Embed Size (px)
Citation preview

L’alimentazione
nella prevenzione
delle allergie: miti
o realtà?
Marzia Duse
Dipartimento di Pediatria e NPI
Università “Sapienza” di Roma

Alimentazione: quando?
Gustav Klimt

Epidemiological and immunological studies
suggest that dietary modification in fetal life
could affect the development of allergic
diseases. Somewhat conflicting findings imply
that there might be critical time windows of
exposure to foods and nutrients during
pregnancy.
Erkkola et al. , PAI 2012
pregnancy.

As maternal antigen
avoidance,
Kramer review of 504 woman suggests that
the avoidance could
- lead to lower birth weight
- increase in pre-term birth

Peto OR Peto OR
(95% CI) (95%CI)
Asthma
Lilja ’88 1.01
(0.66-1.49)
Maternal avoidance during pregnancy: asthma
and any atopic condition in first 12-18 mo.(Kramer 2002)
(0.66-1.49)
Falth-Magnusson ’87 0.71
(0.21-2.41)
Any atopic condition
Lilja ‘88 0.71
(0.34-1.49)
-0.1 –0.2 1 5 10

DA e livelli di IgG a-OVA a 18 mesi in 229 bambini
nati da madri a dieta priva di uovo o a dieta libera
10
20
DA
%
- 30
- 20
-10
IgG
µg
/ml
0 - 0
dieta libera dieta priva di uovo
n. 114 n. 115
0
10
20
30p<0.08
%
<5 5-15 >15 I g Gαααα-OVA µµµµg/mlVance GH et al, Clin Exp Allergy 2004

Prescribing an antigen-
avoidance diet to a
high risk woman during
Szajewska H, IMAJ 2012
high risk woman during
pregnancy or lactation
did not reduce her child’s risk of atopic
diseases such as eczema and asthma.
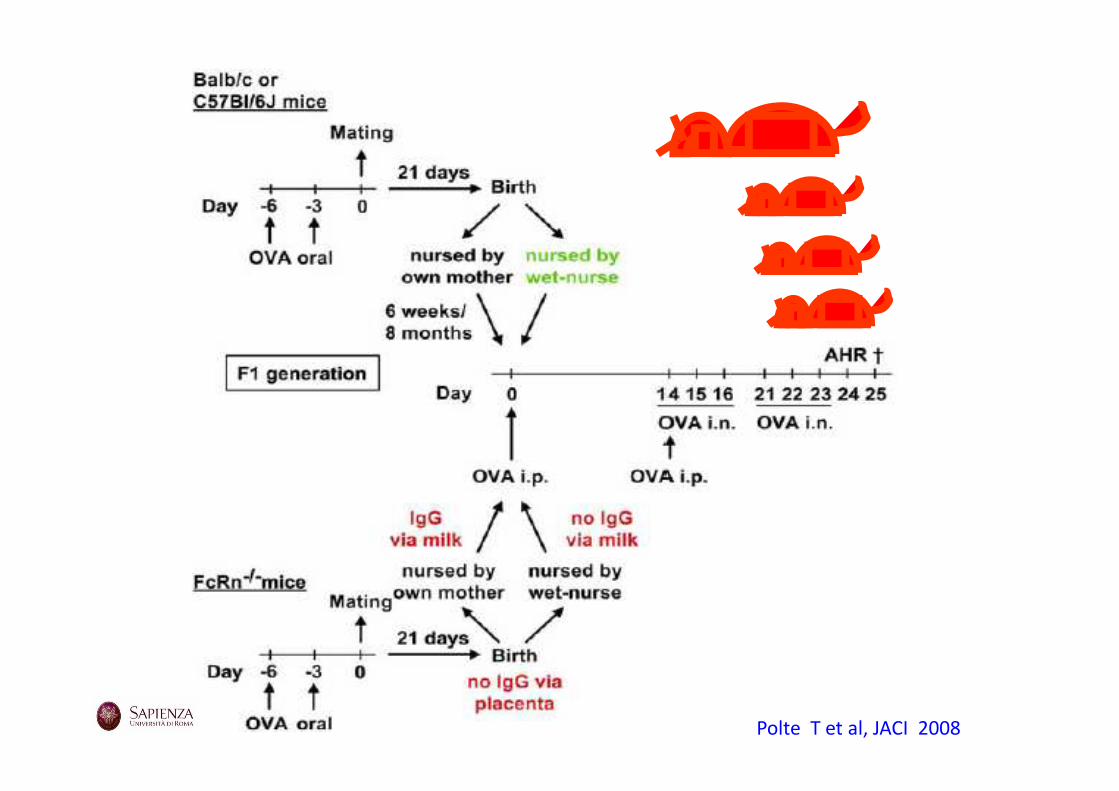
Polte T et al, JACI 2008
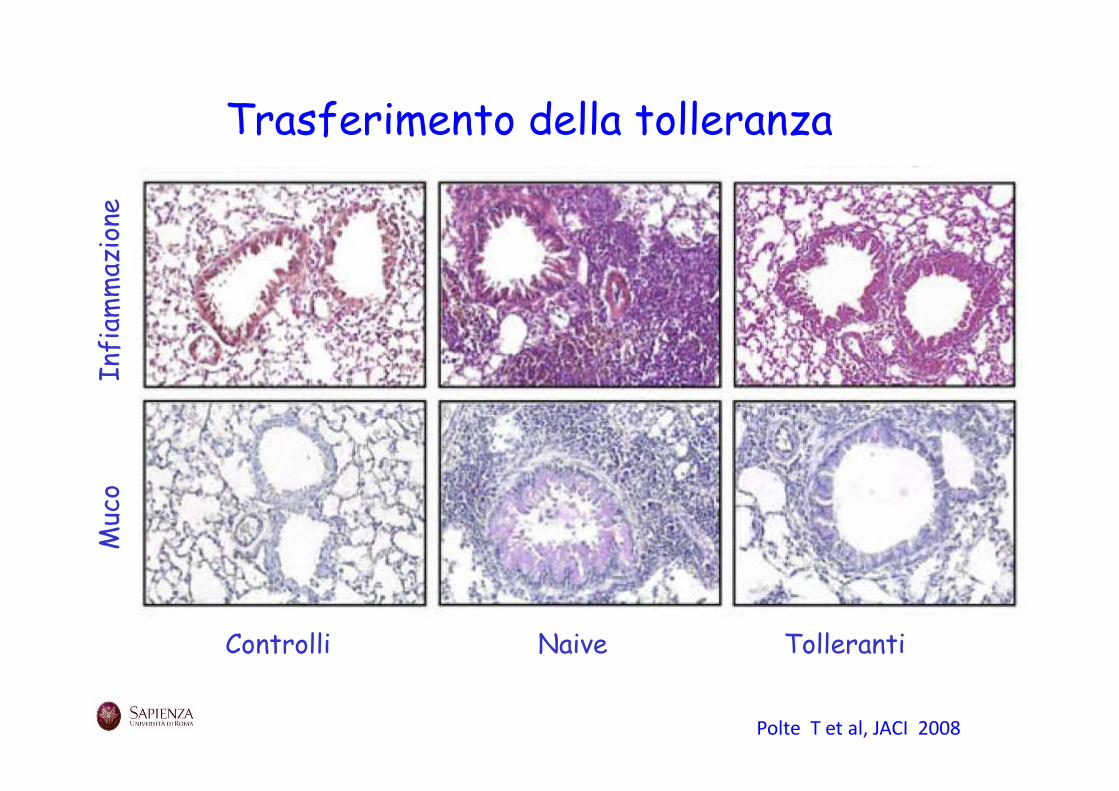
Muco Infiam
mazione
Trasferimento della tolleranza
Polte T et al, JACI 2008
Controlli Naive Tolleranti
Muco Infiam
mazione

Prescott S,. Ann Nutr Metab 2011

Prescott S,. Ann Nutr Metab 2011


The Cochrane Library 2009, Issue 1, last up-to-date 26 July 2006

Prolonged feeding: pHF vs cow’s milk formula, Any allergy

Prolonged feeding: eHF vs pHF, Any allergy
!!
!!!!

Incidence rates of AD obtained from studies comparing
PHF-W to SF limited to articles published after 1995.
Iskedjian M, CMRO 2010

MACS study
Lowe AJ et al, JACI 2011

Unadjusted associations between allocated
formula and risk of allergic disease
Lowe AJ et al, JACI 2011

Meta-analysis results of all reviewed/top tier studies: risk
of AD (PHF-W vs CMF)
.
Alexander DD, Cabana MD, JPGN 2010

Study-Specific-Cumulative incidence of AD
Alexander DD et al, Nutr review 2010
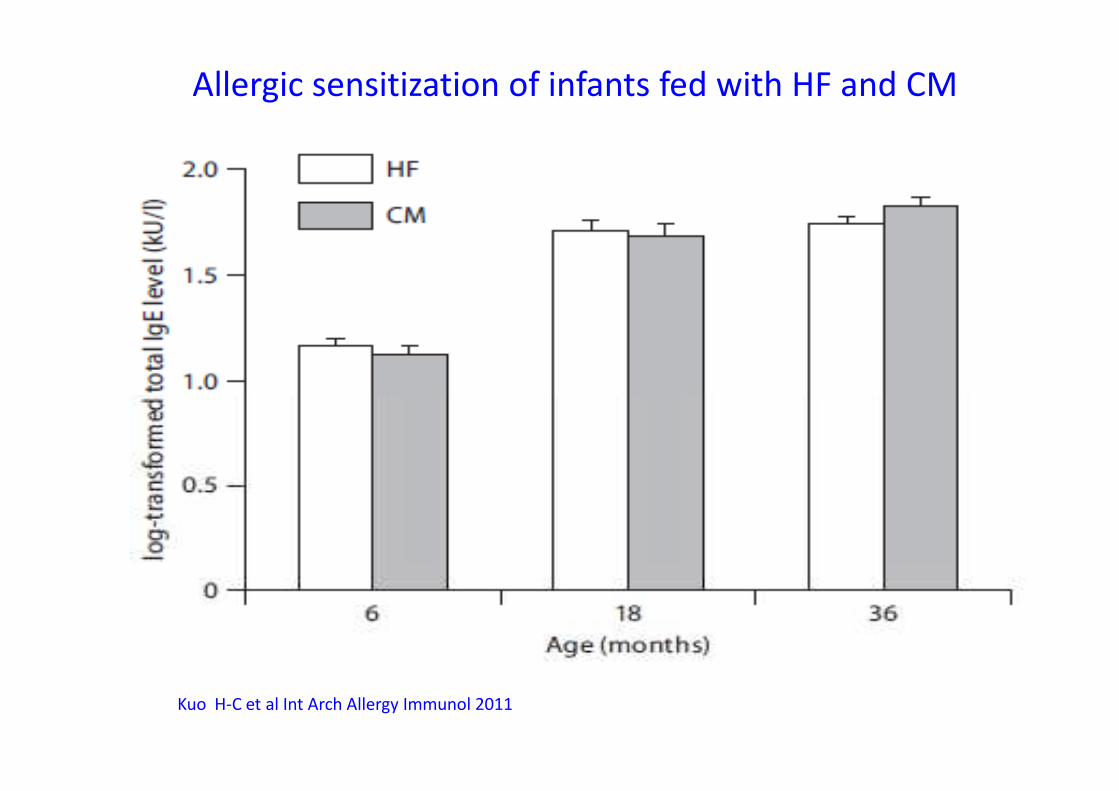
Allergic sensitization of infants fed with HF and CM
Kuo H-C et al Int Arch Allergy Immunol 2011
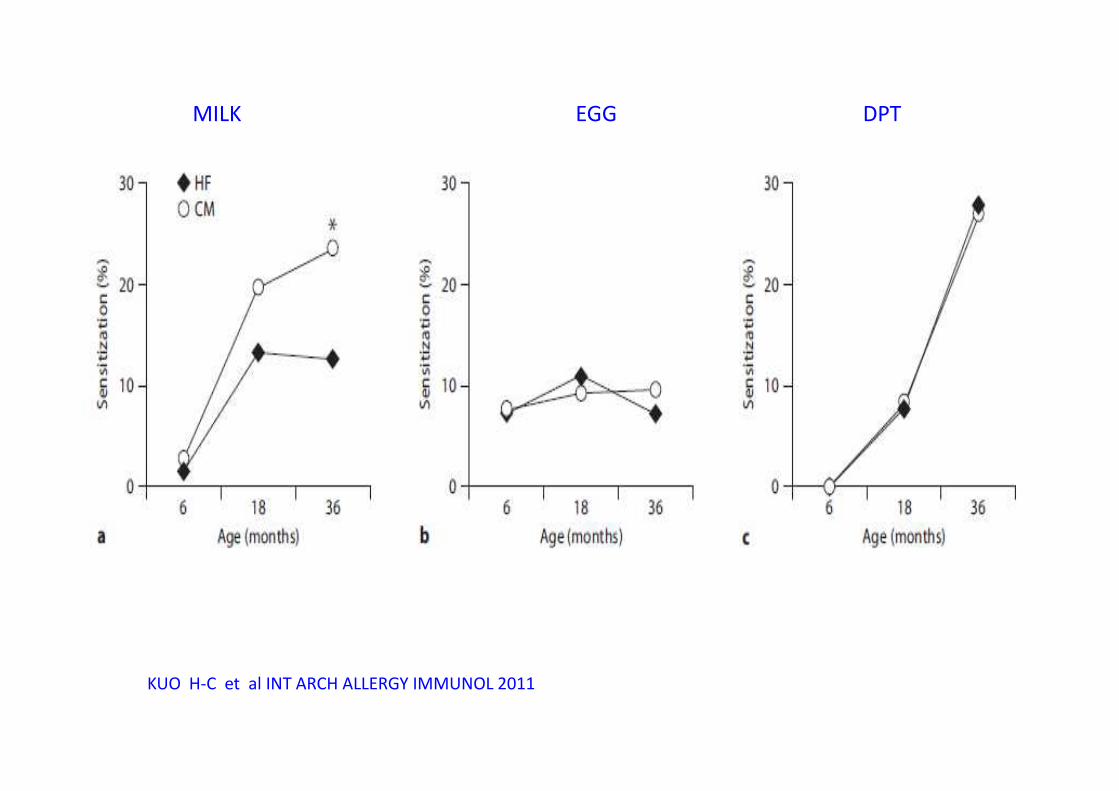
MILK EGG DPT
KUO H-C et al INT ARCH ALLERGY IMMUNOL 2011
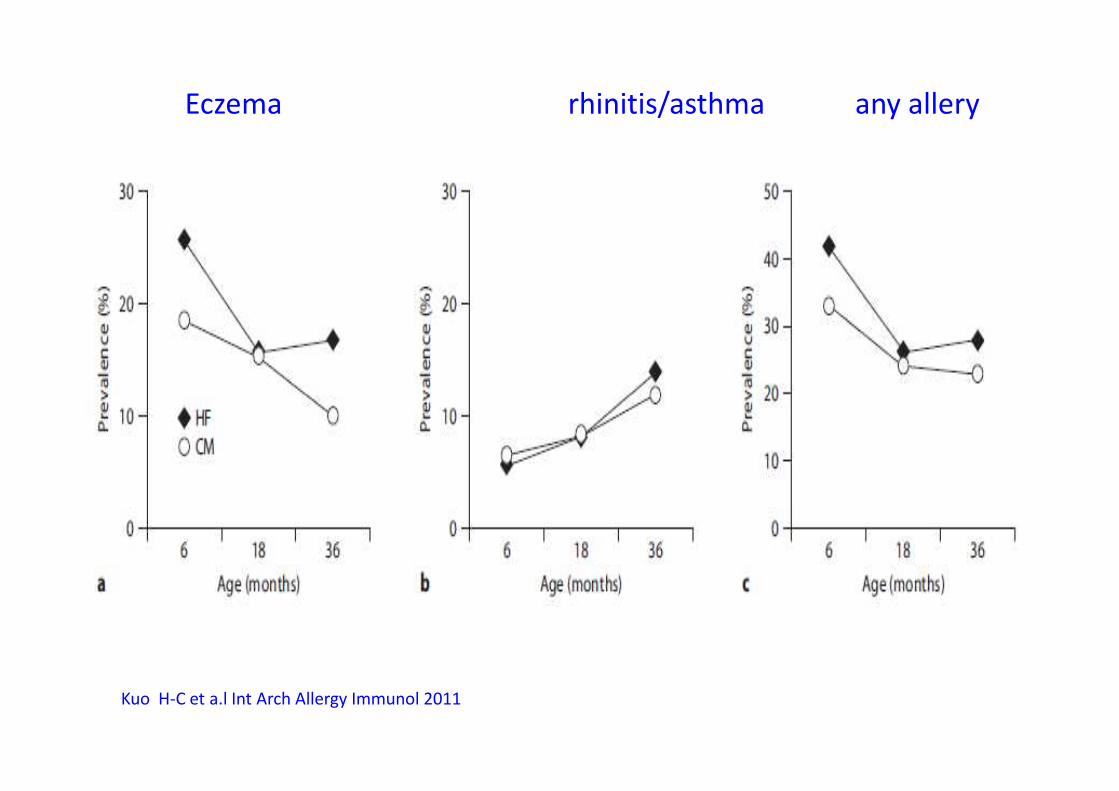
Eczema rhinitis/asthma any allery
Kuo H-C et a.l Int Arch Allergy Immunol 2011
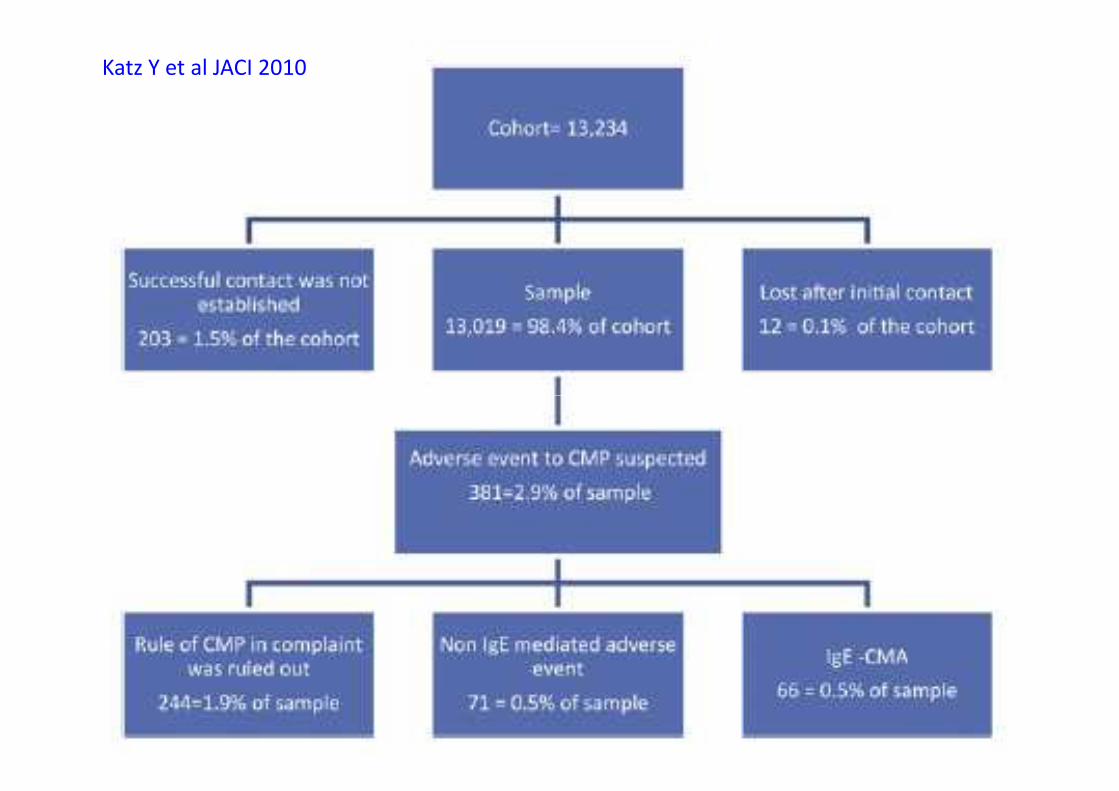
Katz Y et al JACI 2010

Katz Y et al JACI 2010

Prescott S et al. Ann Nutr Met 2011

Du Toit G, et al. JACI 2008
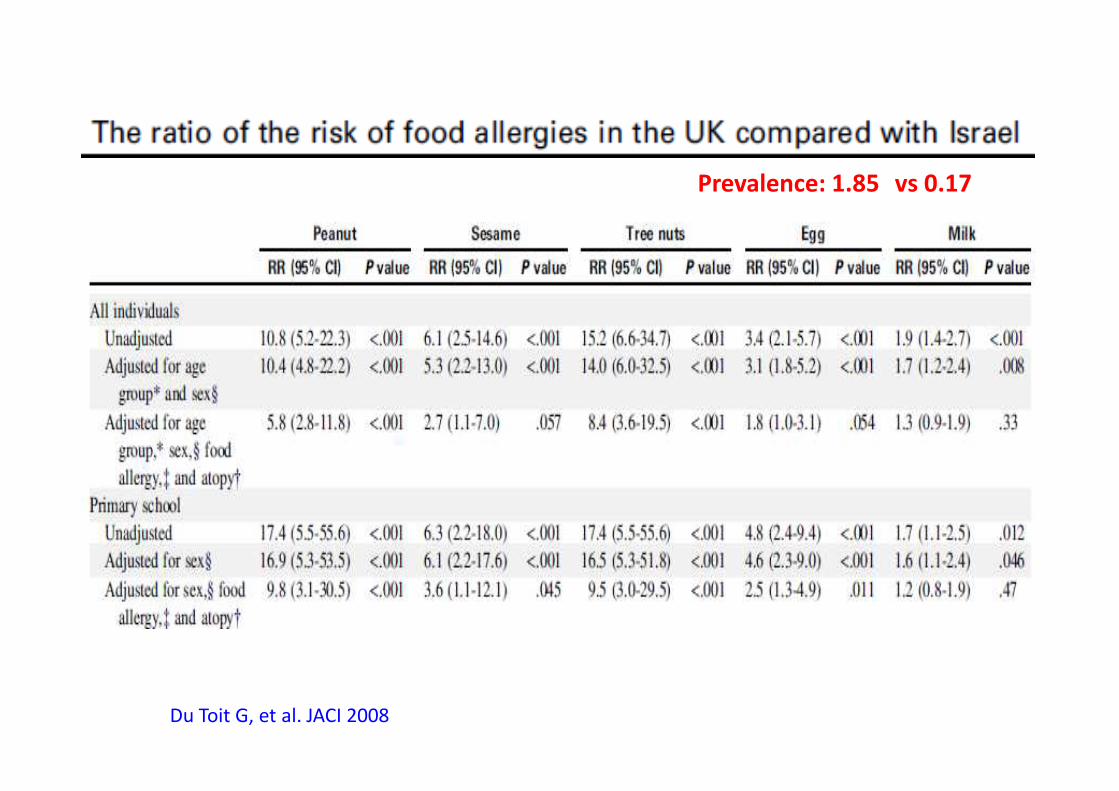
Prevalence: 1.85 vs 0.17
Du Toit G, et al. JACI 2008
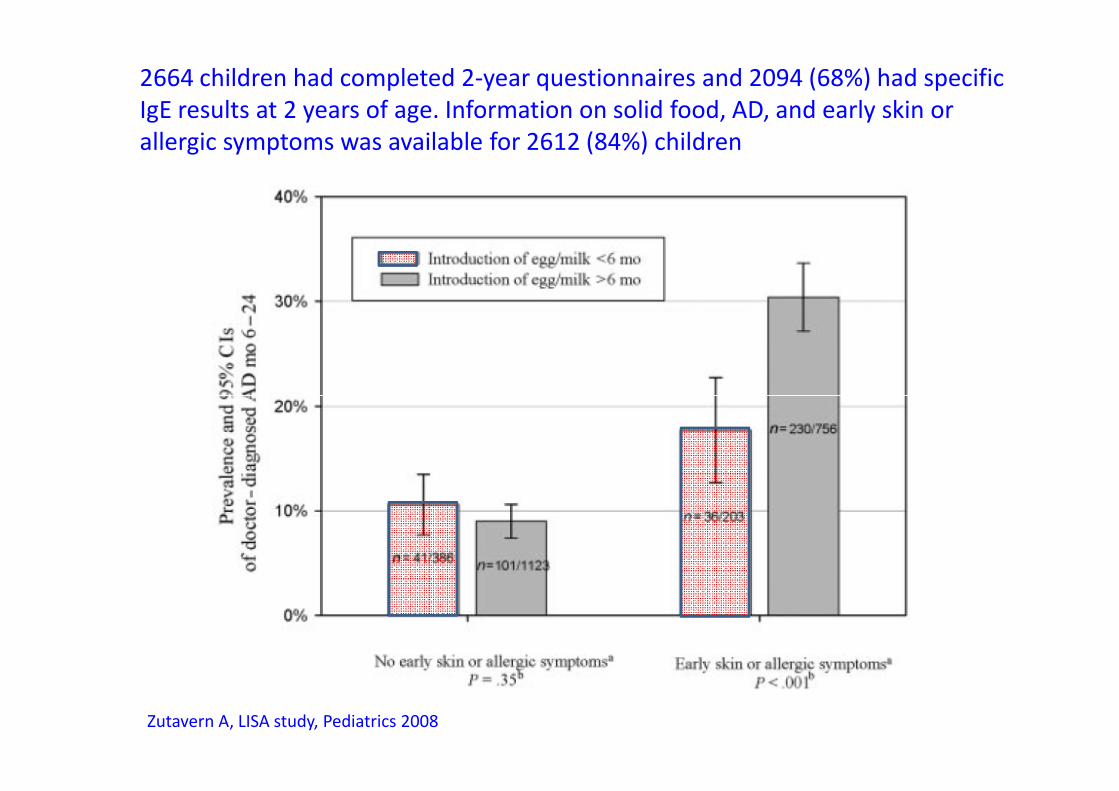
2664 children had completed 2-year questionnaires and 2094 (68%) had specific
IgE results at 2 years of age. Information on solid food, AD, and early skin or
allergic symptoms was available for 2612 (84%) children
Zutavern A, LISA study, Pediatrics 2008


Jarvinen et al. Immunol Allergy Clin N Am 32 (2012) 51–65


Food allergy is defined as an adversehealth effect arising from a specificimmune response that is reproducible onexposure to a given food, and thus is anexample of a defect in the development
Jarvinen et al. Immunol Allergy Clin N Am 32 (2012) 51–65
example of a defect in the developmentor a breakdown in the maintenance oforal tolerance.

Jarvinen et al. Immunol Allergy Clin N Am 32 (2012) 51–65

Prescott. Ann Nutr Metab 2011;59(suppl 1):28–42

Prescott. Ann Nutr Metab 2011;59(suppl 1):28–42

Prescott. Ann Nutr Metab 2011;59(suppl 1):28–42

Breastfeeding
Many studies have shown that breast-feeding may have the protective effectagainst future atopic dermatitis and earlychildhood wheezing. ESPGHAN and theEuropean Society for PaediatricEuropean Society for PaediatricAllergology and Clinical Immunology jointlyrecommend exclusive breast-feeding for4–6 months for allergy prevention, whilethe WHO recommends exclusivebreastfeeding for 6 months.
Misak. Proceedings of the Nutrition Society (2011), 70, 465–471

Dietary products with reduced allergenicity
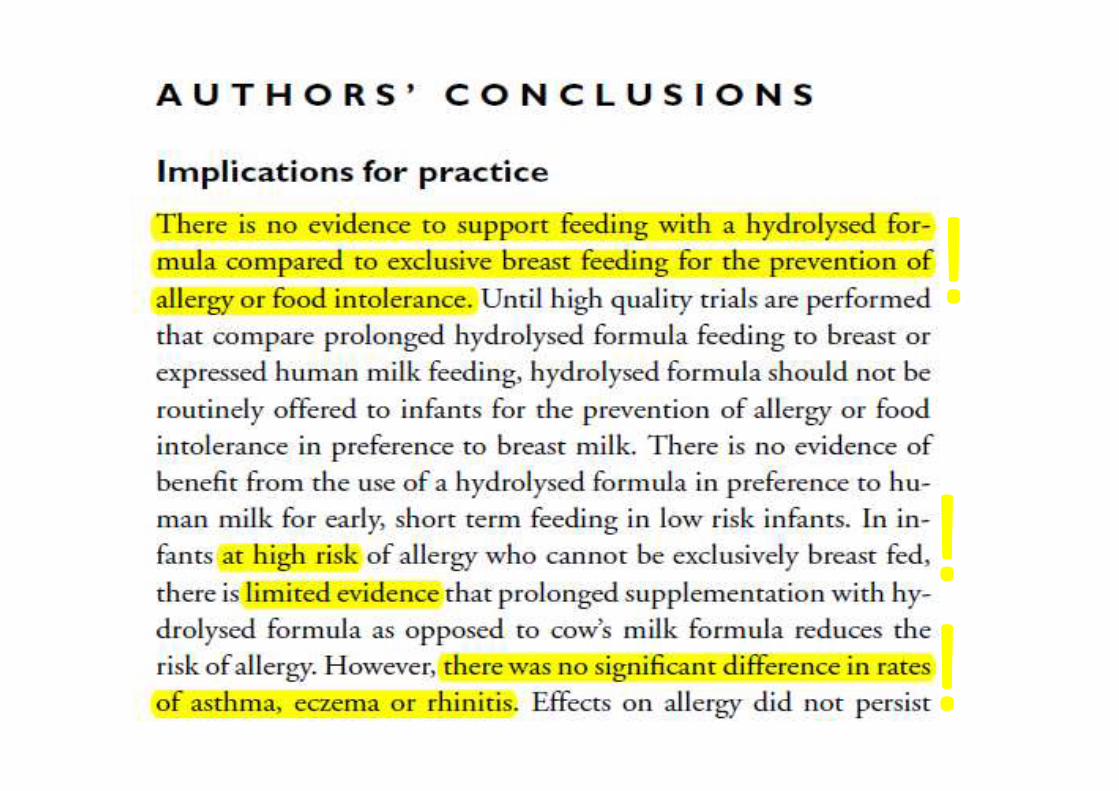
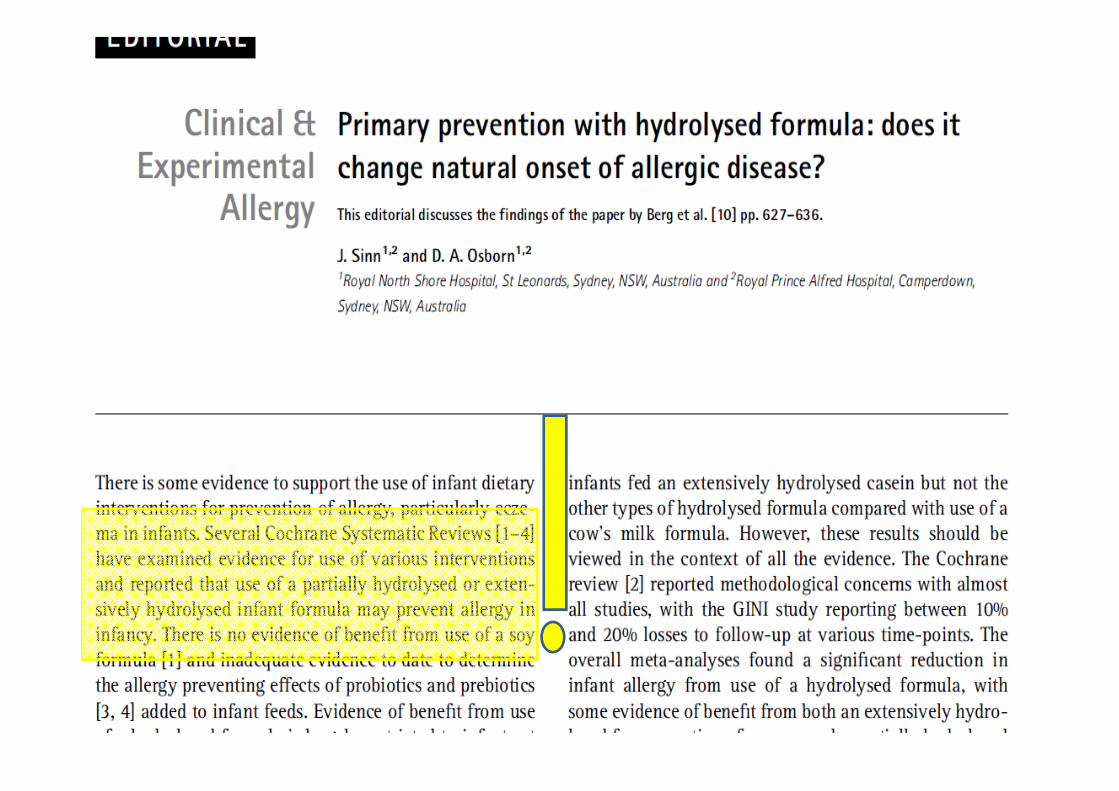
For clinical practice, based on the currentevidence, currently recommendations statethat infants with a documented hereditaryrisk of allergy (i.e., an affected parentand/or sibling) who cannot be breastfedand/or sibling) who cannot be breastfedexclusively should receive a formula withconfirmed reduced allergenicity, i.e., apartially or extensively hydrolyzedformula, as a means of preventing allergicreactions
Szajewska IMAJ • VOL 14 • JANUARY 2012

Chang Kuo et al. Int Arch Allergy Immunol 2011

Lowe et al. J Allergy Clin Immunol 2011;128:360-5

Complementary food
Previously, for complementary feeding, earlyexposure to solid foods during infancy wasassociated with the development of allergicdiseases, particularly eczema. Currently, theguidelines downplay the role of solid foods in thedevelopment of allergies, stating that there is noconvincing scientific evidence that the avoidance ordevelopment of allergies, stating that there is noconvincing scientific evidence that the avoidance ordelayed introduction of potentially allergenic foods(e.g., cow’s milk, egg, peanut, tree nut, fish andseafood) beyond 4–6 months reduces allergies ininfants considered to be at increased risk for thedevelopment of allergic diseases or in those notconsidered to be at increased risk.
Szajewska IMAJ • VOL 14 • JANUARY 2012

Probiotics and/or prebiotics
• Negli ultimi anni è stata posta particolare attenzione alruolo che la flora batterica dell’intestino può svolgere nelpromuovere la maturazione del sistema immunitario fin daiprimi giorni di vita. Nel neonato un appropriato stimolomicrobico è di estrema importanza per equilibrare ilrapporto Th1/Th2, che alla nascita è sbilanciato verso larisposta Th2.risposta Th2.
• Numerosi studi clinici hanno dimostrato che la selezione diceppi batterici come Lactobacilli e Bifidobacteri,attraverso l’integrazione nella dieta di probiotici, puòfacilitare lo sviluppo della tolleranza e, ritardare o evitarela sensibilizzazione agli allergeni.
• Le più recenti matanalisi traggono la conclusione che non cisono sufficienti evidenze per consigliare l’uso deiprobiotici nella prevenzione dell’allergia.

Morisset et al. EuropeanJournal of Clinical Nutrition
(2011) 65, 175–183

Other nutritional interventions
Neither can specific recommendationsbe made for the use of long-chainpolyunsaturated fatty acids,antioxidants (e.g., vitamin C, vitamin E,antioxidants (e.g., vitamin C, vitamin E,beta-carotene, zinc), folate, and vitaminD.
Szajewska IMAJ • VOL 14 • JANUARY 2012

Dieta di eliminazione
• Nelle fasce d’età successive, la rigorosa dieta dieliminazione della durata di un paio di settimane circarimane l’approccio terapeutico tuttora maggiormenteconsolidato. Prevede l’allontanamento dell’agente causaleper un periodo di tempo variabile, finalizzato alla naturaleacquisizione della tolleranza, che in oltre l’80% dei casi siverifica entro i primi 3 anni di vita. Se la dieta dieliminazione comporta un netto miglioramento dei sintomiverifica entro i primi 3 anni di vita. Se la dieta dieliminazione comporta un netto miglioramento dei sintomisenza ricorrere a farmaci, supporta la diagnosi fino allaconferma che è ottenuta con il test di scatenamento.
• Sebbene accettata universalmente come trattamentosintomatico e preventivo nei confronti delle reazioniavverse, la dieta di eliminazione rimane lontana dall’essereconsiderata risolutiva. Comporta piuttosto il costantepericolo di esposizione accidentale all’alimento, conmanifestazioni cliniche anche letali.
Test di Provocazione Orale
Il test alimentare orale (OFC) èconsiderato il test standard diriferimento per la diagnosi di allergiaalimentare, essenziale per laalimentare, essenziale per lapianificazione dei regimi di eliminazione,per ridurre il rischio di esposizioneaccidentale.

Conclusioni
• There were no data suggesting that diet modification changedsensitization of other food allergens or aeroallergens.
• Early nutrition may have profound implications for long-termhealth and atopy later in life, it presents an opportunity toprevent or delay the onset of atopic diseases.
• There have been attempts to reduce the risk of the• There have been attempts to reduce the risk of thedevelopment of allergy using dietary modifications, frompromoting longer breast-feeding and delayed introduction ofpotentially allergenic foods to active prevention of atopy usingspecific dietary components.
• Still, there are many open questions and additional studies areneeded to document the long term effect of dietaryinterventions in infancy to prevent atopic disease.





























