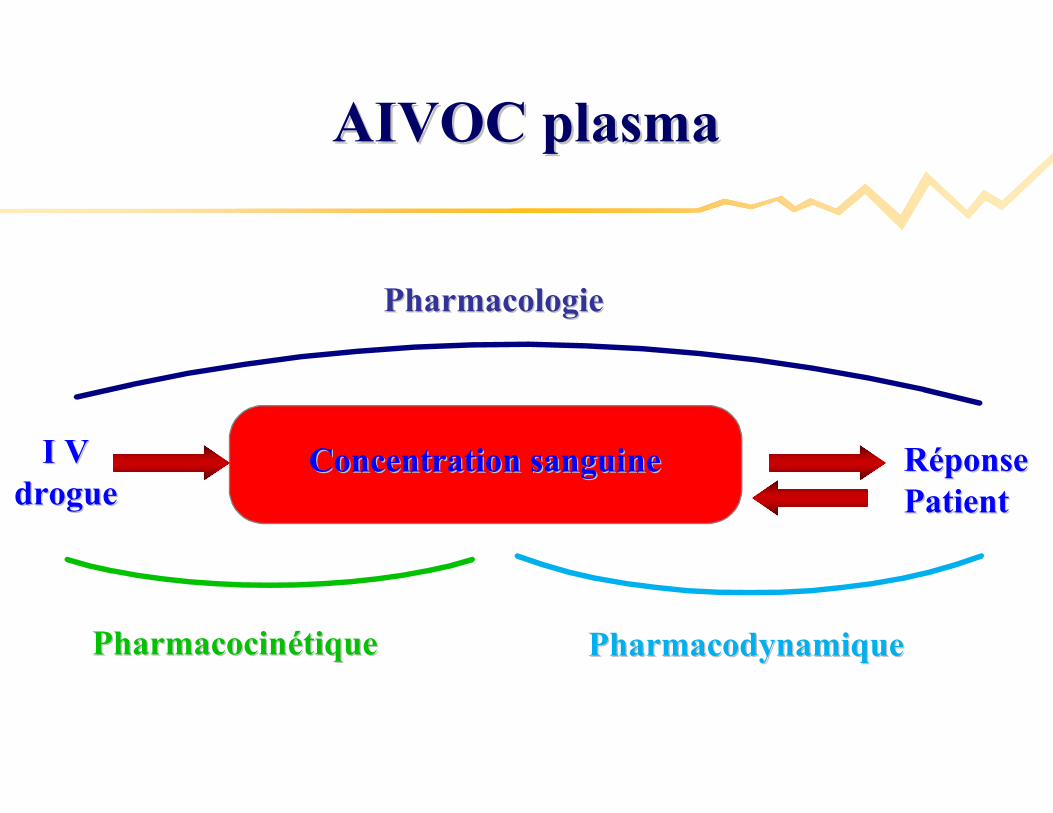
RRééponseponsePatientPatient
PharmacologiePharmacologie
PharmacodynamiquePharmacodynamique
I VI Vdroguedrogue
Concentration sanguineConcentration sanguine
PharmacocinPharmacocinéétiquetique
AIVOC plasmaAIVOC plasma
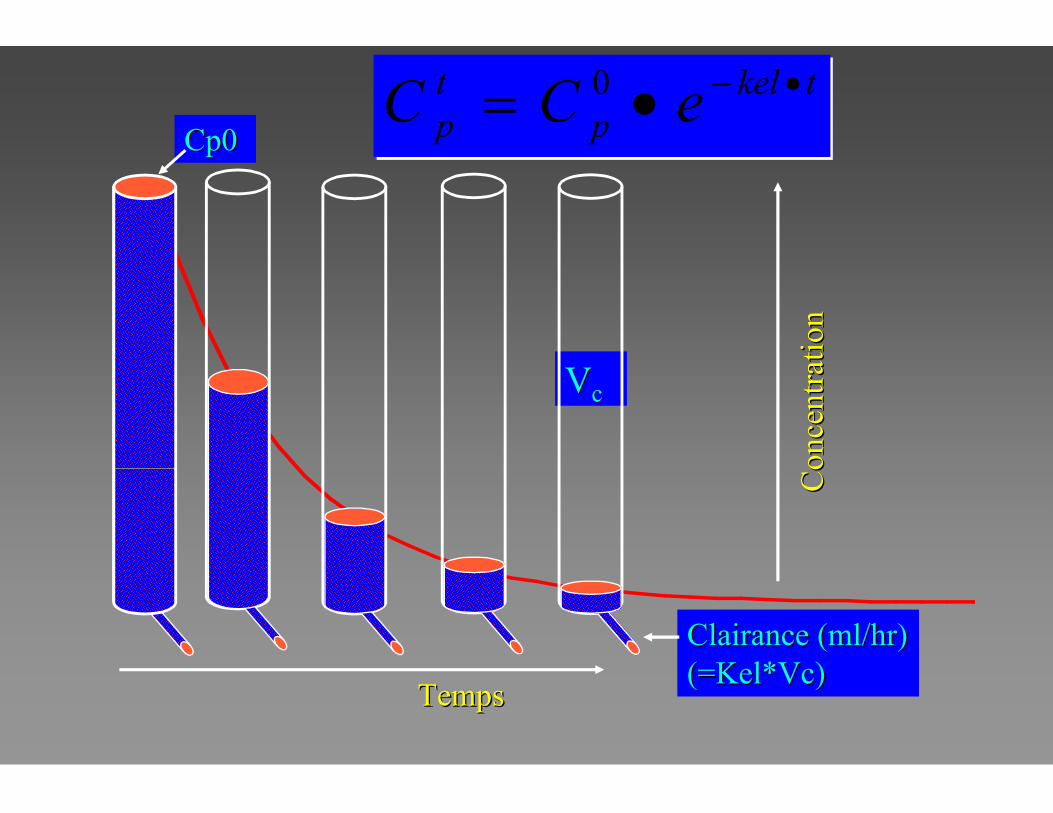
VVcc
TempsTemps
Con
cent
rati
onC
once
ntra
tion
Clairance (ml/hr)Clairance (ml/hr)(=Kel*Vc)(=Kel*Vc)
Cp0Cp0
tkelp
tp eCC 0
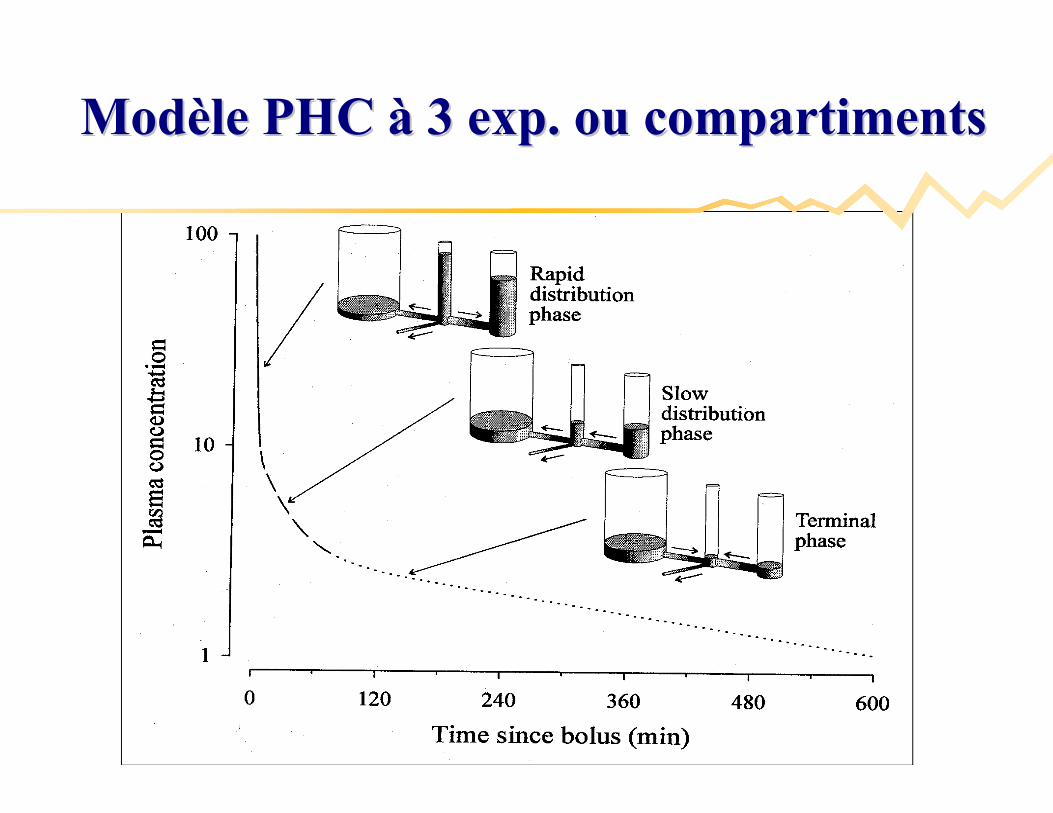
ModModèèle PHC le PHC àà 3 exp. ou compartiments3 exp. ou compartiments
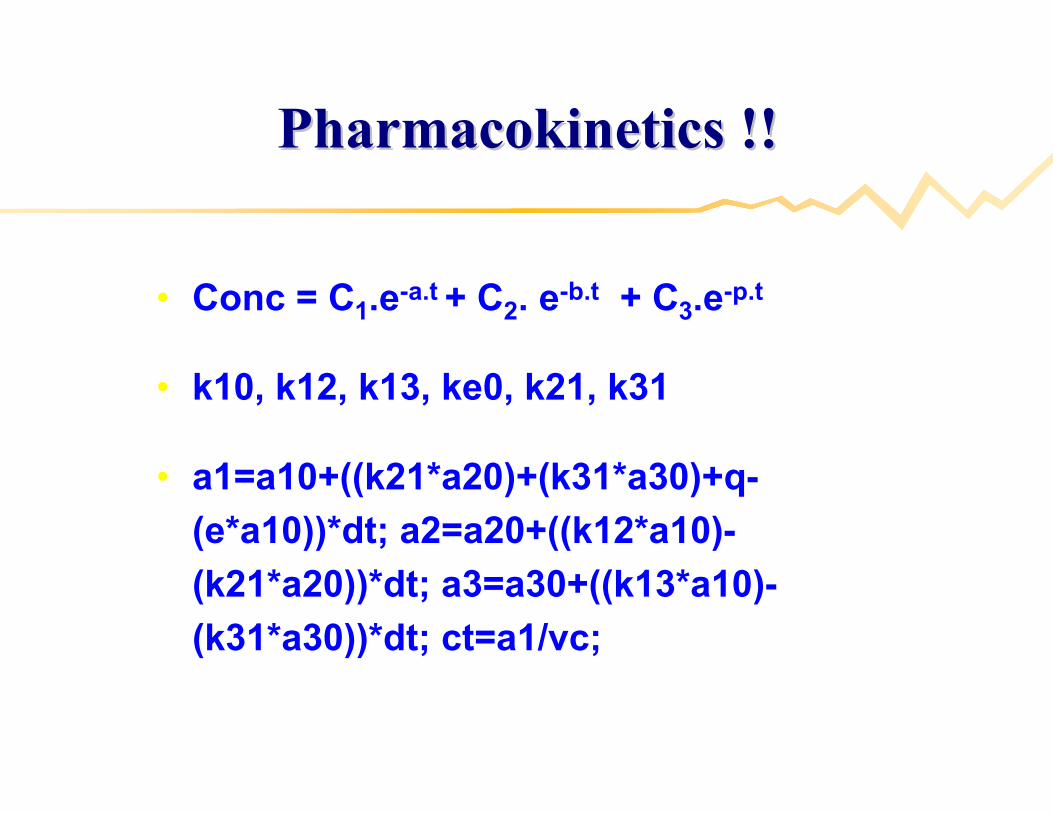
Pharmacokinetics !!Pharmacokinetics !!
• Conc = C1.e-a.t + C2. e-b.t + C3.e-p.t
• k10, k12, k13, ke0, k21, k31
• a1=a10+((k21*a20)+(k31*a30)+q-
(e*a10))*dt; a2=a20+((k12*a10)-
(k21*a20))*dt; a3=a30+((k13*a10)-
(k31*a30))*dt; ct=a1/vc;
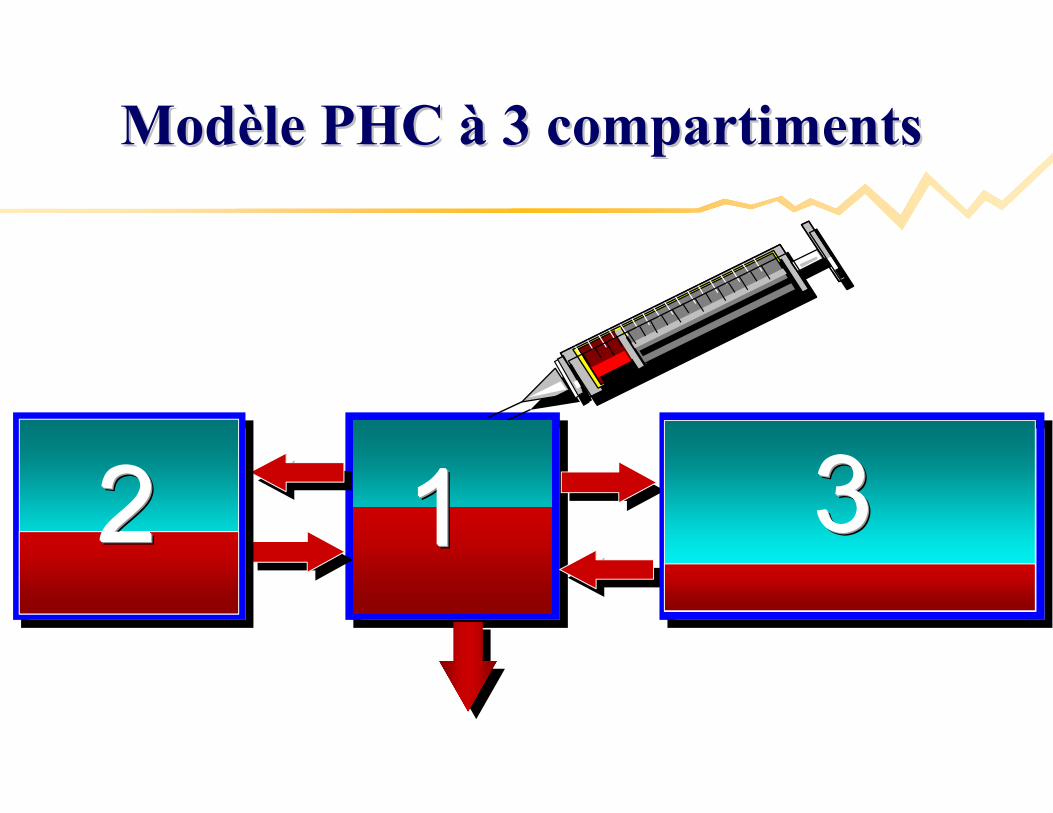
1111 3333
ModModèèle PHC le PHC àà 3 compartiments 3 compartiments
2222
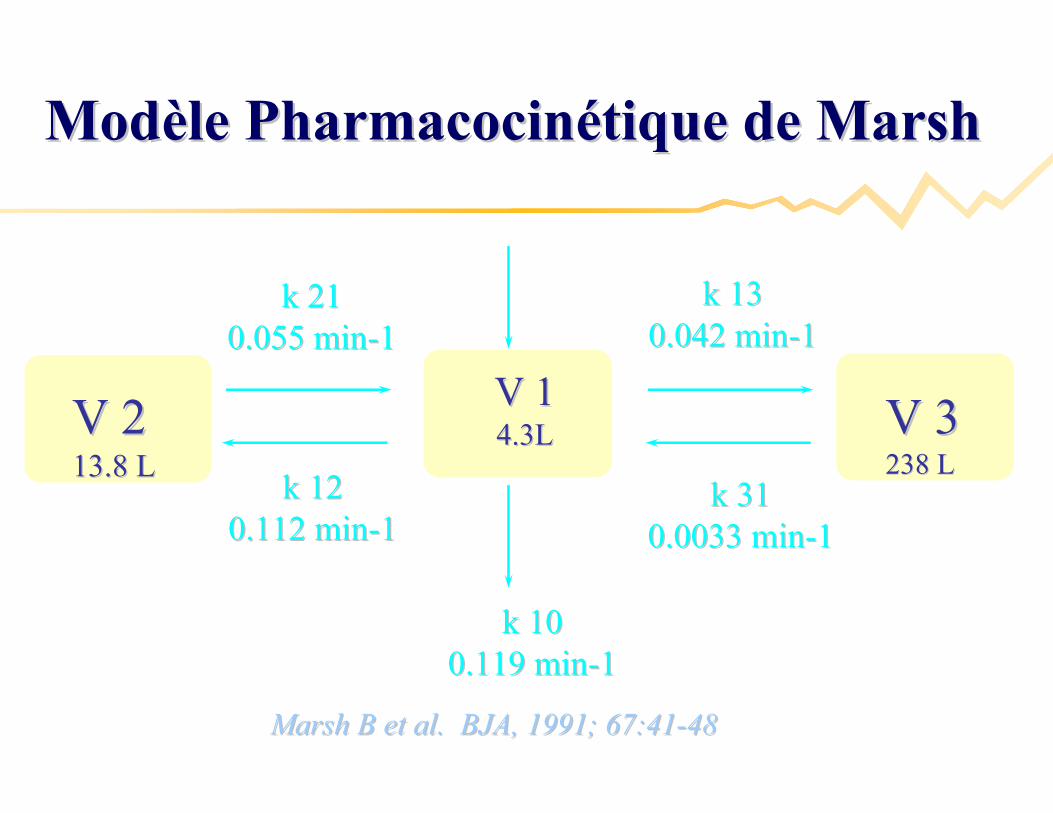
V 1V 14.3L4.3L V 3V 3
238 L238 LV 2V 213.8 L13.8 L
k 21k 210.055 min0.055 min--1 1
k 12k 120.112 min0.112 min--11
k 31k 310.0033 min0.0033 min--11
k 13k 130.042 min0.042 min--11
k 10 k 10 0.119 min0.119 min--11
Marsh B et al. BJA, 1991; 67:41Marsh B et al. BJA, 1991; 67:41--4848
ModModèèle Pharmacocinle Pharmacocinéétique de Marshtique de Marsh
Prototype DiprifusorPrototype Diprifusor
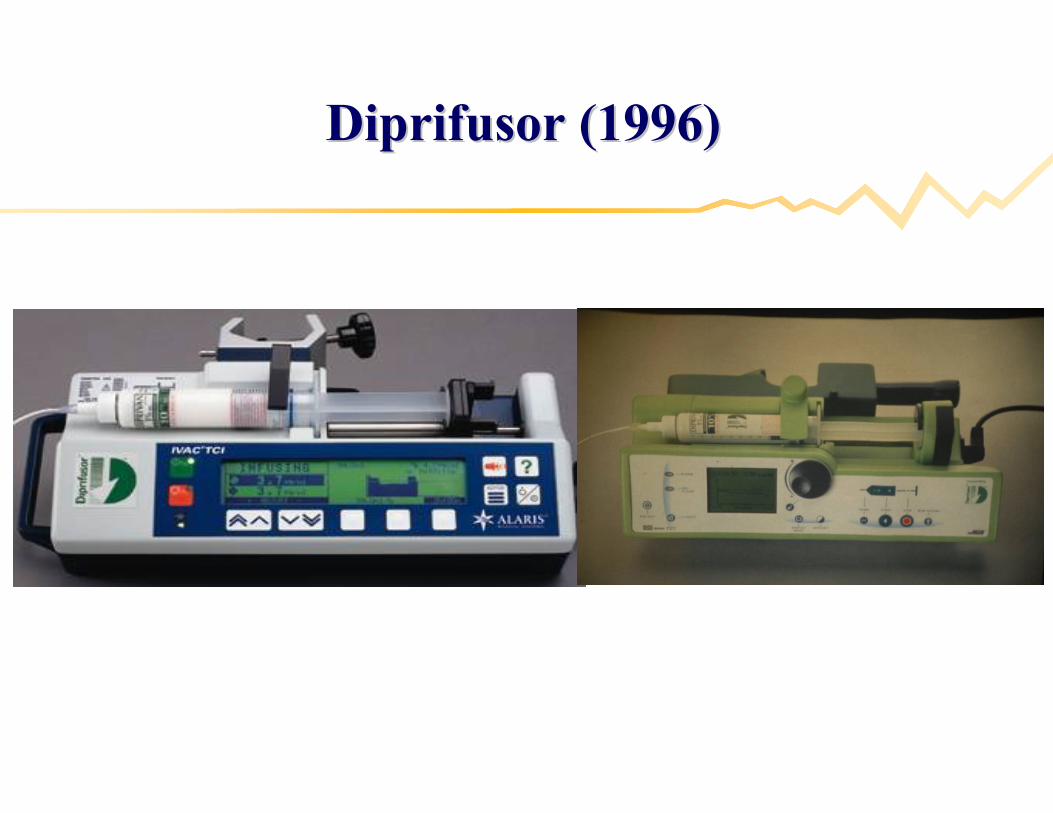
Diprifusor (1996)Diprifusor (1996)
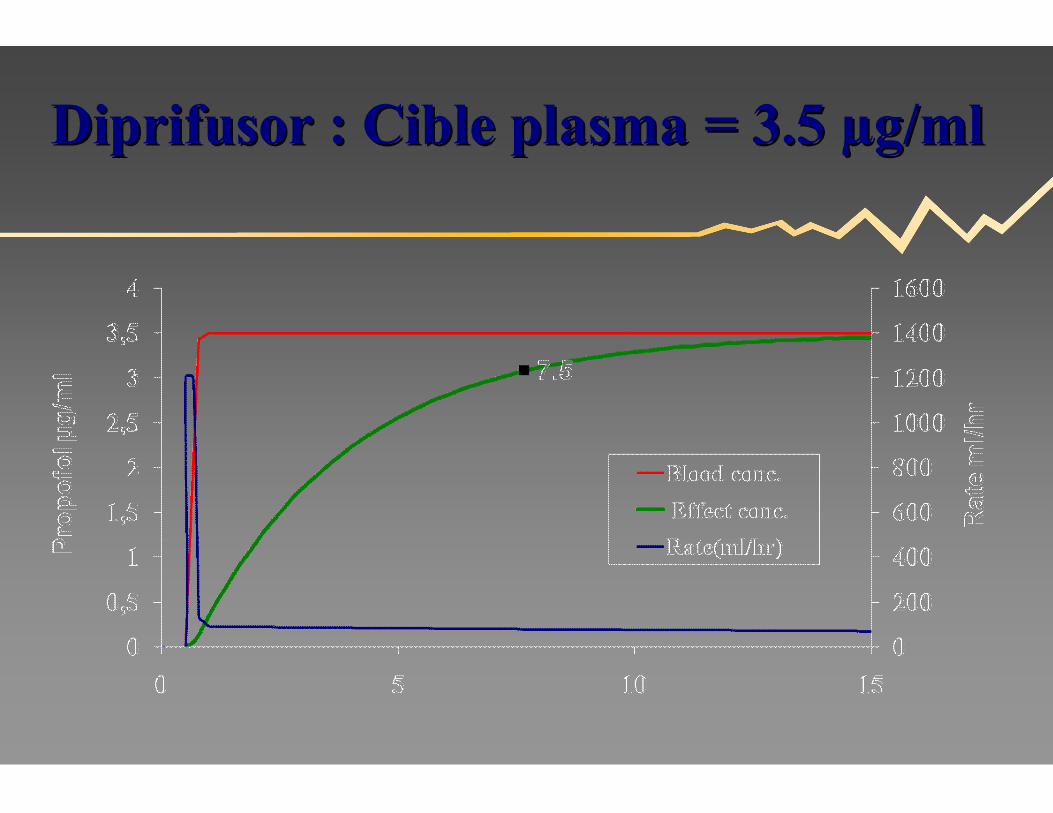
Diprifusor : Cible plasma = 3.5 Diprifusor : Cible plasma = 3.5 µµg/mlg/ml
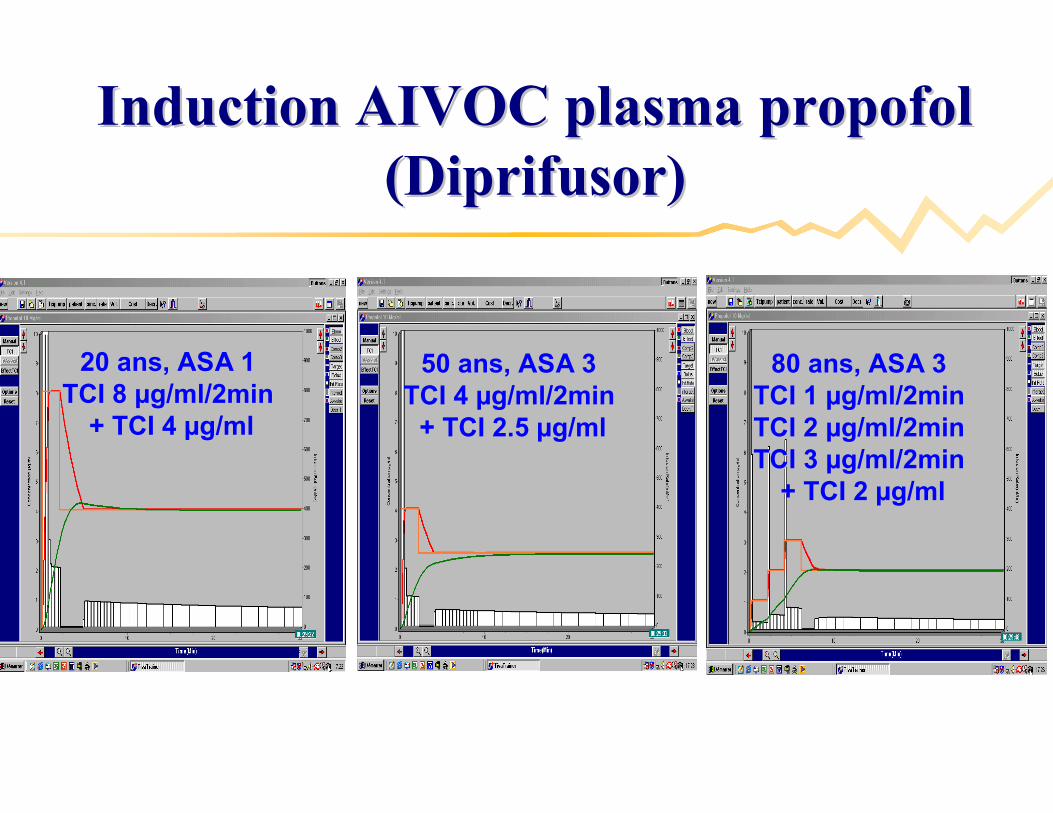
Induction AIVOC plasma propofol Induction AIVOC plasma propofol (Diprifusor)(Diprifusor)
20 ans, ASA 120 ans, ASA 1TCI 8 TCI 8 µµg/ml/2ming/ml/2min
+ TCI 4 + TCI 4 µµg/mlg/ml
50 ans, ASA 350 ans, ASA 3TCI 4 TCI 4 µµg/ml/2ming/ml/2min
+ TCI 2.5 + TCI 2.5 µµg/mlg/ml
80 ans, ASA 380 ans, ASA 3TCI 1 TCI 1 µµg/ml/2ming/ml/2minTCI 2 TCI 2 µµg/ml/2ming/ml/2minTCI 3 TCI 3 µµg/ml/2ming/ml/2min
+ TCI 2 + TCI 2 µµg/mlg/ml
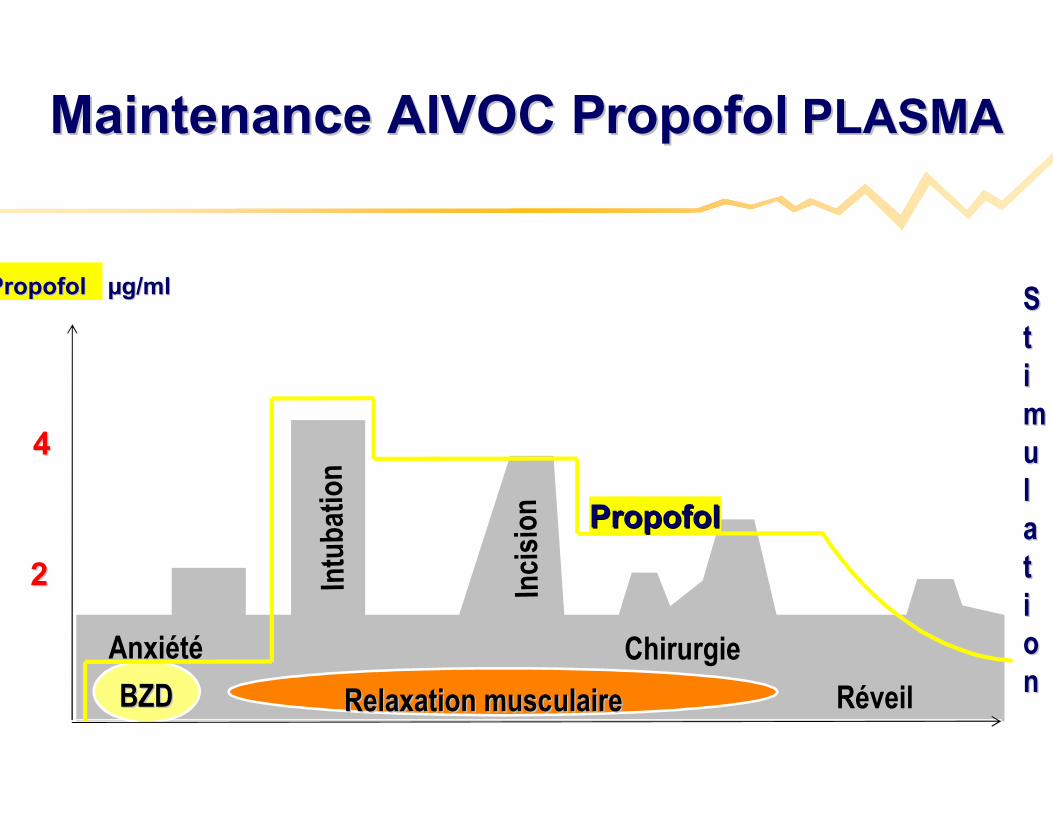
ChirurgieChirurgie
SSttiimmuullaattiioonn
Intu
batio
nIn
tuba
tion
Inci
sion
Inci
sion
RRééveilveil
PropofolPropofol
Relaxation musculaireRelaxation musculaireBZDBZD
22
44
AnxiAnxiééttéé
Maintenance AIVOC PropofolMaintenance AIVOC Propofol PLASMAPLASMA
Propofol Propofol µµg/mlg/ml
•• BBéénnééfices du Diprifusor =fices du Diprifusor =
facile facile àà utiliser avec training minimalutiliser avec training minimal
nombre interventions anesthnombre interventions anesthéésistesiste
incidence des mouvements incidence des mouvements
rapiditrapiditéé du rdu rééveilveil
……
TCI compared with manually controlled infusion TCI compared with manually controlled infusion of propofol : a multicentre studyof propofol : a multicentre study
Servin F et al. Anaesthesia 1998; 53: 82Servin F et al. Anaesthesia 1998; 53: 82--8686
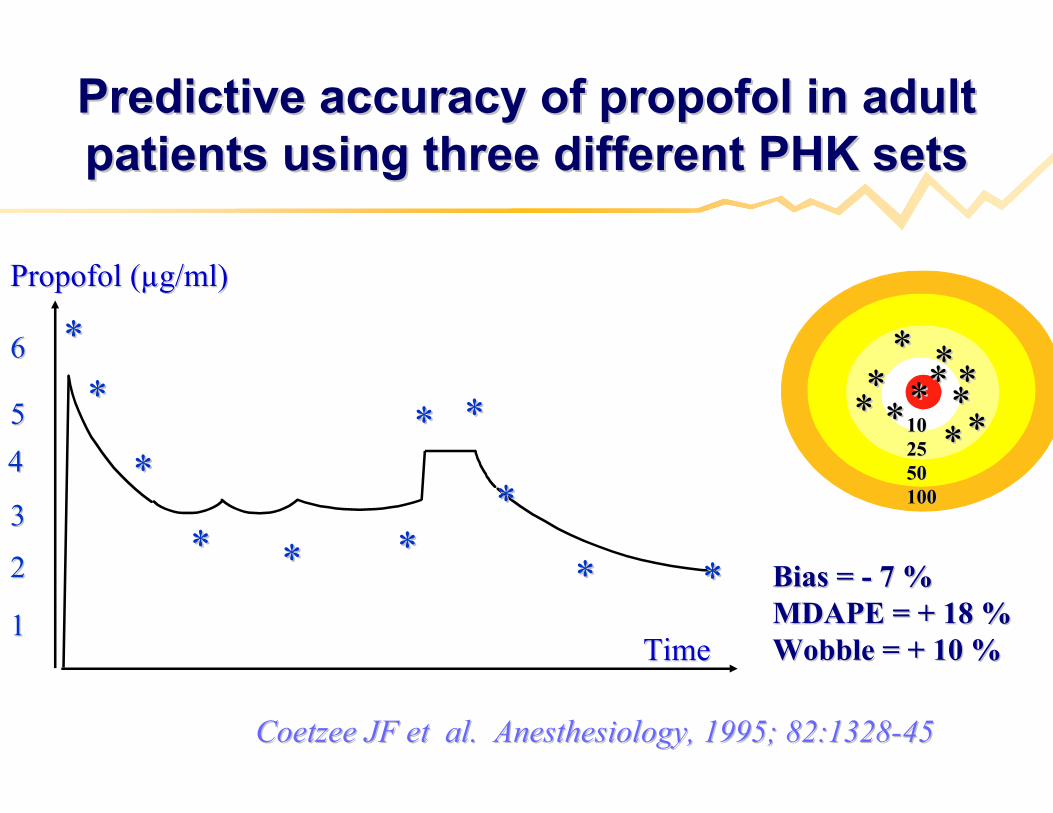
Predictive accuracy of propofol in adult Predictive accuracy of propofol in adult patients using three different PHK setspatients using three different PHK sets
TTimeime
Propofol (Propofol (µµg/ml)g/ml)
22
55
44
33
11
** ****
**
**
Bias = Bias = -- 7 % 7 % MDAPE = + 18 %MDAPE = + 18 %Wobble = + 10 %Wobble = + 10 %
****
****
**
**
**
** **
**
**
**
** **
**
**
101025255050100100
**
Coetzee JF et al. Anesthesiology, 1995; 82:1328Coetzee JF et al. Anesthesiology, 1995; 82:1328--4545
66
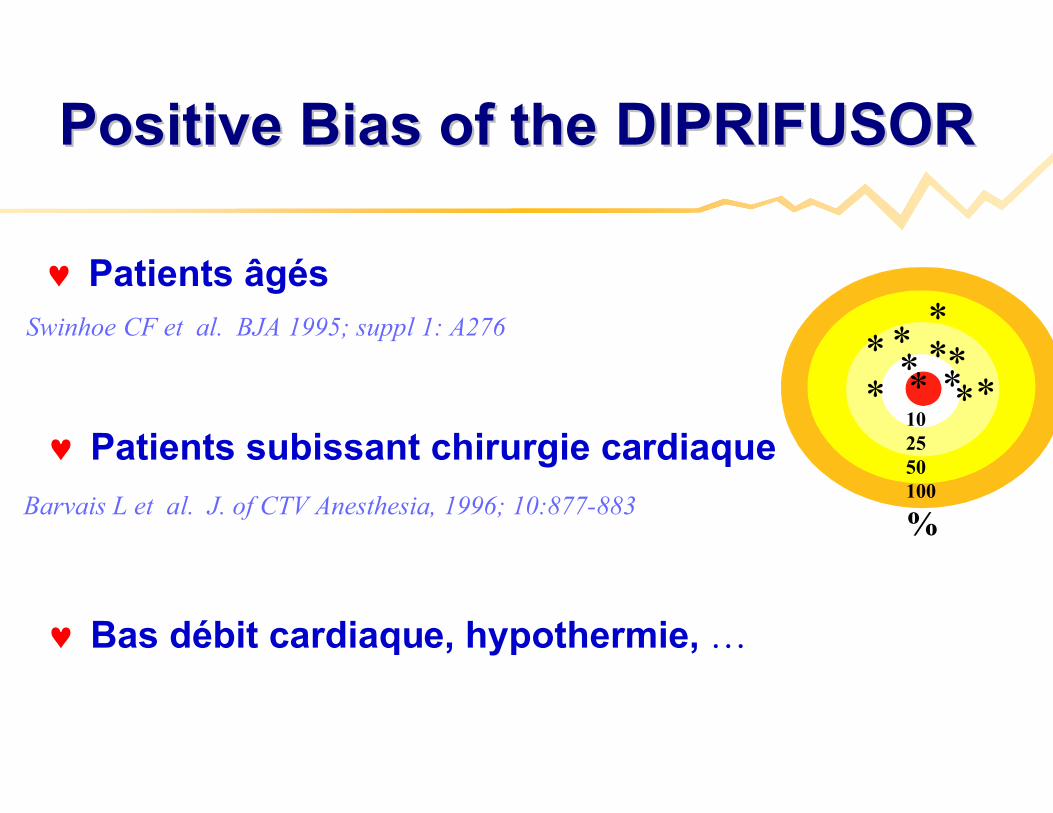
Positive Bias of the DIPRIFUSORPositive Bias of the DIPRIFUSOR
****
** *
** *102550100
%
*
Barvais L et al. J. of CTV Anesthesia, 1996; 10:877-883
Swinhoe CF et al. BJA 1995; suppl 1: A276
Patients âgés
Patients subissant chirurgie cardiaque
Bas débit cardiaque, hypothermie, …
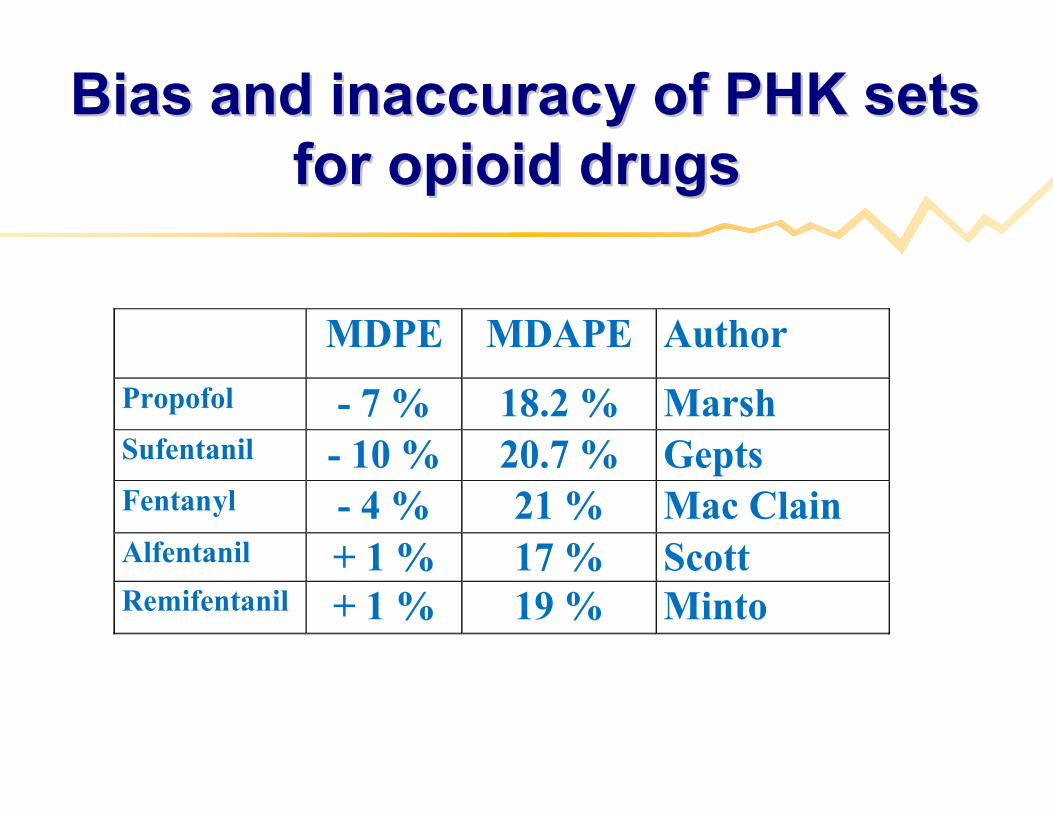
Bias and inaccuracy of PHK sets Bias and inaccuracy of PHK sets for opioid drugs for opioid drugs
MDPE MDAPE Author
Propofol - 7 % 18.2 % MarshSufentanil - 10 % 20.7 % GeptsFentanyl - 4 % 21 % Mac ClainAlfentanil + 1 % 17 % ScottRemifentanil + 1 % 19 % Minto
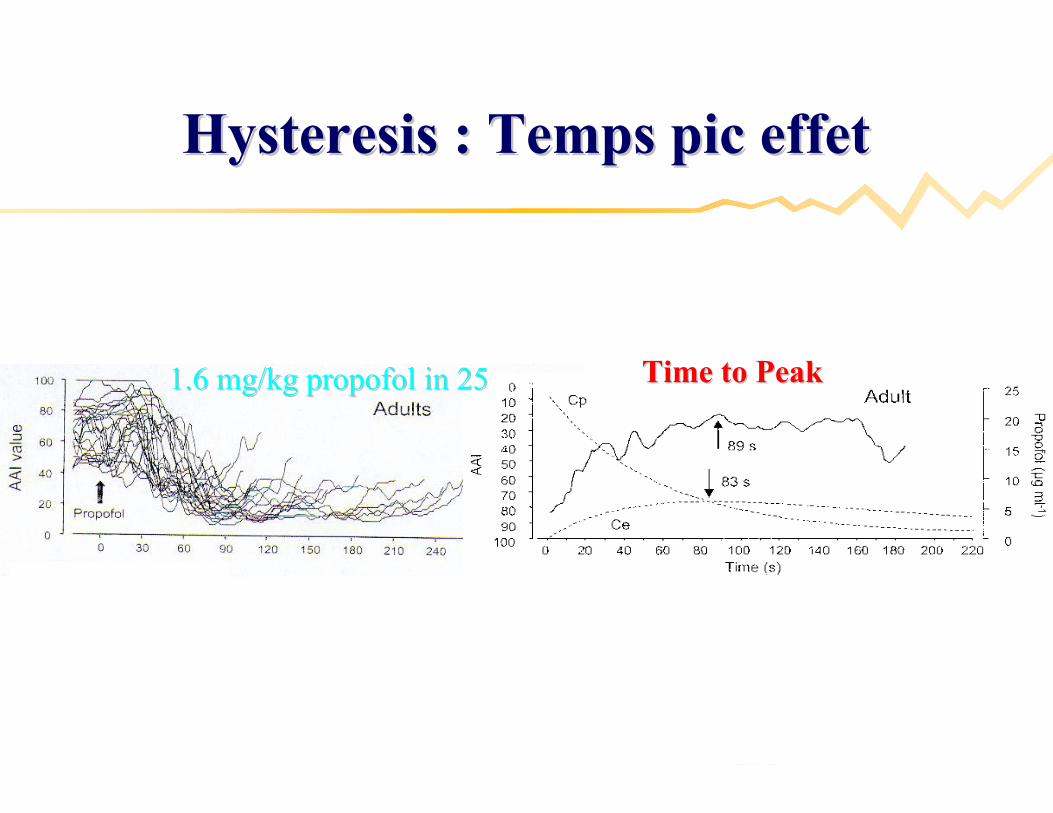
1.6 mg/kg propofol in 251.6 mg/kg propofol in 25 Time to PeakTime to Peak
Hysteresis : Temps pic effetHysteresis : Temps pic effet
Munoz et alMunoz et al, Anesthesiology, 2004, Anesthesiology, 2004, December, 101, December, 101:1269:1269--7474
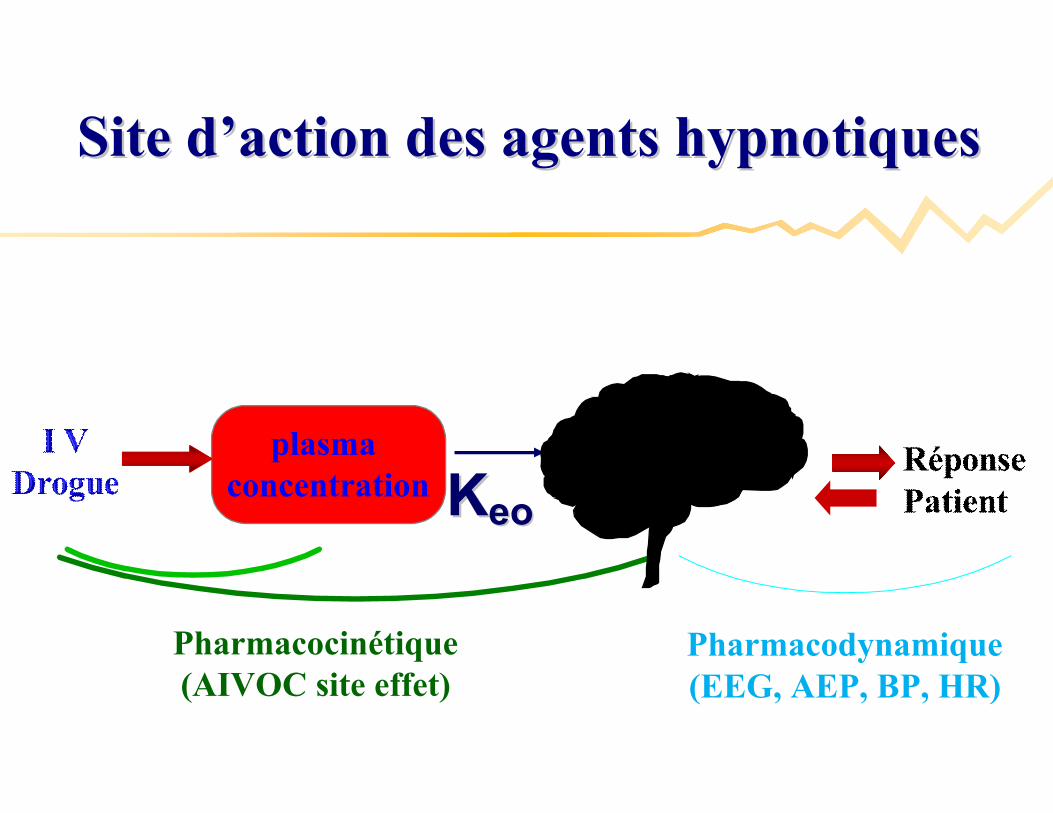
Pharmacodynamique(EEG, AEP, BP, HR)
plasma concentration KKeoeo
Pharmacocinétique(AIVOC site effet)
Site dSite d’’action des agents hypnotiquesaction des agents hypnotiques
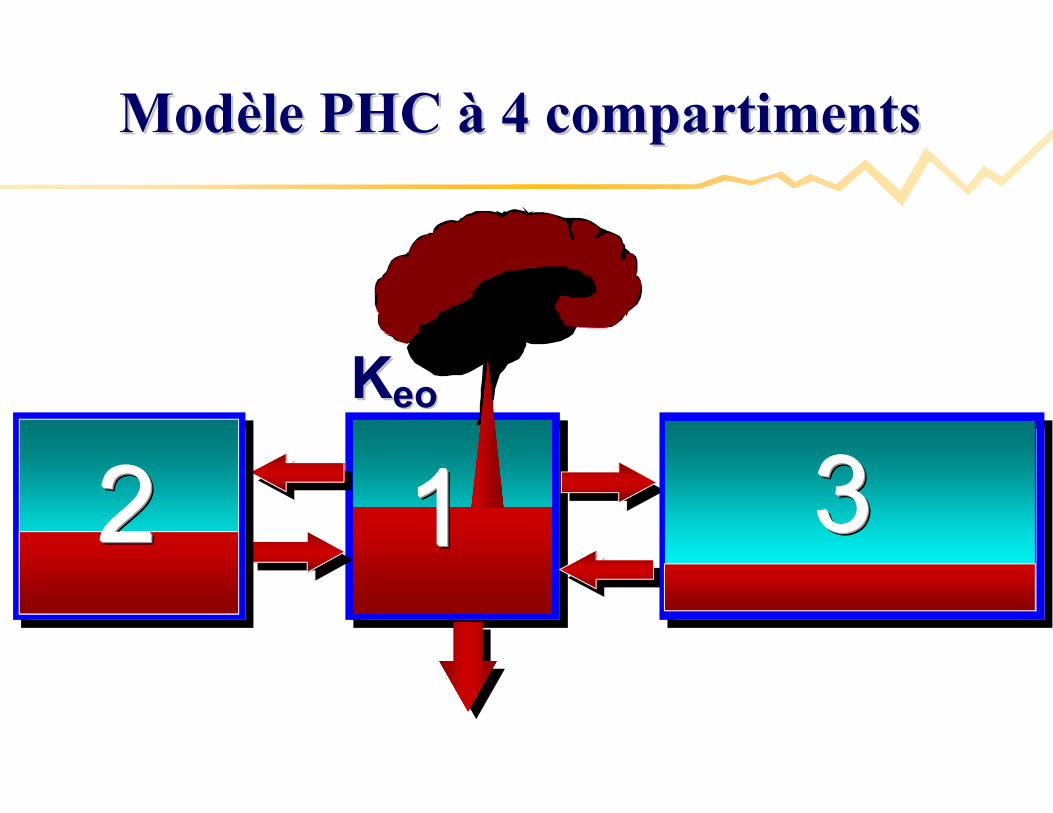
1111 33332222
ModModèèle PHC le PHC àà 4 compartiments4 compartiments
KKeoeo
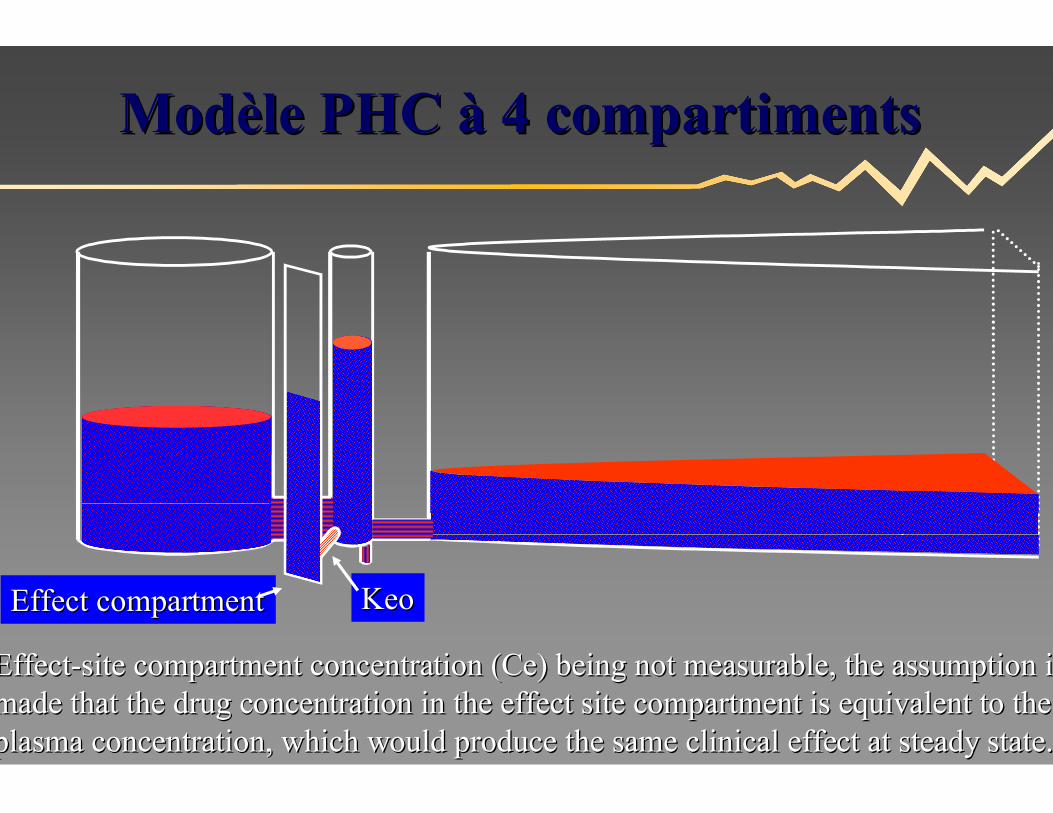
KeoKeoEffect compartmentEffect compartment
EffectEffect--site compartment concentration (Ce) being not measurable, the assite compartment concentration (Ce) being not measurable, the assumption is sumption is made that the drug concentration in the effect site compartment made that the drug concentration in the effect site compartment is equivalent to the is equivalent to the plasma concentration, which would produce the same clinical effeplasma concentration, which would produce the same clinical effect at steady state.ct at steady state.
ModModèèle PHC le PHC àà 4 compartiments4 compartiments
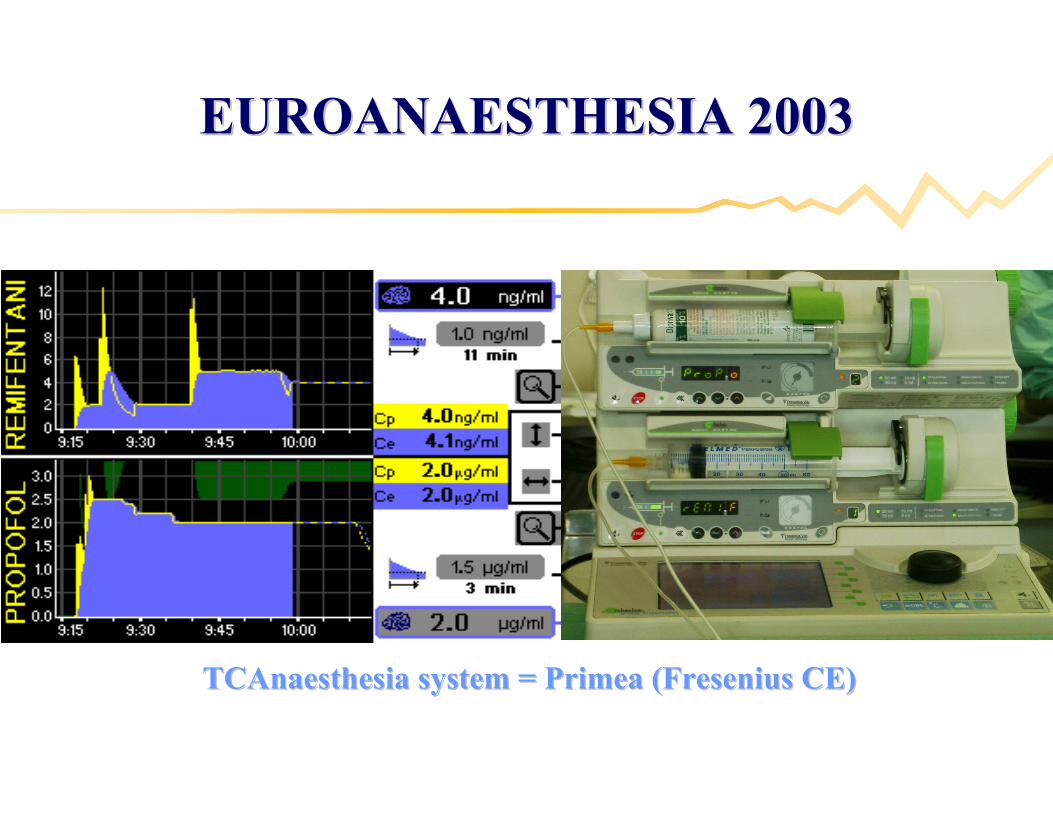
EUROANAESTHESIA 2003EUROANAESTHESIA 2003
TCAnaesthesia system = Primea (Fresenius CE)TCAnaesthesia system = Primea (Fresenius CE)
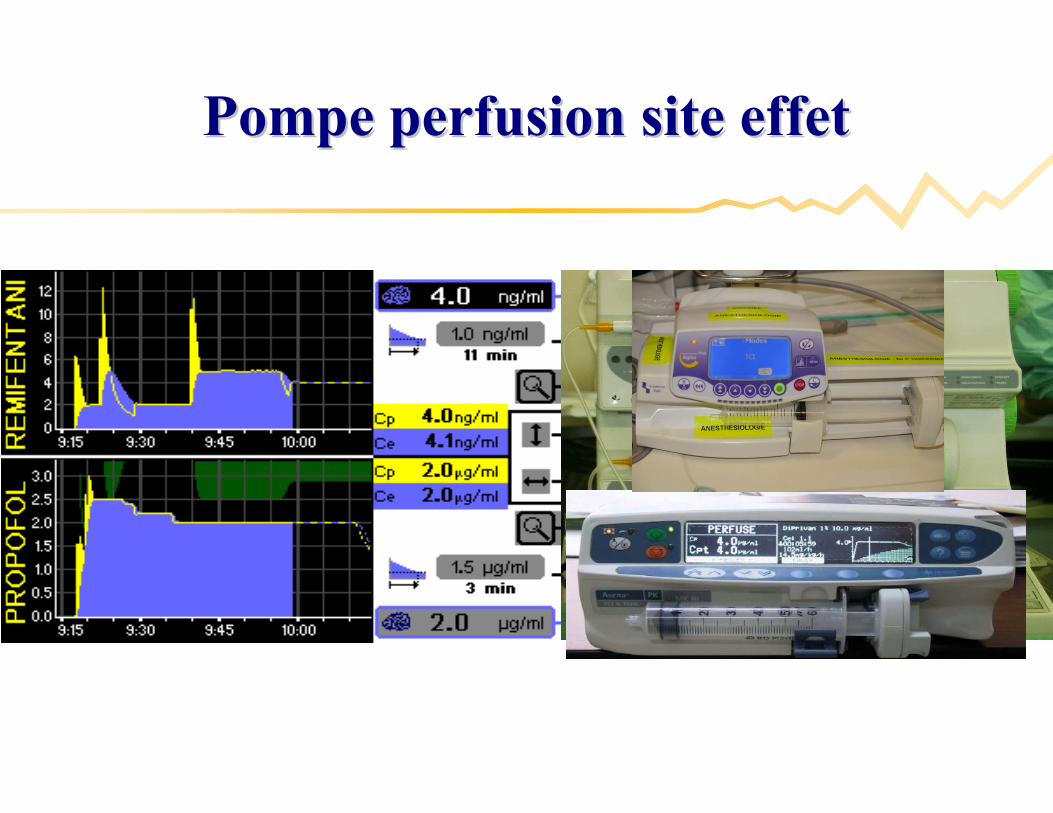
Pompe perfusion site effetPompe perfusion site effet
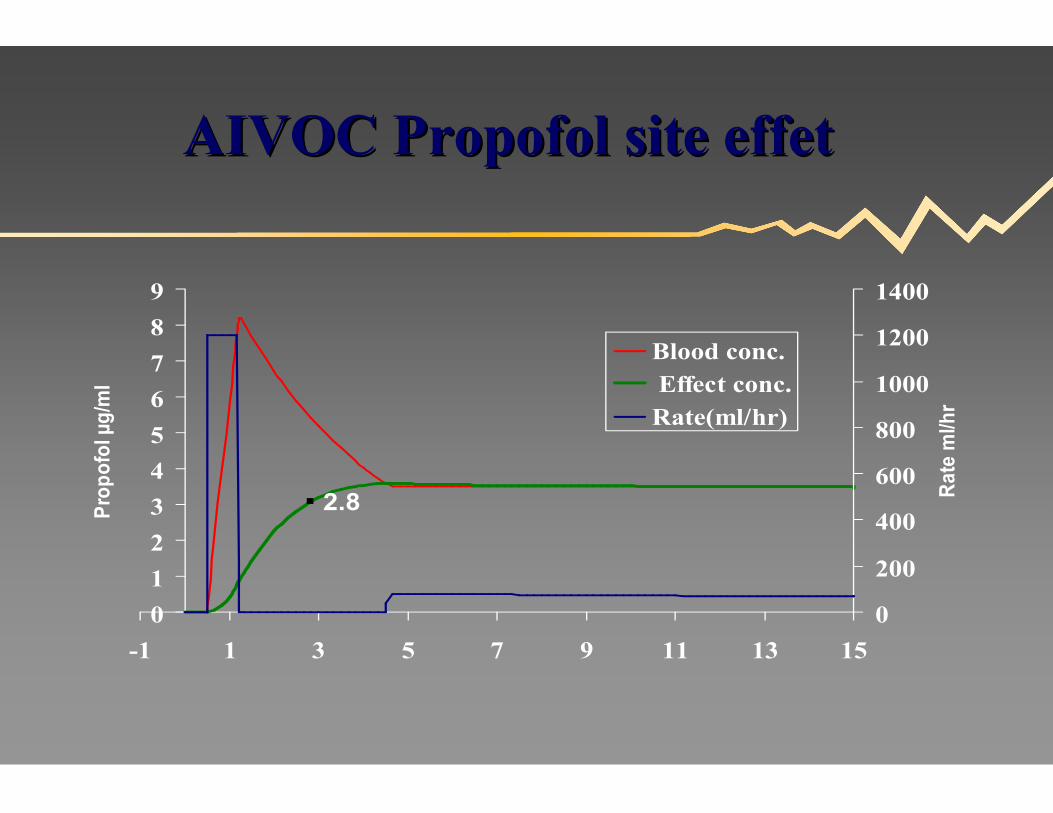
2.8
0
1
2
3
4
5
6
7
8
9
-1 1 3 5 7 9 11 13 15
Pro
pof
ol µ
g/m
l
0
200
400
600
800
1000
1200
1400
Rat
e m
l/hr
Blood conc. Effect conc.Rate(ml/hr)
AIVOC Propofol site effetAIVOC Propofol site effet
0
1
2
3
4
5
6
7
8
9
0 5 10 15 20 25 30 35 40
Pro
pof
ol µ
g/m
l
0
200
400
600
800
1000
1200
1400
Rat
e m
l/hr
Blood conc. Effect conc.Rate(ml/hr)
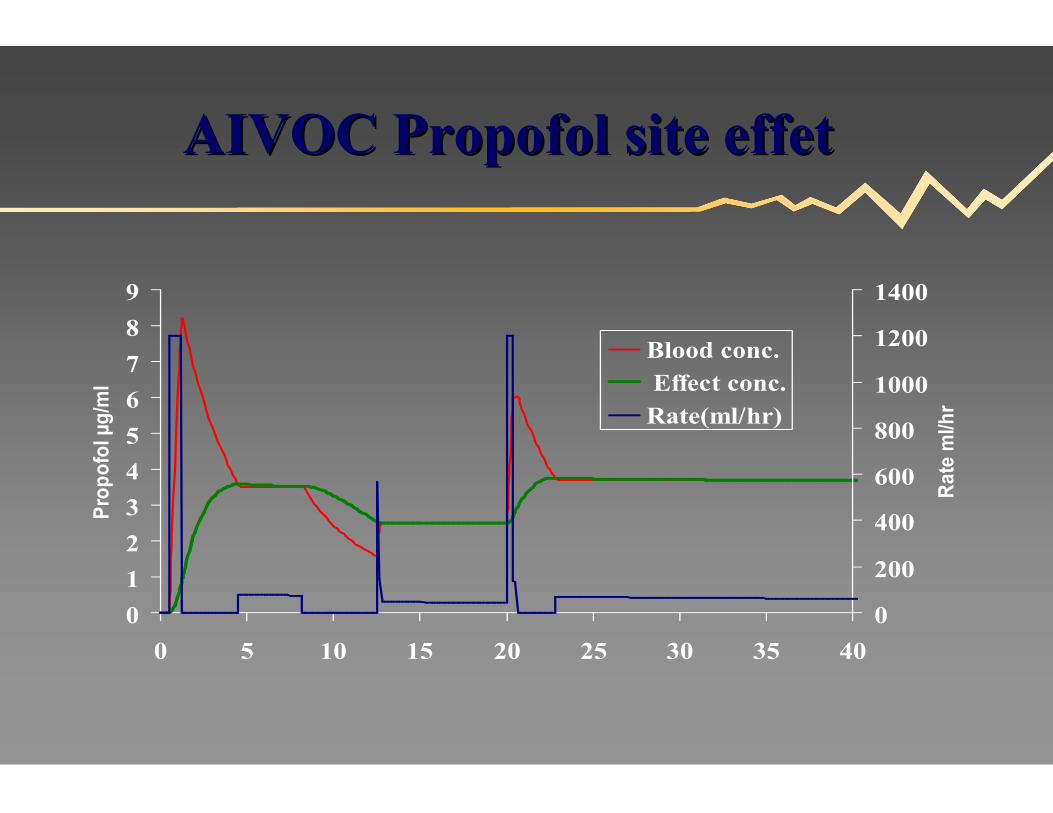
AIVOC Propofol site effetAIVOC Propofol site effet
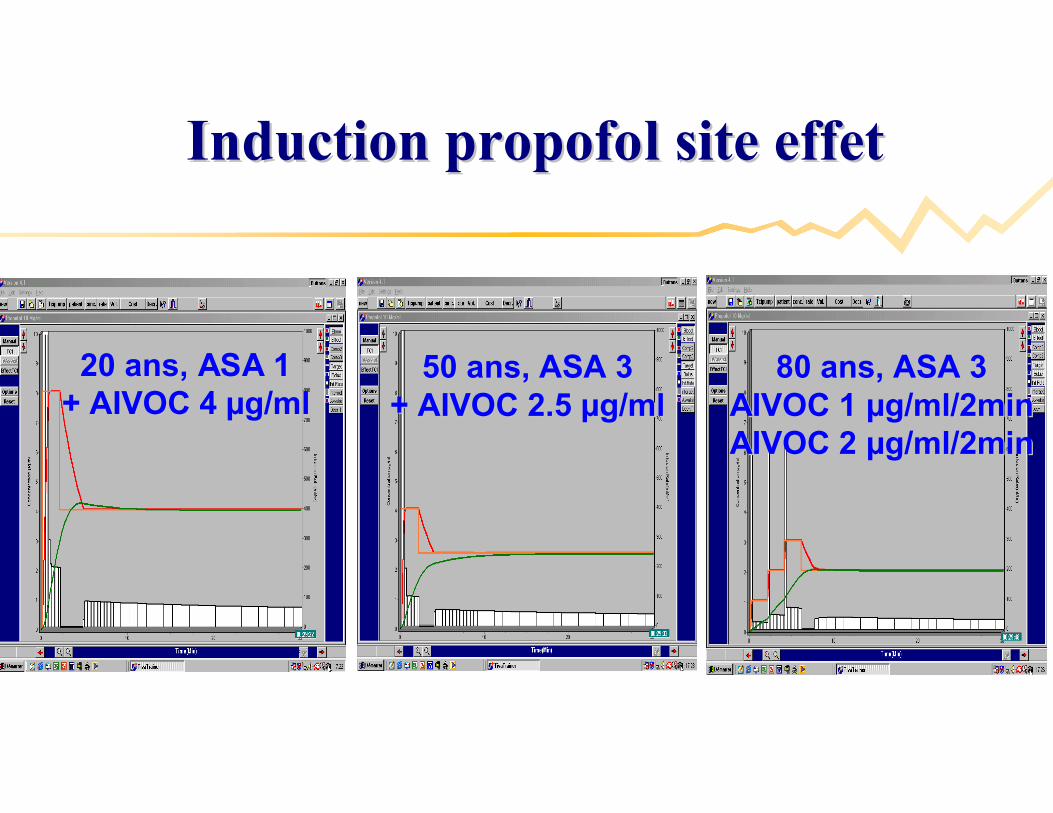
Induction propofol site effet Induction propofol site effet
20 ans, ASA 120 ans, ASA 1+ AIVOC 4 + AIVOC 4 µµg/mlg/ml
50 ans, ASA 350 ans, ASA 3+ AIVOC 2.5 + AIVOC 2.5 µµg/mlg/ml
80 ans, ASA 380 ans, ASA 3AIVOC 1 AIVOC 1 µµg/ml/2ming/ml/2minAIVOC 2 AIVOC 2 µµg/ml/2ming/ml/2min

OneOne--way valve + reduced dead spaceway valve + reduced dead space

Valve uniValve uni--directionnelledirectionnelle

Case report: dCase report: dééconnection voie IV!connection voie IV!

Case report: fuite Propofol!Case report: fuite Propofol!

30 cm ligne perfusion30 cm ligne perfusion==
1.5 ml espace mort1.5 ml espace mort
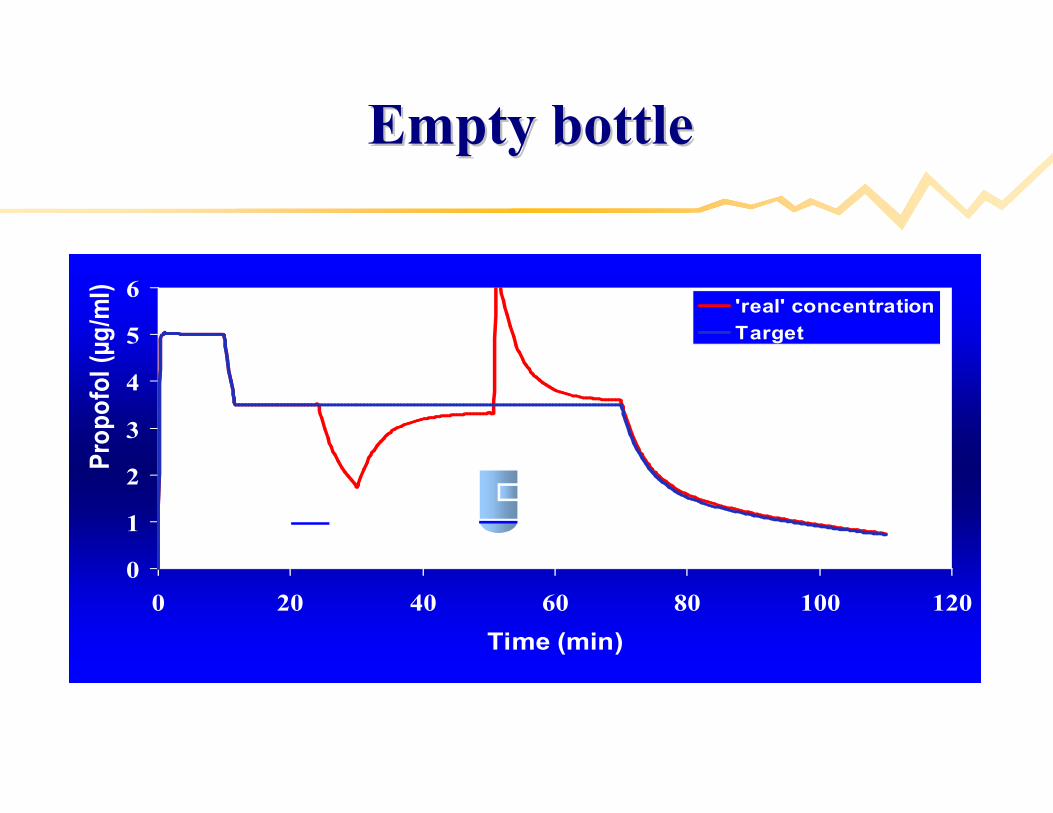
0
1
2
3
4
5
6
0 20 40 60 80 100 120
Time (min)
Pro
pofo
l (µg
/ml)
'real' concentration
Target
Empty bottleEmpty bottle
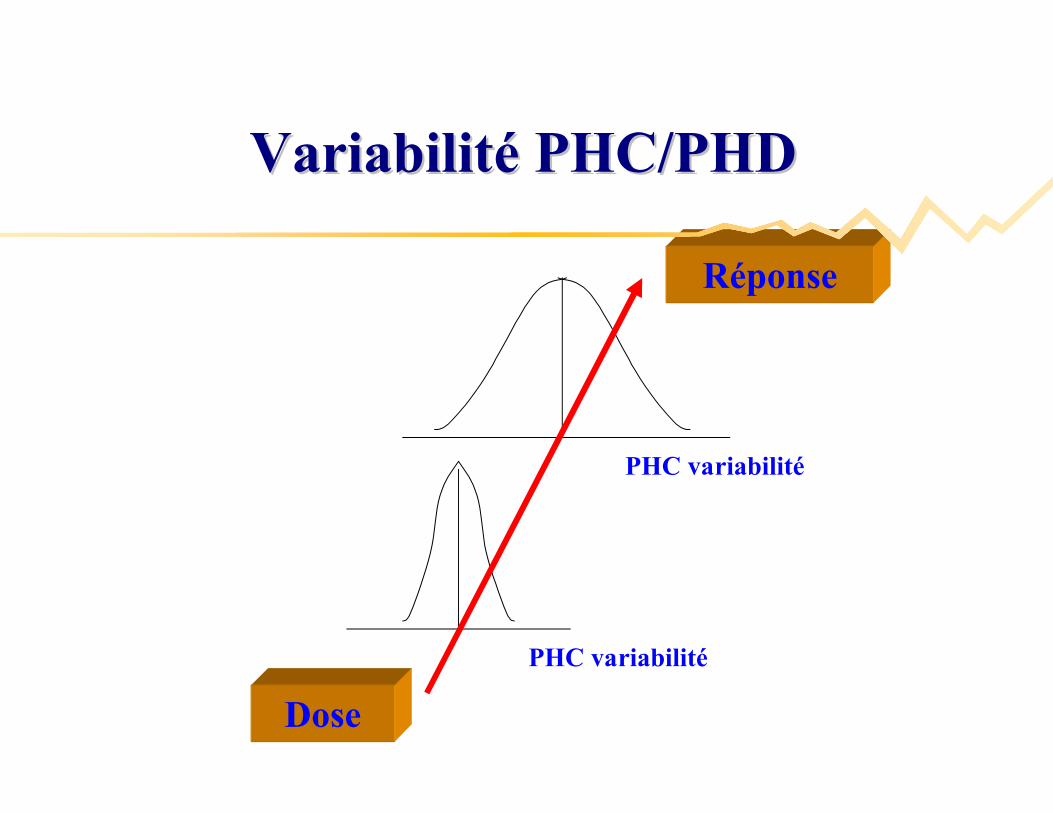
Dose
PHC variabilité
PHC variabilité
Réponse
VariabilitVariabilitéé PHC/PHDPHC/PHD
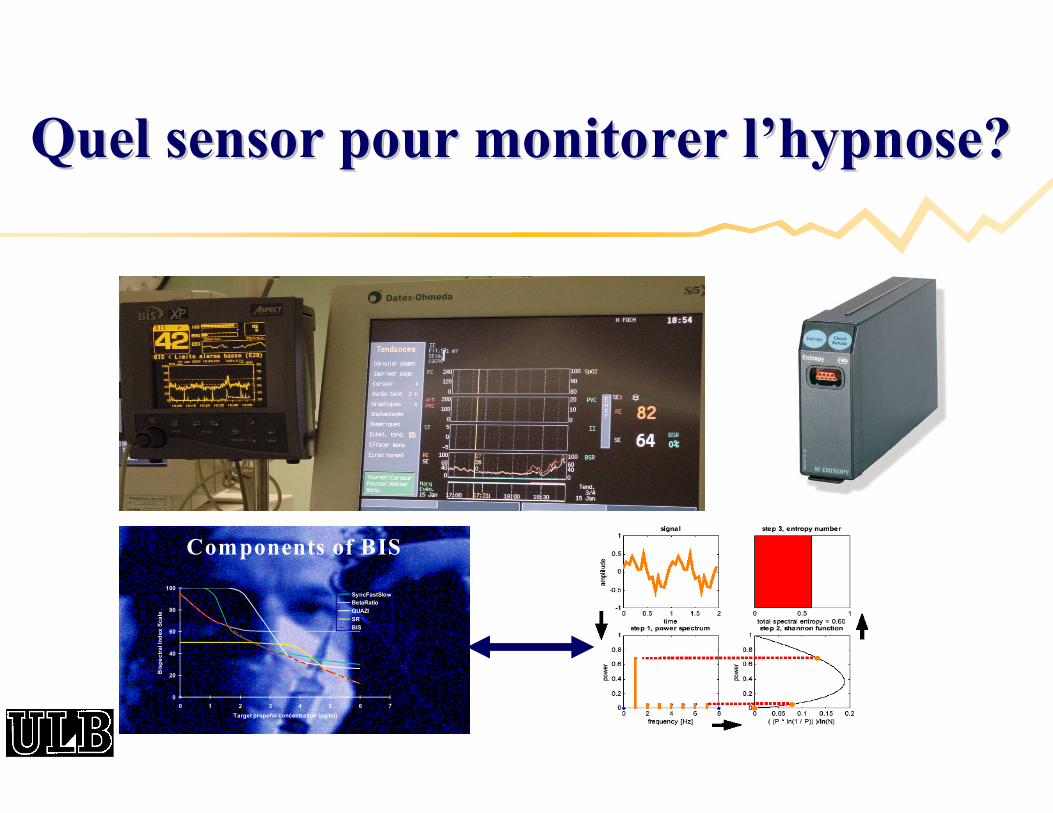
Quel sensor pour monitorer lQuel sensor pour monitorer l’’hypnose?hypnose?
0
20
40
60
80
100
0 1 2 3 4 5 6 7
Target propofol concentration (µg/ml)
Bis
pe
ctr
al In
dex
Sca
le
SyncFastSlowBetaRatio
QUAZI
SR
BIS
Components of BIS
Question : BIS Guided anaesthesia reduces the Question : BIS Guided anaesthesia reduces the incidence of awareness during surgery in adults ?incidence of awareness during surgery in adults ?
Prospective, randomised, doubleProspective, randomised, double--blind, multicentre blind, multicentre trial in high risk adult patients under relaxant GAtrial in high risk adult patients under relaxant GA
Caesarean SectionCaesarean Section
EF < 30%, CI < 2.1 L/min/mEF < 30%, CI < 2.1 L/min/m²², pulm. HT, pulm. HT
OFFOFF--pump, Aortic Stenosispump, Aortic Stenosis
BIS to prevent awareness during anaesthesia: BIS to prevent awareness during anaesthesia:
the Bthe B--Aware randomised controlled trialAware randomised controlled trial
Myles et al, Lancet 2004; 48(1): 20Myles et al, Lancet 2004; 48(1): 20--2626
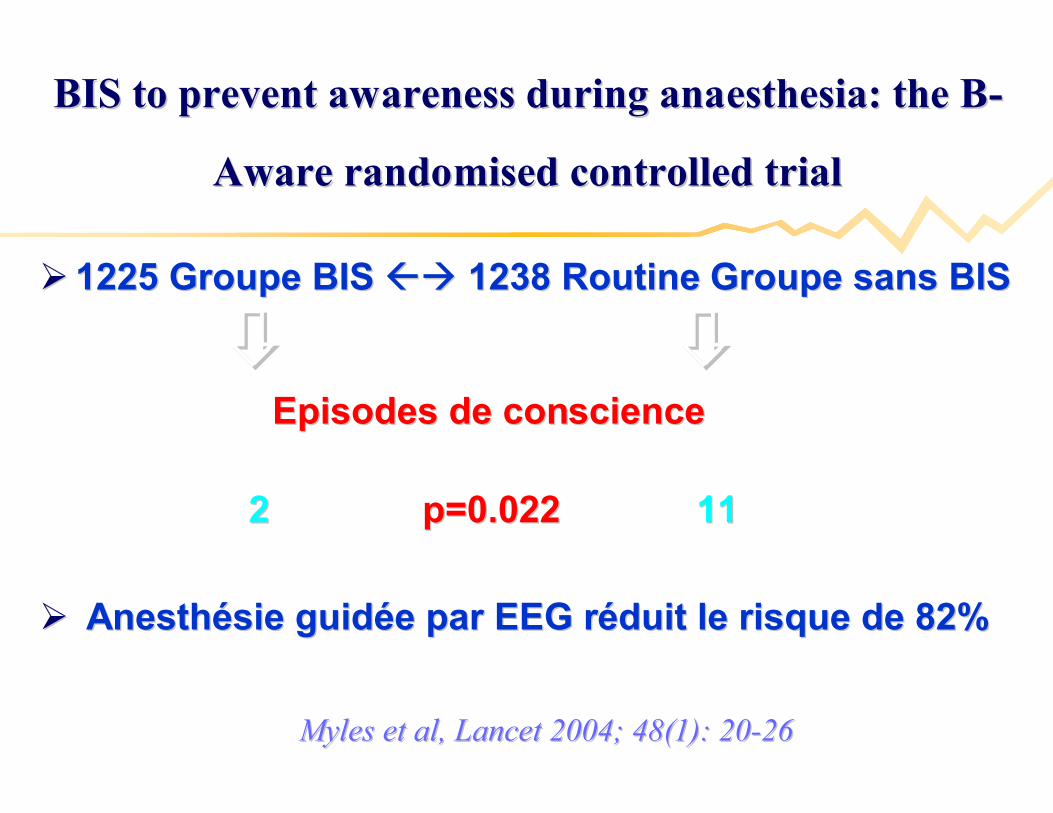
1225 Groupe BIS 1225 Groupe BIS 1238 Routine Groupe sans BIS1238 Routine Groupe sans BIS
Episodes de conscienceEpisodes de conscience
2 2 p=0.022p=0.022 1111
AnesthAnesthéésie guidsie guidéée par EEG re par EEG rééduit le risque de 82%duit le risque de 82%
BIS to prevent awareness during anaesthesia: the BBIS to prevent awareness during anaesthesia: the B--
Aware randomised controlled trialAware randomised controlled trial
Myles et al, Lancet 2004; 48(1): 20Myles et al, Lancet 2004; 48(1): 20--2626
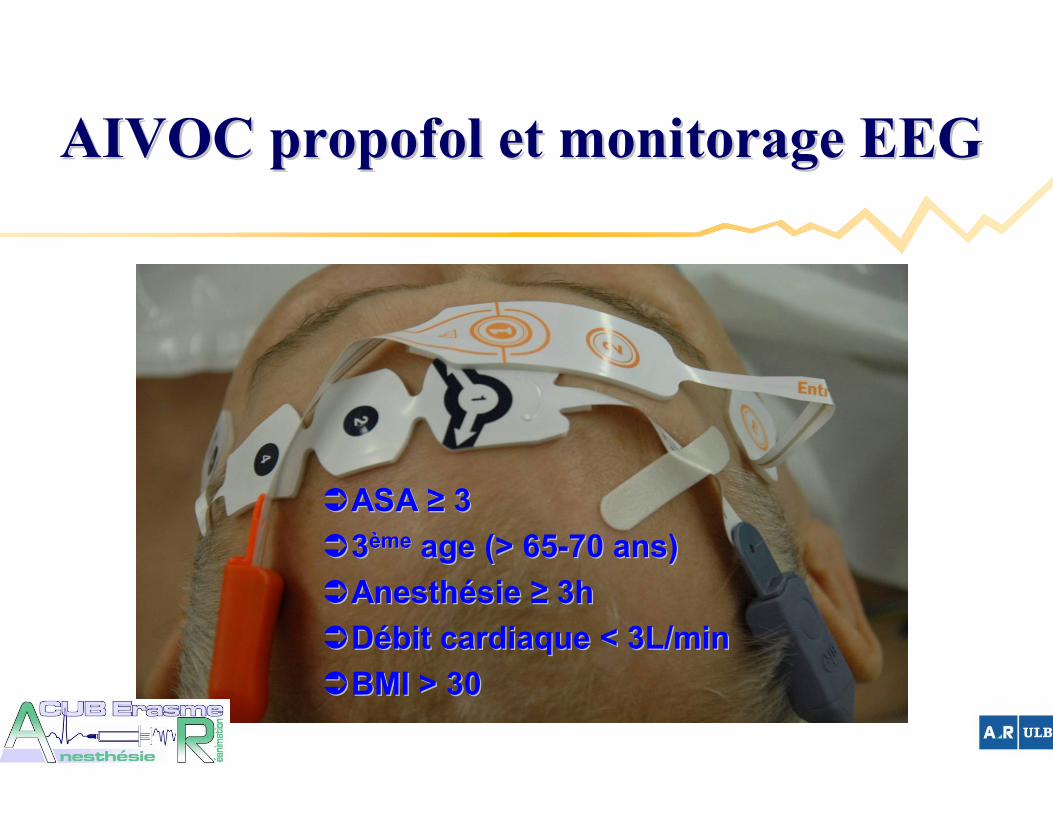
AIVOC propofol et monitorage EEGAIVOC propofol et monitorage EEG
ASA ASA ≥≥ 3 3
33èèmeme age (> 65age (> 65--70 ans)70 ans)
AnesthAnesthéésie sie ≥≥ 3h 3h
DDéébit cardiaque < 3L/minbit cardiaque < 3L/min
BMI > 30BMI > 30
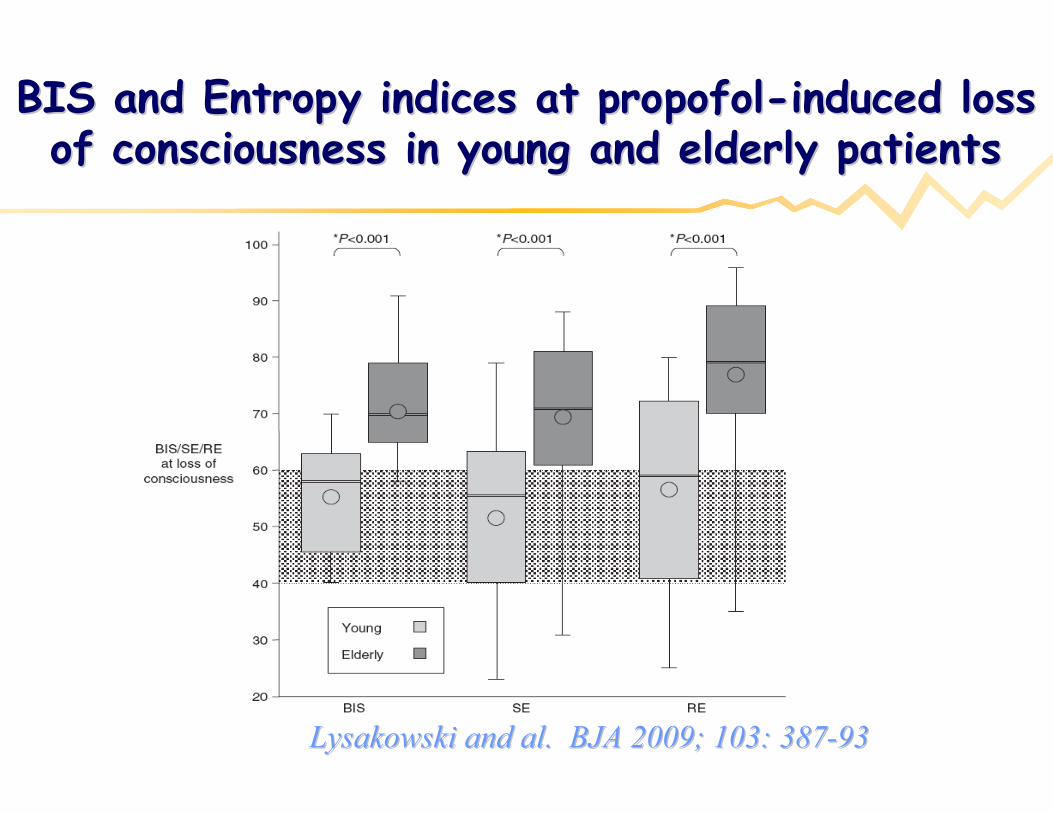
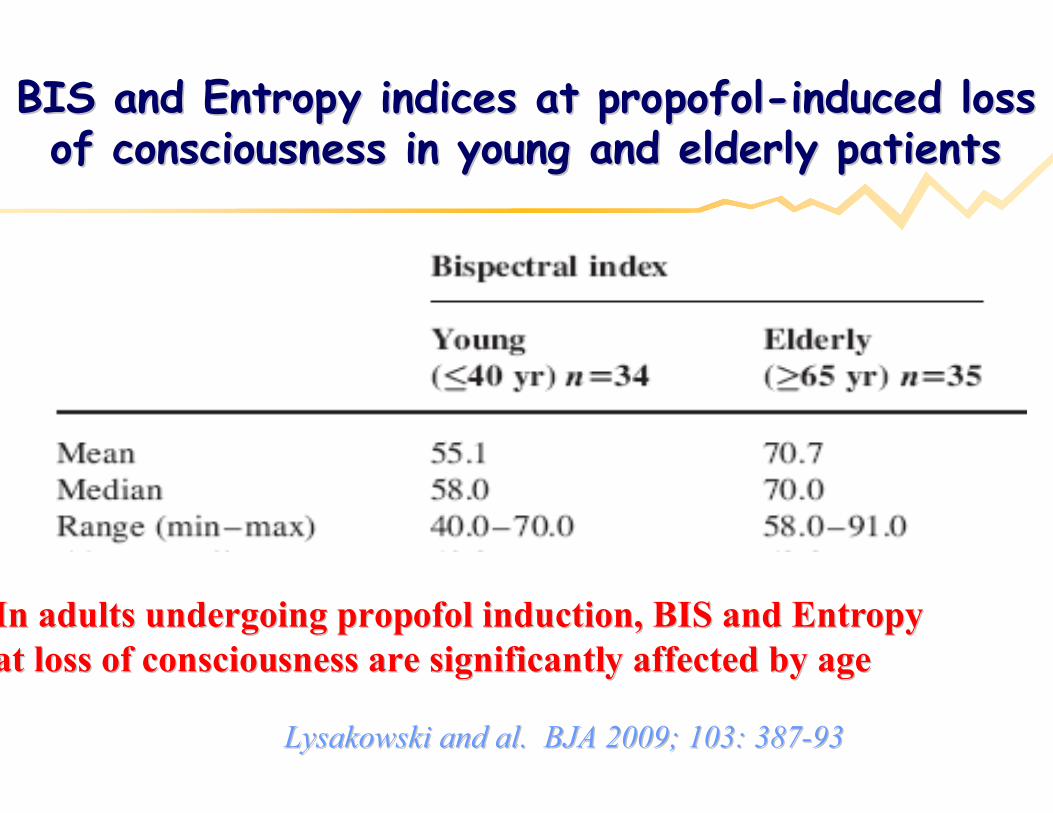
BIS and Entropy indices at propofolBIS and Entropy indices at propofol--induced loss induced loss of consciousness in young and elderly patientsof consciousness in young and elderly patients
Lysakowski and al. BJA 2009; 103: 387Lysakowski and al. BJA 2009; 103: 387--9393
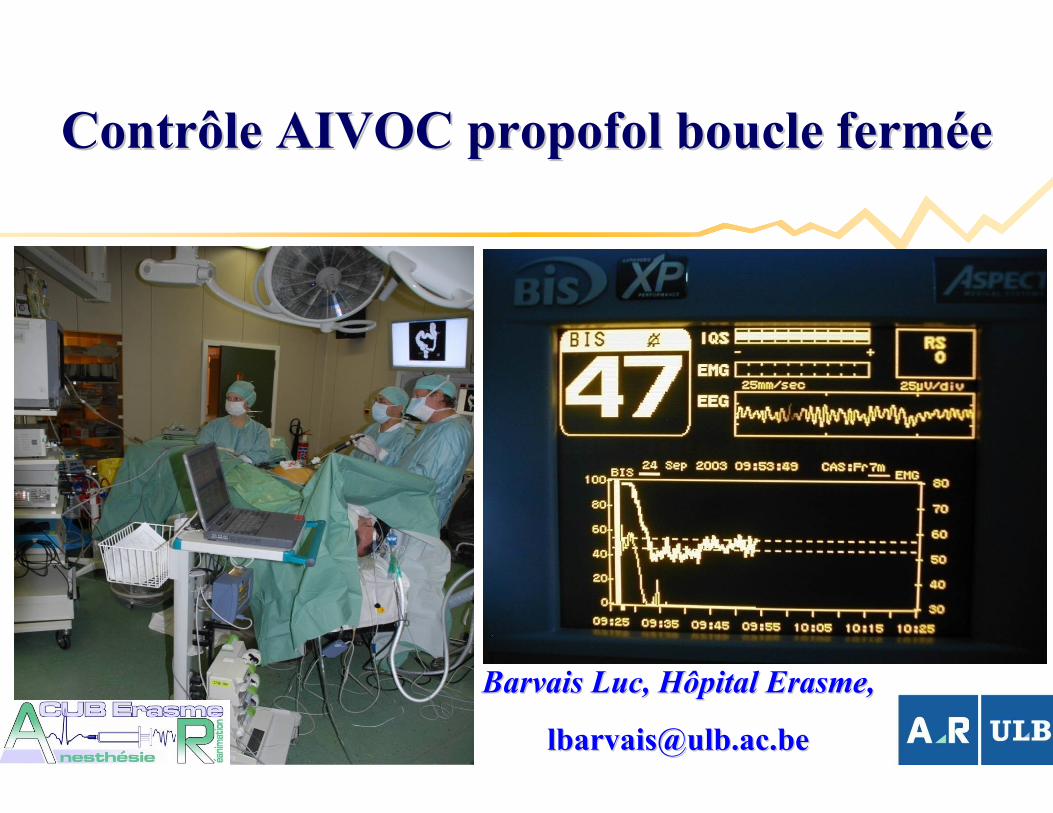
Contrôle AIVOC propofol boucle fermContrôle AIVOC propofol boucle fermééee
Barvais Luc, Hôpital ErasmeBarvais Luc, Hôpital Erasme,,
[email protected]@ulb.ac.be
BIS and Entropy indices at propofolBIS and Entropy indices at propofol--induced loss induced loss of consciousness in young and elderly patientsof consciousness in young and elderly patients
Lysakowski and al. BJA 2009; 103: 387Lysakowski and al. BJA 2009; 103: 387--9393
In adults undergoing propofol induction, BIS and EntropyIn adults undergoing propofol induction, BIS and Entropyat loss of consciousness are significantly affected by ageat loss of consciousness are significantly affected by age
AVANTAGES AIVOCAVANTAGES AIVOC
• AIVOC = prédiction concentrations site action / Halogénés = monitoring concentration expiratoire
• Aussi simple à utiliser qu’un vaporisateur
• Titration indépendante hypnotiques et analgésiques
AVANTAGES TIVAAVANTAGES TIVA
Contrôle sédation avant induction
Moins de pollution Qop et environnement
Pas hépatite
Beaucoup moins de nausées vomissements
Accès airway non lié administration anesthésie
Continuité sédation postopératoire
Réflexe vasoconstriction hypoxique maintenue
Sécurité >> risque hyperthermie maligne
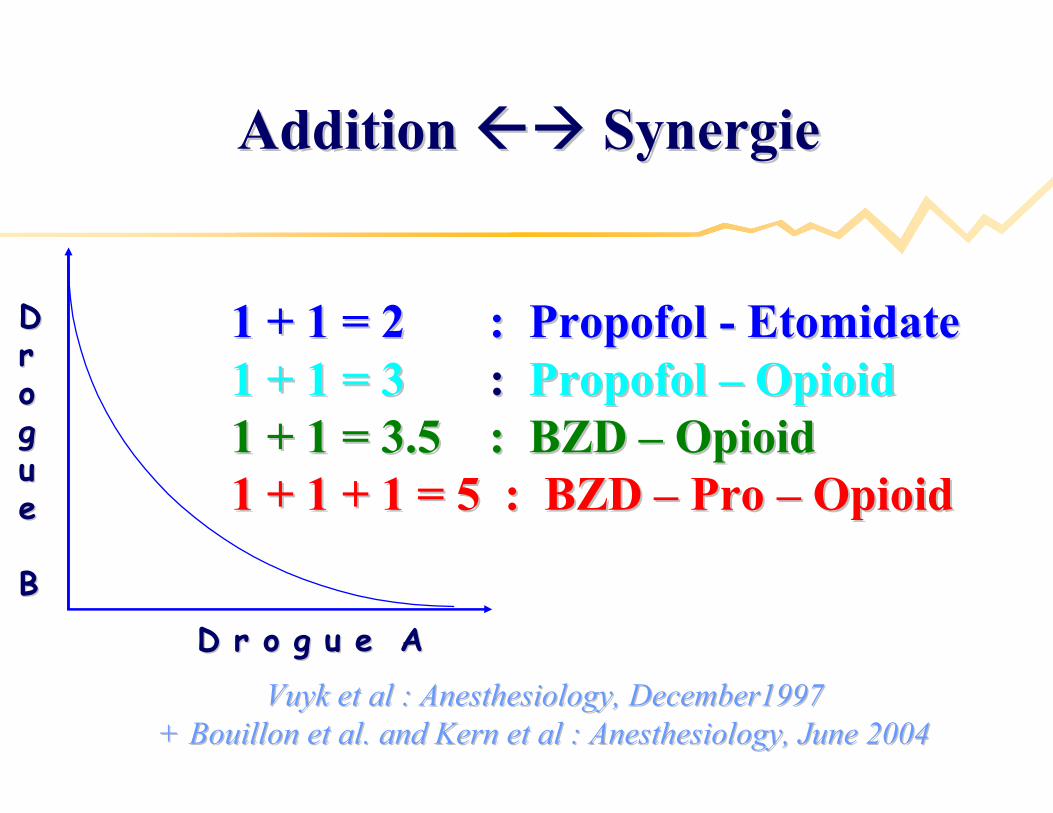
Addition Addition Synergie Synergie
Vuyk et al : Vuyk et al : Anesthesiology, December1997Anesthesiology, December1997+ Bouillon et al. and Kern et al : Anesthesiology, June 2004+ Bouillon et al. and Kern et al : Anesthesiology, June 2004
1 + 1 = 2 : Propofol 1 + 1 = 2 : Propofol -- EtomidateEtomidate1 + 1 = 31 + 1 = 3 : : Propofol Propofol –– OpioidOpioid1 + 1 = 3.5 : BZD 1 + 1 = 3.5 : BZD –– OpioidOpioid1 + 1 + 1 = 5 : BZD 1 + 1 + 1 = 5 : BZD –– Pro Pro –– OpioidOpioid
D r o g u e AD r o g u e A
DDrroogguuee
BB
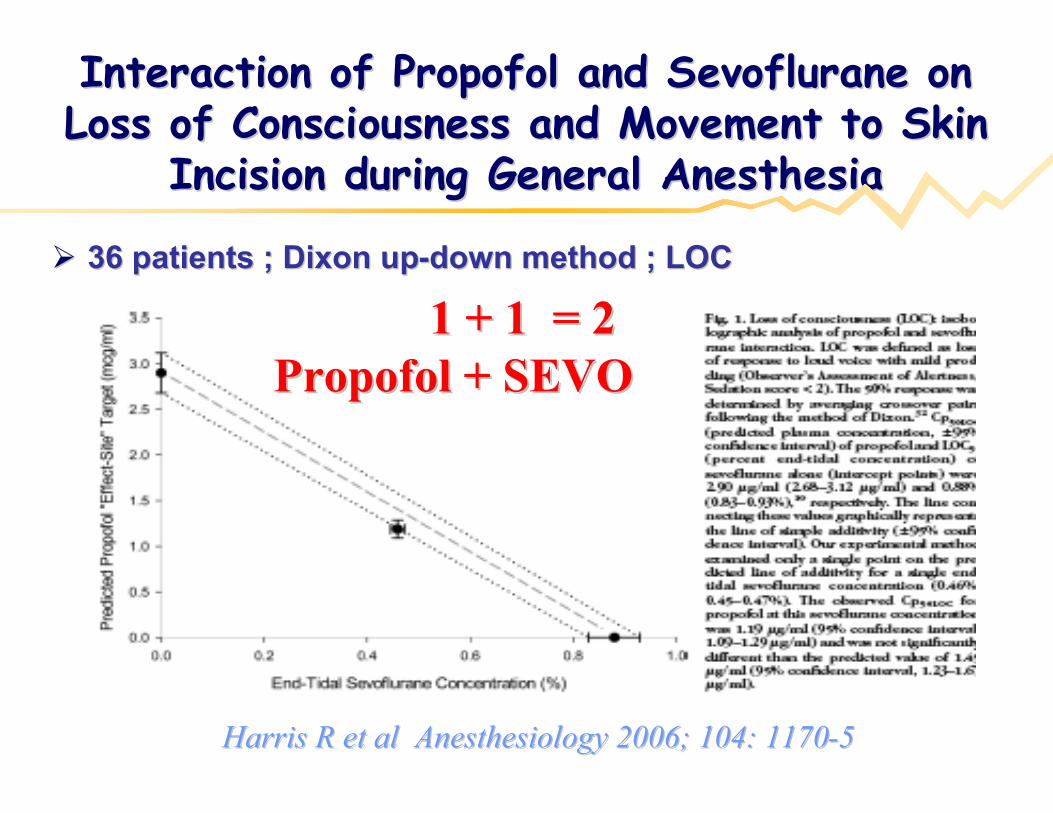
Interaction of Propofol and Sevoflurane on Interaction of Propofol and Sevoflurane on Loss of Consciousness and Movement to Skin Loss of Consciousness and Movement to Skin
Incision during General AnesthesiaIncision during General Anesthesia
36 patients ; Dixon up36 patients ; Dixon up--down method ; LOCdown method ; LOC
Harris R et al Anesthesiology 2006; 104: 1170Harris R et al Anesthesiology 2006; 104: 1170--55
1 + 1 = 2 1 + 1 = 2 Propofol + SEVOPropofol + SEVO
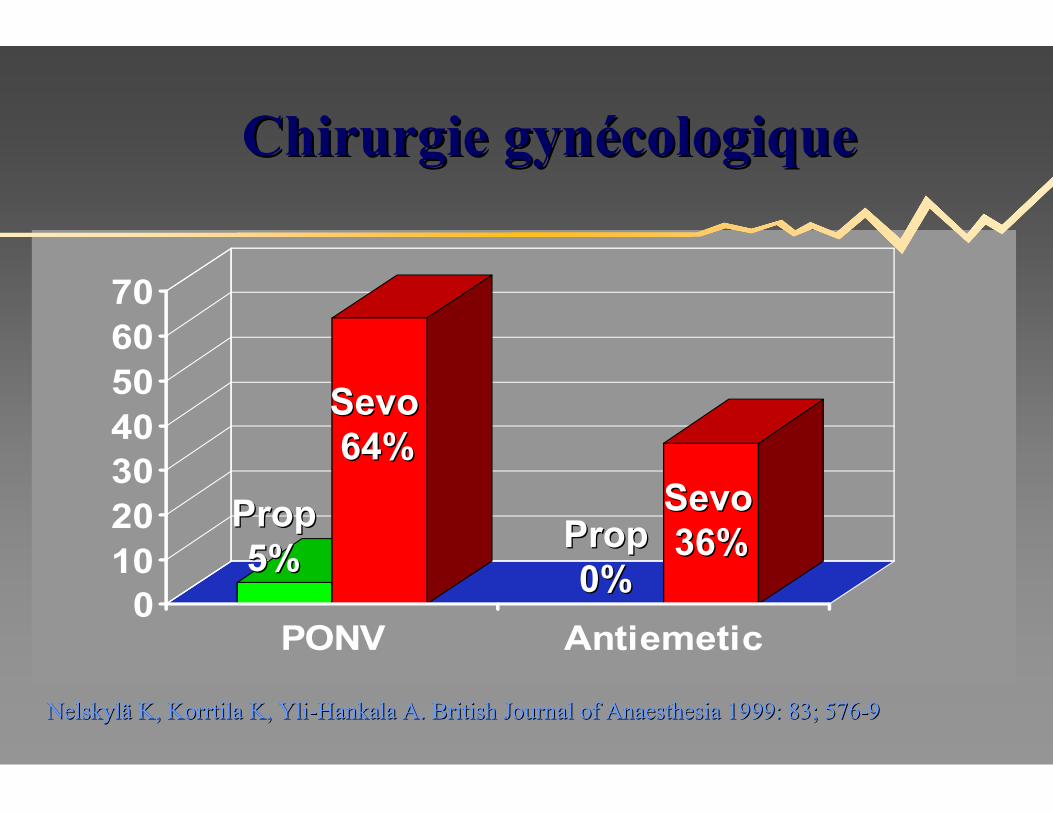
010203040506070
PONV Antiemetic
Chirurgie gynChirurgie gynéécologiquecologique
SevoSevo64%64%
SevoSevo36%36%
PropProp5%5%
PropProp0%0%
NelskylNelskylää K, Korrtila K, YliK, Korrtila K, Yli--Hankala A. British Journal of Anaesthesia 1999: 83; 576Hankala A. British Journal of Anaesthesia 1999: 83; 576--99
PONVPONV

AIVOC = AnesthAIVOC = Anesthéésie Intraveineuse sie Intraveineuse Objectif ConcentrationObjectif Concentration

MerciMerci
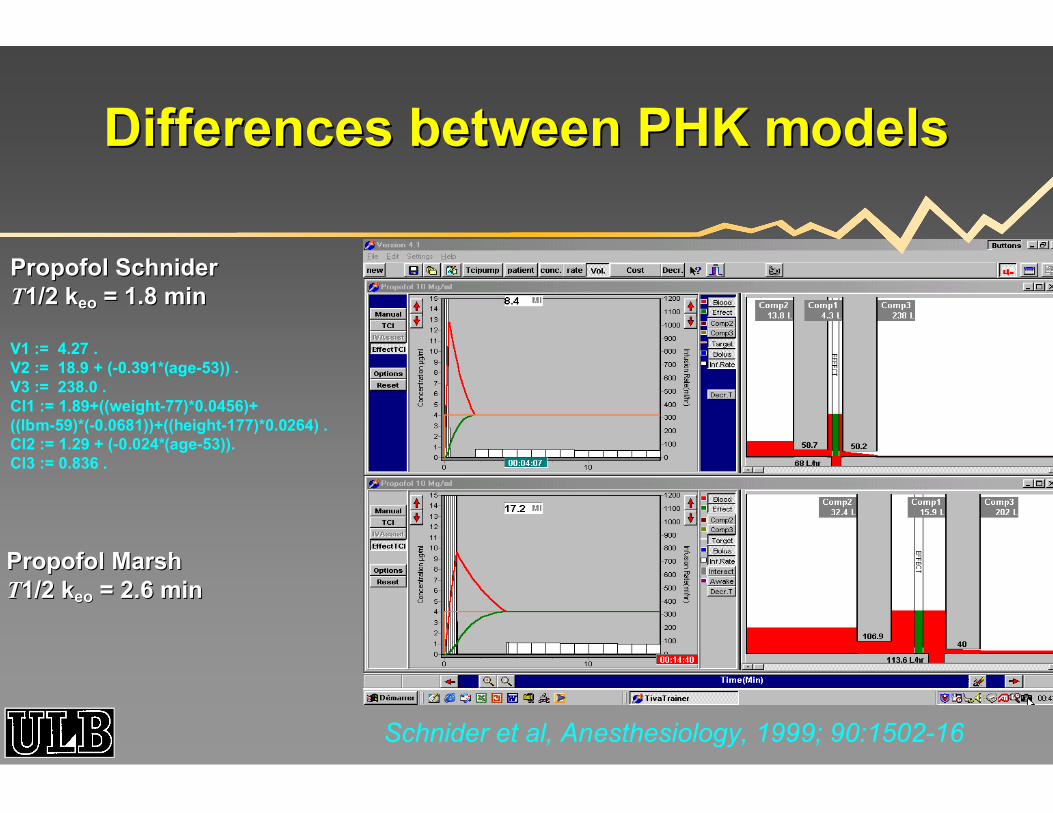
Differences between PHK modelsDifferences between PHK models
Propofol SchniderPropofol SchniderTT1/2 k1/2 keoeo = 1.8 min= 1.8 min
V1 := 4.27 . V2 := 18.9 + (-0.391*(age-53)) . V3 := 238.0 .Cl1 := 1.89+((weight-77)*0.0456)+((lbm-59)*(-0.0681))+((height-177)*0.0264) .Cl2 := 1.29 + (-0.024*(age-53)).Cl3 := 0.836 .
Propofol MarshPropofol MarshTT1/2 k1/2 keoeo = 2.6 min= 2.6 min
Schnider et al, Anesthesiology, 1999; 90:1502-16
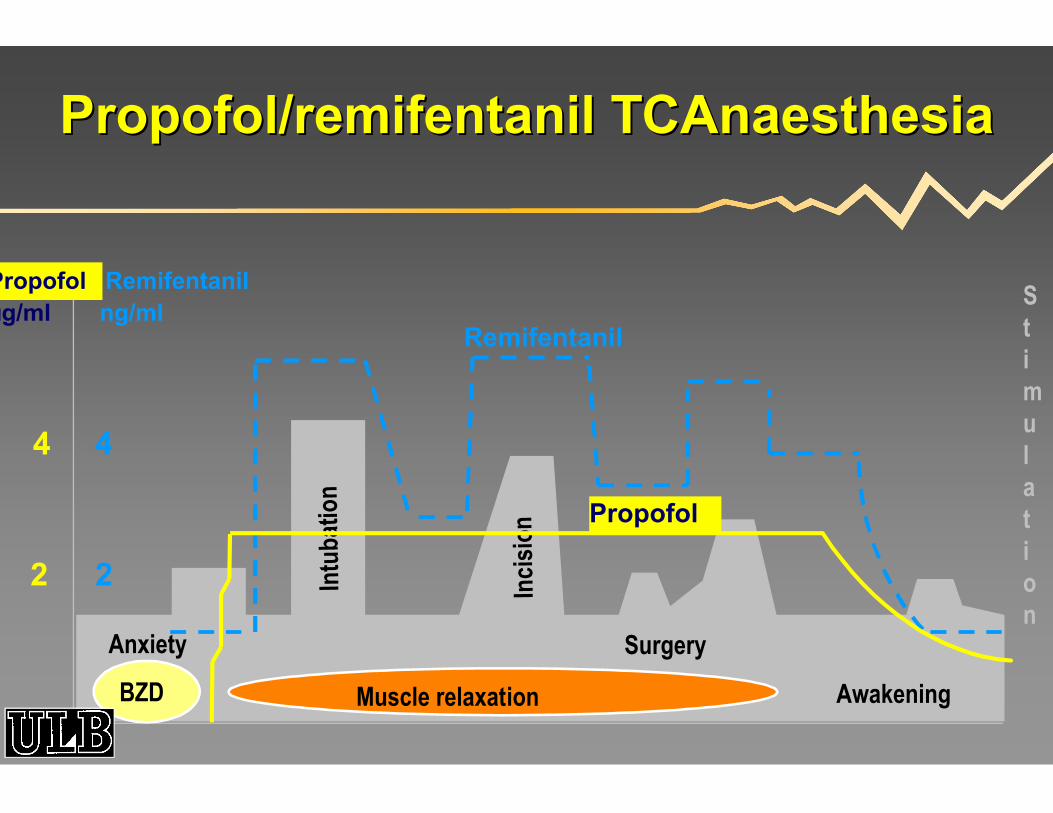
Surgery
Stimulation
Intu
batio
n
Inci
sion
Awakening
Remifentanil
Propofol
Muscle relaxationBZD
2 2
4 4
Anxiety
Propofol/remifentanil TCAnaesthesiaPropofol/remifentanil TCAnaesthesia
Propofol Remifentanilµg/ml ng/ml
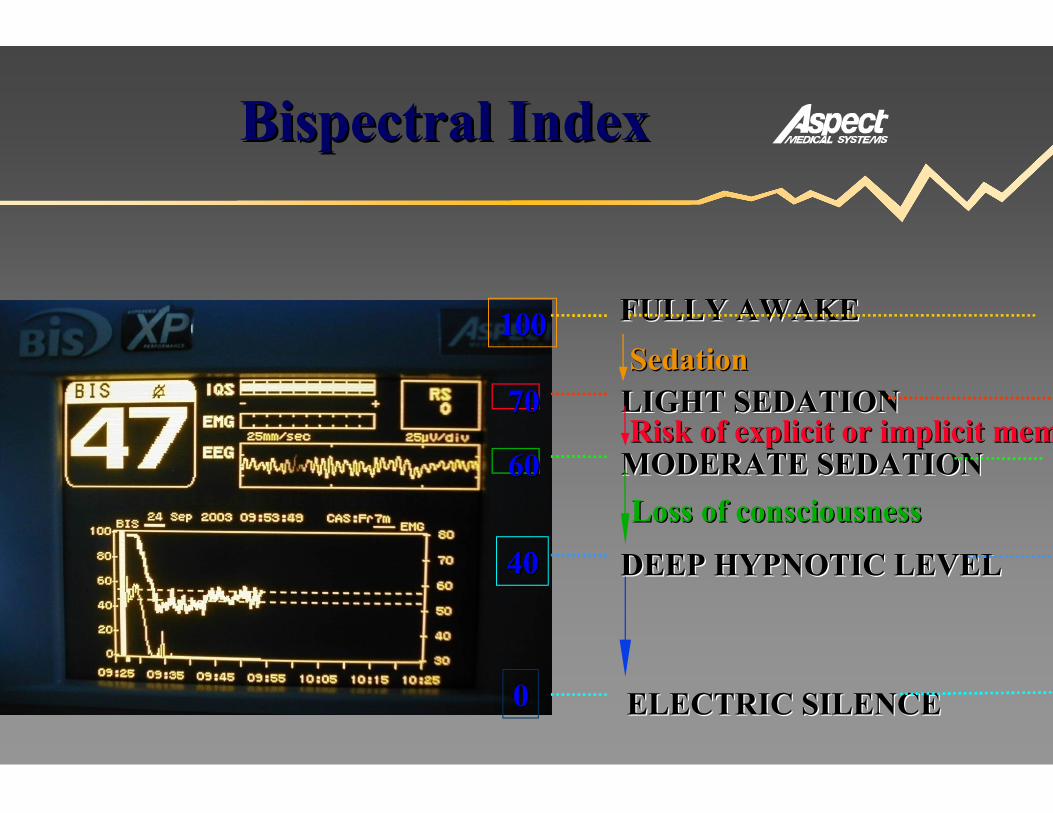
Bispectral IndexBispectral Index
100100
7070
6060
4040
00
LIGHT SEDATIONLIGHT SEDATION
ELECTRIC SILENCEELECTRIC SILENCE
Risk of explicit or implicit memoryRisk of explicit or implicit memory
Loss of consciousnessLoss of consciousness
SedationSedation
FULLY AWAKEFULLY AWAKE
MODERATE SEDATIONMODERATE SEDATION
DEEP HYPNOTIC LEVELDEEP HYPNOTIC LEVEL
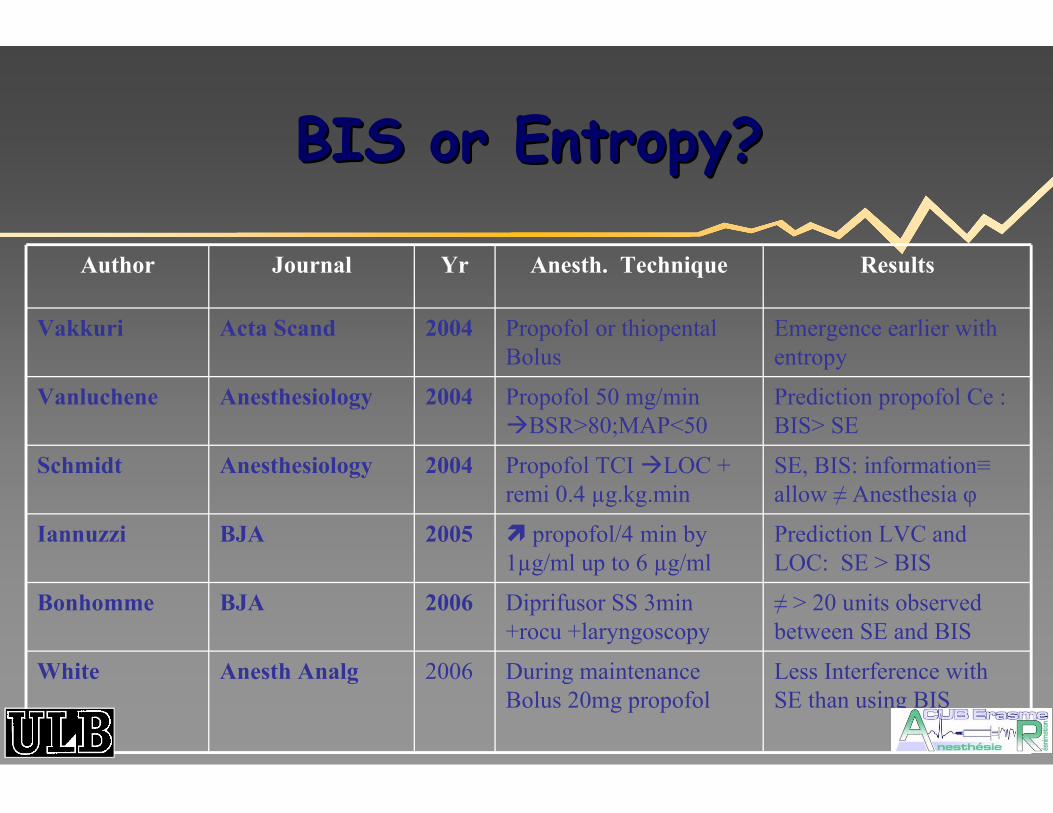
BIS or Entropy?BIS or Entropy?
Author Journal Yr Anesth. Technique Results
Vakkuri Acta Scand 2004 Propofol or thiopental Bolus
Emergence earlier with entropy
Vanluchene Anesthesiology 2004 Propofol 50 mg/min BSR>80;MAP<50
Prediction propofol Ce : BIS> SE
Schmidt Anesthesiology 2004 Propofol TCI LOC + remi 0.4 µg.kg.min
SE, BIS: information≡allow ≠ Anesthesia φ
Iannuzzi BJA 2005 propofol/4 min by 1µg/ml up to 6 µg/ml
Prediction LVC and LOC: SE > BIS
Bonhomme BJA 2006 Diprifusor SS 3min +rocu +laryngoscopy
≠ > 20 units observed between SE and BIS
White Anesth Analg 2006 During maintenance Bolus 20mg propofol
Less Interference with SE than using BIS
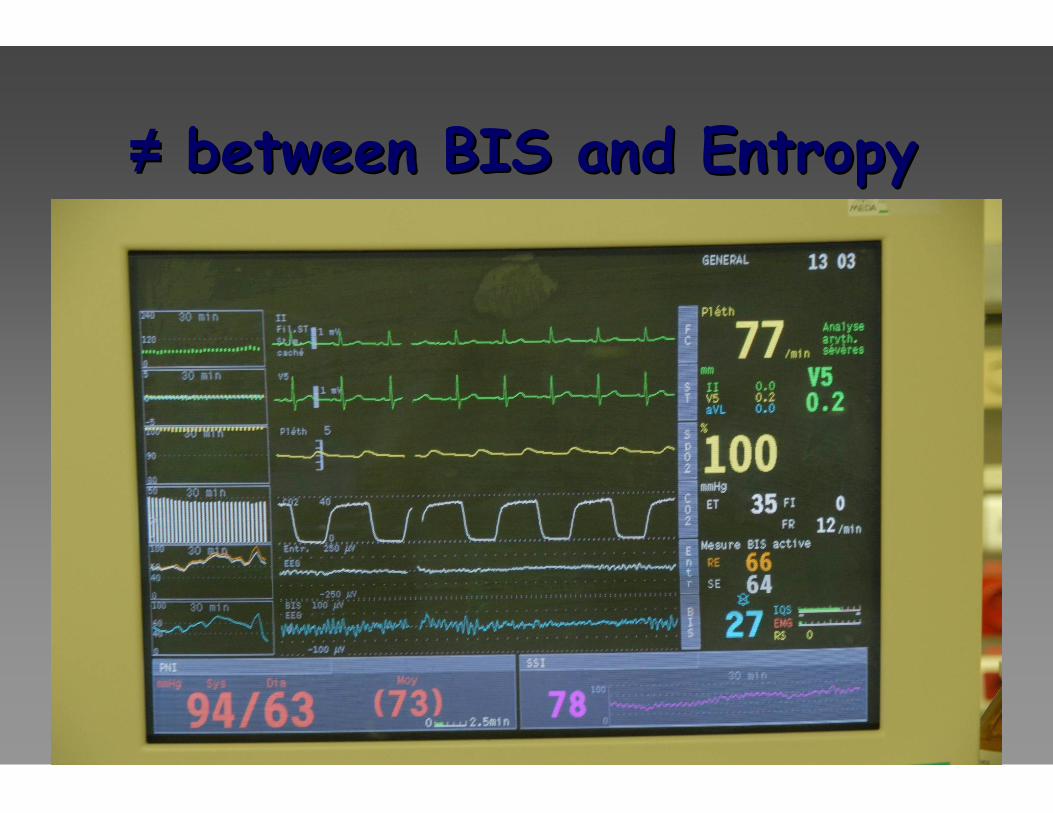
≠≠ between BIS and Entropybetween BIS and Entropy

Duration Duration of actionof action
0
50
100
150
200
250
300
0 0,5 1 2 3 4 5 6 7 8 9
0
50
100
150
200
250
300
0 0,5 1 2 3 4 5 6 7 8 9
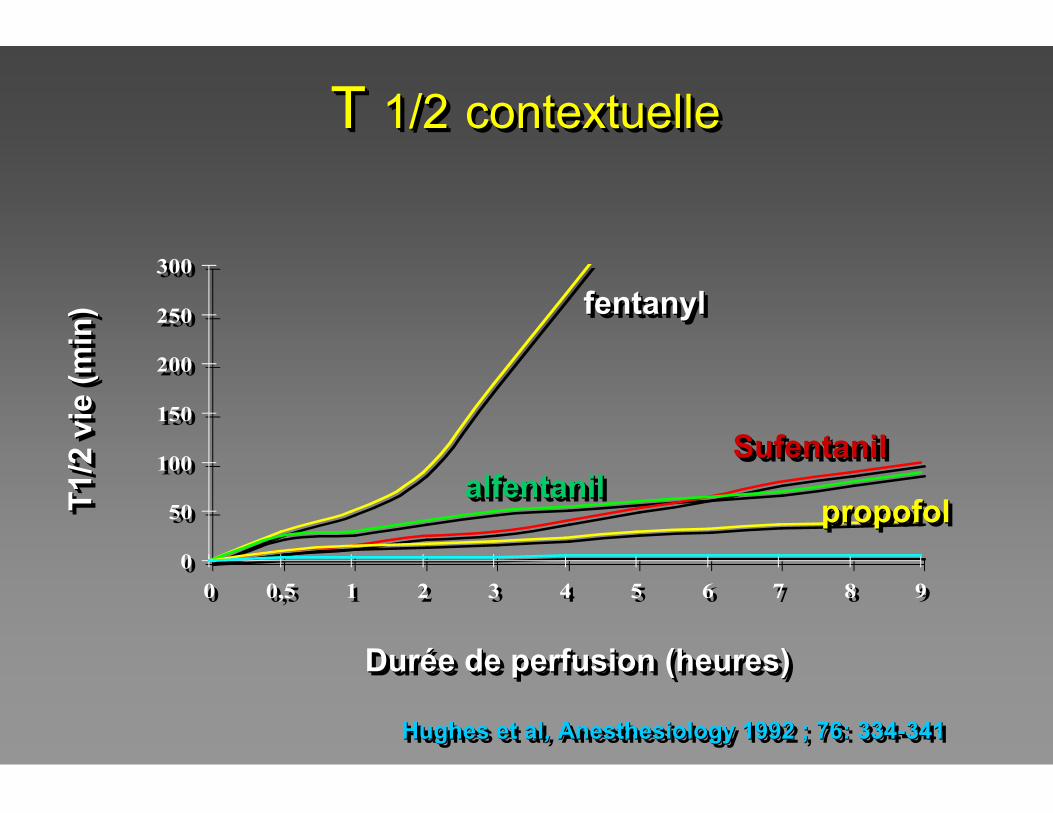
Durée de perfusion (heures)DurDuréée de perfusion (heures)e de perfusion (heures)
fentanylfentanylfentanyl
SufentanilSufentanilSufentanilalfentanilalfentanilalfentanil
propofolpropofolpropofolT1
/2 v
ie (
min
)T
1/2
vie
(m
in)
T1
/2 v
ie (
min
)
Hughes et al, Anesthesiology 1992 ; 76: 334-341Hughes et alHughes et al, , Anesthesiology 1992 ; 76: 334Anesthesiology 1992 ; 76: 334--341341
T 1/2 contextuelleT T 1/21/2 contextuellecontextuelle
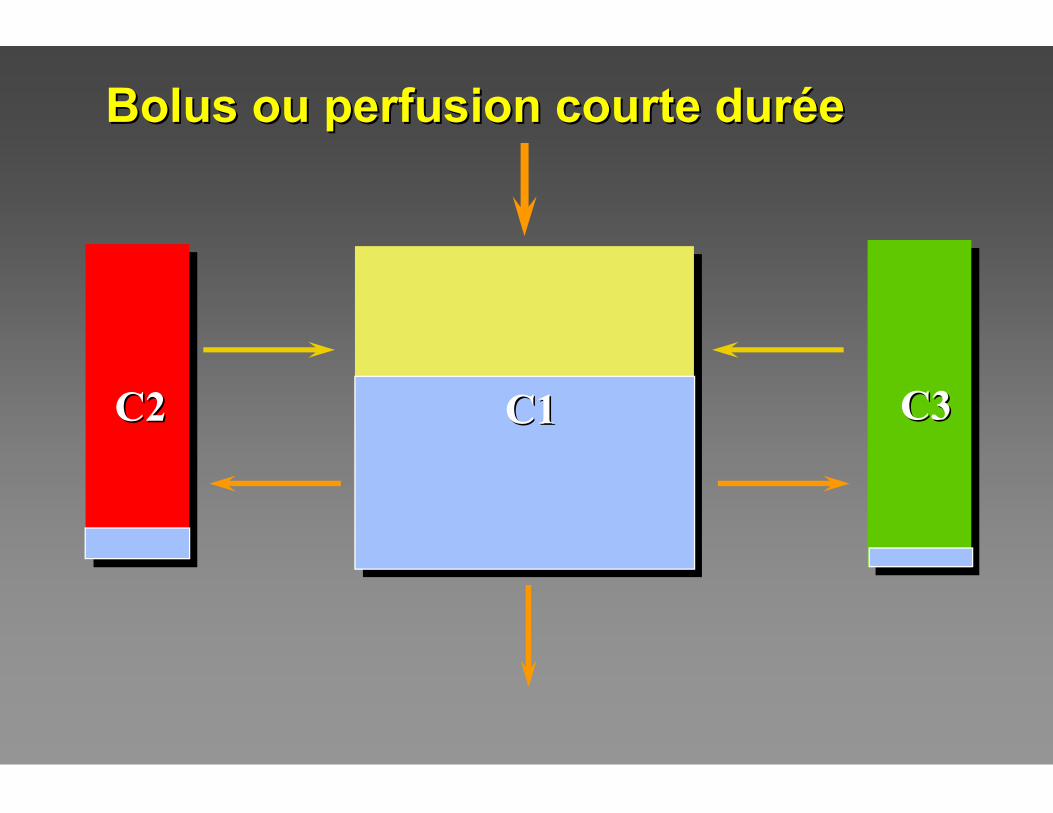
C3C3C2C2 C1C1
Bolus ou perfusion courte durBolus ou perfusion courte durééee
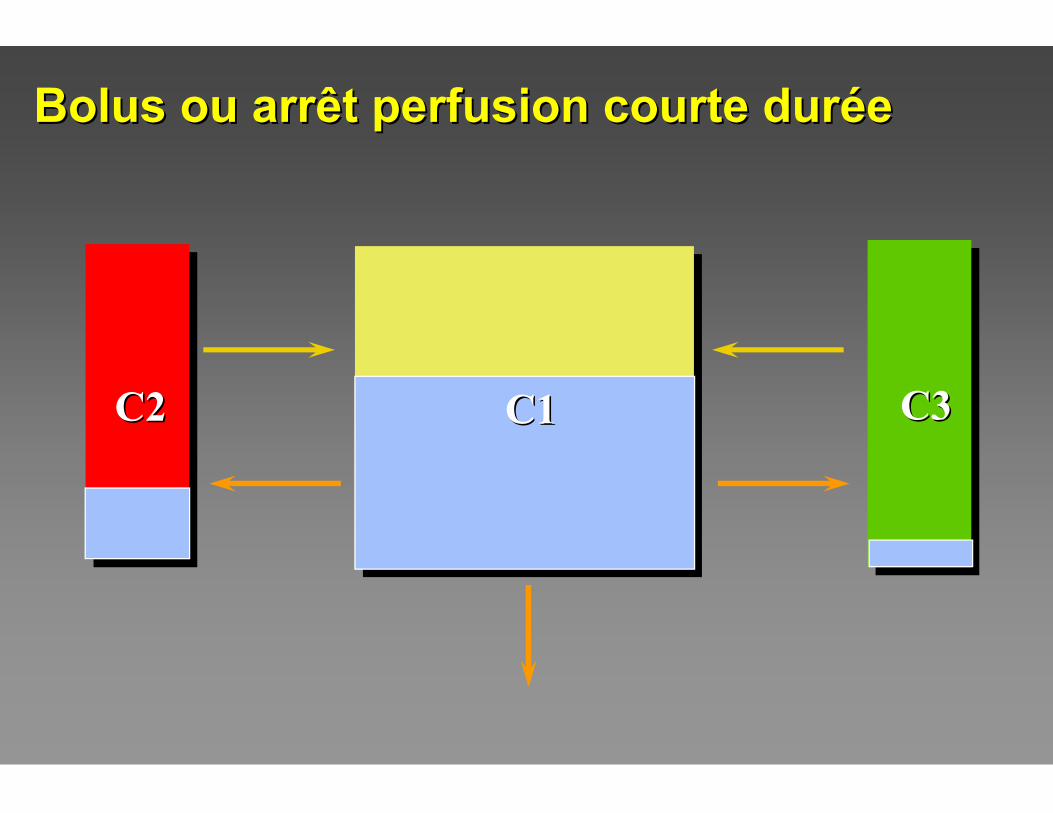
C3C3C2C2 C1C1
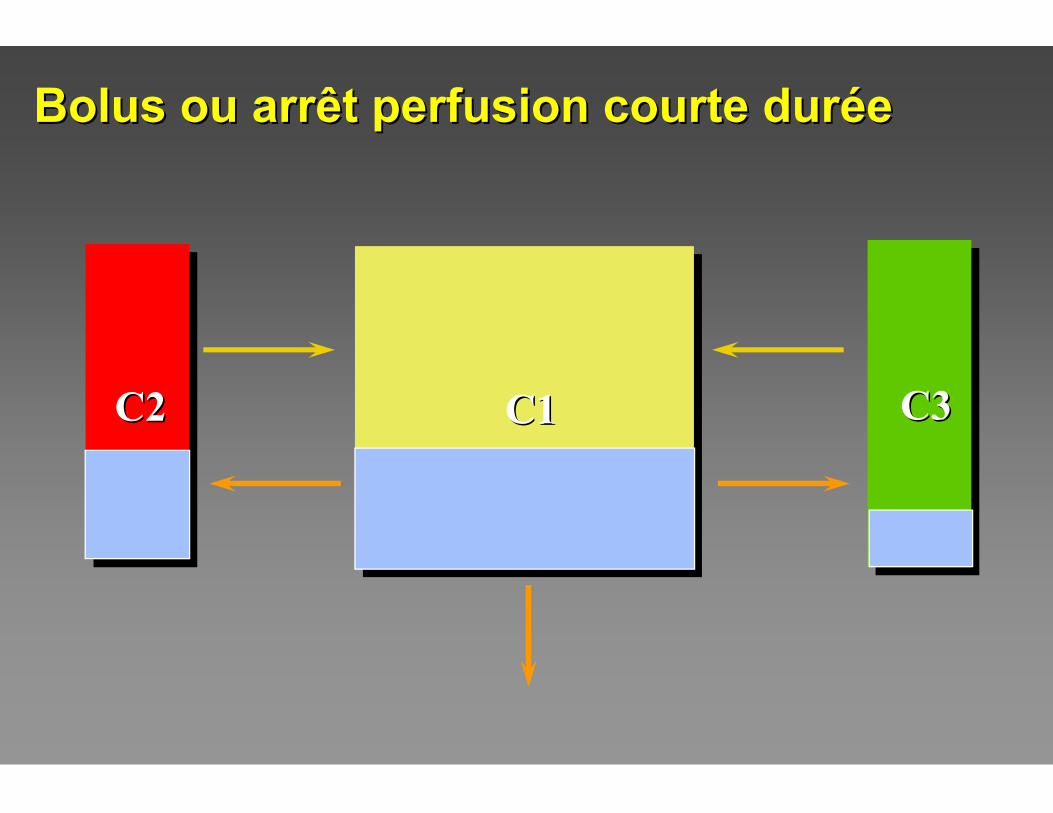
Bolus ou arrêt perfusion courte durBolus ou arrêt perfusion courte durééee
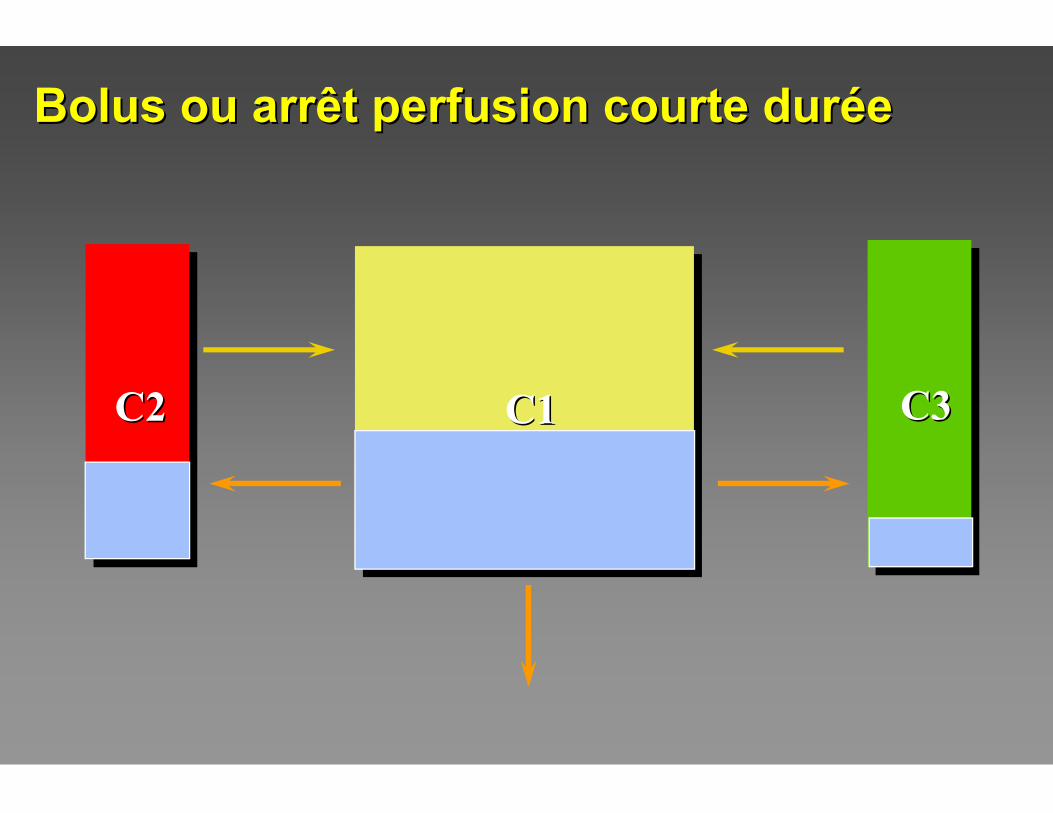
C3C3C2C2 C1C1
Bolus ou arrêt perfusion courte durBolus ou arrêt perfusion courte durééee
C3C3C2C2 C1C1
Bolus ou arrêt perfusion courte durBolus ou arrêt perfusion courte durééee
0
50
100
150
200
10 30 50 70 90 110
0
50
100
150
200
10 30 50 70 90 110
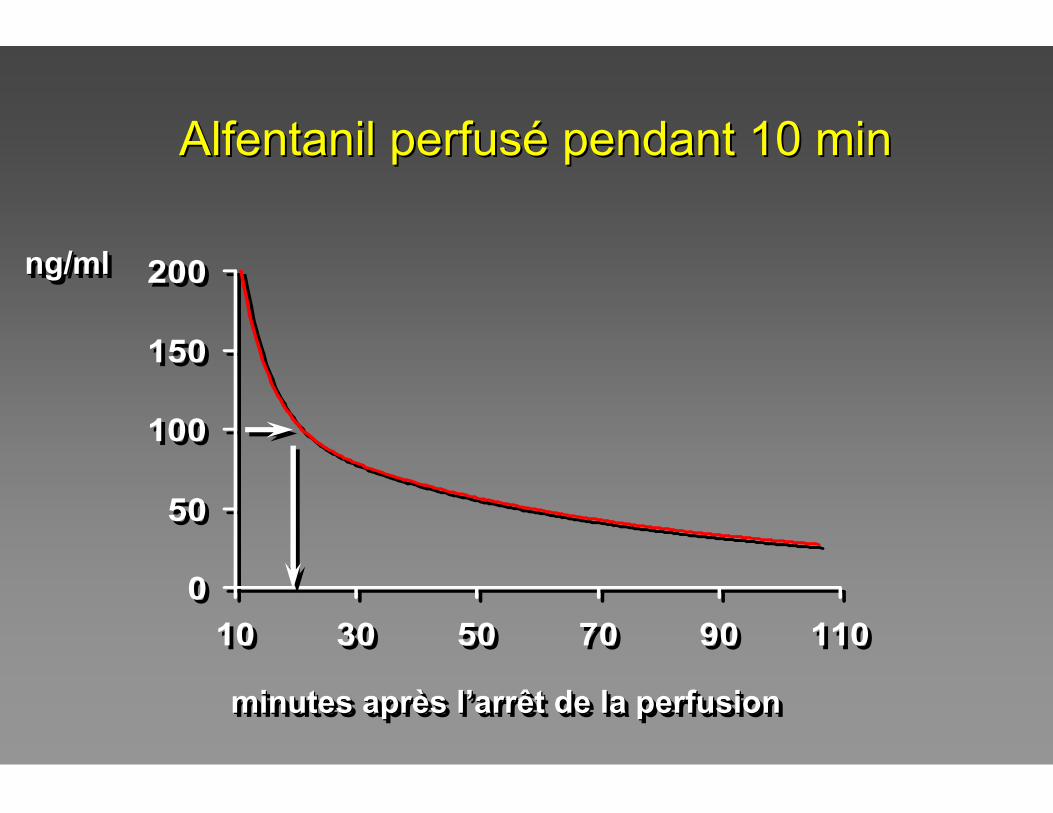
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
Alfentanil perfusAlfentanil perfuséé pendant 10 minpendant 10 min
C3C2C2 C1C1
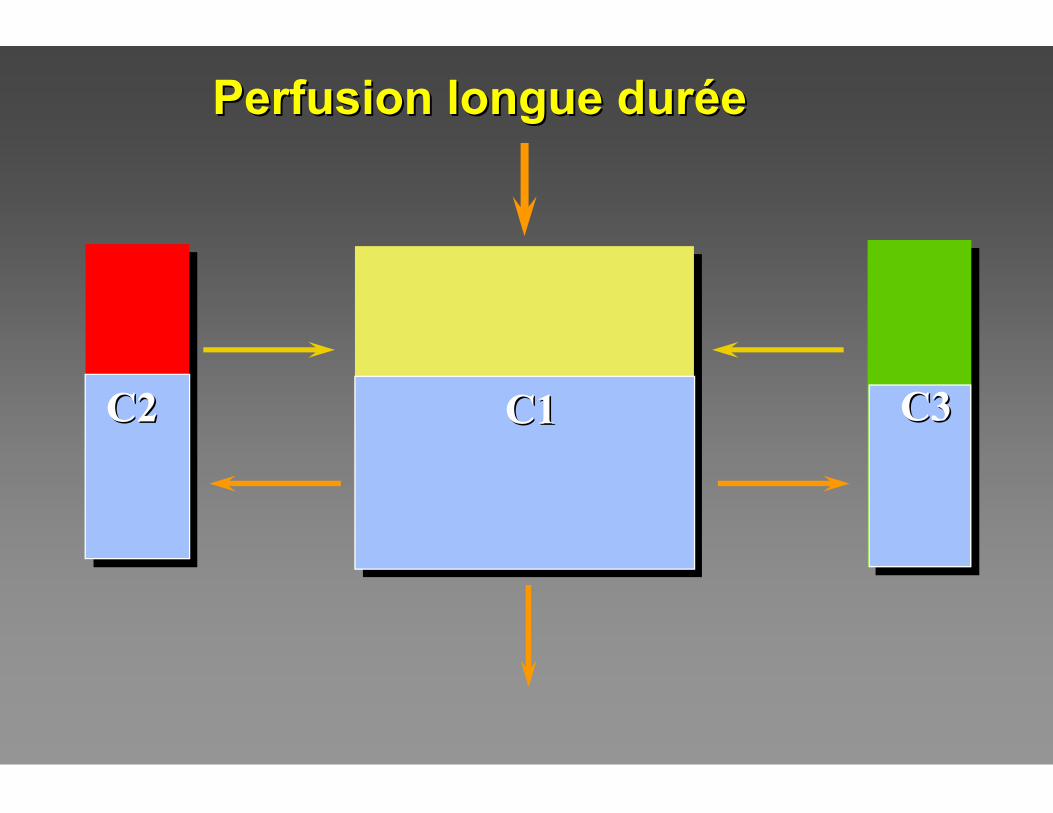
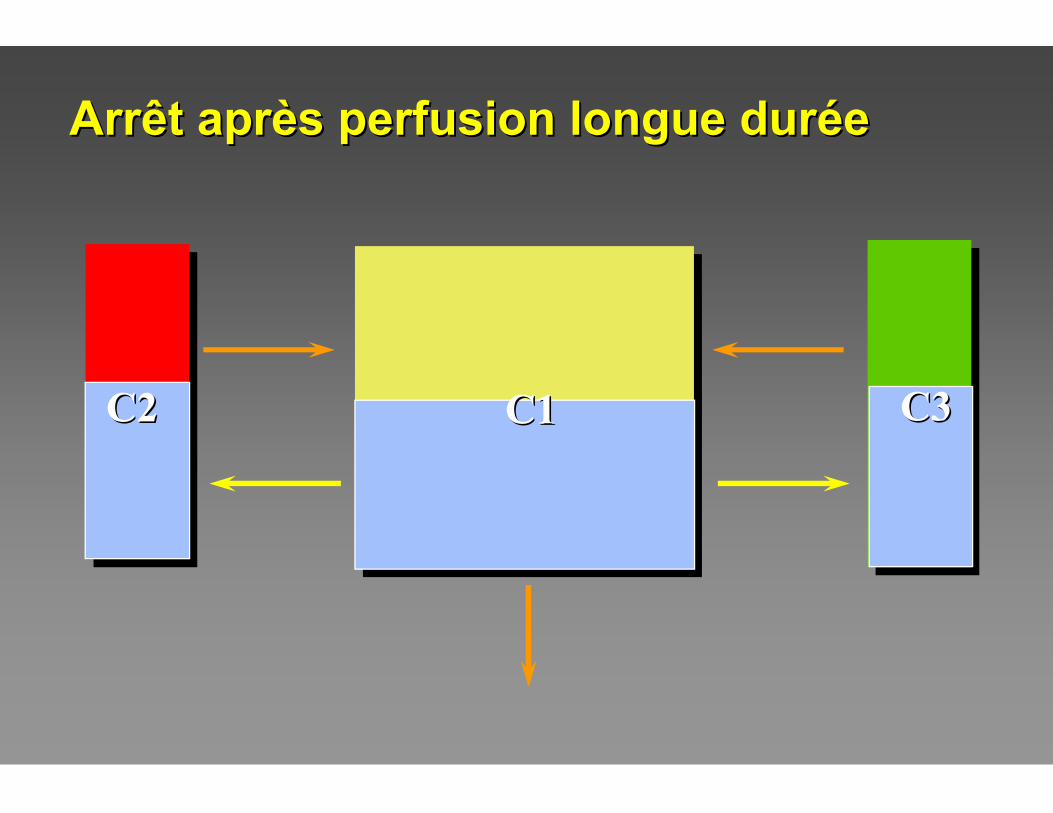
Perfusion longue durPerfusion longue duréée e
C3C3C2C2
C3C2C2 C1C1 C3C3C2C2
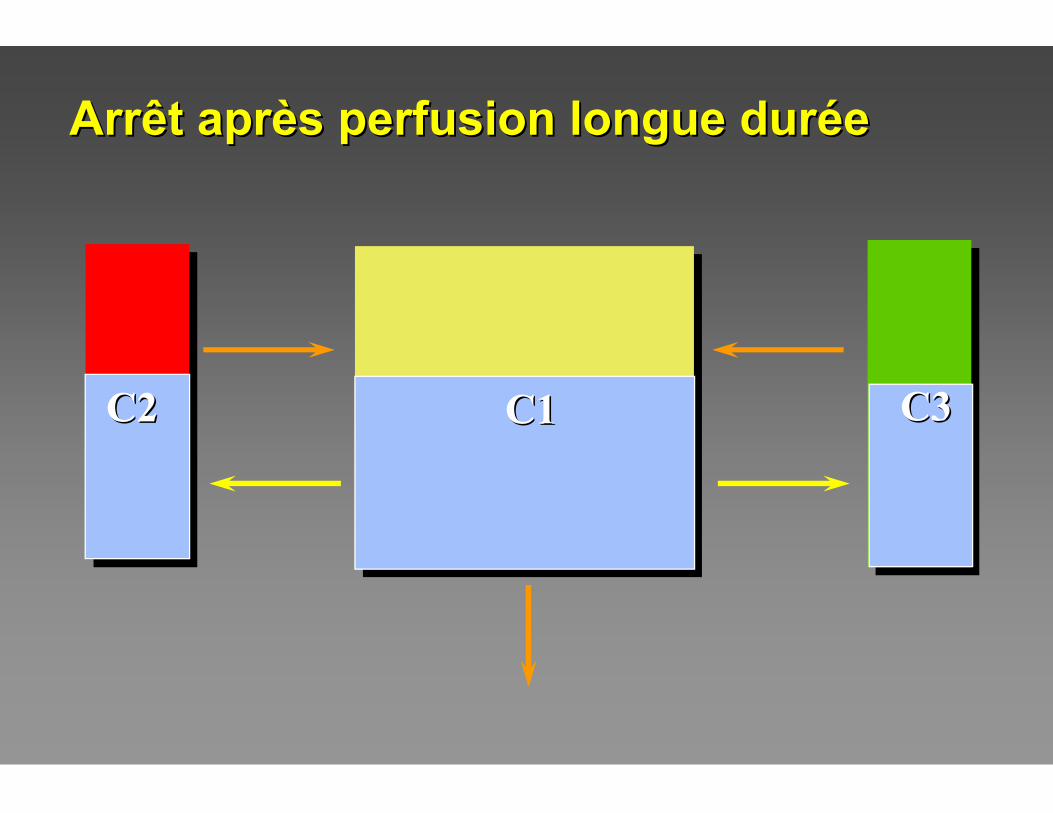
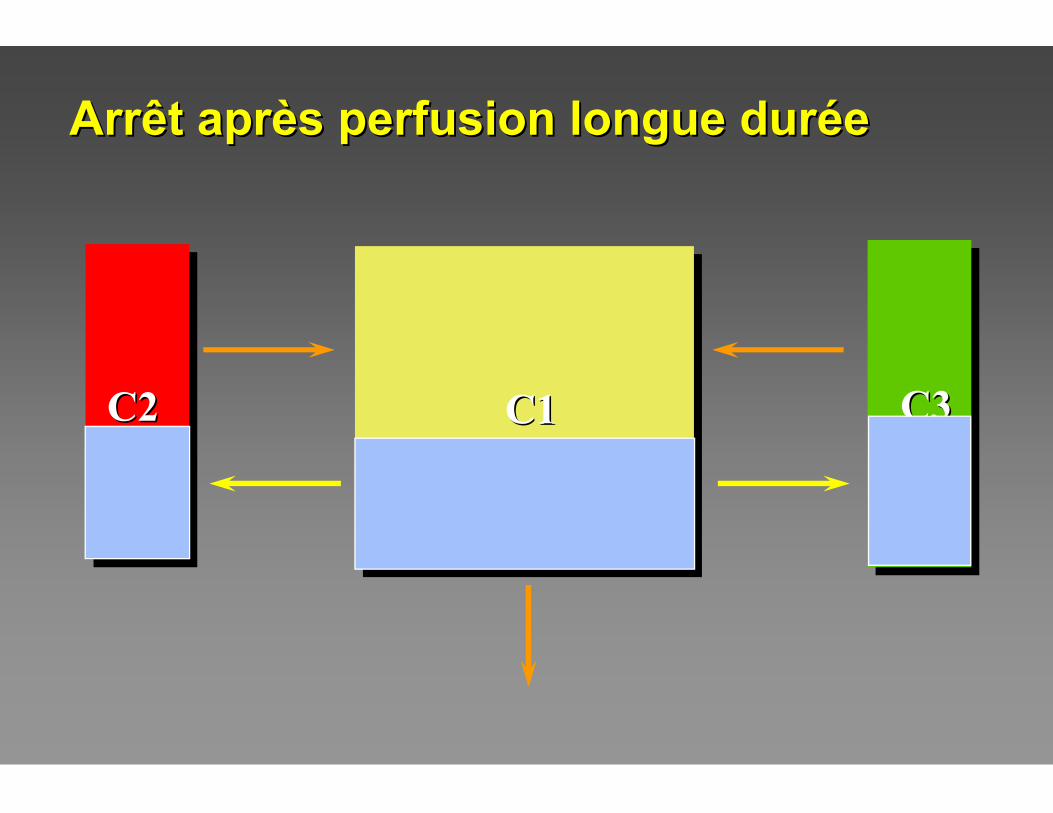
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
C3C2C2 C1C1C2C2 C3C3
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
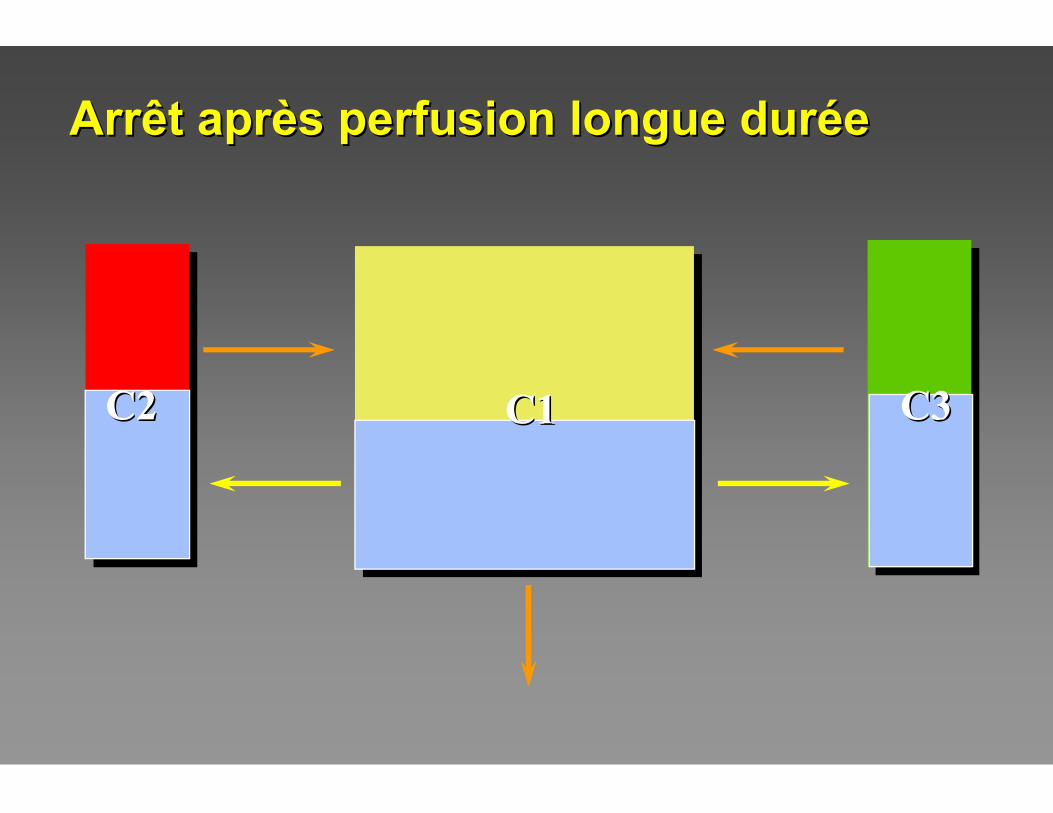
C2C2 C1C1C2C2 C3C3
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
C3C3C2C2 C1C1
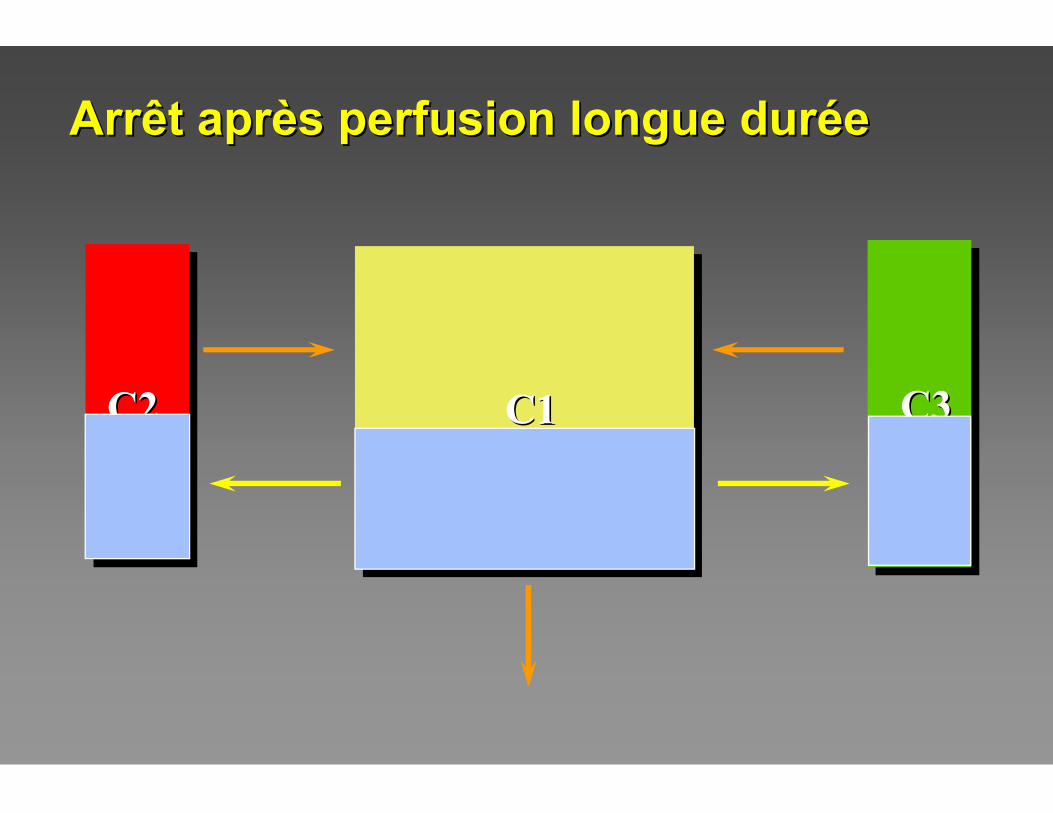
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
C3C3C2C2 C1C1
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
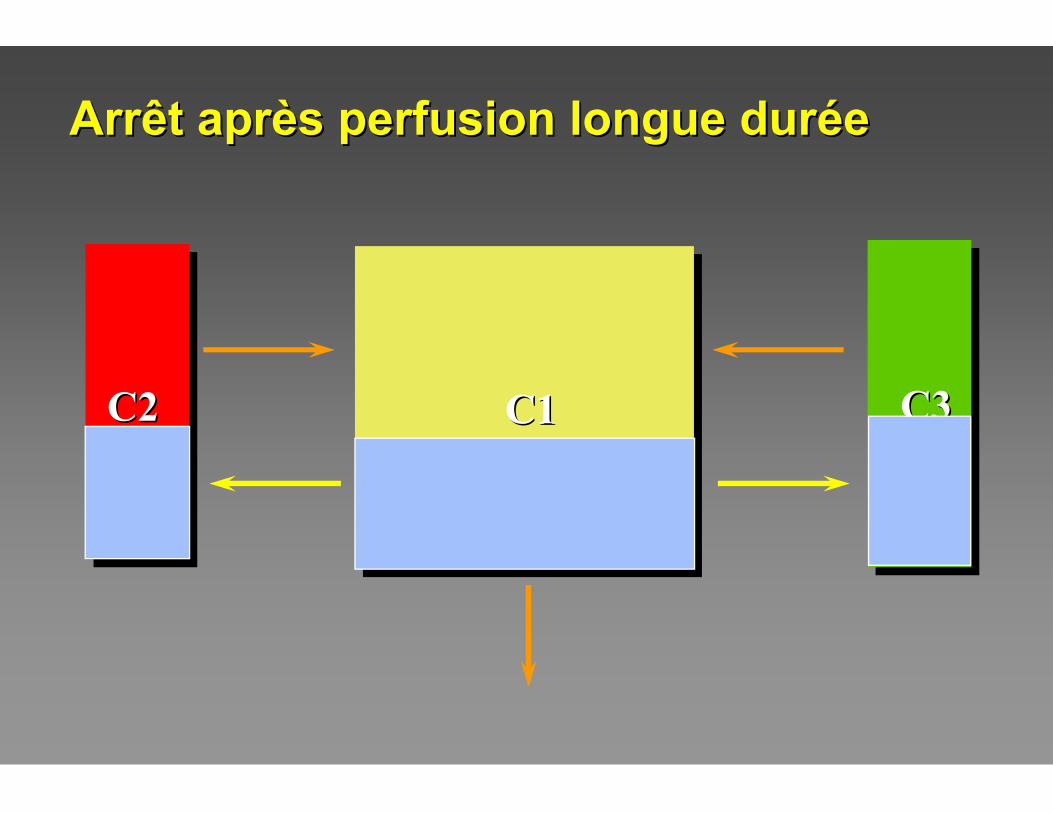
C3C3C2C2 C1C1
Arrêt aprArrêt aprèès perfusion longue durs perfusion longue duréée e
0
50
100
150
200
100 150 200 250 300 350
0
50
100
150
200
100 150 200 250 300 350
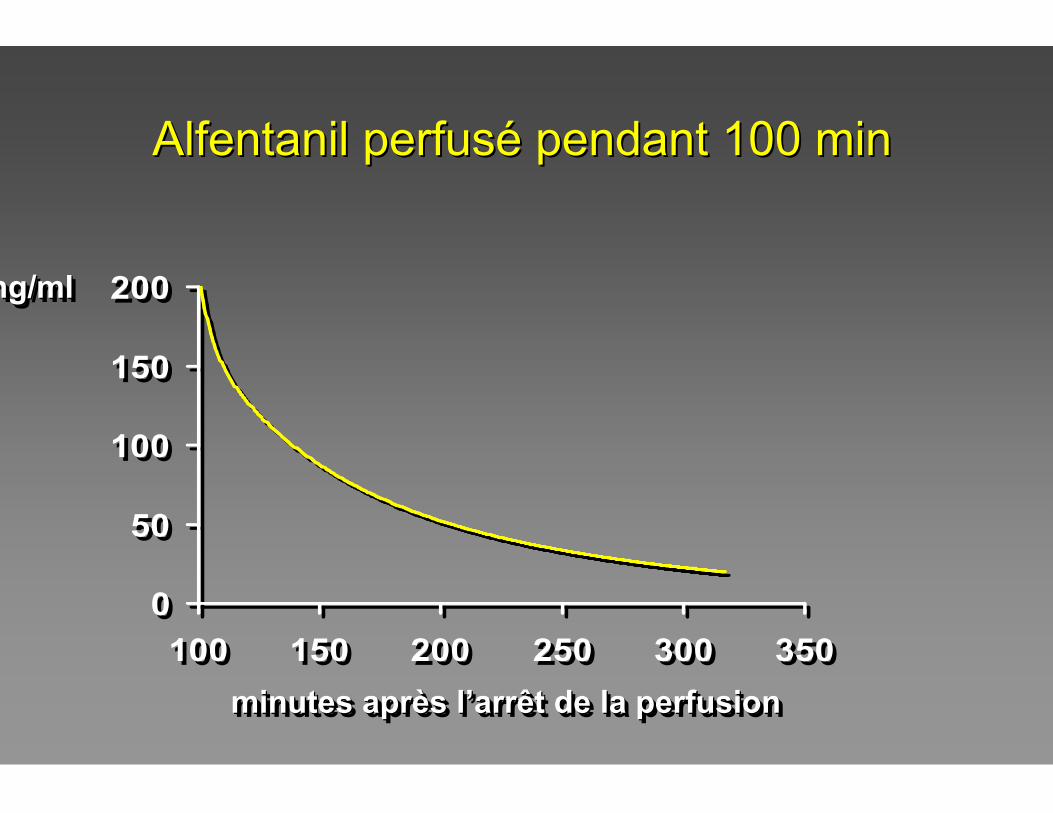
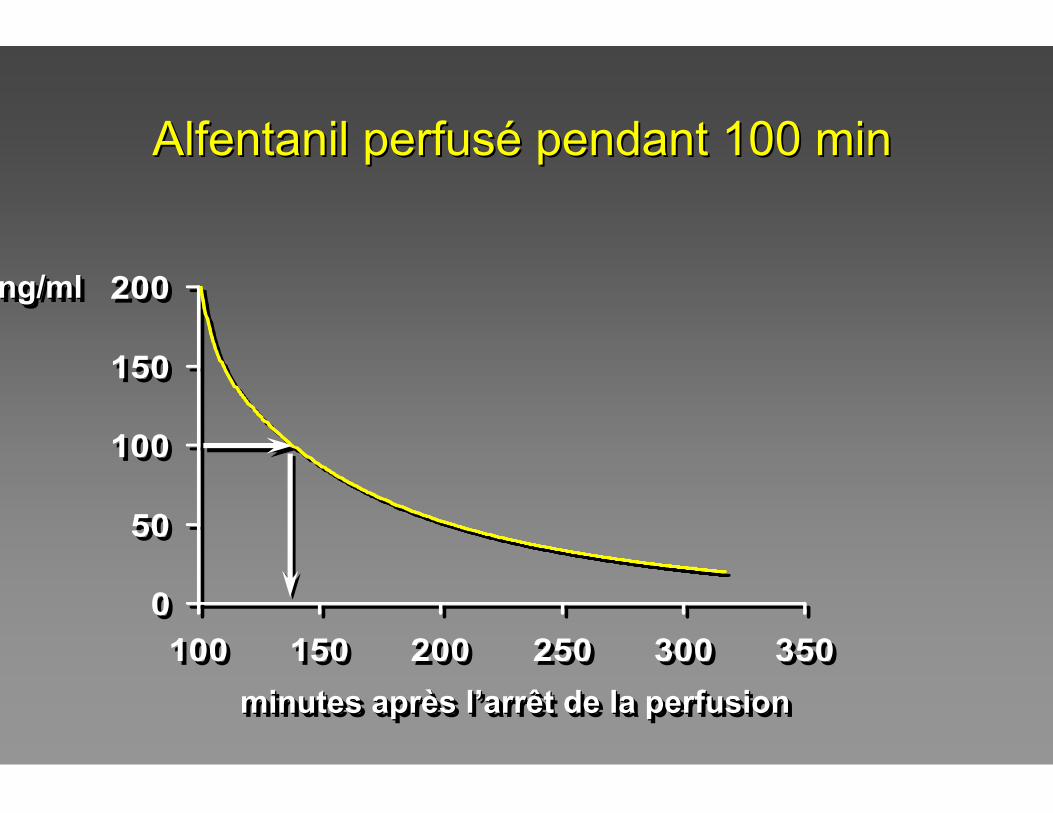
Alfentanil perfusAlfentanil perfuséé pendant 100 minpendant 100 min
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
0
50
100
150
200
100 150 200 250 300 350
0
50
100
150
200
100 150 200 250 300 350
Alfentanil perfusAlfentanil perfuséé pendant 100 minpendant 100 min
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
0
50
100
150
200
100 150 200 250 300 350
0
50
100
150
200
100 150 200 250 300 350
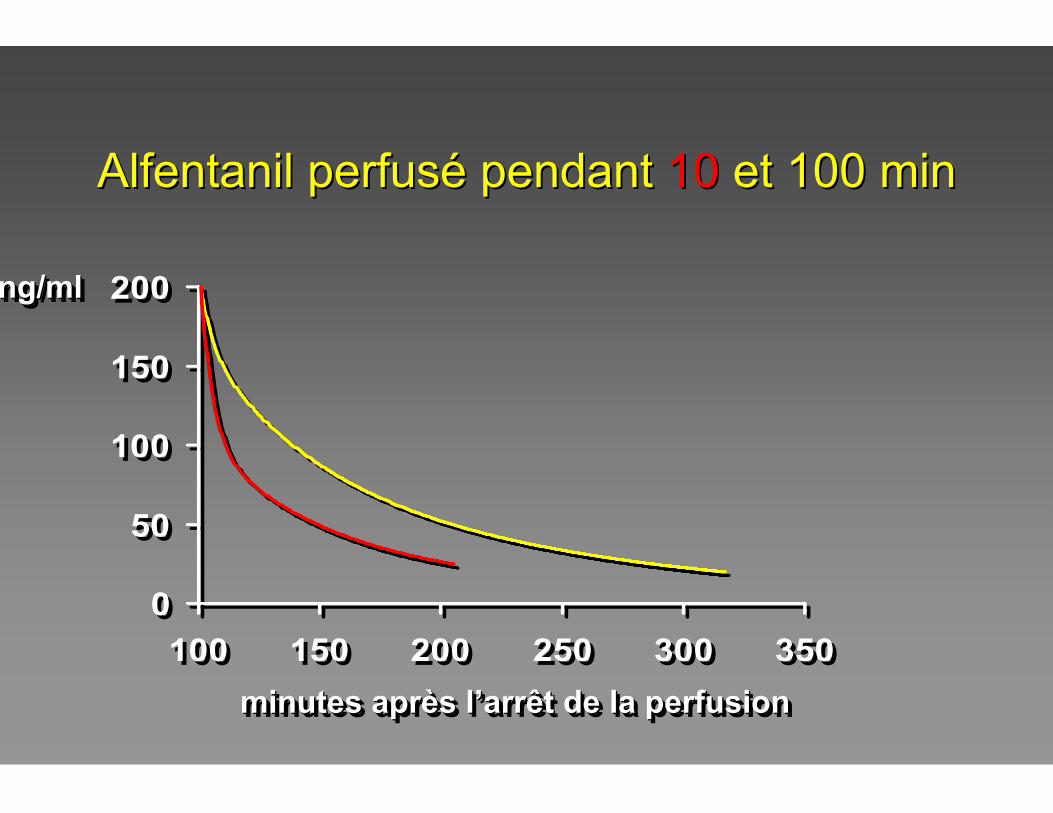
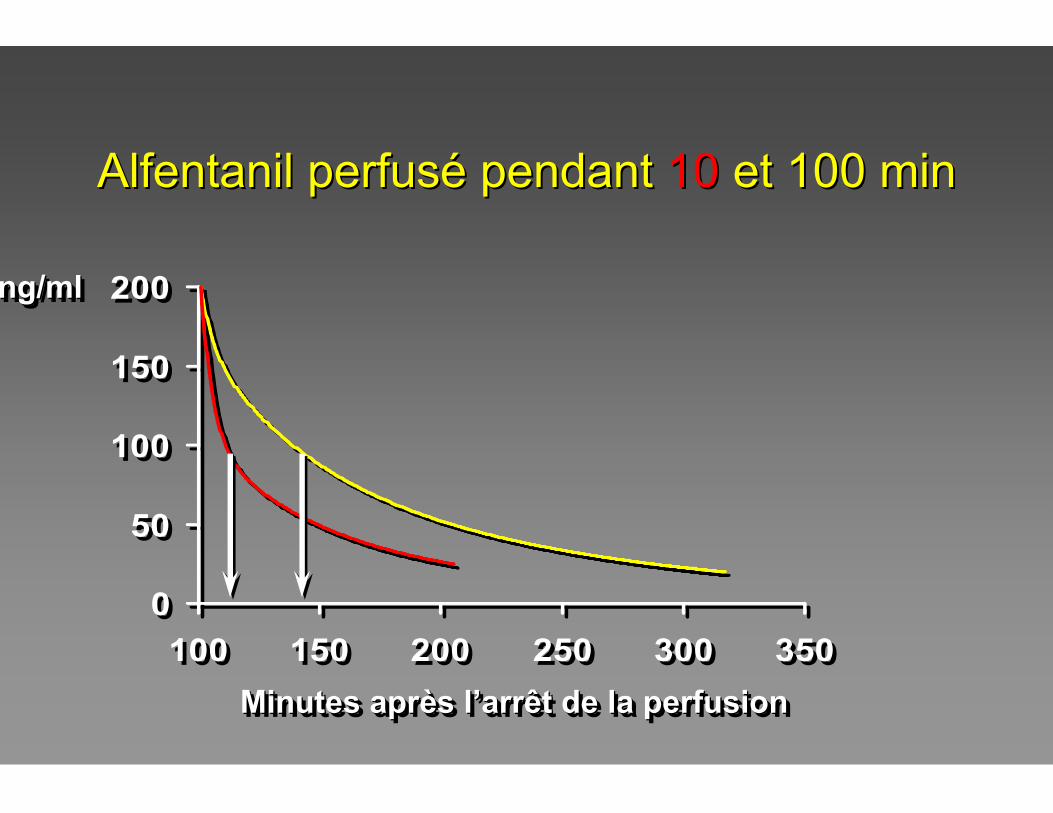
Alfentanil perfusAlfentanil perfuséé pendant pendant 1010 et 100 minet 100 min
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
0
50
100
150
200
100 150 200 250 300 350
0
50
100
150
200
100 150 200 250 300 350
Alfentanil perfusAlfentanil perfuséé pendant pendant 1010 et 100 minet 100 min
Minutes après l’arrêt de la perfusionMinutes aprMinutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
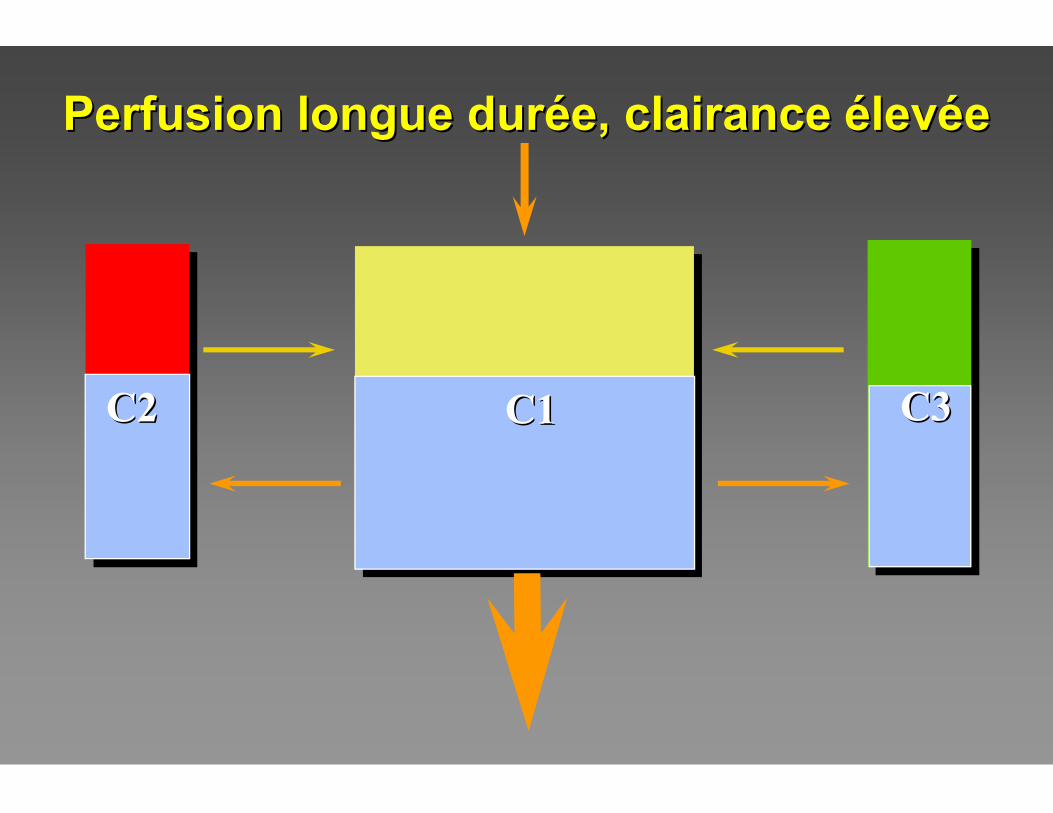
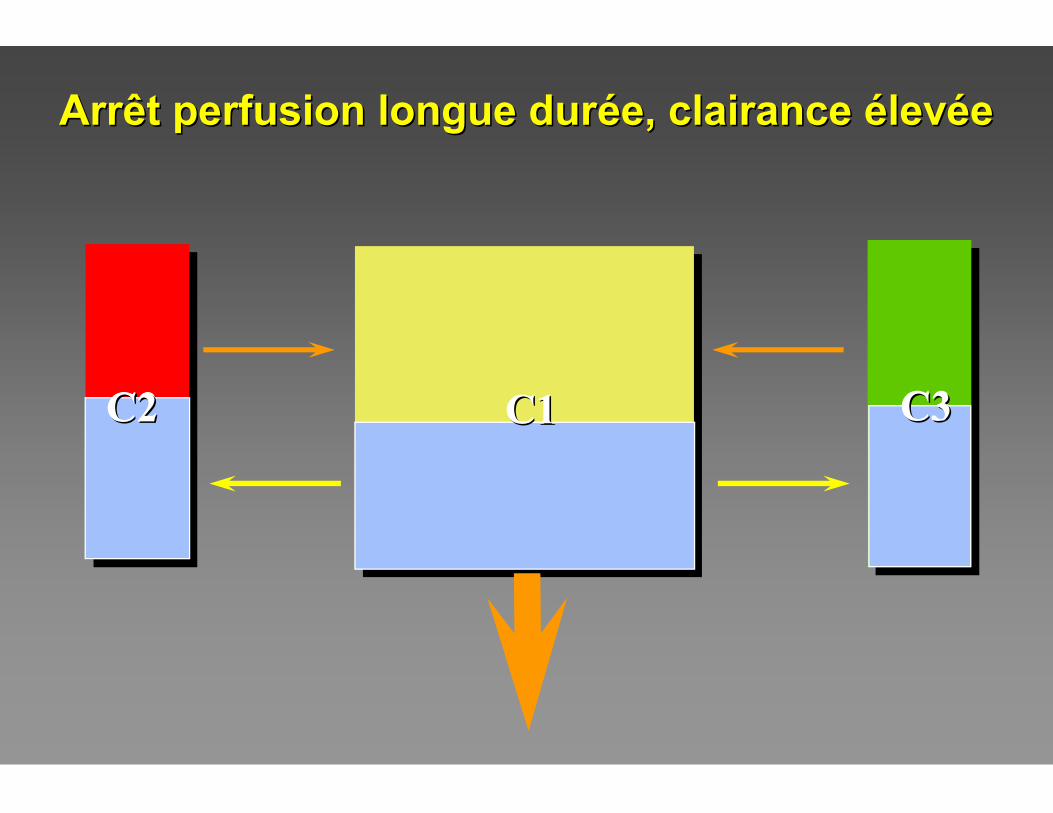
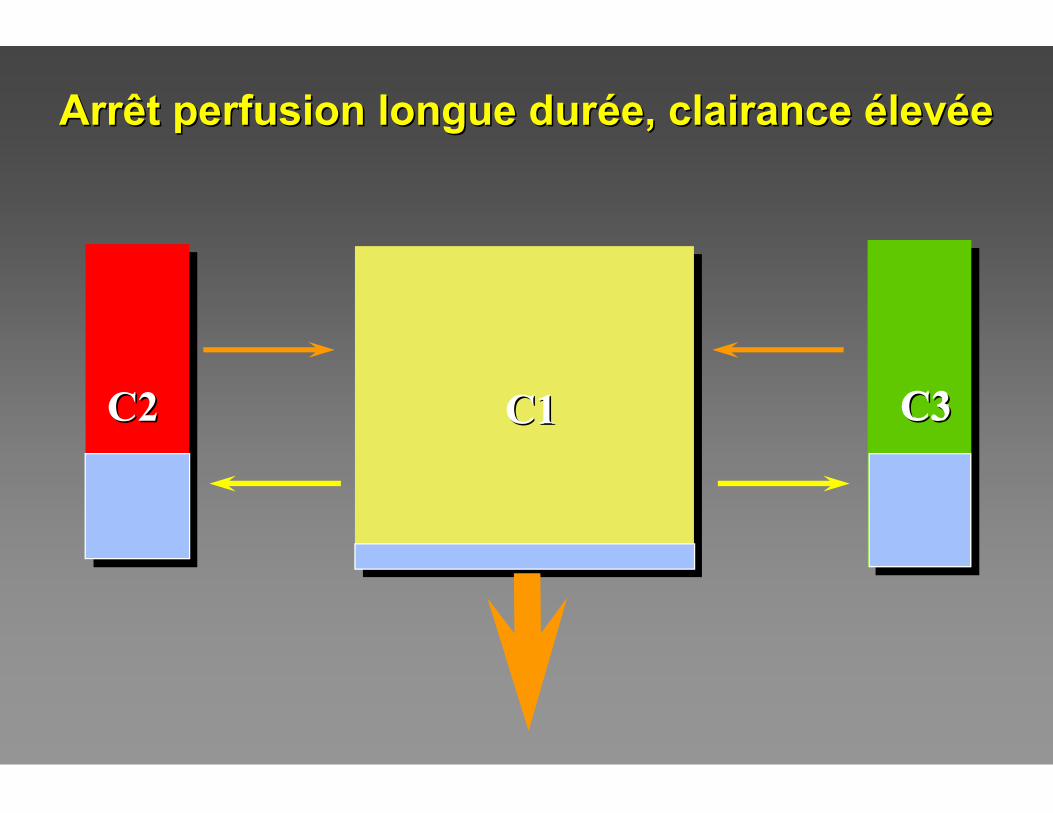
C3C2C2 C1C1
Perfusion longue durPerfusion longue duréée, clairance e, clairance éélevlevééee
C3C3C2C2
C3C2C2 C1C1 C3C3C2C2
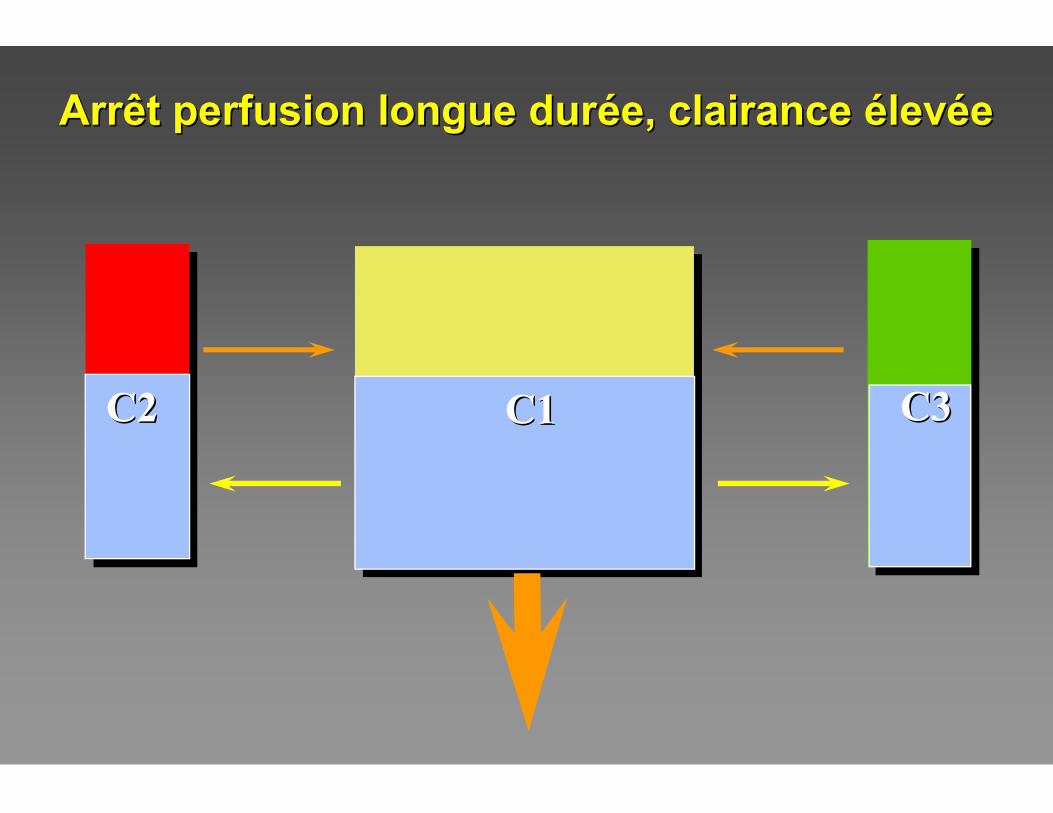
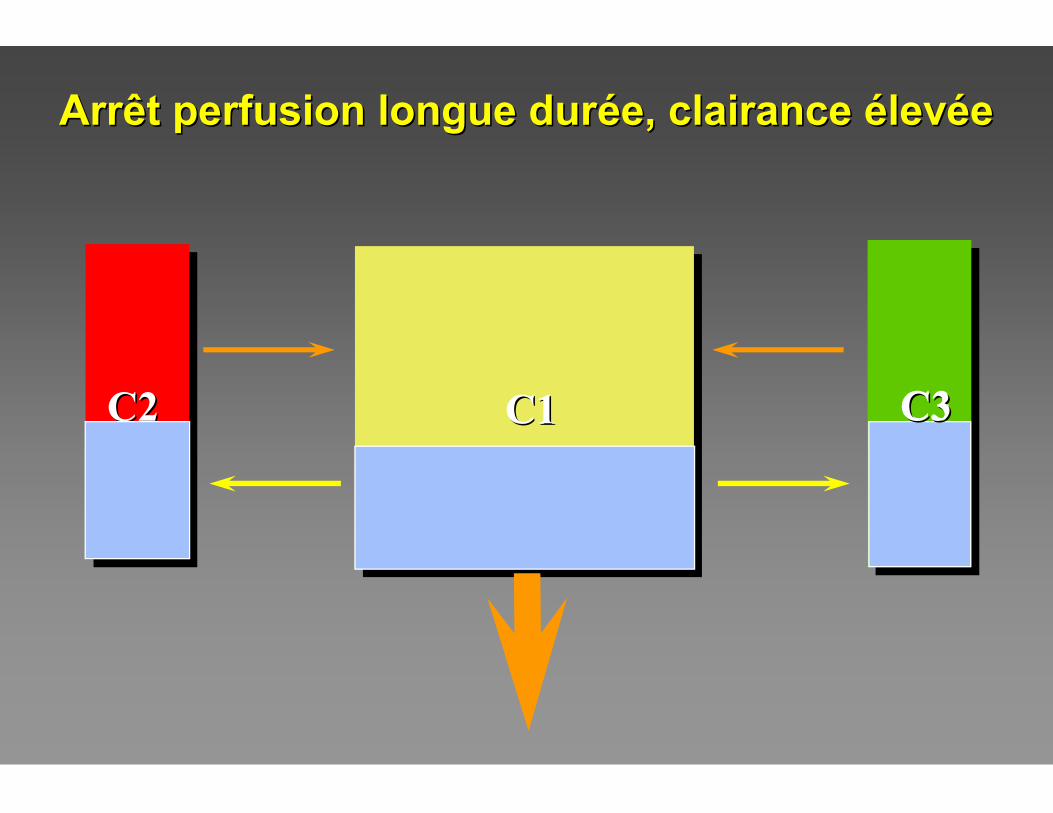
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
C3C2C2 C1C1 C3C3C2C2C2C2
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
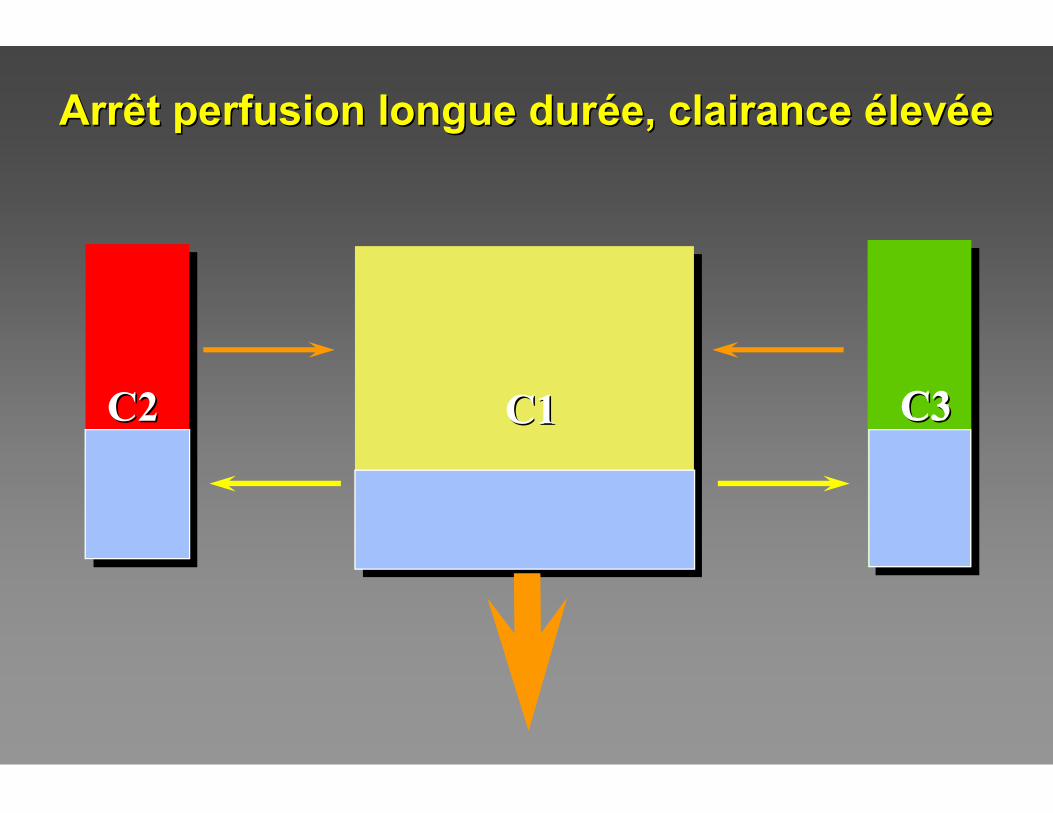
C3C2C2 C1C1 C3C3C2C2
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
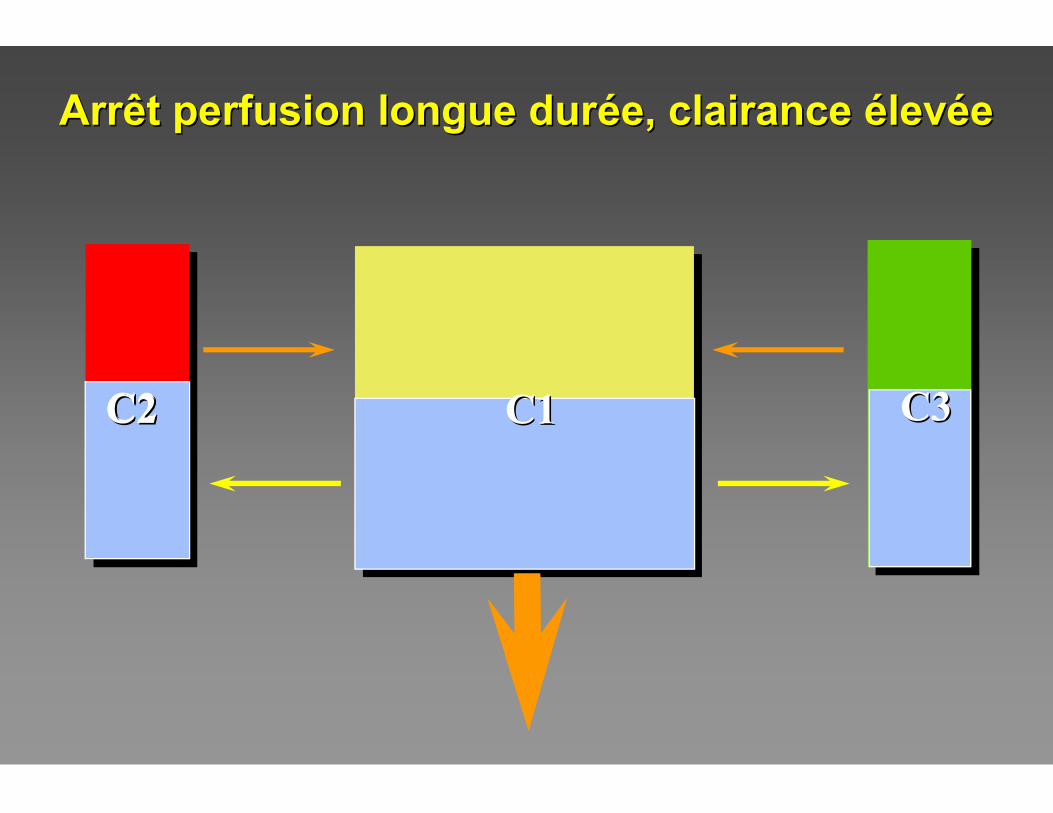
C3C2C2 C1C1 C3C3
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
C3C2C2 C1C1 C3C3
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
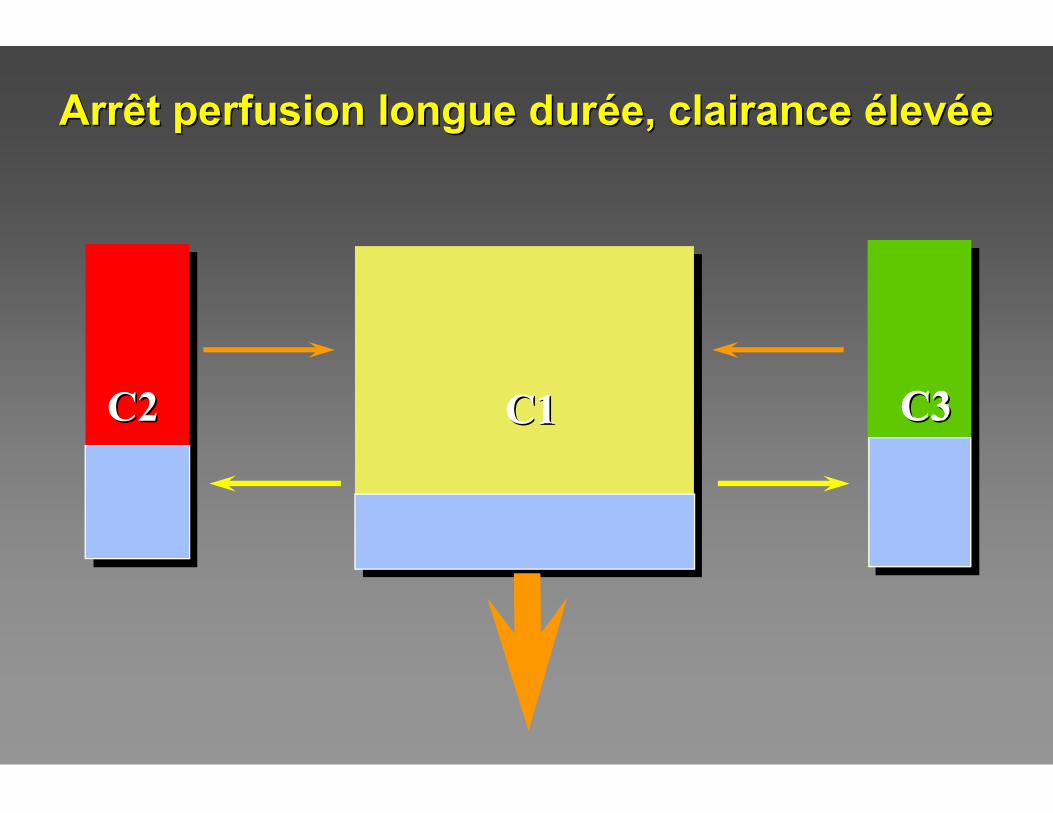
C3C2C2 C1C1 C3C3
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
C3C2C2 C1C1 C3C3
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
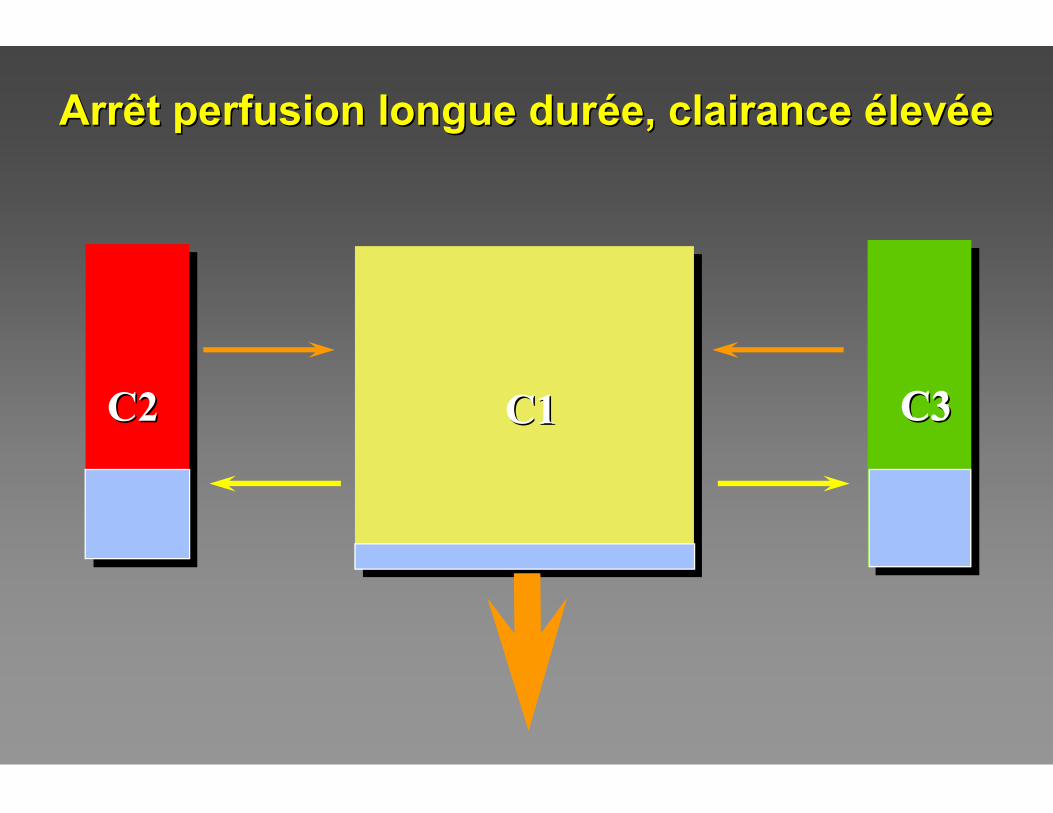
C3C2C2 C1C1 C3C3
Arrêt perfusion longue durArrêt perfusion longue duréée, clairance e, clairance éélevlevééee
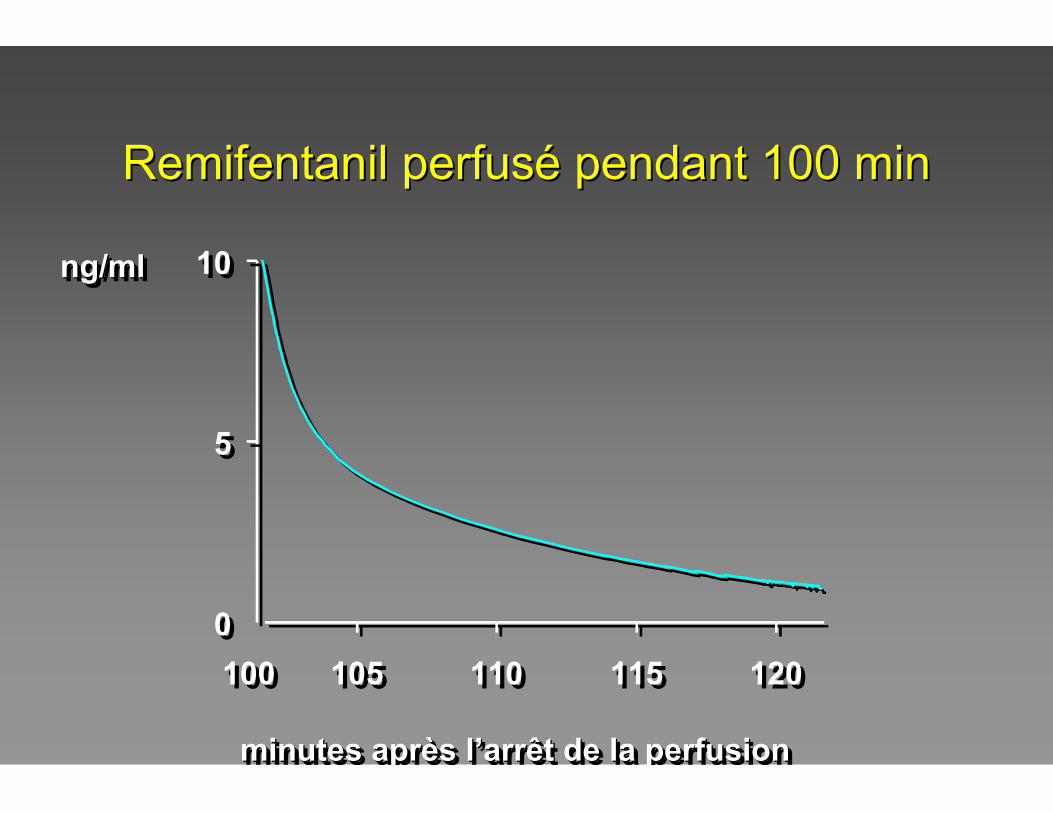
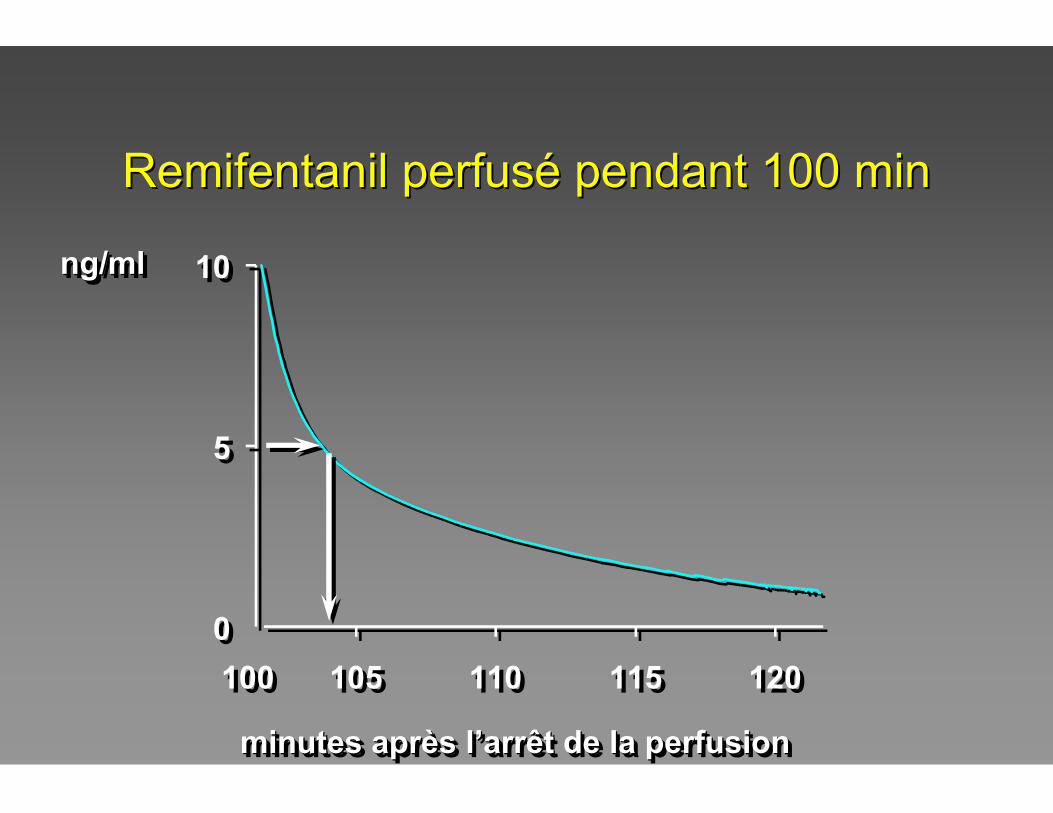
Remifentanil perfusRemifentanil perfuséé pendant 100 minpendant 100 min
00
55
1010
100100 105105 110110 115115 120120
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
00
55
1010
100100 105105 110110 115115 120120
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml
Remifentanil perfusRemifentanil perfuséé pendant 100 minpendant 100 min
0
50
100
150
200
100 150 200 250 300 350
0
5
10
0
50
100
150
200
100 150 200 250 300 350
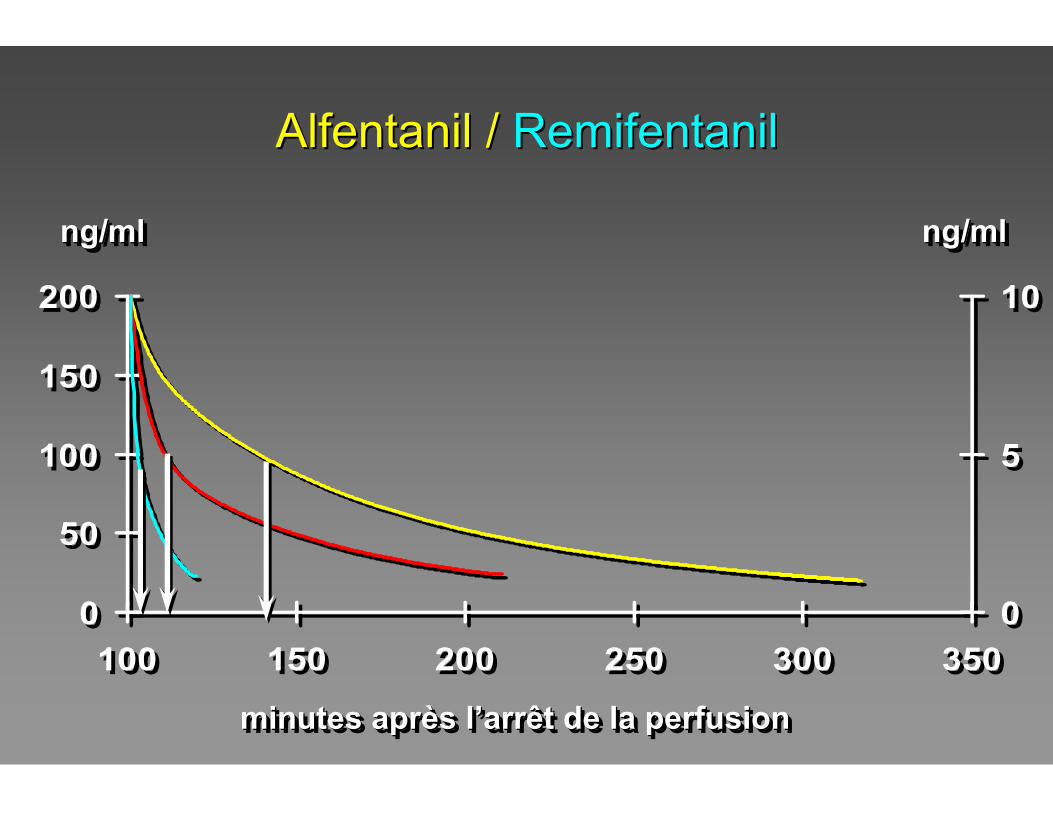
0
5
10
Alfentanil / Alfentanil / RemifentanilRemifentanil
minutes après l’arrêt de la perfusionminutes aprminutes aprèès ls l’’arrêt de la perfusionarrêt de la perfusion
ng/mlng/mlng/ml ng/mlng/mlng/ml
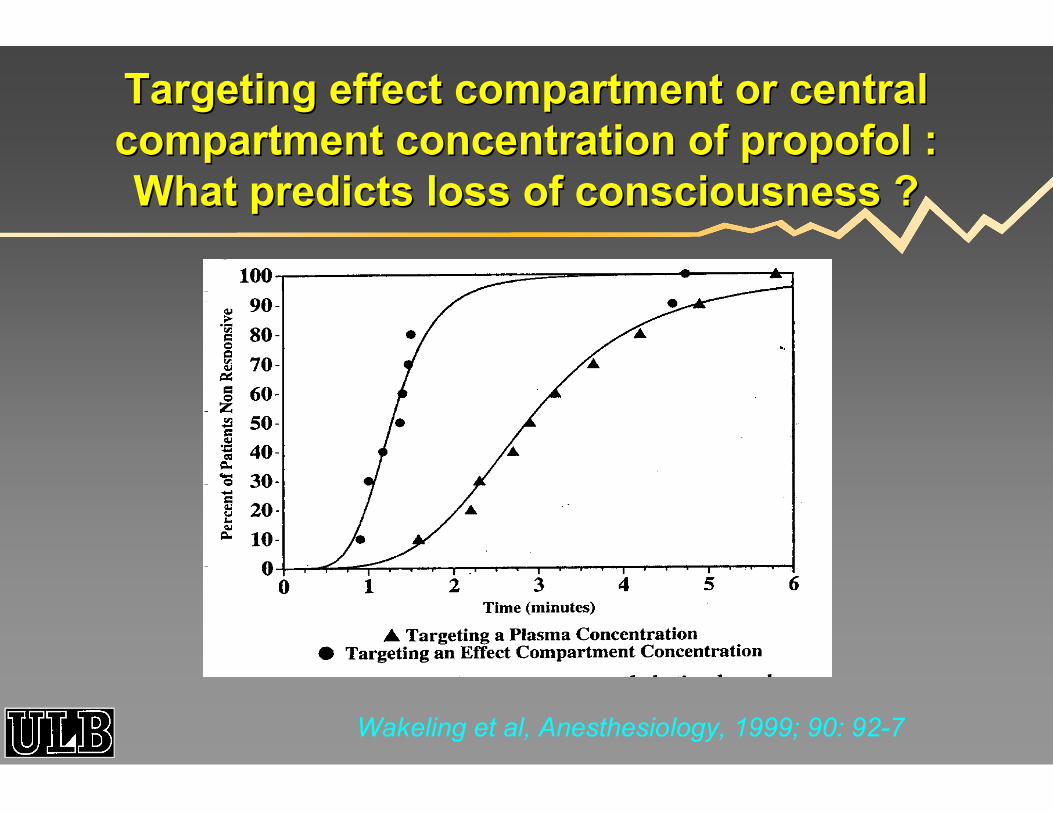
Wakeling et al, Anesthesiology, 1999; 90: 92-7
Targeting effect compartment or central Targeting effect compartment or central compartment concentration of propofol : compartment concentration of propofol : What predicts loss of consciousness ?What predicts loss of consciousness ?
![Dr CHEBIB Cancer Colorectal bis.ppt [Lecture seule] [Mode ......(NFS + Bilan hépatique) D d l’ACE TDM hépatique si l’échographie n’est pas satisfaisante Dosage de l’ACE](https://img.pdfslide.us/doc/110x75/611c13862379e438130f2a45/dr-chebib-cancer-colorectal-bisppt-lecture-seule-mode-nfs-bilan-hpatique.jpg)