Embed Size (px)
Citation preview
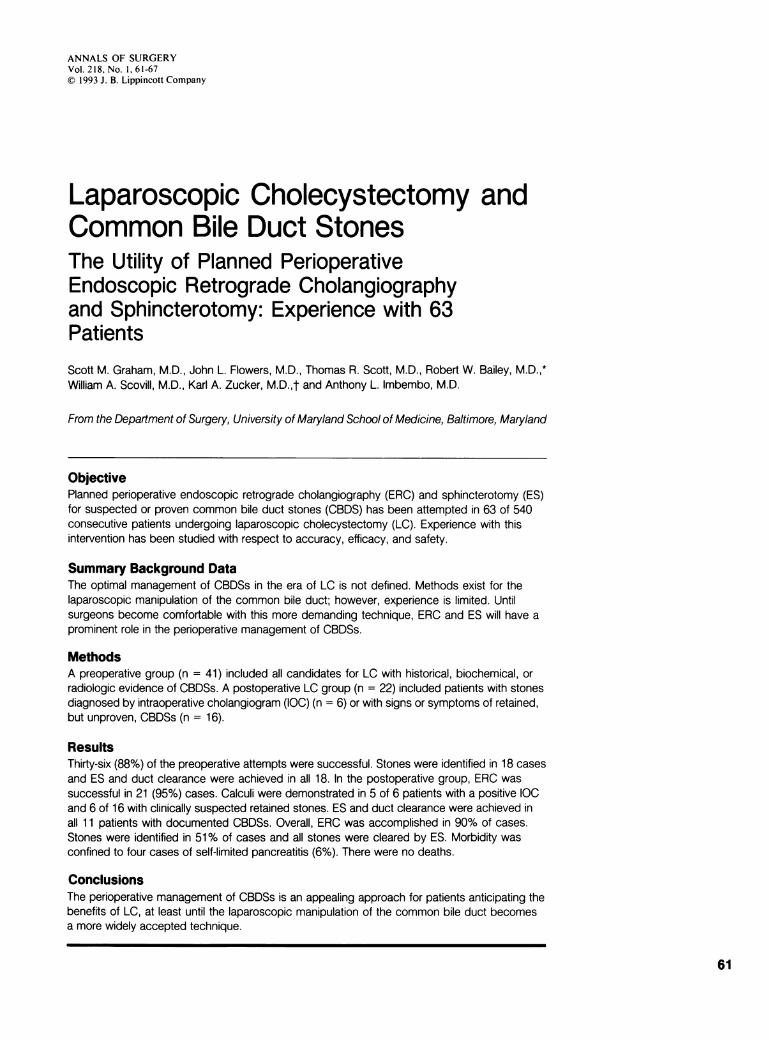
ANNALS OF SURGERYVol. 218, No. 1, 61-67©) 1993 J. B. Lippincott Company
Laparoscopic Cholecystectomy andCommon Bile Duct StonesThe Utility of Planned PerioperativeEndoscopic Retrograde Cholangiographyand Sphincterotomy: Experience with 63PatientsScott M. Graham, M.D., John L. Flowers, M.D., Thomas R. Scott, M.D., Robert W. Bailey, M.D.,*William A. Scovill, M.D., Karl A. Zucker, M.D.,t and Anthony L. Imbembo, M.D.
From the Department of Surgery, University of Maryland School of Medicine, Baltimore, Maryland
ObjectivePlanned perioperative endoscopic retrograde cholangiography (ERC) and sphincterotomy (ES)for suspected or proven common bile duct stones (CBDS) has been attempted in 63 of 540consecutive patients undergoing laparoscopic cholecystectomy (LC). Experience with thisintervention has been studied with respect to accuracy, efficacy, and safety.
Summary Background DataThe optimal management of CBDSs in the era of LC is not defined. Methods exist for thelaparoscopic manipulation of the common bile duct; however, experience is limited. Untilsurgeons become comfortable with this more demanding technique, ERC and ES will have aprominent role in the perioperative management of CBDSs.
MethodsA preoperative group (n = 41) included all candidates for LC with historical, biochemical, orradiologic evidence of CBDSs. A postoperative LC group (n = 22) included patients with stonesdiagnosed by intraoperative cholangiogram (IOC) (n = 6) or with signs or symptoms of retained,but unproven, CBDSs (n = 16).
ResultsThirty-six (88%) of the preoperative attempts were successful. Stones were identified in 18 casesand ES and duct clearance were achieved in all 18. In the postoperative group, ERC wassuccessful in 21 (95%) cases. Calculi were demonstrated in 5 of 6 patients with a positive IOCand 6 of 16 with clinically suspected retained stones. ES and duct clearance were achieved inall 11 patients with documented CBDSs. Overall, ERC was accomplished in 90% of cases.Stones were identified in 51% of cases and all stones were cleared by ES. Morbidity wasconfined to four cases of self-limited pancreatitis (6%). There were no deaths.
ConclusionsThe perioperative management of CBDSs is an appealing approach for patients anticipating thebenefits of LC, at least until the laparoscopic manipulation of the common bile duct becomesa more widely accepted technique.
61
62 Graham and Others
Since its introduction in 1987,1 laparoscopic cholecys-tectomy (LC) has gained rapid acceptance as the pre-
ferred management of symptomatic cholelithiasis. Thistrend has created uncertainty regarding the optimal man-agement of suspected or unexpected common bile ductstones (CBDS) in patients who anticipate the benefits ofminimally invasive surgery. Laparoscopic common bileduct manipulation would probably be the most ideal ap-
proach, and a small but promising experience has beenreported from centers with a special interest in advancedlaparoscopic techniques.2`8 Over time, surgeons may be-come more comfortable with this direct, but more de-manding, technique. In the interim, endoscopic retro-grade cholangiography (ERC) and endoscopic sphincter-otomy (ES) have important roles to play in theperioperative management of CBDSs. The experiencewith planned perioperative ERC and ES at a single insti-tution is presented.
METHODSBetween September 1989 and April 1992, 540 patients
underwent attempts at LC. All patients presenting fortreatment of symptomatic gallbladder disease had his-tory and physical examination, laboratory tests, and ul-trasonographic evaluation ofthe biliary tract. Additionaldiagnostic tests in selected patients included computer-ized tomography, oral cholecystography, or biliary scin-tigraphy. Sixty-three patients had perioperative ERC forsuspected or proven CBDSs and constitute the study pop-ulation. They are divided into preoperative and postoper-ative groups.
Preoperative GroupForty-one patients were suspected of having CBDSs
before surgery. Criteria included any one or more ofthefollowing parameters: ultrasound showing a bile duct di-ameter greater than 8.0 mm; ultrasound showing a
CBDS; serum amylase level greater than 220 units/L(normal, 110 u/L); total serum bilirubin level greaterthan 2.0 mg/dL (normal, 1.0 mg/dL); and serum alka-line phosphatase level greater than 252 IU/L (normal,126 IU/L). The mean age in this group was 51 years
(range, 19-83 years). Fifteen patients were men (37%)and 26 were women (63%).
* Current address: Greater Baltimore Medical Center, Towson, Mary-land.
t Current address: University of New Mexico School of Medicine, Al-buquerque, New Mexico.
Address reprint requests to Scott M. Graham, M.D., Surgical Endos-copy, Department of Surgery, Room N8E24, University of Mary-land Medical Center, 22 South Greene Street, Baltimore, MD 21201.
Accepted for publication September 22, 1992.
Postoperative GroupTwenty-two patients who had undergone LC had
stones detected by intraoperative cholangiography (IOC)(n = 6) or had signs and symptoms of retained, but un-proven, CBDSs (n = 16) after LC. None of the 16 pa-
tients with unproven stones had an IOC at the time ofLC. The mean age in this population was 48 years(range, 28-79 years). Five patients were men (23%) and17 were women (77%).
ERCERC was performed after obtaining informed and wit-
nessed consent from all patients. All patients had normalcoagulation parameters and received intravenous broadspectrum antibiotics. Continuous, noninvasive moni-toring of heart rate, blood pressure, and oxygen satura-tion was maintained. When stones were identified, ESand stone extraction were attempted using standard tech-niques.
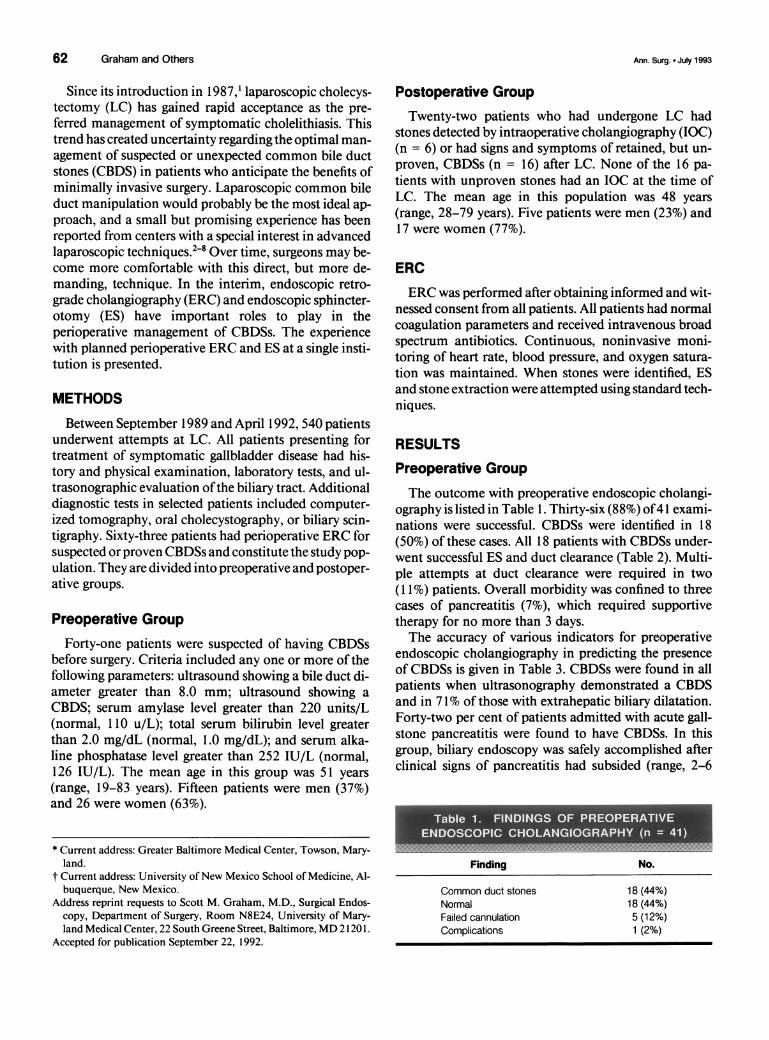
RESULTSPreoperative GroupThe outcome with preoperative endoscopic cholangi-
ography is listed in Table 1. Thirty-six (88%) of41 exami-nations were successful. CBDSs were identified in 18(50%) of these cases. All 18 patients with CBDSs under-went successful ES and duct clearance (Table 2). Multi-ple attempts at duct clearance were required in two(1 1%) patients. Overall morbidity was confined to threecases of pancreatitis (7%), which required supportivetherapy for no more than 3 days.The accuracy of various indicators for preoperative
endoscopic cholangiography in predicting the presenceof CBDSs is given in Table 3. CBDSs were found in allpatients when ultrasonography demonstrated a CBDSand in 71% of those with extrahepatic biliary dilatation.Forty-two per cent of patients admitted with acute gall-stone pancreatitis were found to have CBDSs. In thisgroup, biliary endoscopy was safely accomplished afterclinical signs of pancreatitis had subsided (range, 2-6
Finding No.
Common duct stones 18 (44%)Normal 18 (44%)Failed cannulation 5 (12%)Complications 1 (2%)
Ann. Surg. * July 1993
ERCP and Laparoscopic Cholecystectomy 63
.5- S*:l S=-1¢M
Result No.
Clearance 18 (100%)Attempts
Single 16 (89%)Multiple 2 (11%)
Complications 2 (11%)
days). An elevated bilirubin or alkaline phosphataselevel was predictive in 40% and 38% of cases, respec-tively. Biliary scintigraphy was performed on two pa-tients with chronic biliary colic, but no evidence ofchole-lithiasis. Both studies indicated dyskinesia ofthe gallblad-der and delayed emptying of the common bile duct.Preoperative endoscopic cholangiography demonstrateda CBDS in one of these patients, while the other hadmanometric evidence of biliary dyskinesia and a cysticduct stricture. Except for the three patients who had pan-creatitis after endoscopy, all patients were operated on
within 48 hours of endoscopy.The surgical outcomes of the 41 patients undergoing
preoperative ERC are detailed in Table 4. LC was suc-
cessfully accomplished in 37 (90%) patients. Of 18 pa-tients with a normal preoperative endoscopic cholangio-gram, all had LC and IOC. One patient was found tohave a 2-mm filling defect after "normal" preoperativeendoscopy (false-negative rate, 3%). Because this fillingdefect was small, LC was completed and this patient hasbeen observed without incident for 8 months. Three(17%) of 18 patients who had ES required conversion toopen cholecystectomy because dense inflammation pre-
cluded a safe laparoscopic dissection. Among the fivepatients in whom endoscopic cholangiography failed,only one had an abnormal IOC and required open com-mon bile duct exploration for proven choledocholithia-sis. The remaining four patients had LC alone. Only 2(5%) of 37 patients undergoing LC required hospitaliza-
No. of %Indications No. Stones Predictability
CBDS by ultrasound 6 6 100Dilated CBD by ultrasound 14 10 71Elevated bilirubin level 25 10 40Elevated amylase level 14 6 42Elevated alkaline phosphatase level 24 9 38Abnormal biliary scintigraphy 2 1 50
Laparoscopic
No. %
Open
No. %
ERC 18 100 0 0ES 15 83 3 17Failed 4 80 1 20
Total 37 90 4 10
tion beyond 24 hours. One patient with bullous emphy-sema had a spontaneous pneumothorax on the first post-operative day and required an additional week of hospi-talization. The second was a neurosurgical patient whosehospitalization was extended for purposes ofphysical re-
habilitation. There was no morbidity or mortalityamong the entire surgical group that had preoperativeendoscopic cholangiography.
Postoperative GroupERC was attempted in 22 patients after LC (Table 5).
It was successfully accomplished in 21 (95%) patients,and 11 (52%) patients had retained CBDSs. The patientin whom ERC failed had acute pancreatitis 2 weeks afterLC and unsuccessful IOC. It is presumed that a retainedstone had passed. This patient has been observed for 1
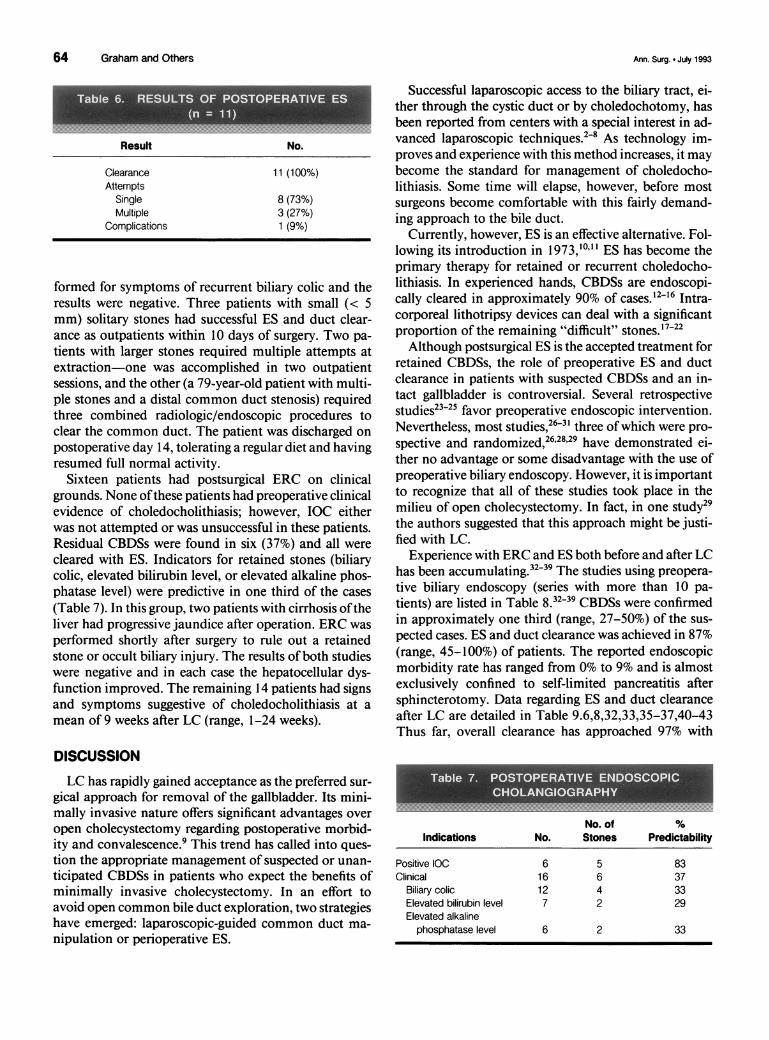
year without sequelae.All 11 patients in whom stones were identified under-
went postoperative ES and had successful duct clearance(Table 6). Three (27%) required multiple attempts toachieve complete duct clearance. There was one instanceof self-limited pancreatitis, which accounted for an over-
all morbidity rate of 4% in this group.Six patients were found to have unsuspected filling
defects during laparoscopic-guided IOC. One patient,who it was thought might have a very small stone, was
observed. Eleven months after surgery, ERC was per-
*.
Finding No.
CBDS 11 (50%)Normal 10 (45%)Failed 1 (5%)Complications 0 (0%)
Vol. 218 * No. 1
64 Graham and Others
Result No.
Clearance 11 (100%)Attempts
Single 8 (73%)Multiple 3 (27%)
Complications 1 (9%)
formed for symptoms of recurrent biliary colic and theresults were negative. Three patients with small (< 5mm) solitary stones had successful ES and duct clear-ance as outpatients within 10 days of surgery. Two pa-
tients with larger stones required multiple attempts atextraction-one was accomplished in two outpatientsessions, and the other (a 79-year-old patient with multi-ple stones and a distal common duct stenosis) requiredthree combined radiologic/endoscopic procedures toclear the common duct. The patient was discharged on
postoperative day 14, tolerating a regular diet and havingresumed full normal activity.
Sixteen patients had postsurgical ERC on clinicalgrounds. None ofthese patients had preoperative clinicalevidence of choledocholithiasis; however, IOC eitherwas not attempted or was unsuccessful in these patients.Residual CBDSs were found in six (37%) and all were
cleared with ES. Indicators for retained stones (biliarycolic, elevated bilirubin level, or elevated alkaline phos-phatase level) were predictive in one third of the cases
(Table 7). In this group, two patients with cirrhosis oftheliver had progressive jaundice after operation. ERC was
performed shortly after surgery to rule out a retainedstone or occult biliary injury. The results ofboth studieswere negative and in each case the hepatocellular dys-function improved. The remaining 14 patients had signsand symptoms suggestive of choledocholithiasis at a
mean of 9 weeks after LC (range, 1-24 weeks).
DISCUSSION
LC has rapidly gained acceptance as the preferred sur-
gical approach for removal of the gallbladder. Its mini-mally invasive nature offers significant advantages over
open cholecystectomy regarding postoperative morbid-ity and convalescence.9 This trend has called into ques-
tion the appropriate management of suspected or unan-
ticipated CBDSs in patients who expect the benefits ofminimally invasive cholecystectomy. In an effort toavoid open common bile duct exploration, two strategieshave emerged: laparoscopic-guided common duct ma-
nipulation or perioperative ES.
Successful laparoscopic access to the biliary tract, ei-ther through the cystic duct or by choledochotomy, hasbeen reported from centers with a special interest in ad-vanced laparoscopic techniques.2 8 As technology im-proves and experience with this method increases, it maybecome the standard for management of choledocho-lithiasis. Some time will elapse, however, before mostsurgeons become comfortable with this fairly demand-ing approach to the bile duct.
Currently, however, ES is an effective alternative. Fol-lowing its introduction in 1973,1o 'l ES has become theprimary therapy for retained or recurrent choledocho-lithiasis. In experienced hands, CBDSs are endoscopi-cally cleared in approximately 90% of cases. 12-16 Intra-corporeal lithotripsy devices can deal with a significantproportion of the remaining "difficult" stones. 17-22Although postsurgical ES is the accepted treatment for
retained CBDSs, the role of preoperative ES and ductclearance in patients with suspected CBDSs and an in-tact gallbladder is controversial. Several retrospectivestudies23125 favor preoperative endoscopic intervention.Nevertheless, most studies,26-3' three ofwhich were pro-
spective and randomized,262829 have demonstrated ei-ther no advantage or some disadvantage with the use ofpreoperative biliary endoscopy. However, it is importantto recognize that all of these studies took place in themilieu of open cholecystectomy. In fact, in one study29the authors suggested that this approach might be justi-fied with LC.
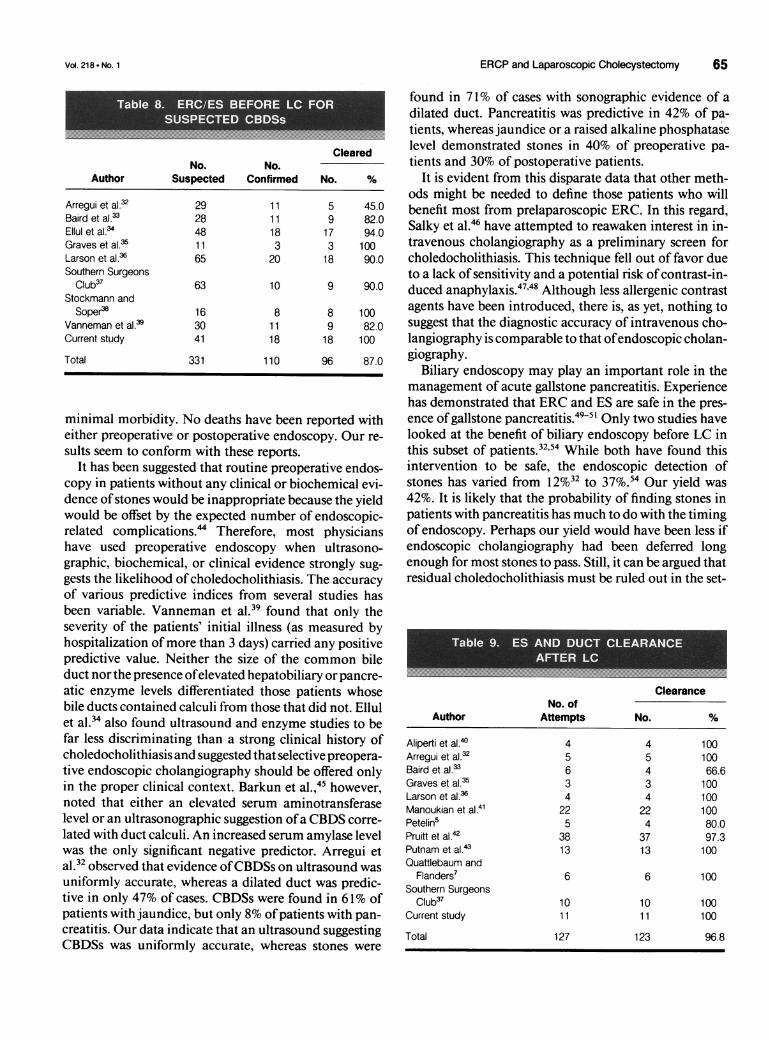
Experience with ERC and ES both before and after LChas been accumulating.32-39 The studies using preopera-tive biliary endoscopy (series with more than 10 pa-tients) are listed in Table 8.3239 CBDSs were confirmedin approximately one third (range, 27-50%) of the sus-
pected cases. ES and duct clearance was achieved in 87%(range, 45-100%) of patients. The reported endoscopicmorbidity rate has ranged from 0% to 9% and is almostexclusively confined to self-limited pancreatitis aftersphincterotomy. Data regarding ES and duct clearanceafter LC are detailed in Table 9.6,8,32,33,35-37,40-43Thus far, overall clearance has approached 97% with
IndicationsNo.of %
No. Stones Predictability
Positive IOC 6 5 83Clinical 16 6 37
Biliary colic 12 4 33Elevated bilirubin level 7 2 29Elevated alkaline
phosphatase level 6 2 33
... ..... ....
Ann. Surg. * July 1993
ERCP and Laparoscopic Cholecystectomy 65
ClearedNo. No.
Author Suspected Confirmed No. %
Arregui et al.32 29 11 5 45.0Baird et al.33 28 11 9 82.0Ellul et al.34 48 18 17 94.0Graves et al.35 11 3 3 100Larson et al.36 65 20 18 90.0Southern Surgeons
Club37 63 10 9 90.0Stockmann and
Soper38 16 8 8 100Vanneman et al. > 30 11 9 82.0Current study 41 18 18 100
Total 331 110 96 87.0
minimal morbidity. No deaths have been reported witheither preoperative or postoperative endoscopy. Our re-
sults seem to conform with these reports.It has been suggested that routine preoperative endos-
copy in patients without any clinical or biochemical evi-dence of stones would be inappropriate because the yieldwould be offset by the expected number of endoscopic-related complications.'4 Therefore, most physicianshave used preoperative endoscopy when ultrasono-graphic, biochemical, or clinical evidence strongly sug-
gests the likelihood of choledocholithiasis. The accuracyof various predictive indices from several studies hasbeen variable. Vanneman et al.39 found that only theseverity of the patients' initial illness (as measured byhospitalization of more than 3 days) carried any positivepredictive value. Neither the size of the common bileduct nor the presence ofelevated hepatobiliary or pancre-atic enzyme levels differentiated those patients whosebile ducts contained calculi from those that did not. Ellulet al.34 also found ultrasound and enzyme studies to befar less discriminating than a strong clinical history ofcholedocholithiasis and suggested that selective preopera-tive endoscopic cholangiography should be offered onlyin the proper clinical context. Barkun et al.,45 however,noted that either an elevated serum aminotransferaselevel or an ultrasonographic suggestion ofa CBDS corre-
lated with duct calculi. An increased serum amylase levelwas the only significant negative predictor. Arregui etal.32 observed that evidence ofCBDSs on ultrasound wasuniformly accurate, whereas a dilated duct was predic-tive in only 47% of cases. CBDSs were found in 61% ofpatients with jaundice, but only 8% of patients with pan-creatitis. Our data indicate that an ultrasound suggestingCBDSs was uniformly accurate, whereas stones were
found in 71% of cases with sonographic evidence of adilated duct. Pancreatitis was predictive in 42% of pa-tients, whereas jaundice or a raised alkaline phosphataselevel demonstrated stones in 40% of preoperative pa-tients and 30% of postoperative patients.
It is evident from this disparate data that other meth-ods might be needed to define those patients who willbenefit most from prelaparoscopic ERC. In this regard,Salky et al.46 have attempted to reawaken interest in in-travenous cholangiography as a preliminary screen forcholedocholithiasis. This technique fell out of favor dueto a lack of sensitivity and a potential risk ofcontrast-in-duced anaphylaxis.47'48 Although less allergenic contrastagents have been introduced, there is, as yet, nothing tosuggest that the diagnostic accuracy of intravenous cho-langiography is comparable to that ofendoscopic cholan-giography.
Biliary endoscopy may play an important role in themanagement of acute gallstone pancreatitis. Experiencehas demonstrated that ERC and ES are safe in the pres-ence of gallstone pancreatitis.49-51 Only two studies havelooked at the benefit of biliary endoscopy before LC inthis subset of patients.32'54 While both have found thisintervention to be safe, the endoscopic detection ofstones has varied from 12%32 to 37%.54 Our yield was42%. It is likely that the probability of finding stones inpatients with pancreatitis has much to do with the timingof endoscopy. Perhaps our yield would have been less ifendoscopic cholangiography had been deferred longenough for most stones to pass. Still, it can be argued thatresidual choledocholithiasis must be ruled out in the set-
.0S; S' iai
ClearanceNo. of
Author Attempts No. %
Aliperti et al.40 4 4 100Arregui et al.32 5 5 100Baird et al.33 6 4 66.6Graves et al.35 3 3 100Larson et al.36 4 4 100Manoukian et al.4' 22 22 100Petelin5 5 4 80.0Pruitt et al.42 38 37 97.3Putnam et al.43 13 13 100Quattlebaum and
Flanders7 6 6 100Southern Surgeons
Club37 10 10 100Current study 11 11 100
Total 127 123 96.8
Vol. 218 * No. 1

66 Graham and Others
ting of gallstone pancreatitis and that preoperative bili-ary endoscopy might be beneficial whether performedearly or late.Concerns remain regarding the potential long-term
risk of sphincterotomy. Although the immediate com-plications of ES are well documented, the long-term ef-fects are less well defined. Stricture formation and stonerecurrence, with or without cholangitis or jaundice, ac-count for nearly all long-term complications. Two stud-ies55'56 with the longest mean follow-up times (49 and 96months) report complication rates of 7% and 13%, re-spectively. These results do not appear to differ signifi-cantly from long-term outcomes after surgery for denovo or retained CBDSs.55 Yet, as no prospective com-parisons of endoscopic versus surgical treatment ofCBDSs have ever been undertaken, a scientific basis fortreatment is lacking. Nevertheless, empiric evidencewould indicate that the benefits of shorter hospitaliza-tion, reduced pain, and faster recovery for a patient hav-ing LC and perioperative sphincterotomy for stones out-weighs both the short-term morbidity of open commonbile duct exploration and the potential long-term se-quelae of ES.Our experience and that of others suggests that
planned perioperative biliary endoscopy can simplifydecision making and diminish the need for an open (orlaparoscopic) common bile duct exploration. Thus far,this approach has been very safe and effective. Currently,intraoperative choledochoscopic methods are restrictedby technical problems. It is, therefore, reasonable to rec-ommend perioperative endoscopic cholangiography andsphincterotomy in patients with suspected or occultCBDSs, at least until the laparoscopic manipulation ofthe common bile duct becomes a more widely acceptedapproach.
AcknowledgmentThe authors thank Ms. Ellen Evans for preparing this manuscript.
References1. Dubois F, Berthelot G, Levard H. Cholecystectomy par coeliosco-
pie. Nouv Presse Med 1989; 18:980-982.2. Shapiro SJ, Gordon LA, Daykhovsky L, Grundfest W. Laparo-
scopic exploration of the common bile duct: experience in 16 se-lected patients. J Laparoendosc Surg 1991; 1:333-341.
3. Hunter JG. Laparoscopic transcystic common bile duct explora-tion. Am J Surg 1992; 163:53-58.
4. Jacobs M, Verdeja JC, Goldstein HS. Laparoscopic choledocho-lithotomy. J Laparoendosc Surg 1991; 1:79-82.
5. Petelin JB. Laparoscopic approach to common duct pathology.Surg Laparosc Endosc 1991; 1:33-41.
6. Phillips E, Carroll B, Daykhovsky L, Fallas M, Panish J. Manage-ment ofcommon bile duct stones (CBD) encountered during lapa-roscopic cholecystectomy (LC). Gastrointest Endosc 1991; 37:245.
7. Quattlebaum JK, Flanders HD. Laparoscopic treatment of com-mon bile duct stones. Surg Laparosc Endosc 1991; 1:26-32.
8. Stoker ME, Leveillee RJ, McCann JC, Maini BS. Laparoscopiccommon bile duct exploration. J Laparosc Endosc Surg 1991;1:287-293.
9. Bailey RW, Zucker KA, Flowers JL, Scovill WA, Graham SM,Imbembo AL. Laparoscopic cholecystectomy: experience with375 consecutive patients. Ann Surg 1991; 214:531-541.
10. Kawai K, Akasaka Y, Murakamy K, Tada M, Kohli Y, NakajimaM. Endoscopic sphincterotomy of the ampulla of vater. Gastroin-test Endosc 1974; 20:148-151.
11. Classen M, Demling L. Endoskopische sphincterotomie der pa-pilla vateri und stein extraction aus dem choledochos. Dtsch MedWochenschr 1974; 99:496-497.
12. Cotton PB. Nonoperative removal ofbile duct stones by duodeno-scopic sphincterotomy. Br J Surg 1980; 67:1-5.
13. Kawai K, Nakajima M. Present status and complications of ESTin Japan. Endoscopy 1983; 15:169-172.
14. Escourrou J, Cordova JA, Lazorthes F, Frexinos J, Ribet A. Earlyand late complications after endoscopic sphincterotomy for biliarylithiasis with and without the gallbladder in situ. Gut 1984;25:598-602.
15. Leese T, Neoptolemos JP, Carr-Locke DL. Successes, failure, earlycomplications and their management following endoscopicsphincterotomy: results in 394 consecutive patients from a singlecenter. Br J Surg 1985; 72:215-219.
16. Ikeda S, Tanaka M, Matsumoto S, Yoshimoto H, Ito H. endo-scopic sphincterotomy: long-term results in 408 patients withcomplete follow up. Endoscopy 1988; 20:13-17.
17. Chung SCS, Leung JWC, Leong HT, Banez VP, Li AKC. Endo-scopic extraction of large common duct stones using a mechanicallithotripsy basket. Gastrointest Endosc 1991; 37:252.
18. Neuhaus H, Hoffmann W, Hogrefe A, Classen M. Cholangiosco-pic dye laser lithotripsy in the nonsurgical treatment of difficultbile duct stones. Gastrointest Endosc 1991; 37:254.
19. Ponchon T, Gagnon P, Valette PJ, Henry L, Chavaillon A. Pulseddye laser lithotripsy of bile duct stones. Gastrointest Endosc 1991;37:250.
20. Schneider MU, Mattek W, Bower W, Domschke W. Mechanicallithotripsy of bile duct stones in 209 patients: effective technicaladvances. Endoscopy 1988; 20:244-253.
21. Seigel JH, Ben-Zvi JS, Pullano WE. Mechanical lithotripsy ofcommon duct stones. Gastrointest Endosc 1990; 36:351-356.
22. Seigel JH, Ben-Zvi JS, Pullano WE. Endoscopic electrohydrauliclithotripsy. Gastrointest Endosc 1990; 36:134-136.
23. Ponchon T, Bory R, Chavaillon A, Fouillet P. Biliary lithiasis:combined endoscopic and surgical treatment. Endoscopy 1989;21:15-18.
24. Heinermann PM, Boeckl 0, Pimpl W. Selective ERCP and preop-erative stone removal in bile duct surgery. Ann Surg 1989;209:267-272.
25. Steigmann GV, Pearlman, MW, Goff JS, Sun JH, Norton LW.Endoscopic cholangiography in stone removal prior to cholecys-tectomy. A more cost effective approach than operative duct explo-ration? Arch Surg 1989; 124:787-790.
26. Neoptolemos JP, Carr-Locke DL, Fossard DP. Prospective ran-domized study of preoperative endoscopic sphincterotomy versussurgery alone for common bile stones. Br Med J 1987; 294:470-474.
27. Miller BM, Kozarek RA, Ryan JA, Ball TJ, Traverso LW. Surgicalversus endoscopic management ofcommon bile duct stones. AnnSurg 1988; 207:135-141.
28. Stain SC, Cohen H, Tsuishoysha M, Donovan AJ. Choledocho-lithiasis: endoscopic sphincterotomy orcommon bile duct explora-tion. Ann Surg 1991; 213:627-634.
29. Steigmann GV, Gough JS, Mansour A, Pearlman N, Reveille RM,Norton L. Precholecystectomy endoscopic cholangiography and
Ann. Surg. * July 1993
ERCP and Laparoscopic Cholecystectomy 67
stone removal is not superior to cholecystectomy, cholangiogra-phy and common duct exploration. Am J Surg 1992; 163:227-230.
30. Neoptolemos JP, Davidson BR, Shaw DE, Lloyd DE, Carr-LockeDL, Fossard DP. Study ofcommon bile duct exploration and endo-scopic sphincerotomy in a consecutive series of 438 patients. Br JSurg 1987; 74:916-921.
31. Neoptolemos JP, Shaw DE, Carr-Locke DL. A multivariate analy-sis of preoperative risk factors in patients with common bile ductstones: implications for treatment. Am Surg 1989; 209:157-161.
32. Arregui ME, Davis CJ, Arkush AM, Nagan RF. Laparoscopic cho-lecystectomy combined with endoscopic sphincterotomy andstone extraction or laparoscopic choledochoscopy and electrohy-draulic lithotripsy for management of cholelithiasis and choledo-cholithiasis. Surg Endosc 1992; 6:10-15.
33. Baird DR, Wilson JP, Mason EM, et al. An early review of 800laparoscopic cholecystectomies at university affiliated communityteaching hospital. Am Surg 1992; 58:206-2 10.
34. Ellul JPM, Wilkinson ML, McColl I, Dowling RH. A predictiveERCP study of patients with gallbladder stones (GBS) and proba-ble choledocholithiasis-predictive factors. Gastrointest Endosc1992; 38:266.
35. Graves HA, Ballinger JF, Anderson WJ. Appraisal of laparoscopiccholecystectomy. Ann Surg 1991; 213:655-664.
36. Larson GM, Vitale FC, Casey J. Multipractice analysis of laparo-scopic cholecystectomy in 1983 patients. Am J Surg 1992;163:221-226.
37. The Southern Surgeons Club. A prospective analysis of 1518 lapa-roscopic cholecystectomies. N Engl J Med 1991; 324:1073-1078.
38. Stockmann PT, Soper NJ. Early results of laparoscopic cholecys-tectomy at a teaching institution. Perspect Gen Surg 1991; 2:1-19.
39. Vanneman W, Kingsbury R, Duberman E, Lee M. When is ERCPindicated before laparoscopic cholecystectomy? Gastrointest En-dosc 1992; 38:265.
40. Aliperti G, Edmundowitz SA, Soper NJ. Early experience withcombined endoscopic sphincterotomy and laparoscopic cholecys-tectomy in patients with choledocholithiasis. Am J Gastroenterol1990; 85:1245.
41. Manoukian AV, Schmalz MJ, Geenen JE, Venu RP, Johnson GK.Post-laparoscopic cholecystectomy problems: "minimally inva-sive" ERCP therapy. Gastrointest Endosc 1992; 38:250.
42. Pruitt RE, Bailey AH, Foust TW, Olsen DO, Spaw A, Reddick EJ.Endoscopic retrograde cholangiography with sphincterotomy andcommon bile duct stone extraction combined with laparoscopic
laser cholecystectomy: our initial experience. Gastrointest Endosc1991; 37:286.
43. Putnam WS, Wegley SJ, Rosen SN, Lewis ST. The impact oflapa-roscopic cholecystectomy on ERCP in a community hospital. Gas-trointest Endosc 1991; 37:246.
44. Cotton PB, Baillie J, Pappas TN, Meyers WS. Laparoscopic chole-cystectomy and the biliary endoscopist. Gastrointest Endosc 1991;37:94-97.
45. Barkun AN, Steinmetz OK, Barkun JS, Gitalescu G. The role ofERCP in laparoscopic cholecystectomy. Gastrointest Endosc1992; 38:247.
46. Salky BA, Bauer JJ, Kreel 1, Gelernt IM, Gorfine SR. Laparo-scopic cholecystectomy: an initial report. Gastrointest Endosc1991; 37:1-8.
47. Cohen M. ERCP before laparoscopic cholecystectomy. Gastroin-test Endosc 1991; 37:495-496.
48. Goodman MW, Ansel HJ, Vennes JA, Lasser RB, Silvis SE. Isintravenous cholangiography still useful? Gastroenterology 1980;79:642-645.
49. Van Der Spuy S. Endoscopy sphincterotomy in the managementof gallstone pancreatitis. Endoscopy 1981; 13:25-26.
50. Safrany L, Cotton PB. A preliminary report: urgent duodenosco-pic sphincterotomy for acute gallstone panceratitis. Surgery 1981;89:424-428.
51. Rosseland AR, Solhaug JH. Early or delayed endoscopic papillo-tomy (EPT) in gallstone pancreatitis. Ann Surg 1984; 199:165-167.
52. Neoptolomos JP, Carr-Locke DL, London NJ, Bailey IA, JamesD, Fossard DP. Controlled trial of urgent endoscopic retrogradecholangiopancreatography and endoscopic sphincterotomy versusconservative treatment for acute pancreatitis due to gallstones.Lancet 1988; 2:979-983.
53. Carr-Locke DL. Acute gallstone pancreatitis in endoscopic ther-apy. Endoscopy 1990; 22:180-183.
54. Buse PE, Edmundowicz SE, Soper NJ, Aliperti G. Management ofacute gallstone panceratitis with ERCP and laparoscopic cholecys-tectomy. Gastrointest Endosc 1992; 38:292.
55. Hawes RH, Cotton PB, Vallon AA. Follow-up 6 to 11 years afterduodenoscopic sphincterotomy for stones in patients with priorcholecystectomy. Gastroenterology 1990; 98:1008-1012.
56. Jacobsen 0, Matzen P. Long-term follow-up study ofpatients afterendoscopic sphincterotomy for choledocholithiasis. Scand J Gas-troenterol 1987; 22:903-906.
Vol. 218 - No. 1

![Left Sided Laparoscopic Cholecystectomy: Case Report and ...open cholecystectomy - before laparoscopic era [2] and 1 case in 2008 [3] and about 50 cases of laparoscopic cholecystectomy](https://img.pdfslide.us/doc/110x75/5f6509906579645fd7227a11/left-sided-laparoscopic-cholecystectomy-case-report-and-open-cholecystectomy.jpg)