Embed Size (px)
Citation preview
Journal of Clinical Periodontology \911\ 4: 115-127Key words; Trauma jrom occlusion - jiggling - periodontkis.Accepted for publication: August 19, 1976.
Lack of effect of trauma fromocclusion on the recurrence
of experimental periodontitisINGVAR ERICSSON AND JAN LINDHE
Department of Periodontology, Faculty of Odontology,University of Gothenburg, Gothenburg, Sweden
Abstract. The experiments were performed in 15 dogs fed a diet which allowed dentalplaque accumulation. A phase of experimental periodontal breakdown was initiated onday 0. After 210 days five dogs were sacrificed. In the remaining 10 dogs the periodontalpockets around the fourth lower premolars {̂P and P4) were eliminated. During surgerya notch was prepared in the root at the level of the marginal termination of the alveolarhone in order to facilitate measurements in histologica! sections. From day 210 to day 450the teeth of the animals were brushed twice daily. After 60 days of healing, i. e. on day270. five of the dogs were sacrificed. Trauma from occlusion of the jiggling type was onday 270 produced in the P4 region of the remaining dogs by the installation of a cap splintand a har device. The final five dogs were sacrificed on day 450. Following sacrifice,tissue sections comprising ^P, ^P, ,M and P.,, P ,̂ Mj were produced and subjected tomicroscopic analysis.
The experiments revealed that, in the dog, forces produced hy occlusal trauma are un-able to induce a phase of progressive destruction of the periodontal tissues in tooth regionswhere the supporting tissues are markedly reduced but non-inflammatory.
Experiments in dogs reported by Saxe et al. man, trauma from occlusion alters the pat-(1967), Svanberg et al. (1973) and Lindhe tern and rate of tissue breakdown in plaque-et al. (1973, 1975) have demonstrated that, indueed periodontal disease. In a reviewin the presence of dental plaque and cal- paper from 1967. GHckman concludedculus, a longstanding gingivitis in most in- "Animal and human studies have led tostances develops into a progressive and the concept that trauma from occlusion isdestructive periodontitis. These observations an integral part of the disease periodontitisdemonstrate the central role played by the rather than an unrelated disease entity.microbial plaque in the etiology of peri- Such a trauma from occlusion is an etio-odontitis and corroborate data from epide- logic factor in the formation of infrahonymiological studies and assessments made in pockets and angular or crater-like osseoushuman autopsy material. defects". This concept, however, has not
It has been claimed (Glickman 1963, been unanimously accepted (for review see1967) that trauma from occlusion is an im- Svanberg 3974, Meitner 1975a).portant co-factor in the pathogenesis of Animal studies by Wentz et al. (1958),marginal periodontitis. According to Glick- Glickman & Smulow (1968), Svanberg &
116 ERICSSON AND LINDHE
Lindhe (1973, 1974) and Kantor et al.(1976) have revealed that experimentallyproduced trauma from occlusion (jiggling)may induce (1) increased tooth mobility (2)angular resorption of the marginal alveolarbone and (3) increased width of the peri-odontal ligament. In animals with normalgingiva or overt gingivitis, jiggling forcesneither induce loss of connective tissueattachment nor result in the formation ofperiodontal pockets. In dogs suffering froma rapidly progressing periodontitis, how-ever, traumatic forces result not only invery pronounced tooth hypermohility butalso in the production of angular osseousdefects, infrabony pockets and an enhancedrate of periodontal tissue breakdown (Lind-he & Svanberg 1974). This influence ofjiggling forces and hypermobile teeth onthe progression of periodontitis was recentlystudied also in squirrel monkeys by Meitner(1975b), He reported that jiggling forcescaused an increase in the apical down-growth of the dentogingival epithelium inonly one area out of four studied. Basedon this finding he discarded the co-factortheory of Glickman.
Treatment of periodontitis must involvethe elimination of plaque and retentionfactors for plaque, as well as the establish-ment of an anatomy in the dentogingivalregion which facilitates proper toothcleaning (Suomi et al. 1971, Ramfjord et al.1973, Lindhe & Nyman 1975). Therefore,the essential question remains, what effecttrauma from occlusion may have once theplaque-induced lesion has heen eliminated.This problem was in part recently studiedin dogs by Lindhe & Ericsson (1976). Aprocess of breakdown of the periodontaltissues was first initiated using a methodoriginally described by Swenson (1947).After 180 days of plaque accumulation, ajiggling-type occlusal trauma was alsointroduced. Periodontitis was treated 100days later by surgical pocket elimination.
scaling and plaque control, but traumafrom occlusion was allowed to persist. Theanalysis of tissue sections obtained 90 daysfollowing elimination of periodontal pock-ets demonstrated that the jiggling forcesdid not detrimentally affect healing.
The aim of the present experiment wasto assess the effect of jiggUng produced byocclusal forces on markedly reduced butnon-inflammatory periodontal tissues.
Material and Methods
Fifteen beagle dogs were used. Duringa preparatory period of several weeks theanimals were subjected to a careful plaquecontrol program. Hence, once a week theirteeth were scaled and twice daily brushedwith toothbrush and dentifrice. At the startof the study all dogs had clinically healthygingiva and normal height of the periodon-tal tissues.
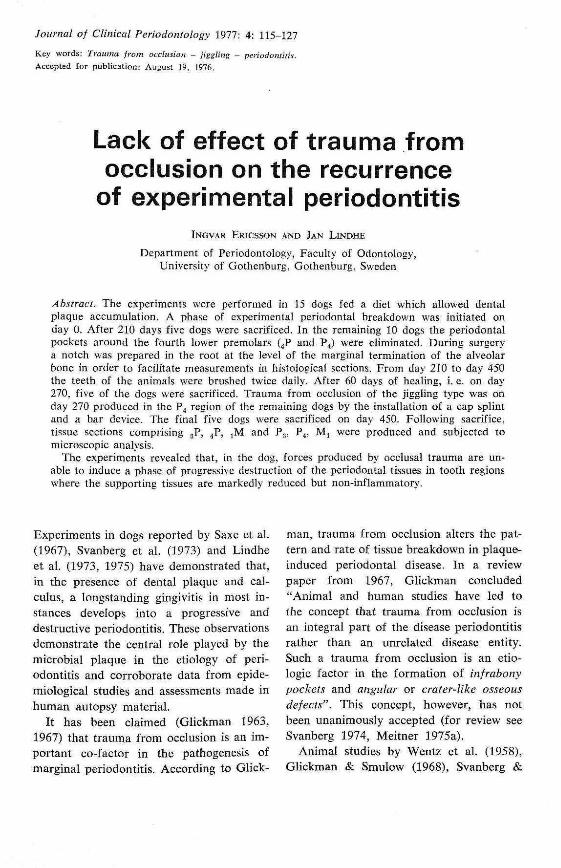
Experimental ProcedureOn day 0 (Fig. 1) a phase of experimentalperiodontitis was initiated in all dogs. Themethod originally described by Swenson(1947) and modified by Lindhe & Svanberg(1974) was utilized. In the regions of thefourth lower premolars (4P and P4) muco-pariosteal flaps were raised. About 1 mm ofthe marginal alveolar bone around these teethwas removed using a bur. To prevent reat-tachment and to enhance plaque formation,copper bands extending down to the surgi-cally established bone level were punchedclose to the teeth. The plaque control regi-men was terminated and the dogs placedon a diet which allowed the accumulationof plaque. Twenty-one days later the cop-per bands were removed and substituted bycotton floss ligatures which were placed atthe level of the cemento-enamel junction(CEJ). 210 days after the installation ofthe copper bands (Fig. 1), the animals hadaccumulated abundant amounts of plaque
TRAUMATIC OCCLUSION AND RECURRENT PERIODONTITIS 117
ElPERIMfHTALPEBIODONTALBBEAKDOWM
POCSETEllMINAIIOM
5CA11NG
NOTCH
310
JIGGLING
i
EIPER1M6NTALPERIOD ON TAlBBEAKDOWN
SCALINGMOICH
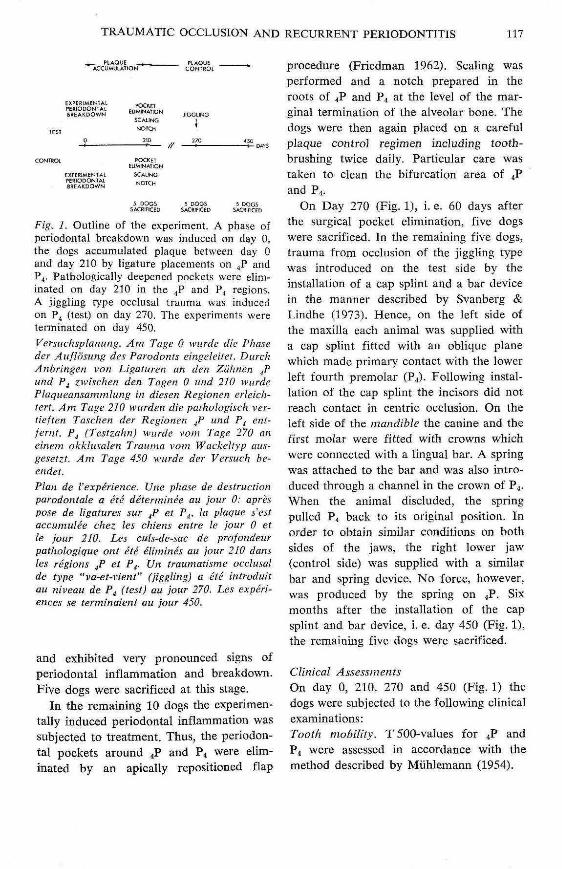
Fig. 1. Outline of the experiment. A phase ofperiodontal breakdown was induced on day 0,the dogs accumulated plaque between day 0and day 210 by ligature placements on P̂ andP^. Pathologically deepened pockets were elim-inated on day 210 in the P̂ and P̂ regions.A jiggling type occlusal trauma was inducedon Pj (test) on day 270. The experiments wereterminated on day 450.Versuchsplanung. Am Tage 0 wtjrde die Phaseder Auflosung des Parodonts eingeleilel. DurchAnhringen von Ligatuien an den Ziihnen 4Pund Pj zwischen den Tagen 0 und 210 wurdePlaqueansammlung in diesen Regionen crlelch-tert. Am Tage 210 wurden die palbologisch ver-lieften Taschen der Regionen jP und P^ enl-fernt. P^ (Teslzahn) wurde vom Tage 270 aneinem okklusalen Trauma, vom Wackeltyp aiis-gesetzt. Am Tage 450 wurde der Vcrsuch be-endei.Plan de Vexperience. line phase de destructionparodontaie a He delerminee au jour 0: apre.'ipose de ligatures sur ^P et P^, la plague s'estaccumulee chez les ehiens entre le jour 0 etle jour 210. Les cuh-de-sac de profondeurpathologique ont ete elimines au jour 210 dansles regions ^P et P^. Un traumatisme ocdusalde type "va-et-vient" (jiggling) a ete introduitau niveau de P^ (test) au jour 270. Les experi-ences se terminaient au jour 450.
and exhibited very pronounced signs ofperiodontal inflammation and breakdown.Five dogs were sacrificed at this stage.
In the remaining 10 dogs the experimen-tally induced periodontal inflammation wassubjected to treatment. Thus, the periodon-tal pockets around 4P and P4 were elim-inated by an apicaliy repositioned flap
procedure (Friedman 3 962). Scaling wasperformed and a notch prepared in theroots of 4P and P4 at the level of the mar-ginal termination of the alveolar bone. Thedogs were then again placed on a carefulplaque control regimen including tooth-brushing twice daily. Particular care wastaken to clean the bifurcation area of 4Pand P4.
On Day 270 (Fig. 1), i. e. 60 days afterthe surgical pocket elimination, five dogswere sacrificed. In the remaining five dogs,trauma from occlusion of the jiggling typewas introduced on the test side by theinstallation of a cap splint and a bar devicein the manner described by Svanberg &Lindhe (1973). Hence, on the left side ofthe maxilla each animal was supplied witha cap splint fitted with an oblique planewhich made primary contact with the lowerleft fourth premolar (P4). Following instal-lation of the cap splint the incisors did notreach contact in centric occlusion. On theleft side of the mandible the canine and thefirst molar were fitted with crowns whichwere connected with a lingual bar. A springwas attached to the bar and was also intro-duced through a channel in the crown of P4.When the animal discluded, the springpulled P4 back to its original position. Inorder to obtain similar conditions on bothsides of the jaws, the right lower jaw(control side) was supplied with a similarbar and spring device. No force, however,was produced by the spring on 4P. Sixmonths after the installation of the capsplint and bar device, i. e. day 450 (Fig. 1),the remaining five dogs were sacrificed.
Clinical AssessmentsOn day 0, 210, 270 and 450 (Fig. 1) thedogs were subjected to the following clinicalexaminations:Tooth mobility. T 500-values for 4P andP4 were assessed in accordance with themethod described by Miihlemann (1954).
118 ERICSSON AND LINDHE
Attachment level. On the mesial aspectof jP and P4 the distance was measuredbetween an amalgam mark made in thecrown of each tooth and the bottom of themesial periodontal pocket (Lindhe et al.1973).Alveolar bone level. Standardized radio-graphs were ohtained of the marginal al-veolar bone in the 4P and P, regions in ac-cordance with a modification, of a methoddescribed by Eggen (1969) and Lindhe et al.(1973). The radiographs were developed ina standardized way and placed in a Dia-visor® (Esselte, Sweden) which produces amagnified (X 10) image of the radiographon a glass screen. The outline of the mar-ginal alveolar bone, the contours, as well asparticular landmarks on the premolars werereproduced on a transparent paper. Usingthe tracings representing day 0 as a guide,the radiographs obtained on days 210, 270and 450 were placed in a Diavisor and theoutlines of the "new" marginal alveolarbone levels were traced on the same paper.This method of assessing bone level altera-tions was recently described in detail byRosiing et al. (1976a).
In the reproductions of the radiographsthe following distanees were measured:
1. CEJ - the apex of the mesialroot
2. CEJ - the corona] level of themarginal alveolar bone.
The measurements were confined to themesial parts of P̂ and P^; the bone levelalterations were expressed as percentagereduction in relation to the length of themesial root.
Histological AssessmentsFollowing sacrifice, the mandibles were dis-sected and divided along the midline. Speci-mens containing the distal portion of thethird premolar, the fourth premolar andthe mesial portion of the first molar wereharvested, fixed in formalin, decalcified in
formic acid, dehydrated and embedded inparaffin. Mesio-distal sections were cut withthe microtome set at 4 p.m apart. The sec-tions were stained with hematoxyfin andeosin. From each biopsy five; sections,20 v̂m apart, were selected. They weremagnified (x 98.4) in a microscope (Leitz,Orthoplan®) and their images depicted onwhite paper. The size of the mesial peri-odontai ligament area (PLA) of 4P and P4was determined by the use of a planimeter(9527-12 Ingut polar compensating plani-meter, Ingut Ltd, Sweden) in the manner
- JE
A
! , C E J - J £
2. CEJ-APEX
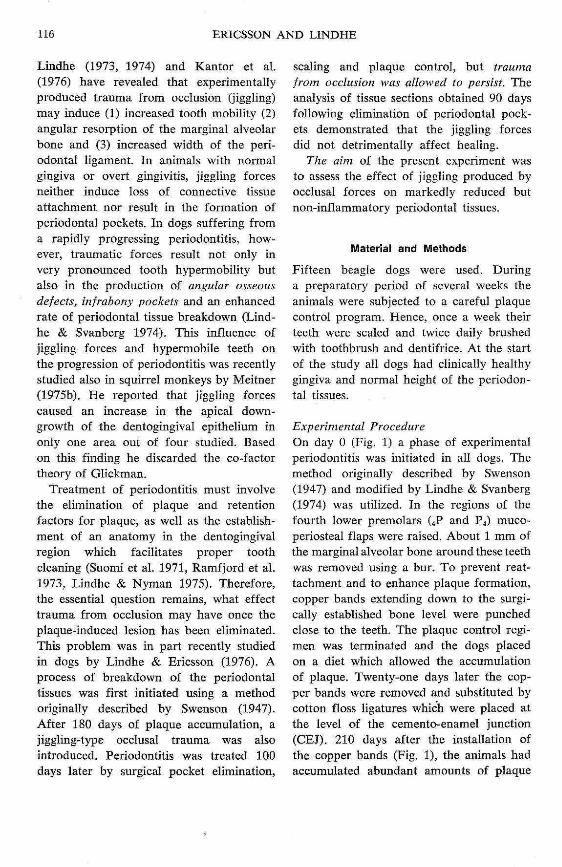
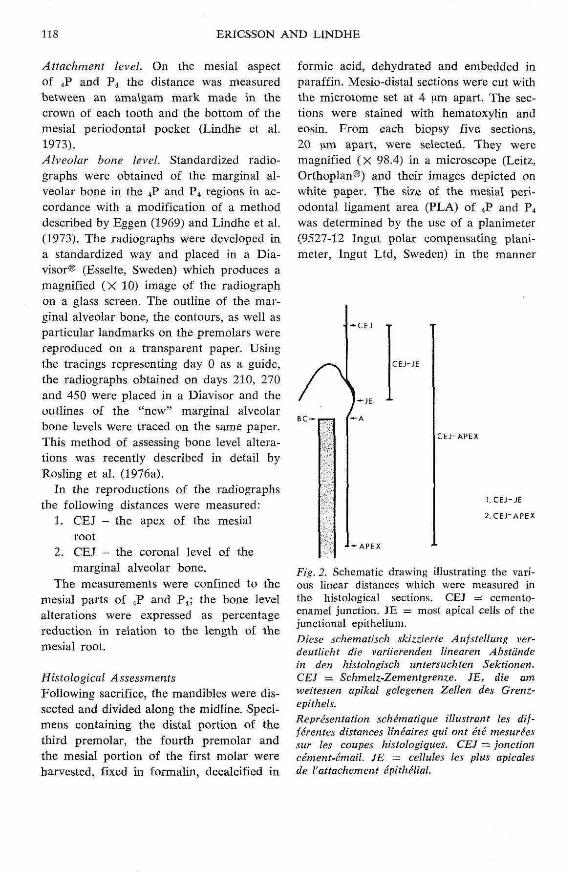
Fig. 2. Schematic drawing illustrating the vari-ous linear distanees which were measured inthe histological sections. CEJ = cemento-enamel junction. JE = most apical celk of thejunctiona! epithelium.Diese schematisch skizzierte Aufsteltung ver~deutlicht die variierenden Unearen Abstandein den histologisch untersuchten Sektionen.CEJ = Schmeiz-Zementgrenze. JE, die am.weitesten apikal gelegenen Zellen des Grenz-epithels.Representation schematique illustrant les dif-fcrentes distanees lineaires Qtii ont ete mesureessur les coupes histologiques. CEJ ~ jonctioncement-email. JE — cellules les plus apicalesde I'attachement epithelial.
TRAUMATIC OCCLUSION AND RECURRENT PERIODONTITIS
described by Svanherg & Lindhe (1973).The vascular cross-section area (VCA)within the PLA was also assessed plani-metrically.
In the sections the linear distances be-tween (1) CEJ and the most apical cells ofJE (2) CEJ and apex of the mesial root,(Fig. 2) were assessed. Loss of connectivetissue attachment was expressed as the quo-
tient 100(%).
Results
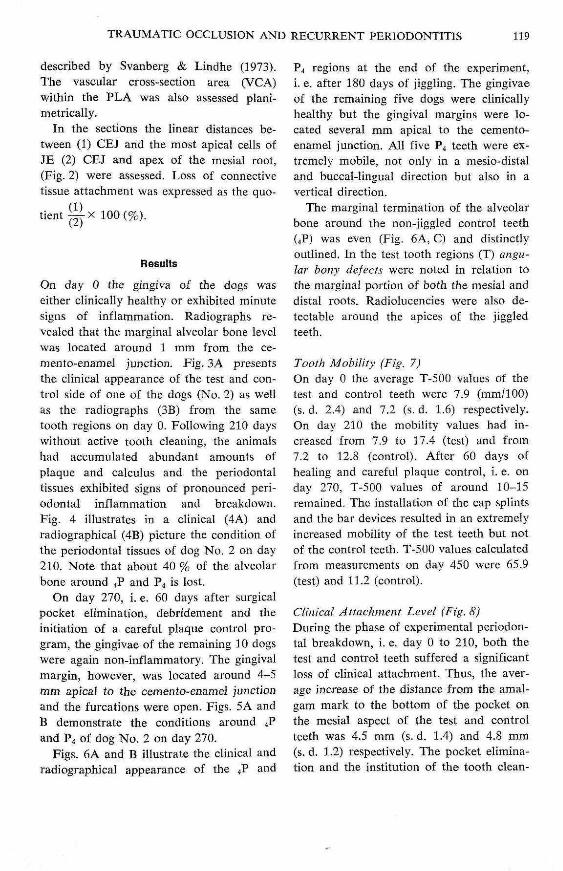
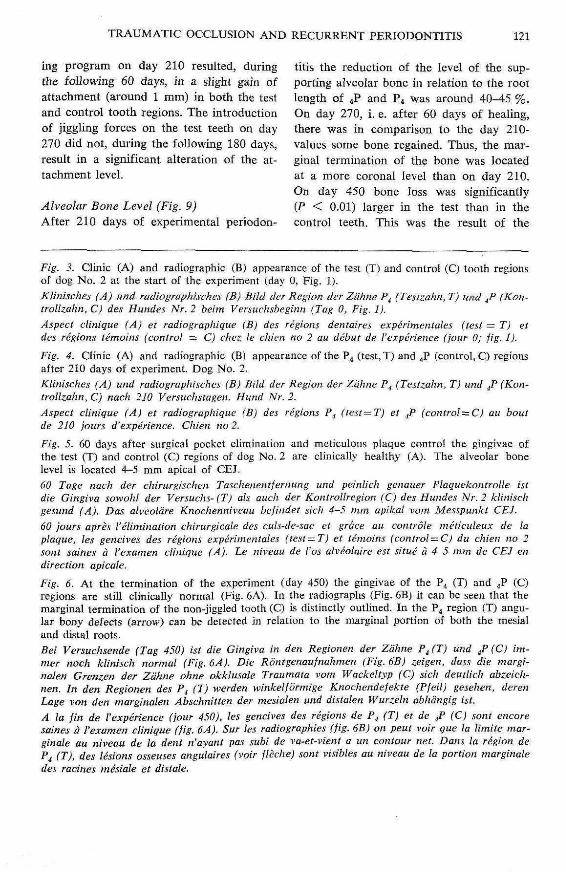
On day 0 the gingiva of the dogs waseither clinically healthy or exhibited minutesigns of inflammation. Radiographs re-vealed that the marginal alveolar bone levelwas located around 1 mm from the ce-mento-enamel junction. Fig. 3A presentsthe clinical appearance of the test and con-trol side of one of the dogs (No. 2) as wel!as the radiographs (3B) from the sametooth regions on day 0. Following 210 dayswithout active tooth cleaning, the animalshad accumulated abundant amounts ofplaque and calculus and the periodontaltissues exhibited signs of pronounced peri-odontal inflammation and breakdown.Fig. 4 illustrates in a chnical (4A) andradiographical (4B) picture the condition otthe periodonta! tissues of dog No. 2 on day210. Note that about 40 % of the alveolarbone around 4P and P,i is lost.
On day 270, i. e. 60 days after surgicalpocket elimination, debridement and theinitiation of a careful plaque control pro-gram, the gingivae of tbe remaining 10 dogswere again non-inflammatory. The gingivalmargin, however, was located around 4-5mm apical to the cemento-enamel junctionand the furcations were open. Figs. 5A andB demonstrate the conditions around 4Pand P4 of dog No. 2 on day 270.
Figs. 6A and B illustrate the clinical andradiographical appearance of the iP and
P4 regions at the end of the experiment,i. e. after 180 days of jiggling. The gingivaeof the remaining five dogs were clinicallyhealthy but the gingival margins were lo-cated several mm apical to the cemento-enamel junction. All five P4 teeth were ex-tremely mobile, not only in a mesio-distaland buccal-lingual direction but also in avertical direction.
TTie marginal termination of the alveolarhone around the non-jiggled control teeth(4P) was even (Fig. 6A, C) and distinctlyouthned. In the test tooth regions (T) angu-lar bony defects were noted in relation tothe marginal portion of both the mesial anddistal roots. Radiolucencies were also de-tectable aronnd the apices of the jiggledteeth.
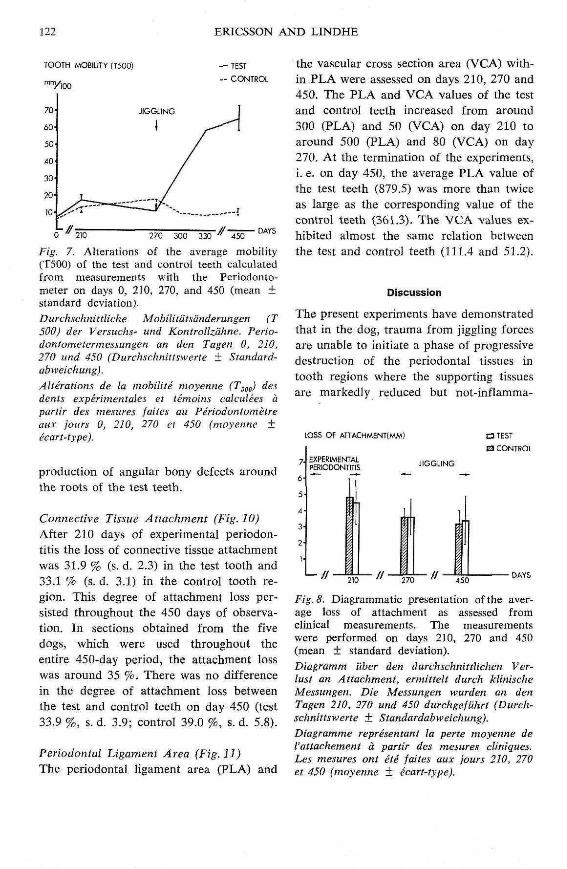
Tooth Mobility (Fig. 7)On day 0 the average T-500 values of thetest and control teeth were 7.9 (mm/100)(s. d. 2.4) and 7.2 (s. d. 1.6) respectively.On day 210 the mobility values had in-creased from 7.9 to 17.4 (test) and from7.2 to 12.8 (control)- After 60 days ofhealing and careful plaque control, i. e. onday 270, T-500 valnes of around 10-15remained. The installation of the cap splintsand the bar devices resulted in an extremelyincreased mobility of the test teeth but notof the control teeth. T-500 values calculatedfrom measurements on day 450 were 65.9(test) and 11.2 (control).
Clinical Attachment Level (Fig. 8}During the phase of experimental periodon-tal breakdown, i. e. day 0 to 210, both thetest and control teeth suffered a significantloss of clinical attachment. Thus, the aver-age increase of the distance from the amal-gam mark to the bottom of the pocket onthe mesial aspect of the test and controlteeth was 4.5 mm (s. d. 1.4) and 4.8 mm(s. d. 1.2) respectively. The pocket elimina-tion and the institution of the tooth clean-
120 ERICSSON AND LINDHE
Fig. 3A Fig. SB
DO
D 2 70
Fig. 6A Fig. 6B
TRAUMATIC OCCLUSION AND RECURRENT PERTODONTITIS 121
ing program on day 210 resulted, during titis the reduction of the level of the sup-the following 60 days, in a slight gain of porting alveolar bone in relation to the rootattachment (around 1 mm) in both the test length of 4P and P4 was around 40-45 %.and control tooth regions. The introduction On day 270, i. e. after 60 days of healing,of jiggling forces on the test teeth on day there was in comparison to the day 210-270 did not, during the following 180 days, values some bone regained. Thus, the mar-result in a significant alteration of the at- ginal termination of the bone was locatedtachment level. at a more coronal level tiian on day 210.
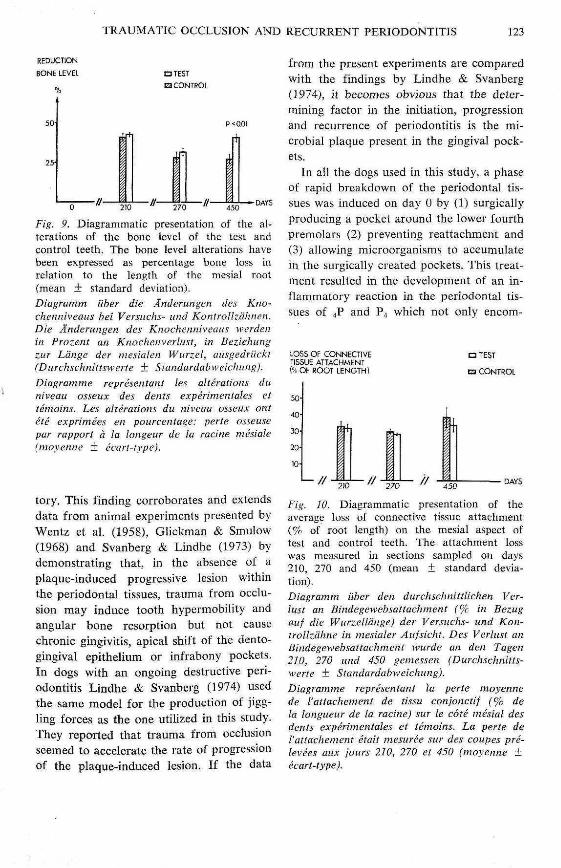
On day 450 bone loss was significantlyAlveolar Bone Level (Fig. 9) (P < 0.01) larger in the test than in theAfter 210 days of experimental periodon- control teeth. This was the result of the
Fig. 3. Clinic (A) and radiographic (B) appearance of the test (T) and control (C) tooth regionsof dog No. 2 at the start of the experiment (day 0, Fig. 1).Kliiiisches (A) und radiographisches (B) Bild der Region der Zdhne P^ (Testzahn, T) und J^ (Kon-trollzahn, C) des Hundes Nr. 2 beim Versuchsbeginn (Tag 0, Fig. 1).Aspect clinigue (A) et radiographique (B) des regions dentaires experimentaies {test — T) etdes regions temoins (control =: C) chez le chien no 2 au debut de Vexperience (jour 0; fig. 1).Fig. 4. Clinic (A) and radiographic (B) appearance of the P^ (test, T) and P̂ (control, C) regionsafter 210 days of experiment. Dog No. 2.Klinisches (A) und radiographisches (B) Bild der Region der Zahne F^ (Testzahn, T) und jP (Kon-trollzahn, C) nach 210 Versuchslagen. Hund Nr. 2.Aspect clinigue (A) et radiographique fJS) des regions F^ (lesi = T) et ^P (contro!. = C) au boutde 210 lours d'experience. Chien no 2.Fig. 5. 60 days after surgical pocket elimination and meticulous plaque control the gingivae ofthe test (T) and control (C) regions of dog No. 2 are clinically healthy (A). The alveolar bonelevel is located 4-5 mm apical of CEJ.60 Tage nach der chirurgischen Taschenentfernung und peiniieh genauer Plaquekontrolle isldie Gingiva sowohl der Versuchs- (T) ah auch der Kontroilregion (C) des Hundes Nr. 2 klinischgesund (A). Das alveolare Knochenniveau befindet sick 4-5 mm apikal vom Messpunkt CEJ.60 jours apres I'ellminalion chirurgicale des culs-de-sac et grace au controle meticuleux de laplaque, les gencives des regions experimentaies (test=.T) et temoins (control = C) du chien no 2sont saines a Vexamen clinique (A). Le niveau de I'os alveolaire est situe a 4-5 mm de CEJ endirection apieale.Fig. 6. At the termination of the experiment (day 450) the gingivae of the P^ (T) and ^P (C)regions are still clinically normal (Fig. 6A). In the radiographs (Fig. 6BJ it can be seen that themarginal termination of the non-jiggled tooth (C) is distinctly outlined. In the P^ region (T) angu-lar bony defects (arrow) can be detected in relation to the marginal portion of both the mesialand distal roots.Bei Versuchsende (Tag 450) ist die Gingiva in den Regionen der Zdhne P^ (T) und J' (C) im-nier noch klinisch normal (Fig. 6Aj. Die Rontgenaufnahmen (Fig. 6B) zeigen, dass die margi-nalen Grenzen der Zdhne ohne okklusale Traumata vom Wackeltyp (C) sick deutlich abzeich-nen. In den Regionen des P^ (T) werden winkelformige Knochendefekte (Pjeilj gesehen, derenLage von den marginalen Abschnitten der mesialen und distalen Wurzeln abhangig ist.A la fin de Vexperience (jour 450), les gencives des regions de P^ (T) et de ^P (C) sont encoresaines a Vexamen clinique (fig. 6A). Sur les radiographies (fig. 6B) on peut voir gue la limite mar-ginale au niveau de la dent n'ayant pas subi de va-et-vient a un contour net. Dam la region dePj (T), des lesions osseuses angulaires (voir flcche) sont visibles au niveau de la portion marglnaledes racines mesiale et distale.
322 ERICSSON AND LINDHE
TOOTH MOBILITY (T500)
270 300 330 450DAYS
Fig. 7. Alterations of the average mobility(T500} of the test and control teeth calculatedfrom measurements with the Periodonto-meter on days 0, 210, 270, and 450 (mean ±standard deviation).Durchschnittliche Mobiiitalsunderungen (T500) der Versuchs' und Kontrollzahne. Perio-dontometermessungen an den Tagen 0, 210,270 und 450 (Durchschnittswerte + Standard-abweichung).Alterations de la mobilite moyenne (T.^gg) desdents experimentales el temoins caiculees apartir des mesures faites au Periodontometreaux jours 0, 210, 270 el 450 (moyenne ±ecart-type).
production of angular bony defects aroundthe roots of the test teeth.
Connective Tissue Attachment (Fig. 10)After 210 days of experimental periodon-titis the loss of connective tissue attachmentwas 31.9 % (s. d. 2.3) in the test tooth and33.1 % (s. d. 3.1) in the control tooth re-gion. This degree of attachment loss per-sisted throughout the 450 days of observa-tion. In sections obtained from the fivedogs, which were used throughout theentire 450-day period, the attachment losswas around 35 %. There was no differencein the degree of attachment loss betweenthe test and control teeth on day 450 (test33.9 %, s. d. 3.9; control 39.0 %, s. d. 5.8).
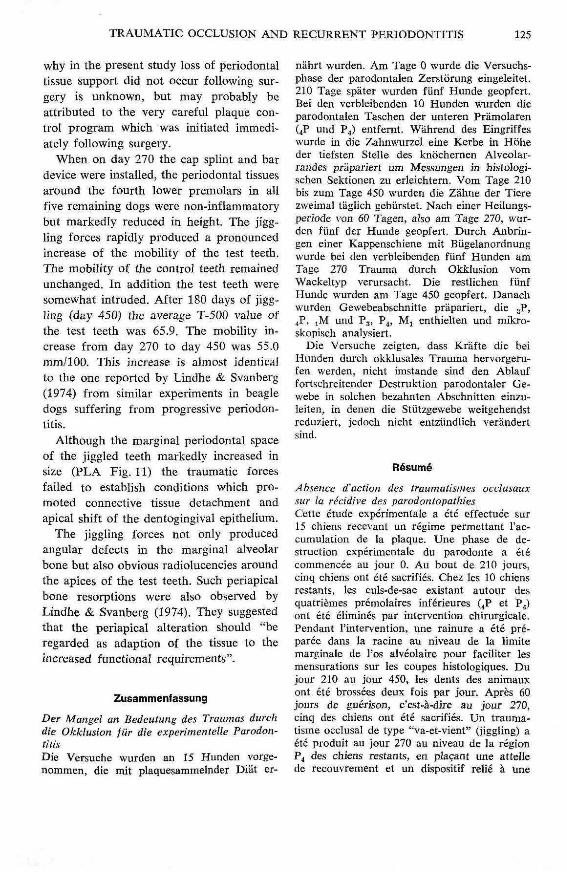
Periodontal Ligament Area (Fig. JJ)The periodontai ligament area (PLA) and
the vascular cross section area (VCA) with-in PLA were assessed on days 210, 270 and450. The PLA and VCA values of the testand control teeth increased from around300 (PLA) and 50 (VCA) on day 210 toaround 500 (PLA) and 80 (VCA) on day270. At the termination of the experiments,i. e. on day 450, the average PLA value ofthe test teeth (879.5) was more than twiceas large as the corresponding value of thecontrol teeth (361.3). The VCA values ex-hibited almost the same relation betweenthe test and control teeth (111.4 and 51.2).
Discussion
The present experiments have demonstratedthat in the dog, trauma from jiggling forcesare unable to initiate a phase of progressivedestruction of the periodontal tissues intooth regions where the supporting tissuesare markedly reduced but not-inflamma-
LOSS OF ATTACHMENT(MMJ a TEST
P CONTROLEXPERIMENTALPERIODONTITIS
Fig. 8. Diagrammatic presentation of the aver-age loss of attachment as assessed fromclinical measurements. The measurementswere performed on days 210, 270 and 450(mean ± standard deviation).Diagramm uber den durchschnittlichen Ver-lust an Attachment, ermittelt durch klinischeMessungen. Die Messungen wurden an denTagen 210. 270 und 450 durchgefiihrt (Durch-schnittswerte ± Standardabweichung).Diagramme representant la perte moyenne deI'attachement ci partir des mesures cliniques.Les mesures ont He faites aux jours 210, 270et 450 (moyenne + ecart-type).
TRAUMATIC OCCLUSION AND RECURRENT PERIODONTITIS 123
REDUCTiON
BONE LEVEL OTESTB3 CONTROL
Fig. 9. Diagrammatic presentation of the al-terations of the bone level of the test andcontrol teeth. The bone level alterations havebeen expressed as percentage bone loss inrelation to the length of the mesial root(mean ± standard deviation).Diagramm iiber die Anderungen des Kno-ehenniveaus bei Ver.^iichs~ und Kontrollzahncn.Die Anderungen des Knochenniveaus werdenin Prozent an Knochenverlust, in Bcziehungzur Ldnge der mesialen Wurzel, ausgedriickt(Durehschnittswerte ± Slandardabweiehungj.Diagramme representant les alterations duniveau osseux des dents experimentaies ettemoins. Les alterations du niveau osseux ontete exprimees en pourcentage: perte osseusepar rapport a la longeur de la racine mesiale(moyenne ± ecari-type).
tory. This finding corroborates and extendsdata from animal experiments presented byWentz et al. (1958), Glickman & Smulow(1968) and Svanberg & Lindhe (1973) bydemonstrating that, in the absence of aplaque-induced progre.ssive lesion withinthe periodontal tissues, trauma from occlu-sion may induce tooth hypermobility andangular bone resorption but not causechronic gingivitis, apical shift of the dento-gingival epithelium or infrabony pockets.In dogs with an ongoing destructive peri-odontitis Lindhe & Svanberg (1974) usedthe same model for the production of jigg-ling forces as the one utilized in this study.They reported that trauma from occlusionseemed to accelerate the rate of progressionof the plaque-induced lesion. If the data
from the present experiments are comparedwith the findings by Lindhe & Svanberg(1974), it becomes obvious that the deter-mining factor in the initiation, progressionand recurrence of periodontitis is the mi-crobial plaque present in the gingival pock-ets.
In ai! the dogs used in this study, a phaseof rapid breakdown of the periodontal tis-sues was induced on day 0 by (1) surgicallyproducing a pocket around the lower fourthpremolars (2) preventing reattachment and(3) allowing microorganisms to accumulatein the surgically created pockets. This treat-ment resulted in the development of an in-flammatory reaction in the periodontal tis-sues of 4P and P4 which not only encom-
LOSS OF CONNECTIVETISSUE ATTACHMENT1% OF ROOT LENGTH)
• TEST
m CONTROL
DAYS
Fig. 10. Diagrammatic presentation of theaverage loss of connective tissue attachment(% of root length) on the mesial aspect oftest and control teeth. The attachment losswas measured in sections sampled on days210, 270 and 450 (mean ± standard devia-tion).Diagramm liber den durehsehnittlichen Ver-lust an Bindegewebsattachment (% in Bezugaiif die Wurzellange) der Versuehs- und Kon-Irollzahne in mesialer Aufsicht. Des Verlust anBindegewebsattachment wurde an den Tagen210, 270 und 450 gemessen (Durehschnitts-werte ± Standardahweichung).Diagramme representant la perte moyennede Vattachement de tissu conjonctif (% dela longueur de la racine) sur le cote mesial desdents experimentaies et temoins. La perte deVattaehement etait mesuree sur des coupes prc-levees aux jours 210, 270 et 450 (moyenne ±ecart-type).

124 ERICSSON AND LINDHE
lOOO'C3TESTdCONTROL
• / /VCA " 210 " 270 " 450
Fig. 11. Diagrammatic presentation of theaverage size of the periodontal ligament area(PLA) and the vascular cross section area(VCA) of the test and control teeth on days210, 270 and 450 (mean ± standard devia-tion).Diagramm iiber die Ouerschnittsbreiten(Durchschnittswerte) der Wurzelhaut (PLA)und der Gefassregion (VCA) bei Versuchs-und Kontrollzahnen an den Tagen 210, 270und 450. (Durchschnittswerte ± Standardab-weichung).Diagramme representant la superficie moy-enne du desmodonte (PLA) et de la sectiontransversale des vaisseaux (VCA) au niveaudes dents experimentales et temoins aux jours210, 270 et 450 (moyenne ± ecart-type).
passed the gingiva but also deteriorateda considerable portion of the periodontalligament and the supporting alveolar bone.The figures describing clinical loss of at-tachment, reduction of alveolar bone heightand loss of connective tissue attachment as-sessed on day 210 revealed that the methodutilized produced a severe lesion but alsothat the destruction could be produced witha high degree of reproducibillty. Similarmodels for production of progressive peri-odontal breakdown have earlier been usedby, e. g. Swenson (1947), Rovin et al.(1966), Kennedy & Poison (1973), Lindhe& Svanberg (1974), Schroeder & Lindhe(1975) and Ericsson et al. (1975). Since the
mere ligature placement will not causebreakdown of the supporting tissues in theabsence of microorganisms (Rovin et al.1966), the ligature in this kind of experi-ment probably operates as a plaque collec-tor and provides in addition to retentionperhaps also particular living conditions forplaque-forming bacteria (Schroeder &Lindhe 1975).
Elimination of the periodontal pockets,calculus and plaque and institution of acareful plaque control program from day210 and onwards resulted in a resolutionof the lesion. Thus, on day 270 the gingivadisplayed no clinical or histological signs ofinflammation. The marginal termination ofthe alveolar bone was smooth and distinctand no signs of an ongoing bone resorptioncould be detected in the histological sec-tions. The fact that elimination of plaqueand calculus and establishment of a properplaque control program resulted in peri-odontal health has earlier been describedby Lindhe et al. (1973) in dogs and bySuomi et al. (1971), Ramfjord et at. (1973,1975) and Lindhe & Nyman (1975) in hu-mans.
During surgery on day 210 a notch wasprepared at the level of the marginal borderof the alveolar bone. In all sections fromthe five dogs sacrificed on day 270 theapical cells of the junctional epitheliumwere found to be located within the notch.Furthermore, the marginal border of thealveolar bone was also located at the notchlevel. This means that the surgical treat-ment neither resulted in further resorptionof the alveolar bone nor in loss of connec-tive tissue attachment. This is at variancewith data presented by Donnenfeldt &Glickman (1964), Pfeifer (1965) and Don-nenfeldt et al. (1970). Rosling et al. (1976b)presented data from a clinical study whichindicated that the surgical treatment of theperiodontal tissues inevitably caused someresorption of alveolar bone. The reason
TRAUMATIC OCCLUSION AND RECURRENT PERIODONTITIS 125
why in the present study loss of periodontaltissue support did not occur following sur-gery is unknown, but may probably beattributed to the very careful plaque con-trol program which was initiated immedi-ately following surgery.
When on day 270 the cap splint and bardevice were installed, the periodontal tissuesaround the fourth lower premolars in ailfive remaining dogs were non-inflammatorybut markedly reduced in height. The jigg-ling forces rapidly produced a pronouncedincrease of the mobility of the test teeth.The mobility of the control teeth remainedunchanged. In addition the test teeth weresomewhat intruded. After 180 days of jigg-hng (day 450) the average T-500 value ofthe test teeth was 65.9. The mobility in-crease from day 270 to day 450 was 55.0mm/100. This increase is almost identicalto the one reported by Lindhe & Svanberg(1974) from similar experiments in beagledogs suffering from progressive periodon-titis.
Although the marginal periodontal spaceof the jiggled teeth markedly increased insize (PLA Fig. 11) the traumatic forcesfailed to estabhsh conditions which pro-moted connective tissue detachment andapical shift of the dentogingival epithelium.
The jiggling forces not only producedangular defects in the marginal alveolarbone but also obvious radiolucencies aroundthe apices of the test teeth. Such periapicalbone resorptions were also observed byLindhe & Svanberg (1974). They suggestedthat the periapical alteration should "beregarded as adaption of the tissue to theincreased functional requirements".
ZusammenfassungDer Mangel an Bedeutung des Traumas durchdie Okklusion fur die experimentelle Parodon-titisDie Versuche wurden an 15 Hunden vorge-nommen, die mit plaquesammelnder Diat er-
nahrt wurden. Am Tage 0 wurde die Versuchs-phase der parodontalen Zerstorung eingeleitet.210 Tage spater wurden fUnf Hunde geopfert.Bei den verbleibenden 10 Hunden wurden dieparodontalen Taschen der unteren Pramolaren(4P und P4) entfemt. Wahrend des Eingriffeswurde in die Zahnwurzei eine Kerbe in Hoheder tiefsten Stelle des knochernen Alveolar-randes prapariert um Messungen in histologi-schen Sektionen zu erleichtem. Vora Tage 210bis zum Tage 450 wurden die Zahne der Tierezweimal tagiich gebiirstet. Nach einer Heilungs-periode von 60 Tagen, also am Tage 270, wur-den funf der Hunde geopfert. Durch Anbrin-gen einer Kappenschiene mit Biigelanordnungwurde bei den verbleibenden fUnf Hunden amTage 270 Trauma durch Okklusion vomWackeltyp verursacht. Die restlichen funfHunde wurden am Tage 450 geopfert. Danachwurden Gewebeabschnitte prapariert, die 3P,4P, iM und P3, P4, Ml enthielten und mikro-skopisch analysiert.
Die Versuche zeigten, dass Krafte die beiHunden durch okklusales Trauma herv'orgeni-fen werden, nicht imstande sind den Ablauffortschreitender Destruktion parodontaler Ge-webe in solchen bezahnten Abschnitten einzu-leiten, in denen die Stlitzgewebe weitgebendstreduziert, jedoch nicht entzUndlich verandertsind.
Resume
Absence d'action des traumatismes occlusauxsur la recidive des parodontopathiasCette etude experimental a ete effectuee sur15 chiens recevant un regime permettant l'ac-cumulation de la plaque. Une phase de de-struction experimentale du parodonte a etecommencee au jour 0. An bout de 210 jours,cinq chiens ont ete sacrifies. Chez les 10 chiensrestants, les culs-de-sac existant autour desquatriemes premolaires inferieures (4P et P )̂ont ete elimines par intervention chirurgicale.Pendant ['intervention, une rainure a ete pre-paree dans la racine au niveau de la limitemarginale de I'os alveolaire pour faciliter lesmensurations sur les coupes histologiques. Dujour 210 au jour 450, les dents des animauxont ete brossees deux fois par jour. Apres 60jours de guerison, c'est-a-dire au jour 270,cinq des chiens ont ete sacrifies. Un trauma-tisme occlusal de type '"va-et-vient" (jiggling) aete produit au jour 270 au niveau de la regionP4 des chiens restants, en pla^ant une attellede recouvrement et un dispositif relie a une
ERICSSON AND LINDHE
barre, Les cinq derniers chiens ont ete sacri-fies au jour 450. Apres le sacrifice, des coupescomprenant 3P. 4P, jM et P3, P^, Mj ont etepreparees et analysees au microscope.
II ressort des resultats de ces experiencesque, chez le chien, les forces produites lors detraumatismes occlusaux ne sont pas en etat decauser une phase de destructioti des tissus paro-dontaux dans les regions dentaires oti les tissusparodontaux sont fortement reduits, mais iioninfiammatoires.
ReferencesDonnenfeldt. O. W. & Glickman, I. (1964) The
apically repositioned flap - a clinical study.Journal of Periodontology 35, 381-387.
Donnenfeldt, O. W., Hoag, P. M. & Weiss-man, D. P. (1970) A clinical study on theeffects of osteoplasty. Journal of Periodonto-logy 41, 131-141.
Eggen, S. (1969) Standardiserad intraoral ront-genteknifc. Sveriges Tandliikarforbunds Tid-ning 17, 867-872.
Ericsson, 1., Lindhe, J., Rylander, H. & Oka-raoto, H. (1975) Experimental periodontalbreakdown in the dog. Scandinavian Journalof Dental Research 83, 189-192.
Friedman, N. (1962) Mucogingival snrgery:The apically repositioned flap. Journal ofPeriodontology 33, 328-340.
Glickman, I. (1963) Inflammation and traumafrom occlusion, co-destructive factors inchronic periodontal disease. Journal of Peri-odontology 34, 5-10.
Glickman, I. (1967) Occlusion and periodon-tium. Journal of Dental Research 46, suppl.I, 53-59.
Glickman, I. & Smulow, J. B. (1968) Adaptivealterations in the periodontium of the Rhesusmonkey in chronic trauma from occlusion.Journal of Periodontology 39, 101-105.
Kantor, M., Poison, A. M. & Zander, H. A.(1976) Reversibility of alveolar bone lossafter removal of causative agents. lADRAbstract No. 981.
Kennedy, J. E. & Poison, A. M. (1973) Experi-mental marginal periodontitis in squirrelmonkeys. Journal of Periodontology 44, 140-144.
Lindhe, J. & Ericsson, I. (1976) The influenceof trauma from occlusion on reduced buthealthy periodontal tissues in dogs. Journalof Clinical Periodontology 3, 110-122.
Lindhe, J., Hamp, S. E. & Loe, H. (1973) Ex-perimental periodontitis in the beagle dog.Journal of Periodontal Research 8, 63-70.
Lindhe, L, Hamp, S. E. & Loe, H. (1975)Plaque-induced periodontal disease in beagledogs. Journal of Periodontal Research 10,243-255.
Lindhe, J. & Nyman, S. (1975) The effect ofplaque control and surgical pocket elimina-tion on the establishment and maintenanceof periodontal health. A longitudinal studyof periodontal therapy in cases of advancedperiodontal disease. Journal of ClinicalPeriodontology 2, 67-77.
Lindhe, J. & Svanberg, G. (1974) Influence oftrauma from occlusion on progression ofexperimental periodontitis in the beagle dog.Journal of Clinical Periodontology 1, 3—14.
Meitner, S. (1975a) Co-destruetive factors ofmarginal periodontitis and repetitive mechan-ical injury. Thesis. Rochester, New York.
Meitner, S. (1975b) Co-destructive factors ofmarginal periodontitis and repetitive mechan-ical injur>'. Journal of Dental Research 54C,78-85.
Muhlemann, H. R. (1954) Tooth mobility. Themeasuring method. Initial and secondarytooth mobility. Journal of Periodontology 25,22-29.
Pfeifer, J. S. (1965) The reaction of alveolarbone to flap procedures in man. Periodon-tics 3, 135-140.
Ramfjord, S. P., Knowles, J. W., Nissle, R. R.,Schick, R. A. & Burgett, F. G. (1973) Longi-tudinal study of periodontal therapy. Journalof Periodontology 44, 66-77.
Ramfjord, S. P., Knowles, J. W., Nissle, R. R.,Burgett, F. G. & Schick, R. A. (1975) Re-sults following three modalities of periodon-tal therapy. Journal of Periodontology 46,522-526.
Rosling, B., Nyman, S. & Lindhe, J. (1976a)The effect of systematic plaque control onbone regeneration in infrabony pockets. Jour-nal of Clinical Periodontology 3, 38-53,
Rosling, B., Nyman, S., Lindhe, J. & Jem, B,(1976b) The healing potential of the peri-odontal tissues following different techniquesof periodontal surgery in plaque-free denti-tions. Journal of Clinical Periodontology 3,233-250.
Rovin, S., Costich, E- & Gordon, H, (1966)The influence of bacteria and irritation inthe initiation of periodontal disease in germ-free and conventional rats. Journal of Peri-odonlal Research 1, 193-204.
TRAUMATIC OCCLUSION AND RECURRENT PERIODONTITIS 127
Saxe, S. R., Greene, 3. C , Bohannan, H. M. &Vermillion, J. R. (1967) Oral debris, calculusand periodontal disease in the beagle dog.Perlodontics 5, 217-225.
Schroeder, H. E. & Lindhe, J. (1975) Conver-sion of stable established gingivitis in thedog into destructive periodontitis. Archivesof Oral Biology 20, 775-782.
Suomi, J. D., Greene J. C , Vermillion, J. R.,Doyle, J., Chang, J. J. & Leatherwood, E. C.(1971) The effeet of controlled oral hygieneprocedures on the progression of periodontaldisease in adults; Results after third and finalyear. Journal oj Periodontology 42, 152-160.
Svanberg, G. (1974) Experimental trauma fromocclusion in the dog. Thesis. Gothenburg.
Svanberg, G. & Lindhe, J. (1973) Experimentaltooth hypermobility in the dog. OdontologlskRevy 24, 269-282.
Svanberg, G., Lindhe, J., Hugosson, A. &Grondahl, H. G. (1973) Effect of nutritionalhyperparathyroidism on experimental peri-
odontitis in the dog. Scandinavian Journal ofDental Research 81, 155-162.
Svanberg, G. & Lindhe, J. (1974) Vascular re-aetions in the periodontal ligament incidentto trauma from oeclusion. Journal of Clini-cal Periodontology 1, 58-69.
Swenson, H. M. (1947) Experimental periodon-tal pockets in dogs. Journal oj Dental Re-search 26, 273-275.
Wentz, F. M., Jarahak, J. & Orban, B. (1958)Experimental occlusal trauma imitatingcuspal interferences. Journal oj Periodonto-logy 29, 117-127.
Address:Department oj PeriodontologyFaculty oj OdontologyFackS-400 33 Gdteborg 33Sweden