Embed Size (px)
Citation preview

Large Polyp Removal
Objective
To demonstrate the nursing role in the care of the patient having a large polyp removal
Disclosures:I have none
Large Polyps
Usually sessile, serrated, may be adenomas and often located in the cecum or right colon, but can be found in any section of the colon.
Because of the polyp size and location, these are high risk procedures for perforation, especially if located in the cecum or right colon.
Patients are prepped as usual for a colonoscopy, and a clean colon is critical because of the use of electro cautery and Argon, so stressing prep instructions and compliance is especially important.
Patients are screened at scheduling for blood thinners, and if prescribed, they are stopped prior to procedure to reduce the chance of a bleed. Clearance for safely stopping blood thinners from the prescribing physician is imperative.
These procedures should be scheduled for 1 hour procedure time, patients have the usual duration of recovery time.
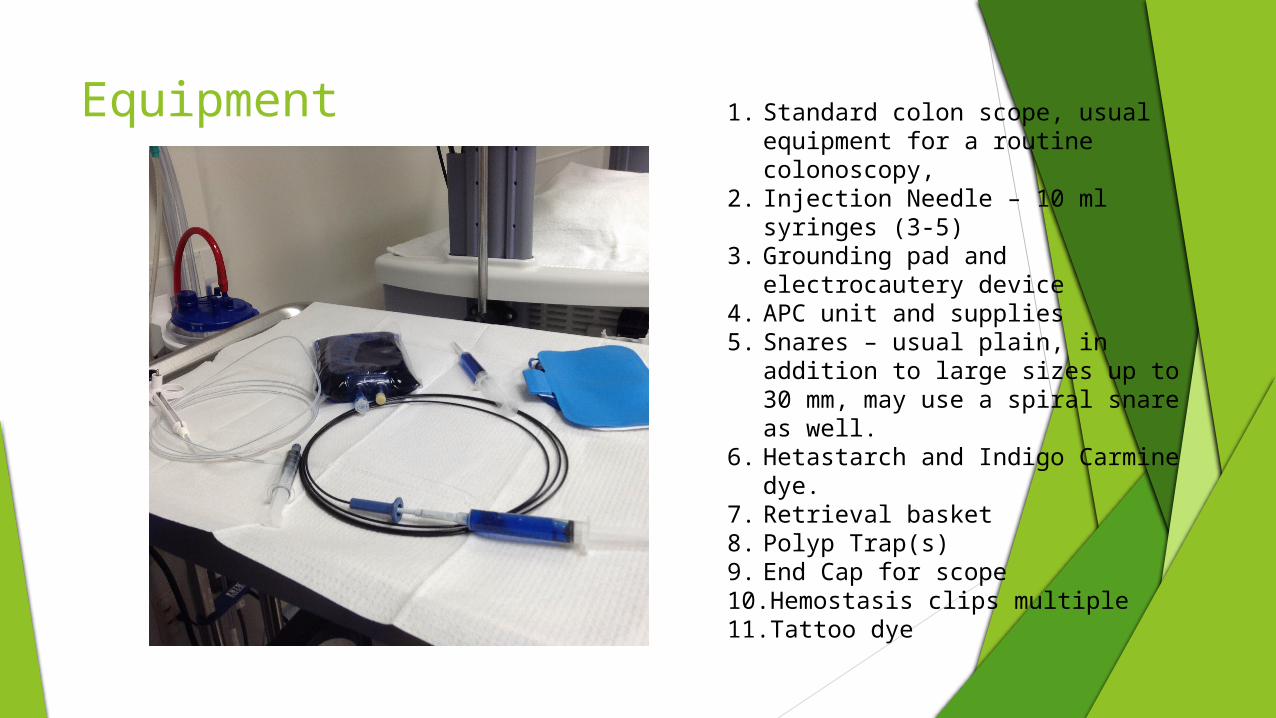
Equipment 1. Standard colon scope, usual equipment for a routine colonoscopy,
2. Injection Needle – 10 ml syringes (3-5)
3. Grounding pad and electrocautery device
4. APC unit and supplies5. Snares – usual plain, in addition to
large sizes up to 30 mm, may use a spiral snare as well.
6. Hetastarch and Indigo Carmine dye.
7. Retrieval basket8. Polyp Trap(s)9. End Cap for scope10.Hemostasis clips multiple11.Tattoo dye
Mixing the Hetastarch – Indigo Carmine Mixture
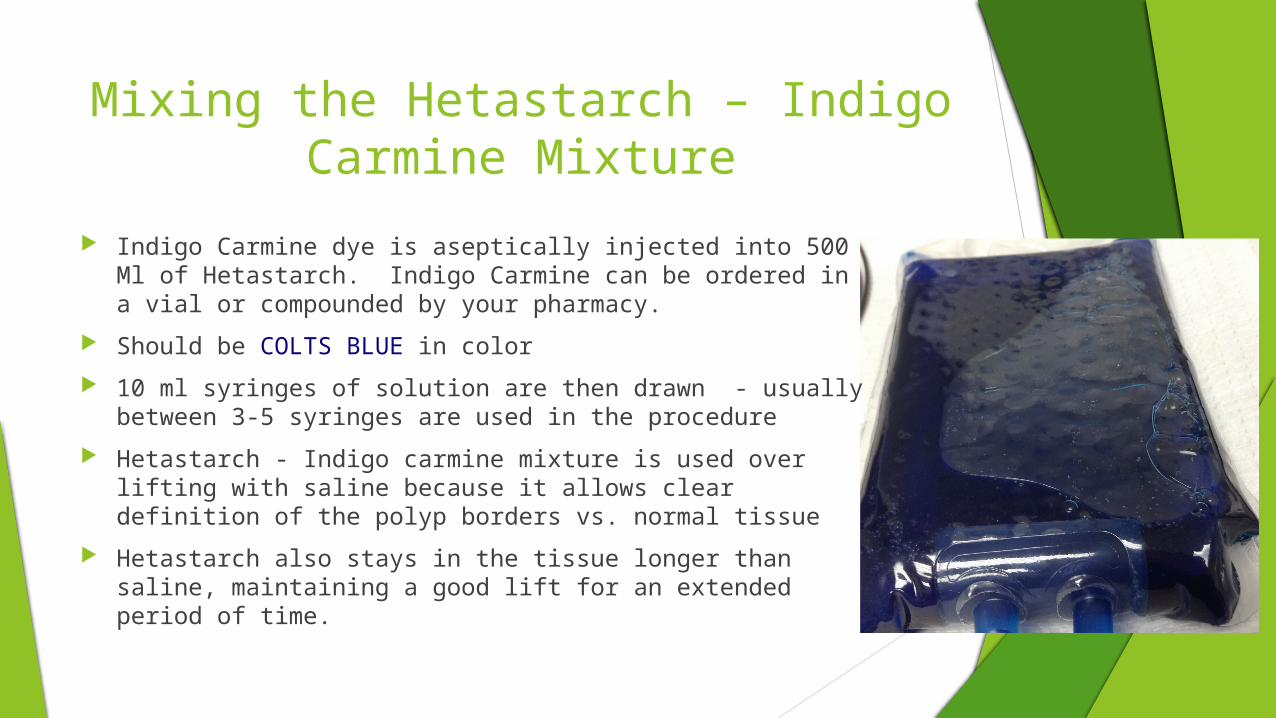
Indigo Carmine dye is aseptically injected into 500 Ml of Hetastarch. Indigo Carmine can be ordered in a vial or compounded by your pharmacy.
Should be COLTS BLUE in color
10 ml syringes of solution are then drawn - usually between 3-5 syringes are used in the procedure
Hetastarch - Indigo carmine mixture is used over lifting with saline because it allows clear definition of the polyp borders vs. normal tissue
Hetastarch also stays in the tissue longer than saline, maintaining a good lift for an extended period of time.
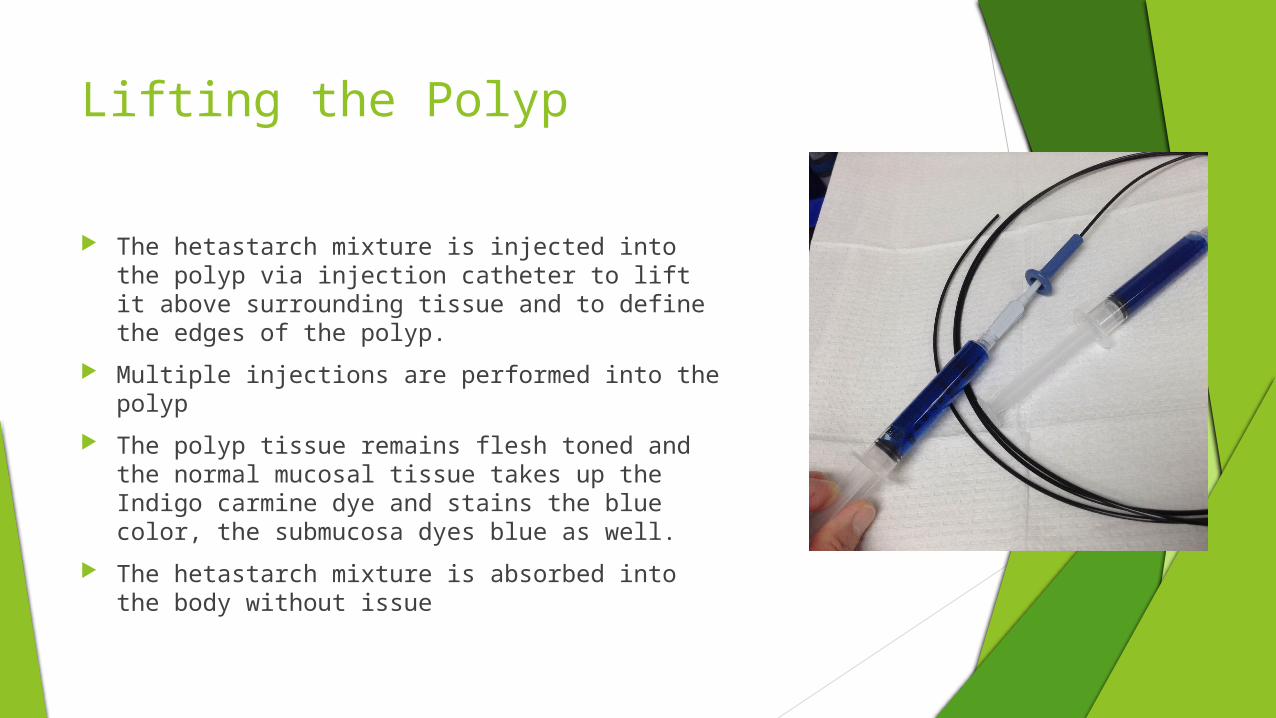
Lifting the Polyp
The hetastarch mixture is injected into the polyp via injection catheter to lift it above surrounding tissue and to define the edges of the polyp.
Multiple injections are performed into the polyp
The polyp tissue remains flesh toned and the normal mucosal tissue takes up the Indigo carmine dye and stains the blue color, the submucosa dyes blue as well.
The hetastarch mixture is absorbed into the body without issue
Snaring the polyp The patient is grounded for electrocautery, with safety assessment for
implants and body metal completed prior to procedure.
Standard Elecrocautery settings are usual
May use a variety of sizes of snares, and often the polyp is removed in multiple large sections
Spiral Snares have a helix loop that wraps around the oval snare loop, allowing a “grabbing and gathering of tissue”. These can feel jerky and require a bit of practice to gain your feel. These snares are larger than the usual snare so it takes a bit longer to close up tight on the polyp tissue, and you must be snug for an adequate burn to occur.
Occasionally the polyp tissue is suctioned up into the end cap, much like performing an EMR, and you will be required to snug up on the polyp, but have no visual. Make sure you have a good tactile sense for when you are snug, but use caution to not transect through before cautery is applied.
You will want to come through the polyp smoothly and with an even, steady motion to allow a good thermal transfer, and a clean cut.
ARGON Plasma Coagulation
Argon may be used to clean up the perimeter edges of the polyp by destroying any remaining polyp tissue and to create hemostasis.
The patient is grounded to the APC as directed by the manufacturer, with standard precautionary assessments completed.
The argon unit is set to the physicians desired settings, the probe is purged and then passed to the physician for use.
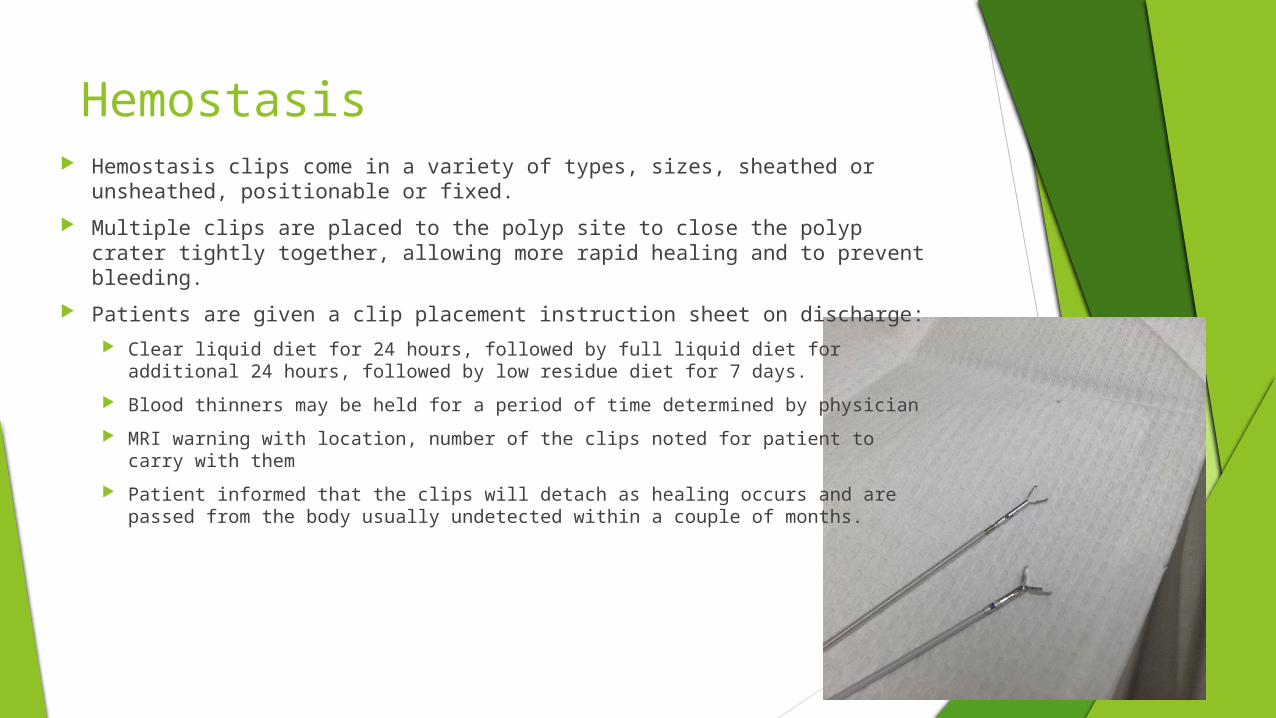
Hemostasis Hemostasis clips come in a variety of types, sizes, sheathed or
unsheathed, positionable or fixed.
Multiple clips are placed to the polyp site to close the polyp crater tightly together, allowing more rapid healing and to prevent bleeding.
Patients are given a clip placement instruction sheet on discharge:
Clear liquid diet for 24 hours, followed by full liquid diet for additional 24 hours, followed by low residue diet for 7 days.
Blood thinners may be held for a period of time determined by physician
MRI warning with location, number of the clips noted for patient to carry with them
Patient informed that the clips will detach as healing occurs and are passed from the body usually undetected within a couple of months.
Tattoo Often area of removal is tattooed for identification later.
Injection needle and Tattoo dye are used in normal fashion
Follow-up
Patients may return for follow-up colonoscopy inspection of site , usually within 3-6 months depending on the pathology of the polyp removed, patient history and completeness of initial removal.
Lets Watch…..
Video removed to decrease the size of the file so it could be uploaded to the web site.
Thanks to….
Dr. Doug Rex, MD
andMy fellow staff members at DRES, Springmill Surgery for their help and assistance…

Thanks
!
Questions and….