Embed Size (px)
Citation preview

Lecture 1: Autonomic Nervous System Organisation of the Autonomic Nervous System
- Somatic: Provides sensory and motor innervation
○ A part of the somatic nervous system innervates the dermatomes of thorax, abdomen and pelvis. - Autonomic: Provides innervation to the viscera
○ Sympathetic ○ Parasympathetic
Somatic Neurons - Sensory fibres
○ Bring information about touch, pressure and pain from the periphery to the CNS. ○ Originate from body wall ➔ Spinal nerve ➔ Dorsal root ganglion (cell body) ➔ Dorsal horn ➔ Ascend up to CNS
- Motor fibres ○ Carry information from the CNS to skeletal muscles for movement. ○ Originates in ventral horn ➔ Ventral root ➔ Spinal nerve ➔ To muscle
- Spinal nerves run laterally. - In the context of the thorax, abdomen and pelvis, spinal nerves provides segmental innervation to the body wall.
○ Forms basis of dermatomes.

Autonomic neurons - Sympathetic: Some of the sympathetic neurons will ascend or descend through the chain to access the top and bottom. - Parasympathetic: Most of the parasympathetic innervation are from the vagus nerve.
SYMPATHETIC PARASYMPATHETIC
Short preganglionic neurons - Some lumbar neurons bypass the sympathetic chain and run in splanchnic
nerves which leads to the prevertebral ganglia ➔ Pelvic viscera
Long preganglionic neurons - Run in vagus nerve for thorax and abdomen. - Run in pelvic splanchnic nerves for pelvis.
Synapse with postganglionic neurons - In sympathetic trunk ➔ Thorax or head - In prevertebral ganglia, which is in front of the abdominal aorta, and not in the
sympathetic trunk ➔ Abdomen
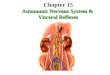
Synapse with postganglionic neurons near viscera.
Sympathetic neurons - Originate from the intermediolateral nucleus/horn ➔ Ventral root ➔ Spinal nerve ➔ Communicating rami ➔ Sympathetic chain
ganglion - Rami communicantes
○ Connects spinal nerves with sympathetic chain ○ White communicating rami = More distal
● White because the preganglionic sympathetic neurons are myelinated. ○ Grey communicating rami = More proximal
- Postganglionic neurons can also go through the grey communicating rami and into the spinal nerve, which will go out of the body wall to blood vessels, sweat glands etc.
Visceral afferent neurons Visceral afferent neurons: Sensory neurons that innervate viscera. - Follows sympathetic pathway back to CNS from the viscera. - Can also follow parasympathetic pathways via the vagus nerve back to CNS. - Take information about the state of the viscera back to the CNS
➔ Visceral state contributes to all sorts of reflexes. ○ Sensory to viscera ○ Distension of viscera ○ Visceral pain
Referred pain - Pain associated with viscera is usually referred to body wall/skin. - Referred pain is the perception of pain in areas other than the site of stimulation, usually due to a common spinal segmental origin of
the nerves to the site of stimulation and the site to which the pain is referred. - Probably due to the convergence of the two inputs, one somatic and one visceral sensory neuron, to the same population of neurons or
one neuron at a given spinal segmental level. - Visceral pain is referred to somatic regions. - Somatic pain can be referred to other somatic regions. - Pain is often referred to the body walls and limbs.
○ Heart attack ➔ Refer pain to T1-T4 - The brain can't tell that information is coming from the viscera because the body doesn't have a good map of the organs, but it has a
good map of the body wall due to frequent stimulation. ○ Since it can't distinguish between these two groups of inputs, it will refer pain out to the dermatome associated with that spinal
cord segment because it has a familiarity with that map.

Referred pain from paired viscera
Unpaired viscera - GIT and associated glands and ducts: Develop in midline, but migrate away from it.
➔ Associated orifices: mouth, anal canal remains in midline. - Nerve supply from both sides of spinal cord. - Visceral pain referred to midline skin over origin of viscera, because dual sensory nerve reaches both sides of spinal cord simultaneously. - Pain only referred to local overlying skin when somatic nerves involved.

Lecture 2: Thoracic Walls and Breast Thoracic wall - Function: To protect the viscera within ➔ Heart, lungs - Forms mechanical basis of breathing. - Includes:
○ Thoracic cage: Ribs, sternum, vertebrae ○ Covering: Skin, muscle
Thoracic cage - Ribs
○ 12 ribs ○ Each rib, except for floating ribs, associates with a costal cartilage anteriorly and these costal cartilages attach to the sternum. ○ Costal cartilage ➔ Contributes to mobility of thorax which is important for breathing. ➔ Allows thoracic cage to expand in breathing. ○ Classification
Attachment: True, false, floating ■ Ribs 1-7
■ True ribs ■ Attach directly to the sternum via their own costal cartilage.
■ Ribs 8-10 ■ False ribs ■ Have costal cartilage that extends anteriorly from them, but
attaches to the costal cartilage of the rib above. ■ No direct attachment to the sternum.
■ Ribs 11-12 ■ Floating ribs ■ No anterior attachment at all. ■ Mobile
Features: Typical, atypical ■ Ribs 3-9
■ Typical ribs ■ Curved and flat ■ Angle ➔ Most of the bend of the rib. ■ Costal groove ➔ At inferior surface of rib.
➔ Shelters and protects neurovascular structures that run through intercostal spaces.
■ Posterior end (Head): Superior and inferior facet ➔ Articulate with the demifacets on the vertebral body.
➔ Superior facet articulates with inferior demifacet of the vertebral body above. ➔ Inferior facet articulates with the superior demifacet of the vertebral body below (same number).
● Neck ➔ Small narrowing ➔ Articular facet: Articulates with the transverse process of the vertebrae.
➔ Tubercle: Attachment for ligaments associated with the costotransverse joint. ■ Ribs 1-2, 10-12
■ Atypical ribs ■ All have slightly different features. ■ Rib 1 ➔ Flat in the coronal plane unlike other ribs that are flat vertically.
➔ 2 grooves for the subclavian vessels over the top of the rib. ➔ Scalene tubercle for attachment of scalene muscles of the neck. - Sternum
○ Commonly known as breastplate.

○ 3 parts ■ Manubrium
■ Jugular notch: Has defined sensory innervated periosteum which can hurt if pressed ➔ Pressure point ■ Clavicular notch: Articulation of medial clavicle ■ Articulates with rib 1 below clavicular notch. ■ Articulates partly with rib 2.
■ Body of sternum ■ Xiphoid process
■ Largely cartilaginous for most of our life, but become less cartilaginous as it starts to ossify later in life.
■ Forms some attachment to the diaphragm. ○ Manubriosternal joint: Articulation between manubrium and sternum.
● Defined bump ■ Allows palpation of rib 2 ➔ Rib 2 attaches via its costal cartilage at this joint.
● Angle of Louis/Sternal angle: Angle which forms lump at manubriosternal joint. ● Plane of Louis: Horizontal line through the thorax which forms a transverse plane through sternal angle.
■ Significance of Plane of Louis: ✩ Aortic arch ✩ 2nd Rib ✩ T4/5 vertebrae ✩ Bifurcation of trachea
- Thoracic vertebrae ○ 2 articular points
● Costovertebral joint: Joint where head of rib articulates with body of the vertebrae. ■ The rib articulates at the top of the body of the vertebrae with the same number.
● Costotransverse joint: Joint where articular facet distal to the neck of rib articulates with transverse process of vertebrae. Intercostal space - Intercostal space: Space between ribs.
○ Intercostal veins, arteries and nerves run between the internal intercostal muscle layer and the innermost intercostal muscle layer.
○ They are sheltered superiorly in the intercostal space under the costal groove of the rib above.
■ Importance: For injections, penetrate above the rib below to avoid damaging neurovascular bundle in intercostal space.
- Intercostal muscles ○ 3 Layers
● External intercostal muscles ■ Superficial layer ■ Fibre direction: Anteroinferiorly ■ Breaks down anteriorly at costochondral junction ➔ Continues as external intercostal membrane. ■ Action: Elevate the ribs
● Internal intercostal muscles ■ Intermediate layer ■ Fibre direction: Posteroinferiorly ➔ Perpendicular to external intercostal muscles. ■ Breaks down posteriorly and continues as a membrane. ■ Action ➔ Lateral to costochondral junction: Depress ribs because they have the opposite fibre direction to the
external intercostal muscles. ➔ Medial to costochondral junction: Elevate the ribs because of the 3D shape of ribs.
● Innermost intercostal muscles ■ Deep layer ■ Fibre direction: Posteroinferiorly ➔ Same direction as internal intercostal muscles which means it has the same function.

■ Tend to be broken down and patchy particularly around the posterior end. ✩ Importance: Allows us to see neurovascular structures running through the intercostal space in the posterior thoracic
wall. - Intercostal nerves
○ Intercostal nerves are extensions of segmental spinal nerves ➔ Ventral rami of spinal nerves coming from each thoracic spinal cord segment.
○ These ventral rami continue in the intercostal space and are now referred to as intercostal nerves. ○ Intercostal nerves give off a muscular and cutaneous branches.
● Supplies all intercostal muscles and overlying skin in their respective space. ● Forms basis of the 12 thoracic dermatomes ➔ Clinical importance: Maps out patterns of referred pain.
■ T4: Strip over nipples ■ T10: Strip over belly button
○ Intercostal nerves terminate anteriorly via some cutaneous branches. ● Cutaneous supply: Skin anteriorly, laterally and posteriorly until the angle to the ribs.
■ The dorsal rami of the spinal nerves supply the hypaxial muscles and the skin medial to angle of rib on the posterior side - Intercostal vessels
○ Internal intercostal arteries ● Posterior intercostal arteries
■ Branch of aorta which run through the intercostal space with the intercostal nerve to the anterior side. ■ Gives off branches that supply both the muscle and the skin.
● Anterior intercostal arteries ■ Branch of internal thoracic artery at the front end of the thorax which runs through the intercostal space.
✩ Internal thoracic artery: A branch of the subclavian artery which descend posteriorly and laterally along the whole length of the sternum.
● Anterior and posterior intercostal arteries anastomose with each other somewhere on the anterior thoracic wall. ■ Clinical importance: Provides an alternative route for blood to some of the skin and muscles in this intercostal space.
Internal intercostal arteries can be used for coronary bypass surgery. Superficial muscles - Superficial muscles: Muscles that sit on top of the thoracic cage.
○ Pectoralis major ● Attachments: 2 heads ➔ Medial part of the clavicle, sternum
Medial part of humerus ● Adductor muscle: Brings humerus/arm towards the midline. ● If you fix the attachments on the humerus by putting our hands on our hips or knees or leaning on a bench, contracting the
muscle will act on the thoracic cage by expanding it which will allow more air to get into the lungs. ○ Accessory muscle of respiration.
○ Pectoralis minor
● Attachments: Coracoid process of scapula and ribs 3-5 along the costochondral junction ● Action: Elevate ribs or stabilise scapula.
○ Serratus anterior
● Attachments: Lateral aspect of the ribs 1-8 and the medial border of the anterior surface of the scapula. ● Action: Protract scapula ➔ Punching muscle
Expand thoracic cage if humerus is fixed.
○ Serratus posterior ● There are superior and inferior muscles. ● Attachments on ribs.

Coverings of the thoracic cage - The most superficial part of the thoracic cage includes skin which has sweat glands, fat, nerves, blood and lymphatic vessels. - Embedded between the skin and some of the superficial muscles is the mammary gland.
Breast - Mammary gland - Mammary gland sits on the fascia superficial to the pectoralis major.
○ ⅔ sit over pectoralis major from rib 2 - rib 6. ○ Lateral ⅓ sit over serratus anterior muscle. ○ Axillary tail: Part of the mammary gland that extends up into the the axilla.
● Can give false positives since lymph nodes can get swollen in the axilla from breast cancer. ○ Mammary glands enlarge during pregnancy and grow during puberty.
- Suspensory ligaments: Connective tissue that run from the skin, through the gland, between lobules and attach to pectoralis major. ○ Anchors the breast in place.
- Nipple: Centre of areola ○ Usually sits in the 4th intercostal space in the midclavicular line in nulliparous women. ○ Has openings for lactiferous duct. ○ Smooth muscle around nipple.
● Importance: Reflex causes contraction of smooth muscle making nipple erect, so the baby can latch onto it. ○ No fat, hair or sweat glands.
- Areola: Pigmented area of skin around nipple. ○ Contains sebaceous glands which secrete oily substances for lubrication when feeding.
- Retromammary space: Space between the mammary gland and the pectoralis major. ○ Important for reconstructive surgery - breast cancer, plastic surgery
● Silicon implants can be placed in the retromammary space ➔ Shape can be seen very well. ● Implants can be placed deep to pectoralis major ➔ Bring breast forward. ● Half the implants can be placed in retromammary space and the other half can be placed deep to pectoralis major.
- Consist of 15-20 lobules of glandular tissue. ○ Each lobule contains alveoli which is the milk secreting portion of the lobule. ○ Each lobule is drained by its own duct called the lactiferous duct which opens independently on the nipple. ○ Between lobules, there are lots of fat.
- Lactiferous sinus: Dilated portion of duct which is proximal to the where the ducts opens up to the nipple. ○ This is where a bit of milk can accumulate in a lactating mother. ○ Importance: Suction is required to draw milk from the full lobule and for this reflex to be continue, babies need to be encouraged to
keep sucking which is done by the bit of milk present.

Mammograms - Mammograms: X-ray of breast tissue used to identify tumours. - 2 types:
○ Dense: Younger women ● There is a lot of connective tissues and glands which can give false positives.
○ Fatty: Older women ● Less dense in appearance ➔ Hard to see suspensory ligaments
Breast- Blood supply and venous drainage - Medial side: Supplied by small branches of the internal thoracic artery which are given off through the anterior intercostal spaces. - Lateral side: Supplied by branches of the lateral thoracic artery and some branches of the posterior intercostal arteries.
Breast- Lymphatics - Lymphatic system of the breast is derived mostly from the superficial subareolar plexus that is around the areola. - Connections of the subareolar plexus:
○ Medially to the bronchomediastinal trunk via the parasternal lymph nodes. ● Parasternal lymph nodes lie adjacent to the sternum in the distal parts of
the intercostal space and close to the bronchomediastinal trunk. ○ Some communicate with the lymphatic system of abdomen. ○ 75% of lymph moves upwards through axillary lymph nodes and into the
subclavian trunks. ● Subclavian trunks from each side will take lymph back towards the
brachiocephalic vein and if: ■ Right side: Right subclavian trunk ➔ Drains into right lymphatic duct. ■ Left side: Left subclavian trunk ➔ Drains into thoracic duct.
- DRAINING INTO LEFT BRACHIOCEPHALIC VEIN
○ Thoracic duct: Collects lymph from abdomen and lower limb. ● Lymph vessels that drain into the thoracic duct:
■ Left jugular trunk: Lymph from left side of head. ■ Left subclavian trunk: Lymph from left upper limb. ■ Left bronchomediastinal trunk: Lymph from left side of thorax
● Drains left upper limb, thorax, head and the entire body below the level of diaphragm.
- DRAINING INTO RIGHT BRACHIOCEPHALIC VEIN
○ Right lymphatic duct ● Lymph vessels that drain into the right lymphatic duct:
■ Right jugular trunk: Lymph from right side of head. ■ Right subclavian trunk: Lymph from right upper limb ■ Right bronchomediastinal trunk: Lymph from right side of thorax.
● Drains right upper limb, thorax and head.

Breast cancer - Tumors are able to metastasise via the lymphatic system. - Cancer cells that enter a lymphatic vessel usually pass through a number of lymph nodes before entering the venous system.
○ Lodge in nodes to form metastases that can be palpated, usually in the axillary lymph node, to give indication of the presence of cancer.
● Cancer can also metastasise via other routes to other nodes instead. ■ e.g. Into the thorax via the parasternal lymph nodes or abdomen via abdominal connections.
- Breast cancer is usually derived from glandular epithelium in the 15-20 lobules. - May appear as jagged mass on mammogram ➔ Difficult to identify in younger women with dense breast mammogram. - Cancer cells can damage suspensory ligaments passing through breast tissue.
○ As a result, the skin becomes thick or dimpled over area where the cancer is, or the nipple inverts due to the shortening of the suspensory ligaments.
Breast- men - Usually no glandular development.
○ Males can get glandular development if there is hormonal imbalance. - Some small duct development.
○ Breast cancer can develop from the duct system ➔ Males can still get breast cancer. - Little fat