Embed Size (px)
DESCRIPTION
The Florida BRITE Project: Screening and Brief Interventions for Older Adult at Risk of Substance Misuse . Larry Schonfeld, Ph.D . Interim Executive Director, Florida Mental Health Institute [email protected] http://BRITE.fmhi.usf.edu Presented at the FADAA/FCCMH Conference Aug. 7, 2013. - PowerPoint PPT Presentation
Citation preview

The Florida BRITE Project: Screening and Brief Interventions for Older
Adult at Risk of Substance Misuse
Larry Schonfeld, Ph.D.Interim Executive Director, Florida Mental Health Institute
[email protected] http://BRITE.fmhi.usf.edu
Presented at the FADAA/FCCMH Conference Aug. 7, 2013

Today’s presentation• Overview of substance abuse issues
and treatment for older adults• Presentation on the Florida BRITE
Project– Pilot project funded by Florida DCF
(2004-07)– Expansion through national SBIRT
initiative funded by SAMHSA/CSAT $14 million grant
• Lessons learned from conducting SBIRT in Florida

Alcohol and Illicit Drugs

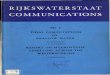
National Household Survey: % Adults Aged 18+ Reporting past month use of alcohol/drugs by age group in 2000 (NHSDA, 2001)
Perc
ent
Repo
rtin
g U
se in
Pas
t M
onth12% of 55+ age group are
either binge or heavy alcohol users
Any Illicit Drug Use
Any Alcohol Use
"Binge" Al-cohol use
Heavy Alcohol Use
0
10
20
30
40
50
60
7015
.9
56.8
37.8
12.8
7.8
58.3
30.3
7.6
4.9
53.0
21.1
5.3
1.0
37.5
9.4
2.3
18 to 2526 to 3435 to 5455 or Older

U.S. Substance Abuse Treatment Admissions in 2006
Trunzo & Henderson (Gerontological Society of America presentation 2008)
50+ yrs11%25-34 yrs
25%
35-44 yrs27%
50-54 yrs: 6%
55-59 yrs: 3%
60-64 yrs: 1%65+ yrs: <1%
NALL ADMISSIONS = 1,798,000NADMISSIONS OVER 50 = 189,000
45-49 yrs11%
18-24 yrs18%
<18 yrs8%

Admissions Under 50 and Age 50+by Primary Substance
20%
38%47%
58%66% 70%
18%
18%15%
12%9%
11%
14% 14%11%
8%6%
3%18% 17%12% 11% 7%
18%
13%
9%
<50 50-54 55-59 60-64 65-69 70+
Sedatives/Tranqs.
Narcotic Analgesics*
Methamphetamine/Amphets.
Cocaine
Heroin
Marijuana
Alcohol & Drug
Alcohol Only
* Excludes methadone

Older adults are often “hidden” alcohol abusers
• Fewer indicators compared to younger adults:• DUI’s• Work-related problems• Marital Problems• Peer pressure
• In contrast, older adults are more likely to be isolated, drinking alone– More likely to identified in healthcare settings
as secondary problem to the reason for admissions to ER, primary care.

Alcohol Affects the Elderly Differently
• Induced impairment increases with age due to:– Higher body fat content, less lean muscle mass,
and reduced water volume (alcohol is water soluble)
– Decreased absorption rate in gastrointestinal system due to decreased blood flow
• Affects alcohol’s distribution within the body • Affects alcohol’s elimination• Results in increased sensitivity and
decreased tolerance to alcohol and drugs in older individuals
• Drugs and alcohol remain in the body longer and at higher rates of concentration

Medication misuse

Older Adults: Adverse Drugs Events
• People age 65+ make up 12% of U.S. Population, but – account for 34% of all prescription medication
use – account for 30% of all over-the-counter
medication use– Annually, 1 in 3 adults ages 65+ experience
adverse drug events
• Susceptible to problems due to altered:– pharmacodynamics (how the drug affects
individual)– pharmacokinetics (how the body absorbs,
distributes, metabolizes, eliminates a drug)

Misuse in older people is often unintentional
(Glantz, 1981; Schwartz et al., 1962).• Difficulty of regimen (too many meds to keep
track)• Memory issues• Adverse drug reactions• Synergistic effects of multiple drugs• Cost & Access• Multiple prescribing physicians• Lack of understanding of the instructions
– They are less likely to ask physician or pharmacist questions or receive written information about prescriptions (Olins, 1985).
• Use of/interactions with OTC meds (Coons et al., 1988)
• Early discontinuation of medications

Medications & Alcohol Use• Use of drugs in combination with
alcohol carries greater risk:– hepatoxicity with acetaminophen– increased lithium toxicity– enhanced CNS depression for
those prescribed tricyclic antidepressants
– death - for those taking benzodiazepines and barbiturates

Treatment Recommendations

Expert panel recommendations for screening and treating the older adult:SAMHSA/CSAT Treatment Improvement Protocol (TIP) #26

TIP#26 Expert Panel Recommendations1. Age-specific, group treatment that is supportive,
not confrontational2. Attend to depression, loneliness; address losses.3. Teach skills to rebuild social support network4. Employ staff experienced in working with elders5. Link with aging, medical, institutional settings6. Content should be age-appropriate and offered at
a slower pace.7. Create a “culture of respect” for older clients8. Broad, holistic approach recognizing age-specific
psychological, social & health aspects.9. Adapt treatment as needed to address gender
issues

FMHI - developed group treatment Relapse prevention, Cognitive-behavioral/Self-management
skills• Gerontology Alcohol Project (1979-1981) –successfully
treated late onset, older alcohol abusers and improving social support, mood (Dupree, Broskowski & Schonfeld, 1984)
• Substance Abuse Program for Elderly (1986-1994) extended GAP approach to all older adults irrespective of age of onset and type of substance (Schonfeld & Dupree, 1991; Schonfeld , et al., 1995; Schonfeld & Dupree, 1995; 1998)
• Replications - programs in other states based on our model• Chelsea Arbor Older Adult Recovery Center in Ann Arbor,
Michigan (1990’s)• GET SMART Program (West Los Angeles VA Hospital; 2000-2011)
(Schonfeld et al. 2000) • Zablocki VA Medical Center (Milwaukee, 2006) • Older Adult Substance Abuse Treatment Program – Tennessee
(2005 - 2008) (Outlaw et al. 2012)

The Result:A 16-session curriculum manual for conducting brief treatment
(Dupree & Schonfeld, CSAT, 2005)
http://kap.samhsa.gov/products/manuals/pdfs/substanceabuserelapse.pdf

A Three Stage CBT/Self-Management Treatment Approach
(Dupree & Schonfeld, SAMHSA/CSAT manual, 2005)
1. For each person begin by identifying his/her antecedents and consequences for substance use to create an individualized “substance use behavior chain” using the Substance Abuse Profile for the Elderly
2. Teach the person how to identify the components of that chain so that he or she can understand the high risk situations for alcohol or drug use.
3. Teach specific skills to address these high risk situations to prevent relapse.

A Three Stage CBT/Self-Management Treatment Approach
(Dupree & Schonfeld, SAMHSA/CSAT manual, 2005)
1. For each person begin by identifying his/her antecedents and consequences for substance use to create an individualized “substance use behavior chain” using the Substance Abuse Profile for the Elderly
2. Teach the person how to identify the components of that chain so that he or she can understand the high risk situations for alcohol or drug use.
3. Teach specific skills to address these high risk situations to prevent relapse.

However, a change was needed• In Florida, the actions of several task forces and
Florida Coalition on Optimal MH and Aging shaped a new agenda:– identified elders as an underserved population– Policy changes identifying them as a target
pop.
• Despite older adults’ positive outcomes in treatment programs, relatively few actually entered treatment.– In 2000, less than 2% of adults in Florida’s
treatment for substance abuse problems, were age 60+ despite the fact that they represent about 24% of the population

SBIRTA national initiative for
screening, brief intervention, and referral to treatment

SpecializedTreatment
PrimaryPrevention
BriefIntervention
None
Mild
Moderate Severe
Substance Abuse Severity and Level of CareAdapted from the SAMHSA TIP #34 (1999) and Institute of Medicine (1990)
Substance Abuse Severity

Screening and Brief InterventionsEarly Examples
• Used within Emergency Departments– Bernstein E, Bernstein J, Levenson S: Project ASSERT: An ED-
based intervention to increase access to primary care, preventive services, and the substance abuse treatment system. Ann Emerg Med , 1997; 30:181-189.
• Used within primary care practices as “Brief Physician Advice” for older adults– Fleming, MF., Manwell, LB, Barry, KL, Adams, W, & Stauffacher,
EA Brief physician advice for alcohol problems in older adults: A randomized community-based trial. J Fam Pract; 1999 48(5): 378-84

http://sbirt.samhsa.gov/about.htm

SBIRT Core Components

Motivational Interviewing (MI)• People who “screen positive” for substance
misuse may be reluctant to seek help and are often ambivalent about making a decision to change behavior
• Confrontation & labeling will produce “resistance” or the person will be labeled as being “in denial.” Resistance can also be raised prior to treatment (e.g., spouses, employers, coercion from the legal system).
• With MI, resistance is viewed as a reaction to the in-session behavior of the counselor.

Key Principles of Motivational Interviewing
• Avoiding labeling and confrontation• Enhance Self-efficacy (confidence in
one’s coping strategies)• Enhance internal-attribution• Roll with resistance – use it to further
explore client’s views• Use cognitive dissonance as a tool – the
client is asked to provide more and more evidence that problem(s) exist

Videos – examples of Brief Intervention
• Boston University: BNI-ART Institutehttp://www.bu.edu/bniart/sbirt-in-health-care/sbirt-educational-materials/sbirt-videos/
• Provide scenarios for using screening and brief intervention during the delivery of healthcare.
• Videos illustrate the use of MI techniques

The Pilot: Florida BRITE Project 2004-07
(BRief Intervention and Treatment for Elders)
• 3,497 people ages 60+ screened and/or served
Schonfeld et al (2010) Am. J. of Public Health• Four sites in pilot project
• Broward County Elderly & Veterans Services = 2,116• Gulf Coast Jewish Family Services (Pinellas) = 638• Coastal Behavioral Health Care (Sarasota) = 426• Center for Drug Free Living (Orange) =
317• Most (67%) identified via BRITE outreach &
prescreening at health fairs, senior centers, and via referral network.
• Positive prescreens invited to participate in BI– Most received multiple sessions of brief intervention

Broward County Elderly & Veterans Services
Gulf Coast Jewish Family
Services
Coastal Behavioral HealthCare
The Florida BRITE ProjectPilot Project (2004-2007)
Center for Drug Free Living – added in
2005Orlando

The Pilot: Florida BRITE Project 2004-07
(BRief Intervention and Treatment for Elders)
• Purpose: to identify people ages 60+ who misused or were at risk for misusing:– Alcohol– Prescription medications– Over-the-counter (OTC) medications– Illicit drugs
• Depression and suicide risk also screened by BRITE– Depression - most frequent antecedent to
substance abuse in elders (Dupree et al., 1984; Schonfeld & Dupree, 1991, Schonfeld et al., 2000)
– Elders - highest rate of suicides among all age-groups

The Pilot: Florida BRITE Project 2004-07
(BRief Intervention and Treatment for Elders)• 10% - referred for potential alcohol
problems 69% of all 3,497 screened were drinkers 18% of drinkers had 3 or more drinks on a
drinking day
• 26% referred for prescription misuse 32% needed education/assistance on proper
med use 17% could not recall purpose of 1 or more meds 11% reported wrong amount for 1 or more meds 8% took medications for wrong
reasons/symptom• 8% referred for potential OTC misuse• 1% referred for illicit drug use

• Depression (Short-Geriatric Depression Scale)– 64% of all referrals were for depression
SGDS scores: 25% moderate, 10% serious
– Among those referred for reasons other than depression:SGDS: 18% moderate, 4% serious
• Suicide Risk: Only 0.6% referred for suicide risk– But 13% contemplated suicide at some time in
the past (most of these within the past year)
The Pilot: Florida BRITE Project 2004-07
(BRief Intervention and Treatment for Elders)

• Significant decrease in alcohol scores at D/C (n=102) – No further changes at 30 day follow-ups (n =60)
• Prescription Medications: a 32% decrease in “flags” at D/C over the number at baseline (n=180)
• OTCs: 23 of 24 people flagged at baseline, no flag at D/C
• Illicit drugs: 75% of those with flags at baseline (n=12) showed no flag at D/C
• Significant decrease1 in depression scores at D/C (n=323) – Further decrease at 30 day follow-up (n = 203)
The Pilot: Outcomes 2004-07Significant improvement at D/C and Follow-
ups

From Pilot Project to Federal Grant

State SBIRT Grants Through 2010

Florida BRITE Project – the SBIRT Grant:
(BRief Intervention and Treatment for Elders)
• $14 million SAMHSA/CSAT grant to Florida – Five years: Oct. 2006-Sept. 2011– Funding mostly went towards direct
services– Large scale screening in medical, other
settings• Majority of people are expected to screen
negative (receive Screening & Feedback only)• Positive screens were typically followed by 1
session of Brief Intervention • People could receive 5 BI or 12 BT sessions• Referred out for detox, residential care, etc.

30 provider agencies contracted to conduct
screening in over 70 sites in 18 counties

SBIRT Approach• Universal prescreening (7 items: alcohol,
drugs, medications, depressive symptoms)
• Full screen (ASSIST) for those with positive prescreens
• Level of risk dictates type of service:– Screening & Feedback (SF) for negative screens– Brief Intervention (BI) for moderate risk– Brief Treatment (BT) for moderate to high risk– Referral to Treatment (RT) - high risk/problem
use

Prescreen – Part 1

Prescreen – Part 2

Alcohol, Smoking and Substance Involvement Screening Test (ASSIST)World Health Organization (WHO)
• An interview style screen administered only if there is a positive prescreen
• The ASSIST was developed to help healthcare professionals detect and manage substance use
• Scores provide a “level of risk” for alcohol or for other substances and type of service that follows:– Low risk = screening & feedback (SF) about
results– Moderate risk = indicates the need for brief
intervention (BI) using motivational interviewing
– Moderate to High Risk = Brief treatment (BT)– High Risk = Referral to treatment

Past 30 days of Substance Use Yes # DaysMean (sd)
Used any alcohol? 4,915 (60.2%) 18.2 (10.4)Used alcohol to intoxication (5+ drinks in one sitting) 1,554 (19.0%) 12.4 (10.2)Used alcohol to intoxication (<4 drinks in one sitting & felt high)
1,815 (22.2%) 9.7 (8.4)
Intoxication (either 5+ drinks or 1-4 drinks & felt high) 1,102 (13.5%) 17.9 (11.4)
Used illegal drugs 435 (5.3%) 11.4 (10.3)Used both alcohol & drugs on same day 4,915 (60.2%) 18.2 (10.4)
Florida BRITE Project Reasons for Positive Screens at Baseline
(n=8,165)

BRITE Services Received• For those who screened positive and
agreed to receive services:
o BI n = 6,338o BT n = 675o RT n = 899

Positive Screens – by Provider Category
Total Aging MentalHealth
HealthCare
Substance Abuse
Positive ScreensTotal Screened% Positives
8,16585,001
9.6%
1,994 16,01912.4%
1,358 14,649
9.3%
3,46943,772
7.9%
1,281 10,49012.2%

Aging 36%
Behav. Health 22%
Health 29%
SA 10%
Unknown 2%
Clients Receiving Either BI, BT, or RT by Category of Service
Provider

Past 30 Day Use of Alcohol and Drugs:Baseline versus Six Month Follow-up
InitialInterview
Follow-upInterview
ASSIST Questions N Days N Days%
Decrease Sig. p)
Use any alcohol 133 9.01 134 2.41 73.3 <.001Use alcohol to intox. with 5+ drinks 31 5.10 31 2.68 47.5 .024Used alcohol to intox. with 4 or fewer drinks and felt “high 32 4.81 32 2.84 41.0 .031
Used illicit drugs 132 7.37 133 1.89 74.4 <.001
Used both alcohol & drugs on same day 14 8.29 14 2.86 65.5 .038

Sustainability of SBIRT• Nationally, a number of actions and events
are fostering SBIRT’s sustainability:– The BIG (Brief Intervention Group) Initiative for
EAP programs and Hospitals cross North America
– American College of Surgeons’ Committee on Trauma requires SBIRT in Level I & II trauma centers
– Billing codes for SBIRT available to providers– Local adoption of BRITE as a model in Florida
and nationally (to bill through Older Americans Act $s)

Billing codes for SBI were adopted Feb. 2008
• Reimbursement for screening and brief intervention is available through commercial insurance CPT codes, Medicare G codes, and Medicaid HCPCS codes
• Florida has not approved Medicaid codes for billing purposes

Payer Code DescriptionFee
Schedule
CommercialInsurance CPT
99408
Alcohol and/or substance abuse structured screening and brief intervention services; 15 to 30 minutes
$33.41
CPT 99409
Alcohol and/or substance abuse structured screening and brief intervention services; greater than 30 minutes
$65.51
MedicareG0396
Alcohol and/or substance abuse structured screening and brief intervention services; 15 to 30 minutes
$29.42
G0397Alcohol and/or substance abuse structured screening and brief intervention services; greater than 30 minutes
$57.69
Medicaid H0049 Alcohol and/or drug screening $24.00
H0050 Alcohol and/or drug service, brief intervention, per 15 minutes $48.00


Health Care providers who can provide SBIRT services under Medicare
• Medicare pays for medically reasonable & necessary SBIRT services in physicians’ offices & outpatient hospitals
• Physicians, Physician Assistants, Nurse Practitioners, Clinical Nurse Specialists, Clinical Psychologists, or Clinical Social Workers can bill for SBIRT
• To bill Medicare, providers of MH services must be:– Licensed or certified to perform mental health
services by the state in which they perform the services;
– Qualified to perform the specific mental health services rendered; and
– Working within their State Scope of Practice Acthttp://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/SBIRT_Factsheet_ICN904084.pdf

BRITE as an Evidence Based Practice for Older
Adults• A 2012 Issue Brief published by SAMHSA
and U.S. Admin. on Aging identified BRITE as one of the evidence-based practices for behavioral health services to older Americans.
• For states that adopt the model, staff from aging services can now implement BRITE and their agency can be reimbursed by each state’s department of aging from federal funding.

Conclusions• SBIRT is an evidence-based, national
initiative applied mostly in hospitals and primary care
• SBIRT focuses on risky/problematic use
• Florida BRITE Project found that:– Screening conducted in a variety of settings– Aging services have higher % of positive screens– Alcohol is the most problematic substance– Med. misuse - a major issue, but difficult to
assess
• SBIRT model is sustainable

The End
Questions?