Embed Size (px)
Citation preview

Lecture (21)

• Indications for chest Radiography
• Clinical Problem• Chest pain• Acute aortic dissection• Pulmonary embolus• Pericardial effusion• Pleural effusion• Vascular disease• Chest trauma• Pneumonia follow up• Haemoptysis• Non specific chest pain• Chest trauma• Upper respiratory tract infection• Chronic obstructive lung disease• Chest masses• Chest infection ( consolidation )• Pneumothorax • Hydropneumothorax• Hydrohaemopneumothorax• Haemothorax

• Chest ProjectionsBasic viewsPA/ APUpright Lateral RAO / LAORPO/LPO
PA chest Exposure factors
Kv mAs FFD (cm) Grid Focus Cassette
75-80 15 180 non broad 35x43
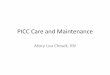
Patient Position Patient erect, feet spread slightly, weight Distributed on both feetChin raised resting against cassetteHands on lower hips, palms out and elbows flexed

• Part position• Align Medial sagittal plane to midline
of cassette• Ensure no rotation of thorax• Rotate shoulders forward to allow scapula
to move laterally away from lung fields• Depress shoulders to downward to move
clavicles below the lung apices • Make exposure at end of second full inspiration• Central Ray
Perpendicular to medial sagittal plane• Center Point
• At level of T7 (Inferior angle of scapula )

• Structure shown• Both lungs from apices to costophrenic angles • The air filled trachea from T1 down • Hilum region markings• Heart &great vessels• Bony Thorax

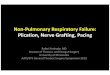
• AP Chest (For Stretcher or bed patients
Patient Position Patient is supine in cartIf possible raised the headedcart or bed
into a semi erect position Role patient shoulders forward by rotating armmedially or internallyPart Position Align Medial sagittal plane to midline of cassetteEnsure no rotation of thoraxTop of film 4-5 cm above shoulders Place caste crosswise to avoid lateral cutoffMake exposure at end of second full inspirationCentral RayAngled caudad to be perpendicular to long axis of the sternum Center Point At level of T7 (3-4 inches below jugular noch


• AP Chest (For Stretcher or bed patients
Patient Position Patient is supine in cartIf possible raised the headedcart or bed
into a semi erect position Role patient shoulders forward by rotating armmedially or internallyPart Position Align Medial sagittal plane to midline of cassetteEnsure no rotation of thoraxTop of film 4-5 cm above shoulders Place caste crosswise to avoid lateral cutoffMake exposure at end of second full inspirationCentral RayAngled caudad to be perpendicular to long axis of the sternum Center Point At level of T7 (3-4 inches below jugular noch

• Structure shown• Both lungs from apices to costophrenic angles • The air filled trachea from T1 down • Hilum region markings• Heart will appear enlarged due to• magnification from short FFD• Bony Thorax• Notes:• Crosswise alignment of cassette need accurate
perpendicular • alignment of central ray to cassette to avoid grid cutoff• If pleural effusion is suspected decubitus position is
recommended• to demonstrate air-fluid level