Embed Size (px)
Citation preview

492
●
●
Chapter
22Chapter
22Management of PatientsWith Upper RespiratoryTract Disorders
LEARNING OBJECTIVESOn completion of this chapter, the learner will be able to:
1. Describe nursing management of patients with upper airwaydisorders.
2. Compare and contrast the upper respiratory tract infections withregard to cause, incidence, clinical manifestations, management,and the significance of preventive health care.
3. Use the nursing process as a framework for care of patients withupper airway infection.
4. Describe nursing management of the patient with epistaxis.5. Use the nursing process as a framework for care of patients under-
going laryngectomy.

Many upper airway disorders are relatively minor, and theireffects are limited to mild and temporary discomfort and incon-venience for the patient. However, other upper airway disordersare acute, severe, and life-threatening and may require permanentalterations in breathing and speaking. Thus, the nurse must havegood assessment skills, an understanding of the wide variety ofdisorders that may affect the upper airway, and an awareness ofthe impact of these alterations on patients.
Because many of the disorders are treated outside the hospitalor at home by patients themselves, patient teaching is an impor-tant aspect of nursing care. When caring for patients with acute,life-threatening disorders, the nurse needs highly developed as-sessment and clinical management skills, along with a focus onrehabilitation needs.
Upper Airway InfectionsUpper airway infections are common conditions that affect mostpeople on occasion. Some infections are acute, with symptomsthat last several days; others are chronic, with symptoms that lasta long time or recur. Patients with these conditions seldom re-quire hospitalization. However, nurses working in communitysettings or long-term care facilities may encounter patients whohave these infections. Thus, it is important for the nurse to rec-ognize the signs and symptoms and to provide appropriate care.
RHINITISRhinitis is a group of disorders characterized by inflammation andirritation of the mucous membranes of the nose. It may be classi-fied as nonallergic or allergic. It is estimated that 10% to 15% ofthe population of the United States has allergic rhinitis (Middletonet al., 1998). Rhinitis may be an acute or chronic condition.
PathophysiologyNonallergic rhinitis may be caused by a variety of factors, in-cluding environmental factors such as changes in temperature orhumidity, odors, or foods; infection; age; systemic disease; drugs(cocaine) or prescribed medications; or the presence of a foreignbody. Drug-induced rhinitis is associated with use of antihyper-tensive agents and oral contraceptives and chronic use of nasal de-congestants. Rhinitis also may be a manifestation of an allergy(see Chap. 53), in which case it is referred to as allergic rhinitis.Figure 22-1 shows the pathological processes involved in rhinitisand sinusitis.
Clinical ManifestationsThe signs and symptoms of rhinitis include rhinorrhea (exces-sive nasal drainage, runny nose), nasal congestion, nasal discharge(purulent with bacterial rhinitis), nasal itchiness, and sneezing.Headache may occur, particularly if sinusitis is also present.
Medical ManagementThe management of rhinitis depends on the cause, which may beidentified in the history and physical examination. The examinerasks the patient about recent symptoms as well as possible expo-sure to allergens in the home, environment, or workplace. If viralrhinitis is the cause, medications are given to relieve the symp-toms. In allergic rhinitis, tests may be performed to identifypossible allergens. Depending on the severity of the allergy, de-sensitizing immunizations and corticosteroids may be required(see Chap. 53 for more details). If symptoms suggest a bacterialinfection, an antimicrobial agent will be used (see “Medical Man-agement of Sinusitis”).
PHARMACOLOGIC THERAPYMedication therapy for allergic and nonallergic rhinitis focuseson symptom relief. Antihistamines are administered for sneezing,itching, and rhinorrhea. Oral decongestant agents are used fornasal obstruction. In addition, intranasal corticosteroids may beused for severe congestion, and ophthalmic agents are used to re-lieve irritation, itching, and redness of the eyes.
Nursing ManagementTEACHING PATIENTS SELF-CAREThe nurse instructs the patient with allergic rhinitis to avoid orreduce exposure to allergens and irritants, such as dusts, molds,animals, fumes, odors, powders, sprays, and tobacco smoke. Thepatient is instructed about the importance of controlling the en-vironment at home and work. Saline nasal or aerosol sprays maybe helpful in soothing mucous membranes, softening crusted se-cretions, and removing irritants. The nurse instructs the patientin the proper use of and technique for administrating nasal med-ications. To achieve maximal relief, the patient is instructed toblow the nose before applying any medication into the nasal cav-ity. In the case of infectious rhinitis, the nurse reviews with thepatient hand hygiene technique as a measure to prevent trans-mission of organisms. The nurse teaches methods to treat symp-toms of the viral rhinitis. In the elderly and other high-riskpopulations, the nurse reviews the value of receiving a vaccination
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 493
Glossaryalaryngeal communication: alternative
modes of speaking that do not involve the normal larynx; used by patients whoselarynx has been surgically removed
aphonia: impaired ability to use one’s voicedue to disease or injury to the larynx
apnea: cessation of breathingdysphagia: difficulties in swallowingepistaxis: hemorrhage from the nose due to
rupture of tiny, distended vessels in themucous membrane of any area of the nose
herpes simplex: cold sore (cutaneous viralinfection with painful vesicles and
erosions on the tongue, palate, gingival,buccal membranes, or lips)
laryngitis: inflammation of the larynx; maybe due to voice abuse, exposure to irri-tants, or infectious organisms
laryngectomy: removal of all or part of thelarynx and surrounding structures
pharyngitis: inflammation of the throat;usually viral or bacterial in origin
rhinitis: inflammation of the mucous mem-branes of the nose; may be infectious,allergic, or inflammatory in origin
rhinorrhea: drainage of a large amount offluid from the nose
sinusitis: inflammation of the sinuses; maybe acute or chronic; may be viral, bacterial,or fungal in origin
submucous resection: surgical procedure tocorrect nasal obstruction due to deviatedseptum; also called septoplasty
tonsillitis: inflammation of the tonsils, usu-ally due to an acute infection
xerostomia: dryness of the mouth from avariety of causes

in the fall in order to achieve immunity prior to the beginning ofthe “flu season.”
VIRAL RHINITIS (COMMON COLD)The term “common cold” often is used when referring to anupper respiratory tract infection that is self-limited and caused bya virus (viral rhinitis). Nasal congestion, rhinorrhea, sneezing,sore throat, and general malaise characterize it. Specifically, theterm “cold” refers to an afebrile, infectious, acute inflammation
of the mucous membranes of the nasal cavity. More broadly, theterm refers to an acute upper respiratory tract infection, whereasterms such as “rhinitis,” “pharyngitis,” and “laryngitis” distinguishthe sites of the symptoms. It can also be used when the causativevirus is influenza (“the flu”). Colds are highly contagious becausevirus is shed for about 2 days before the symptoms appear andduring the first part of the symptomatic phase. It is estimated thatadults in the United States average two to four colds each year.The common cold is the most common cause of absenteeismfrom work and school (Mandell, Bennett, & Dolin, 2000).
The six viruses known to produce the signs and symptoms ofthe viral rhinitis are rhinovirus, parainfluenza virus, coronavirus,respiratory syncytial virus (RSV), influenza virus, and adenovirus.Each virus may have multiple strains. For example, there are over100 strains of rhinovirus, which accounts for 50% of all colds.The incidence of viral rhinitis follows a specific pattern during theyear, depending on the causative agent (Fig. 22-2). Even thoughviral rhinitis can occur at any time of the year, three waves ac-count for the epidemics in the United States:
• In September, just after the opening of school• In late January• Toward the end of April
Immunity after recovery is variable and depends on many fac-tors, including a person’s natural host resistance and the specificvirus that caused the cold.
Clinical ManifestationsSigns and symptoms of viral rhinitis are nasal congestion, runnynose, sneezing, nasal discharge, nasal itchiness, tearing watery eyes,“scratchy” or sore throat, general malaise, low-grade fever, chills,
494 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
FIGURE 22-1 Pathophysiologic processes in rhinitis and sinusitis. Althoughpathophysiologic processes are similar in rhinitis and sinusitis, they affect dif-ferent structures. In rhinitis (A), the mucous membranes lining the nasal pas-sages become inflamed, congested, and edematous. The swollen nasal conchaeblock the sinus openings, and mucus is discharged from the nostrils. Sinusitis(B) is also marked by inflammation and congestion, with thickened mucoussecretions filling the sinus cavities and occluding the openings.
Dischargingmucus
Occludedsinusopenings
Edematousconchae; polypsmay develop
A. Rhinitis
B. Sinusitis
Thick mucusoccludessinus cavityand preventsdrainage
Enlargednasalmucosa
Physiology/Pathophysiology
FIGURE 22-2 Schematic diagram incidence of viral rhinitis (commoncold) in the United States and the frequency of the causative agents. Redrawnfrom Goldman, L. & Bennett, J. C. (eds.) (2000) Cecil textbook of medicine(21st ed., Vol. 2). Philadelphia: W. B. Saunders, p. 1791.

and often headache and muscle aches. As the illness progresses,cough usually appears. In some people, viral rhinitis exacerbatesthe herpes simplex, commonly called a cold sore (Chart 22-1).
The symptoms last from 1 to 2 weeks. If there is significantfever or more severe systemic respiratory symptoms, it is nolonger viral rhinitis but one of the other acute upper respiratorytract infections. Allergic conditions can also affect the nose, mim-icking the symptoms of a cold.
Medical ManagementThere is no specific treatment for the common cold or influenza.Management consists of symptomatic therapy. Some measuresinclude providing adequate fluid intake, encouraging rest, pre-venting chilling, increasing intake of vitamin C, and using ex-pectorants as needed. Warm salt-water gargles soothe the sorethroat and nonsteroidal anti-inflammatory agents (NSAIDs)such as aspirin or ibuprofen relieve the aches, pains, and fever inadults. Antihistamines are used to relieve sneezing, rhinorrhea,and nasal congestion. Topical (nasal) decongestant agents may re-
lieve nasal congestion; however, if they are overused they maycreate a rebound congestion that may be worse than the originalsymptoms. Some research suggests that zinc lozenges may reducethe duration of cold symptoms if taken within the first 24 hoursof onset (Prasad, Fitzgerald, & Bao, 2000). Amantadine (Symme-trel) or rimantadine (Flumadine) may be prescribed prophylac-tically to decrease the signs and symptoms as well. Antimicrobialagents (antibiotics) should not be used because they do not affectthe virus or reduce the incidence of bacterial complications.
Nursing ManagementTEACHING PATIENTS SELF-CAREMost viruses can be transmitted in several ways: direct contactwith infected secretions; inhalation of large particles that land ona mucosal surface from coughing or sneezing; or inhalation ofsmall particles (aerosol) that may be suspended in the air for upto an hour. It is important to teach the patient how to break thechain of infection. Hand washing remains the most effective mea-sure to prevent transmission of organisms. The nurse teachesmethods to treat symptoms of the common cold and preventivemeasures (Chart 22-2).
ACUTE SINUSITISThe sinuses, mucus-lined cavities filled with air that drain nor-mally into the nose, are involved in a high proportion of upperrespiratory tract infections. If their openings into the nasal pas-sages are clear, the infections resolve promptly. However, if theirdrainage is obstructed by a deviated septum or by hypertrophiedturbinates, spurs, or nasal polyps or tumors, sinus infection maypersist as a smoldering secondary infection or progress to an acutesuppurative process (causing purulent discharge). Sinusitis af-fects over 14% of the population and accounts for billions of dol-lars in direct health care costs (Tierney, McPhee, & Papadakis,2001). Some individuals are more prone to sinusitis because oftheir occupations. For example, continuous exposure to environ-mental hazards such as paint, sawdust, and chemicals may resultin chronic inflammation of the nasal passages.
PathophysiologyAcute sinusitis is an infection of the paranasal sinuses. It fre-quently develops as a result of an upper respiratory infection, suchas an unresolved viral or bacterial infection, or an exacerbation ofallergic rhinitis. Nasal congestion, caused by inflammation, edema,and transudation of fluid, leads to obstruction of the sinus cavi-ties (see Fig. 22-1). This provides an excellent medium for bac-terial growth. Bacterial organisms account for more than 60% ofthe cases of acute sinusitis, namely Streptococcus pneumoniae,Haemophilus influenzae, and Moraxella catarrhalis (Murray &Nadel, 2001). Dental infections also have been associated withacute sinusitis.
Clinical ManifestationsSymptoms of acute sinusitis may include facial pain or pressureover the affected sinus area, nasal obstruction, fatigue, purulentnasal discharge, fever, headache, ear pain and fullness, dentalpain, cough, a decreased sense of smell, sore throat, eyelid edema,or facial congestion or fullness. Acute sinusitis can be difficultto differentiate from an upper respiratory infection or allergicrhinitis.
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 495
Colds and Cold Sores (Herpes Simplex Virus)
The herpes simplex virus (HSV-1) produces the familiar herpeslabialis, commonly called a cold sore or fever blister. In the past,this painful blisterlike lip sore was thought to be caused by a coldor a fever. Even now that scientists recognize the origin of herpeslabialis, the condition is still referred to as a cold sore. The herpesvirus infection remains latent in cells of the lips or nose and is acti-vated by stress, sunlight, and febrile illnesses from the common coldto streptococcal pneumonia, meningococcal meningitis, and evenmalaria.
The incubation period is 2 to 12 days. The virus is transmittedprimarily by direct contact with infected secretions. The virus mayalso be transmitted from an asymptomatic person. Small vesicles,single or clustered, may erupt on the lips, inside the mouth, in-cluding the tongue, soft and hard palate, gums, buccal mucosa, andthe pharynx. These soon rupture, forming sore shallow ulcers thatincrease in number. The gums may bleed and feel painful.
The herpes virus may subside spontaneously in 10 to 14 days.If it does not, acyclovir, an antiviral agent, may be administeredorally or topically to minimize the symptoms and the duration orlength of the flare-up. Analgesics, such as acetaminophen (Tylenol)with codeine or aspirin with codeine, are helpful in relieving painand discomfort. Topical anesthetics, such as lidocaine (Xylocaine)or dyclonine (Dyclone), and over-the-counter preparations, such asHerpecin-L, may relieve oral pain. Applications of drying lotionsor liquids may help to dry the lesions.
Chart22-1
Chart22-1
With permission from Goodheart, H. P. (1999). Photoguide of commonskin disorders: Diagnosis and management. Baltimore: LippincottWilliams & Wilkins.

Assessment and Diagnostic FindingsA careful history and physical examination are performed. Thehead and neck, particularly the nose, ears, teeth, sinuses, pharynx,and chest, are examined. There may be tenderness to palpationover the infected sinus area. The sinuses are percussed using theindex finger, tapping lightly to determine if the patient experi-ences pain. The affected area is also transilluminated; with sinusi-tis, there is a decrease in the transmission of light (see Chap. 21,Fig. 21-8). Sinus x-rays may be performed to detect sinus opac-ity, mucosal thickening, bone destruction, and air–fluid levels.Computed tomography scanning of the sinuses is the most effec-tive diagnostic tool. It is also used to rule out other local or sys-temic disorders, such as tumor, fistula, and allergy.
ComplicationsAcute sinusitis, if left untreated, may lead to severe and occa-sionally life-threatening complications such as meningitis, brainabscess, ischemic infarction, and osteomyelitis. Other complica-
tions of sinusitis, although uncommon, include severe orbital cel-lulitis, subperiosteal abscess, and cavernous sinus thrombosis.
Medical ManagementThe goals of treatment of acute sinusitis are to treat the infection,shrink the nasal mucosa, and relieve pain. There is a growing con-cern over the inappropriate use of antibiotics for viral upper res-piratory infections; such overuse has resulted in antibiotics beingless effective (more resistant) in treating bacterial infections suchas sinusitis. As a result, careful consideration is given to the po-tential pathogen before antimicrobial agents are prescribed.
The antimicrobial agents of choice for a bacterial infectionvary in clinical practice. First-line antibiotics include amoxicillin(Amoxil), trimethoprim/sulfamethoxazole (Bactrim, Septra), anderythromycin. Second-line antibiotics include cephalosporins suchas cefuroxime axetil (Ceftin), cefpodoxime (Vantin), and cef-prozil (Cefzil) and amoxicillin clavulanate (Augmentin). Newerand more expensive antibiotics with a broader spectrum include
496 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
Chart 22-2Home Care Checklist • Preventing and Managing Upper Respiratory Infections
At the completion of the home care instruction, the patient or caregiver will be able to:
Prevention• Identify strategies to prevent infection and, if infected, to prevent spread of infection to others ✓ ✓
Perform hand hygiene oftenUse disposable tissuesAvoid crowds during the flu seasonAvoid individuals with colds or respiratory infectionsObtain influenza vaccination, if recommended (especially if elderly or diagnosed with a chronic illness)
• Practice good health habits ✓ ✓
Eat a nutritious dietGet plenty of rest and sleepAvoid or reduce stress when possibleExercise appropriatelyAvoid smoking or second-hand smoke and excessive intake of alcoholIncrease humidity in house, especially during winterPractice adequate oral hygiene
• Avoid allergens, if allergies are associated with upper respiratory infections ✓
Prevention and Management• Identify strategies to control the environment ✓ ✓
Adequately humidify (avoid overhumidifying) living quartersPlace a dehumidifier in the basement, if appropriateProvide central ventilation fans, air conditioning with microstatic air filtersReduce irritants (dust, chemical, tobacco smoke) when possibleLimit exposure to animals and house pets, particularly in the bedroom
Management• Describe strategies to relieve symptoms of upper respiratory infection ✓ ✓
Gargle with salt waterIncrease fluid intake, particularly of hot liquidsProvide warm, moist air by shower or humidifier to relieve swollen mucous membranesAvoid irritants (dust, chemicals, tobacco smoke) when possible
• Recognize signs and symptoms of infection and state when to contact a health care provider ✓ ✓
Upper respiratory infection symptoms persisting longer than 7 to 10 daysExtreme red throat or white patches on the back of the throatDiscolored drainage or foul-smelling nasal dischargeProlonged fever of 100.5°F (38°C) >2 daysShortness of breath, wheezingSwollen lymph nodesSevere pain or tenderness around the eyes or persistent pain in sinus areasSevere headache
Patient Caregiver

macrolides, azithromycin (Zithromax), and clarithromycin(Biaxin). Quinolones such as ciprofloxacin (Cipro), levofloxacin(Levaquin) (used with severe penicillin allergy), and sparfloxacin(Zagam) have also been used. The course of treatment is usually10 to 14 days. A recent report found little difference in clinicaloutcomes between first-line and second-line antibiotics; however,costs were greater when newer second-line antibiotics were used(Piccirillo, Mager, Frisse et al., 2001).
Use of oral and topical decongestant agents may decrease mu-cosal swelling of nasal polyps, thereby improving drainage of thesinuses. Heated mist and saline irrigation also may be effective foropening blocked passages. Decongestant agents such as pseudo-ephedrine (Sudafed, Dimetapp) have proven effective because oftheir vasoconstrictive properties. Topical decongestant agentssuch as oxymetazoline (Afrin) may be used for up to 72 hours. Itis important to administer them with the patient’s head tiltedback to promote maximal dispersion of the medication. Guaife-nesin (Robitussin, Anti-Tuss), a mucolytic agent, may also be ef-fective in reducing nasal congestion.
In 2000, the U.S. Food and Drug Administration issued apublic health advisory concerning phenylpropanolamine, whichpreviously had been commonly used in oral decongestants anddiet pills. The voluntary recall of products containing this ingre-dient was based on a study linking its use with hemorrhagic strokein women. Men may also be at risk (Kernan et al., 2000).
Antihistamines such as diphenhydramine (Benadryl), ceti-rizine (Zyrtec), and fexofenadine (Allegra) may be used if an al-lergic component is suspected. If the patient continues to havesymptoms after 7 to 10 days, the sinuses may need to be irrigatedand hospitalization may be required.
Nursing ManagementTEACHING PATIENTS SELF-CAREPatient teaching is an important aspect of nursing care for the pa-tient with acute sinusitis. The nurse instructs the patient aboutmethods to promote drainage such as inhaling steam (steam bath,hot shower, and facial sauna), increasing fluid intake, and apply-ing local heat (hot wet packs). The nurse also informs the patientabout the side effects of nasal sprays and about rebound conges-tion. In the case of rebound congestion, the body’s receptors,which have become dependent on the decongestant sprays tokeep the nasal passages open, close and congestion results afterthe spray is discontinued.
The nurse stresses the importance of following the recom-mended antibiotic regimen, because a consistent blood level of themedication is critical to treat the infection. The nurse teaches thepatient the early signs of a sinus infection and recommends pre-ventive measures such as following healthy practices and avoidingcontact with people who have upper respiratory infections (seeChart 22-2).
The nurse should explain to the patient that fever, severeheadache, and nuchal rigidity are signs of potential complica-tions. If fever persists despite antibiotic therapy, the patientshould seek additional care.
CHRONIC SINUSITISChronic sinusitis is an inflammation of the sinuses that persistsfor more than 3 weeks in an adult and 2 weeks in a child. It is es-timated that 32 million people a year develop chronic sinusitis.
PathophysiologyA narrowing or obstruction in the ostia of the frontal, maxillary,and anterior ethmoid sinuses usually causes chronic sinusitis, pre-venting adequate drainage to the nasal passages. This combinedarea is known as the osteomeatal complex. Blockage that persistsfor greater than 3 weeks in an adult may occur because of infec-tion, allergy, or structural abnormalities. This results in stagnantsecretions, an ideal medium for infection. The organisms thatcause chronic sinusitis are the same as those implicated in acutesinusitis. Immunocompromised patients, however, are at in-creased risk for developing fungal sinusitis. Aspergillus fumigatusis the most common organism associated with fungal sinusitis.
Clinical ManifestationsClinical manifestations of chronic sinusitis include impaired mu-cociliary clearance and ventilation, cough (because the thick dis-charge constantly drips backward into the nasopharynx), chronichoarseness, chronic headaches in the periorbital area, and facialpain. These symptoms are generally most pronounced on awak-ening in the morning. Fatigue and nasal stuffiness are also com-mon. In addition, some patients experience a decrease in smelland taste and a fullness in the ears.
Assessment and Diagnostic FindingsA careful history and diagnostic assessment, including a com-puted tomography scan of the sinuses or magnetic resonanceimaging (if fungal sinusitis is suspected), are performed to ruleout other local or systemic disorders, such as tumor, fistula, andallergy. Nasal endoscopy may be indicated to rule out underlyingdiseases such as tumors and sinus mycetomas (fungus balls). Thefungus ball is usually a brown or greenish-black material with theconsistency of peanut butter or cottage cheese.
ComplicationsComplications of chronic sinusitis, although uncommon, includesevere orbital cellulitis, subperiosteal abscess, cavernous sinusthrombosis, meningitis, encephalitis, and ischemic infarction.
Medical ManagementMedical management of chronic sinusitis is almost the same asfor acute sinusitis. The antimicrobial agents of choice includeamoxicillin clavulanate (Augmentin) or ampicillin (Ampicin).Clarithromycin (Biaxin) and third-generation cephalosporinssuch as cefuroxime axetil (Ceftin), cefpodoxime (Vantin), andcefprozil (Cefzil) have also been effective. Levofloxacin (Lev-aquin), a quinolone, may also be used. The course of treatmentmay be 3 to 4 weeks. Decongestant agents, antihistamines, salinesprays, and heated mist may also provide some symptom relief.
SURGICAL MANAGEMENTWhen standard medical therapy fails, surgery, usually endo-scopic, may be indicated to correct structural deformities that ob-struct the ostia (openings) of the sinus. Excising and cauterizingnasal polyps, correcting a deviated septum, incising and drainingthe sinuses, aerating the sinuses, and removing tumors are someof the specific procedures performed. When sinusitis is caused bya fungal infection, surgery is required to excise the fungus ball andnecrotic tissue and drain the sinuses. Oral and topical cortico-
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 497

steroids are usually prescribed. Antimicrobial agents are admin-istered before and after surgery. Some patients with severe chronicsinusitis obtain relief only by moving to a dry climate.
Nursing ManagementBecause the patient usually performs care measures for sinusitis athome, nursing management consists mainly of patient teaching.
TEACHING PATIENTS SELF-CAREThe nurse teaches the patient how to promote sinus drainage byincreasing the environmental humidity (steam bath, hot shower,and facial sauna), increasing fluid intake, and applying local heat(hot wet packs). The nurse also instructs the patient about the im-portance of following the medication regimen. Instructions onthe early signs of a sinus infection are provided and preventivemeasures are reviewed.
ACUTE PHARYNGITISAcute pharyngitis is an inflammation or infection in the throat,usually causing symptoms of a sore throat.
PathophysiologyMost cases of acute pharyngitis are caused by viral infection. Whengroup A beta-hemolytic streptococcus, the most common bacte-rial organism, causes acute pharyngitis, the condition is known asstrep throat (Bisno, 2001). The body responds by triggering an in-flammatory response in the pharynx. This results in pain, fever,vasodilation, edema, and tissue damage, manifested by redness andswelling in the tonsillar pillars, uvula, and soft palate. A creamy ex-udate may be present in the tonsillar pillars (Fig. 22-3).
Uncomplicated viral infections usually subside promptly,within 3 to 10 days after the onset. However, pharyngitis causedby more virulent bacteria such as group A beta-hemolytic strep-tococci is a more severe illness. If left untreated, the complicationscan be severe and life-threatening. Complications include sinusitis,otitis media, peritonsillar abscess, mastoiditis, and cervical adeni-tis. In rare cases the infection may lead to bacteremia, pneumonia,meningitis, rheumatic fever, or nephritis.
Clinical ManifestationsThe signs and symptoms of acute pharyngitis include a fiery-redpharyngeal membrane and tonsils, lymphoid follicles that areswollen and flecked with white-purple exudate, and enlarged andtender cervical lymph nodes and no cough. Fever, malaise, andsore throat also may be present.
Assessment and Diagnostic FindingsRapid screening tests for streptococcal antigens such as the latexagglutination (LA) antigen test and solid-phase enzyme immuno-assays (ELISA), optical immunoassay (OIA), streptolysin titers,and throat cultures are used to determine the causative organism,after which appropriate therapy is prescribed. Nasal swabs andblood cultures may also be necessary to identify the organism(Corneli, 2001).
Medical ManagementViral pharyngitis is treated with supportive measures since an-tibiotics will have no effect on the organism. Bacterial pharyngi-tis is treated with a variety of antimicrobial agents.
PHARMACOLOGIC THERAPYIf a bacterial cause is suggested or demonstrated, penicillin is usu-ally the treatment of choice. For patients who are allergic to peni-cillin or have organisms that are resistant to erythromycin (onefifth of group A beta-hemolytic streptococci and most S. aureusorganisms are resistant to penicillin and erythromycin), cepha-losporins and macrolides (clarithromycin and azithromycin) maybe used. Antibiotics are administered for at least 10 days toeradicate the infection from the oropharynx.
Severe sore throats can also be relieved by analgesic medica-tions, as prescribed. For example, aspirin or acetaminophen(Tylenol) can be taken at 3- to 6-hour intervals; if required, acet-aminophen with codeine can be taken three or four times daily.Antitussive medication, in the form of codeine, dextromethor-phan (Robitussin DM), or hydrocodone bitartrate (Hycodan),may be required to control the persistent and painful cough thatoften accompanies acute pharyngitis.
NUTRITIONAL THERAPYA liquid or soft diet is provided during the acute stage of the dis-ease, depending on the patient’s appetite and the degree of dis-comfort that occurs with swallowing. Occasionally, the throat isso sore that liquids cannot be taken in adequate amounts bymouth. In severe situations, fluids are administered intravenously.Otherwise, the patient is encouraged to drink as much fluid as pos-sible (at least 2 to 3 L per day).
Nursing ManagementThe nurse instructs the patient to stay in bed during the febrilestage of illness and to rest frequently once up and about. Used tis-sues should be disposed of properly to prevent the spread of in-fection. It is important to examine the skin once or twice daily for
498 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
FIGURE 22-3 Pharyngitis—inflam-mation without exudate. (A) Rednessand vascularity of the pillars and uvulaare mild to moderate. (B) Redness isdiffuse and intense. Each patient wouldprobably complain of a sore throat.From Bickley, L. S. (2003). Bates’ guideto physical examination and history tak-ing (8th ed.). Philadelphia: LippincottWilliams & Wilkins.
A B

possible rash, because acute pharyngitis may precede some othercommunicable diseases (ie, rubella).
Warm saline gargles or irrigations are used depending on theseverity of the lesion and the degree of pain. The benefits of thistreatment depend on the degree of heat that is applied. The nurseteaches the patient about the recommended temperature of thesolution: high enough to be effective and as warm as the patientcan tolerate, usually 105°F to 110°F (40.6°C to 43.3°C). Irri-gating the throat properly is an effective means of reducing spasmin the pharyngeal muscles and relieving soreness of the throat.Unless the purpose of the procedure and its technique are un-derstood clearly by the patient and family, the results may be lessthan satisfactory.
An ice collar also can relieve severe sore throats. Mouth care mayadd greatly to the patient’s comfort and prevent the developmentof fissures (cracking) of the lips and oral inflammation when bac-terial infection is present. The nurse instructs the patient to resumeactivity gradually. A full course of antibiotic therapy is indicated inpatients with group A beta-hemolytic streptococcal infection inview of the possible development of complications such as nephri-tis and rheumatic fever, which may have their onset 2 or 3 weeksafter the pharyngitis has subsided. The nurse instructs the patientand family about the importance of taking the full course of ther-apy and informs them about the symptoms to watch for that mayindicate complications.
CHRONIC PHARYNGITISChronic pharyngitis is a persistent inflammation of the pharynx.It is common in adults who work or live in dusty surroundings,use their voice to excess, suffer from chronic cough, and habitu-ally use alcohol and tobacco.
Three types of chronic pharyngitis are recognized:
• Hypertrophic: characterized by general thickening and con-gestion of the pharyngeal mucous membrane
• Atrophic: probably a late stage of the first type (the mem-brane is thin, whitish, glistening, and at times wrinkled)
• Chronic granular (“clergyman’s sore throat”): character-ized by numerous swollen lymph follicles on the pharyn-geal wall
Clinical ManifestationsPatients with chronic pharyngitis complain of a constant sense ofirritation or fullness in the throat, mucus that collects in the throatand can be expelled by coughing, and difficulty swallowing.
Medical ManagementTreatment of chronic pharyngitis is based on relieving symptoms,avoiding exposure to irritants, and correcting any upper respira-tory, pulmonary, or cardiac condition that might be responsiblefor a chronic cough.
Nasal congestion may be relieved by short-term use of nasalsprays or medications containing ephedrine sulfate (Kondon’sNasal) or phenylephrine hydrochloride (Neo-Synephrine). If thereis a history of allergy, one of the antihistamine decongestant med-ications, such as Drixoral or Dimetapp, is taken orally every 4 to6 hours. Aspirin or acetaminophen is recommended for its anti-inflammatory and analgesic properties.
Nursing ManagementTEACHING PATIENTS SELF-CARETo prevent the infection from spreading, the nurse instructs thepatient to avoid contact with others until the fever subsides.Alcohol, tobacco, second-hand smoke, and exposure to cold areavoided, as are environmental or occupational pollutants if pos-sible. The patient may minimize exposure to pollutants by wear-ing a disposable facemask. The nurse encourages the patient to drink plenty of fluids. Gargling with warm saline solutionsmay relieve throat discomfort. Lozenges will keep the throatmoistened.
TONSILLITIS AND ADENOIDITISThe tonsils are composed of lymphatic tissue and are situated oneach side of the oropharynx. The faucial or palatine tonsils andlingual tonsils are located behind the pillars of fauces and tongue,respectively. They frequently serve as the site of acute infection(tonsillitis). Chronic tonsillitis is less common and may be mis-taken for other disorders such as allergy, asthma, and sinusitis.
The adenoids or pharyngeal tonsils consist of lymphatic tissuenear the center of the posterior wall of the nasopharynx. Infec-tion of the adenoids frequently accompanies acute tonsillitis.Group A beta-streptococcus is the most common organism asso-ciated with tonsillitis and adenoiditis.
Clinical ManifestationsThe symptoms of tonsillitis include sore throat, fever, snoring,and difficulty swallowing. Enlarged adenoids may cause mouth-breathing, earache, draining ears, frequent head colds, bronchi-tis, foul-smelling breath, voice impairment, and noisy respiration.Unusually enlarged adenoids fill the space behind the posteriornares, making it difficult for the air to travel from the nose to thethroat and resulting in a nasal obstruction. Infection can extendto the middle ears by way of the auditory (eustachian) tubes andmay result in acute otitis media, which can lead to spontaneousrupture of the eardrums and further extension of the infectioninto the mastoid cells, causing acute mastoiditis. The infectionalso may reside in the middle ear as a chronic, low-grade, smol-dering process that eventually may cause permanent deafness.
Assessment and Diagnostic FindingsA thorough physical examination is performed and a careful his-tory is obtained to rule out related or systemic conditions. Thetonsillar site is cultured to determine the presence of bacterial in-fection. In adenoiditis, if recurrent episodes of suppurative otitismedia result in hearing loss, the patient should be given a com-prehensive audiometric examination (see Chap. 59).
Medical ManagementTonsillectomy is usually performed for recurrent tonsillitis whenmedical treatment is unsuccessful and there is severe hypertrophy,asymmetry, or peritonsillar abscess that occludes the pharynx,making swallowing difficult and endangering the airway (partic-ularly during sleep). Enlargement of the tonsils is rarely an indi-cation for their removal; most children normally have largetonsils, which decrease in size with age. Despite the continuingdebate over the effectiveness of many tonsillectomies, the opera-tion is still a common surgical procedure in the United States.
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 499

Tonsillectomy or adenoidectomy is indicated only if the pa-tient has had any of the following problems: repeated bouts oftonsillitis; hypertrophy of the tonsils and adenoids that couldcause obstruction and obstructive sleep apnea; repeated attacksof purulent otitis media; suspected hearing loss due to serous oti-tis media that has occurred in association with enlarged tonsilsand adenoids; and some other conditions, such as an exacerba-tion of asthma or rheumatic fever. Appropriate antibiotic therapyis initiated for patients undergoing tonsillectomy or adenoidec-tomy. The most common antimicrobial agent is oral penicillin,which is taken for 7 days. Amoxicillin and erythromycin arealternatives.
Nursing ManagementPROVIDING POSTOPERATIVE CAREContinuous nursing observation is required in the immediatepostoperative and recovery period because of the significant riskof hemorrhage. In the immediate postoperative period, the mostcomfortable position is prone with the head turned to the side toallow drainage from the mouth and pharynx. The nurse must notremove the oral airway until the patient’s gag and swallowing re-flexes have returned. The nurse applies an ice collar to the neck,and a basin and tissues are provided for the expectoration ofblood and mucus.
Bleeding may be bright red if the patient expectorates bloodbefore swallowing it Often, however, the patient swallows theblood, which immediately becomes brown because of the actionof the acidic gastric juice.
Hemorrhage is a potential complication after a tonsillectomyand adenoidectomy. If the patient vomits large amounts of darkblood or bright-red blood at frequent intervals, or if the pulse rateand temperature rise and the patient is restless, the nurse notifiesthe surgeon immediately. The nurse should have the followingitems ready for examination of the surgical site for bleeding: alight, a mirror, gauze, curved hemostats, and a waste basin.
Occasionally, suture or ligation of the bleeding vessel is re-quired. In such cases, the patient is taken to the operating roomand given general anesthesia. After ligation, continuous nursingobservation and postoperative care are required, as in the initialpostoperative period.
If there is no bleeding, water and ice chips may be given to thepatient as soon as desired. The patient is instructed to refrainfrom too much talking and coughing because these activities canproduce throat pain.
TEACHING PATIENTS SELF-CARETonsillectomy and adenoidectomy usually do not require hospi-talization and are performed as outpatient surgery with a shortlength of stay. Because the patient will be sent home soon aftersurgery, the patient and family must understand the signs andsymptoms of hemorrhage. Hemorrhage usually occurs in the first12 to 24 hours. The patient is instructed to report frank redbleeding to the physician.
Alkaline mouthwashes and warm saline solutions are useful incoping with the thick mucus and halitosis that may be presentafter surgery. It is important to explain to the patient that a sorethroat, stiff neck, and vomiting may occur in the first 24 hours.A liquid or semiliquid diet is given for several days. Sherbet andgelatin are acceptable foods. The patient should avoid spicy, hot,acidic, or rough foods. Milk and milk products (ice cream andyogurt) may be restricted because they may make removal ofmucus more difficult.
The nurse explains to the patient that halitosis and someminor ear pain may occur for the first few days. The nurse in-structs the patient to avoid vigorous tooth brushing or gargling,since these actions could cause bleeding.
PERITONSILLAR ABSCESSA peritonsillar abscess is a collection of purulent exudate betweenthe tonsillar capsule and the surrounding tissues, including thesoft palate. It is believed to develop after an acute tonsillar infec-tion, which progresses to a local cellulitis and abscess.
Clinical ManifestationsThe usual symptoms of an infection are present, together withsuch local symptoms as a raspy voice, odynophagia (a severe sen-sation of burning, squeezing pain while swallowing), dysphagia(difficulty swallowing), otalgia (pain in the ear), and drooling. Anexamination shows marked swelling of the soft palate, often oc-cluding almost half of the opening from the mouth into the phar-ynx, unilateral tonsillar hypertrophy, and dehydration.
Assessment and Diagnostic FindingsAspiration of purulent material (pus) by needle aspiration is re-quired to make the appropriate diagnosis. The aspirated materialis sent for culture and Gram’s stain. A CTscan is performed whenit is not possible to aspirate the abscess.
Medical ManagementAntibiotics (usually penicillin) are extremely effective in control-ling the infection in peritonsillar abscess. If antibiotics are pre-scribed early in the course of the disease, the abscess may resolvewithout needing to be incised.
SURGICAL MANAGEMENTIf treatment is delayed, the abscess is evacuated as soon as possi-ble. The mucous membrane over the swelling is first sprayed witha topical anesthetic and then injected with a local anesthetic. Sin-gle or repeated needle aspirations are performed to decompressthe abscess. The abscess may also be incised and drained. Theseprocedures are performed best with the patient in the sitting po-sition to make it easier to expectorate the pus and blood that ac-cumulate in the pharynx. Almost immediate relief is experienced.Approximately 30% of patients with peritonsillar abscess have in-dications for tonsillectomy (Tierney et al., 2001).
Nursing ManagementConsiderable relief may be obtained by the use of topical anes-thetic agents and throat irrigations or the frequent use of mouth-washes or gargles, using saline or alkaline solutions at a temperatureof 105°F to 110°F (40.6°C to 43.3°C). The nurse instructs thepatient to gargle at intervals of 1 or 2 hours for 24 to 36 hours.Liquids that are cool or at room temperature are usually welltolerated.
LARYNGITISLaryngitis, an inflammation of the larynx, often occurs as a re-sult of voice abuse or exposure to dust, chemicals, smoke, andother pollutants, or as part of an upper respiratory tract infection.
500 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION

It also may be caused by isolated infection involving only thevocal cords.
The cause of infection is almost always a virus. Bacterial inva-sion may be secondary. Laryngitis is usually associated with aller-gic rhinitis or pharyngitis. The onset of infection may be associatedwith exposure to sudden temperature changes, dietary deficien-cies, malnutrition, and an immunosuppressed state. Laryngitis iscommon in the winter and is easily transmitted.
Clinical ManifestationsSigns of acute laryngitis include hoarseness or aphonia (completeloss of voice) and severe cough. Chronic laryngitis is marked bypersistent hoarseness. Laryngitis may be a complication of upperrespiratory infections.
Medical ManagementManagement of acute laryngitis includes resting the voice, avoid-ing smoking, resting, and inhaling cool steam or an aerosol. If thelaryngitis is part of a more extensive respiratory infection due toa bacterial organism or if it is severe, appropriate antibacterialtherapy is instituted. The majority of patients recover with con-servative treatment; however, laryngitis tends to be more severein elderly patients and may be complicated by pneumonia.
For chronic laryngitis, the treatment includes resting the voice,eliminating any primary respiratory tract infection, eliminat-ing smoking, and avoiding second-hand smoke. Topical corti-costeroids, such as beclomethasone dipropionate (Vanceril)inhalation, may also be used. These preparations have no sys-temic or long-lasting effects and may reduce local inflammatoryreactions.
Nursing ManagementThe nurse instructs the patient to rest the voice and to maintaina well-humidified environment. If laryngeal secretions are presentduring acute episodes, expectorant agents are suggested, alongwith a daily fluid intake of 3 L to thin secretions.
NURSING PROCESS: THE PATIENT WITH UPPER AIRWAY INFECTIONAssessmentA health history may reveal signs and symptoms of headache, sorethroat, pain around the eyes and on either side of the nose, diffi-culty in swallowing, cough, hoarseness, fever, stuffiness, and gen-eralized discomfort and fatigue. Determining when thesymptoms began, what precipitated them, what if anything re-lieves them, and what aggravates them is part of the assessment.It also is important to determine any history of allergy or the ex-istence of a concomitant illness.
Inspection may reveal swelling, lesions, or asymmetry of thenose as well as bleeding or discharge. The nurse inspects the nasalmucosa for abnormal findings such as increased redness, swelling,or exudate, and nasal polyps, which may develop in chronicrhinitis.
The nurse palpates the frontal and maxillary sinuses for ten-derness, which suggests inflammation, and then inspects thethroat by having the patient open the mouth wide and take a deepbreath. The tonsils and pharynx are inspected for abnormal find-
ings such as redness, asymmetry, or evidence of drainage, ulcera-tion, or enlargement.
Next the nurse palpates the trachea to determine the midlineposition in the neck and to detect any masses or deformities. Theneck lymph nodes also are palpated for associated enlargementand tenderness.
DiagnosisNURSING DIAGNOSESBased on the assessment data, the patient’s major nursing diag-noses may include the following:
• Ineffective airway clearance related to excessive mucus pro-duction secondary to retained secretions and inflammation
• Acute pain related to upper airway irritation secondary toan infection
• Impaired verbal communication related to physiologicchanges and upper airway irritation secondary to infectionor swelling
• Deficient fluid volume related to increased fluid loss sec-ondary to diaphoresis associated with a fever
• Deficient knowledge regarding prevention of upper respi-ratory infections, treatment regimen, surgical procedure, orpostoperative care
COLLABORATIVE PROBLEMS/POTENTIAL COMPLICATIONSBased on assessment data, potential complications may include:
• Sepsis• Meningitis• Peritonsillar abscess• Otitis media• Sinusitis
Planning and GoalsThe major goals for the patient may include maintenance of apatent airway, relief of pain, maintenance of effective means ofcommunication, normal hydration, knowledge of how to preventupper airway infections, and absence of complications.
Nursing InterventionsMAINTAINING A PATENT AIRWAYAn accumulation of secretions can block the airway in patientswith an upper airway infection. As a result, changes in the respi-ratory pattern occur, and the work of breathing required to getbeyond the blockage increases. The nurse can implement severalmeasures to loosen thick secretions or to keep the secretions moistso that they can be easily expectorated. Increasing fluid intakehelps thin the mucus. Use of room vaporizers or steam inhalationalso loosens secretions and reduces inflammation of the mucousmembranes. To enhance drainage from the sinuses, the nurse in-structs the patient about the best position to assume; this dependson the location of the infection or inflammation. For example,drainage for sinusitis or rhinitis is achieved in the upright posi-tion. In some conditions, topical or systemic medications, whenprescribed, help to relieve nasal or throat congestion.
PROMOTING COMFORTUpper respiratory tract infections usually produce localized dis-comfort. In sinusitis, pain may occur in the area of the sinuses or
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 501

may produce a general headache. In pharyngitis, laryngitis, ortonsillitis, a sore throat occurs. The nurse encourages the patientto take analgesics, such as acetaminophen with codeine, as pre-scribed, which will help relieve this discomfort. Other helpfulmeasures include topical anesthetic agents for symptomatic reliefof herpes simplex blisters (see Chart 22-1) and sore throats, hotpacks to relieve the congestion of sinusitis and promote drainage,and warm water gargles or irrigations to relieve the pain of a sorethroat. The nurse encourages rest to relieve the generalized dis-comfort and fever that accompany many upper airway conditions(especially rhinitis, pharyngitis, and laryngitis). The nurse in-structs the patient in general hygiene techniques to prevent thespread of infection. For postoperative care following tonsillec-tomy and adenoidectomy, an ice collar may reduce swelling anddecrease bleeding.
PROMOTING COMMUNICATIONUpper airway infections may result in hoarseness or loss of speech.The nurse instructs the patient to refrain from speaking as muchas possible and to communicate in writing instead, if possible.Additional strain on the vocal cords may delay full return of thevoice.
ENCOURAGING FLUID INTAKEIn upper airway infections, the work of breathing and the respi-ratory rate increase as inflammation and secretions develop. This,in turn, may increase insensible fluid loss. Fever further increasesthe metabolic rate, diaphoresis, and fluid loss.
Sore throat, malaise, and fever may interfere with a patient’swillingness to eat. The nurse encourages the patient to drink 2 to3 L of fluid per day during the acute stage of airway infection, un-less contraindicated, to thin secretions and promote drainage.Liquids (hot or cold) may be soothing, depending on the illness.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-CarePrevention of most upper airway infections is difficult because ofthe many potential causes. However, most upper respiratory in-fections are transmitted by hand-to-hand contact. Therefore, it isimportant to teach the patient and family how to minimize thespread of infection to others. Other preventive strategies are iden-tified in Chart 22-2. The nurse advises the patient to avoid ex-posure to others at risk for serious illness if respiratory infectionis transmitted. Those at risk include elderly adults, immuno-suppressed people, and those with chronic health problems.
The nurse teaches patients and their families strategies to re-lieve symptoms of upper respiratory infections. These include in-creasing the humidity level, encouraging adequate fluid intake,getting adequate rest, using warm water gargles or irrigations andtopical anesthetic agents to relieve sore throat, and applying hotpacks to relieve congestion. The nurse reinforces the need to com-plete the treatment regimen, particularly when antibiotics areprescribed.
Continuing CareReferral for home care is rare. However, it may be indicated forthe person whose health status was compromised before the onsetof the respiratory infection and for those who cannot manage self-care without assistance. In such circumstances, the home carenurse assesses the patient’s respiratory status and progress in re-covery. The nurse may advise elderly patients and those whowould be at increased risk from a respiratory infection to consider
an annual influenza vaccine. A follow-up appointment with theprimary care provider may be indicated for patients with com-promised health status to ensure that the respiratory infection hasresolved.
MONITORING AND MANAGING POTENTIAL COMPLICATIONSWhile major complications of upper respiratory infections arerare, the nurse must be aware of them and assess the patient forthem. Because most patients with upper respiratory infections aremanaged at home, patients and their families must be instructedto monitor for signs and symptoms and to seek immediate med-ical care if the patient’s condition does not improve or if the pa-tient’s physical status appears to be worsening.
Sepsis and meningitis may occur in patients with compro-mised immune status or in those with an overwhelming bacterialinfection. The patient with an upper respiratory infection andfamily members are instructed to seek medical care if the patient’scondition fails to improve within several days of the onset ofsymptoms, if unusual symptoms develop, or if the patient’s con-dition deteriorates. They are instructed about signs and symp-toms that require further attention: persistent or high fever,increasing shortness of breath, confusion, and increasing weak-ness and malaise. The patient with sepsis requires expert care totreat the infection, stabilize vital signs, and prevent or treat sep-ticemia and shock. Deterioration of the patient’s condition ne-cessitates intensive care measures (eg, hemodynamic monitoringand administration of vasoactive medications, intravenous fluids,nutritional support, corticosteroids) to monitor the patient’s sta-tus and to support the patient’s vital signs. High doses of antibi-otics may be administered to treat the causative organism. Thenurse’s role is to monitor the patient’s vital signs, hemodynamicstatus, and laboratory values, administer needed treatment, alle-viate the patient’s physical discomfort, and provide explanations,teaching, and emotional support to the patient and family.
Peritonsillar abscess may develop following an acute infectionof the tonsils. The patient requires treatment to drain the abscessand receives antibiotics for infection and topical anesthetic agentsand throat irrigations to relieve pain and sore throat. Follow-upis necessary to ensure that the abscess resolves; tonsillectomy maybe required. The nurse assists the patient in administering throatirrigations and instructs the patient and family about the impor-tance of adhering to the prescribed treatment regimen and rec-ommended follow-up appointments.
Otitis media and sinusitis may develop with upper respiratoryinfection. The patient and family are instructed about the signsand symptoms of otitis media and sinusitis and about the impor-tance of follow-up with the primary health care practitioner toensure adequate evaluation and treatment of these conditions.
EvaluationEXPECTED PATIENT OUTCOMESExpected patient outcomes may include:
1. Maintains a patent airway by managing secretionsa. Reports decreased congestionb. Assumes best position to facilitate drainage of secretions
2. Reports feeling more comfortablea. Uses comfort measures: analgesics, hot packs, gargles,
restb. Demonstrates adequate oral hygiene
3. Demonstrates ability to communicate needs, wants, levelof comfort
502 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION

4. Maintains adequate fluid intake5. Identifies strategies to prevent upper airway infections and
allergic reactionsa. Demonstrates hand hygiene techniqueb. Identifies the value of the influenza vaccine
6. Demonstrates an adequate level of knowledge and per-forms self-care adequately
7. Becomes free of signs and symptoms of infectiona. Exhibits normal vital signs (temperature, pulse, respira-
tory rate)b. Absence of purulent drainagec. Free of pain in ears, sinuses, and throat
Obstruction and Trauma of the Upper Respiratory AirwayOBSTRUCTION DURING SLEEPA variety of respiratory disorders are associated with sleep, themost common being sleep apnea syndrome. Sleep apnea syn-drome is defined as cessation of breathing (apnea) during sleep.
PathophysiologySleep apnea is classified into three types:
• Obstructive—lack of air flow due to pharyngeal occlusion• Central—simultaneous cessation of both air flow and res-
piratory movements• Mixed—a combination of central and obstructive apnea
within one apneic episode
The most common type of sleep apnea syndrome, obstructivesleep apnea, will be presented here.
Clinical ManifestationsIt is estimated that 12 million Americans have sleep apnea (Na-tional Institute of Health, 2000). It is more prevalent in men, es-pecially those who are older and overweight. Cigarette smokingis a risk factor. Obstructive sleep apnea is defined as frequent andloud snoring and breathing cessation for 10 seconds or more forfive episodes per hour or more, followed by awakening abruptlywith a loud snort as the blood oxygen level drops. Patients withsleep apnea may experience anywhere from five apneic episodesper hour to several hundred per night. Other symptoms includeexcessive daytime sleepiness, morning headache, sore throat, in-tellectual deterioration, personality changes, behavioral disorders,enuresis, impotence, obesity, and complaints by the partner thatthe patient snores loudly or is unusually restless during sleep(Chart 22-3).
The obstruction may be caused by mechanical factors such asa reduced diameter of the upper airway or dynamic changes in theupper airway during sleep. The activity of the tonic dilator mus-cles of the upper airway is reduced during sleep. These sleep-related changes may predispose the patient to increased upperairway collapse with the small amounts of negative pressuregenerated during inspiration. Obstructive sleep apnea may beassociated with obesity and with other conditions that reducepharyngeal muscle tone (eg, neuromuscular disease, sedative/hypnotic medications, acute ingestion of alcohol). The diagnosisof sleep apnea is made based on clinical features plus polysomno-graphic findings (sleep test), in which the cardiopulmonary sta-tus of the patient is monitored during an episode of sleep.
The effects of obstructive sleep apnea can seriously tax theheart and lungs. Repetitive apneic events result in hypoxia andhypercapnia, which triggers a sympathetic response. As a conse-quence, patients have a high prevalence of hypertension and anincreased risk of myocardial infarction and stroke. In patientswith underlying cardiovascular disease, the nocturnal hypoxemiamay predispose to dysrhythmias.
Medical ManagementPatients usually seek medical treatment because their partners ex-press concern or because they experience excessive sleeplessness atinappropriate times or settings (eg, while driving a car). A varietyof treatments are used. In mild cases, the patient is advised toavoid alcohol and medications that depress the upper airway andto lose weight. In more severe cases involving hypoxemia with se-vere CO2 retention (hypercapnia), the treatment includes con-tinuous positive airway pressure or bilevel positive airway pressuretherapy with supplemental oxygen via nasal cannula. These treat-ment methods are described in Chapter 25.
Surgical procedures (eg, uvulopalatopharyngoplasty) may beperformed to correct the obstruction. As a last resort, a trache-ostomy is performed to bypass the obstruction if the potential forrespiratory failure or life-threatening dysrhythmias exists. The tra-cheostomy is unplugged only during sleep. Although this is an ef-fective treatment, it is used in a limited number of patients becauseof its associated physical disfigurement (Murray & Nadel, 2001).
PHARMACOLOGIC THERAPYTreatment of central sleep apnea also includes medication. Pro-triptyline (Triptil) given at bedtime is thought to increase therespiratory drive and improve upper airway muscle tone. Med-roxyprogesterone acetate (Provera) and acetazolamide (Diamox)have been recommended for sleep apnea associated with chronicalveolar hypoventilation, but their benefits have not been well es-tablished. Administration of low-flow nasal oxygen at night canhelp relieve hypoxemia in some patients but has little effect onthe frequency or severity of apnea.
Nursing ManagementThe patient with obstructive sleep apnea may not recognize thepotential consequences of the disorder. Therefore, the nurse ex-plains the disorder in language that is understandable to the
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 503
Chart 22-3 • ASSESSMENT
Obstructive Sleep Apnea
Clinical features of obstructive sleep apnea include:Excessive daytime sleepinessFrequent nocturnal awakeningInsomniaLoud snoringMorning headachesIntellectual deteriorationPersonality changes, irritabilityImpotenceSystemic hypertensionDysrhythmiasPulmonary hypertension, cor pulmonalePolycythemiaEnuresis
patient and relates symptoms (daytime sleepiness) to the under-lying disorder. The nurse also instructs the patient and familyabout treatments, including the correct and safe use of oxygen, ifprescribed.
EPISTAXIS (NOSEBLEED)A hemorrhage from the nose, referred to as epistaxis, is causedby the rupture of tiny, distended vessels in the mucous membraneof any area of the nose. Rarely does epistaxis originate in thedensely vascular tissue over the turbinates. Most commonly, thesite is the anterior septum, where three major blood vessels enterthe nasal cavity: (1) the anterior ethmoidal artery on the forwardpart of the roof (Kesselbach’s plexus), (2) the sphenopalatineartery in the posterosuperior region, and (3) the internal maxil-lary branches (the plexus of veins located at the back of the lateralwall under the inferior turbinate).
There are a variety of causes associated with epistaxis, includingtrauma, infection, inhalation of illicit drugs, cardiovascular dis-eases, blood dyscrasias, nasal tumors, low humidity, a foreign bodyin the nose, and a deviated nasal septum. Additionally, vigorousnose blowing and nose picking have been associated with epistaxis.
Medical ManagementManagement of epistaxis depends on the location of the bleedingsite. A nasal speculum or headlight may be used to determine thesite of bleeding in the nasal cavity. Most nosebleeds originatefrom the anterior portion of the nose. Initial treatment may in-clude applying direct pressure. The patient sits upright with thehead tilted forward to prevent swallowing and aspiration of bloodand is directed to pinch the soft outer portion of the nose againstthe midline septum for 5 or 10 minutes continuously. If this mea-sure is unsuccessful, additional treatment is indicated. In anteriornosebleeds, the area may be treated with a silver nitrate applica-tor and Gelfoam, or by electrocautery. Topical vasoconstrictors,
such as adrenaline (1�1,000), cocaine (0.5%), and phenylephrinemay be prescribed.
If bleeding is occurring from the posterior regions, cottonpledgets soaked in a vasoconstricting solution may be insertedinto the nose to reduce the blood flow and improve the exam-iner’s view of the bleeding site. Alternatively, a cotton tamponmay be used to try to stop the bleeding. Suction may be used toremove excess blood and clots from the field of inspection. Thesearch for the bleeding site should shift from the anteroinferiorquadrant to the anterosuperior, then to the posterosuperior, andfinally to the posteroinferior area. The field is kept clear by usingsuction and by shifting the cotton tampon. Only about 60% ofthe total nasal cavity can actually be seen, however.
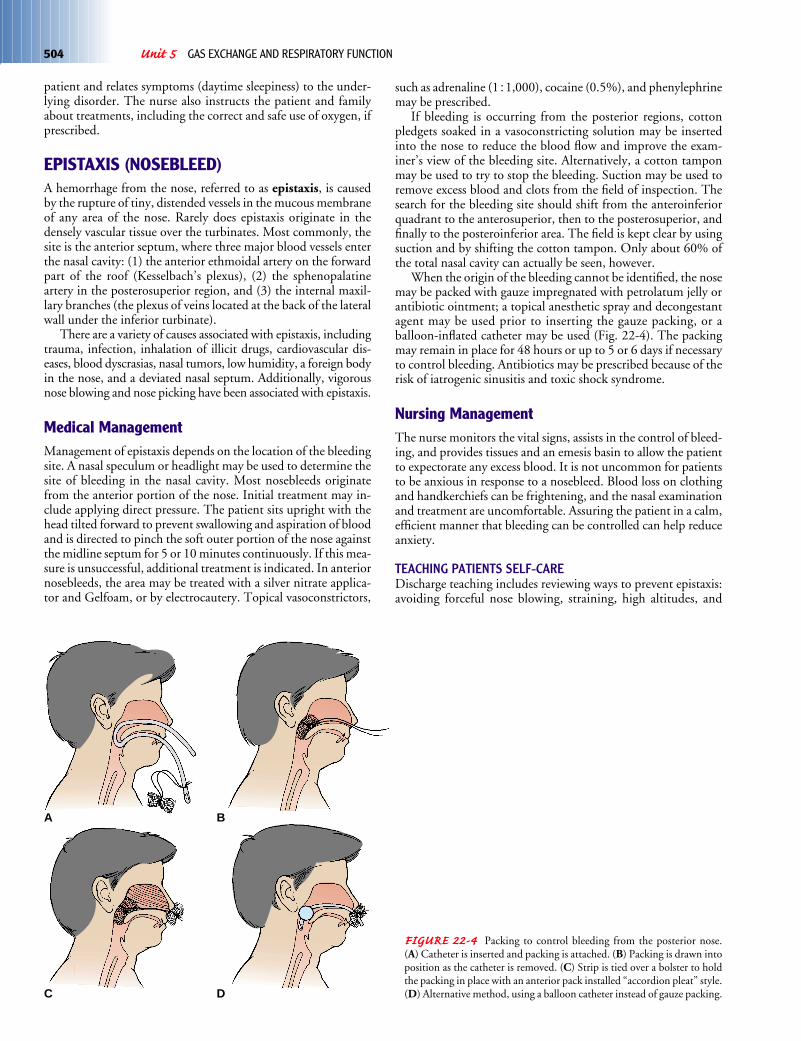
When the origin of the bleeding cannot be identified, the nosemay be packed with gauze impregnated with petrolatum jelly orantibiotic ointment; a topical anesthetic spray and decongestantagent may be used prior to inserting the gauze packing, or aballoon-inflated catheter may be used (Fig. 22-4). The packingmay remain in place for 48 hours or up to 5 or 6 days if necessaryto control bleeding. Antibiotics may be prescribed because of therisk of iatrogenic sinusitis and toxic shock syndrome.
Nursing ManagementThe nurse monitors the vital signs, assists in the control of bleed-ing, and provides tissues and an emesis basin to allow the patientto expectorate any excess blood. It is not uncommon for patientsto be anxious in response to a nosebleed. Blood loss on clothingand handkerchiefs can be frightening, and the nasal examinationand treatment are uncomfortable. Assuring the patient in a calm,efficient manner that bleeding can be controlled can help reduceanxiety.
TEACHING PATIENTS SELF-CAREDischarge teaching includes reviewing ways to prevent epistaxis:avoiding forceful nose blowing, straining, high altitudes, and
504 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
FIGURE 22-4 Packing to control bleeding from the posterior nose. (A) Catheter is inserted and packing is attached. (B) Packing is drawn intoposition as the catheter is removed. (C) Strip is tied over a bolster to holdthe packing in place with an anterior pack installed “accordion pleat” style.(D) Alternative method, using a balloon catheter instead of gauze packing.
A B
C D

nasal trauma (including nose picking). Adequate humidificationmay prevent drying of the nasal passages. The nurse instructs thepatient how to apply direct pressure to the nose with the thumband the index finger for 15 minutes in the case of a recurrentnosebleed. If recurrent bleeding cannot be stopped, the patient isinstructed to seek additional medical attention.
NASAL OBSTRUCTIONThe passage of air through the nostrils is frequently obstructed bya deviation of the nasal septum, hypertrophy of the turbinatebones, or the pressure of nasal polyps, which are grapelike swellingsthat arise from the mucous membrane of the sinuses, especiallythe ethmoids. This obstruction also may lead to a condition ofchronic infection of the nose and result in frequent episodes ofnasopharyngitis. Frequently, the infection extends to the sinusesof the nose. When sinusitis develops and the drainage from thesecavities is obstructed by deformity or swelling within the nose,pain is experienced in the region of the affected sinus.
Medical ManagementThe treatment of nasal obstruction requires the removal of theobstruction, followed by measures to overcome whatever chronicinfection exists. In many patients an underlying allergy requirestreatment. At times endoscopic surgery is necessary to drain thenasal sinuses. The specific procedure performed depends on thetype of nasal obstruction found. Usually, surgery is performedunder local anesthesia.
If a deviation of the septum is the cause of the obstruction, thesurgeon makes an incision into the mucous membrane and, afterraising it from the bone, removes the deviated bone and cartilagewith bone forceps. The mucosa then is allowed to fall back inplace and is held there by tight packing. Generally, the packingis soaked in liquid petrolatum so that it can be removed easily in24 to 36 hours. This operation is called a submucous resectionor septoplasty.
Nasal polyps are removed by clipping them at their base witha wire snare. Hypertrophied turbinates may be treated by apply-ing an astringent agent to shrink them.
Nursing ManagementMost of these procedures are performed on an outpatient basis.If the patient is hospitalized, the nurse elevates the head of thebed to promote drainage and to help alleviate discomfort fromedema. Frequent oral hygiene is encouraged to overcome drynesscaused by breathing through the mouth.
FRACTURES OF THE NOSEThe location of the nose makes it susceptible to injury by a widevariety of causes. In fact, nasal fractures are more common thanthose of any other bone in the body. Fractures of the nose usuallyresult from a direct assault. As a rule, no serious consequences re-sult, but the deformity that may follow often gives rise to ob-struction of the nasal air passages and to facial disfigurement.
Clinical ManifestationsThe signs and symptoms of a nasal fracture are bleeding from thenose externally and internally into the pharynx, swelling of thesoft tissues adjacent to the nose, and deformity.
Assessment and Diagnostic FindingsThe nose is examined internally to rule out the possibility that theinjury may be complicated by a fracture of the nasal septum anda submucosal septal hematoma. Because of the swelling andbleeding that occur with a nasal fracture, an accurate diagnosiscan be made only after the swelling subsides.
Clear fluid draining from either nostril suggests a fracture ofthe cribriform plate with leakage of cerebrospinal fluid. Becausecerebrospinal fluid contains glucose, it can readily be differenti-ated from nasal mucus by means of a dipstick (Dextrostix). Usu-ally, careful inspection or palpation will disclose any deviations ofthe bone or disruptions of the nasal cartilages. An x-ray may re-veal displacement of the fractured bones and may help rule outextension of the fracture into the skull.
Medical ManagementAs a rule, bleeding is controlled with the use of cold compresses.The nose is assessed for symmetry either before swelling has oc-curred or after it has subsided. The patient is referred to a spe-cialist, usually 3 to 5 days after the injury, to evaluate the need torealign the bones. Nasal fractures are surgically reduced 7 to 10 daysafter the injury.
Nursing ManagementThe nurse instructs the patient to apply ice packs to the nose for20 minutes four times each day to decrease swelling. The patientwho experiences bleeding from the nose (epistaxis) because of in-jury or for unexplained reasons is usually frightened and anxious.The packing inserted to stop the bleeding may be uncomfortableand unpleasant, and obstruction of the nasal passages by the pack-ing forces the patient to breathe through the mouth. This in turncauses the oral mucous membranes to become dry. Mouth rinseswill help to moisten the mucous membranes and to reduce theodor and taste of dried blood in the oropharynx and nasopharynx.
LARYNGEAL OBSTRUCTIONEdema of the larynx is a serious, often fatal, condition. The lar-ynx is a stiff box that will not stretch. It contains a narrow spacebetween the vocal cords (glottis) through which air must pass.Swelling of the laryngeal mucous membranes, therefore, may closeoff the opening tightly, leading to suffocation. Edema of the glot-tis occurs rarely in patients with acute laryngitis, occasionally inpatients with urticaria, and more frequently in patients with se-vere inflammations of the throat, as in scarlet fever. It is an occa-sional cause of death in severe anaphylaxis (angioneurotic edema).
Foreign bodies frequently are aspirated into the pharynx, thelarynx, or the trachea and cause a twofold problem. First, theyobstruct the air passages and cause difficulty in breathing, whichmay lead to asphyxia; later, they may be drawn farther down,entering the bronchi or a bronchial branch and causing symp-toms of irritation, such as a croupy cough, expectoration of bloodor mucus, or labored breathing. The physical signs and x-ray find-ings confirm the diagnosis.
Medical ManagementWhen the obstruction is caused by edema resulting from an al-lergic reaction, treatment includes administering subcutaneousepinephrine or a corticosteroid (see Chap. 53) and applying an
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 505

ice pack to the neck. In emergencies caused by obstruction by aforeign body, when signs of asphyxia are apparent, immediatetreatment is necessary. Frequently, if the foreign body has lodgedin the pharynx and can be visualized, the finger can dislodge it.
If the obstruction is in the larynx or the trachea, the nurse orother rescuer tries the subdiaphragmatic abdominal thrustmaneuver (Chart 22-4). If all efforts are unsuccessful, an im-mediate tracheotomy is necessary (see Chap. 25 for furtherdiscussion).
Cancer of the LarynxCancer of the larynx is a malignant tumor in the larynx (voicebox). It is potentially curable if detected early. It represents lessthan 1% of all cancers and occurs about four times more fre-quently in men than in women, and most commonly in persons50 to 70 years of age. The incidence of laryngeal cancer contin-ues to decline, but the incidence in women versus men continuesto increase. Each year in the United States, approximately 9,000new cases are discovered, and 3,700 persons with cancer of thelarynx will die (American Cancer Society, 2002).
Carcinogens that have been associated with the developmentof laryngeal cancer include tobacco (smoke, smokeless) and alco-hol and their combined effects, exposure to asbestos, mustard gas,wood dust, cement dust, tar products, leather, and metals. Othercontributing factors include straining the voice, chronic laryngi-tis, nutritional deficiencies (riboflavin), and family predisposition(Chart 22-5).
A malignant growth may occur in three different areas of thelarynx: the glottic area (vocal cords), supraglottic area (area abovethe glottis or vocal cords, including epiglottis and false cords),and subglottis (area below the glottis or vocal cords to the cricoid).Two thirds of laryngeal cancers are in the glottic area. Supraglotticcancers account for approximately one third of the cases, sub-glottic tumors for less than 1%. Glottic tumors seldom spread iffound early because of the limited lymph vessels found in thevocal cords (Lenhard, Osteen, & Gansler, 2001).
Clinical ManifestationsHoarseness of more than 2 weeks’ duration is noted early in thepatient with cancer in the glottic area because the tumor impedesthe action of the vocal cords during speech. The voice may soundharsh, raspy, and lower in pitch. Affected voice sounds are notearly signs of subglottic or supraglottic cancer. The patient maycomplain of a cough or sore throat that does not go away and painand burning in the throat, especially when consuming hot liquidsor citrus juices. A lump may be felt in the neck. Later symptomsinclude dysphagia, dyspnea (difficulty breathing), unilateral nasal
506 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
Performing the Abdominal Thrust Maneuver
To assist a patient or other person who is choking on a foreign object,the nurse performs the abdominal thrust maneuver (sometimes calledthe Heimlich maneuver) according to guidelines set forth by theAmerican Heart Association. (Note: Hands crossed at the neck is theuniversal sign for choking.)
1. Stand behind the person who is choking.2. Place both arms around the person’s waist.3. Make a fist with one hand with the thumb outside the fist.4. Place thumb side of fist against the person’s abdomen above
the navel and below the xiphoid process.5. Grasp fist with other hand.6. Quickly and forcefully exert pressure against the person’s di-
aphragm, pressing upward with quick, firm thrusts.7. Apply thrusts 6 to 10 times until the obstruction is cleared.8. The pressure from the thrusts should lift the diaphragm, force
air into the lungs, and create an artificial cough powerfulenough to expel the aspirated object.
Chart22-4
Chart22-4
Chart 22-5Risk Factors for Laryngeal Cancer
CarcinogensTobacco (smoke, smokeless)Combined effects of alcohol and tobaccoAsbestosSecond-hand smokePaint fumesWood dustCement dustChemicalsTar productsMustard gasLeather and metals
Other FactorsStraining the voiceChronic laryngitisNutritional deficiencies (riboflavin)History of alcohol abuseFamilial predispositionAge (higher incidence after 60 years of age)Gender (more common in men)Race (more prevalent in African Americans)Weakened immune system

obstruction or discharge, persistent hoarseness, persistent ulcera-tion, and foul breath. Cervical lymph adenopathy, unplannedweight loss, a general debilitated state, and pain radiating to theear may occur with metastasis.
Assessment and Diagnostic FindingsAn initial assessment includes a complete history and physical ex-amination of the head and neck. This will include assessment ofrisk factors, family history, and any underlying medical condi-tions. An indirect laryngoscopy, using a flexible endoscope, isinitially performed in the otolaryngologist’s office to visually eval-uate the pharynx, larynx, and possible tumor. Mobility of thevocal cords is assessed; if normal movement is limited, the growthmay affect muscle, other tissue, and even the airway. The lymph
nodes of the neck and the thyroid gland are palpated to determinespread of the malignancy (Haskell, 2001).
If a tumor of the larynx is suspected on an initial examination,a direct laryngoscopic examination is scheduled. This examina-tion is done under local or general anesthesia and allows evalua-tion of all areas of the larynx. Samples of the suspicious tissue areobtained for histologic evaluation. The tumor may involve any ofthe three areas of the larynx and may vary in appearance.
Squamous cell carcinoma accounts for over 90% of the casesof laryngeal carcinoma (Haskell, 2001). The staging of the tumorserves as a framework for the therapeutic regimen. The TNMclassification system, developed by the American Joint Commit-tee on Cancer (AJCC) (Chart 22-6), is the accepted method usedto classify head and neck tumors. The classification of the tumordetermines the suggested treatment modalities. Because many of
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 507

these lesions are submucosal, biopsy may require that an incisionbe made using microlaryngeal techniques or using a CO2 laser totransect the mucosa and reach the tumor.
Computed tomography and magnetic resonance imaging(MRI) are used to assess regional adenopathy and soft tissue andto help stage and determine the extent of a tumor. MRI is alsohelpful in post-treatment follow-up in order to detect a recur-rence. Positron emission tomography (PET scan) may also beused to detect recurrence of a laryngeal tumor after treatment.
Medical ManagementTreatment of laryngeal cancer depends on the staging of thetumor, which includes the location, size, and histology of thetumor and the presence and extent of cervical lymph node in-volvement. Treatment options include surgery, radiation therapy,and chemotherapy. The prognosis depends on a variety of factors:tumor stage, the patient’s gender and age, and pathologic featuresof the tumor, including the grade and depth of infiltration. Thetreatment plan also depends on whether this is an initial diagno-sis or a recurrence. Small glottic tumors, stage I and II, with noinfiltration to the lymph nodes are associated with a 75% to 95%survival rate. Patients with stage III and IV or advanced tumorshave a 50% to 60% survival rate and have a 50% chance of re-currence and a 30% chance of metastasis. The highest risk of la-ryngeal cancer recurrence is in the first 2 to 3 years. Recurrenceafter 5 years is rare and is usually due to a new primary malig-nancy (Lenhard et al., 2001) (Chart 22-7).
Surgery and radiation therapy are both effective methods inthe early stages of cancer of the larynx. Chemotherapy tradition-ally has been used for recurrence or metastatic disease. It has alsobeen used more recently in conjunction with either radiation
therapy to avoid a total laryngectomy or preoperatively to shrinka tumor before surgery. A complete dental examination is per-formed to rule out any oral disease. Any dental problems are re-solved, if possible, prior to surgery. If surgery is to be performed,a multidisciplinary team evaluates the needs of the patient andfamily to develop a successful plan of care (Forastiere et al., 2001).
SURGICAL MANAGEMENTRecent advances in surgical techniques for treating laryngeal can-cer may minimize the ensuing cosmetic and functional deficits.Depending on the location and staging of the tumor, four differ-ent types of laryngectomy (surgical removal of part or all of thelarynx and surrounding structures) are considered:
• Partial laryngectomy• Supraglottic laryngectomy• Hemilaryngectomy• Total laryngectomy
Some microlaryngeal surgery can be performed endoscopi-cally. The CO2 laser can be used for the treatment of manylaryngeal tumors, with the exception of large vascular tumors.
Partial Laryngectomy. A partial laryngectomy (laryngofissure–thyrotomy) is recommended in the early stages of cancer in theglottic area when only one vocal cord is involved. The surgery isassociated with a very high cure rate. It may also be performed fora recurrence when high-dose radiation has failed. A portion of thelarynx is removed, along with one vocal cord and the tumor; allother structures remain. The airway remains intact and the pa-tient is expected to have no difficulty swallowing. The voice qual-ity may change or the patient may be hoarse.
Supraglottic Laryngectomy. A supraglottic laryngectomy is in-dicated in the management of early (stage I) supraglottic andstage II lesions. The hyoid bone, glottis, and false cords are re-moved. The true vocal cords, cricoid cartilage, and trachea remainintact. During surgery, a radical neck dissection is performed onthe involved side. A tracheostomy tube (see Chap. 25) is left inthe trachea until the glottic airway is established. It is usuallyremoved after a few days and the stoma is allowed to close. Nutri-tion is provided through a nasogastric tube until there is healing,followed by a semisolid diet. Postoperatively, the patient may ex-perience some difficulty swallowing for the first 2 weeks. Aspirationis a potential complication since the patient must learn a newmethod of swallowing (supraglottic swallowing). The chief ad-vantage of this surgical procedure is that it preserves the voice,even though the quality of the voice may change. Speech therapyis required before and after surgery. The major problem is the highrisk for recurrence of the cancer; therefore, patients are selectedcarefully.
Hemilaryngectomy. A hemilaryngectomy is performed whenthe tumor extends beyond the vocal cord but is less than 1 cm insize and is limited to the subglottic area. It may be used in stage Iglottic lesions. In this procedure, the thyroid cartilage of the lar-ynx is split in the midline of the neck and the portion of the vocalcord (one true cord and one false cord) is removed with the tumor.The arytenoid cartilage and half of the thyroid are removed. Thepatient will have a tracheostomy tube and nasogastric tube inplace for 10 to 14 days following surgery. The patient is at risk foraspiration postoperatively. Some change may occur in the voicequality. The voice may be rough, raspy, and hoarse and have lim-ited projection. The airway and swallowing remain intact.
508 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
SituationA 68-year-old attorney was diagnosed with cancer of the larynx 8 years ago. He was treated successfully with radiation therapy, re-sulting in an altered voice quality. Recently, he has complained ofshortness of breath and difficulty swallowing. In the past fewmonths, he also has noticed a marked change in his voice and phys-ical condition, which he attributed to “winter colds.”
After a complete physical exam and an extensive diagnosticworkup and biopsy, it is determined that the cancer has recurred ata new primary site. His health care provider recommends surgery(a total laryngectomy) and chemotherapy as the best options. Thepatient states that he is not willing to “lose my voice and my liveli-hood” but instead will “take my chances.” He has also expressedconcern about his quality of life after surgery. His family has ap-proached you about trying to convince him to have surgery.
DilemmaThe patient’s right to refuse treatment conflicts with the family’swishes and recommendation from his health care provider.
Discussion1. Is the patient making a decision based upon all pertinent infor-
mation concerning his health status, treatment, options,risk/benefits, and long-term prognosis?
2. What arguments can be made to support the patient’s decisionto forego treatment?
3. What arguments can be made to question the patient’sdecision to forego treatment?
Chart 22-7 • Ethics and Related Issues

Total Laryngectomy. A total laryngectomy is performed in themost advanced stage IV laryngeal cancer, when the tumor extendsbeyond the vocal cords, or for recurrent or persistent cancer fol-lowing radiation therapy. In a total laryngectomy, the laryngealstructures are removed, including the hyoid bone, epiglottis,cricoid cartilage, and two or three rings of the trachea. The tongue,pharyngeal walls, and trachea are preserved. A total laryngec-tomy will result in permanent loss of the voice and a change inthe airway.
Many surgeons recommend that a radical neck dissection beperformed on the same side as the lesion even if no lymph nodesare palpable because metastasis to the cervical lymph nodes iscommon. Surgery is more difficult when the lesion involves themidline structures or both vocal cords. With or without neck dis-section, a total laryngectomy requires a permanent tracheal stomabecause the larynx that provides the protective sphincter is nolonger present. The tracheal stoma prevents the aspiration of foodand fluid into the lower respiratory tract. The patient will haveno voice but will have normal swallowing. A total laryngectomychanges the manner in which airflow is used for breathing andspeaking, as depicted in Figure 22-5. Complications that mayoccur include a salivary leak, wound infection from the develop-ment of a pharyngocutaneous fistula, stomal stenosis, and dys-phagia secondary to pharyngeal and cervical esophageal stricture.
RADIATION THERAPYThe goal of radiation therapy is to eradicate the cancer and pre-serve the function of the larynx. The decision to use radiationtherapy is based on several factors, including the staging of thetumor (usually used for stage I and stage II tumors as a standardtreatment option) and the patient’s overall health status, lifestyle(including occupation), and personal preference. Excellent resultshave been achieved with radiation therapy in patients with early-stage (I and II) glottic tumors when only one vocal cord is in-volved and there is normal mobility (ie, moves with phonation)and in small supraglottic lesions. One of the benefits of radiationtherapy is that patients retain a near-normal voice. A few may de-velop chondritis (inflammation of the cartilage) or stenosis; asmall number may later require laryngectomy.
Radiation therapy may also be used preoperatively to reducethe tumor size. Radiation therapy is combined with surgery in ad-vanced (stages III and IV) laryngeal cancer as adjunctive therapyto surgery or chemotherapy, and as a palliative measure. A vari-ety of clinical trials have combined chemotherapy and radiationtherapy in the treatment of advanced laryngeal tumors. Earlystudies suggest that combined modality therapy may improve thetumor’s response to radiation therapy. Radiation therapy com-bined with chemotherapy may be an alternative to a total laryn-gectomy.
The complications from radiation therapy are a result ofexternal radiation to the head and neck area, which may also in-clude the parotid gland responsible for mucus production. Thesymptoms may include acute mucositis, ulceration of the mucousmembranes, pain, xerostomia (dry mouth), loss of taste, dys-phasia, fatigue, and skin reactions. Later complications may in-clude laryngeal necrosis, edema, and fibrosis.
SPEECH THERAPYThe loss or alteration of speech is discussed with the patient andfamily before surgery, and the speech therapist conducts a pre-operative evaluation. During this time, the nurse should informthe patient and family about methods of communication that willbe available in the immediate postoperative period. These include
writing, lip speaking, and communication or word boards. A sys-tem of communication is established with the patient, family,nurse, and physician and implemented consistently after surgery.
A postoperative communication plan is also developed. Thethree most common techniques of alaryngeal communicationare esophageal speech, artificial larynx (electrolarynx), and tra-cheoesophageal puncture. Training in these techniques beginsonce medical clearance is obtained from the physician.
Esophageal Speech. Esophageal speech was the primary methodof alaryngeal speech taught to patients until the 1980s. The pa-tient needs the ability to compress air into the esophagus andexpel it, setting off a vibration of the pharyngeal esophageal seg-ment. The technique can be taught once the patient begins oralfeedings, approximately 1 week after surgery. First, the patient
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 509
Nasal cavitySoft palate
PharynxEpiglottisLarynxVocal cordsTrachea
Diaphragm
Lung
Speech
Minimalair enteringnose andmouth
Surgicaltie-off
Air flowingto lungs inand out ofopening inneck
FIGURE 22-5 Total laryngectomy produces a change in airflow for breath-ing and speaking. (A) Normal airflow. (B) Airflow after total laryngectomy.
A
B

learns to belch and is reminded to do so an hour after eating.Then the technique is practiced repeatedly. Later, this consciousbelching action is transformed into simple explosions of air fromthe esophagus for speech purposes. Thereafter, the speech thera-pist works with the patient in an attempt to make speech intelli-gible and as close to normal as possible. Because it takes a longtime to become proficient, the success rate is low.
Electric Larynx. If esophageal speech is not successful, or untilthe patient masters the technique, an electric larynx may be usedfor communication. This battery-powered apparatus projectssound into the oral cavity. When the mouth forms words (artic-ulated), the sounds from the electric larynx become audiblewords. The voice that is produced sounds mechanical, and somewords may be difficult to distinguish. The advantage is that thepatient is able to communicate with relative ease while workingto become proficient at either esophageal or tracheoesophagealpuncture speech.
Tracheoesophageal Puncture. The third technique of alaryngealspeech is tracheoesophageal puncture (Fig. 22-6). This techniqueis the most widely used because the speech associated with it mostresembles normal speech (the sound produced is a combinationof esophageal speech and voice), and it is easily learned. A valveis placed in the tracheal stoma to divert air into the esophagus andout of the mouth. Once the puncture is surgically created and hashealed, a voice prosthesis (Blom–Singer) is fitted over the punc-ture site. To prevent airway obstruction, the prosthesis is re-moved and cleaned when mucus builds up. A speech therapistteaches the patient how to produce sounds. Moving the tongueand lips to form the sound into words produces speech as before.Tracheoesophageal speech is successful in 80% to 90% of pa-tients (DeLisa & Gans, 1998).
NURSING PROCESS: THE PATIENT UNDERGOINGLARYNGECTOMYAssessmentThe nurse assesses the patient for the following symptoms:hoarseness, sore throat, dyspnea, dysphagia, or pain and burningin the throat. The neck is palpated for swelling.
If treatment includes surgery, the nurse must know the natureof the surgery to plan appropriate care. If the patient is expectedto have no voice, a preoperative evaluation by the speech thera-pist is indicated. The patient’s ability to hear, see, read, and writeis assessed. Visual impairment and functional illiteracy may cre-ate additional problems with communication and require creativeapproaches to ensure that the patient is able to communicate anyneeds.
In addition, the nurse determines the psychological readinessof the patient and family. The idea of cancer is terrifying to mostpeople. Fear is compounded by the possibility of permanentlylosing one’s voice and, in some cases, of having some degree ofdisfigurement. The nurse evaluates the patient’s and family’s cop-ing methods to support them effectively both preoperatively andpostoperatively.
DiagnosisNURSING DIAGNOSESBased on all the assessment data, major nursing diagnoses mayinclude the following:
• Deficient knowledge about the surgical procedure and post-operative course
• Anxiety and depression related to the diagnosis of cancerand impending surgery
• Ineffective airway clearance related to excess mucus pro-duction secondary to surgical alterations in the airway
• Impaired verbal communication related to anatomic deficitsecondary to removal of the larynx and to edema
• Imbalanced nutrition: less than body requirements, related toinability to ingest food secondary to swallowing difficulties
• Disturbed body image and low self-esteem secondary tomajor neck surgery, change in the structure and function ofthe larynx
• Self-care deficit related to pain, weakness, fatigue, muscu-loskeletal impairment related to surgical procedure and post-operative course
COLLABORATIVE PROBLEMS/POTENTIAL COMPLICATIONSBased on assessment data, potential complications that may de-velop include:
• Respiratory distress (hypoxia, airway obstruction, trachealedema)
• Hemorrhage• Infection• Wound breakdown
Planning and GoalsThe major goals for the patient may include attainment of an ad-equate level of knowledge, reduction in anxiety, maintenance ofa patent airway (patient is able to handle own secretions), effec-
510 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
Voice prosthesis
Tracheostomavalve
FIGURE 22-6 Schematic representation of tracheoesophageal puncturespeech (TEP). Air travels from the lung through a puncture in the posteriorwall of the trachea into the esophagus and out the mouth. A voice prosthe-sis is fitted over the puncture site.

tive use of alternative means of communication, attainment ofoptimal levels of nutrition and hydration, improvement in bodyimage and self-esteem, improved self-care management, and ab-sence of complications.
Nursing InterventionsTEACHING THE PATIENT PREOPERATIVELYThe diagnosis of laryngeal cancer is associated with misconcep-tions and fears. Many people assume that loss of speech and dis-figurement are inevitable with this condition. Once the physicianexplains the diagnosis to the patient, the nurse clarifies any mis-conceptions by identifying the location of the larynx, its function,the nature of the surgical procedure, and its effect on speech. In-formational materials (written and audiovisual) about the surgeryare given to the patient and family for review and reinforcement.
If a complete laryngectomy is planned, the patient shouldknow that the natural voice will be lost, but that special trainingcan provide a means for communicating. However, the ability tosing, laugh, or whistle will be lost. Until this training is initiated,the patient needs to know that communication will be possibleby using the call light or special communication board and bywriting. The nurse answers questions about the nature of thesurgery and reinforces the physician’s explanation that the patientwill lose the ability to vocalize, but that a rehabilitation programis available. The multidisciplinary team conducts an initial as-sessment of the patient and family. The team might include thenurse, physician, respiratory therapist, speech therapist, clinicalnurse specialist, social worker, dietitian, and home care nurse.
Next, the nurse reviews equipment and treatments for post-operative care with the patient and family, teaches importantcoughing and deep-breathing exercises, and assists the patient toperform a return demonstration. The nurse clarifies the patient’srole in the postoperative and rehabilitation periods.
REDUCING ANXIETY AND DEPRESSIONBecause surgery of the larynx is performed most commonly for amalignant tumor, the patient may have many questions: Will thesurgeon be able to remove all of the tumor? Is it cancer? Will Idie? Will I choke? Will I suffocate? Will I ever speak again? Whatwill I look like? The psychological preparation of the patient is asimportant as the physical preparation.
Any patient undergoing surgery may have many fears. In la-ryngeal surgery, these fears may relate to the diagnosis of cancerand may be compounded by the possibility of permanent loss ofthe voice and disfigurement. The nurse provides the patient andfamily with opportunities to ask questions, verbalize feelings,and discuss perceptions. It is important to address any questionsand misconceptions the patient and family have. During the pre-operative or postoperative period, a visit from someone who hashad a laryngectomy may reassure the patient that people are avail-able to help and that rehabilitation is possible.
MAINTAINING A PATENT AIRWAYThe nurse promotes a patent airway by positioning the patientin the semi-Fowler’s or Fowler’s position after recovery from anes-thesia. Observing the patient for restlessness, labored breathing,apprehension, and increased pulse rate helps the nurse identifypossible respiratory or circulatory problems. Medications that de-press respiration, particularly opioids, should be used cautiously.As with other surgical patients, the nurse encourages the laryn-gectomy patient to turn, cough, and take deep breaths. If neces-sary, suctioning may be performed to remove secretions. The
nurse also encourages and assists the patient with early ambula-tion to prevent atelectasis and pneumonia.
If a total laryngectomy was performed, a laryngectomy tubewill most likely be in place. (In some instances a laryngectomytube is not used; in others it is used temporarily, and in many itis used permanently.) The laryngectomy tube, which is shorterthan a tracheostomy tube but has a larger diameter, is the pa-tient’s only airway. The care of this tube is the same as for a tra-cheostomy tube (see Chap. 25). The nurse cleans the stoma dailywith saline solution or another prescribed solution. If a non–oil-based antibiotic ointment is prescribed, the nurse applies itaround the stoma and suture line. If crusting appears around thestoma, the nurse removes the crusts with sterile tweezers and ap-plies additional ointment.
Wound drains may be in place to assist in removal of fluid andair from the surgical site. Suction also may be used, but cautiously,to avoid trauma to the surgical site and incision. The nurse ob-serves, measures, and records drainage. When drainage is less than50 to 60 mL/day, the physician usually removes the drains.
Frequently, the patient coughs up large amounts of mucusthrough this opening. Because air passes directly into the tracheawithout being warmed and moistened by the upper respiratorymucosa, the tracheobronchial tree compensates by secreting ex-cessive amounts of mucus. Therefore, the patient will have fre-quent coughing episodes and may develop a brassy-sounding,mucus-producing cough. The nurse should reassure the patientthat these problems will diminish in time as the tracheobronchialmucosa adapts to the altered physiology.
After the patient coughs, the tracheostomy opening must bewiped clean and clear of mucus. A simple gauze dressing, wash-cloth, or even paper towel (because of its size and absorbency)worn below the tracheostomy may serve as a barrier to protectthe clothing from the copious mucus that the patient may expelinitially.
One of the most important factors in decreasing cough, mucusproduction, and crusting around the stoma is adequate humidi-fication of the environment. Mechanical humidifiers and aerosolgenerators (nebulizers) increase the humidity and are importantfor the patient’s comfort.
The laryngectomy tube may be removed when the stoma iswell healed, within 3 to 6 weeks after surgery. The nurse can teachthe patient how to clean and change the tube (see Chap. 25) andremove secretions.
PROMOTING ALTERNATIVE COMMUNICATION METHODSUnderstanding the patient’s postoperative needs is critical. Alter-native means of communication are established and used consis-tently by all personnel who come in contact with the patient—forexample, a call bell or hand bell may be placed within easy reachof the patient. Because a Magic Slate often is used for communi-cation, the nurse should document which hand the patient usesfor writing so that the opposite arm can be used for intravenousinfusions. (The nurse should discard any old notes used for com-munication to ensure the patient’s privacy.) If the patient cannotwrite, a picture-word-phrase board or hand signals can be used.Preoperatively, the nurse reviews the system of communicationto be used postoperatively with the patient.
Because it is very time-consuming to have to write everythingor communicate through gestures, the inability to speak can bevery frustrating. The patient may become impatient and angrywhen not understood. In such cases, other staff members need tobe alert to the problem and also recognize that the patient will beunable to use the intercom system.
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 511

The return of communication is generally the ultimate goal inthe rehabilitation of the laryngectomy patient. The nurse workswith the patient, speech therapist, and family to encourage use ofalternative communication methods.
PROMOTING ADEQUATE NUTRITIONPostoperatively, the patient may not be permitted to eat or drinkfor 10 to 14 days. Alternative sources of nutrition and hydrationinclude intravenous fluids, enteral feedings through a nasogastrictube, and parenteral nutrition.
Once the patient is ready to start oral feedings, the nurse ex-plains that thick liquids will be used first because they are easy toswallow. The nurse instructs the patient to avoid sweet foods,which increase salivation and suppress the appetite. Solid foodsare introduced as tolerated. The nurse instructs the patient torinse the mouth with warm water or mouthwash and to brush theteeth frequently.
The patient can expect to have a diminished sense of taste andsmell for a period of time after surgery. Inhaled air passes directlyinto the trachea, bypassing the nose and the olfactory end organs.Because taste and smell are so closely connected, taste sensationsare altered. In time, however, the patient usually accommodatesto this problem and olfactory sensation adapts, often with returnof interest in eating. The nurse observes the patient for any diffi-culty swallowing, particularly when eating resumes, and reportsits occurrence to the physician.
PROMOTING POSITIVE BODY IMAGE AND SELF-ESTEEMDisfiguring surgery and an altered communication pattern are athreat to a patient’s body image and self-esteem. The reaction offamily members and friends is a major concern for the patient.The nurse encourages the patient to express any feelings about thechanges brought about by surgery, particularly those related tofear, anger, depression, and isolation.
A positive approach is important when caring for the patient.Promoting self-care activities is part of this approach. It is im-portant for the patient and family to begin participating in self-care activities as soon as possible. The nurse needs to be a goodlistener and a support to the family, especially when explainingthe tubes, dressings, and drains that are in place postoperatively.Referral to a support group, such as Lost Chord or New Voiceclubs (through the International Association of Laryngectomees)and I Can Cope (through the American Cancer Society), may helpthe patient and family deal with the changes in their lives. Groupssuch as Lost Chord and New Voice promote and support the re-habilitation of people who have had a laryngectomy by providingan opportunity for exchanging ideas and sharing information.
MONITORING AND MANAGING POTENTIAL COMPLICATIONSThe immediate potential complications after laryngectomy in-clude respiratory distress and hypoxia, hemorrhage, infection,and wound breakdown.
Respiratory Distress and HypoxiaThe nurse monitors the patient for signs and symptoms of respi-ratory distress and hypoxia, particularly restlessness, irritation,agitation, confusion, tachypnea, use of accessory muscles, and de-creased oxygen saturation on pulse oximetry (SpO2). Any changein the respiratory status requires immediate intervention. Ob-struction needs to be ruled out immediately by suctioning andhaving the patient cough and breathe deeply. Hypoxia and air-way obstruction, if not immediately treated, are life-threatening.
The nurse contacts the physician immediately if nursing measuresdo not improve the patient’s respiratory status.
HemorrhageBleeding at the surgical site from the drains or with tracheal suc-tioning may signal the occurrence of hemorrhage. The nurseshould notify the surgeon of any active bleeding immediately.Bleeding may occur at a variety of sites, including the surgical site,drains, or trachea. Rupture of the carotid artery is especially dan-gerous. Should this occur, the nurse should apply direct pressureover the artery, summon assistance, and provide emotional sup-port to the patient until the vessel can be ligated. It is importantto monitor vital signs for changes, particularly increased pulserate, decreased blood pressure, and rapid deep respirations. Cold,clammy, pale skin may indicate active bleeding.
InfectionThe nurse observes for postoperative infection. Early signs of in-fection include an increase in temperature and pulse, a change inthe type of wound drainage, or increased areas of redness or ten-derness at the surgical site. Other signs include purulent drainage,odor, and increased wound drainage. The nurse reports any sig-nificant change to the surgeon.
Wound BreakdownWound breakdown due to infection, poor wound healing, or de-velopment of a fistula or as a result of radiation therapy or tumorgrowth can create a life-threatening emergency. The carotidartery, which is close to the stoma, may rupture from erosion ifthe wound does not heal properly. The nurse observes the stomaarea for wound breakdown, hematoma, and bleeding and reportsany significant changes to the surgeon. If wound breakdown oc-curs, the patient must be monitored carefully and identified asbeing at high risk for carotid hemorrhage.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-CareThe nurse has an important role in the recovery and rehabilita-tion of the laryngectomy patient. In an effort to facilitate the pa-tient’s ability to manage self-care, discharge instruction begins assoon as the patient is able to participate. Nursing care and patientteaching in the hospital, outpatient setting, and rehabilitation orlong-term care facility must take into consideration the manyemotions, physical changes, and lifestyle changes experienced bythe patient. In preparing the patient to go home, the nurse as-sesses the patient’s readiness to learn and the level of knowledgeabout self-care management. The nurse also reassures the patientand family that most self-care management strategies can be mas-tered. The patient will need to learn a variety of self-care behav-iors, including tracheostomy and stoma care, wound care, andoral hygiene. In addition, the nurse instructs the patient aboutthe need for safe hygiene and recreational activities.
Tracheostomy and Stoma Care. The nurse provides specific in-structions to the patient and family about what to expect fromthe tracheostomy and its management. The nurse teaches the pa-tient and family caregiver to perform suctioning and emergencymeasures and tracheostomy and stoma care. The nurse stressesthe importance of humidification at home and instructs the fam-ily to set up a humidification system before the patient returnshome. In addition, the nurse cautions the patient and family thatair-conditioned air may be too cool or too dry, and thus too irri-tating, for the patient with a new laryngectomy. (See Chap. 25for details about tracheostomy care.)
512 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION

Hygiene and Safety Measures. The nurse instructs the patientand family about safety precautions needed because of the struc-tural changes resulting from the surgery. Special precautions areneeded in the shower to prevent water from entering the stoma.Wearing a loose-fitting plastic bib over the tracheostomy or sim-ply holding the hand over the opening is effective. Swimming isnot recommended, however, because people with a laryngectomycan drown without getting their face wet. Barbers and beauticiansneed to be alerted so that hair sprays, loose hair, and powder donot get near the stoma, because they can block or irritate the tra-chea and possibly cause infection. These self-care points are sum-marized in Chart 22-8.
Recreation and exercise are important, and all but very strenu-ous exercise can be enjoyed safely. Avoidance of strenuous exerciseand fatigue is important because, when tired, the patient has moredifficulty speaking, which can be discouraging. Additional safetypoints to address include the need for the patient to wear or carrymedical identification, such as a bracelet or card, to alert medicalpersonnel to the special requirements for resuscitation should thisneed arise. When resuscitation is needed, direct mouth-to-stomaventilation should be performed. For home emergency situations,prerecorded emergency messages for police, the fire department, orother rescue services can be kept near the phone to be used quickly.
The nurse instructs and encourages the patient to perform oralcare on a regular basis to prevent halitosis and infection. If the pa-tient is receiving radiation therapy, there will be a decrease insaliva, and synthetic saliva may be required. The nurse instructsthe patient to drink water or sugar-free liquids throughout theday and to use a humidifier at home. Brushing the teeth or den-tures and rinsing the mouth several times a day will assist in main-taining proper oral hygiene.
Continuing CareReferral for home care is an important aspect of postoperativecare for the patient who has had a laryngectomy and will assist thepatient and family in the transition to the home. The home carenurse assesses the patient’s general health status and the ability ofthe patient and family to care for the stoma and tracheostomy.
The nurse assesses the surgical incisions, nutritional and respira-tory status, and adequacy of pain management. The nurse assessesnot only for signs and symptoms of complications but also for thepatient’s and family’s knowledge of which signs and symptomsto report to the physician. During the home visit, the nurse iden-tifies and addresses other learning needs of the patient and family,such as adaptation to physical, lifestyle, and functional changes.It is important to assess the patient’s psychological status as well.The home care nurse reinforces previous teaching and providesreassurance and support to the patient and family as needed.
The nurse encourages the person who has had a laryngectomyto have regular physical examinations and to seek advice con-cerning any problems related to recovery and rehabilitation. Thepatient is also reminded to participate in health promotion activ-ities and health screening and about the importance of keepingscheduled appointments with the physician, speech therapist, andother health care providers.
EvaluationEXPECTED PATIENT OUTCOMESExpected patient outcomes may include:
1. Acquires an adequate level of knowledge, verbalizing anunderstanding of the surgical procedure and performingself-care adequately
2. Demonstrates less anxiety and depressiona. Expresses a sense of hopeb. Is aware of available community organizations and agen-
cies such as the Lost Chord or New Voice groupsc. Participates in support group, such as I Can Cope
3. Maintains a clear airway and handles own secretions; alsodemonstrates practical, safe, and correct technique for clean-ing and changing the laryngectomy tube
4. Acquires effective communication techniquesa. Uses assistive devices and strategies for communication
(Magic Slate, call bell, picture board, sign language, lipreading, computer aids)
b. Follows the recommendations of the speech therapist
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 513
Chart 22-8Home Care Checklist • The Patient With a Laryngectomy
At the completion of the home care instruction, the patient or caregiver will be able to:
• Demonstrate methods to clear the airway and handle secretions ✓ ✓
• Explain the rationale for maintaining adequate humidification with a humidifier or nebulizer ✓ ✓
• Demonstrate how to clean the skin around the stoma and how to use ointments and tweezers to remove encrustations ✓ ✓
• State the rationale for wearing a loose-fitting protective cloth at the stoma ✓ ✓
• Discuss the need to avoid cold air from air conditioning and the environment to prevent irritation of the airway ✓ ✓
• Demonstrate safe technique in changing the laryngectomy tube ✓ ✓
• Identify the signs and symptoms of wound infection and state what to do about them ✓ ✓
• Describe safety or emergency measures to implement in case of breathing difficulty or bleeding ✓ ✓
• State the rationale for wearing or carrying special medical identification and ways to obtain help in an emergency ✓ ✓
• Explain the importance of covering the stoma when showering or bathing ✓ ✓
• Identify fluid and caloric needs ✓ ✓
• Describe mouth care and discuss its importance ✓ ✓
• Demonstrate alternative communication methods ✓ ✓
• Identify support groups and agency resources ✓ ✓
• State the need for regular check-ups and reporting of any problems immediately ✓ ✓
Patient Caregiver

5. Maintains balanced nutrition and adequate fluid intake6. Exhibits improved body image, self-esteem, and self-concept
a. Expresses feelings and concernsb. Participates in self-care and decision makingc. Accepts information about support group
7. Exhibits no complicationsa. Vital signs (blood pressure, temperature, pulse, respira-
tory rate) normalb. No redness, tenderness, or purulent drainage at surgical
sitec. Demonstrates a patent airway and appropriate respira-
tionsd. No bleeding from surgical site and minimal bleeding
from drainse. No wound breakdown
8. Adheres to rehabilitation and home care programa. Practices recommended speech therapyb. Demonstrates proper methods for caring for stoma and
laryngectomy tube (if present)c. Verbalizes understanding of symptoms that require
medical attentiond. States safety measures to take in emergenciese. Performs oral hygiene as prescribed
REFERENCES AND SELECTED READINGS
BooksAmerican Cancer Society. (2002). Cancer facts and figures. Atlanta:
American Cancer Society Inc.Bast, R. C., Kufe, D. W., Pollock, R. E., et al. (Eds.) (2000). Holland &
Frei cancer medicine (5th ed.) Hamilton: B.C. Decker, Inc.DeLisa, J. A., & Gans, B. M. (1998). Rehabilitation medicine principles
and practice (3d ed.). Philadelphia: Lippincott-Raven.Goldman, L., & Bennett, J. C. (Eds.) (2000). Cecil textbook of medicine
(21st ed.). Philadelphia: W. B. Saunders.Green, E., et al. (Eds.) (2002). AJCC cancer staging manual (6th ed.).
New York: Springer-Verlag.Haskell, C. M. (2001) Cancer treatment (5th ed.). Philadelphia:
W. B. Saunders.Lenhard, R. E., Osteen, R. T., & Gansler, T. (2001) The American Can-
cer Society’s clinical oncology (1st ed.). Atlanta: American Cancer So-ciety Inc.
Mandell, G. L., Bennett, J. E., & Dolin, R (Eds.) (2000). Principlesand practice of infectious diseases (5th ed.). Philadelphia: ChurchillLivingstone.
McKenry, L. M., & Salerno, E. (2001). Mosby’s principles in nursing(21st ed.). St. Louis: Mosby.
Middleton, E., Ellis, E. F., Yunginger, J. W., et al. (1998). Allergy: prin-ciples and practice (Vol. II, 5th ed.). St. Louis: Mosby.
Murray, J. F., & Nadel, J. A. (2001). Textbook of respiratory medicine(Vols. 1 & 2, 3d ed.). Philadelphia: W. B. Saunders.
Peckenpaugh, N. J., & Poleman, C. M. (1999). Nutrition essentials anddiet therapy (8th ed.). Philadelphia: W. B. Saunders.
Tierney, L. M., McPhee, S. J., & Papadakis, M. A. (2001). Currentmedical diagnosis and treatment 2001 (40th ed.). New York: LangeMedical Books/McGraw Hill.
Tintinalli, J. E., Kelen, G. D., & Stapczynski, J. S. (2000). Emergencymedicine: A comprehensive study guide (5th ed.). New York: McGraw-Hill.
Townsend, C. M. (Ed.) (2001). Sabiston textbook of surgery (16th ed.).Philadelphia: W. B. Saunders.
Yarbro, C. H., Goodman, M., Frogge, M. H., & Groenwald, S. L. I.(Eds.) (2000). Cancer nursing: Principles and practice (5th ed.).Boston: Jones & Bartlett.
JournalsAsterisks indicate nursing research articles.GeneralCasale, T. B., Condemi, J., LaForce, C., et al. (2001). Effect of omal-
izumab on symptoms of seasonal allergic rhinitis: A randomized con-trolled trial. Journal of the American Medical Association, 286(23),2956–2967.
Chan, E., & Welsh, C. H. (1998). Geriatric respiratory medicine. Chest,114(6), 1704–1733.
Upper Respiratory InfectionsBisno, A. L. (2001) Primary care: Acute pharyngitis. New England Jour-
nal of Medicine, 344(3), 205–211.Cifu, A., & Levinson, W. (2000) Influenza. Journal of the American
Medical Association, 284(22), 2847–2849.Cooper, R. J., Hoffman, J. R., Bartlett, J. G., et al. (June 2001). Centers
for Disease Control and Prevention. Principles of appropriate an-tibiotic use for acute pharyngitis in adults: background. Annals ofEmergency Medicine. 37(6), 711–719.
Corneli, H. (2001). Rapid strep tests in the emergency department: Anevidence-based approach. Pediatric Emergency Care, 17(4), 272–278.
Ebell, M. H., Smith, M. A., Barry, H. C., Ives, K., & Carey, M. (2000).Does this patient have strep throat? Journal of the American MedicalAssociation, 284(22), 2912–2918.
Hall, C. B. (2001). Respiratory syncytial virus and parainfluenza virus.New England Journal of Medicine, 344(25), 1917–1928.
Hickner, J. M. (2001). Acute rhinosinusitis: A diagnostic and therapeu-tic challenge. Journal of Family Practice, 50(1), 38–40.
Hickner, J. M., Bartlett, J. G., Besser, R. E., et al. (2001). AmericanAcademy of Family Physicians/American Society of Internal Medi-
514 Unit 5 GAS EXCHANGE AND RESPIRATORY FUNCTION
1. A 36-year-old teacher is diagnosed with acute sinusitis.She has been self-medicating with over-the-counter medica-tions for the past 2 weeks with no relief. What assessmentand treatment should the nurse anticipate? What teachingand management strategies would you discuss with thepatient? What is the rationale for your approach?
2. Your 68-year-old patient is scheduled for total laryngec-tomy for treatment of laryngeal cancer. What informationwould you provide to the patient about managing changes in breathing and speech that are expected in the immediatepostoperative period and in the long term? What informa-tion would you provide to the patient’s family?
3. You are making the first home visit to a patient who has just been discharged from the hospital following treat-ment for pneumonia and a 60-lb weight loss. He had alaryngectomy 8 months ago to treat laryngeal cancer. Whatwill be the focus of your initial home visit? What aspects ofassessment and nursing management are key at this point in caring for this patient? How would you assist this patientand his family to plan his care for the next month? Next 6 months?
4. Your patient, age 36, has been admitted to the emergencydepartment with profuse epistaxis following a car crash. Hetells you that he has hemophilia and is HIV-positive as a re-sult of repeated use of clotting factors. What are the initialmeasures you would use to stop the bleeding? What other op-tions are available if the bleeding does not stop within a rea-sonable period? How will his HIV status and the diagnosis ofhemophilia affect your plan of care for him?
Critical Thinking Exercises??

cine. Centers for Disease Control Infectious Diseases Society ofAmerica. Principles of appropriate antibiotic use for acute rhinosi-nusitis in adults: background. Annals of Internal Medicine, 134(6),498–505.
Kearney, K. (2001). Emergency: Epiglottis. American Journal of Nurs-ing, 101(8), 37–38.
Kernan, W. N., Viscoli, C. M., Brass, L. M., et al. (2000). Phenyl-propanolamine and the risk of hemorrhagic stroke. New EnglandJournal of Medicine, 343(25), 1826–1832.
Luna, B., Drew, R. H., & Perfect, J. R. (2000). Agents for the treatmentof invasive fungal infections. Otolaryngologic Clinics of North Amer-ica, 33(4), 277–299.
Mattila, P. (2001). Causes of tonsillar disease and frequency of tonsil-lectomy operations. Archives of Otolaryngology- Head & Neck Surgery,127(1), 37–44.
Piccirillo, J. F., Mager, D. E., Frisse, M. E., Brophy, R. H. & Goggin,A. (2001). Impact of first-line vs. second-line antibiotics for thetreatment of acute uncomplicated sinusitis. Journal of the AmericanMedical Association, 286(15), 1849–1856.
Prasad, A. S., Fitzgerald, J. T., Bao, B., et al. (2000). Duration of symp-toms and plasma cytokine levels in patients with the common coldtreated with zinc acetate: A randomized, double-blind, placebo-controlled trial. Annals of Internal Medicine, 133(4), 245–252.
Sly, M. (1999). Changing prevalence of allergic rhinitis and asthma.Annals of Allergy, Asthma, & Immunology, 82(3), 233–252.
Snow, V., Mottur-Pilson, C., Hickner, J. M., et al. (2001). Principlesof appropriate antibiotic use for acute sinusitis in adults. Annals ofInternal Medicine, 134(6), 495–497.
Stephenson, K. (2000). Acute and chronic pharyngitis across the lifespan.Lippincott’s Primary Care Practice. Ear, Nose, and Throat Problems,4(5), 471–489.
Stone, S., Gonzales, R., Maselli, J., & Lowenstein, S. R. (2000). Antibi-otic prescribing for patients with colds, upper respiratory tract infec-tions, and bronchitis: A national study of hospital-based emergencydepartments. Annals of Emergency Medicine. 36(4), 320–327.
Youngs, R. (2000) Sinusitis in adults. Current Opinion in PulmonaryMedicine, 6(3), 217–220.
Obstruction and Trauma of the AirwayBoehlecke, B. A. (2000). Epidemiology and pathogenesis of sleep-
disordered breathing. Current Opinion in Pulmonary Medicine,6(6), 471–478.
Flemons, W. W. (2002). Clinical practice. Obstructive sleep apnea.New England Journal of Medicine, 347(7), 498–504.
Goldberg, R. (2000). Treatment of obstructive sleep apnea, other thanwith continuous positive airway pressure. Current Opinion in Pul-monary Medicine, 6(6), 496–500.
Harding, S. M. (2000). Complications and consequences of obstruc-tive sleep apnea. Current Opinion in Pulmonary Medicine, 6(6),485–489.
Krieger, A. C. & Redeker, N. S. (2002) Obstructive sleep apnea syn-drome: its relationship with hypertension. Journal of CardiovascularNursing, 17(1), 1–11.
Krishna, P., & Lee, D. (2001). Post-tonsillectomy bleeding: A meta-analysis. Laryngoscope, 111(8), 1358–1361.
Liu, J., Anderson, K. E., Willging, J. P., et al. (2001). Post-tonsillectomyhemorrhage: What is it and what should be recorded? Archives of Oto-laryngology—Head & Neck Surgery, 127(10), 1271–1275.
Marchiondo, K. (2000). Pickwickian syndrome: The challenge of severesleep apnea. MedSurg Nursing, 9(4), 183–188.
Narkiewicz, K., Kato, M., Phillips, B. G., et al. (1999). Nocturnal con-tinuous positive airway pressure decreases daytime sympathetic traf-fic in obstructive sleep apnea. Circulation, 100(23), 2332–2335.
National Institutions of Health. (2000). NHLBI study shows associa-tion between sleep apnea and hypertension (Press release, 4-11-00).http://www.nhlbi.nih.gov/about/ncsdr.
Nieto, F. J., Young, T. B., Lind, B. K., et al. (2000). Association ofsleep-disordered breathing, sleep apnea, and hypertension in a large
community-based study. Sleep Heart Health Study. Journal of theAmerican Medical Association, 283(14), 1829–1836.
Parker, K. P. & Dunbar, S. B. (2002). Sleep and heart failure. Journalof Cardiovascular Nursing, 17(1), 12–29.
Peppard, P. E., Young, T., Palta, M., et al. (2000). Longitudinal studyof moderate weight change and sleep-disordered breathing. Journalof the American Medical Association, 284(23), 3015–3021.
Redeker, N. S. (2002). Why is sleep relevant to cardiovascular disease?Journal of Cardiovascular Nursing, 17(1), v–ix.
Cancer of the LarynxBauer, A. M. (2001). Current trends in surgical management of head and
neck carcinomas. Nursing Clinics of North America, 36(3), 501–506.*Dropkin, M. J. (2001). Anxiety, coping strategies and coping behaviors
in patients undergoing head and neck cancer surgery. Cancer Nurs-ing, 24(2), 143–148.
Finizia, C., & Bergman, B. (2001). Health-related quality of life in pa-tients with laryngeal cancer: A post-treatment comparison of differ-ent modes of communication. Laryngoscope, 111(5), 918–923.
Forastiere, A., Koch, W., Trotti, A., & Sidransky, D. (2001). Head andneck cancer. New England Journal of Medicine, 345(26), 1890–1900.
Friedman, M., Landsberg, R., Pryor, S., et al. (2001). The occurrence ofsleep-disordered breathing among patients with head and neck can-cer. Laryngoscope, 111(11), 1917–1919.
*Hemsley, B. (2001). Nursing the patient with severe communicationimpairment. Journal of Advanced Nursing, 35(6), 827–835.
Koch, W. (2001). A fail-safe technique for endoscopic tracheoesophagealpuncture. Laryngoscope, 111(9), 1663–1665.
*Major, M. S., Bumpous, J. M., Flynn, M. B., & Schill, K. (2001).Quality of life after treatment for advanced laryngeal and hypopha-ryngeal cancer. Laryngoscope, 111(8), 1379–1382.
Owen, C., et al. (2001). The psychosocial impact of head and neck can-cer. Clinical Otolaryngology & Allied Sciences, 26(5), 351–356.
Rose, P., & Yates, P. (2001). Quality of life experienced by patients re-ceiving radiation treatment for cancers of the head and neck. CancerNursing, 24(4), 255–263.
Serra, A. (2000). Tracheostomy care. Nursing Standard, 14(42), 45–55.Tamura, E. (2001). Clinical assessment of intralaryngeal ultrasonography.
Laryngoscope, 111(10), 767–770. Weinstein, G. S., El-Sawy, M. M., Ruiz, C., et al. (2001). Laryngeal
preservation with supracricoid partial laryngectomy results in im-proved quality of life when compared with total laryngectomy. Laryn-goscope, 111(12), 191–199.
RESOURCES AND WEBSITES
American Cancer Society, 1599 Clifton Rd., NE, Atlanta, GA 30329-4251; (404) 320-3333; (800) ACS-2345; http://www.cancer.org.
American Lung Association, 1740 Broadway, New York, NY 10019-4374; (212) 315-8700; http://www.lungusa.org.
American Sleep Apnea Association, 1424 K Street, NW, Suite 302,Washington, DC 20005; 202-293-3650; http://www.sleepapnea.org.
International Association of Laryngectomees, 7400 N. Shadeland Ave.,Suite 100, Indianapolis, IN 46250; (317) 570-4568; http://www.larynxlink.com.
National Cancer Institute (NCI), Bldg. 31, 31 Center Drive, MSC2580, Bethesda, MD 20892-2580; http://cancernet.nci.nih.gov.
National Institute of Allergy and Infectious Disease, Building 31, 31Center Drive MSC 2520, Bethesda, MD 20892-2520; http://www.niaid.nih.gov.
National Heart, Lung, and Blood Institute (NHBLI), National Insti-tutes of Health, Bldg. 31, Rm. 4A21, Bethesda, MD 20892; 301-592-8573 800-575-9355; http://www.nhlbi.nih.gov.
National Sleep Foundation, 1522 K Street NW, Suite 500, Washington,DC 20005; 202-437-3471; Fax: 202-347-3472; http://www.sleepfoundation.org.
Voice Center at Eastern Virginia Medical School, Norfolk, VA 23507;http://www.voice-center.com.
Chapter 22 Management of Patients With Upper Respiratory Tract Disorders 515