-
7/29/2019 Laparoscopy in Infertility
1/75
Dr. Mohamed El SherbinyMD Ob.& Gyn. Senior Consultant
Damietta, Egypt
Laparoscopy in
InfertilityAn Evidence Based View
-
7/29/2019 Laparoscopy in Infertility
2/75
Sources of Evidences
National Guideline Clearinghouse 2000National Institute of
Clinical
Excellence(NICE)Guideline. Fertility2004
ESHRE guideline(2005)
Royal College of Obstetricians and Gynaecologists(RCOG)
infertility , 1999 & Endometriosis ,2006
Society of Obstetricians and
Gynaecologists of Canada (SOGC) 244- 2010Cochrane Library
Up To Date 2-19 May 2011
PubMed
-
7/29/2019 Laparoscopy in Infertility
3/75
The availability of assisted reproductive
technology (ART) has reduced the needfor laparoscopic
reconstructive surgery
in infertile women.However, there are still many
important indications for laparoscopy.
Is There Still a Role for Laparoscopy
in Female Infertility?
-
7/29/2019 Laparoscopy in Infertility
4/75
When fertility surgery is indicated, operative
laparoscopy results in outcome are as good
as those performed via open laparotomy.
However laparoscopy is associated with
Shorter Hospital Stay
Lower Incidence Of Ileus
Faster Recovery
Less Morbidities
Lower Postoperative Adhesion Formation
Laparoscopy Versus Laparotomy?
Togas Tulandi., Up to Date 19.2: May 2011
-
7/29/2019 Laparoscopy in Infertility
5/75
Less contamination of the surgical field with
glove powder or lint
Bleeding is reduced due to tamponade of
small vessels by the pneumoperitoneum
Drying of tissues is minimal because surgery
occurs in a closed environment
Why Does Laparoscopy Have Lower
Postoperative Adhesion Formation?
Togas Tulandi., UpToDate 19.2: May 2011
-
7/29/2019 Laparoscopy in Infertility
6/75
Laparoscopy in Infertility
Diagnostic Laparoscopy
Operative Laparoscopy
-
7/29/2019 Laparoscopy in Infertility
7/75
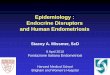
Female Infertility Workup
P4 /HSG
IVF/ ICSI
Laparoscopy
Laparoscopicablation
Minimal
or Mild
Moderate /Severe Mild Moderate
or Severe
AnovulationDysovulation :
Induction
Endometriosis
Obstruction or
Adhesion: traumatic or
inflammatory
AdhesiolysisResection ? /Fenestration ? Laparoscopic
Adhesiolysis
Laparoscopic
UnexplainedP4=Mid luteal phase progesterone
COH + IUI
Laparoscopy
LaparoscopicDrilling
El Sherbiny
f
-
7/29/2019 Laparoscopy in Infertility
8/75
Indications of Laparoscopy
in Female InfertilityI. Diagnostic LaparoscopyII. Operative
Laparoscopy
Adhesiolysis
Fimbrioplasty
Cornual Obstruction: Laparoscopic guided catheterization
Endometriosis:
Implant: ablation (electro-surgery or Laser)
Endometriomas: Excision, Fenestration & ablation
PCOS: Ovarian Drilling
Hydrosalpinx before IVF:
Salpingectomy
Proximal tubal occlusion & salpingostomy
-
7/29/2019 Laparoscopy in Infertility
9/75
Diagnostic
Laparoscopy
-
7/29/2019 Laparoscopy in Infertility
10/75
ESHRE Capri workshop 2000
Basic Routine Infertility Investigation
National Guideline Clearinghouse 2000
RCOG Guidelines: Grade B Recommendation 1999
Tests which have an establishedcorrelation with pregnancy
are:
Semen analysis
Tubal patency by HSG or laparoscopy
Mid luteal progesterone for the diagnosis of
ovulation
?
-
7/29/2019 Laparoscopy in Infertility
11/75
What Are The Tubal Patency Testing?
Transcervical Media:
HSG
Laparoscopy
HyCoSy
(Hysterosalpingo-Contrast Synography)
Direct cannulation of the fallopian tubes:Radiological:
Selective Salpingography
Hysteroscopic Guided by Laparoscopy
-
7/29/2019 Laparoscopy in Infertility
12/75
Women who are not known to have co-morbidities (such as PID,
previous ectopic
pregnancy or endometriosis) should be
offered HSG to screen for tubal occlusion.This is a reliable
test for ruling out tubal
occlusion, it is less invasive and makes
more efficient use of resources thanlaparoscopy.
National Institute of Clinical
Excellence(NICE)Guideline.Fertility2004
Grade B
When HSG and When Laparoscopy?
-
7/29/2019 Laparoscopy in Infertility
13/75
Women who are thought to have
co-morbidities should be offered
laparoscopyand dyeso that tubal andother pelvic pathology can be
assessed at
the same time.
National Institute of Clinical Excellence(NICE)Guideline.
Fertility2004
Grade B
When HSG and When Laparoscopy?
-
7/29/2019 Laparoscopy in Infertility
14/75
Test for Tubal Patency
No co-morbidities
National Institute of Clinical
Excellence(NICE)Guideline.Fertility2004
Co-morbidities
Laparoscopy
& DyeHSG
Or
HyCoSy
Grade B
Grade B
Grade A
l i d f ili
-
7/29/2019 Laparoscopy in Infertility
15/75
Case presentation A 27 year old woman, BMI 26
Primary infertility 4 years
No history of pelvic pain, infection or
ectopic pregnancy or pelvic surgery.
SemenFertile semen
Volume :4 ml
Count: 48 million/mL
Unexplained Infertility
Motility: 55% progressive
Normal forms:50%
-
7/29/2019 Laparoscopy in Infertility
16/75
She received empirical 6 cycles CC,
then 2 cycles HMG
ML Phase progesterone 12ng/ml
HSG: OK
-
7/29/2019 Laparoscopy in Infertility
17/75
Which of The Following is
Recommended for Our Patient?
1. Laparoscopy to exclude
endometriosis or adhesion
2. IUI 3 cycles
3. IUI + HMG, for 3 cycles
4. IVF/ICSI
-
7/29/2019 Laparoscopy in Infertility
18/75
There is still a considerable debate
regarding the place of laparoscopy
for cases of unexplained infertility.
Unexplained Infertility
A Place for Laparoscopy?
U l i d I f tilit
-
7/29/2019 Laparoscopy in Infertility
19/75
There has been a growing tendency for
bypassing diagnostic laparoscopy in
unexplained infertility.In their opinion this approach would
probably prove to be the most cost
effective and efficient treatment protocol.
Fatum, et al . (2002) Hum. Reprod.,17;1-3
Balasch (2000) Hum. Reprod., 15, 22512257
Badawy et al (BJOG 2008) .
Unexplained Infertility
A Place for Laparoscopy?
U l i d I f tilit
-
7/29/2019 Laparoscopy in Infertility
20/75
However, there were several reports indicating that in
infertile couples, laparoscopy revealed abnormal
findings in 21-78% with normal HSG.
After the treatment of these abnormal findings, higher
pregnancy rates can often be achieved by timing
intercourse or an IUI.
Cundiff et al. J Reprod Med 1995;40:1924. couples,.
Tanahatoe et al (2003) Hum Reprod 18,811.
Capelo et al(2003) Fertil Steril2003; 80:1450-1453.Nakagawa et
al 2007).. J. Obstet. Gynaecol. 2007; 33; 665-670
Unexplained Infertility
A Place for Laparoscopy?
-
7/29/2019 Laparoscopy in Infertility
21/75
Which of The Following is
Recommended?
1. Laparoscopy to exclude
endometriosis or adhesion2. IUI 3 cycles
3. IUI + HMG, for 3 cycles.
4. IVF/ICSIAs this patient is young and the period of
infertility is not
to long, laparoscopy may be a good choice.
-
7/29/2019 Laparoscopy in Infertility
22/75
Diagnostic laparoscopy can beavoided in:
Older women
Those with multiple infertility factors
These women are better served by IVF, instead ofa surgical
approach to treatment.
The presence of endometriosis and adhesionsdoes not markedly
influence the effectiveness ofIVF.
Togas Tulandi., Up to Date 19.2: May 2011
-
7/29/2019 Laparoscopy in Infertility
23/75
The following images are
examples of possible findingsduring laparoscopy that
include:
Normal laparoscopic findings Mild fimbrial adhesions
Moderate adhesions
Severe adhesions Hydrosalpinx
-
7/29/2019 Laparoscopy in Infertility
24/75Normal Laparoscopic Findings
Positive methyline blue test
Positive methyline blue test
Normal left adnxa
Normal left adnxa and Douglas pouch
-
7/29/2019 Laparoscopy in Infertility
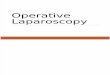
25/75
Mild fimbrial adhesionFimbria
Fine band of
adhesion
FimbriaFine
adhesion
Fimbria
Broad band
of adhesion
Moderate adhesion
DouglasPouch
-
7/29/2019 Laparoscopy in Infertility
26/75
Severe Adhesions
Dr.Sherbiny
-
7/29/2019 Laparoscopy in Infertility
27/75
Hydrosalpinx
-
7/29/2019 Laparoscopy in Infertility
28/75
Operative Laparoscopy for
Female Infertility
-
7/29/2019 Laparoscopy in Infertility
29/75
Adhesiolysis
Fimbrioplasty
Cornual Obstruction: Laparoscopicguided catheterization
Tubal Laparoscopic Procedures
Wh i T b l S
-
7/29/2019 Laparoscopy in Infertility
30/75
When is Tubal Surgery
Recommended ?For women with mild tubal disease, tubal
surgery may be more effective than no
treatment.
In centres where appropriate expertise is
available it may be considered as a treatment
option.
National Institute of Clinical
Excellence(NICE)Guideline.Fertility2004
Grade D
-
7/29/2019 Laparoscopy in Infertility
31/75
Adhesiolysis of the left tube with micro- scissor
Uterus
L. Ovary
L. Tube
-
7/29/2019 Laparoscopy in Infertility
32/75
R .Ovary
Cutting band of adhesion
What is Recommended for
-
7/29/2019 Laparoscopy in Infertility
33/75
What is Recommended forModerate to Severe Tubal Disease?
IVF should be considered as the first
line treatment for moderate to severedistal tubal disease.
RCOG Guidelines : Grade B Recommendation
-
7/29/2019 Laparoscopy in Infertility
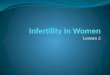
34/75
Phimosis of the fimbrial end: Dilatation with Maryland
forceps
Dr.Sherbiny
Phimosis with
methyline Blue jetPhimosis: delayed
methyline blue spill
Free methyline
blue spill
Dilatation with
Maryland forceps
-
7/29/2019 Laparoscopy in Infertility
35/75
Cornual ObstructionIf the fallopian tubes are not
visualized on HSG, a repeat
procedure should be done to
exclude the possibility of tubal
spasm.
-
7/29/2019 Laparoscopy in Infertility
36/75
Bilateral Cornual Obstruction
Tubal Catheterization
-
7/29/2019 Laparoscopy in Infertility
37/75
Tubal Catheterization
or Cannulation
For women with proximal tubal obstructionselective
salpingography plus tubal
catheterization, or Hysteroscopic tubal
cannulation (laparoscopic guided), may betreatment options
because these
treatments improve the chance of
pregnancy.
National Institute of Clinical
Excellence(NICE)Guideline.Fertility2004
Grade B
Hysteroscopic tubal catheterization or
-
7/29/2019 Laparoscopy in Infertility
38/75
Hysteroscopic tubal catheterization orCannulation laparoscopic
guided
Dr.SherbinyDr.Sherbiny
Laparoscopic guided
Catheterization
Hysteroscopic catheterization
Guide wire
Passage of inspissated material with M.blue at injection through
the catheter
-
7/29/2019 Laparoscopy in Infertility
39/75
Alternatively and
much cheaper, is to
use a pediatric
ureteric catheter
Passage of inspissated material with M.
blue at injection through the catheter
Laparoscopic guided
Catheterization
Hysteroscopic catheterization
-
7/29/2019 Laparoscopy in Infertility
40/75
Tubal Surgery Versus IVF
At present, the available research is not
adequate to determine the effectiveness.
More research is needed, including informationabout adverse
outcomes and costs.
Pandian et al The Cochrane review 2007 revised 2009Issue 1,
2009
Dr.Sherbiny
Wikimedia
http://upload.wikimedia.org/wikipedia/commons/8/86/Sperm-egg.jpghttp://upload.wikimedia.org/wikipedia/commons/8/86/Sperm-egg.jpghttp://upload.wikimedia.org/wikipedia/commons/8/86/Sperm-egg.jpg
-
7/29/2019 Laparoscopy in Infertility
41/75
Endometrioses
Associated Infertility:
The Role of Laparoscopy
Diagnostic
Operative
S i l Vi li ti f L i
-
7/29/2019 Laparoscopy in Infertility
42/75
Typical Endometriosis:
Black Endometriosis
Blue Endometriosis
Atypical (subtle) Endometriosis: Red Endometriosis: Red pink,
flam-like & clear
White Endometriosis
White Yellow Brown
Peritoneal Defect
American Society For Reproductive Medicine (ASRM)
Surgical Visualization of Lesions
Typical Endometriosis
-
7/29/2019 Laparoscopy in Infertility
43/75
Classic bluish black endometriotic implants
Typical Endometriosis
Black Endometriosis
Blue Endometriosis
Black Blue
-
7/29/2019 Laparoscopy in Infertility
44/75
Typical EndometriosisIn the majority of instances, the
laparoscopic appearances ofendometriosis lesions are
quitecharacteristic: black-blue, powder-burnappearance.
Diagnosis in most cases is simple, withoutthe need for a
biopsy.
Surgical Visualization of Lesions
-
7/29/2019 Laparoscopy in Infertility
45/75
Atypical Endometriosis= Subtle Endometriosis
= Non-pigmented EndometriosisEndometriotic lesions that lack
the
typical black-blue, powder-burnappearanceJansen &
Russel,1986
Surgical Visualization of Lesions
American Society For Reproductive Medicine (ASRM) 1996
-
7/29/2019 Laparoscopy in Infertility
46/75
-
7/29/2019 Laparoscopy in Infertility
47/75
Red Endometriosis (Pink)
Yellow Brown Endometriosis
Clear Endometriosis
ASRM Classification
-
7/29/2019 Laparoscopy in Infertility
48/75
ASRM ClassificationThe most widely used system was introduced
by
the American Society for ReproductiveMedicine (ASRM) in 1979 and
revised in 1996 .
This system assigns a point score based upon the
size, depth, and location of endometriotic
implants and associated adhesions. The system
was revised for women with infertility to help
predict success in achieving pregnancy following
treatment of endometriosis.
Robert S Schenken, UpToDate 2-19 May 2011
American Society For Reproductive Medicine (ASRM)
-
7/29/2019 Laparoscopy in Infertility
49/75
51
Stage I: Minimal (score 1-5)
Stage II: Mild (score 6-15)
Stage III: Moderate (score 16-40)
Stage IV: Severe (score >40)
American Society For Reproductive Medicine (ASRM)
Endometriosis
-
7/29/2019 Laparoscopy in Infertility
50/75
Endometriotic Cyst
=
Endometrioma
Endometriosis
-
7/29/2019 Laparoscopy in Infertility
51/75
Implant:
Diagnosis
Ablation (electro-surgery or Laser )
Endometriomas:
Excision
Fenestration & ablation
EndometriosisAssociated Infertility
-
7/29/2019 Laparoscopy in Infertility
52/75
Laparoscopic Surgery
1. Laparoscopic treatment of minimal or mild
endometriosis improves pregnancy rates
regardless of the treatment modality. (I)
SOGC Clinical Practice Guidelines 244, 2010
Jacobson et al , Cochrane Library Review, 20 JAN 2010
Laparoscopic treatment: Ablation or excision of implants and
adhesions via Mechanical, electro-surgery or LASER surgery
-
7/29/2019 Laparoscopy in Infertility
53/75
Monoplar Ablation
of Endometriotic
Implant
-
7/29/2019 Laparoscopy in Infertility
54/75
Laparoscopic Treatment
2. The effect on fertility of surgical
treatment of deeply infiltrating
endometriosis is controversial. (II)
3. Laparoscopic excision of ovarian
endometriomas more than 3 cmin diameter may improve fertility.
(II)
SOGC Clinical Practice Guidelines 244, 2010
O l i Di d 20%
-
7/29/2019 Laparoscopy in Infertility
55/75
Ovulation Disorders - 20%
The WHO classification is three groups:
Group I: hypothalamic pituitary failure
(hypothalamic amenorrhoea or
hypogonadotrophic hypogonadism)
Group II: hypothalamic pituitary dysfunction
predominately polycystic ovary syndrome (PCOS)Group III: ovarian
failure
National Institute for Clinical Excellence (NICE) 2004
-
7/29/2019 Laparoscopy in Infertility
56/75
Polycystic Ovary
Syndrome
(PCOS)
Rotterdam Diagnostic
-
7/29/2019 Laparoscopy in Infertility
57/75
When 2 out of 3 features are present:
Oligomenorrhoea and/or Anovulation
Clinical Hyperandrogenism and/or
hyperandrogenemia
Polycystic ovaries (U/S)
After exclusion of other etiologies.
Rotterdam DiagnosticCriteria Of PCOS May 2003
What are?
Rotterdam
U/S Criteria
-
7/29/2019 Laparoscopy in Infertility
58/75
At least one of the following:
12 or more follicles measuring 29 mm in diameter
Increased ovarian volume (>10 cm3
) The distribution of follicles and a description of the stroma
are
not required for diagnosis.
The presence of a single PCO is sufficient to provide the
diagnosis.
Rotterdam U/S Criteriaof PCO 2003
-
7/29/2019 Laparoscopy in Infertility
59/75
PCO
Management of PCOS
-
7/29/2019 Laparoscopy in Infertility
60/75
First Step:
Lifestyle modification: Weight loss 10%Second Step:
Clomiphene citrate (CC) or Tamoxifen
Third Step:Improving the CC Resistant: Metformin
Fourth Step:
Gonadotropin Versus Drilling Intrauterineinsemination
Fifth Step:
IVF /ICSI
Management of PCOS
PCOS: Laparoscopic Drilling
-
7/29/2019 Laparoscopy in Infertility
61/75
Laparoscopic ovarian drilling with either
diathermy or laser is an effectivetreatment for anovulation in
women with
clomiphene-resistant PCOS.
PCOS: Laparoscopic Drilling
RCOG Guidelines : Grade A
58National Institute of Clinical Excellency(NICE) 2004
-
7/29/2019 Laparoscopy in Infertility
62/75
PCOS Drilling Optimization
A strategy of minimizing the number ofdiathermy points to:
4/ovary
For 4 s
At 40 W
Armar et al. Fertil Steril 1990;53:459.
Complications of
-
7/29/2019 Laparoscopy in Infertility
63/75
Tubo-ovarian adhesions can occur, buttend to be milder than with
the classic
wedge resection.
Ovarian drilling is the commonest cause of
pelvic adhesion in Egypt.
The ovaries can undergo irreparabledamage and atrophy.
Naether, 1993; Greenblatt, 1993
Dabirashrafi, 1989).
Complications of
Laparoscopic Drilling
Laparoscopic Ovarian Drilling
-
7/29/2019 Laparoscopy in Infertility
64/75
Multiple holes are made on the surface of
the ovary using either laser or
electrocautery.
This results in a decrease in circulating
androgen levels, with resumption of
cyclic ovulation.
Ovulation rate: 80 %
Pregnancy rates at 12 m: 54 to 68%.
Laparoscopic Ovarian Drilling
Togas Tulandi., Up to Date 19.2: May 2011
Laparoscopic Ovarian Drilling
-
7/29/2019 Laparoscopy in Infertility
65/75
Techniques:ElectrocauteryLaser "drilling"
Multiple biopsyEach share a common goal of creating
focal areas of damage in the ovarian
cortex and stroma.There is no evidence that one method
consistently produces superior clinical
results.
Laparoscopic Ovarian Drilling
Barry W Donesky., Up to Date 19.2: May 2011
Laparoscopic Ovarian Drilling
-
7/29/2019 Laparoscopy in Infertility
66/75
Laparoscopic ovarian drilling is recommended
in those women who meet the followingcriteria:
Failure of ovulation despite an adequate trialof clomiphene
citrate and metformin
Body mass index 30 kg/m2
An elevated serum luteinizing hormoneconcentration (>10
IU/L)
Absence of other causes of infertility
Laparoscopic Ovarian Drilling
Togas Tulandi., Up to Date 19.2: May 2011
Advantage of Drilling
-
7/29/2019 Laparoscopy in Infertility
67/75
No cyclic monitoring of ovulationMore cost-effective as results
in several
ovulatory cycles
No increased risk of multiple gestationor ovarian
hyperstimulation
Pregnancy rates are similar to
gonadotropin therapyLower spontaneous abortion rate in
some studies
Advantage of DrillingOver Gonadotropin Therapy
Barry W Donesky., UpToDate 19.2: May 2011
-
7/29/2019 Laparoscopy in Infertility
68/75
Laparoscopic
Management ofHydrosalpinges
Prior to IVF
-
7/29/2019 Laparoscopy in Infertility
69/75
Hydrosalpnex
-
7/29/2019 Laparoscopy in Infertility
70/75
Dr.Sherbiny
Incomplete
septation
Hydrosalpnex (Ultrasonography ) : Oblong shape with
incomplete
septations
Laparoscopic Management of
-
7/29/2019 Laparoscopy in Infertility
71/75
Laparoscopic Management ofHydrosalpinges Prior to IVF
Laparoscopic salpingectomy should be
considered for all women with
hydrosalpinges prior to IVF treatment
as it improves IVF pregnancy rates.
Johnson et al (2004 ) Cochrane Systematic Reviews 2009 Issue
4
NICE Guideline 2004 Infertility
-
7/29/2019 Laparoscopy in Infertility
72/75
Laparoscopic Management of
-
7/29/2019 Laparoscopy in Infertility
73/75
Laparoscopic tubal occlusion is an alternative to
laparoscopic salpingectomy in improving IVF
pregnancy rates in women with hydrosalpinges.
Further research is required to assess the value of
aspiration of hydrosalpinges prior to or during
IVF procedures.
Johnson et al (2010 ) Cochrane Systematic Reviews Issue 1,
2010
A more recent evidence
Laparoscopic Management of
Hydrosalpinges Prior to IVF
-
7/29/2019 Laparoscopy in Infertility
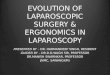
74/75
Tubal bipolar coagulation Cutting of the medial
part of the tube
SalpingostomySalpingostomy
Laparoscopic tubal occlusion & salpingostomy of
Hydrosalpinges prior to IVF to improve pregnancy rate
Thank You
-
7/29/2019 Laparoscopy in Infertility
75/75
Thank You