Embed Size (px)
Citation preview

Leptospirosis
Sung Chul Hwang Dept. of Pulmonary and Critical Care MedicineAjou University School of Medicine

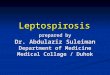
LeptospiraLeptospira
Scanning electron micrograph of Leptospira interrogans strain RGA. Two spirochetes bound to a 0.2 µm filter.Strain RGAwas isolated in 1915 by Uhlenhuth and Fromme from the blood of a soldier in Belgium. CDC/NCID/Rob Weyant [email protected]

Order: SpirochaetaesFamily: Spirochaetaceae
Genus: Treponema Borrelia
Family: LeptospiraceaeGenus: Leptospira
Taxonomy

General Overview of Spirochaetales
Gram-negative spirochetes• Spirochete from Greek for “coiled hair”
Extremely thin and can be very long Tightly coiled helical cells with tapered
ends Motile by periplasmic flagella (a.k.a., axial
fibrils or endoflagella)

General Overview of Spirochaetales
Outer sheath encloses axial fibrils wrapped around protoplasmic cylinder•Axial fibrils originate from insertion pores at both poles of cell
•May overlap at center of cell in Treponema and Borrelia, but not in Leptospira
•Differering numbers of endoflagella according to genus & species

Periplasmic Flagella Diagram

Tightly Coiled Spirochete
AF
OS = outer sheathAF = axial fibrils
Leptospira interrogans

Cross-Section of Spirochete with
Periplasmic Flagella
NOTE: a.k.a., endoflagella, axial fibrils or axial filaments.
(Outer sheath)
Cross section of Borrelia burgdorferi

Genus Species DiseaseTreponema pallidum ssp. pallidum
pallidum ssp. endemicumpallidum ssp. pertenuecarateum
Syphilis Bejel YawsPinta
Borrelia burgdorferirecurrentisMany species
Lyme disease (borreliosis)Epidemic relapsing feverEndemic relapsing fever
Leptospira interrogans Leptospirosis (Weil’s Disease)
Spirochaetales Associated Human Diseases

Introduction• Spirochetal disease, finely coiled, motile,
0.1 x 6 – 20• Systemic infection manifested as
widespread vasculitis• Zoonosis• L. interogans 23 serogroups and 187
serovars• L. biflexa : non-pathogenic, saprophyte

Epidemiology• Disease of the wild animals• Incidental human infection by direct or
indirect contact with the animal• 20-40s active males: farmers or soldiers in
harvest time• 9-10 peak into November

Reservoires of Infection
• Rats• Dogs• Live stocks• Rodents including rabbits• Wild animals• Cats

Sources of Human Infections
• Contaminated Water or soil from infected urine
• Direct animal contacts• Occupational exposure : farmers, vets,
abattoire workers• Recreational exposure : campers, swimmers,
visiting graveyards

Leptospirosis in Humans• Incubation period: 2-30 days, usually 5-14 days
• Broad spectrum of manifestationsAcute undifferentiated feverDengue-like syndrome (fever, headache, myalgia)Aseptic meningitisWeill’s disease (jaundice, renal failure, bleeding)Pulmonary hemorrhage syndrome
• Case fatality rate is 5-40%>50% for pulmonary hemorrhage syndrome
• Major cause of hemorrhagic fever Albert Icksang Ko, MD

Routes of Infection• Contact with water or soil contaminated animals• Direct contact with the by urine from infected source,
farmer, vets, butchers, recreational activities• Rodents carry EH fever, scrub typhus, paratyphus,
leptospirosis• Factors for high incidence : rain during harvest time,
carrier rate in rodents• Spirochetes survive longer in wet swampy conditions

Pathogenesis• Entry sites : skin wounds or abrasions in hand and
feet and mucous membranes, conjunctiva, nasal, oral
• Bacteremia involving the entire body including eye, CSF
• Systemic effect and vasculitis due to endotoxin (hyaluronidase) and burrowing motility
• Hemorrhagic necrosis esp. in liver, lung, and kidneys jaundice, ARF, hemorrhages

Clinical typesTypes 1986 1987Pneumonitis 33% 57.7%Rash type 17%Weil’s disease 15%Renal failure 13% 53.8%“Flue-like” 15% 13.5%Acute Hepatitis 8%Combination 86.5%

Phase I (Septicemic)
• Following incubation period of 7-10 days• High spiking fever, headaches, myalgia,
arthralgias• Lasting 4 – 7 days• Proteinuria and increased creatinnine• Organism detectable but serologic diagnosis not
possible

Phase II (Immune)
• Much more variable• Induction of IgM Antibodies• 1- 3 day freedom recurrence of
symptoms• Lower fever, CNS signs• Maybe cultured from urine but not from
blood or CSF

Weil’s Disease• Less common but severe form• Mild phase I, initially• Followed by severe Jaundice , Azotemia,
and Hemorrhage from Lungs, GI tract, and other organs (3-6 day)
• Oliguric renal failure and Liver dysfunction dominate the clinical picture

Clinical Signs of Leptospirosis • Pulmonary infiltrates, pneumonitis, hemorrhages• Conjunctival injection• Jaundice• Muscle tenderness• Abdominal tenderness• CVA tenderness• Abnormal auscultation• Erythema, petechiae, neck stiffness, adenopathy

Albert Icksang Ko, MD
Clinical Signs of Leptospirosis•Conjunctival injection/hemorrhage

Clinical Signs of LeptospirosisConjunctival injection/hemorrhage

Laboratory Diagnosis
• Microbiologic identification : Blood or CSF first 10 days Urine second week (Fletcher’s, EMJH Medium)
• Serology: screeningMicroscopic Slide Agglutination (MST), titration & serogroup identification Microscopic Agglutination (MAT), detection of IgM (ELISA)

• Presentation of early-phaseleptospirosis is non-specific.
• Misdiagnosis is common: Dengue Malaria Scrub typhus
• Misdiagnosis leads to pooroutcomes (Am J Trop Med Hyg 2001;65:657):
42% of leptospirosis cases sought care in the 1st three days of illness Of these, 61% were diagnosed as dengue Associated with increased ICU admission
(OR, 2.7 [0.8-9.5]) and mortality (OR, 5.1 [0.8-55.0]).
A Tarde, Salvador, June 1996
Barriers to Timely Identification and Treatment
Albert Icksang Ko, MD

Need for Rapid Diagnostics for Leptospirosis
•Current serologic tests have<30-50% sensitivity during the1st week of illness
•Lig proteins are immunodominant antigens (J Clin Microbiol 2007;45:1528) Sensitivity and specificity >90-95%
•Improved sensitivity (80%) during the 1st week of illness.
•Fiocruz-Cornell is developing a Lig-based lateral flow assay Point-of-care diagnosis Clinical evaluation in 2009Albert Icksang Ko, MD

Chest X-rays
• 33 – 64 % of patientssjows abnormality• Bilateral nodules, rosette densities• Diffuse ill-defined infiltrates• Massive confluent consolidation• Bilateral, Non-lobar, peripheral predominance• Rare pleural reaction• Complete resolution within 5 to 10 days

Differential Diagnosis
• EH fever• Rickettsial disease : Scrub typhus, murine
typhus• Acute viral hepatitis• Sepsis• Influenza• Aseptic Meningitis

Treatment
• Early anti-microbial therapy is importantshorten the course and prevent carrier state
• Choice : Penicillin G, Ampicillin• May cause “ Jarish-Herxheimer type
reaction” • Mild cases oral Doxycycline or Amoxicillin

Prevention
• Vaccination of domestic animals• Rodent control• Protective gloves and boots• Avoid swimming in contaminated waters• Vaccination in endemic region

• Reduce reservoir densityPesticidesDeny access to human living environmentDeny access to food and waterRemove food sources and ecological habitats
• Limitations:Pesticides are costly.Rodent control can not be accomplished by
chemical interventions alone (recrudescence, pesticide resistance).
Control of Rodent Sources of Transmission
Albert Icksang Ko, MD

Prevent Exposures to Transmission Sources• Disinfecting areas of contaminated
environment (hypochlorite)
• Protective clothing (boots, gloves)
• Cleaning wounds after exposure
• Prevention of contact with ill or dead animals
• Health education on risk exposures
• Remove transmission sources

What good does it do to treat people's illnesses ...
then send them back to the conditions that made them sick?
Michael Marmot, Commission of Social Determinants of Health, WHO