Embed Size (px)
Citation preview

OLIF: OBLIQUE LUMBAR INTERBODY FUSION
Richard G. Fessler, MD, PhDRush University Medical Center
Chicago, IL

DISCLOSURE
• Royalty• DePuy, Stryker
• Professional Societies• President: ISMISS• Vice President: SICCMI
• Editorial Board• Neurosurgery, Neurosurgical Reviews, JSDT, Spinal Surgery, Operative Neurosurgery, Internet Journal of
Minimally Invasive Spinal Technology, Pan Arab Journal of Neurosurgery, Journal of CraniovertebralJunction and Spine, The Scientific World Journal
• In Queue Innovations• Co-owner

ANATOMY

POSITIONING
• True direct lateral• Bean bag• Arm support• Tape skin• Position over break in table


INCISION/DISSECTION

LOCALIZATION/STIMULATION

DILATION/RETRACTION

DISCECTOMY AND TRIAL

CAGE PLACEMENT

• 16 study systematic review• 2364 levels, 30% 1 level, 17% 2 level; 13% # levels not reported
• Mean EBL 110 mL, OR time 95 min, fusion 93%• Intraoperative complications 1.5%• Postoperative complications 9.9%
• Transient thigh pain and/or numbness 1.5% • HF weakness 3%• These generally resolved by 3 m
• Did not evaluate radiographic parameters

• 137 cases, 340 levels RR• Complications 11.7%
• Ileus 2.9%• Subsidence 4.4%• Vascular injury 2.9%
• Fusion at 6 m – 97.9%• Did not examine radiographic
parameters





LATERAL ENDOSCOPIC APPROACH*
• First developed by Fessler and MacMillan in 1992, presented in 1994, and published by McAfee in 1998
• Minimally invasive retroperitoneal approach• Classic laparoscopy• 19 patients: L 2/3 – L 4/5• Majority of patients treated had previous posterior surgery
• Technique further advanced by Ozgur et al in 2006 as XLIF• Direct vision• Minimize approach morbidity by avoiding retroperitoneal structures• 13 patient with axial back pain without severe central stenosis who failed 6m
conservative therapy• Excluded stenosis, rotatory scoliosis, >grade 1 and mobile spondylolisthesis
*Hybrid of LIFF and OLIF

RETROPERITONEAL ENDOSCOPIC LUMBAR FUSION
Requires four incisions
Small enough for tight seal
CO2 insufflation
Mark using fluoroscopy

BALLOON DISSECTION

RETRACT ILIOPSOASMUSCLE
Steinman Pins

RELF TECHNIQUE

Protects all adacent tissues
TAP IN OUTER CANNULA

GRAFT PLACEMENT

THA
NK YO
U

PERCUTANEOUS LUMBAR FUSION SET
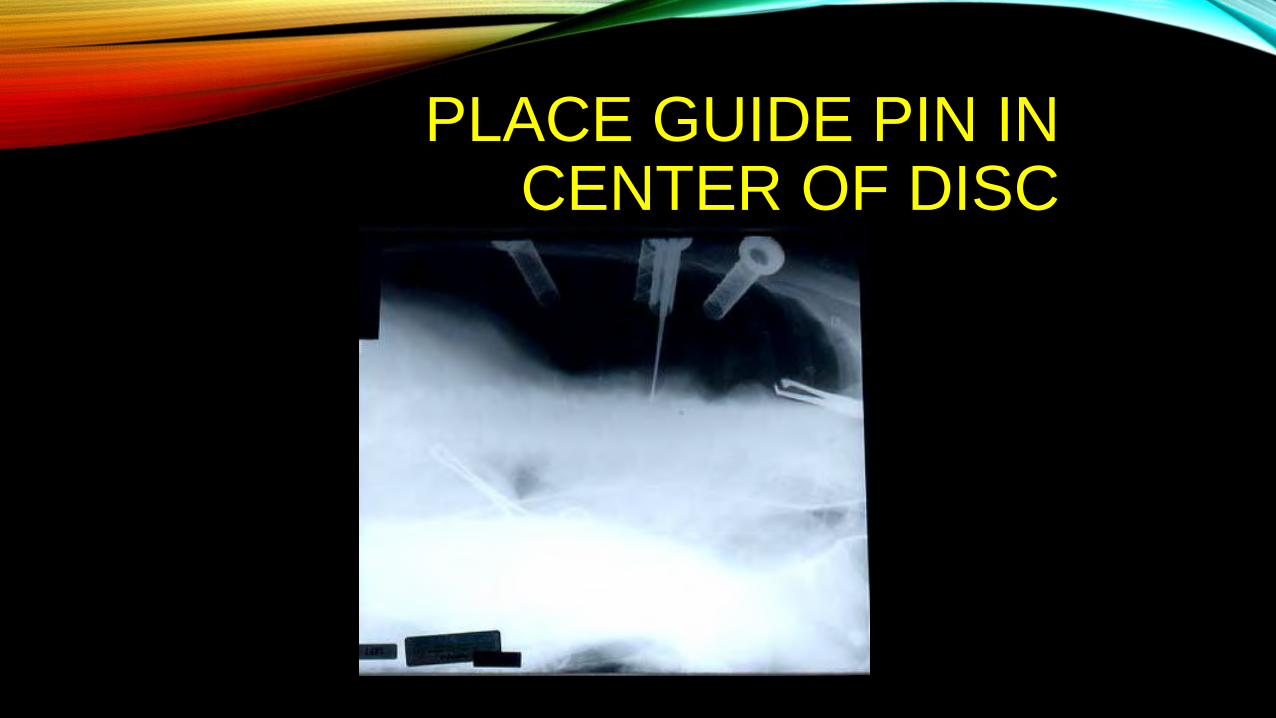
PLACE GUIDE PIN IN CENTER OF DISC

PERFORM DISCECTOMY
Trephine over guide pin
Curettage and Pituitary Rongeurs

DISTRACTION
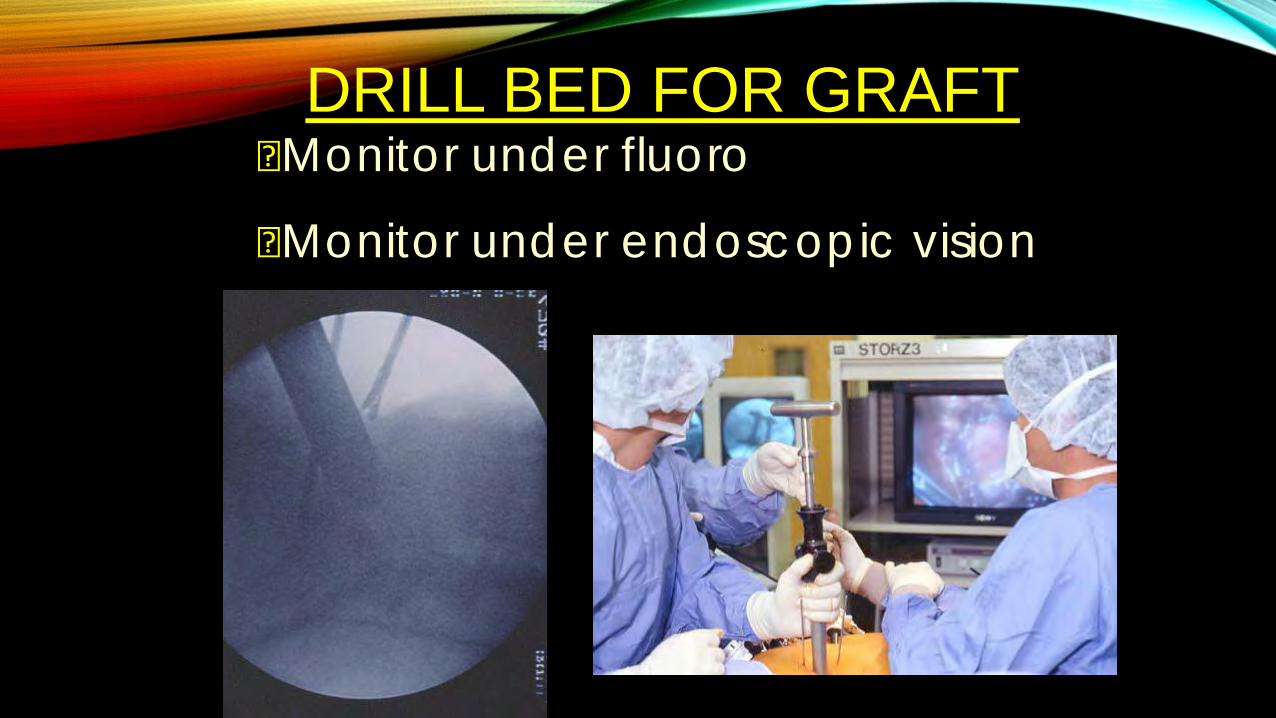
DRILL BED FOR GRAFTMonitor under fluoro
Monitor under endoscopic vision

L 2/3 = 3
L 3/4 = 5
L 4/5 = 11
PATIENTS

FOLLOW - UPMean = 3 years
Range = 2 - 5 years

RESULTS:
ADDITIONAL POSTERIOR FUSION
7 / 19 patients

LOCALIZATION
• Fluoroscopic Localization• Directly over the mid-disc for
one level• In between discs for two levels• Can use longer incision if >2• Can use multiple incisions
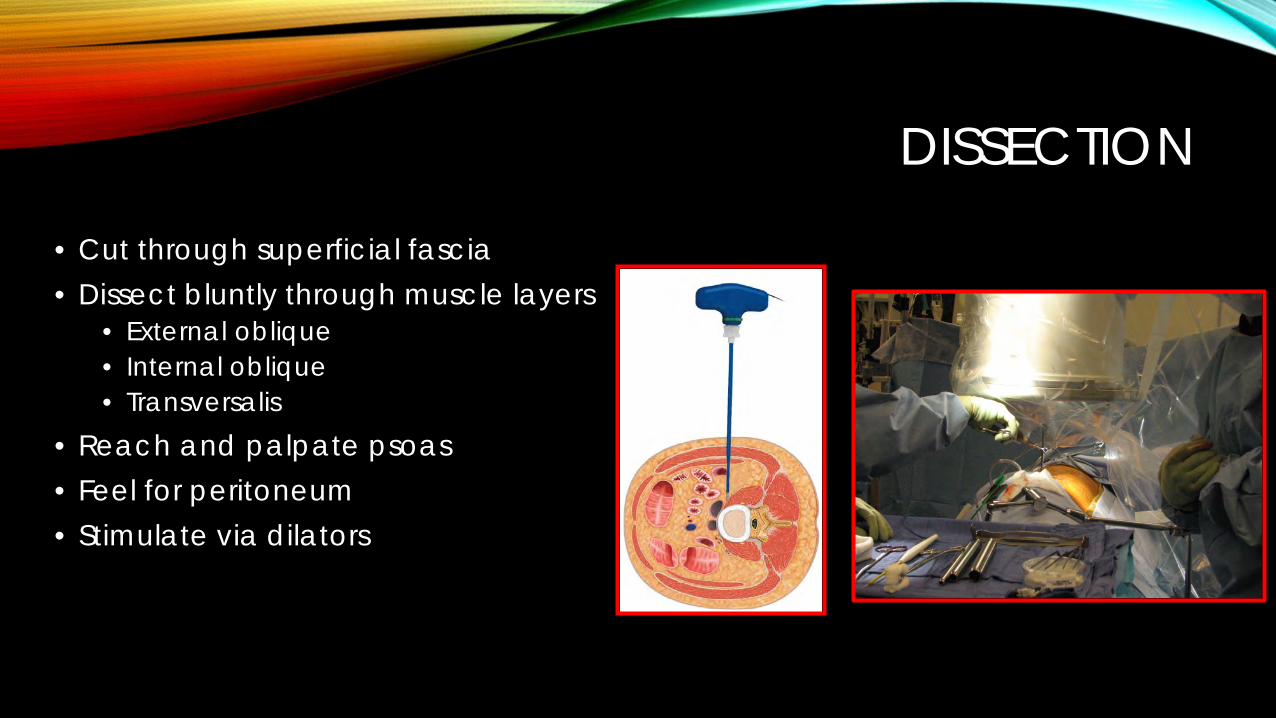
DISSECTION
• Cut through superficial fascia• Dissect bluntly through muscle layers
• External oblique• Internal oblique• Transversalis
• Reach and palpate psoas• Feel for peritoneum• Stimulate via dilators






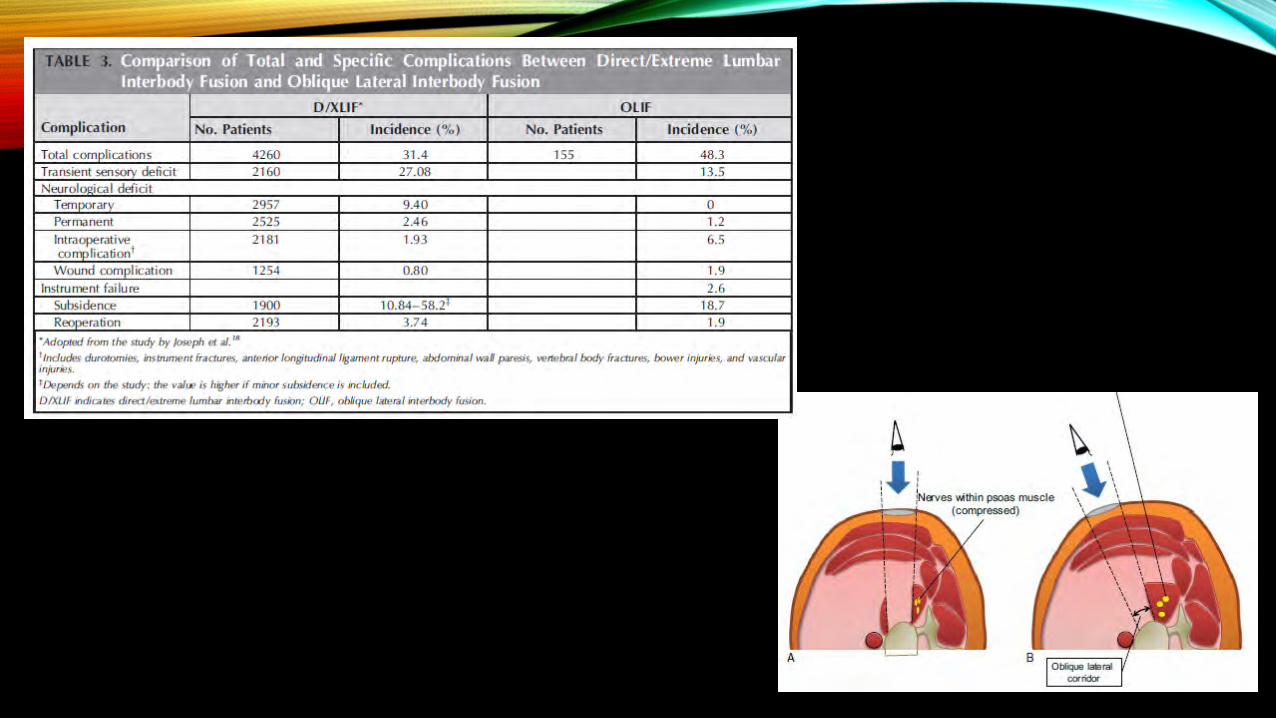
COMPLICATIONS• Unique set of approach-related complications• Monitor L2-5 myotomes for lumbar plexus
• Anterior thigh numbness and pain – genitofemoral nerve • Resolution in 69% and 75% at 6m (Moller et al.)
• Psoas weakness*• Most common; Anand et al. 75% of patients• Majority resolve; Moller et al. - 84% at 6 m
• Retroperitoneal hematoma and surgical hernia• Motor nerves to abdominal wall – paresis with abnormal bulging
• Rates highly variable in the literature • Rodgers et al. 2011 - 600 patients XLIF 1% approach and 6.2% overall
• *Did not consider thigh pain and psoas weakness as complications• Alimi et al. 2014 thigh numbness in 4.4 % and weakness in 2.2% - all resolved but 1 case

CLINICAL OUTCOMES• Alimi et al. 2014
• 145 levels in 90 patients,17.6m clinical f/u• 84.8% of patient had excellent, good or fair functional outcome• ODI, VAS for back buttock and leg pain all significantly improved
• Lee et al. 2014• 116 levels in 90 patients, 1 year f/u• 87.8% CT confirmed fusion• ODI, VAS all significantly improved
• Kotwal et al. 2012• 237 levels in 118 patients, 2 year f/u• 88% CT confirmed fusion• ODI, VAS significantly improved
• Rodgers et al.• 66 patients, 1 year f/u, 1 - 2 levels• 96.6% CT confirmed fusion• 90% patients ‘satisfied or very satisfied’





























