Embed Size (px)
Citation preview

Published by Articulate® Storyline www.articulate.com
Laboratory Management Information Systems in Daily Practice
1. Welcome
1.1 Opening Animation
Published by Articulate® Storyline www.articulate.com
1.2 Title + Faculty
Published by Articulate® Storyline www.articulate.com
1.3 Course Outline
Notes:
This course will follow Dr. Jones, a laboratory director, through a scenario in which he will select a new laboratory information system. Click on the buttons to see how the course will develop.
The introduction will: explain why the LIS decision-making process is so important, explain what an LIS is, outline the different LIS models, and introduce the course scenario.
Next, we will discuss functionalities, including LIS architecture and core elements, lab workflow, automation, compliance, and meaningful use.
In the third section, we will address integration factors. In this section we will: outline the other systems with which an LIS integrates, including instruments, HIS, and EMR; explain how an LIS integrates with other systems; as well as explain HL7 and LOINC.
The selection section will outline factors to consider when selecting an LIS and suggest how to organize the selection and contracting process.
Finally, we will conclude by returning to the scenario to discuss recommendations and long-term implementation outcomes. Then, we’ll wrap up by providing final thoughts from the faculty and discuss the future of LISs.
Published by Articulate® Storyline www.articulate.com
Intro 2 (Slide Layer)
1.4 Course Objectives
Notes:
Upon completion of this course, you will: demonstrate knowledge of laboratory information systems, understand how different LIS systems affect your laboratory, understand the process of system integration, and have the ability to assess and select a new laboratory information system.
Published by Articulate® Storyline www.articulate.com
2. Introduction
2.1 What is an LIS?
Notes:
Let’s start by discussing what an LIS is. Click on the computer to learn more.
As the simplest possible definition, a Laboratory Information System, or LIS for short, is the information technology solution - a software program - that allows the clinical laboratory to effectively manage the many classes of data that are concurrently housed or otherwise managed within its walls. In the era of laboratory medicine before the information technology age, functions currently subsumed by the LIS were carried out by the combined use of paper-based log books, note card indexes, and other paper-based systems.
These approaches, although effective in small volume settings, exhibited several key vulnerabilities including the lack of an automatic and systematic method for maintaining redundant copies of information. A simple loss of a single bench log book, for example, could spell disaster for being able to correctly identify specimens and their respective results. In the 1960’s and 1970’s as information technology became a possibility for laboratory use, initial efforts with deployment of computers in the laboratory were quickly able to point out the immense benefit of computational tracking critical categories of lab data.
Published by Articulate® Storyline www.articulate.com
What is an LIS? - Copy (Slide Layer)
Notes:
Additionally, the LIS is often an integral component of one or more electronic interfaces necessary to maintain communications with the healthcare enterprise at large. Examples of high-level functionality that are electronically enabled by the use of an LIS include the following: inbound patient registration data (insurance and demographics), inbound laboratory orders, outbound clinical laboratory results and outbound results addenda and amended findings.
As LISs have evolved, they have taken on additional categories of data stewardship, such as reagent lot tracking, courier tracking, regulatory compliance and lab policy and procedure documentation, to name a few areas. In essence, the LIS has become the “nervecenter” for the lab, where every critical piece of information is available in a single data repository.
Published by Articulate® Storyline www.articulate.com
2.2 Why the Decision is Important
Notes:
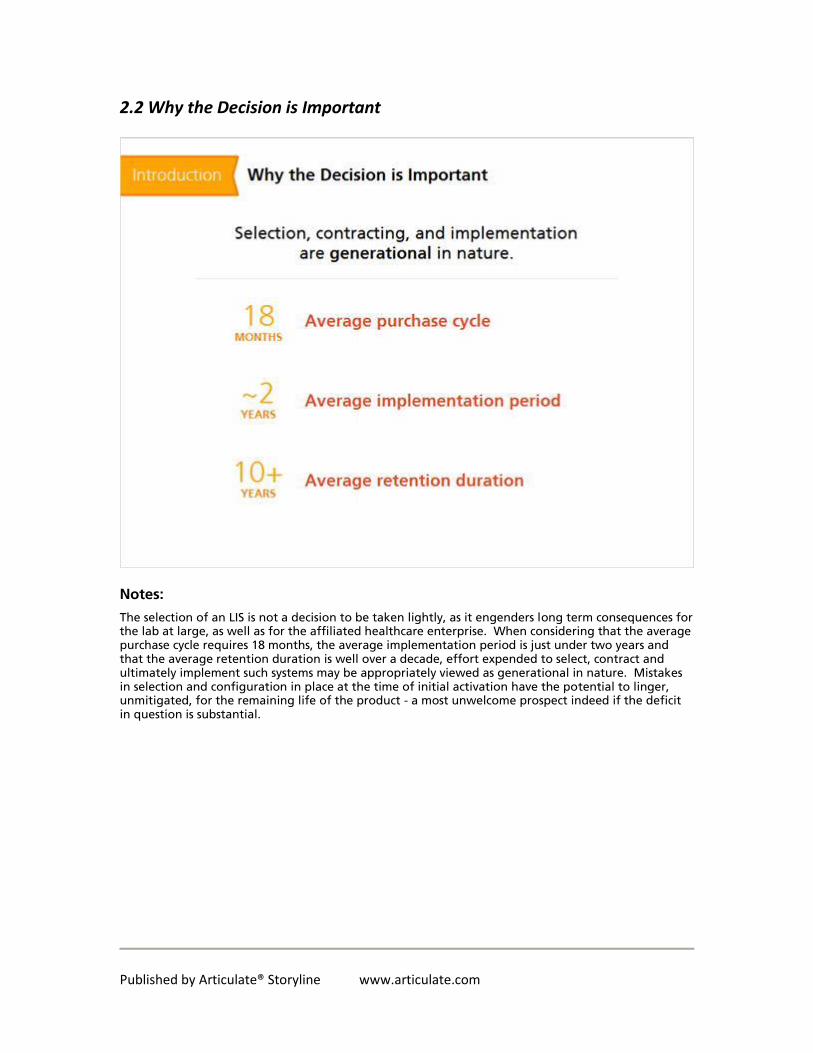
The selection of an LIS is not a decision to be taken lightly, as it engenders long term consequences for the lab at large, as well as for the affiliated healthcare enterprise. When considering that the average purchase cycle requires 18 months, the average implementation period is just under two years and that the average retention duration is well over a decade, effort expended to select, contract and ultimately implement such systems may be appropriately viewed as generational in nature. Mistakes in selection and configuration in place at the time of initial activation have the potential to linger, unmitigated, for the remaining life of the product - a most unwelcome prospect indeed if the deficit in question is substantial.
Published by Articulate® Storyline www.articulate.com
2.3 Email from CIO
Notes:
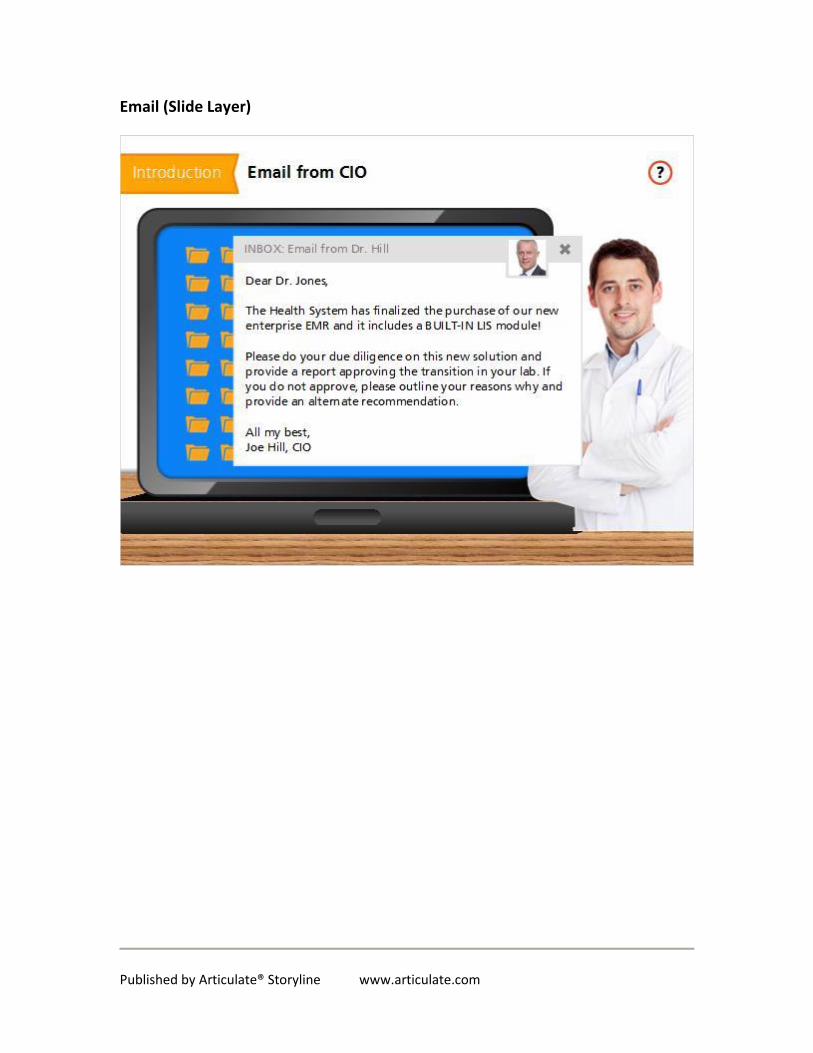
Dr. Jones is a lab director at a large hospital. His lab has a legacy laboratory information system they use for AP, CP, and blood bank. But, recently the CIO of this health system informed Dr. Jones that they have purchased an expensive enterprise EMR solution that includes a "built-in" LIS module. She asks Dr. Jones to decide if this would be a beneficial transition for his lab. It looks like Dr. Jones has received an email from the CIO. Click on the inbox icon to read the email.
Published by Articulate® Storyline www.articulate.com
Email (Slide Layer)
Published by Articulate® Storyline www.articulate.com
2.4 What NOT to Do
Notes:
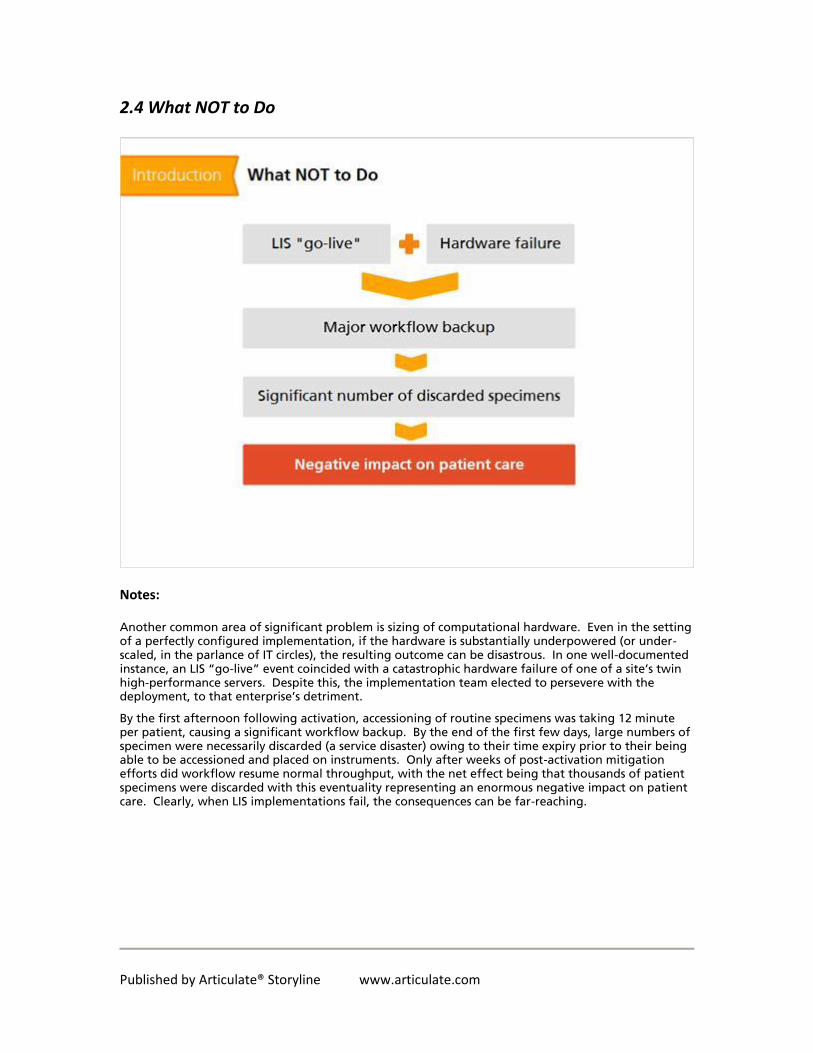
Another common area of significant problem is sizing of computational hardware. Even in the setting of a perfectly configured implementation, if the hardware is substantially underpowered (or under-scaled, in the parlance of IT circles), the resulting outcome can be disastrous. In one well-documented instance, an LIS “go-live” event coincided with a catastrophic hardware failure of one of a site’s twin high-performance servers. Despite this, the implementation team elected to persevere with the deployment, to that enterprise’s detriment.
By the first afternoon following activation, accessioning of routine specimens was taking 12 minute per patient, causing a significant workflow backup. By the end of the first few days, large numbers of specimen were necessarily discarded (a service disaster) owing to their time expiry prior to their being able to be accessioned and placed on instruments. Only after weeks of post-activation mitigation efforts did workflow resume normal throughput, with the net effect being that thousands of patient specimens were discarded with this eventuality representing an enormous negative impact on patient care. Clearly, when LIS implementations fail, the consequences can be far-reaching.
Published by Articulate® Storyline www.articulate.com
2.5 Upcoming Laboratory Plans
Notes:
As Dr. Jones begins this process, he must consider the upcoming plans of his laboratory. These are: the lab’s plan to grow their outreach business with clients outside of its health system, the need to start a blood donor program, and the lab’s intent to start performing more molecular tests including next generation sequencing in house.
Published by Articulate® Storyline www.articulate.com
3. Functionalities
3.1 Core Elements
Notes:
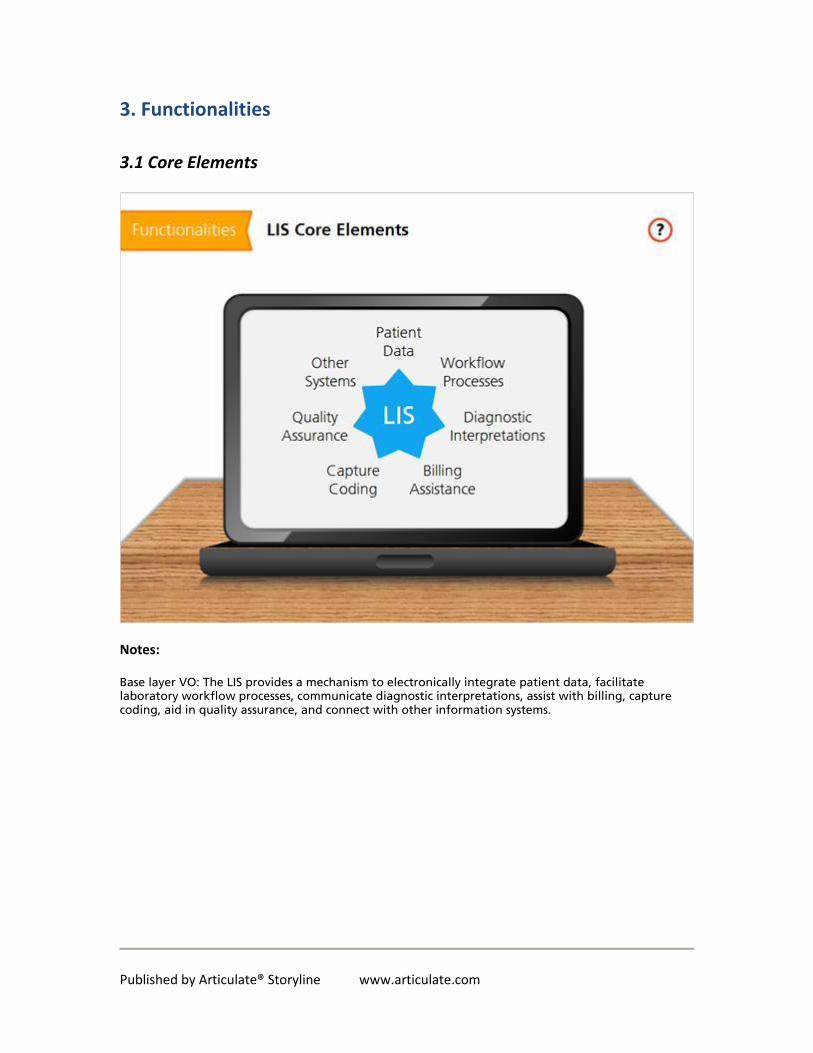
Base layer VO: The LIS provides a mechanism to electronically integrate patient data, facilitate laboratory workflow processes, communicate diagnostic interpretations, assist with billing, capture coding, aid in quality assurance, and connect with other information systems.
Published by Articulate® Storyline www.articulate.com
3.2 Building Blocks of Lab Information Systems
Notes:
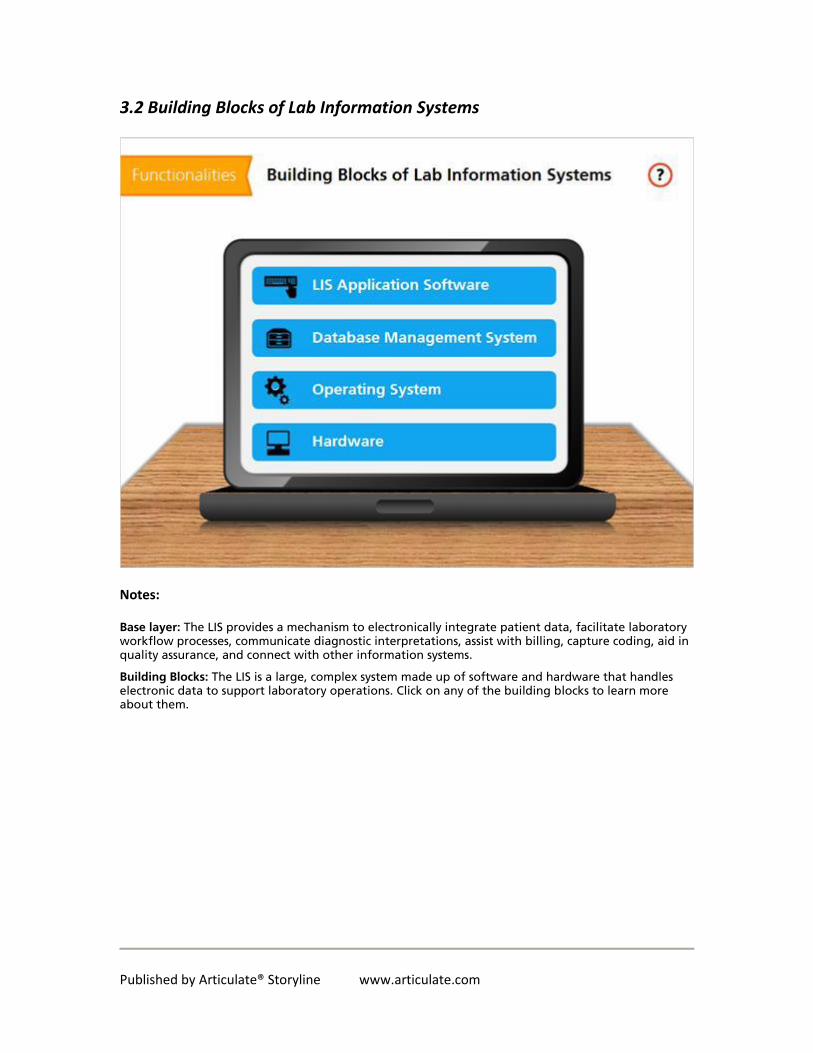
Base layer: The LIS provides a mechanism to electronically integrate patient data, facilitate laboratory workflow processes, communicate diagnostic interpretations, assist with billing, capture coding, aid in quality assurance, and connect with other information systems.
Building Blocks: The LIS is a large, complex system made up of software and hardware that handles electronic data to support laboratory operations. Click on any of the building blocks to learn more about them.
Published by Articulate® Storyline www.articulate.com
3.3 LIS Application Software
LIS Application Software: The software layer used to perform predefined laboratory functions is the LIS application software. On the “front end” (user view) laboratory staff interact with this layer of the LIS by using built-in user interfaces. On the “back end” (administrative view) the LIS application software interacts with the Database Management System (DBMS) or with computer/network hardware, to communicate the user’s commands.
Published by Articulate® Storyline www.articulate.com
3.4 DBMS
DBMS: Databases are the core of any LIS. They store all the information related to patients, specimens and test results, as well information related to various steps in the workflow of the laboratory. Data in the LIS are stored and organized in files (often called dictionaries or maintenance tables) that are structured (typically in a relational database) based on pre-defined formats and templates.
These maintenance files are components of the LIS database that play a significant role in defining data formats, structures, and rules. Examples of dictionaries include tables that contain specimen part types, list of doctor’s names, menu of special stains, billing codes, users passwords, and so on. These electronic databases are managed by specialized software called a Database Management System (DBMS), which helps control the access, organization, storage, management, querying and retrieval of data.
Published by Articulate® Storyline www.articulate.com
3.5 Operating System
Operating System: The operating system (OS) is a complex set of programs that manages all the hardware and software resources (program applications). The OS allows the LIS applications to communicate and control the computer hardware resources such as memory, portals, peripheral devices, and networking. The main operating systems currently in use are Microsoft Windows, Mac OS, UNIX and Linux.
Published by Articulate® Storyline www.articulate.com
3.6 Hardware
Hardware: LIS hardware components include computers (servers, workstation personal computers, and terminals), networking equipment and peripheral devices (e.g. printers, fax machines, barcode scanners, digital imaging devices, etc.).
Published by Articulate® Storyline www.articulate.com
3.7 LIS Architecture
Notes:
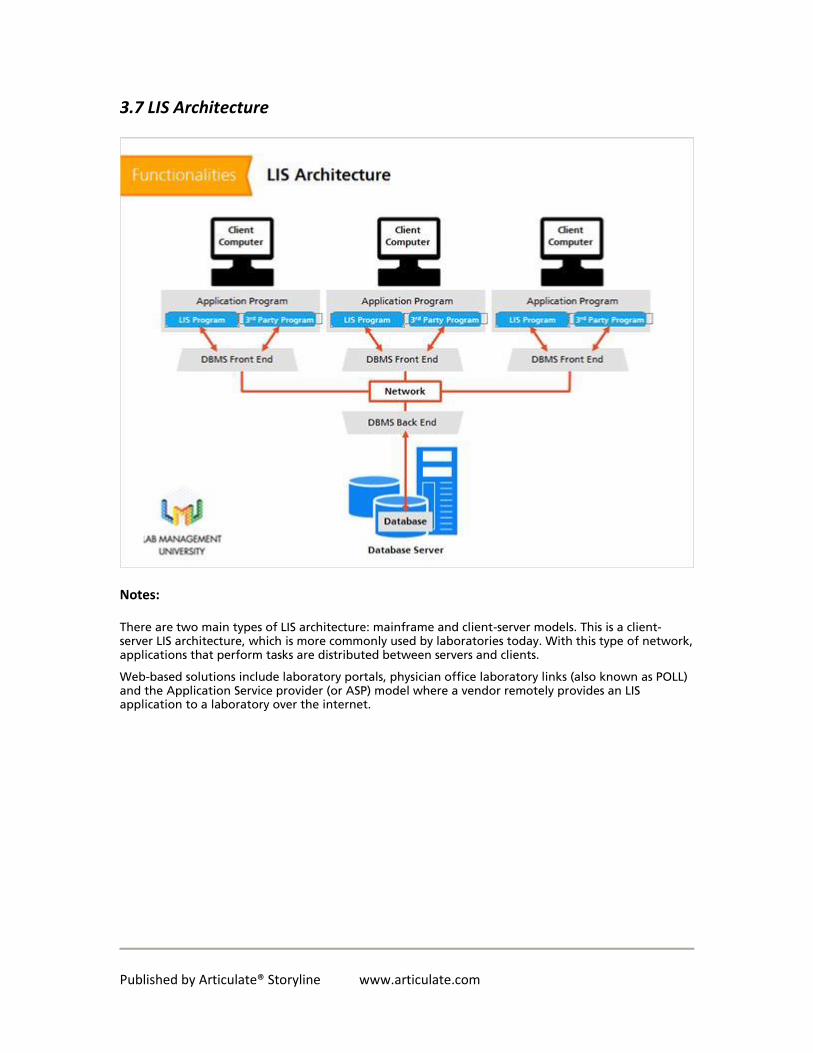
There are two main types of LIS architecture: mainframe and client-server models. This is a client-server LIS architecture, which is more commonly used by laboratories today. With this type of network, applications that perform tasks are distributed between servers and clients.
Web-based solutions include laboratory portals, physician office laboratory links (also known as POLL) and the Application Service provider (or ASP) model where a vendor remotely provides an LIS application to a laboratory over the internet.
Published by Articulate® Storyline www.articulate.com
3.8 Lab Workflow
Notes:
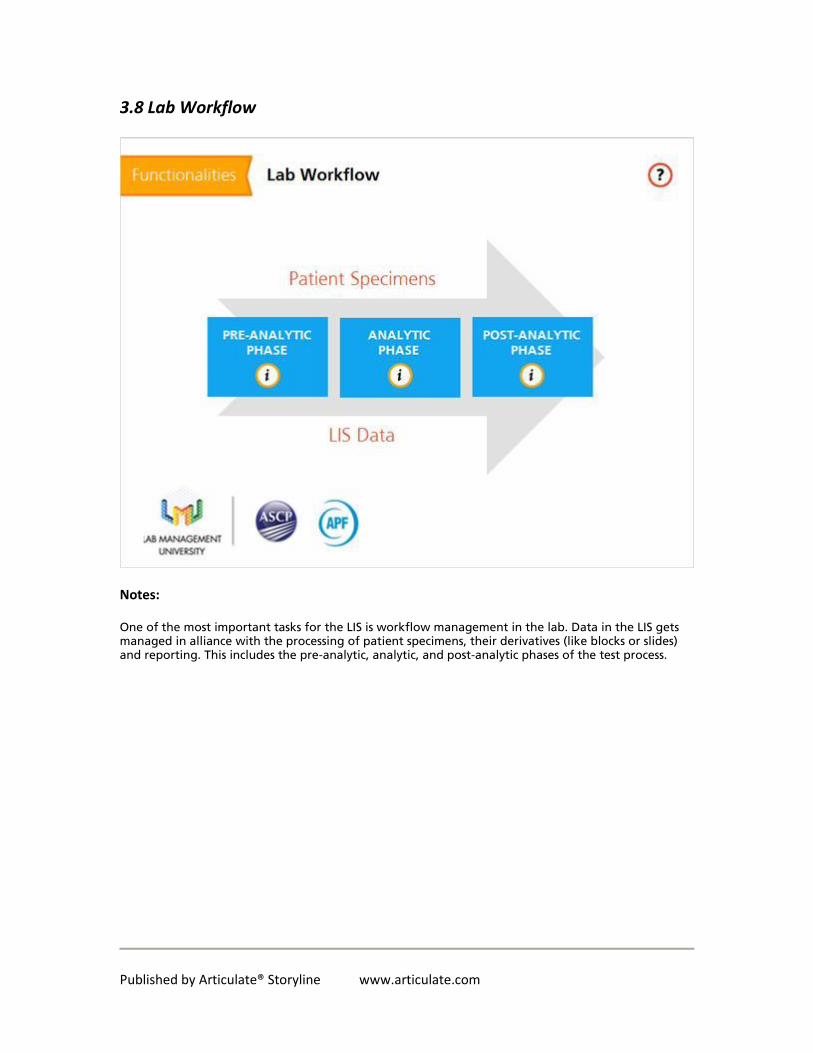
One of the most important tasks for the LIS is workflow management in the lab. Data in the LIS gets managed in alliance with the processing of patient specimens, their derivatives (like blocks or slides) and reporting. This includes the pre-analytic, analytic, and post-analytic phases of the test process.
Published by Articulate® Storyline www.articulate.com
3.9 Automation
Notes:
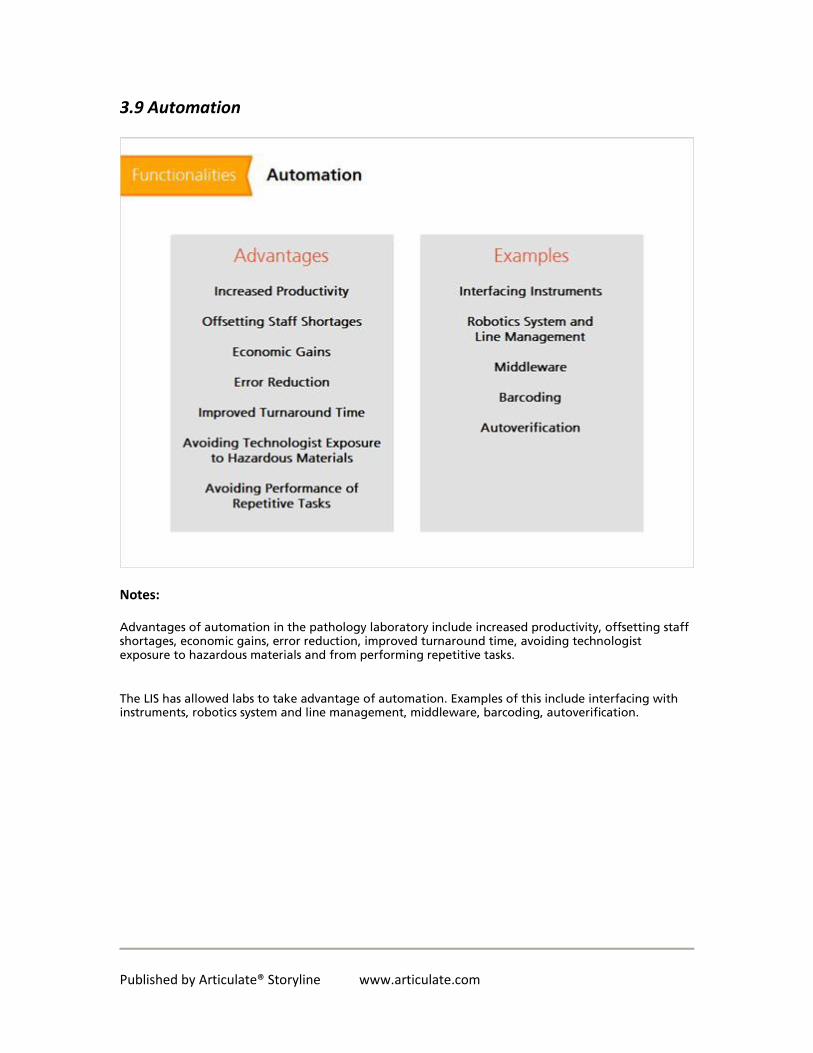
Advantages of automation in the pathology laboratory include increased productivity, offsetting staff shortages, economic gains, error reduction, improved turnaround time, avoiding technologist exposure to hazardous materials and from performing repetitive tasks.
The LIS has allowed labs to take advantage of automation. Examples of this include interfacing with instruments, robotics system and line management, middleware, barcoding, autoverification.
Published by Articulate® Storyline www.articulate.com
3.10 Compliance
Notes:
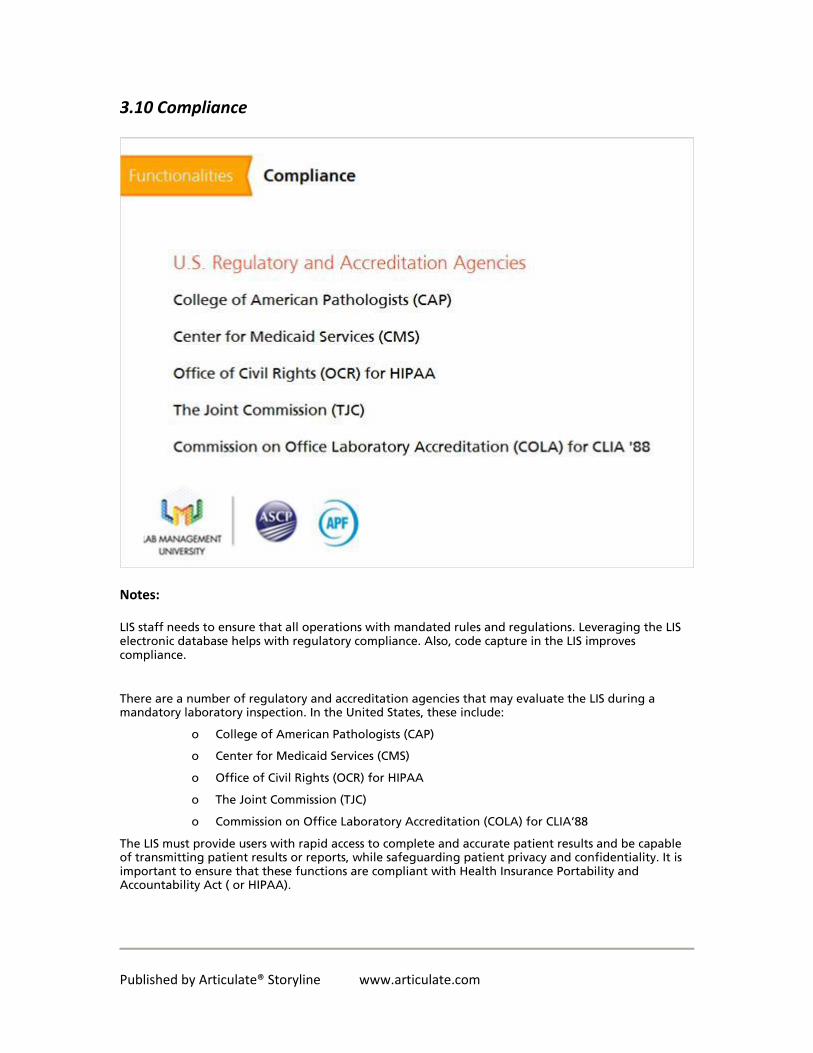
LIS staff needs to ensure that all operations with mandated rules and regulations. Leveraging the LIS electronic database helps with regulatory compliance. Also, code capture in the LIS improves compliance.
There are a number of regulatory and accreditation agencies that may evaluate the LIS during a mandatory laboratory inspection. In the United States, these include:
o College of American Pathologists (CAP)
o Center for Medicaid Services (CMS)
o Office of Civil Rights (OCR) for HIPAA
o The Joint Commission (TJC)
o Commission on Office Laboratory Accreditation (COLA) for CLIA’88
The LIS must provide users with rapid access to complete and accurate patient results and be capable of transmitting patient results or reports, while safeguarding patient privacy and confidentiality. It is important to ensure that these functions are compliant with Health Insurance Portability and Accountability Act ( or HIPAA).
Published by Articulate® Storyline www.articulate.com
3.11 Meaningful Use
Notes:
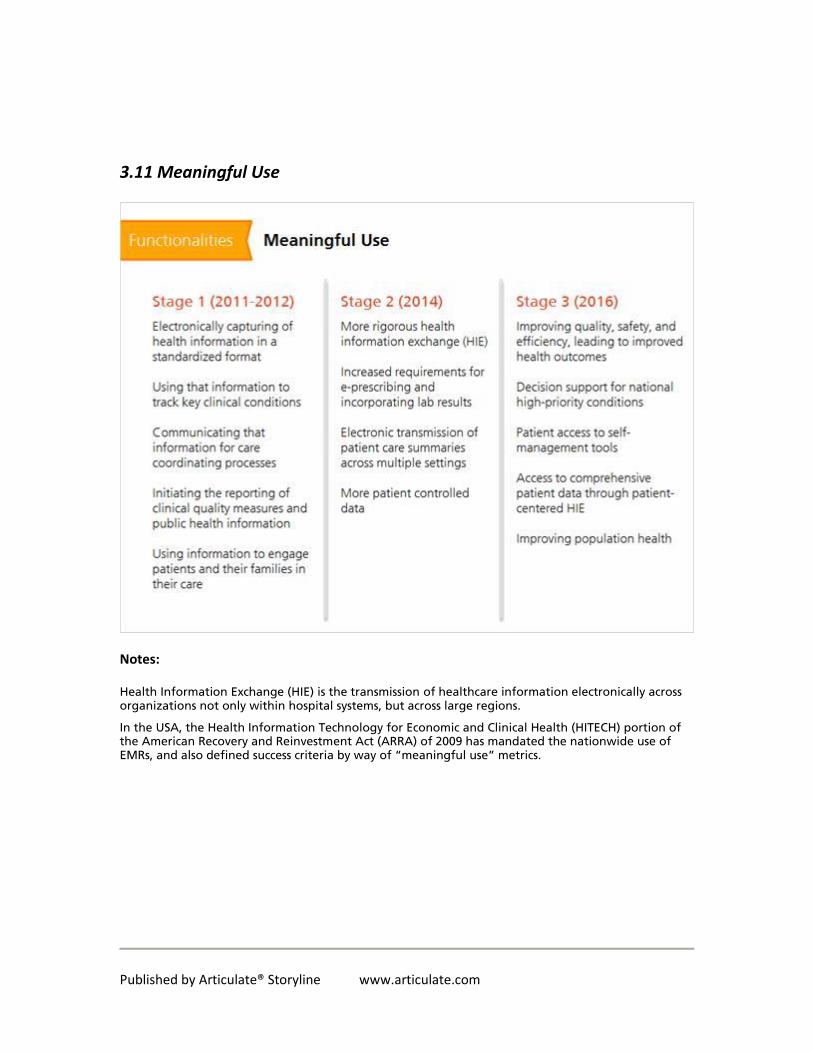
Health Information Exchange (HIE) is the transmission of healthcare information electronically across organizations not only within hospital systems, but across large regions.
In the USA, the Health Information Technology for Economic and Clinical Health (HITECH) portion of the American Recovery and Reinvestment Act (ARRA) of 2009 has mandated the nationwide use of EMRs, and also defined success criteria by way of “meaningful use” metrics.
Published by Articulate® Storyline www.articulate.com
3.12 Knowledge Check
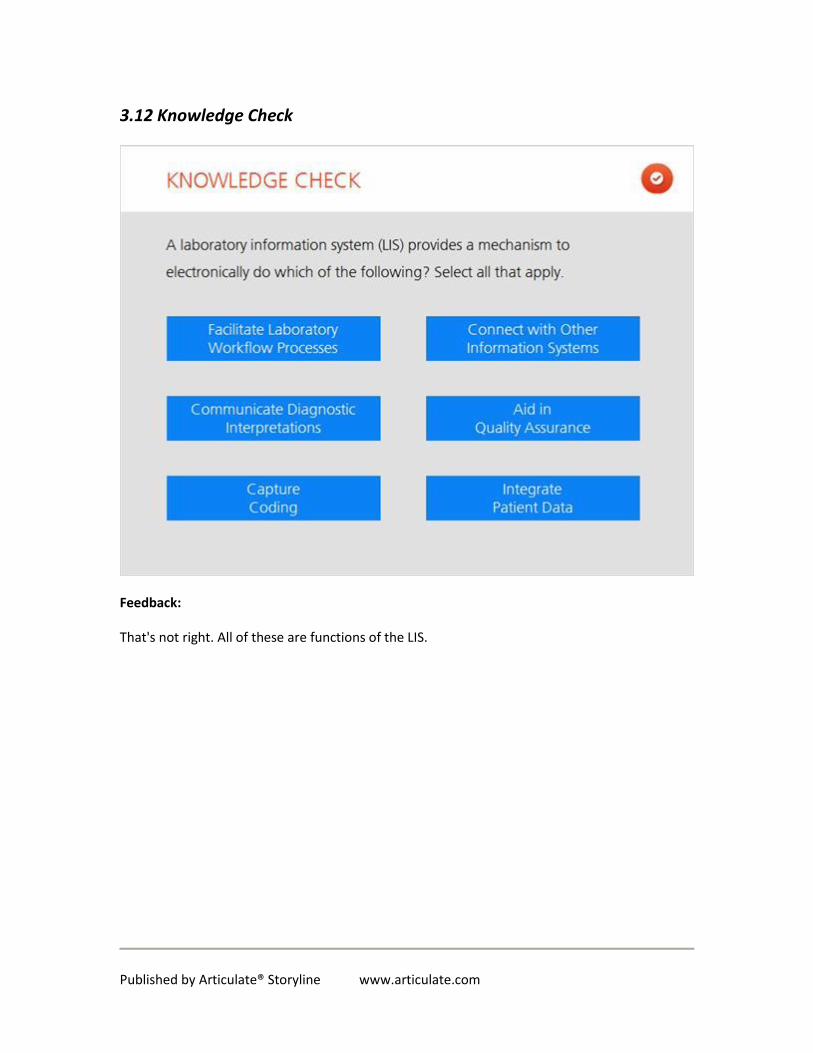
Feedback:
That's not right. All of these are functions of the LIS.
Published by Articulate® Storyline www.articulate.com
4. Integration
4.1 Interfaces and Enterprise-Wide LIS Integration Topics
Notes:
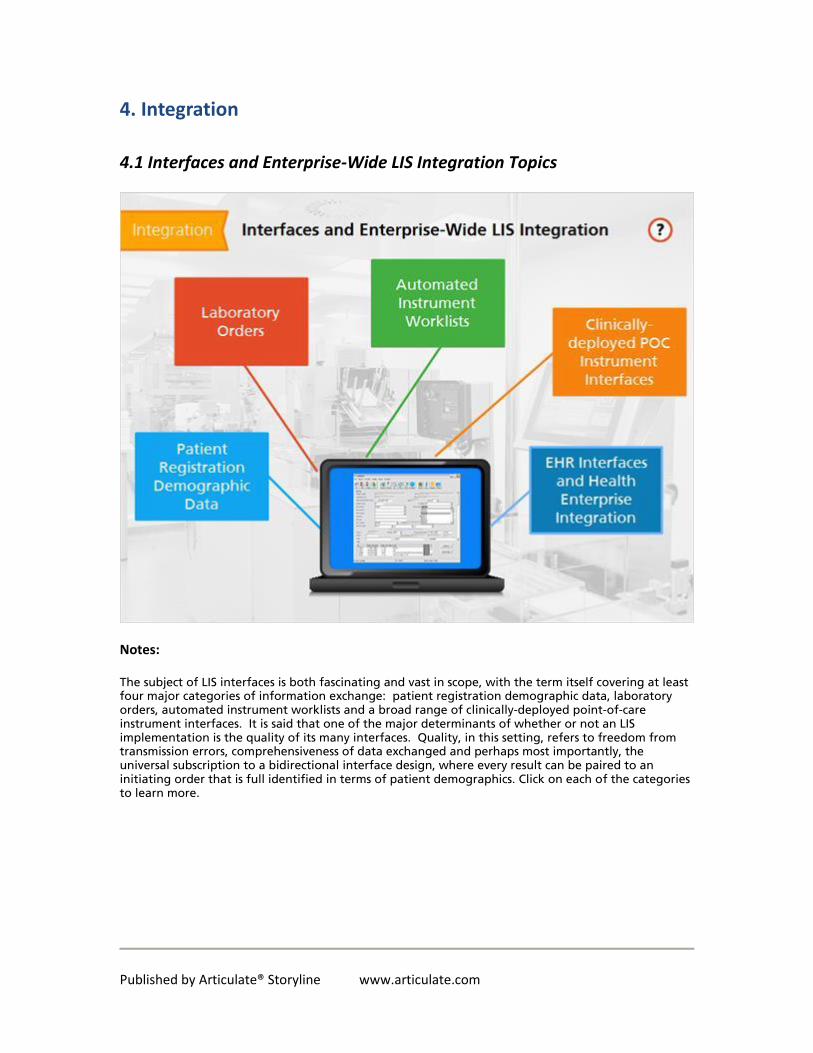
The subject of LIS interfaces is both fascinating and vast in scope, with the term itself covering at least four major categories of information exchange: patient registration demographic data, laboratory orders, automated instrument worklists and a broad range of clinically-deployed point-of-care instrument interfaces. It is said that one of the major determinants of whether or not an LIS implementation is the quality of its many interfaces. Quality, in this setting, refers to freedom from transmission errors, comprehensiveness of data exchanged and perhaps most importantly, the universal subscription to a bidirectional interface design, where every result can be paired to an initiating order that is full identified in terms of patient demographics. Click on each of the categories to learn more.

Published by Articulate® Storyline www.articulate.com
Patient Reg (Slide Layer)
Notes:
Also known as the ADT interface or feed (Admissions Discharges and Transfers), this interface is an essential one, in that it ensures that all patient demographics in the LIS exactly match those of the greater health enterprise. Consider, for example the standard workflow of the emergency department, where patient identities are only discovered after some time after presenting or being admitted. In such cases, it it essential that initial “John/Jane Doe” placeholder demographics are replaced with the correct ones, across every federated information system on the overall health enterprise. The LIS being updated with an appropriate “Update” HL7 message is an essential requirement of sound management principles of demographics. Similarly, the ADT feed provides updated information to the LIS on the whereabouts of the patient (room and bed number) such that if patient bedside phlebotomy is a component of the LIS implementation, the daily patient blood draw list can be informed by the most recent (and correct) location of the patient, preventing needless loss of time on the phlebotomists’ part, to track down patients in the setting of their transfer, which turns out to be a common occurrence.

Published by Articulate® Storyline www.articulate.com
Orders (Slide Layer)
Notes:
As a consequence of the recent Meaningful Use legislation, more and more health enterprises are implementing Computerized Physician Electronic Order Entry (CPOE), which has very specific consequences for the LIS. First and foremost, this should be viewed as an extremely positive development, if correctly implemented, as with the use of CPOE, it finally becomes possible to fully reconcile orders to results in an automated fashion, thereby identifying waylaid or otherwise stalled orders at the earliest possible time. Additionally, use of CPOE avoids all the usual vagaries associated with paper orders, such a transcription errors, incorrect assignment of patient identity and worst of all, the entire loss of the paper requisition, which can effectively “delete” the order.

Published by Articulate® Storyline www.articulate.com
Automated Instrument Worklists (Slide Layer)
Reduction in the number and extent of errors in the laboratory environment is extremely important for patient safety and adequate health care delivery. Automated instrument worklists offer a variety of benefits that range from decreasing the number of manual, error-prone steps to increasing operational capacity and additional revenue for the laboratory.
Automation can minimize preanalytical processing errors, resulting in improved accuracy of reported results and fewer patient redraws. In addition, automation systems can locate and track specimens throughout the preanalytical, analytical, and post-analytical processes, reducing the chances of losing a sample. A potential drawback to relying upon an automated system to identify, aliquot, and route samples is that it requires a capable information system. Information systems that assign the same identification number to all samples collected at the same time from the same patient cannot distinguish among the different sample types (e.g., heparinized versus EDTA blood) and cannot, therefore, aliquot or route the samples properly. To truly realize this benefit of automation, a laboratory information system that assigns a unique specimen identifier to each individual specimen is essential.
Most laboratories that have implemented automation have reported an improvement in TATs and all have seen more consistent TATs with considerably fewer outliers. This translates into increased patient and physician satisfaction with laboratory services and fewer calls to the laboratory regarding outliers. Several features contribute to improved or more consistent TATs. Automation optimizes specimen processing by supporting a continuous flow of specimens and reducing the time specimens spend waiting to be placed into the centrifuge or aliquoted. This optimization allows both routine and stat tests to be reported in a timely manner and decreases the need for priority stat testing. The analytical phase is also improved, as the detection modules and software will alert the technologist to any interferences without delaying the processing of other samples and will automatically divert

Published by Articulate® Storyline www.articulate.com
specimens to another analyzer when one analyzer has technical problems. Finally, several vendors offer a post-analytical storage unit or tray, enabling quick and efficient retrieval for automatic dilutions, repeat analysis, or add-on testing.
Automation of manual and potentially dangerous steps can decrease repetitive motions, biohazard exposure, and walking traffic in the laboratory. With an adequate information technology infrastructure, specimens can be placed directly on the automation track, eliminating manual accessioning and relabeling.
Some employees may fear that automation will replace their function in the laboratory; however, the technologists’ time saved by automation is precious. The time saved can be used to complete tasks that require more careful attention or visual comparison, or to bring new tests or technologies into the laboratory.

Published by Articulate® Storyline www.articulate.com
Clinically-deployed... (Slide Layer)
Selection and deployment of point-of-care (POC) instrumentation presents unique challenges, because many POC solution suites incorporate an aggregation layer (in the form of a distinct software package) in addition to numerous physical instruments and associated docking cradles that must be integrated into the enterprise. Such software will often require its own hardware or a hardware abstraction layer, if it is managed from a virtualized environment. This imposes additional training and stewardship expectations on the dedicated IT staff entrusted with the POCs ongoing operation. Moreover, interfaces are not standardized and often require specialized initial programming and customization. Expertise is will be required to maintain the system and to resolve operational challenges. Certainly, with POC solutions, the guiding operational challenge is to normalize the overall implementation, so that the POC instrument appears as similar as possible to any other conventional single instrument interface connected to the LIS
Published by Articulate® Storyline www.articulate.com
EHR (Slide Layer)
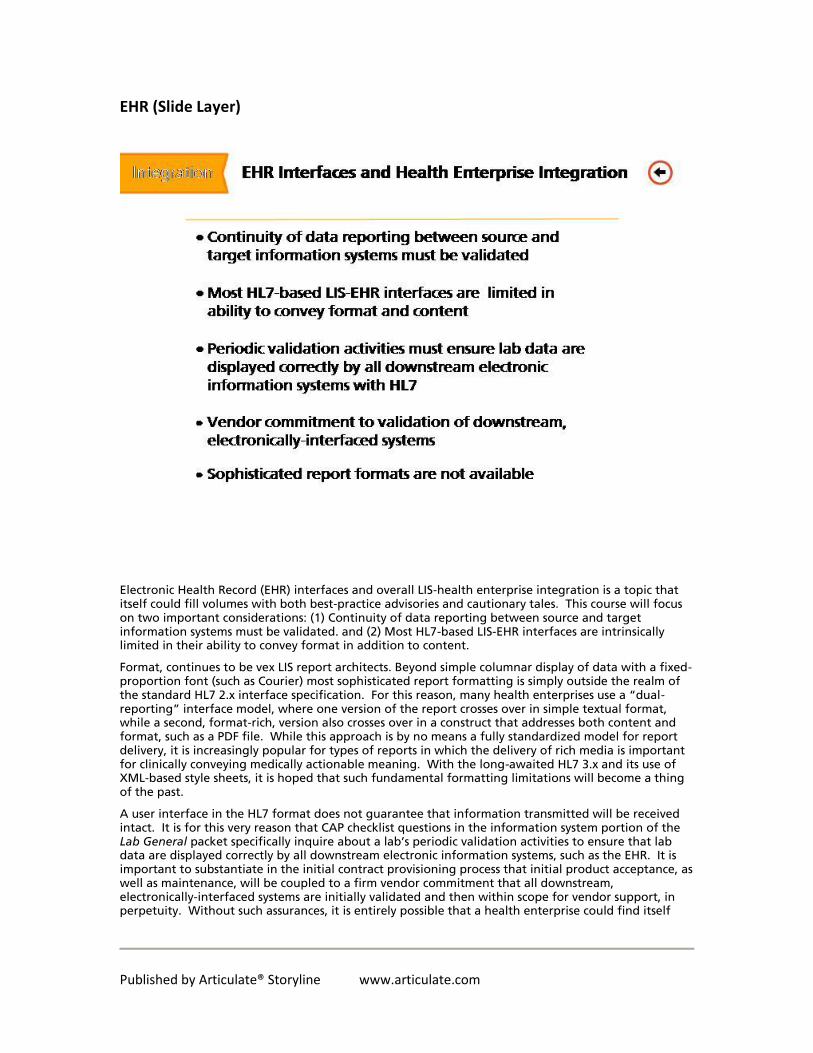
Electronic Health Record (EHR) interfaces and overall LIS-health enterprise integration is a topic that itself could fill volumes with both best-practice advisories and cautionary tales. This course will focus on two important considerations: (1) Continuity of data reporting between source and target information systems must be validated. and (2) Most HL7-based LIS-EHR interfaces are intrinsically limited in their ability to convey format in addition to content.
Format, continues to be vex LIS report architects. Beyond simple columnar display of data with a fixed-proportion font (such as Courier) most sophisticated report formatting is simply outside the realm of the standard HL7 2.x interface specification. For this reason, many health enterprises use a “dual-reporting” interface model, where one version of the report crosses over in simple textual format, while a second, format-rich, version also crosses over in a construct that addresses both content and format, such as a PDF file. While this approach is by no means a fully standardized model for report delivery, it is increasingly popular for types of reports in which the delivery of rich media is important for clinically conveying medically actionable meaning. With the long-awaited HL7 3.x and its use of XML-based style sheets, it is hoped that such fundamental formatting limitations will become a thing of the past.
A user interface in the HL7 format does not guarantee that information transmitted will be received intact. It is for this very reason that CAP checklist questions in the information system portion of the Lab General packet specifically inquire about a lab’s periodic validation activities to ensure that lab data are displayed correctly by all downstream electronic information systems, such as the EHR. It is important to substantiate in the initial contract provisioning process that initial product acceptance, as well as maintenance, will be coupled to a firm vendor commitment that all downstream, electronically-interfaced systems are initially validated and then within scope for vendor support, in perpetuity. Without such assurances, it is entirely possible that a health enterprise could find itself
Published by Articulate® Storyline www.articulate.com
unexpectedly strapped with a hefty time and materials bill for mitigating a suddenly failing LIS-EHR interface owing to an unanticipated change on the EHR side (and through no direct fault of the LIS vendor).
4.2 Technical Aspects: Long-term Costs and Staffing
Notes:
A typical LIS is attached to myriad instrument and foreign system interfaces. It is not surprising the development and subsequent maintenance responsibilities become a significant component of the long-term burden of stewardship of such information systems. However, it’s not uncommon for project planners to underestimate the staffing levels needed to implement all identified interfaces in a new LIS implementation. It’s even more common for these same planners to underestimate the long-term staffing needs, which, paradoxically, often increase beyond initial implementation levels, to maintain such systems. Staffing errors like these, when large in magnitude, can lead to a team’s being chronically under-staffed to appropriately manage an overall system. This can decrease the LIS’s reporting capabilities and even extend downtime. For this reason, whenever identified, a shortfall of staffing in the interface team should be immediately recognized as an operational crisis, and should be immediately mitigated, to the extent possible. To be clear, many contemporary LIS- I.T. failures are directly linked to inconsistent staffing of technical support teams, and especially, to lack of continuity in system coverage from the interface team.

Published by Articulate® Storyline www.articulate.com
4.3 Technical Aspects: Instrument Interfaces
Notes:
Fundamentally, challenges in stewardship of instrument interfaces arise in two major categories: technical aspects of functionality, including the interface message specification, and contractual issues.
In the case of the technical aspects of deployment, the reality that still plagues the clinical LIS field is the persisting lack of a universal standard for instrument interfaces. Because of this lack, every new instrument purchase becomes a mini-implementation project in its own right, to achieve suitable bi-directional IT connectivity. Although many manufacturers use HL7 as the general data exchange protocol, there are sufficient differences between specific instrument and LIS implementations of HL7 to render each deployment unique and therefore, time-consuming and potentially expensive.
The rule of thumb in the industry is that any new instrument interface will cost anywhere between $15,000 and $30,000, and will take at least six months to implement. Consequently, in the overall value proposition grid that ultimately drives the selection process, interface expense and deployment time, should be significant weighting factors when selecting a new instrument. Thus, a cutting-edge instrument might not appear as attractive a choice after factoring in extensive deployment expenses and a long lead-time to final clinical activation.
Published by Articulate® Storyline www.articulate.com
4.4 Technical Aspects: Factoring Value
Notes:
The rule of thumb in the industry is that any new instrument interface will cost anywhere between $15,000 and $30,000, and will take at least six months to implement. Consequently, in the overall value proposition grid that ultimately drives the selection process, interface expense and deployment time, should be significant weighting factors when selecting a new instrument. Thus, a cutting-edge instrument might not appear as attractive a choice after factoring in extensive deployment expenses and a long lead-time to final clinical activation.
Published by Articulate® Storyline www.articulate.com
5. Selection
5.1 Selection Factors
Notes:
Click on any of the buttons to learn more about each of the LIS selection factors.
Published by Articulate® Storyline www.articulate.com
5.2 Goals
Notes:
Why are you looking to replace your LIS in the first place? Your current LIS may not be perfect or even optimal, but by itself that’s not a good reason to change it. Implementing a new LIS is a major undertaking. Make sure that you truly need a new system before embarking on this long journey.
Published by Articulate® Storyline www.articulate.com
5.3 Landscape
Vendors (Slide Layer)
Notes:
Click on the buttons to learn more about issues regarding the landscape.
Vendors in the Marketplace: There are many vendors and LISs in the marketplace. Most cater to smaller labs and specialty-specific boutique labs, with a smaller number of vendors offering a full range of functionality for larger labs.

Published by Articulate® Storyline www.articulate.com
Enterprise... (Slide Layer)
Notes:
This plays out at two levels.
A hospital or health system may have a contract with a large vendor for its electronic health/medical record (EHR/EMR), and that vendor may have a laboratory information system as one of its offerings. Often, the annual license for this LIS will be included in the EHR license, and thus there will be a large apparent financial incentive for the lab to use this LIS. On the other hand, if this LIS does not meet the laboratory’s needs well, then it may be advantageous over the long run to choose a different LIS despite the up front license and integration costs.
With a laboratory, there are often specialized functions such as anatomic pathology and genetics that may not be well handled by a “general” LIS that fits the need of, say, clinical chemistry. Such cases may justify using a separate, best of breed LIS for that particular function. This approach may lead to significant additional licensing and integration costs. Note that for certain functions such as blood bank donor center, a best of breed system may be the only option.
Published by Articulate® Storyline www.articulate.com
Lab's Vision (Slide Layer)
Notes:
What is the laboratory’s vision of the future? Does it plan to grow, add specialty functions, and/or differentiate itself in particular ways in the future? All these will impact which LIS would be best.
Published by Articulate® Storyline www.articulate.com
5.4 Functionality
Notes:
It is important to take a complete inventory of all specimen handling, testing, resulting and business functions handled by the current LIS. Also review functions that may not be handled by the current LIS but could be handled by a different system
Pay particular attention to idiosyncratic workflows within your laboratory. An LIS will typically enforce many aspects of workflow, and it will be important for a laboratory to assess which aspects of workflow are truly necessary, and which can safely be changed.
It is common for laboratories to pay disproportionate attention to functions that are poorly served by their current LISs. This is risky, because it discounts the functions where its current LIS may be superior to alternatives.
Microbiology, chemistry, flow cytometry, anatomic pathology, etc. all require their own separate consideration of workflow and other requirements, regardless of whether the laboratory expects to use a single LIS or a best of breed approach.
What interfaces are required now or in the future to instruments and other LISs (e.g. reference lab LISs). It is much more compelling to know that a particular LIS has implemented a successful interface with a particular external system, than for that LIS vendor to simply claim that capability
Regulatory compliance is a key category of LIS functionality, particularly if your laboratory is subject to additional rules that don’t apply to all U.S. laboratories (New York Dept of Health, FDA Good Laboratory Practice, etc.)
Published by Articulate® Storyline www.articulate.com
5.5 Back-End Technology
Notes:
An LIS sits atop a database management system, operating system, hardware (servers and workstations), etc. In most cases these systems will be 3rd party systems rather than proprietary to the LIS vendor. The key issue to consider here is the long-term prospect for each system. A laboratory may retain an LIS for twenty years or more, and it is important to know that each of these underlying technologies will remain well supported over this time period. This includes broad availability of expertise for these systems. In general, the most widely used technologies from well-established vendors are most likely to age well.
Published by Articulate® Storyline www.articulate.com
5.6 Vendor Characteristics
Notes:
Just as with employees, the best predictor of future performance is past performance. Consider how well each vendor has served the needs of its clients and how well it has kept its long-term promises.
What is the vendor’s vision of its own future, and how well does that match your laboratory’s vision? Does this vendor focus on laboratories similar to your own? If they produce other products, e.g. an EHR, how does their commitment to their LIS fit into their overall corporate plans?
What are the size and reputation of the vendor’s technical support organization? Can they effectively support your laboratory?
Financial strength: If your laboratory is to maintain an LIS for twenty or more years, then that requires that the vendor stays in business for the same time period.
Published by Articulate® Storyline www.articulate.com
5.7 Performance
Notes:
A closely related issue is performance. A laboratory needs to define its transaction volume, response time, uptime and other requirements, and pay particular attention to future requirements (e.g. if growth is anticipated). “Sizing” LIS hardware to meet performance needs is a highly technical estimation function typically performed by bidding vendors, but be aware that vendors may undersize the hardware in order to keep the apparent costs down in the bid.
Some vendors may offer off-site (“cloud”) hosting of data center functions. This simplifies a number of back-end functions (backups, server maintenance, operating system upgrades, etc.). Laboratories need to compare the cost of such offers against their own available resources (e.g. hospital data center) and also determine performance requirements.
Published by Articulate® Storyline www.articulate.com
5.8 Support
Notes:
Vendors have different types of processes and systems for technical support. Initial response time, escalation process, and process for categorizing complaints (defect, enhancement, critical vs. noncritical, et.) are all important.
Published by Articulate® Storyline www.articulate.com
5.9 Price
Notes:
Price includes up-front license, annual maintenance, hardware, 3rd party software, professional services during implementation, and/or other fees. It is important to consider the full set of costs in order to properly compare different vendor offerings.
Published by Articulate® Storyline www.articulate.com
5.10 Knowledge Check
Feedback:
That's right! All of these are beneficial questions.
Published by Articulate® Storyline www.articulate.com
5.11 Selection Process
Notes:
Click on the buttons to learn more about each of the selection process elements.
Published by Articulate® Storyline www.articulate.com
5.12 Team
Notes:
It is valuable to engage all major stakeholders within the laboratory, and include personnel with deep knowledge of each analytic, logistic and business process.
Plan on a major time commitment for this committee.
The selection process will benefit from a clearly defined process and clear decision-making roles.
Given the large and critical role of project management during the implementation phase, it is logical to identify a dedicated project manager (or managers) early on to also run the selection process. Vendors may supply additional project management support, but this is not a function that should be fully outsourced.
Outside consultants can be a valuable addition to the selection team, but be sure to retain decision-making within your own laboratory’s permanent leadership.
Published by Articulate® Storyline www.articulate.com
5.13 Requirements Documentation
Notes:
The requirements gathered during the first phase need to be formally documented and shared with vendors. This typically takes the form of a request for proposal (RFP) or request for information (RFI).
Given the complexity of modern laboratories, it may be helpful to have a “Bidder’s conference” as part of the RFP/RFI process in which vendor representatives can learn more about your laboratory, its requirements, and your planned selection process.
Published by Articulate® Storyline www.articulate.com
5.14 References
Notes:
External information sources can be a useful source of vendor comparison information. This may be particularly helpful in the early phases, such as determining which vendors to contact with an RFP/RFI.
Vendors are understandably protective of their customer lists, but you should insist on a complete list along with the ability to reach out to other laboratories on that list.
On-site visits of client sites are often helpful in order to see and ask first-hand questions about how well systems meet the needs of different lab operations.

Published by Articulate® Storyline www.articulate.com
5.15 System Demonstrations
Notes:
System demonstrations are a traditional step in a selection process, and can either be extremely helpful or dangerously misleading.
Demonstrations should be orchestrated by the selection team, not the vendors. The purpose is not for vendors to show off their systems; the purpose is for you to objectively compare and evaluate.
Limit the number of demonstrating vendors to a number that can be managed within a very tight time interval, and if possible hold demonstrations on the same day. This typically means two or three companies, and requires careful upfront screening of vendor RFP/RFI responses to narrow the participants.
Most importantly, tightly script the presentations according to functions and specific workflows, and aggressively manage the vendor representatives to hold them accountable to the script and the allotted time for each item.
Published by Articulate® Storyline www.articulate.com
5.16 Contracting Process
Notes:
A contract for an LIS can be extremely long and detailed. Keeping in mind that verbal promises made during the selection process are unlikely to be enforceable, it is advisable to include in the contract all of the detail contained in the RFP/RFI responses.
Professional services typically comprise a large portion of implementation costs. Ensure that the contract specifies the nature of these services in sufficient detail. In particular, ensure the right to prescreen resumes/credentials of individual consultants, and ensure the right to dismiss underperforming consultants.
The contract is the basis for a (hopefully) very long-term business relationship. It can make the difference between a huge success and a painful failure. In addition to your own organization’s legal review, make sure that your lab leadership engages in all of the contract details.
Published by Articulate® Storyline www.articulate.com
5.17 Knowledge Check
Feedback: The correct answer is: It's a good idea to invite potential vendors to your lab to learn
about its unique needs.
Published by Articulate® Storyline www.articulate.com
6. Conclusion
6.1 Two-Person Scenario
Notes:
Let’s get back to the scenario with Dr. Jones. How will he answer the email and/or present to the CIO? Based on what you’ve learned in this course, select your best recommendation to the CIO: A, B, or C.
Published by Articulate® Storyline www.articulate.com
Published by Articulate® Storyline www.articulate.com
Choice1 (Slide Layer)
Published by Articulate® Storyline www.articulate.com
Choice2 (Slide Layer)
Published by Articulate® Storyline www.articulate.com
Choice3 (Slide Layer)
email (Slide Layer)
Published by Articulate® Storyline www.articulate.com
6.2 Epilogue
Notes:
As you may recall, three factors were involved in Dr. Jones’ decision-making process: Growing outreach business, the blood donor program, and next-generation sequencing and molecular testing. Click on each of the folders to learn more about how that program has been affected by his decision 24 months later.
Published by Articulate® Storyline www.articulate.com
6.3 Outreach Business
Notes:
To grow a lab’s outreach business from an informatics perspective, the following factors are key: The ability to easily establish & maintain interfaces between your LIS and the many EMRs out there. If this task is too much for your lab to handle, there are consulting companies and middleware solutions that can help. It is also important to align such informatics projects with your laboratory’s business & marketing efforts.
Published by Articulate® Storyline www.articulate.com
6.4 Blood Donor
Notes:
Not every LIS includes a blood-donor module. A blood-donor system is a very specialized information system, and is not likely to be included within an LIS that is bundled within an EMR. Therefore, if a donor program is important for your institution to support, you will need to evaluate blood bank systems or stand-alone donor systems that can specifically meet this requirement.
Published by Articulate® Storyline www.articulate.com
6.5 Molecular Testing
Notes:
Molecular testing is not something every LIS can easily handle. The reason is that molecular data are often large and complicated (for example, next-generation sequencing with many variants), the workflow is unique (for example, wet and dry bench data requirements), and reporting of molecular results is often difficult (as in complex mutations). Therefore, a lab that wants to offer new molecular tests will need to either purchase a best-of-breed molecular LIS, customize their existing LIS in partnership with the vendor, or develop its own software.
Published by Articulate® Storyline www.articulate.com
6.6 Congratulations!
Notes:
Congratulations! You have successfully completed the eLearning course: Laboratory Management Information Systems in Daily Practice.





























