Embed Size (px)
Citation preview
Örebro University School of Medicine Degree project, 15 ECTS May 2016
Septoplasty for nasal obstruction in Region Örebro County – A retrospective study
evaluating postoperative complications and quality of life
version 2
Author: Sarmed Finjan Supervisor: Åke Davidsson MD. Ph.D.
2
Table of contents
Abstract 3
Introduction and background 3
Nasal obstruction 3
Septal deviation 4
Septoplasty 4
Objective 5
Methods 5
Ethics 7
Statistics 7
Results 7
Discussion 10
Conclusions 12
References 13
Appendix 17
A 17
B 18
C 20
D 22
3
Abstract
Background
The nasal septum is a key element in the nasal construct. By separating the two nasal cavities it
contributes to ensuring optimal airflow in and out of the nose. The nasal septum can become
deviated from trauma, congenital abnormalities and iatrogenic or other causes. The deviation
constricts airflow and leads to nasal obstruction. It is possible to correct this deviation with nasal
septoplasty, one of the most commonly performed procedures involving the nose.
Objective
We wanted to evaluate the quality of septoplasty in Region Örebro County by studying
postoperative complications and quality of life in patients that underwent septoplasty.
Methods
In this retrospective study 140 patients who underwent septoplasty in Region Örebro County were
evaluated for postoperative complications (bleeding, infection, hematoma, synechiae or septal
perforation). 85 of those patients were also evaluated regarding quality of life. Data was gathered
from patient journals and the Swedish National Quality Registry for Septoplasty.
Results
We found that postoperative complications as defined were seen in 12,8% of patients. We observed
a statistically significant improvement in self-assessed degree of nasal obstruction (p<0.01) and
self-assessed impact on daily activities and/or sleep (p<0.01). 61% of patients reported symptomatic
improvement after surgery, however only 21% answered they experienced no symptoms.
Conclusions
We concluded that the observed complication and improvement rates are in line with those
observed in other studies and that further long-term evaluation of our patients is required.
Introduction and background
Nasal obstruction
Nasal obstruction can stem from a deviated nasal septum, nasal polyposis and hypertrophy of the
turbinates or adenoid. Different forms of rhinitis, drugs or other etiologies can cause congestion
which in turn leads to nasal obstruction [1]. When assessing nasal obstruction, a need arises to
objectively quantify the subjective perception of nasal obstruction. Acoustic rhinometry and
rhinomanometry can be used for this purpose. Acoustic rhinometry utilizes reflecting sound waves
(sent into the nostrils) to confirm and locate the site of nasal obstruction [2]. Cross-sectional area
(CSA) values are obtained for different parts of the nasal cavity. Rhinomanometry utilizes
differences in airflow and pressure to calculate nasal airway resistance [3]. These methods can help
4
the physician ascertain the nature and grade of nasal obstruction. Here we choose to focus on the
deviated nasal septum as a cause of nasal obstruction.
Septal deviation
The nasal septum is the midline structure of the nose separating the nasal cavities. It is comprised of
quadrangular cartilage, the perpendicular plate of ethmoid bone, vomer and the crests of the nasal,
frontal, maxilla and palatine bones [4].
Several studies have made efforts to determine the prevalence of nasal septal deviation. In
newborns, studies have shown a prevalence as high as 22% [5]. Mladina et al., using a a strict
classification system, showed in a large international study that the prevalence in the adult
population is 89% [6].
Septal deviations have a wide range of etiologies, including but not limited to trauma, infections
and polyps [7].
The nasal septum can become deviated as early as during intrauterine life or birth [5]. Constant
compression of the nose or developmental abnormalities that occur in the uterus can cause a septal
deviation. During normal birth, the fetal head rotates within the birth canal. Depending on the
position of the fetus, it may acquire a septal deviation corresponding to the direction of the rotation.
This occurs because the cartilage becomes displaced during the rotation.
If sustained by an early age, even microfractures and the subsequent asymmetrical healing and
growth of the entire nose and face may lead to a deviated nasal septum later in life [8-10].
As previously mentioned, trauma is a common cause of nasal septal deviation. Assault, accidents
and sports are the most common etiologies of nasal bone fractures [11,12] and it has been observed
that over 90% of nasal bone fractures are associated with a corresponding septal fracture [13].
Septal fractures may in turn lead to hematoma, infection and subsequent septal abscesses and
necrosis [14]. Deformities in the septal cartilage and bone give rise to a septal deviation, which can
cause nasal obstruction [15].
Septoplasty
Septoplasty is one of the most commonly performed ENT (Ear, Nose and Throat) procedures.
Approximately 3000 septoplasties were performed in Sweden in 2014 [16].
The procedure is commonly performed under general anesthesia. Topical decongestant is applied to
the nose, followed by injections of local anesthetic.
5
There are three main approaches to septoplasty: endonasal, endoscopic and extracorporeal.
Endonasal septoplasty is the most commonly performed form of septoplasty. It is therefore
described. A hemitransfixion incision is made along the leading edge to reach the subperichondrial
plane. The mucoperichondrial flap is elevated and dissection is continued onto vomer and along the
inferior border of the quadrilateral cartilage. The quadrilateral cartilage is mobilized and the
deformity corrected or excised. Maxillary crest spurs are removed. The quadrilateral cartilage is
repositioned and fixed with bilateral sutures. The incision is closed with quilting sutures [17]. The
nose is then packed with a nasal packing material.
Endoscopic septoplasty utilizes endoscopic visualization. Improved visualization, minimal mucosal
elevation [18] and less postoperative complications [19] are advantages that the endoscopic
approach has over the endonasal. However, when the septal deviation is deflecting caudally or
associated with an external nasal deformity, the endonasal or extracorporeal approach is preferred.
Extracorporeal septoplasty is used for correcting the most substantial septal deviations. In the
procedure, the septum is extracted. It is then corrected and reinserted [20]. When the extent of the
septal deformity is too great, autologous cartilage grafts (costal or conchal for instance) can be used
to reconstruct the septum [21].
Objective The objective of this report was to study the quality of septoplasty in Region Örebro County.
Beyond two clinical visits after surgery, patients undergoing septoplasty are not followed up in any
regard by our clinics. Therefore, a need exists to determine if the surgery results are satisfactory.
This was accomplished by evaluating postoperative complications and quality of life in patients that
had undergone septoplasty. Firstly, we wanted to determine the rate of postoperative complications.
Secondly, we wanted to evaluate patient satisfaction and improvements in symptomatology after
surgery.
Methods
We performed a retrospective review of all patients who underwent septoplasty with the indication
nasal obstruction at Örebro University Hospital, Karlskoga Hospital and Lindesberg Hospital from
March 2013 to March 2015. 170 patients were identified.
6
Patient data regarding age, gender, preoperative rhinomanometric measurements, postoperative
complications and follow-up visit (defined as a visit to the clinic six months to one year after
surgery) were collected. Postoperative complications were defined as following
1. Bleeding. Patient has postoperatively been admitted for overnight admission or been in
contact with and examined by an ENT specialist for nasal bleeding. Trivial bleedings were
excluded.
2. Infection. Patient has postoperatively visited and been examined by an ENT specialist for
classical symptoms of infection (fever, swelling, etc) and was prescribed antibiotics.
3. Hematoma. Patient has postoperatively been examined by an ENT specialist and a
hematoma was discovered.
4. Synechiae. Patient has postoperatively been examined by an ENT specialist and synechiae
were discovered.
5. Septal perforation. Patient had septal perforation at follow-up visit.
One week postoperatively patients are examined with nasal endoscopy. Six months to one year
postoperatively patients are invited for a follow-up visit. No routine for postoperative
rhinomanometry exists at our clinics.
Patients who underwent surgery on other indications as acute trauma, tumor or cosmetic reasons
were excluded. Patients who had surgery performed on their sinuses, adenoid, tonsils, nasal polyps
or had rhinoplasty performed simultaneously were also excluded. 30 patients were excluded.
Anonymized data regarding patient-reported symptoms, quality on life, result and information of
surgery was collected from the Swedish National Quality Registry for Septoplasty. The data
collected concerned the same three hospitals, however, data for the year of 2013 was not available.
Patients fill out a questionnaire concerning the nature and grade of nasal obstruction. Patients grade
their nasal obstruction accordingly “None”, “Mild”, “Moderate” or “Severe”. Impact on daily
activities is ranked in the same manner. Smoking habits, length and weight preoperatively are also
assessed (Appendix A). The preoperative questionnaire is complemented with diagnostic
information by an ENT specialist. A perioperative questionnaire (Appendix B) is filled out by the
surgeon. One month postoperatively the patients receive a questionnaire by mail concerning
postoperative complications (Appendix C). One year postoperatively the patients receive a
questionnaire by mail with the same questions as the the preoperative questionnaire but with
additional questions regarding lasting complications and expectations of surgery (Appendix D). 89
patients were included in the questionnaire. 4 patients were excluded for not completing the
questionnaire correctly.
7
Ethics
Approvals to study patient journals were acquired from the operations managers at the ENT clinics
at the corresponding hospital of Örebro, Karlskoga and Lindesberg. No registries containing
individual patient data were created. Ethics approval was deemed unnecessary since this is a quality
project by a student.
Statistics
Conventional arithmetics were used for calculation of means, sums, percentages and standard
deviations. Wilcoxon signed-rank test was used for paired categorical variables. Spearman’s rank
correlation test was used for correlation. All tests were two-tailed and conducted at 5% significance.
IBM® SPSS® Statistics version 23 was used for statistical analysis and figures. Microsoft Excel ®
version 15.19.1 was used for tables.
Results
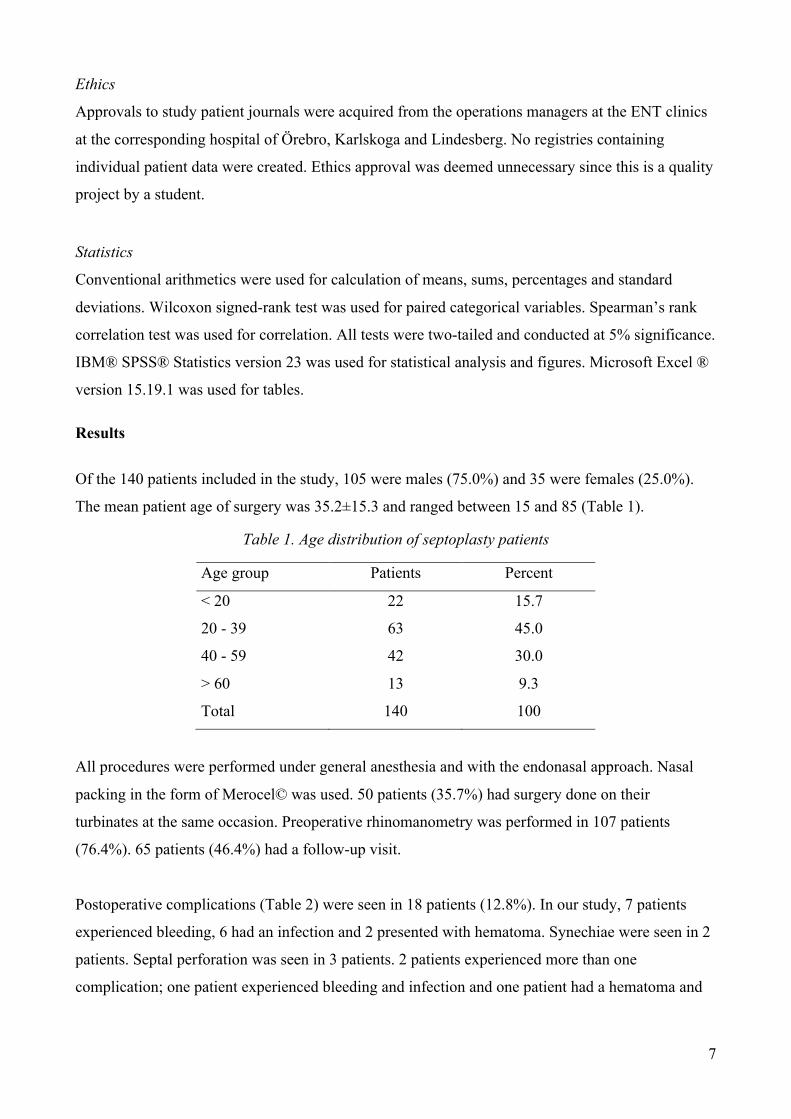
Of the 140 patients included in the study, 105 were males (75.0%) and 35 were females (25.0%).
The mean patient age of surgery was 35.2±15.3 and ranged between 15 and 85 (Table 1).
Table 1. Age distribution of septoplasty patients
Age group Patients Percent
< 20 22 15.7
20 - 39 63 45.0
40 - 59 42 30.0
> 60 13 9.3
Total 140 100
All procedures were performed under general anesthesia and with the endonasal approach. Nasal
packing in the form of Merocel© was used. 50 patients (35.7%) had surgery done on their
turbinates at the same occasion. Preoperative rhinomanometry was performed in 107 patients
(76.4%). 65 patients (46.4%) had a follow-up visit.
Postoperative complications (Table 2) were seen in 18 patients (12.8%). In our study, 7 patients
experienced bleeding, 6 had an infection and 2 presented with hematoma. Synechiae were seen in 2
patients. Septal perforation was seen in 3 patients. 2 patients experienced more than one
complication; one patient experienced bleeding and infection and one patient had a hematoma and
8
infection. No correlation was found between postoperative complications and sex, age or turbinate
surgery.
Table 2. Complications of septoplasty (n=20)
Complications Cases Percent of all septoplasties (n=140)
Bleeding 7 5.0
Hematoma 2 1.4
Infection 6 4.3
Synechiae 2 1.4
Septal perforation 3 2.1
Questionnaire data from 85 patients was analyzed. Response rate to the preoperative questionnaire
was 91.8%. Response rate to the one-month postoperative questionnaire was 44.7%. Response rate
to the one-year postoperative questionnaire was also 44.7%.
32 patients (84.2%) answered that they were adequately informed of the procedure. 8 patients
(21.1%) reported they had sought medical attention because of postoperative complications. 21
patients (55.3%) answered that the result of the surgery was what they had expected. We observed a
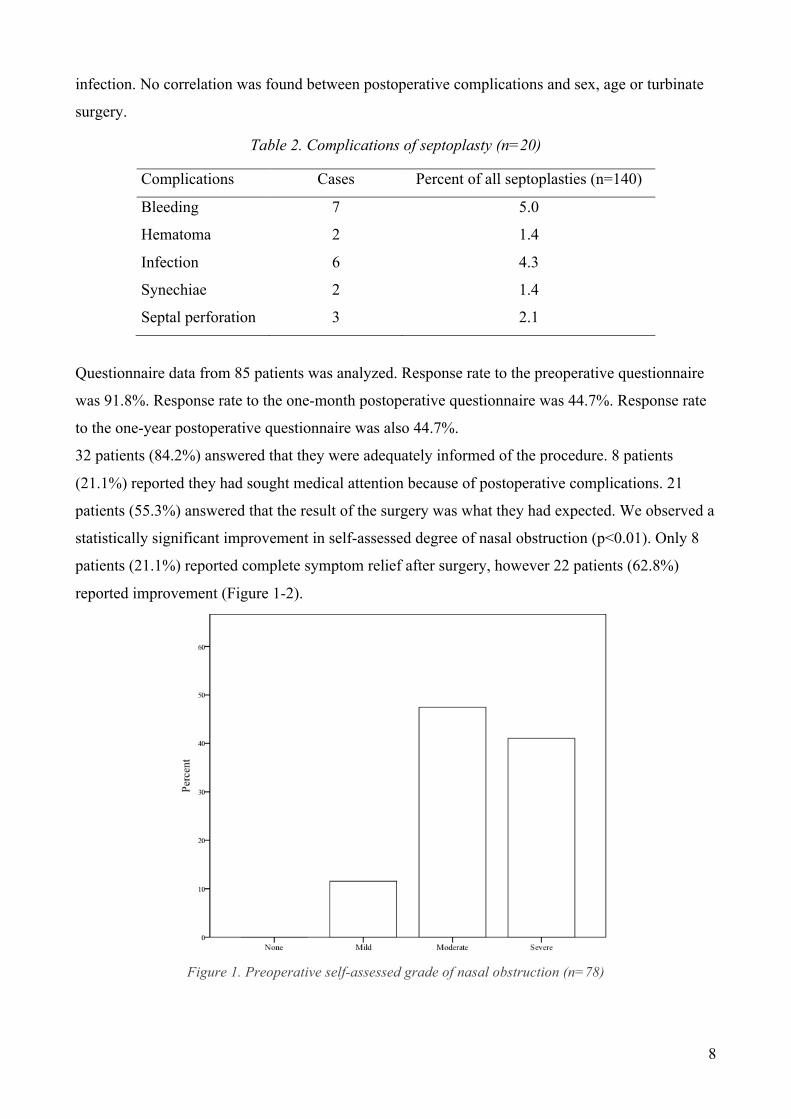
statistically significant improvement in self-assessed degree of nasal obstruction (p<0.01). Only 8
patients (21.1%) reported complete symptom relief after surgery, however 22 patients (62.8%)
reported improvement (Figure 1-2).
Figure 1. Preoperative self-assessed grade of nasal obstruction (n=78)
9
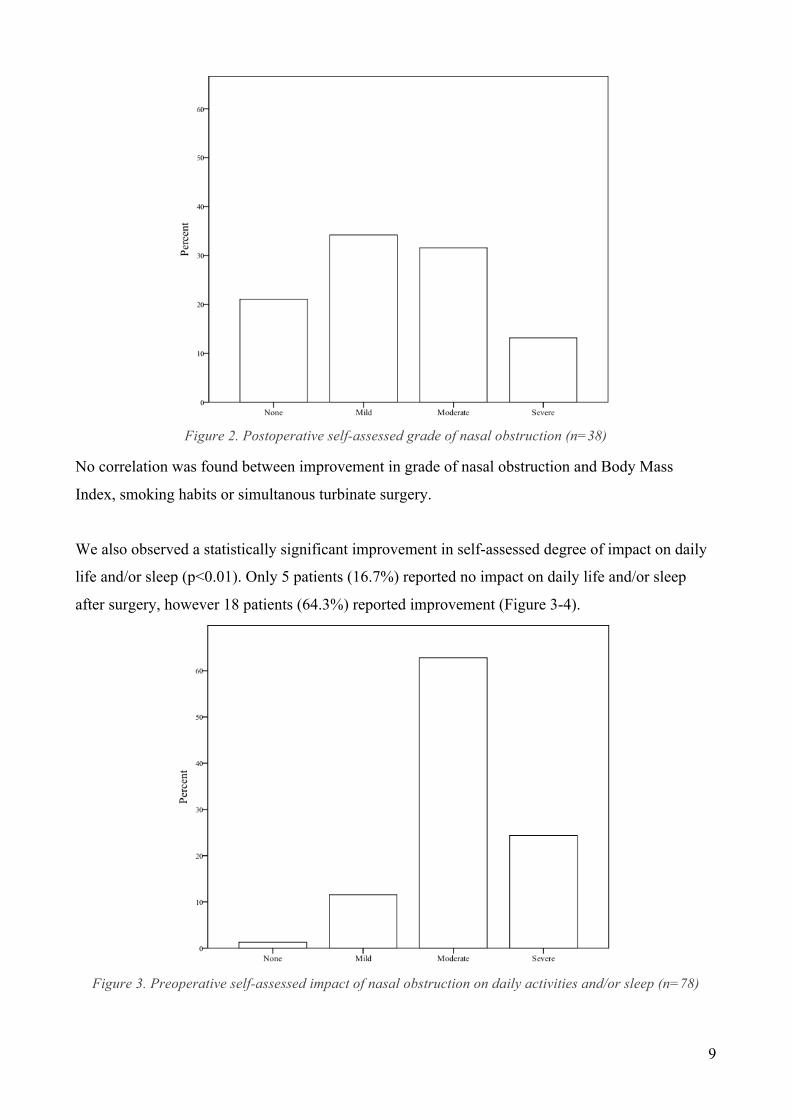
Figure 2. Postoperative self-assessed grade of nasal obstruction (n=38)
No correlation was found between improvement in grade of nasal obstruction and Body Mass
Index, smoking habits or simultanous turbinate surgery.
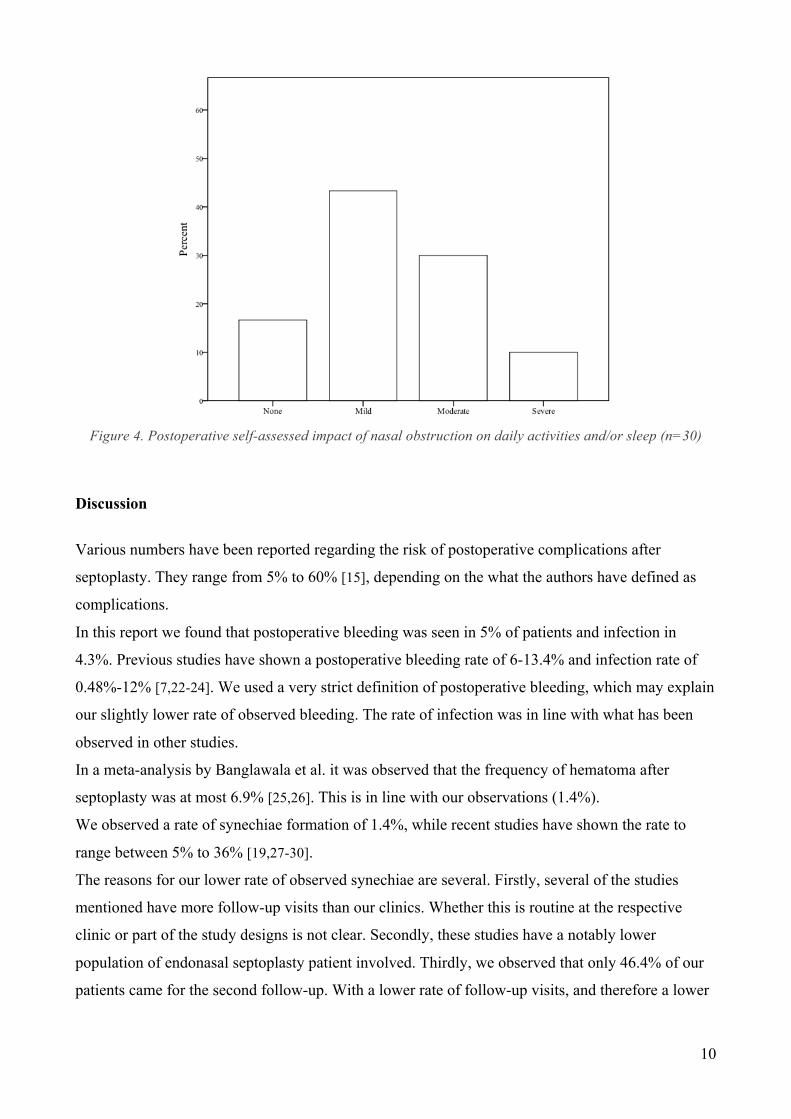
We also observed a statistically significant improvement in self-assessed degree of impact on daily
life and/or sleep (p<0.01). Only 5 patients (16.7%) reported no impact on daily life and/or sleep
after surgery, however 18 patients (64.3%) reported improvement (Figure 3-4).
Figure 3. Preoperative self-assessed impact of nasal obstruction on daily activities and/or sleep (n=78)
10
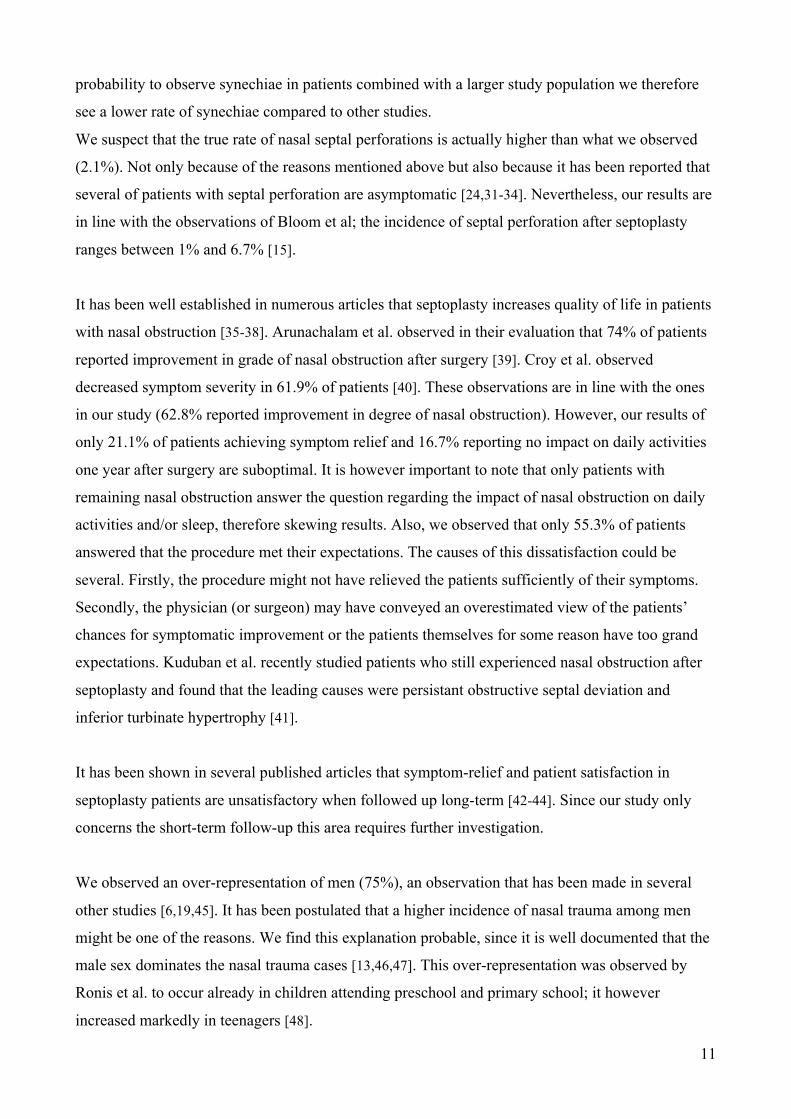
Figure 4. Postoperative self-assessed impact of nasal obstruction on daily activities and/or sleep (n=30)
Discussion
Various numbers have been reported regarding the risk of postoperative complications after
septoplasty. They range from 5% to 60% [15], depending on the what the authors have defined as
complications.
In this report we found that postoperative bleeding was seen in 5% of patients and infection in
4.3%. Previous studies have shown a postoperative bleeding rate of 6-13.4% and infection rate of
0.48%-12% [7,22-24]. We used a very strict definition of postoperative bleeding, which may explain
our slightly lower rate of observed bleeding. The rate of infection was in line with what has been
observed in other studies.
In a meta-analysis by Banglawala et al. it was observed that the frequency of hematoma after
septoplasty was at most 6.9% [25,26]. This is in line with our observations (1.4%).
We observed a rate of synechiae formation of 1.4%, while recent studies have shown the rate to
range between 5% to 36% [19,27-30].
The reasons for our lower rate of observed synechiae are several. Firstly, several of the studies
mentioned have more follow-up visits than our clinics. Whether this is routine at the respective
clinic or part of the study designs is not clear. Secondly, these studies have a notably lower
population of endonasal septoplasty patient involved. Thirdly, we observed that only 46.4% of our
patients came for the second follow-up. With a lower rate of follow-up visits, and therefore a lower
11
probability to observe synechiae in patients combined with a larger study population we therefore
see a lower rate of synechiae compared to other studies.
We suspect that the true rate of nasal septal perforations is actually higher than what we observed
(2.1%). Not only because of the reasons mentioned above but also because it has been reported that
several of patients with septal perforation are asymptomatic [24,31-34]. Nevertheless, our results are
in line with the observations of Bloom et al; the incidence of septal perforation after septoplasty
ranges between 1% and 6.7% [15].
It has been well established in numerous articles that septoplasty increases quality of life in patients
with nasal obstruction [35-38]. Arunachalam et al. observed in their evaluation that 74% of patients
reported improvement in grade of nasal obstruction after surgery [39]. Croy et al. observed
decreased symptom severity in 61.9% of patients [40]. These observations are in line with the ones
in our study (62.8% reported improvement in degree of nasal obstruction). However, our results of
only 21.1% of patients achieving symptom relief and 16.7% reporting no impact on daily activities
one year after surgery are suboptimal. It is however important to note that only patients with
remaining nasal obstruction answer the question regarding the impact of nasal obstruction on daily
activities and/or sleep, therefore skewing results. Also, we observed that only 55.3% of patients
answered that the procedure met their expectations. The causes of this dissatisfaction could be
several. Firstly, the procedure might not have relieved the patients sufficiently of their symptoms.
Secondly, the physician (or surgeon) may have conveyed an overestimated view of the patients’
chances for symptomatic improvement or the patients themselves for some reason have too grand
expectations. Kuduban et al. recently studied patients who still experienced nasal obstruction after
septoplasty and found that the leading causes were persistant obstructive septal deviation and
inferior turbinate hypertrophy [41].
It has been shown in several published articles that symptom-relief and patient satisfaction in
septoplasty patients are unsatisfactory when followed up long-term [42-44]. Since our study only
concerns the short-term follow-up this area requires further investigation.
We observed an over-representation of men (75%), an observation that has been made in several
other studies [6,19,45]. It has been postulated that a higher incidence of nasal trauma among men
might be one of the reasons. We find this explanation probable, since it is well documented that the
male sex dominates the nasal trauma cases [13,46,47]. This over-representation was observed by
Ronis et al. to occur already in children attending preschool and primary school; it however
increased markedly in teenagers [48].
12
Journal data created before the year of 2013 were stored in paper format making information as
previous history of nasal surgery difficult to obtain, and as such, were not included in the study.
Furthermore, data from the Swedish National Quality Registry for Septoplasty was also only
available from the end of the year of 2013.
Regarding patient-assessed quality of life and symptomatology, we experienced some difficulties in
comparing our results to those of our international colleagues. Since our questionnaires neither
utilize a scoring system nor go into great detail when assessing symptoms and quality of life, our
ability to draw conclusions is limited to comparing broad patterns.
Conclusions
This study has attempted to review the quality of septoplasty in Region Örebro County. We
conclude that our complication rates are in line with those observed in other articles. We also
conclude that our results regarding quality of life in patients are difficult to interpret because of low
response rate and difficulties in comparison. However, when comparing broad patterns such as
subjective improvement in symptoms, our results reflect those of previous studies.
13
References 1. Corey JP, Houser SM, Ng BA. Nasal congestion: a review of its etiology, evaluation, and
treatment. Ear Nose Throat J. 2000 Sep;79(9):690–8.
2. Fisher EW, Lund VJ, Scadding GK. Acoustic Rhinometry in Rhinological Practice: Discussion Paper. J R Soc Med. SAGE Publications; 1994 Jul 1;87(7):411–3.
3. Dadgarnia MH, Baradaranfar MH, Mazidi M, Azimi Meibodi SMR. Assessment of Septoplasty Effectiveness using Acoustic Rhinometry and Rhinomanometry. Iran J Otorhinolaryngol. 2013;25(71):71–8.
4. Johnson J, Rosen C, Bailey B. Bailey's Head and Neck Surgery - Otolaryngology. 5 ed. Vol. 1. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2013.
5. Kawalski H, Spiewak P. How septum deformations in newborns occur. Int J Pediatr Otorhinolaryngol. 1998 Jun;44(1):23–30.
6. Mladina R, Čujić E, Šubarić M, Vuković K. Nasal septal deformities in ear, nose, and throat patients. American Journal of Otolaryngology. 2008 Mar;29(2):75–82.
7. Pirsig W. Growth of the deviated septum and its influence on midfacial development. Facial plast Surg. 1992 Oct;8(4):224–32.
8. Flint PW, Haughey BH, Robbins KT, Thomas JR, Niparko JK, Lund VJ, et al. Cummings Otolaryngology - Head and Neck Surgery. Elsevier Health Sciences; 2014. 1 p.
9. Kim YM, Rha K-S, Weissman JD, Hwang PH, Most SP. Correlation of asymmetric facial growth with deviated nasal septum. The Laryngoscope. 2011 Apr 14;121(6):1144–8.
10. Hartman C, Holton N, Miller S, Yokley T, Marshall S, Srinivasan S, et al. Nasal Septal Deviation and Facial Skeletal Asymmetries. Anat Rec. 2016 Jan 22;299(3):295–306.
11. Nakai MMY. Twenty Years of Statistics and Observation of Facial Bone Fracture. Acta Oto-Laryngologica. 2009 Jul 8;118(538):261–5.
12. Erdmann D, Follmar KE, DeBruijn M, Bruno AD, Jung S-H, Edelman D, et al. A Retrospective Analysis of Facial Fracture Etiologies. Annals of Plastic Surgery. 2008 Apr;60(4):398–403.
13. Rhee SC, Kim YK, Cha JH, Kang SR, Park HS. Septal Fracture in Simple Nasal Bone Fracture. Plastic and Reconstructive Surgery. 2004 Jan;113(1):45–52.
14. Kuhnel TS, Reichert TE. Trauma of the midface. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2015;14:45.
15. Bloom JD, Kaplan SE, Bleier BS, Goldstein SA. Septoplasty Complications: Avoidance and Management. Otolaryngologic Clinics of North America. 2009 Jun;42(3):463–81.
16. Vården i siffror [Internet]. [Place unknown]: Kansliet för nationella kvalitetsregister; 2016. Operationsfrekvens avseende septumplastik [cited 2016 May 2]. Available from: https://www.vardenisiffror.se/registry/registry?descriptionSource=Patientregistret%2C%20Socialstyrelsen
14
17. Mochloulis G, Seymour FK, Stephens J. ENT and Head and Neck Procedures. CRC Press; 2014.
18. Hwang PH, McLaughlin RB, Lanza DC, Kennedy DW. Endoscopic septoplasty: indications, technique, and results. Otolaryngol Head Neck Surg. SAGE Publications; 1999 May;120(5):678–82.
19. Sathyaki DC, Geetha C, Munishwara GB, Mohan M, Manjuanth K. A Comparative Study of Endoscopic Septoplasty Versus Conventional Septoplasty. Indian J Otolaryngol Head Neck Surg. 2013 Nov 24;66(2):155–61.
20. Sataloff RT. Sataloff’s Comprehensive Textbook of Otolaryngology: Head & Neck Surgery. Jaypee Brothers,Medical Publishers Pvt. Limited; 2015.
21. Wu P, Hamilton G III. Extracorporeal Septoplasty: External and Endonasal Techniques. Facial plast Surg. 2016 Feb 10;32(01):022–8.
22. Ganesan S, Prior AJ, Rubin JS. Unexpected overnight admissions following day-case surgery: an analysis of a dedicated ENT day care unit. Annals of The Royal College of Surgeons of England. Royal College of Surgeons of England; 2000 Sep 1;82(5):327.
23. Mäkitie A. Postoperative Infection Following Nasal Septoplasty. Acta Oto-Laryngologica. 2000;120(543):165–6.
24. Rettinger G, Kirsche H. Complications in septoplasty. Facial plast Surg. Copyright © 2006 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA; 2006 Nov;22(4):289–97.
25. Awan MS, Iqbal M. Nasal packing after septoplasty: a randomized comparison of packing versus no packing in 88 patients. Ear Nose Throat J. 2008 Nov;87(11):624–7.
26. Banglawala SM, Gill M, Sommer DD, Psaltis A, Schlosser R, Gupta M. Is nasal packing necessary after septoplasty? A meta-analysis. Int Forum Allergy Rhinol. 2013 May;3(5):418–24.
27. Gupta M, Motwani G. Comparative study of endoscopic aided septoplasty and traditional septoplasty in posterior nasal septal deviations. Indian J Otolaryngol Head Neck Surg. 2005 Oct;57(4):309–11.
28. Gulati SP, Wadhera R, Ahuja N, Garg A, Ghai A. Comparative evaluation of endoscopic with conventional septoplasty. Indian J Otolaryngol Head Neck Surg. Springer-Verlag; 2009 Mar 31;61(1):27–9.
29. Bothra R, Mathur NN. Comparative evaluation of conventional versus endoscopic septoplasty for limited septal deviation and spur. J Laryngol Otol. Cambridge University Press; 2009 Jul;123(7):737–41.
30. Champagne C, de Régloix SB, Genestier L, Crambert A, Maurin O, Pons Y. Endoscopic vs. conventional septoplasty: A review of the literature. Eur Ann Otorhinolaryngol Head Neck Dis. Elsevier Masson SAS; 2016 Feb 1;133(1):43–6.
31. Newton JR, White PS, Lee MSW. Nasal septal perforation repair using open septoplasty and unilateral bipedicled flaps. J Laryngol Otol. Cambridge University Press; 2006 Mar 8;117(01):52–5.
15
32. Kim DW, Egan KK, O'Grady K, Toriumi DM. Biomechanical strength of human nasal septal lining: comparison of the constituent layers. The Laryngoscope. John Wiley & Sons, Inc; 2005 Aug;115(8):1451–3.
33. Morre TD, Van Camp C, Clement PA. Results of the endonasal surgical closure of nasoseptal perforations. Acta Otorhinolaryngol Belg. 1995;49(3):263–7.
34. Lumsden A, Shakeel M, Ah-See KL, Supriya M. Management of nasal septal perforation: Grampian experience. Austin Journal of Otolaryngology. 2015.
35. Stewart MG, Smith TL, Weaver EM, Witsell DL, Yueh B, Hannley MT, et al. Outcomes after nasal septoplasty: results from the Nasal Obstruction Septoplasty Effectiveness (NOSE) study. Otolaryngol Head Neck Surg. 2004 Mar;130(3):283–90.
36. Schwentner I, Dejakum K, Schmutzhard J, Deibl M, Sprinzl G. Does nasal septal surgery improve quality of life? Acta Oto-Laryngologica. 2006 Jul 1;126(7):752–7.
37. Calder NJ, Swan IRC. Outcomes of septal surgery. J Laryngol Otol. Cambridge University Press; 2007 Mar 12;121(11).
38. Mondina M, Marro M, Maurice S, Stoll D, de Gabory L. Assessment of nasal septoplasty using NOSE and RhinoQoL questionnaires. European Archives of Oto-Rhino-Laryngology. Springer-Verlag; 2012 Oct;269(10):2189–95.
39. Arunachalam PS, Kitcher E, Gray J, Wilson JA. Nasal septal surgery: evaluation of symptomatic and general health outcomes. Clin Otolaryngol Allied Sci. Blackwell Science Ltd; 2001 Oct;26(5):367–70.
40. Croy I, Hummel T, Pade A, Pade J. Quality of life following nasal surgery. The Laryngoscope. Wiley Subscription Services, Inc., A Wiley Company; 2010 Apr;120(4):826–31.
41. Kuduban O, Bingol F, Budak A, Kucur C. The Reason of Dissatisfaction of Patient after Septoplasty. Eurasian J Med. 2015 Nov 12;47(3):190–3.
42. Dinis PB, Haider H. Septoplasty: Long-term evaluation of results. American Journal of Otolaryngology. 2002 Mar;23(2):85–90.
43. Konstantinidis I, Triaridis S, Triaridis A, Karagiannidis K, Kontzoglou G. Long term results following nasal septal surgery. Auris Nasus Larynx. 2005 Dec;32(4):369–74.
44. Sundh C, Sunnergren O. Long-term symptom relief after septoplasty. Eur Arch Otorhinolaryngol. 2015 Oct;272(10):2871–5.
45. Kulkarni SV, Kulkarni VP, Burse K, Bharath M, Bharadwaj C, Sancheti V. Endoscopic Septoplasty: A Retrospective Analysis of 415 Cases. Indian J Otolaryngol Head Neck Surg. Springer India; 2015 Jul 1;67(3):248–54.
46. Hwang K, You SH, Kim SG, Lee SI. Analysis of nasal bone fractures; a six-year study of 503 patients. J Craniofac Surg. 2006 Mar;17(2):261–4.
47. Mohammadi A, Ghasemi-Rad M. Nasal bone fracture--ultrasonography or computed tomography? Med Ultrason. 2011 Dec;13(4):292–5.

16
48. Ronis M, Veidere L, Marnauza D. Nasal Bone Fractures In Children And Adolescents. Patient Demographics, Etiology of The Fracture and Evaluation of Plain Film Radiography as a Diagnostic Method in Children’s Clinical University Hospital. Mechanics, Materials Science & Engineering Journal. Magnolithe; 2016.
17
Appendix A
18
19
B
20
21
C
22
D