Embed Size (px)
DESCRIPTION
lapatinib paper
Citation preview

Clinical Therapeutics/Volume 30, Number 8, 2008
New Drug
Lapatinib: A Dual Inhibitor of Human Epidermal Growth Factor Receptor Tyrosine Kinases
PatrickJ. Medina, PharmD, BCOp1; and Susan Goodin, PharmD, FCCP, BCOP 2,3
1College of Pharmacy, University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma; 2Divi- sion of Pharmaceutical Sciences, The Cancer Institute of New Jersey, New Brunswick, New Jersey; and 3Divi- sion of Medical Oncology, University of Medicine and Dentistry of New Jersey/Robert Wood Johnson Medical School, New Brunswick, New Jersey
ABSTRACT Background: Lapatinib, the first dual inhibitor of
epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) tyrosine kinases, was approved by the US Food and Drug Ad- ministration (FDA) in 2007. It is indicated for use in combination with capecitabine for the treatment of patients with advanced breast cancer or metastatic breast cancer (MBC) whose tumors overexpress HER2 (ErbB2) and who have received previous treatment that included an anthracycline, a taxane, and trastuzumab.
Objective: This review summarizes the pharmacolo- gy, pharmacokinetics, clinical efficacy, and safety pro- file of lapatinib, and its current and potential role in the treatment of breast cancer and other malignancies.
Methods: Relevant English-language publications were identified through searches of MEDLINE (1966- May 2008), the American Society of Clinical Oncology abstracts database (2000-2007), abstracts from the San Antonio Breast Cancer Symposium (2005-2007), and the FDA Web site (January 2008). Search terms included lapatinib, GW572016, HER2, EGFR, recep- tor tyrosine kinase, dual-receptor blockade, adverse events, and clinical trials.
Results: The Tma:~ of lapatinib after oral adminis- tration is 3 to 4 hours. Dividing the dose or adminis- tering it with food, particularly a high-fat meal, in- creases the AUC >2-fold. Lapatinib is metabolized primarily by the cytochrome P450 3A4 isozyme, with 1 metabolite remaining active against EGFR but not HER2. Due to drug accumulation, the tu2 of lapatinib is 24 hours with continuous dosing. In a Phase III trial comparing lapatinib and capecitabine with capeci- tabine alone in women with HER2-positive, locally advanced breast cancer or MBC that had progressed
after treatment with an anthracycline, a taxane, and trastuzumab, the combination of lapatinib and capeci- tabine was associated with a numeric improvement in response rate compared with capecitabine alone (22% vs 14%, respectively; P = NS) and a significant in- crease in time to progression (6.2 vs 4.3 months; hazard ratio = 0.57; 95% CI, 0.43-0.77; P < 0.001). Lapatinib has been reported to have antitumor activi- ty in Phase II trials when used as first-line therapy for MBC, in patients with inflammatory breast cancer, and in patients with central nervous system metasta- ses. Phase II trials in other solid tumor types found modest activity. The approved dosing of lapatinib is 1250 mg PO QD given continuously in combination with capecitabine 2000 mg/m -~ daily administered in 2 divided doses on days i to 14 of a 21-day cycle. The most common clinical toxicities of all grades associ- ated with lapatinib used in combination with capeci- tabine in the pivotal clinical trial were diarrhea (65 %), hand-foot syndrome (53 %), nausea (44%), rash (29%), and fatigue (24%). Cardiac toxicity appears to be less frequent with lapatinib than with trastuzumab.
Conclusions: Lapatinib is a dual inhibitor of the EGFR and HER2 tyrosine kinases. It is approved by the FDA for use in combination with capecitabine for the treatment of HER2-positive MBC that has pro- gressed with standard treatment. In clinical trials, this combination was associated with a significant im- provement in the time to progression in patients with MBC. Lapatinib's efficacy in other malignancies that
Accepted for publication June 9, 2008. doi:l 0.1016/j.clinthera.2008.08.008 0149-2918/$32.00
© 2008 Excerpta Medica Inc. All rights reserved.
1426 Volume 30 Number 8

p.J. Medina and S. Goodin
overexpress EGFR and/or HER2 is under evaluation. (Clin Ther. 2008;30:1426-1447) © 2008 Excerpta Medica Inc.
Key words: lapatinib, GW572016, HER2, EGFR, dual-receptor inhibitor, pharmacokinetics, adverse events, clinical trials.
I N T R O D U C T I O N Breast cancer is the leading form of cancer and the second leading cause of cancer death in women in the United States. In 2007, there were an estimated 178,480 new cases and 40,460 deaths resulting from breast cancer in the United States.1 Although the ma- jority of diagnosed cases are local or regional, meta- static breast cancer (MBC) is present at the initial di- agnosis in -5% to 10% of patients. In addition, 10% to 20% of patients will have a recurrence after breast- conservation surgery plus radiation therapy, with up to 25% being locally extensive or metastatic at the time of recurrence, e Although advances in adjuvant therapy have decreased relapse rates, the treatment of metastatic disease, both at the initial diagnosis and after initial therapy, remains a significant challenge.
Approximately 25% of breast cancers diagnosed are human epidermal growth factor receptor 2 (HER2, or ErbB2) positive. 3 Compared with patients with non-HER2-positive tumors, patients with HER2- positive tumors have been reported to have more ag- gressive disease that is more often lymph-node posi- tive. HER2 overexpression has been reported to be a poor prognostic factor and a predictive risk factor for decreased disease-flee survival and overall survival (OS) in patients with breast cancer. 3,4 Trastuzumab was ap- proved in 1998 for the treatment of MBC and more recently for use in the adjuvant setting in patients whose tumors overexpress HER2. 5 Trastuzumab is a humanized immunoglobulin G antibody that targets the extracellular domain of the HER2 receptor. Al- though the exact mechanism of action is unknown, HER2 concentrations at the cellular level may be de- creased, preventing both homodimerization and het- erodimerization of HER2 receptors, thereby prevent- ing downstream signal transduction. 6 Unfortunately, trastuzumab is associated with both de novo and ac- quired resistance; therefore, there is a need for new agents that target the HER family of receptors through a different mechanism of action and have a different pharmacokinetic profile.
Lapatinib* was approved by the US Food and Drug Administration (FDA) on March 13, 2007, for use in combination with capecitabine in the treatment of patients with advanced breast cancer or MBC whose tumors overexpress HER2 and who have received previous therapy including an anthracycline, a taxane, and trastuzumab. On December 17, 2007, the Euro- pean Medicines Agency issued a positive opinion rec- ommending conditional marketing approval for lapatinib.
This article reviews the pharmacology, spectrum of activity, and pharmacokinetics of lapatinib; potential drug interactions; and the results of clinical trials evaluating the efficacy and tolerability of lapatinib in MBC. Because the HER family of receptors is involved in numerous malignancies in addition to breast cancer, including renal cell carcinoma, colon cancer, head and neck cancers, glioblastoma, and others, 6 clinical trials of lapatinib in other malignancies that overexpress HER2 and/or epidermal growth factor receptor (EGFR) are also reviewed.
M E T H O D S Relevant English-language literature was identified through searches of MEDLINE (1966-May 2008), the American Society of Clinical Oncology abstracts database (2000-2007), abstracts from the San Anto- nio Breast Cancer Symposium (2005-2007), and the FDA Web site (January 2008). Search terms included lapatinib, GW572016, HER2, EGFR, receptor tyro- sine kinase, dual-receptor blockade, adverse events, and clinical trials. Abstracts and posters presented at national and international scientific meetings were also reviewed. All identified clinical-trial data and presentations were reviewed, as were preclinical data that supported the clinical observations or were felt to be clinically relevant.
CHEMISTRY Lapatinib (GW572016) is a compound developed from the quinazoline core found in other ErbB ty- rosine kinase (TK) inhibitors. Its chemical name is N-{3-chloro-4-[(3-fluorobenzyl)oxy]-phenyl}-6-[5- ({ [2-(methyls ulfonyl)ethyl] amino }methyl)- 2-furyl]- 4-quinazolinamine. 7 Its molecular formula is C29H26CIFN404S, and its molecular weight is 581.06.
*Trademark: Tykerb ~ in the United States, Tyverb ~ in Europe (GlaxoSmithKline, Research Triangle Park, North Carolina).
August 2008 1427

Clinical Therapeutics
In humans, lapatinib is administered as the mono- hydrate ditosylate derivative(C29H26C1FN404S[CrH803S]2 H)O), which has a molecular weight of 943.5. 8 The structural formula of lapatinib ditosylate is shown in Figure 1.
MECHANISM O F A C T I O N The HER, or ErbB, family of receptors contains 4 known members, HER1, HER2, HER3, and HER4. 9 HER1 (also called EGFR) and HER2 are often over- expressed, or have increased activity, in breast, lung, and colon cancers, among others. <9 Although HER3 and HER4 are assumed to be involved in cancer growth and proliferation, their exact role is currently undefined.
Structurally, all members of the HER family contain 3 regions, an extracellular ligand binding site, a trans- membrane domain, and a TK tail. 9,1° Receptor di- merization is required for TK phosphorylation to occur, which in turn activates signal transduction. Dimeriza- tion can occur with a member of the same family, re- suiting in a homodimer, or with a member of a different subtype, resulting in a heterodimer. The type of dimer that is formed affects the downstream signal event; heterodimers of HER2 and EGFR lead to strong mito- genic signals and cellular proliferation when HER2 is overexpressed, whereas homodimers of the HER family may lead to weak or no signaling.ll When the HER2 gene is amplified, HER2 is overexpressed on the sur- face of breast cancer cells and is able to drive the growth of the malignancy through homodimerization.
The interaction between HER2 and EGFR provides a strong rationale for targeting both receptors of this signaling pathway, particularly in clinical circumstances in which HER2 is overexpressed.
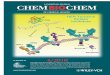
Lapatinib is an orally administered small-molecule inhibitor that targets both EGFR and HER2.1-),13 It targets the TK domain of these receptors by reversibly binding to the adenosine triphosphate binding site of the kinase. This interaction prevents the phosphory- lation and subsequent signal transduction of both the Ras/Raf mitogen-activated protein kinase and the phosphoinositol-3-kinase/Akt pathways, leading to an increase in apoptosis and decreased cellular prolifera- tion.i-),13 Figure 2 depicts the mechanism of action of lapatinib.
In addition to inhibiting wild-type HER receptors, lapatinib is able to inhibit truncated forms of these receptors. 14 Truncated forms of HER2 have been identified that lack the extracellular binding domain. These fragments, which may develop through shed- ding of the extracellular domain of the HER2 recep- tor, are collectively known as p95HER2 receptors. 14 They have been identified in MBC cell lines and have potent TK activity. In vitro and in vivo evidence sug- gests that lapatinib is able to reduce downstream phos- phorylation and to inhibit cell growth in cell lines transfected with p95HER2.14
SPECTRUM OF ACTIVITY In the United States, lapatinib is approved for use in patients with MBC whose tumors overexpress HER2. 8
o c
H3C - - S
II o o
Figure 1. Structural Formula of lapatinib ditosylate.
1428 Volume 30 Number 8

P.J. M e d i n a a n d S. G o o d i n
EGF TG F-e Amphiregulin 13-Cellulin HB-EGF Epiregulin
T
A
Extracellular
Heregulin No known NRG1 ligands
HER2 HER2 EGFR HER3 EGFR EGFR HER2 HER2 p95HER2 EGFR
I'I I'I I'F LapatinibxN~/p ~ P ' ' P LapatinibxN~/ ¢ ~ / / LapatinibN~,~/p ~p Lapatinib
S ~ PI3-K Ras ~ Raf-1 ~ ' ~
Akt M EK Intracellular
MAPK
Gene transcription Cell cycle progression Cell survival
Figure 2. Mechanism of action of lapatinib. Activation of human epidermal growth factor receptor (HER) 2 can occur through homodimerization or heterodimerization with another member of the HER family. On ligand binding to an epidermal growth factor receptor (EGFR) (eg, EGG transforming growth factor-(* [TGF-cx], amphiregulin) or HER3 (eg, heregulin, neuregulin 1 [NRG1]), HER2 forms a het- erodimer to activate downstream signaling. Lapatinib is a dual inhibitor of both EGFR and HER2 tyrosine kinases, inhibiting phosphorylation of the receptors and preventing downstream signal transduction of phosphoinositol-3-kinase (PI3-K) (cell survival) and Ras (cell proliferation). In addi- tion, lapatinib is active against truncated forms of HER2 (p95HER2). HB-EGF = heparin-binding EGF; PTEN = phosphatase and tensin homologue; Raf-1 = murine leukemia viral oncogene homologue 1; M EK = mitogen-activated protein kinase kinase; MAPK = mitogen-activated protein kinase.
However, EGFR and HER2 are implicated in the de- velopment and progression of many tumor types, sug- gesting that lapatinib may have a range of antitumor activity. 10
Early in vitro kinase assays indicated that lapatinib was highly selective for EGFR and HER2 enzymes, with 50% inhibitory concentrations (IC50) of 10.8 nmol/L and 9.2 nmol/L, respectively.15 The additional kinases tested were not inhibited until IC50 values reached >3500 nmol/L, with the exception of HER4, for which the IC50 was 367 nmol/L. The same investigative group examined the efficacy of lapatinib in cell lines over-
expressing EGFR and HER2. Growth of BT474 (breast), HN5 (head and neck), A-431 (vulva), CaLu-3 (lung), and N87 (gastric) cell lines was inhibited, with a mean IC50 <0.16 p.mol/L.16 Dose-dependent inhibi- tion of HN5 and BT474 tumor xenograft growth was also seen at doses of 30 and 100 mg/kg, both given twice daily, with complete inhibition of tumor growth at the higher dose. 16
Lapatinib's activity in breast cancer was further tested against a panel of 22 breast cancer cell lines hav- ing varying degrees of EGFR and HER2 expression. 17 Sensitivity to lapatinib was directly related to expres-
August 2008 1429

Clinical Therapeutics
sion of HER2 but not EGFR. Breast cancer cell lines containing HER2 gene amplification and increased HER2 expression were most sensitive to lapatinib's in- hibitory effects compared with EGFR-overexpressing cell lines (IC50 <1.0 vs 4.7-18.6 btmol/L, respective- ly). 17 Lapatinib was associated with dose- and time- dependent phosphorylation of EGFR, HER2, Akt, and ERK (extracellular signal-regulated kinases) in HER2- overexpressing breast cancer cell lines (BT474). 17
Lapatinib has also been reported to have activity against trastuzumab-resistant cells. In HER2-overexpressing cell lines conditioned with trastuzumab, lapatinib at concentrations of 5 btmol/L significantly inhibited tumor growth, as measured in terms of percent cell viability, compared with controls (P < 0.001); in the same cell line, trastuzumab did not have a signifi- cant effect on cell viability compared with controls. 17 The combination of lapatinib + trastuzumab was also reported to have synergistic activity in HER2- overexpressing cell lines, enhancing apoptosis of these cell lines. 17,18 The ability of lapatinib to inhibit trastuzumab-resistant cells may be a result of its abili- ty to inhibit p95HER2 receptors, as mentioned earlier, or its effects on insulinlike growth factor-1 (IGF-1) signaling. 14,19
IGF-1 signaling has recently been identified as a potential mechanism of resistance to trastuzumab, with the ability to signal downstream independently of the HER2 receptor.19 In trastuzumab-resistant SKBR3 cells, lapatinib decreased phosphorylation of EGFR and HER2, along with decreasing downstream sig- nals. 19 After the introduction of IGF-1, lapatinib at concentrations of i btmol/L inhibited IGF-l-stimulated phosphorylation of the IGF-1 receptor, blocked the cross-signaling and activation of HER2, inhibited cell growth, and induced apoptosis. 19 The cytotoxic ef- fects of lapatinib were increased when it was com- bined with c~IR3, a monoclonal antibody against the IGF-1 receptor. > In addition, elevated IGF-1 levels predicted a response to lapatinib in a subset of 15 pa- tients from a Phase I trial (N = 33). 12
Overexpression of both EGFR and HER2 has been associated with tamoxifen resistance. 2° Lapatinib has been reported to restore tamoxifen sensitivity in estro- gen receptor-positive, tamoxifen-resistant cell lines. Lapatinib + tamoxifen was associated with a 2.5- to 5-fold increase in p27 and a synergistic 5-fold de- crease in cyclin D 1 compared with either agent alone, leading to decreased cell-cycle progression in MCF-7
breast cancer cell lines. 21 This strategy is currently be- ing evaluated in clinical trials.
P HARMACO KI N ETICS Phase I trials evaluating the pharmacokinetics of la- patinib have been conducted in healthy volunteers as well as in adult and pediatric cancer patients. Single- dose studies may not accurately predict systemic ex- posure (AUC) or the tl/2 of lapatinib, as concentra- tions accumulate with multiple doses. 22 The relation- ship between concentration and response has not been adequately defined, but the incidence of diarrhea has been found to increase at higher doses, not at higher serum concentrations, suggesting that this adverse ef- fect was the result of unabsorbed drug. 23 The develop- ment of rash did not appear to be dose or serum relat- ed. 23 The pharmacokinetic properties of lapatinib are discussed in the following paragraphs and summa- rized in Table I.
Absorption Lapatinib was developed as an oral agent and has
no intravenous equivalent for assessment of its bio- availability. On administration of doses of 25, 100, or 175 mg for 8 days in 27 healthy men, oral absorption was delayed by -30 minutes and the Tma:~ was 3 to
Table I. Summary of the pharmacokinetic pa- rameters oflapatinib when administered at the doses approved by the US Food and Drug Administration. 8,23,24
Parameter Value
Absorption Tma x 3-4 h Cma x 2.43 I~g/m L AUC 36.2 I~g • h/mL
Distribution Vd/L >2200 L
Metabolism CYP3A4,* CYP3A5, CYP2C19, and CYP2C8
Elimination tl/2 Single dose 14.2 h Multiple doses 24 h
*Primary metabolic route.
1430 Volume 30 Number 8

P.J. Medina and S. Goodin
4 hours, ee Time-dependent increases in Cma x and AUC were detected at the higher doses (100 and 175 mg) but not at the lower dose.
Lapatinib has also exhibited delayed absorption in 67 patients with various advanced solid tumors, with Cm~ x occurring at 3 to 6 hours after administration and 2-fold accumulation at day 20. e3 Patients in this Phase I trial were assigned to 1 of 5 dosing cohorts for assessment of pharmacokinetics and toxicity. Concen- trations, including Cm~ x and AUC, increased with higher doses, although the effects were variable, pos- sibly as a result of food intake not being controlled on days 2 to 19. The median dose required to produce a Cmi n of 0.3 to 0.36 pg/mL (the m e a n Cmi n of respond- ers) was 900 mg. e3 This Cmi n w a s above concentra- tions required to exert antitumor effects in preclinical models, le
At the FDA-approved dose of 1250 mg/d, the steady-state Cm~ x and AUC were 2.43 t~g/mL and 36.2 t~g " h/mL, respectively.S, > Administering lapatinib in divided daily doses increased the steady-state AUC ~2-fold compared with the same total dose adminis- tered once daily. 8,e4 With multiple daily dosing of la- patinib, steady state was achieved within 6 to 7 days. 8 Systemic exposure to lapatinib was increased when the drug was administered with food, the greatest effect occurring with a high-fat meal. 8,e3-e5 The AUC was increased by 325% and 167% when taken with high- and low-fat meals, respectively, e3,e5 However, because clinical studies of lapatinib were performed with dosing on an empty stomach, it is recommended that the drug be taken in this way. 8
Distribution At concentrations of 1 btmol/L, lapatinib was highly
bound (>99%) to albumin and (*-1 acid glycoprotein. 8,> The results of in vitro studies have indicated that lapa- tinib is a substrate for and an inhibitor of P-glycoprotein (pgp).8 The volume of distribution (Vd/L) of the ter- minal phase of lapatinib was >2200 L, much greater than the volume of body water, indicating good drug distribution.S, 24
Metabolism The findings of in vitro studies indicate that lapa-
tinib is primarily metabolized to oxidated metabolites by the cytochrome P450 (CYP) 3A4, 3A5, 2C19, and 2C8 isozymes. 8,23,24 Approximately 70% of its me- tabolism is through CYP3A4. 24 No metabolite consti-
tutes >15% of recovered drug. One metabolite (GW690006) remains active against EGFR but not HER2, whereas other metabolites appear to be inactive. 24
Elimination Lapatinib is primarily eliminated hepatically, with
27% of an oral dose recovered in feces and <2% recov- ered in the urine. 8 The elimination tl/2 was 14.2 hours in single-dose studies 8 and ~24 hours with repeated dosing (as a result of drug accumulation). 8,24
Special Populations Lapatinib was administered at oral doses ranging
from 300 to 1150 mg/m 2 per dose BID in 34 pediatric patients with central nervous system (CNS) tumors. 26 Lapatinib Cma x occurred 3 to 4 hours after dosing, with a delay in absorption similar to that seen in adults. 23,26 The lapatinib AUC0_12 was linearly related to the ad- ministered dose after the second course of therapy, but not after the first. Clearance was not dose related but was related to dexamethasone coadministration and the course of therapy, with the second course of thera- py and dexamethasone both significantly decreasing lapatinib clearance (P < 0.005). After the second course of therapy, the elimination rate constant was 0.17 h -1, indicating a tl/2 of 4 hours, and the Vd/L was 65.6 L/m-). 8,-)6 These values did not differ significantly from those after the first course of lapatinib.
No publications were identified concerning the ef- fects of sex, race, ethnicity, or age on the pharmaco- kinetics of lapatinib. In patients with severe hepatic dysfunction (Child-Pugh class C), the AUC of lapa- tinib was increased by >60% and the tl/2 was ~3 times that in individuals without hepatic dysfunction. 8,24 Dose reductions to 750 mg/d are recommended in this patient population. 8 The effect of renal dysfunction on the pharmacokinetics of lapatinib is currently un- known, but is expected to be minimal based on the limited renal elimination of lapatinib.
DRUG INTERACTIONS Lapatinib is a major substrate for and inhibitor of CYP3A4 and an inhibitor of CYP2C8. In healthy vol- unteers receiving ketoconazole, a CYP3A4 inhibitor, the AUC of lapatinib was increased 3.6-fold relative to control, and the tl/2 increased 1.7-fold relative to control, s,> In contrast, carbamazepine, a CYP3A4 inducer, decreased the AUC of lapatinib by ~75%. 8'24
August 2008 1431

Clinical Therapeutics
Few data were found on the use of lapatinib and other CYP inducers or inhibitors, although similar interac- tions may be expected. The package insert recommends avoidance of strong CYP3A4 inhibitors (eg, azole an- tifungals, clarithromycin, HIV medications [eg, indi- navir], and grapefruit), s If coadministration of a strong CYP3A4 inhibitor is necessary, reduction of the lapatinib dose to 500 mg/d is predicted to adjust the lapatinib AUC within the target range, s If the strong CYP3A4 inhibitor is discontinued, a washout period of -1 week should be allowed before adjusting the lapatinib regimen to the indicated dose. Similarly, strong CYP3A4 inducers (eg, dexamethasone, pheny- toin, carbamazepine, rifampin, phenobarbital, St. John's wort) should be avoided in patients taking lapatinib. In patients receiving a strong CYP3A4 in- ducer in combination with lapatinib, the lapatinib dose should be titrated gradually from 1250 up to 4500 mg/d based on tolerability, s
Limited data regarding drug interactions with lapa- tinib and other anticancer agents were identified by the literature search. In a Phase I trial of lapatinib in com- bination with FOLFIRI (folinic acid, 5-fluorouracil, and irinotecan), the AUC of SN-38, the active metabo- lite of irinotecan, was increased by - 4 0 % . 27 No other notable interactions occurred. A Phase I trial of lapa- tinib + paclitaxel reported 21% and 23% increases in the AUCs of lapatinib and paclitaxel, respectively. -)8 Pharmacokinetic studies of lapatinib in combination with docetaxel, capecitabine, letrozole, and FOLFOX (folinic acid, 5-fluorouracil, and oxaliplatin) reported no significant interactions. -)8-31 Based on preclinical data indicating synergy between the 2 agents, the com- bination of lapatinib + trastuzumab was studied in a Phase I dose-escalation trial in 54 patients with ad- vanced breast cancer. 3-) No pharmacokinetic interac- tion was observed between the 2 agents; however, the optimally tolerated dose of lapatinib was 1000 mg/d with standard-dose trastuzumab.
Lapatinib has been reported to inhibit Pgp, which may increase concentrations of Pgp substrates (eg, anthracyclines, taxanes, vinca alkaloids). 8,-)4 No for- mal pharmacokinetic studies of this interaction have been published, but care may be warranted when coadministering lapatinib with substrates of Pgp.
CLI NICAL EFFICACY Lapatinib has been evaluated in Phase II and III trials in various forms of breast cancer (MBC, 33~1 inflam-
matory breast cancer [IBC], 42,43 and breast cancer with CNS metastases 44~6) (Table II). Because of its dual-receptor activity at HER2 and EGFR, lapatinib also has been evaluated in a number of other tumor types in which EGFR plays a role, including Phase II trials in non-small cell lung c a n c e r ( N S C L C ) , 47 malig- nant tumors of the salivary glands, 48 biliary tree and hepatocellular cancer, 49 squamous cell carcinoma of the head and neck, s° hormone-sensitive prostate can- cer,51 gastric cancer, 52 metastatic colorectal cancer, 53 and transitional cell carcinoma of the urothehum, ~ " ~4 and a Phase III trial in advanced renal cell carcinoma 55 (Table III). Most Phase II trials involved lapatinib monotherapy; the majority of data from these trials is available in abstract form only, and no statistical analyses were performed.
M e t a s t a t i c Breas t Cancer Evidence for the efficacy of lapatinib in MBC was
derived from trials of monotherapy and combination therapy involving patients with trastuzumab-refractory MBC; patients with MBC refractory to an anthracy- cline, a taxane, capecitabine, and trastuzumab; and as first-line therapy for MBC.
Monotherapy Burstein et a133 reported on a multinational, open-
label Phase II trial of the efficacy and tolerability of lapatinib monotherapy in patients with advanced or refractory MBC who had previously been treated with an anthracycline, a taxane, capecitabine, and (in HER2-positive tumors only) trastuzumab. The study involved 2 cohorts: cohort A enrolled 140 patients with tumors that overexpressed HER2 (HER2 posi- tive), defined as either 3+ on immunohistochemistry (IHC), or 2+ on IHC and HER2 amplified or positive on fluorescent in situ hybridization (FISH); cohort B enrolled 89 patients with tumors that did not overex- press HER2 (HER2 negative). The majority (76%) of patients had received >4 previous lines of therapy, and 95% had stage IV disease at study entry. The median trastuzumab exposure in patients with HER2-positive tumors was 76 weeks, and most patients (97%) had received >12 weeks of previous trastuzumab therapy. Patients in each cohort received oral lapatinib 1500 mg QD at least 1 hour before or after the morning meal. According to the response evaluation criteria in solid tumors (RECIST), 56 no objective responses occurred in any of the patients with HER2-negative tumors in
1432 Volume 30 Number 8

P.J. Medina and S. Goodin
Table II. Clinical trials o f lapatinib in patients with advanced or metastatic breast cancer (M BC).
No. of Treatment Authors Patient Population Patients Regimens
Burstein et a133 Cohort A: HER2-posiuve 140 Lapaunib Phase II, MBC refractory to an 1500 mg QD international, anthracycline, a taxane, OL capecitabine, and
trastuzumab
Cohort B: HER2-negauve 89 MBC refractory to an anthracycline, a taxane, and capecitabine
Lapatinib 1500 mg QD
Response
RR: 4.3%~; clinical benefid: 5.7%; median TTP: 9.1 wk; median PFS: 9.1 wk; median survival: 29.4 wk
No objective responses; median TTP: Z6 wk; median PFS: Z6 wk; median survival: 18.6 wk
Blackwell et a134 HER2-posiuve MBC 78 Lapaunib Phase II, refractory to 1500 mg QD MC, OL trastuzumab
PR: 7.7%; clinical benefitt: 21.8%
Iwata et al 3s HER2-positive MBC 45 Lapatinib Phase II, refractory to an 1500 mg QD MC, OL anthracycline, a taxane,
capecitabine, and trastuzumab
Clinical benefitf: 33.3%
Gomez et a136 Phase II, MC, R, OL
First-line treatment of HER2-posiuve advanced breast cancer or MBC
138 Lapatinib 1500 mg QD (n = 69) o r
Lapat in ib 500 mg BID (n = 69)
RR: 24%; clinical benefid: 31%; PFS at 6 mo: 43%~ no difference in clinical activity between doses
Geyer et a137 39 and Cameron el: al 4°
Phase III, MC, R, OL
HER2-posiuve locally advanced breast cancer or MBC that had progressed with regimens including an anthracycline, a taxane, and trastuzumab
399 Lapaunib 1250 mg QD + capeckabine 1000 mg/m 2 PO BID on days 1-14 of a 21-day cycle OF
Capecitabine 1250 mg/m 2 PO BID on days 1-14 of a 21-day cycle
Median TTP: 6.2 mo (combination) vs 4.3 mo (capecitabine alone) (HR = 0.57~ 95% CI, 0.43-0.77~ P < 0.001)~ improved PFS with combination vs capeckabine alone (HR = 0.55; 95% CI, 0.4-0.74~ P < 0.001)
Di Leo et a141 Phase III, MC, R, DB, PC
First-line therapy o f HER2-negauve or unknown advanced breast cancer or MBC
580 Lapadnib 1500 mg QD + paclitaxel 175 mg/m 2 IV q3wk OF
Placebo + paclitaxel 175 mg/m 2 IV q3wk
RR: 35.1% vs 25.3%, combination vs paclitaxel monotherapy, respectively (P = 0.008)~ clinical benefitf: 40.5% vs 31.9% (P = 0.025)~ no difference in TTP or OS
(continued)
August 2008 1433

Clinical Therapeutics
Table II (continued).
Authors
Johnston et a142 Phase II, MC, OL
Cristofanil l i et a143 Phase II, MC, OL
L inet a144
Phase II, MC, OL
L inet al 4s
Phase II, MC, OL
Patient Population
ErbB2-positive (cohort A) or ErbB2-negative (cohort B) recurrent or refractory I BC
Newly diagnosed IBC
HER2-positive MBC with CNS metastases
No. of Patients
Cohort A: 30 Cohort B: 15
ErbB2 positive: 21 ErbB2 negative: 2
39
Treatment Regimens
Lapatinib 1500 mg QD
Neoadjuvant lapatinib 1500 mg QD + paclitaxel 80 mg/m 2 IV qwk for 12 wk
Lapatinib 750 mg BID
Response
Cohort A: 2 CRs, 13 PRs; cohort B: 1 PR
Clinical response: ErbB2 positive, 95%; ErbB2 negative, 100%; pathologic response: not reported
PR: 2.6%
Lapatinib 750 mg BID
HER2-positive MBC 241 with CNS metastases and previous CNS radiotherapy
Lin et a146 Extension o f previous 51 Lapatinib + PR: 20%; SD >8 wk: Phase II, study 4s in patients capecitabine 35%; median PFS: MC, OL whose disease 15.8 wk
progressed during lapat inib monotherapy
PR: 6%; SD >8 wk: 42%; median PFS: 15.1 wk; PFS at 6 mo: 22%
OL = open label; HER2 = epidermal growth factor receptor 2 (ErbB2); RR = response rate (complete response [CR] + partial response [PR]); TTP = time to progression; PFS = progression-free survival; MC = multicenter; R = randomized; HR = hazard ratio; DB = double blind; PC = placebo controlled; OS = overall survival; IBC = inflammatory breast cancer; CNS = central nervous system; SD = stable disease. *As determined by investigators' assessment. fCR, PR, and SD _>24 weeks. t PR and SD _>16 weeks.
cohort B. In HER2-positive patients, there were 3 par- tial responses (PRs) and 3 complete responses (CRs), for a response rate of 4.3% by the investigators' as- sessment or 1.4% (2 PRs) by independent review. 33 All responders according to the investigators' assess- ment exhibited HER2 overexpression of 3+ by IHC, and 5 of the 6 responders were HER2 amplified by FISH. A clinical benefit (CR, PR, + stable disease [SD] >24 weeks) occurred in 5.7% of HER2-positive pa- tients according to both the investigators' and inde- pendent reviews. The median time to progression (TTP) and median progression-free survival (PFS) were both 9.1 weeks in HER2-positive patients and 7.6 weeks in
HER2-negative patients by independent review; me- dian survival was 29.4 weeks in HER2-positive pa- tients and 18.6 weeks in HER2-negative patients.
A planned interim analysis of a similar open-label, Phase II trial of lapatinib monotherapy in 78 HER2- positive patients with refractory MBC found a clinical benefit rate (PR + SD >16 weeks) of 21.8%. 34 Simi- larly, preliminary results from an open-label, Phase II trial conducted in Japan in 45 patients with HER2- overexpressing MBC refractory to an anthracycline, a taxane, capecitabine, and trastuzumab indicated a clinical benefit (CR, PR, + SD >24 weeks) of 33.3%. 35 Collectively, these studies support the activity of lapa-
1434 Volume 30 Number 8

P.J. Medina and S. Goodin
Table III. Clinical trials of lapat in ib for solid tumors other than breast cancer.
No. of Treatment Authors Patient Population Patients Regimen Response
Smylie el: a147 First- or second-line treatment 131 Lapal:inib 1500 mg Phase II, of advanced or metastatic QD MC, R, OL NSCLC with BAC or no or
smoking history (target Lapal:inib 500 mg population: n = 56) or no BAC BID or a smoking history (nonl:argel: population: n = 75)
Malignant salivary gland cancer 36 Agulnik el: a148 Phase II, MC, OL
Ramanal:han el: a149 Phase II, MC, OL
Abidoye el: al so Phase II, MC, OL
Sridhar el: a151 Phase II, MC, OL
lqbal el: al s2 Phase II, OL
Fields el: al s3 Phase II, MC, OL
WOlfing el: al g4 Phase II, MC, OL
Ravaud et al ss
Phase III, MC, R, OL
Biliary tree cancer 17
Hepatocellular carcinoma
Head and neck cancer with (arm A) and without (arm B) previous exposure to an EGFR inhibitor
37
42
Hormone-sensitive prostate 23 cancer, no previous hormonal therapy, corticosteroid therapy, or chemotherapy
First-line treatment of advanced 47 or metastatic gastric cancer
Lapatinib 1500 mg QD
Lapatinib 1500 mg QD
Lapatinib 1500 mg QD
Lapatinib 1500 mg QD
Lapatinib 1500 mg QD
Lapatinib 1500 mg QD
Target population: PR, 2%; SD _>24 wk, 25% Nontarget population: PR, 1%; SD _>24 wk, 37%
No objective responses; SD _>6 mo: 36%
No PRs; SD: 29%; median PFS: 1.8 mo; median OS: 5.2 mo
PR: 5%; SD: 35%; median PFS: 2.3 mo; median OS: 6.2 mo
No objective responses; SD: 37% (arm A) and 20% (arm B)
No responses
PR: 7%; SD: 20%
Second-line treatment of metastatic colorectal cancer
86 Lapatinib 1250 mg PR: 1% QD
Second-line treatment of locally 59 advanced or metastatic transitional cell carcinoma of the urothelium
Advanced renal cell carcinoma 416
Lapatinib 1250 mg QD
PR: 2%; SD: 31%; median TI-P: 8.6 wk; median OS: 1Z9 wk
Lapatanib 1250 mg QD o r
Hormonal therapy (tamoxifen or megestrol acetate)
TTP: 15.3 wk (lapatinib) vs 15.4 wk (hormonal therapy) (P = NS); OS: 46.9 vs 43.1 wk, respectively (P = NS)
MC = multicenter; R = randomized; OL = open label; NSCLC = non-small cell lung cancer; BAC = bronchioloalveolar carcinoma; PR = partial response; SD = stable disease; PFS = progression-flee survival; OS = overall survival; EGFR = epidermal growth factor receptor; TTP = time to progression.
August 2008 1435

Clinical Therapeutics
tinib monotherapy in this heavily pretreated popula- tion that had progressed with previous trastuzumab- containing regimens.
Gomez et a136 reported the results of an interna- tional, randomized, open-label Phase II study of lapa- tinib monotherapy as first-line treatment in patients with HER2-positive advanced breast cancer or MBC. Patients were randomized to receive oral lapatinib ei- ther as 1500 mg QD (n = 69) or 500 mg BID (n = 69). Patients had a median age of 53 years and an Eastern Cooperative Oncology Group (ECOG) performance status of 0 (33%) or 1 (67%). The majority of patients (76%) had estrogen receptor- and progesterone receptor-negative tumors. Overall, there was a 24% response rate (CR + PR) and a clinical benefit (CR, PR, + SD >24 weeks) of 31%, with no significant dif- ferences in these outcomes between treatment groups. Most responses (32/33) occurred by week 12, with a median time to response of 7.9 weeks. The responses were durable, with a median duration of response of 28.4 weeks and a 6-month PFS of 43%. The re- sponse rate to lapatinib monotherapy administered as either 1500 mg QD or 500 mg BID in the first-line setting in this trial was comparable to historical data for trastuzumab in the first-line treatment of HER2- overexpressing MBC. 57
In this trial, the biomarkers ErbB1-4, PTEN (phos- phatase and tensin homologue), and c-myc were evalu- ated as predictors of response in patient tumor blocks. 58 For the first 65 blocks analyzed, an elevation in HER2 expression was significantly associated with a response to lapatinib treatment (P = 0.02) and with clinical benefit (P < 0.01). These data support further investi- gation of lapatinib as first-line treatment for MBC with HER2 overexpression.
Combination Therapy Lapatinib's efficacy in the monotherapy trials led
to its evaluation in combination with capecitabine in HER2-positive MBC that was refractory to regimens including an anthracycline, a taxane, and trastuzu- mab, and in combination with paclitaxel as first-line treatment for HER2-negative or unknown MBC.
Lapatinib was approved by the FDA based on the interim results of a randomized, open-label, Phase III trial for 324 women with HER2-positive (3+ by IHC or 2+ by IHC and amplified by FISH), locally ad- vanced breast cancer or MBC that had progressed after treatment with regimens that included an an-
thracycline, a taxane, and trastuzumab. 8,37 Patients were randomly assigned in a 1:1 ratio to receive oral lapatinib 1250 mg QD on an ongoing basis and oral capecitabine 2000 mg/m -) given in 2 divided doses on days 1 through 14 of a 21-day cycle, or monotherapy with capecitabine 2500 mg/m -) given in 2 divided doses on days 1 through 14 of a 21-day cycle. The primary end point, TTP, was defined as the time from randomization to tumor progression or death related to breast cancer.
Geyer et a137 performed a prespecified interim analy- sis after the occurrence of 146 investigator-reported disease-progression events. After data validation, analy- sis of the primary end point by an independent data safety and monitoring committee included 121 disease- progression events. The baseline characteristics of the combination lapatinib + capecitabine and capecita- bine monotherapy groups were well balanced, with a median age of 54 and 51 years, respectively; an ECOG performance status of 0 in 59% and 55%; hormone receptor (estrogen and progesterone) negativity in 49% and 50%; metastatic disease in 96% each; and a me- dian duration of previous trastuzumab therapy of 42 and 44 weeks.
After independent review, the interim analysis of TTP met the prespecified criteria for early reporting based on the superiority of lapatinib + capecitabine relative to capecitabine monotherapy. 37 There were 49 disease-progression events in the combination- therapy group and 72 in the monotherapy group, and the median TTP was 8.4 and 4.4 months, respectively. The hazard ratio (HR) for TTP with combination therapy was 0.49 (95% CI, 0.34-0.71; P < 0.001). Combination therapy was also associated with a nu- merically, but not statistically significantly, higher re- sponse rate (22% vs 14%). Because the interval since the last exposure to trastuzumab differed between patients, persistent levels of trastuzumab may have enhanced the activity of lapatinib. However, a planned exploratory analysis found that the interval between administration of trastuzumab and randomization had no effect on TTP in either treatment group. 38 At the time of the interim analysis, there were no differ- ences in OS between groups, and 22% of patients in both groups had died.
In an update of efficacy data and biomarker analy- ses from the preceding pivotal Phase III trial, 399 wom- en had been randomized to treatment at the time of accrual closure by the independent data and safety
1436 Volume 30 Number 8

p.J. Medina and S. Goodin
monitoring committee. 39,4° The updated analysis in- cluded 82 disease-progression events with the combi- nation of lapatinib + capecitabine and 102 events with capecitabine monotherapy. 4° Baseline characteristics and the median duration of previous trastuzumab therapy remained balanced in the 2 groups after the accrual of an additional 75 patients. The median TTP for combination therapy was 6.2 months, compared with 4.3 months for capecitabine alone (HR = 0.57; 95% CI, 0.43-0.77; P < 0.001), indicating a 43% re- duction in the relative risk of progression with the addition of lapatinib to capecitabine. Similarly, there was an improvement in PFS (HR = 0.55; 95% CI, 0.40- 0.74; P < 0.001), indicating a 45% relative risk reduc- tion in PFS with combination therapy. There were no associations between PFS and any of the clinical char- acteristics of visceral disease, the number of metastatic sites, hormone-receptor positivity, or the duration of previous trastuzumab treatment. Although there was a reported improvement in OS with combination therapy (HR = 0.78), the difference did not reach sta- tistical significance. An exploratory analysis found fewer cases with CNS involvement at first progression in the combination-therapy group compared with the monotherapy group (4 vs 13, respectively; P = 0.045). Exploratory analyses of biomarkers for PFS in 241 pa- tients with centrally confirmed eligible HER2 status found that increased levels of circulating extracellular- domain HER2 predicted a benefit from combination therapy relative to capecitabine alone (HR = 0.45; 95% CI, 0.31-0.65; P < 0.001). The results of this trial support continuing development of lapatinib as a component of combination therapy and investigation in early-stage breast cancer.
In a Phase III, multicenter, randomized, double- blind, placebo-controlled trial of first-line treatment for untested or HER2-negative advanced breast cancer or MBC, 41 580 patients were randomized in a 1:1 ratio to receive oral lapatinib 1500 mg QD + paclitaxel 175 mg/ m -) q3wk, or placebo + paclitaxel 175 mg/m -) q3wk. No patients had received previous trastuzumab therapy, 87% presented with metastatic disease, and 55% had received previous adjuvant chemotherapy or hormonal therapy. At the time of data analysis, 97% (561) of patients had progression or withdrew from the study. In an intent-to-treat analysis of investigators' assess- ments, there was a significantly higher response rate (CR + PR) in the HER2 untested or unknown popula- tion with combination therapy compared with pacli-
taxel monotherapy (35.1% vs 25.3%, respectively; P = 0.008). Similarly, the rate of clinical benefit at 6 months was significantly higher with combination therapy than with monotherapy (40.5% vs 31.9%; P = 0.025), but there were no significant differences in the median duration of response, TTP, or OS. After centralized HER2 testing by IHC or FISH, 19% (52) of the combination group and 15% (39) of the mono- therapy group had confirmed HER2-positive disease. On analysis by HER2 status, patients with HER2- positive disease who received combination therapy had significant improvements versus monotherapy with respect to response rate (60% vs 36%; P = 0.027); median duration of response (7.4 vs 5.5 months; P = NS); and median TTP (6.1 vs 5.8 months; P = 0.011). Although dual inhibition was hypothesized to have an effect in HER2-negative disease, combination therapy did not achieve the primary end point of a significant improvement in TTP compared with monotherapy in the HER2-untested population (6.7 vs 5.3 months). However, the results in patients with HER2-positive disease were encouraging, and ongoing trials by this investigative group are evaluating lapatinib in combi- nation with weekly paclitaxel in HER2-positive ad- vanced breast cancer.
Inflammatory Breast Cancer Results from preclinical studies and the response
rate (3 PRs and 1 CR) in a Phase I study of lapatinib in 5 heavily pretreated patients with IBC 23 led to the evaluation of lapatinib monotherapy in patients with recurrent or refractory IBC. Johnston et a142 reported the final results of a multicenter, open-label, Phase II study of oral lapatinib 1500 mg QD in 2 patient cohorts---cohort A included 30 patients with tumors that were HER2 positive (IHC 2+/3+ or FISH posi- tive), and cohort B included 15 patients with tumors that were IHC 1+ for HER2 overexpression or did not overexpress HER2. This patient population was heavily pretreated, with a median of 4 and 3 previous chemotherapy regimens in cohorts A and B, respec- tively, 86% and 80% of whom had received previous therapy with an anthracycline. In cohort A, 50% of patients had previously received trastuzumab. The study population had a median age of 54 years, and dermal lymphatic invasion was present in the majority of tumor biopsies in cohorts A and B (73% and 80 % ). In cohort A, 50 % (15) o f patients had a clinical response in the skin and/or in measurable disease
August 2008 1437

Clinical Therapeutics
(RECIST). With respect to the best clinical response in individual patients, there were 2 CRs and 13 PRs in the chest wall/skin or by RECIST, with all responses in the skin occurring in the first 4 weeks. The median dura- tion of overall response in cohort A was 16.9 weeks (range, 8-31.7 weeks at the time of the evaluation), and the median PFS was 14 weeks (95% CI, 15-32). In cohort B, only 1 patient had a clinical response (PR), and this cohort was subsequently closed. An evaluation of biomarkers in clinical responders in co- hort A found that 67% were PTEN deficient and 83% were positive for IGF-1R42, both of which have been associated with resistance to trastuzumab monothera- py in small studies. 59 Phosphorylated HER3 expression and lack of p53 expression were significantly associ- ated with response (P < 0.05 by multivariate analysis; P = 0.021 and 0.033, respectively, by univariate analy- sis). These biomarker analyses suggested the possibili- ty of a lack of cross-resistance with trastuzumab, but this requires evaluation in larger clinical trials.
Preliminary data from an open-label, Phase II study in 23 patients with newly diagnosed IBC indicated that the neoadjuvant combination of oral lapatinib 1500 mg QD and paclitaxel 80 mg/m 2 IV weekly for 12 weeks was associated with a 95% (20/21) clinical response in patients with ErbB2-overexpressing tu- mors and a 100% (2/2) response in patients with ErbB1- positive/ErbB2-nonoverexpressing tumors. 43 Accord- ing to the preliminary data from this small study, lapatinib was clinically active neoadjuvantly in these heavily pretreated patients with IBC, the most aggres- sive and lethal form of breast cancer.
Breast Cancer with Central Nervous System Metastases
CNS metastases represent a challenge in the man- agement of patients with MBC, and there is no con- sensus on what medical therapy to offer patients whose CNS metastases have progressed after radiotherapy. Although both stereotactic radiosurgery and whole- brain radiotherapy (WBRT) are effective palliatively, death may occur in these patients due to progressive disease within the CNS. 6° Unlike trastuzumab, lapa- tinib is a small molecule that is hypothesized to cross the blood-brain barrier and, therefore, may have clini- cal activity in brain metastases. 61
In an open-label, Phase II trial, Lin et a144 evaluated oral lapatinib at a starting dose of 750 mg BID in 4-week cycles in patients with HER2-positive breast
cancer and new or progressive brain metastases. All 39 patients had developed brain metastases while re- ceiving trastuzumab (median of 2 previous trastuzumab- containing chemotherapy regimens), and 37 had progres- sion after radiation, with a median time of 5.9 months from the last radiation to study entry. There was 1 PR, constituting an objective response rate (RECIST) of 2.6%, which did not achieve the prespecified level of activity. Sixteen patients had measurable non-CNS dis- ease and 4 achieved a PR in non-CNS sites. The me- dian TTP was 3 months (95% CI, 2.3-3.7); in the 1 patient with a CNS objective response, the TTP was 11.3 months. Although the data were exploratory, there was some evidence of clinical benefit, with 7 pa- tients free of progression in both CNS and non-CNS sites at 16 weeks and 3 patients with CNS volumetric declines of >30%. Based on the volumetric results from this study, exploration of lapatinib in HER2- positive CNS disease is continuing.
To further characterize the activity of oral lapatinib 750 mg BID in patients with HER2-positive breast cancer with metastatic CNS disease, the same investi- gative group conducted a larger trial with a design and eligibility criteria similar to those in the previous trial, except that patients must have received pre- vious radiotherapy to the eNg. 45 Instead of using the RECIST criteria, response was defined as a volumetric reduction of CNS lesions (by 50% for a PR) in the absence of new lesions, need for an increased dose of steroids, progressive neurologic signs/symptoms, or progressive extra-CNS disease. The 241 patients in this study had a median age of 49 years and an ECOG performance status of 0 (25%), 1 (44%), or 2 (31%); 87% had concurrent non-CNS disease. Patients had been heavily pretreated, with 88% having received >3 chemotherapy regimens, 44% having received >3 trastuzumab + chemotherapy regimens, and 73% having received WBRT. Using the CNS composite cri- teria, a PR was reported in 6% (15) of patients, and 42% (102) of patients had SD of >8 weeks. CNS volu- metric reductions of >50% occurred in 7% of pa- tients. The median PFS for all patients was 15.1 weeks, and the 6-month rate of PFS was 22%. Among CNS responders, the median PFS was longer than in non- responders (25.3 vs 15.3 weeks, respectively).
An extension of this trial was conducted in patients with either CNS or non-CNS disease that progressed radiographically during lapatinib monotherapy. 45,46 These patients were treated with lapatinib + capecita-
1438 Volume 30 Number 8

p.J. Medina and S. Goodin
bine at the FDA-approved combination doses. Results have been reported for 51 patients, of whom 20% (10) had a PR (volumetric reduction of >50% in the CNS), and 35% (18) had SD (volumetric reduction of >20% in the CNS). 46 Median PFS was 15.8 weeks. Although, as in the previous trial, lapatinib did not achieve the target response rate, it had modest but durable activi- ty in the management of CNS metastases. Preliminary data from the extension study suggest a potential for improved responses with lapatinib combined with other agents in this patient population. Ongoing trials of lapatinib + capecitabine or topotecan and lapatinib + radiotherapy should provide further insight into the role of lapatinib in the management of this difficult- to-treat population.
Other Malignancies Non-Small Cell Lung Cancer
Smylie et a147 presented the results of a Phase II, multicenter, randomized, open-label trial comparing oral lapatinib 1500 mg QD with lapatinib 500 mg BID as first- or second-line therapy in 2 populations of patients with advanced or metastatic NSCLC: those with bronchioloalveolar carcinoma (BAC) or no smok- ing history (target population), and patients who did not have BAC or had a smoking history (nontarget population). Efficacy was assessed in these 2 popula- tions, and tissue was analyzed for mutations and/or amplifications. Of the 131 patients in this trial, 56% were female, and the median age was 66 years; 20% had BAC and 71% did not have BAC. The majority (70%) were current or former smokers and were pre- viously untreated (99%). There were 56 patients in the target population and 75 in the nontarget popula- tion. There were no CRs in either population. In the target population, there was 1 (2%) PR and 14 (25%) patients had SD _>24 weeks. In the nontarget popula- tion, there was 1 (1%) PR and 28 (37%) patients had SD _>24 weeks. There were no responses in patients with ErbB1 mutations or those who harbored EGFR copy increases. There were no mutations in HER2, and 2 tumors harbored HER2 copy number increases. With a median treatment duration of 9.1 weeks, there were no notable differences in efficacy or toxicity in the once-daily versus the twice-daily regimen.
In this study, lapatinib's dual inhibition of EGFR and HER2 did not appear to be associated with any benefits in NSCLC. The prevalence of mutations in EGFR and HER2 in this population was lower than
has been reported in larger trials; therefore, it is not possible to determine lapatinib's activity in patients with these mutations.
Malignant Tumors of the Salivary Glands Agulnik et a148 evaluated patients with progressive,
recurrent, or metastatic adenoid cystic carcinoma (ACC) and non-ACC malignant salivary gland tumors in a multicenter, open-label, Phase II trial of oral lapatinib 1500 mg QD. There were no objective responses among the 36 evaluable patients, although SD >6 months was documented in 13 (36%) patients. Before initiating therapy, these patients had a mean TTP of 3 months. Over a median follow-up of 15.8 months, PFS was 3.4 months.
Results from correlative studies of EGFR or ErbB2 expression in this trial suggested greater therapeutic effect in patients with non-ACC when there was a high degree of marker expression, 48 but this requires further testing. Although there were no objective re- sponses documented in the previous study, stabiliza- tion of disease in a group of patients with progressive disease at enrollment is clinically relevant, supporting the cytostatic activity of lapatinib in patients with malignant salivary gland tumors.
Biliary Tree and Hepatocellular Cancer Ramanathan et a149 presented the findings of a
multicenter, open-label, Phase II trial of oral lapati- nib 1500 mg QD given continuously in patients with advanced biliary tree cancer (BTC) or hepatocellular carcinoma (HCC). This study, which employed a 2-stage design allowing for early termination at the first stage if treatment was not effective, enrolled 17 pa- tients with BTC (5 gallbladder, 9 intrahepatic, and 3 extrahepatic tumors) and 37 patients with HCC. The median age of the population was 62 years, and the majority of patients were male (63%) and white (68 %), with an ECOG performance status of 0 (46%), 1 (42%), or 2 (12%). Patients had Child-Pugh class A hepatic impairment, and 65% and 43% of BTC and HCC patients, respectively, had received 1 previous drug therapy. Only 1 stage of BTC patients was ac- crued, as there were no PRs, and 5 (29%) patients had SD. In patients with BTC, PFS was 1.8 months (95% CI, 1.7-5.2), with an OS of 5.2 months. Among pa- tients with HCC, there were 2 (5%) PRs and 13 (35%) patients with SD, which was associated with a median PFS of 2.3 months (95% CI, 1.7-5.6) and a
August 2008 1439

Clinical Therapeutics
median OS of 6.2 months. Of the 2 PRs, 1 patient had received no previous therapy and 1 had received trans- catheter arterial chemoembolization. Skin rash of any grade occurred in 20 patients receiving lapatinib. Skin rash may have been correlated with efficacy, as the probability of PFS and OS was significantly cor- related with the occurrence of rash, similar to reports from other trials involving EGFR inhibitors. 62 Pa- tients with rash had a PFS of 5 months, compared with 2 months in patients with no rash (P = 0.03); similarly, rash was associated with OS of 10 months, compared with 5 months in patients without rash (P = 0.004).
Although lapatinib was inactive in these patients with BTC and did not the meet study definition of a response in patients with HCC, its activity in HCC may be promising. However, evaluation of lapatinib in HCC is limited by the lack of available molecular markers that may be correlated with activity.
Squamous Cell Carcinoma of the Head and Neck Because EGFR inhibitors have reported activity in
patients with recurrent and metastatic squamous cell carcinoma of the head and neck, Abidoye et al 5° evaluated the effects of oral lapatinib 1500 nag QD in 2 groups, patients without previous exposure to an EGFR inhibitor (arm A) and patients with previous exposure (arm B). In the 42 evaluable patients, no objective responses were observed in either cohort. In an intent-to-treat analysis, SD was observed in 37% of patients in arm A and 20% of patients in arm B. Lapatinib appeared to have little clinical activity as a single agent in patients with squamous cell carcinoma of the head and neck who were EGFR-inhibitor naive or who had refractory disease.
Hormone-Sensitive Prostate Cancer In a multicenter, open-label, Phase II trial presented
by Sridhar et al, 51 23 patients with hormone-sensitive prostate cancer who had received no previous hor- monal therapy, corticosteroid therapy, or chemothera- py were treated with oral lapatinib 1500 nag QD. Patients had a median age of 67 years and a me- dian baseline prostate-specific antigen (PSA) level of 7.5 ng/mL; 96% had an ECOG performance status of 0. There were no PSA responses in the 17 patients who had completed treatment at the time of report- ing; the median TTP was 4.6 months, with a 6-month PFS estimate of 49%. Although only preliminary data
were reported, lapatinib monotherapy did not appear to be effective in these patients with hormone-sensitive prostate cancer.
Gastric Cancer Iqbal et a152 presented the results of an open-label,
Phase II trial of oral lapatinib 1500 nag QD as first- line therapy in 46 patients with advanced or meta- static gastric cancer. Men accounted for 65% of ac- crued patients, and the median age was 68.7 years. There were 3 (7%) confirmed PRs and 2 (4%) uncon- firmed PRs; 9 (20%) patients had SD. The median TTP was 2 months, with an OS of 5 months. Given this modest activity in patients with gastric cancer, fur- ther investigation of combination regimens that in- clude lapatinib is warranted.
Colorectal Cancer In a multicenter, open-label, Phase II trial in 86 pa-
tients with metastatic colorectal cancer that had pro- gressed with first-line therapy consisting of 5-fluorouracil in combination with irinotecan or oxaliplatin, 53 pa- tients received oral lapatinib 1250 mg QD as mono- therapy. Tumor response (RECIST) was assessed by an independent review committee. ErbB expression was not required; however, 54.2% and 44.1% of patients had positive expression (1+, 2+, or 3+) of ErbB1 and ErbB2, respectively. Lapatinib had limited activity in this patient population, with a PR in 1 (1%) patient and minor responses in 5 other patients at week 8. The median TTP and OS were 8.0 and 42.9 weeks, respectively. Although overexpression of ErbB1 and ErbB2 was present, lapatinib had little activity in these patients with metastatic colorectal cancer, and there are no ongoing trials of lapatinib monotherapy or combination therapy for this indication.
Transitional Cell Carcinoma of the Urothelium In a European multicenter, open-label, Phase II
trial of second-line treatment with oral lapatinib 1250 nag QD in 59 patients with advanced or meta- static transitional cell carcinoma of the urothelial tract, 54 independent radiologic review found 1 (2%) confirmed PR and 18 (31%) patients with SD. Of the patients with SD, 6 and 3 had durable responses of 4 and 6 months, respectively. The median TTP was 8.6 weeks, and the median OS was 17.9 weeks. A clinical benefit (CR, PR, + SD for >16 weeks) of 12% was reported.
1440 Volume 30 Number 8

P.J. Medina and S. Goodin
The TTP with lapatinib in this trial was similar to that associated with other second-line therapies. Fu- ture studies of lapatinib should include only patients with ErbB1 or ErbB2 overexpression and should ex- amine lapatinib in combination with other novel agents for the treatment of transitional cell carcinoma of the urothelium.
Advanced Renal Cell Carcinoma A European multicenter, randomized, open-label,
Phase III trial evaluated lapatinib in patients with ad- vanced renal cell carcinoma that expressed EGFR and/or ErbB2. 55 Four hundred sixteen patients whose disease had progressed or had not responded to first- line cytokine therapy were randomized to receive ei- ther oral lapatinib 1250 mg QD or hormonal therapy (tamoxifen or megestrol acetate). Patients were strati- fied by Karnofsky performance status and number of metastatic sites. The groups were well balanced at baseline in terms of relevant prognostic factors, EGFR expression, and predominant site of metastatic disease (the lung). The results of the trial were negative for the primary end point of TTP in the overall population. There was no significant difference between lapati- nib and hormone therapy in median TTP (15.3 and 15.4 weeks, respectively) or median OS (46.9 and 43.1 weeks). However, an exploratory biomarker analysis evaluated the correlation between response and EGFR status by IHC. On independent pathologist review, overexpression of ErbB1 that had moderate to strong complete membrane staining in >10% of tu- mor cells was scored 3+. In the subgroup of 241 pa- tients with 3+ overexpression of ErbB1 by IHC, the median TTP was numerically increased in lapatinib recipients but did not reach statistical significance compared with hormonal therapy (15.1 vs 10.9 weeks). However, the median OS was significantly improved (46.0 vs 37.9 weeks; P = 0.02). This improved OS in patients with ErbB1 3+ tumors was validated by ret- rospective Cox regression analysis.
At the time this comparative trial of lapatinib and hormone therapy was initiated, there were limited treatment options for this patient population that had experienced disease progression while receiving cy- tokine therapy. However, studies are needed to com- pare lapatinib with current standard therapy, includ- ing sunitinib, sorafenib, and temsirolimus, to better define its role, if any, in patients with metastatic renal cell carcinoma.
Special Populations Pediatric Patients
Only 1 pharmacokinetic trial of lapatinib was iden- tified that included children or adolescents. Thirty-four pediatric patients with refractory or recurrent CNS tu- mors were treated with lapatinib at doses ranging from 300 t o 1150 mg/m-). -)6 Response rates were not re- ported, and further study is needed in this population.
Elderly Patients Although no studies were identified that specifi-
cally enrolled elderly patients, 17% of patients in clinical trials of lapatinib + capecitabine in MBC were aged _>65 years, and 1% were aged _>75 years. 37 The effectiveness and tolerability of lapatinib did not ap- pear to be affected by age, although increased sensitivi- ty in some older individuals cannot be ruled out. s
Organ Dysfunction A review of the literature found no pharmacoki-
netic studies in patients with renal impairment or in those undergoing hemodialysis. However, because <2% of a lapatinib dose is eliminated by the kidneys, renal impairment is not likely to affect the clearance of lapatinib, s
In a small study in subjects with moderate or severe hepatic impairment (Child-Pugh classes B and C, re- spectively), systemic exposure (AUC) after a single oral dose of lapatinib 100 mg increased -14% and 63%, respectively, compared with healthy control subjects, s Therefore, increased lapatinib exposure may occur in patients with severe hepatic impairment. Dose reduc- tion to 750 mg/d should be considered; this is predicted to adjust the AUC to within the normal range, although there are no clinical data to support this adjustment in patients with severe hepatic impairmenc 8
Pregnancy and Breastfeeding In rat and rabbit studies, malformations occurred
in rats exposed to lapatinib, and maternal toxicities and abortions occurred in rabbits, s Consequently, la- patinib is classified as pregnancy category D. Women should be advised not to become pregnant when tak- ing lapatinib, and its use is not advised in pregnant or lactating women. 8
ADVERSE EVENTS Similar to other EGFR small-molecule TK inhibitors, lapatinib is well tolerated. The most common clinical
August 2008 1441

Clinical Therapeutics
toxicities of all grades associated with lapatinib used in combination with capecitabine in the pivotal clini- cal trial were diarrhea (65%), hand-foot syndrome (53 %), nausea (44%), rash (29%), and fatigue (24%).39 In this trial, rates of discontinuation as a result of adverse events were 14% each in the combination and monotherapy groups, and dose interruptions and ad- justments due to adverse events were also similar be- tween groups. In an analysis of the quality-adjusted time without symptoms or toxicity in the pivotal Phase III trial of lapatinib + capecitabine in MBC, 37 the longer TTP with combination therapy versus mono- therapy (8.4 vs 4.4 months, respectively; HR = 0.49; 95% CI, 0.34-0.71; P < 0.001) was achieved without an increase in the time with serious adverse events, resulting in greater quality-adjusted survival. 63 Diar- rhea occurred in 65% of patients in the combina- tion group, compared with 34% of patients receiving capecitabine alone. Rash occurred more frequently in the combination-therapy group than in the mono- therapy group (29% vs 14%, respectively); however, the differences in both diarrhea and rash were the re- sult of increases in grade 1 adverse events. > Grade 3 diarrhea occurred in 13% of the combination group and 10% of the capecitabine group, and grade 3 rash occurred in 2% and 1% of the respective groups.
Diarrhea in patients receiving lapatinib may be dose and schedule related. In a pooled analysis of di- arrhea events in 9 completed Phase I, II, and III clini- cal trials in which lapatinib was administered at doses ranging from 1000 to 1500 mg QD as monotherapy or in combination with capecitabine or taxanes, Crown et a164 found that grade 3 diarrhea occurred in 10% to 17% of patients in trials of lapatinib 1500 mg QD, whereas 21% of patients reported diarrhea of grade 3 or higher with lapatinib 750 mg BID. In a trial of lapa- tinib 1500 mg QD + paclitaxel, 2s grade 3 diarrhea occurred in 18% of patients. Crown et al reported that diarrhea occurred in 55% of the 1417 lapatinib- treated patients and 24% of the 676 patients not treated with lapatinib. Diarrhea events with lapatinib were predominantly of grade 1 or 2 severity. There were no fatal lapatinib-related diarrhea events in any of the studies. Lapatinib-related diarrhea appeared to be an early event, occurring before day 6 in 42% of lapatinib recipients; among those not treated with la- patinib, the largest proportion of first diarrhea events (38 %) occurred after 28 days. The median duration of diarrhea with lapatinib was 5 days, with 85% of pa-
tients requiring no dose adjustment or interruption and only 2% discontinuing therapy due to diarrhea. The authors concluded that severe diarrhea did not occur with lapatinib-containing regimens when proac- tive monitoring and appropriate intervention were employed.
Dermatologic events, although of a low grade, are another frequently reported adverse event associated with lapatinib. Lacouture et a165 performed a review of dermatologic events occurring in 1419 patients enrolled in 9 clinical trials of lapatinib. A dermato- logic event was defined as hand-foot syndrome (pal- mar plantar erythrodysesthesia), rash, hair disorder, dry skin, pruritus/urticaria, skin disorder, skin infec- tion, and nail disorder. In patients receiving lapatinib monotherapy, 55% experienced grade 1 or 2 derma- tologic events; no grade 4 events were observed. Rash was the most common dermatologic event (43%) across all studies. Dermatologic events typically devel- oped early (within days 1-14), lasted a median of 29 days, and did not require any intervention or lapa- tinib dose reduction, interruption, or discontinuation.
Because of the cardiac toxicity associated with trastuzumab, 66 which also targets HER2, there was initial concern about potential cardiotoxicity with la- patinib. However, in the pivotal Phase III trial in MBC in patients who had previously received trastuzumab, 37 there were no reported differences in mean left ven- tricular ejection fraction (LVEF) between the 2 treat- ment groups. To further analyze the cardiotoxicity potential of lapatinib, Perez et a167 analyzed data from 44 studies involving 3689 patients enrolled in Phase I-III trials of lapatinib monotherapy and combination therapy in breast cancer and other solid tumors. Car- diotoxicity was evaluated based on symptomatic events, defined as either grade 3 or 4 according to the National Cancer Institute Common Toxicity Criteria (NCI CTCAE) or asymptomatic decreases in LVEF >20% from baseline or below the institutional nor- mal. A cardiac event was reported in 1.6% (n = 60) of patients; the event was not preceded by symptoms in 53 of these 60 patients. The decrease in LVEF resolved or improved in 88% (n = 35) of the 40 patients for whom the outcome was determined. The mean (stan- dard deviation) absolute decrease in LVEF from base- line in all patients was 18.8% (5.2%). The mean time of the onset of LVEF decrease was 13 weeks, and the decrease was rarely severe (0.2%). Finally, unlike tras- tuzumab, there was no significant association of the
1442 Volume 30 Number 8

p.J. Medina and S. Goodin
IIe655Val polymorphism and decreased LVEF with lapatinib. Because many patients who received lapa- tinib had not received previous cardiotoxic agents such as trastuzumab or an anthracycline (n = 2311), it was difficult to evaluate additive effects. The 1.3% reduction in LVEF with lapatinib was less than that associated with trastuzumab (3%-34%). 66 However, further studies are required to determine whether car- diac toxicity differs between these 2 agents.
To assess the cardiac tolerability of the combina- tion of lapatinib + trastuzumab, Storniolo et a168 ana- lyzed data from 4 trials involving 238 patients with HER2-positive MBC, 203 who received the combina- tion of lapatinib + trastuzumab and 35 who received the combination with a taxane. Cardiac tolerability was assessed in a manner similar to that in the study by Perez et al. 67 No patient had a symptomatic car- diac event, 1.7% (n = 4) had a single asymptomatic decrease in LVEF, and 0.4% (n = 1) had 2 asymptom- atic decreases. Two patients with a decrease in LVEF had received previous anthracyclines, and 2 patients had received previous anthracyclines and trastuzu- mab. These preliminary data indicated no incremental risk of cardiac toxicity with the combination of lapa- tinib + trastuzumab, although further studies of the cardiac tolerability of this combination are needed.
DOSING A N D A D M I N I S T R A T I O N Lapatinib is available in 250-mg tablets. The recom- mended oral lapatinib dose for patients with MBC whose tumors overexpresss HER2 (ErbB2) and who have received previous therapy including an anthra- cycline, a taxane, and trastuzumab is 1250 mg QD on days 1 to 21 in combination with capecitabine 2000 mg/m e daily administered in 2 divided doses on days 1 to 14 in a repeated 21-day cycle, s Treatment should be continued until disease progression or the occurrence of intolerable adverse effects. Lapatinib is to be taken as a single dose at least 1 hour before or after a meal. Dose adjustment of lapatinib is recom- mended based on tolerability and should be consid- ered in patients receiving strong CYP3A4 inhibitors or inducers, s
Lapatinib should be discontinued in patients with an LVEF decrease of grade 2 or greater (NCI CTCAE) or whose LVEF decreases below the institution's lower limit of normal. Therapy may be restarted at 1000 mg QD after at least 2 weeks if the LVEF has returned to normal and the patient is asymptomatic, s
Based on lapatinib's route of metabolism and elimi- nation, no dose adjustment is recommended in pa- tients with renal insufficiency. However, dose adjust- ment is recommended in patients with severe hepatic impairment (Child-Pugh class C). A dose reduction to 750 mg/d in patients with severe hepatic impairment is predicted to adjust the AUC to within the normal range, s although there are no clinical data to support adjustment.
P H A R M A C O E C O N O M I C C O N S I D E R A T I O N S A literature search found no pharmacoeconomic analyses of lapatinib in the treatment of MBC. The average wholesale price for a month of lapatinib thera- py is $3625, 69 and the manufacturer has an assistance program for uninsured and underinsured patients. 7°
C O N C L U S I O N S Lapatinib is a dual inhibitor of EGFR and HER2 that has proven activity in HER2-positive MBC. It has in vitro and in vivo activity as a single agent or as part of combination regimens in trastuzumab-resistant tu- mor models; in MBC that has progressed during treat- ment with trastuzumab; and in the first-line treatment of MBC. In Phase II trials in MBC, response rates ranged from 4.3% to 7.7% in trastuzumab-pretreated patients and were 24% in the first-line setting. Pre- liminary data suggest activity in other types of breast cancer, including IBC and breast cancer with CNS metastases. Phase III data from patients whose disease had progressed on an anthracycline, a taxane, and trastuzumab indicated a better response to the combi- nation of lapatinib + capecitabine than to capecitabine alone (22% vs 14%, respectively; P = NS). The com- bination also was associated with significant 43 % and 45% risk reductions in TTP and PFS, respectively. No statistical difference in OS was seen in that trial.
The most common adverse events associated with use of lapatinib as a single agent were diarrhea, rash, nausea, hand-foot syndrome, and fatigue. These ef- fects were generally mild, with few grade 3/4 toxici- ties. Lapatinib administered in combination with cape- citabine was associated with grade 3/4 diarrhea (14%) and grade 3 rash (2%).
Although lapatanib has been associated with sig- nificant activity only in HER2-positive breast cancer, it has reported activity in other tumor types. No sig- nificant clinical activity as an EGFR inhibitor has been found, as the response in other tumors overex-
August 2008 1443

Clinical Therapeutics
pressing EGFR has been limited. In advanced renal cell cancer, a Phase III trial of lapatinib monotherapy re- ported improved activity relative to hormonal therapy in the subgroup of patients whose tumors overexpressed ErbB1, although hormonal therapy would not be con- sidered an appropriate comparative regimen as the standard of care for renal cell carcinoma in the second- line setting. Preliminary data from Phase I/lI trials in other tumor types are mixed, and trials are ongoing.
REFERENCES 1. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007.
CA CancerJ Clin. 2007;57:43-66. 2. Lichter AS, Lippman ME, Danforth DN Jr, et al. Mastec-
tomy versus breast-conserving therapy in the treatment of stage I and II carcinoma of the breast: A randomized trial at the National Cancer Institute. J Clin Oncol. 1992;10: 976-983.
3. Pegram MD, Pauletti G, Slamon DJ. HER-2/neu as a pre- dictive marker of response to breast cancer therapy. Breast
Cancer Res Treat. 1998;52:65-77. 4. Slamon DJ, Clark GM, Wong SG, et al. Human breast
cancer: Correlation of relapse and survival with amplification
of the H ER-2/neu oncogene. Science. 1987;235:177-182. 5. Trastuzumab [package insert]. South San Francisco,
Calif." Genentech; 2003.
6. Gross ME, Shazer RL, Agus DB. Targeting the HER-kinase axis in cancer. Sen, in Onco[. 2004;31 (Suppl 3):9-20.
7. Petrov KG, Zhang YM, Carter M, et al. Optimization and SAR for dual ErbB-1/ErbB-2 tyrosine kinase inhibition in the 6-furanylquinazoline series. Bioorg Med Chen. Lett.
2006;16:4686-4691. 8. Lapatinib [package insert]. Research Triangle Park, NC:
GlaxoSmithKline; 2007. 9. Harari PM, Allen GW, BonnerJA. Biology of interactions:
Antiepidermal growth factor receptor agents.J C[in Onco[.
2007;25:4057-4065. 10. Zhang H, Berezov A, Wang Q, et al. ErbB receptors: From
oncogenes to targeted cancer therapies.J C[in Invest. 2007; 117:2051-2058.
11. Citri A, Yarden Y. EGF-ERBB signalling: Towards the sys- tems level. Nat Rev Mo[ Cell Bio[. 2006;7:505-516.
12. Spector NL, XiaW, Bums H III, et al. Studyofthe biologic effects of lapatinib, a reversible inhibitor of ErbB1 and ErbB2 tyrosine kinases, on tumor growth and survival
pathways in patients with advanced malignancies. J Cfin
Onco[. 2005;23:2502-2512. 13. Lackey KE. Lessons from the drug discovery oflapatinib,
a dual ErbB1/2 tyrosine kinase inhibitor. Curr Top Med Chem. 2006;6:435-460.
14. Scaltriti M, Rojo F, Ocafia A, et al. Expression of p95HER2, a truncated form of the HER2 receptor, and
response to anti-HER2 therapies in breast cancer. J Nail Cancer Inst. 2007;99:628-638.
15. Rusnak DW, Alligood KJ, Mull in RJ, et al. Assessment of epidermal growth factor receptor (EGFR, ErbB1) and HER2 (ErbB2) protein expression levels and response to lapatinib (Tykerb, GW572016) in an expanded panel of human normal and tumour cell lines. Cell Prolif 2007;40: 580-594.
16. Rusnak DW, Lackey K, Affleck K, et al. The effects of the novel, reversible epidermal growth factor receptor/ErbB-2 tyrosine kinase inhibitor, GW2016, on the growth of human normal and tumor-derived cell lines in vitro and in vivo. Mol Cancer Ther. 2001 ;1:85-94.
1 7. Konecny GE, Pegram MD, Venkatesan N, et al. Activity of the dual kinase inhibitor lapatinib (GW572016) against HER-2-overexpressing and trastuzumab-treated breast cancer cells. Cancer Res. 2006;66:1630-1 639.
18. Xia W, Gerard CM, Liu L, et al. Combining lapatinib (GW572016), a small molecule inhibitor of ErbB1 and ErbB2 tyrosine kinases, with therapeutic anti-ErbB2 anti- bodies enhances apoptosis o f ErbB2-overexpressing breast cancer cells. Oncogene. 2005;24:6213-6221.
19. Nahta R, Yuan LX, Du Y, Esteva FJ. Lapatinib induces apoptosis in trastuzumab-resistant breast cancer cells: Effects on insulin-like growth factor I signaling. Mol Cancer Ther. 2007;6:667-674.
20. Knowlden JM, Hutcheson IR, Jones HE, et al. Elevated levels of epidermal growth factor receptor/c-erbB2 het- erodimers mediate an autocrine growth regulatory path- way in tamoxifen-resistant MCF-7 cells. Endocrinology. 2003;144:1032-1044.
21. Chu I, Blackwell K, Chen S, SlingerlandJ.The dual ErbB1/ ErbB2 inhibitor, lapatinib (GW572016), cooperates with tamoxifen to inhibit both cell proliferation- and estrogen- dependent gene expression in antiestrogen-resistant breast cancer. Cancer Res. 2005;65:18-25.
22. Bence AK, Anderson EB, Halepota MA, et al. Phase I pharmacokinetic studies evaluating single and multiple doses of oral GW572016, a dual EGFR-ErbB2 inhibitor, in healthy subjects. Invest New Drugs. 2005;23:39-49.
23. Burris HA III, Hurwitz HI, Dees EC, et al. Phase I safety, pharmacokinetics, and clinical activity study of lapatinib (GW572016), a reversible dual inhibitor of epidermal growth factor receptor tyrosine kinases, in heavily pre- treated patients with metastatic carcinomas. J Clin Oncol. 2005;23:5305-5313.
24. Approval package for: Application number NDA 22-059. Medical reviews [FDA Web site], http://www.fda.gov/ cder/foi/nda/2007/O22059sOOOTOC.htm. Accessed Janu- ary 18, 2008.
25. Reddy N, Cohen R, Whitehead B, et al. A phase I, open- label, three period, randomized crossover study to evalu- ate the effect of food on the pharmacokinetics of lapa-
1444 Volume 30 Number 8

P.J. Medina and S. Goodin
tinib in cancer patients. Clin Phar- macol Ther. 2007;81(Suppl):S16- $I 7. Abstract PI-I 5.
26. Feng B, Fouladi M, Fraga C, et al. Lapatinib pharmacokinetics in pe- diatric patients with recurrent or refractory CNS tumors. Abstract presented at the 2007 AAPS Annual Meeting & Exposition. ht tp: / / abstracts.aapspharmaceutica.com/ expoch arger/index.asp? I D=am07. Accessed January 1 2, 2008.
27. Midgley RS, Kerr DJ, Flaherty KT, et al. A phase I and pharmacokinetic study of lapat in ib in combination with infusional 5-fluorouracil, leu- covorin and irinotecan. Ann Oncol. 2007;18:2025-2029.
28. LoRusso PM, Jones SF, Koch KM, et al. Phase I and pharmacokinetic study of lapatinib and docetaxel in patients with advanced cancer.
J Clin Oncol. 2008;26:3051-3056. 29. Chu QS, Schwartz G, de Bono J,
et al. Phase I and pharmacokinetic study of lapat in ib in combination with capecitabine in patients with advanced solid malignancies. J Clin Oncol. 2007;25:3753-3758.
30. Chu QS, Cianffocca ME, Goldstein LJ, et al. A phase I and pharmacoki- netic study oflapatinib in combina- tion with letrozole in patients with advanced cancer. Clin Cancer Res.
2008;14:4484-4490. 31. SiegeI-Lakhai WS, Beijnen JH, Ver-
venne WL, et al. Phase I phar- macokinetic study of the safety and tolerabil i ty o f lapatinib (GW572016) in combination with oxaliplatin/fluorouracil/leucovorin (FOLFOX4) in patients with solid tumors. Clin Cancer Res. 2007;13: 4495-4502.
32. Storniolo AM, Pegram MD, Over- moyer B, et al. Phase I dose escala- tion and pharmacokinetic study of lapatinib in combination with tras- tuzumab in patients with advanced ErbB2-positive breast cancer. J Clin Oncol. 2008;26:3317-3323.
33. Burstein HJ, Storniolo AM, Franco S, et al. A phase II study oflapatinib
monotherapy in chemotherapy- refractory H ER2-posidve and H ER2- negative advanced or metastatic breast cancer. Ann Oncol. 2008;19: 1068-I 074.
34. Blackwell KL, Burstein H, Pegram M, et al. Determining relevant bio- markers From tissue and serum that may predict response to single agent lapatinib in trastuzumab refractory metastatic breast cancer. J Clin On- co/. 2005;23(Suppl):256s. Abstract 3004.
35. lwata H, Toi M, Fujiwara Y, et al. Phase II clinical study of lapatinib (GW572016) in patients with ad- vanced or metastatic breast cancer. Presented at: 29th San Antonio Breast Cancer Symposium; Decem- ber 14-I 7, 2006; San Antonio, Tex. Abstract 1091.
36. Gomez HL, Doval DC, Chavez MA, et al. EFficacy and safe W of lapa- tinib as first-line therapy for ErbB2- amplified locally advanced or meta- static breast cancer. J Clin OncoL
2008;26:2999-3005. 37. Geyer CE, ForsterJ, Lindquist D, et
al. Lapatinib plus capecitabine for
HER2-positive advanced breast
cancer [published correction ap-
pears in N Eng! J Med. 2007;356:
1487]. N Engl J Med. 2006;355: 2733-2743.
38. Geyer CE, Forster J, Cameron D. Lapadnib plus capecitabine in breast cancer. N Engl J Med. 2007; 356:1471-1472.
39. Geyer CE, Martin A, Newstat B, et al. Lapadnib (L) plus capecitabine (C) in HER2+ advanced breast can- cer (ABC): Genomic and updated efficacy data. J Clin Oncol. 2007;25 (SuppI):40s. Abstract 1035.
40. Cameron D, Casey M, Press M, et al. A phase III randomized comparison of lapatinib plus capecitabine versus capecitabine alone in women with advanced breast cancer that has progressed on trastuzumab: Updated effi- cacy and biomarker analyses. Breast Cancer Res Treat. Published
online ahead of print January 11, 2008.
41. Di Leo A, Gomez H, Aziz Z, et al. Lapatinib (L) with paclitaxel com- pared to paclitaxel as first-line treatment for patients with meta- static breast cancer: A phase III randomized, double-blind study of 580 patients. J Clin Onco/. 2007;25 (Suppl):34s. Abstract 101 I.
42. Johnston S, Trudeau M, Kaufman B, et al. Phase II study of predictive biomarker profiles for response tar- geting human epidermal growth factor receptor 2 (HER-2) in ad- vanced inflammatory breast cancer with lapatinib monotherapy. J Clin Oncol. 2008;26:1066-I 072.
43. Cristofanilli M, Boussen H, Baselga J, et al. A phase II combination study of lapatinib and paclitaxel as neoadjuvant therapy in patients with newly diagnosed inflammatory breast cancer (IBC). Presented at: 29th Annual San Antonio Breast Cancer Symposium; December 14-17, 2006; San Antonio, Tex. Abstract I.
44. Lin NU, Carey LA, Liu MC, et al. Phase II trial of lapatinib for brain metastases in patients with human epidermal growth factor receptor 2- positive breast cancer. J Clin Onco/. 2008;26:1993-I 999.
45. Lin NU, Dieras V, Paul D, et al, for the EGF105084 Study Group. EGF105084, a phase II study of la- patinib for brain metastases in pa- tients (pts) with HER2+ breast can- cer following trastuzu mab (H) based systemic therapy and cranial radio- therapy (RT). J Clin Oncol. 2007; 25(Suppl):35s. Abstract 1012.
46. Lin NU, Paul D, Dieras V, et al. Lapatinib and capecitabine for the treatment of brain metastases in patients with HER2+ breast cancer-an updated analysis from EGF105084. Presented at: 30th An- nual San Antonio Breast Cancer Symposium; December 13-16, 2007; San Antonio, Tex. Abstract 6076.
August 2008 1445

Clinical Therapeutics
47. Smylie M, Blumenschein GR Jr, Dowlati A, et al. A phase II multi- center trial comparing two sched- ules of lapatinib (LAP) as first or
second line monotherapy in sub- jects with advanced or meta- static non-small cell lung cancer (NSCLC) with either bronchiolo- alveolar carcinoma (BAC) or no smoking history. J Clin Oncol. 2007;25(Suppl):412s. Abstract 7611.
48. Agulnik M, Cohen EW, Cohen RB, et al. Phase II study of lapatinib in recurrent or metastatic epidermal growth factor receptor and/or erbB2 expressing adenoid cystic carcinoma and non adenoid cystic carcinoma malignant tumors of the
salivary gland.J Clin Oncol. 2007;25: 3978-3984.
49. Ramanathan RK, Belani CP, Singh DA, et al. Phase II study of lapa- tinib, a dual inhibitor of epidermal
growth factor receptor (EGFR) ty- rosine kinase 1 and 2 (Her2/Neu) in patients (pts) with advanced bili- ary tree cancer (BTC) or hepato- cellular cancer (HCC). A California Consortium (CCC-P) trial. J Clin Oncol. 2006;24(Suppl):181s. Ab- stract 4010.
50. Abidoye OO, Cohen EE, Wong SJ, et al. A phase II study of lapatinib (GW572016) in recurrent/metastatic (R/M) squamous cell carcinoma of the head and neck (SCCHN).J Clin Oncol. 2006;24(Suppl):297s. Abstract 5568.
51. Sridhar SS, Hotte SJ, Chin JL, et al. A multicenter phase II study oflapa- tinib in hormone sensitive prostate cancer (HSPC). Presented at: 2007 Prostate Cancer Symposium; Feb- ruary 22-24, 2007; Orlando; Fla. Abstract 261.
52. Iqbal S, Goldman B, Lenz H J, et al. S0413: A phase II SWOG study of GW572016 (lapatinib) as first line therapy in patients (pts) with ad- vanced or metastatic gastric cancer. J Clin Oncol. 2007;25(Suppl):227s. Abstract 4621.
53. Fields AL, Rinaldi DA, Henderson CA, et al. An open-label multicenter phase II study of oral lapatinib (GW572016) as single agent, second-line therapy in patients with metastatic colorectal cancer. J Clin Oncol. 2005;23(Suppl):266s. Ab- stract 3583.
54. Wcilfing C, Machiels JP, Richel D, et al. A single arm, multicenter, open label, phase II study of lapatinib as 2L treatment of pts with locally advanced~metastatic transitional cell carcinoma (TCC) of the urothe-
lial tract. J Clin Oncol. 2005;23 (Suppl):401 s. Abstract 4594.
55. Ravaud A, Hawkins R, GardnerJP, et al. Lapatinib versus hormone therapy in patients with advanced renal cell carcinoma: A randomized phase III clinical trial. J Clin Oncol. 2008;26:2285-2291.
56. Therasse P, Arbuck SG, Eisenhauer EA, et al, for the European Organi- zation for Research and Treatment ofCancer, the National Cancer In- stitute of the United States, and the
National Cancer Institute of Cana- da. New guidelines to evaluate the response to treatment in solid tu- mors. J Nail Cancer Inst. 2000;92: 205-216.
57. Vogel CL, Cobleigh MA, Tripathy D, et al. Effificacy and safety of trastu- zumab as a single agent in first-line treatment of HER2-overexpressing metastatic breast cancer. J Clin On- co/. 2002;20:719-726.
58. Gomez HL, Chavez MA, Doval DC, et al. Investigation of tumor bio- markers as response predictors in a monotherapy study with lapatinib (L) as a first line treatment in ErbB2 amplified women with breast can- cer. J Clin Oncol. 2007;25(Suppl): 580s. Abstract 10562.
59. Lu Y, Zi X, Zhao Y, et al. Insulin-like growth factor-1 receptor signaling and resistance to trastuzumab (Herceptin).J Nail Cancer Inst. 2001 ; 93:1852-1857.
60. Bendell JC, Domchek SM, Burstein HJ, et al. Central nervous system
metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer.
2003;97:2972-2977. 61. Pestalozzi BC, Brignoli S. Trastu-
zumab in CSF.J Clin Oncol. 2000;18: 2349-2351.
62. Perez-Soler R. Rash as a surrogate marker for efficacy of epidermal growth factor receptor inhibitors in lung cancer. Clin Lung Cancer. 2006; 8(SuppI 1):$7-$14.
63. Sherrill B, AIIshouse A, Amonkar M, Stein S. A quality-adJusted time without symptoms or toxicity (Q-TWiST) analysis comparing lapatinib plus capecitabine com- pared to capecitabine for meta- static breast cancer (MBC). J Clin Oncol. 2007;25(Suppl):38s. Ab- stract 1026.
64. Crown JP, Burris HA III, Boyle F, et al. Pooled analysis of diarrhea events in patients with cancer treat- ed with lapatinib. Breast Cancer Res
Treat. Published online ahead of print January 20, 2008.
65. Lacouture ME, Laabs SM, Koehler M, et al. Analysis of dermatologic events in patients with cancer treat- ed with lapatinib. Breast Cancer Res. Published online ahead of print July 4, 2008.
66. Ewer SM, Ewer MS. Cardiotoxicity profile of trastuzumab. Drug Saf 2008;31:459-467.
67. Perez EA, Koehler M, Byrne J, et al. Cardiac safe W of lapatinib: Pooled analysis of 3689 patients enrolled in clinical trials. Mayo Clin Proc. 2008;83:679-686.
68. Storniolo AM, Koehler M, Preston A, et al. Cardiac safety in patients
(pts) with metastatic breast cancer (MBC) treated with lapatinib (L) and trastuzumab (TRA).J Clin Oncol. 2007;25(Suppl):6s. Abstract 514.
69. New drug bulletin: Lapatinib (Tykerb~-GlaxoS m ith Klin e [Univer-
sity of Utah Hospitals & Clinics Web site], http://uuhsc.utah.edu/ pharmacy/bulletins/NDB_131 .pdf. Accessed January 18, 2008.
1446 Volume 30 Number 8

P.J. Medina and S. Goodin
70. Tykerb ~ Cares. http://www.tykerb. com/hcp/hcp_resources /hcp_ tykerbcares.html?a=tcredirect. Ac- cessed January 18, 2008.
Address correspondence to: Susan Goodin, PharmD, FCCP, BCOP, Director, Division of Pharmaceutical Sciences, The Cancer Institute of New Jersey, 195 Little Albany Street, Room 2040, New Brunswick, NJ 08901. E-mail: [email protected]
August 2008 1447


![Stable Colloidal Drug Aggregates Catch and Release Active … · aggregators (chlorotrianisene, fulvestrant, nilotinib, lapatinib, sorafenib, tetraiodophenolphthalein [TIPT], and](https://img.pdfslide.us/doc/110x75/5d3c361688c993d64f8c99d1/stable-colloidal-drug-aggregates-catch-and-release-active-aggregators-chlorotrianisene.jpg)