Embed Size (px)
Citation preview
La terapia neo-adiuvante
nei tumori infiltranti endovescicali
IV°Meeting Uro-Oncologico UP DATE 2016 SUI TUMORI UROLOGICI
Prof. Andrea B. Galosi
Direttore Clinica Urologia
Ospedali Riuniti Ancona - UNIVPM
Tumore della vescica
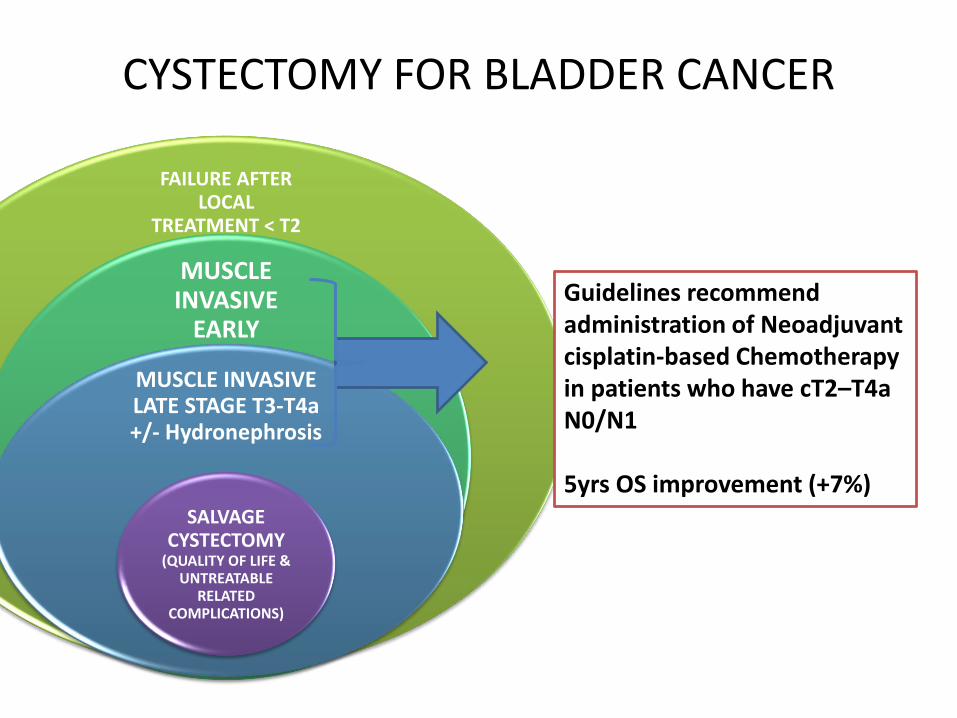
CYSTECTOMY FOR BLADDER CANCER
FAILURE AFTER LOCAL
TREATMENT < T2
MUSCLE INVASIVE
EARLY
MUSCLE INVASIVE LATE STAGE T3-T4a +/- Hydronephrosis
SALVAGE CYSTECTOMY
(QUALITY OF LIFE & UNTREATABLE
RELATED COMPLICATIONS)
Guidelines recommend administration of Neoadjuvant cisplatin-based Chemotherapy in patients who have cT2–T4a N0/N1
5yrs OS improvement (+7%)
Despite Guidelines recommendations
• NAC is largely under-utilised:– only 15% receiving neoadjuvant chemo in recent years
• Reasons– Multiple baseline comorbidities
• cardiac and renal dysfunction
– Advanced age at disease presentation
– Urologist concerns • Increased risk of perioperative morbidity and mortality (8%)
– Oncologist concerns• Morbidity and mortality during CHT
– Lack of Multidisciplinary approach
NeoAdjuvant Chemotherapy (NAC) for B.Cancer
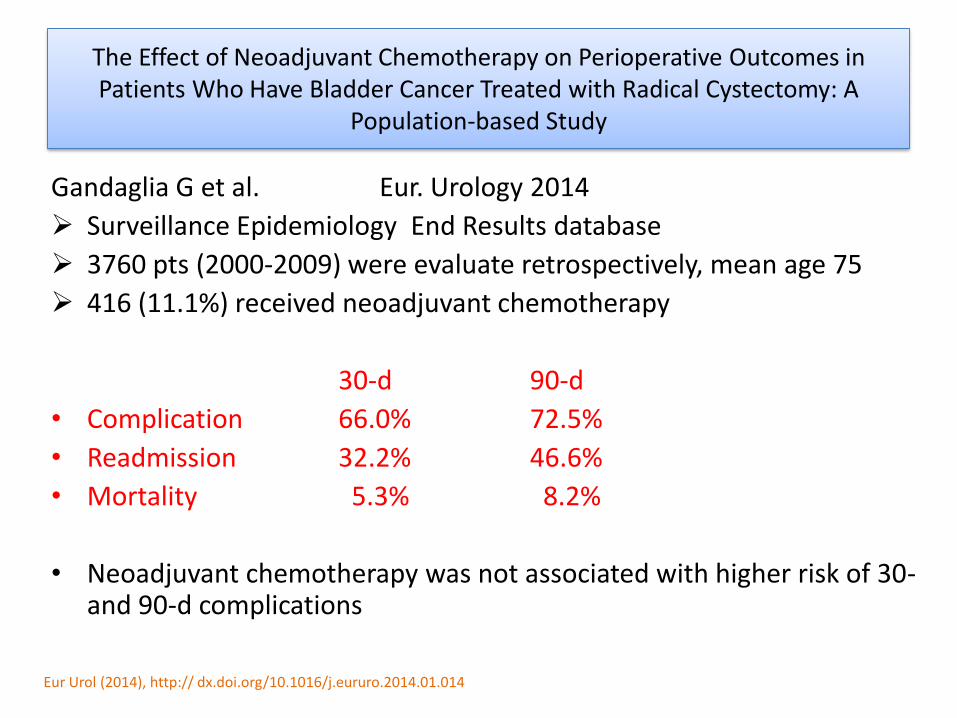
The Effect of Neoadjuvant Chemotherapy on Perioperative Outcomes in Patients Who Have Bladder Cancer Treated with Radical Cystectomy: A
Population-based Study
Gandaglia G et al. Eur. Urology 2014
Surveillance Epidemiology End Results database
3760 pts (2000-2009) were evaluate retrospectively, mean age 75
416 (11.1%) received neoadjuvant chemotherapy
30-d 90-d
• Complication 66.0% 72.5%
• Readmission 32.2% 46.6%
• Mortality 5.3% 8.2%
• Neoadjuvant chemotherapy was not associated with higher risk of 30-and 90-d complications
Eur Urol (2014), http:// dx.doi.org/10.1016/j.eururo.2014.01.014
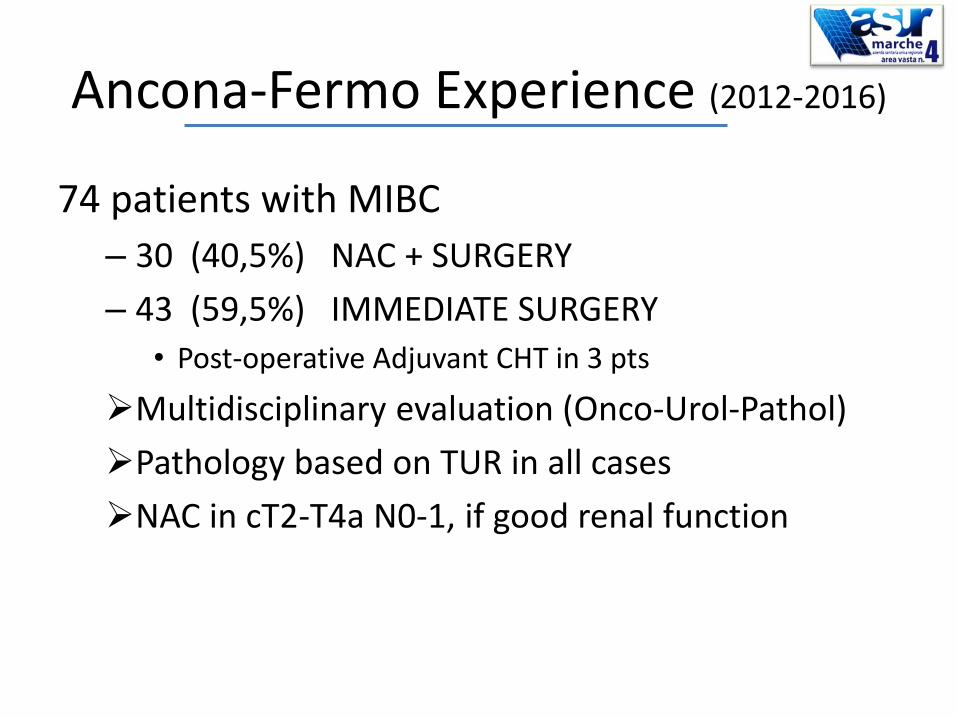
Ancona-Fermo Experience (2012-2016)
74 patients with MIBC
– 30 (40,5%) NAC + SURGERY
– 43 (59,5%) IMMEDIATE SURGERY
• Post-operative Adjuvant CHT in 3 pts
Multidisciplinary evaluation (Onco-Urol-Pathol)
Pathology based on TUR in all cases
NAC in cT2-T4a N0-1, if good renal function
Methods: NeoAdjuvantChemotherapy
1. Baseline chest-abdominal CT
2. Imaging after 2-3 cycles US or CT
3. If response, futhrer 2-3 cycles were added(80%)
4. Re-staging after completed NAC
5. Wash-out/recovery after NAC (3 weeks)
6. Surgery
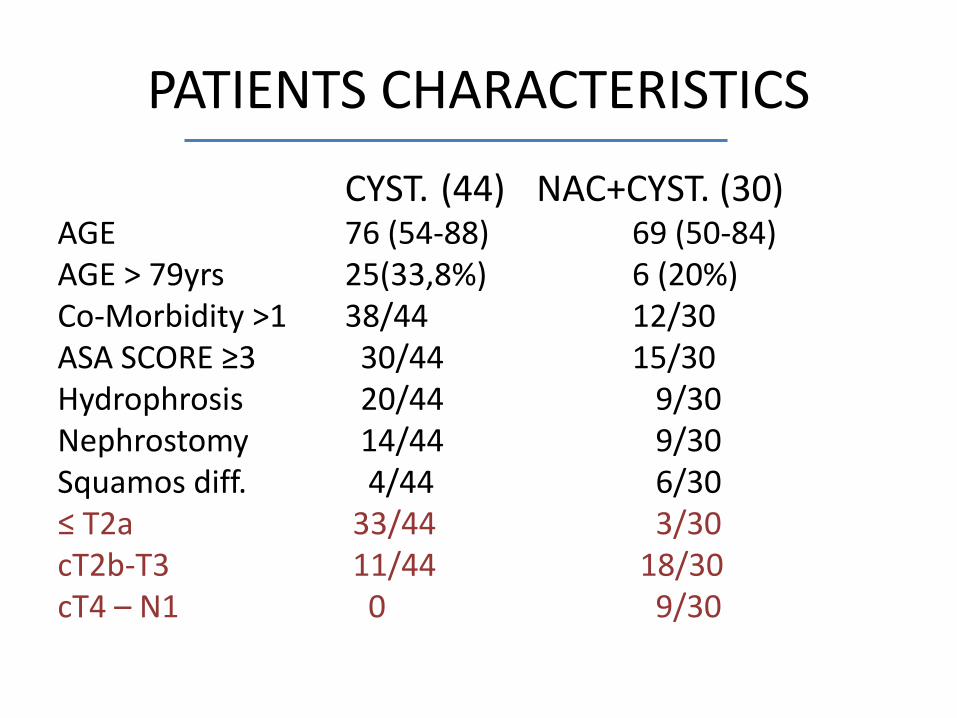
PATIENTS CHARACTERISTICS
CYST. (44) NAC+CYST. (30)AGE 76 (54-88) 69 (50-84)AGE > 79yrs 25(33,8%) 6 (20%)Co-Morbidity >1 38/44 12/30ASA SCORE ≥3 30/44 15/30Hydrophrosis 20/44 9/30Nephrostomy 14/44 9/30Squamos diff. 4/44 6/30≤ T2a 33/44 3/30cT2b-T3 11/44 18/30cT4 – N1 0 9/30
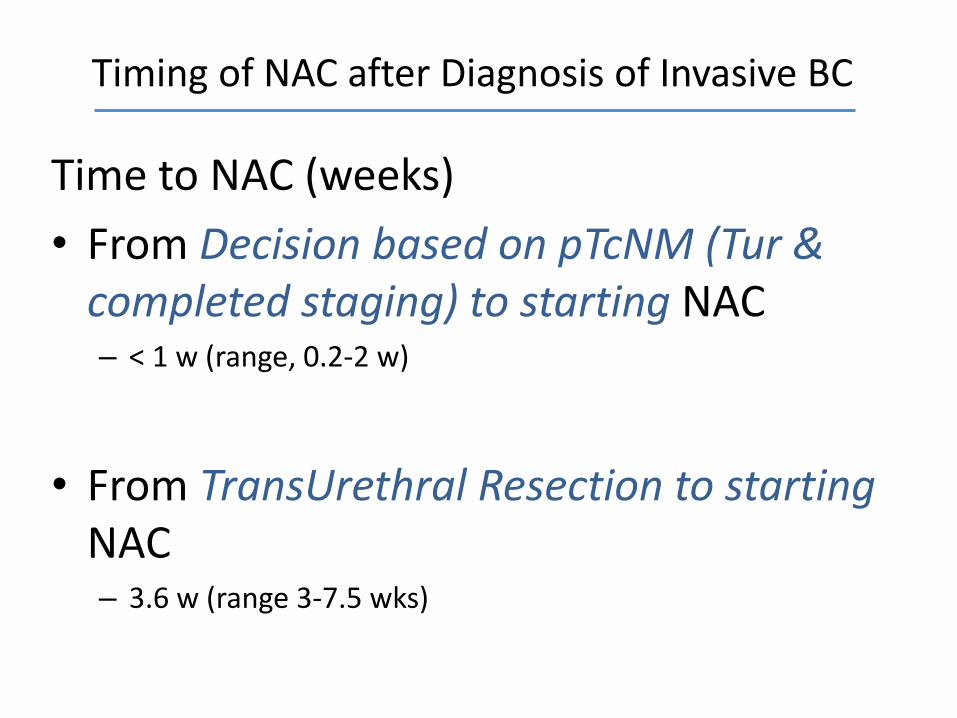
Timing of NAC after Diagnosis of Invasive BC
Time to NAC (weeks)
• From Decision based on pTcNM (Tur &completed staging) to starting NAC– < 1 w (range, 0.2-2 w)
• From TransUrethral Resection to starting NAC– 3.6 w (range 3-7.5 wks)
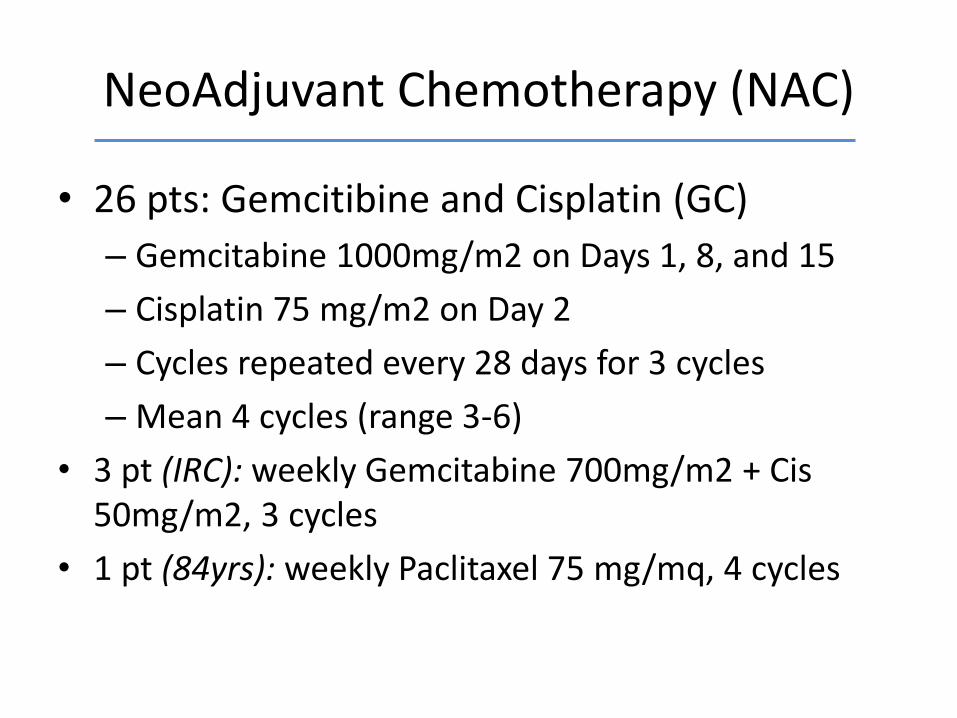
NeoAdjuvant Chemotherapy (NAC)
• 26 pts: Gemcitibine and Cisplatin (GC)
– Gemcitabine 1000mg/m2 on Days 1, 8, and 15
– Cisplatin 75 mg/m2 on Day 2
– Cycles repeated every 28 days for 3 cycles
– Mean 4 cycles (range 3-6)
• 3 pt (IRC): weekly Gemcitabine 700mg/m2 + Cis 50mg/m2, 3 cycles
• 1 pt (84yrs): weekly Paclitaxel 75 mg/mq, 4 cycles
• Ancillary procedures– 3 pt Bilateral hydronephrosis: Nephrostomy + stent– 6 pts Monolateral hydronephr.: Nephrostomy– 2 times Nephrostomy displacement– Placement of filter in the v. cava before surgery
• 4 Deep Venous Trombosis detectet at re-staging CT– 2 asymptomatic Pulmonary Embolism
• 3 Infection (2 UTI, 1 Respiratory)• 2 Mild worseing renal funcion, reversable (1.7, 3.1)• 10 Transient Thrombocitopenia, 2 neutropenia• Any BLEEDING
NeoAdjuvantChemotherapy (NAC)
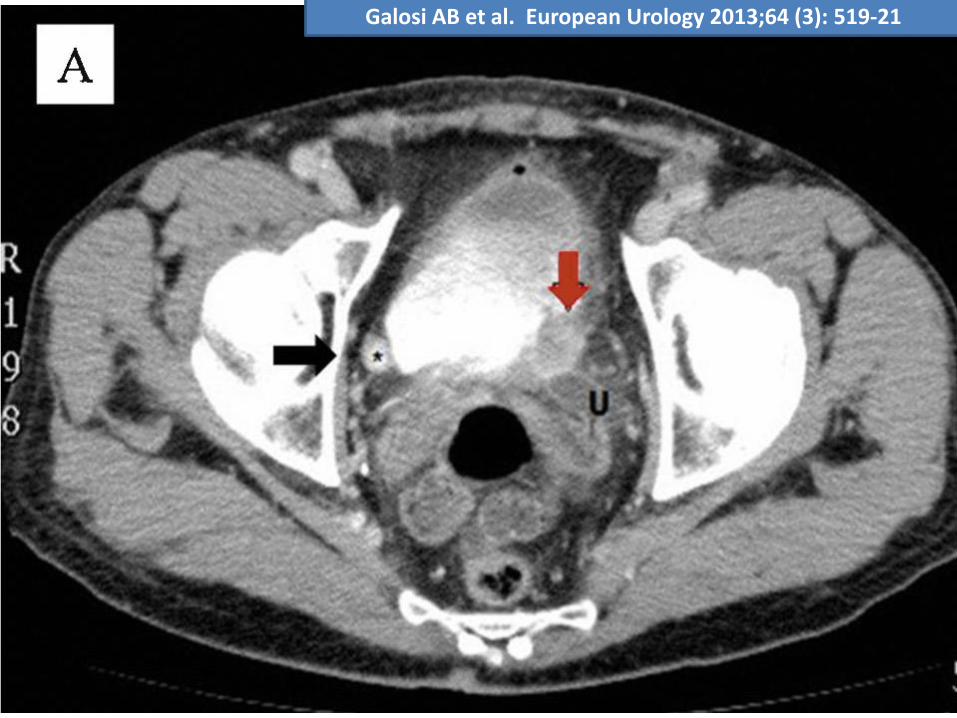
Galosi AB et al. European Urology 2013;64 (3): 519-21
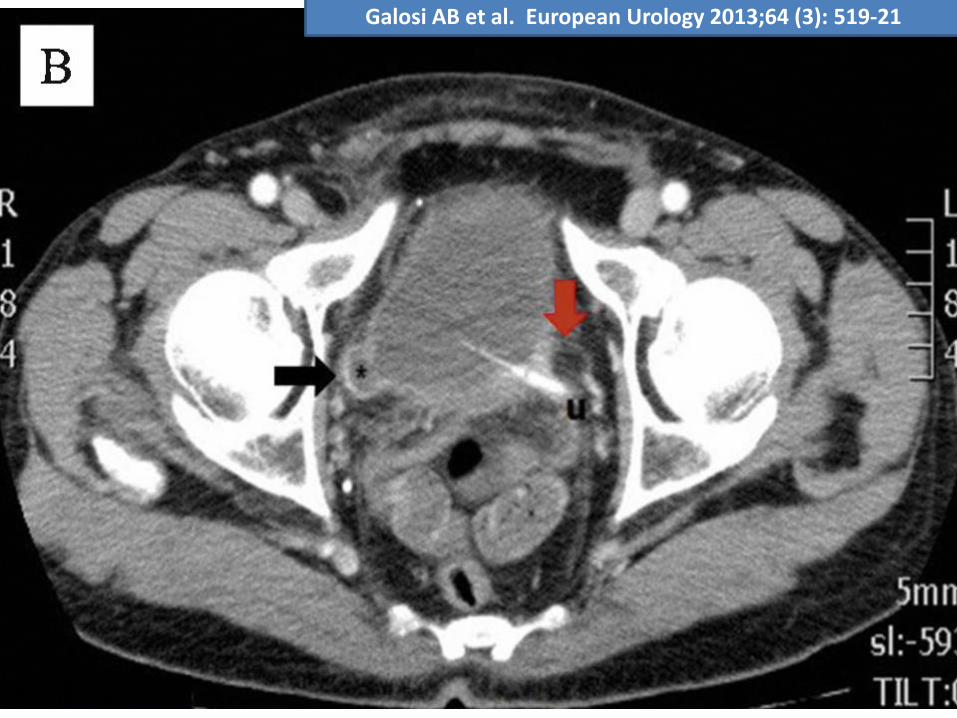
Galosi AB et al. European Urology 2013;64 (3): 519-21
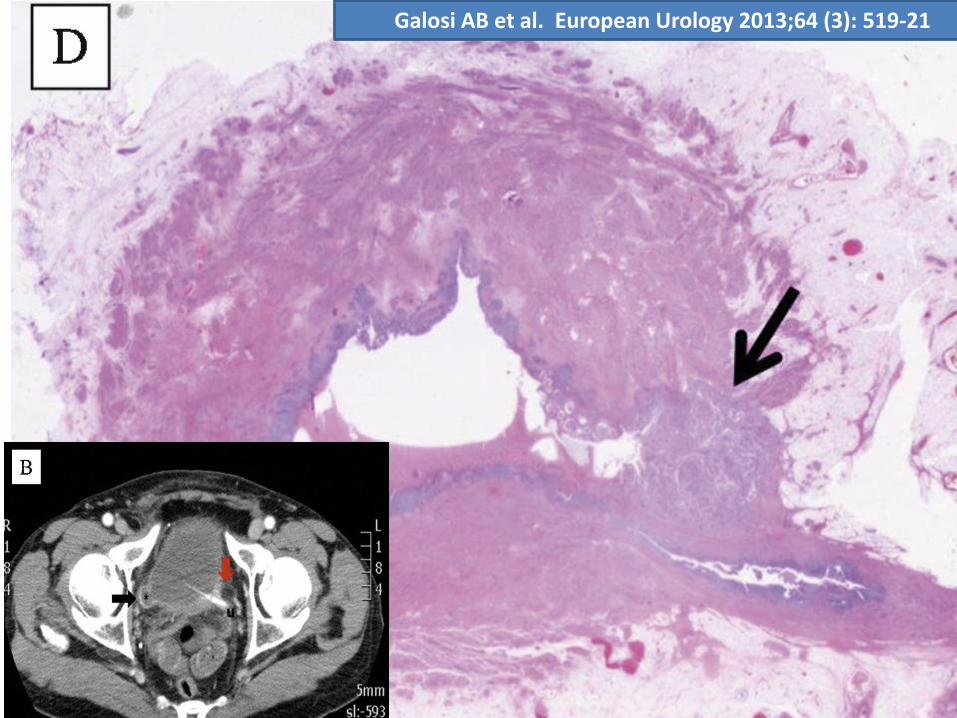
Galosi AB et al. European Urology 2013;64 (3): 519-21
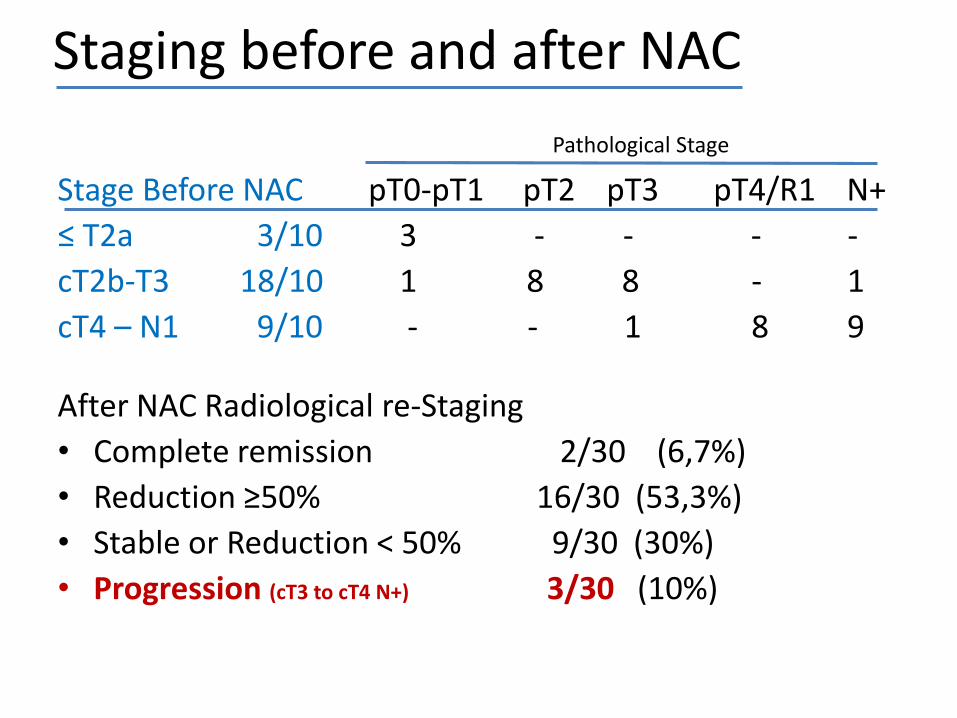
Staging before and after NAC
Stage Before NAC pT0-pT1 pT2 pT3 pT4/R1 N+
≤ T2a 3/10 3 - - - -
cT2b-T3 18/10 1 8 8 - 1
cT4 – N1 9/10 - - 1 8 9
After NAC Radiological re-Staging
• Complete remission 2/30 (6,7%)
• Reduction ≥50% 16/30 (53,3%)
• Stable or Reduction < 50% 9/30 (30%)
• Progression (cT3 to cT4 N+) 3/30 (10%)
Pathological Stage
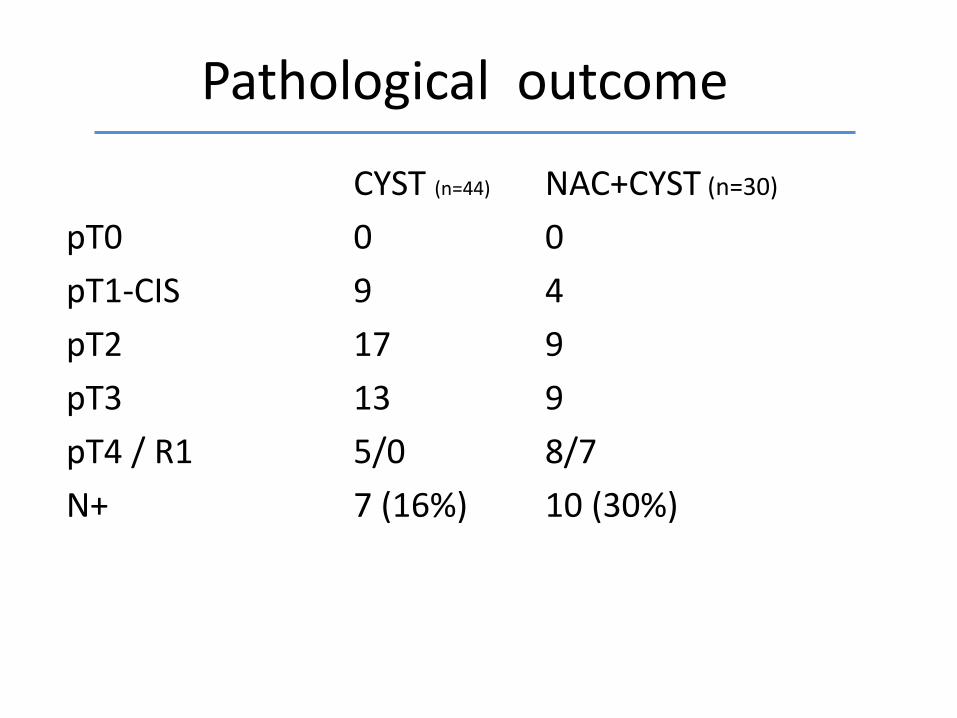
Pathological outcome
CYST (n=44) NAC+CYST (n=30)
pT0 0 0
pT1-CIS 9 4
pT2 17 9
pT3 13 9
pT4 / R1 5/0 8/7
N+ 7 (16%) 10 (30%)
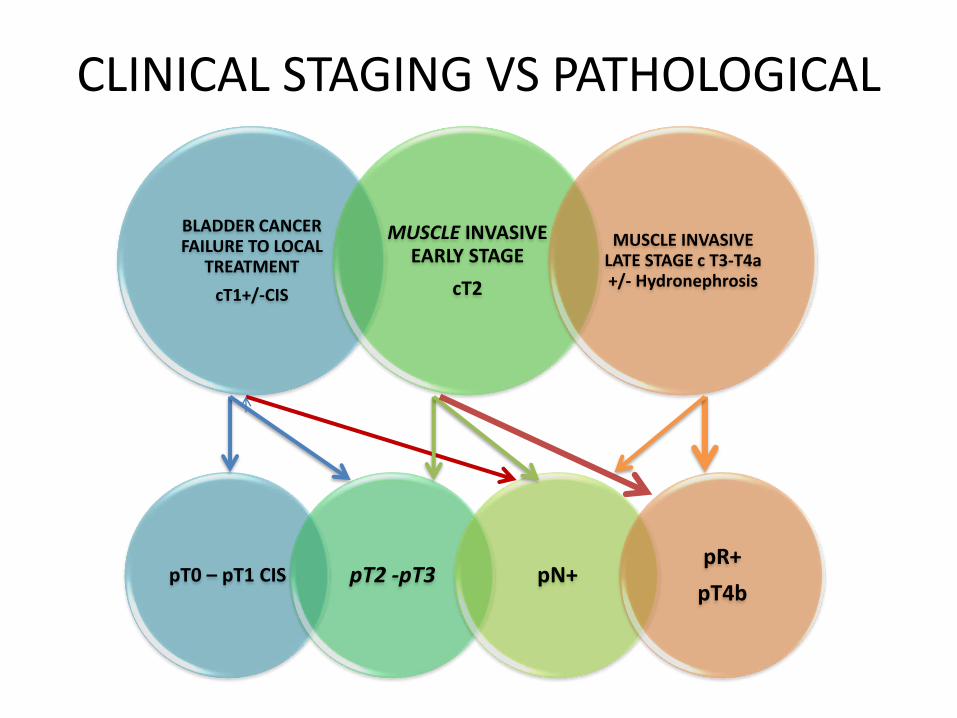
CLINICAL STAGING VS PATHOLOGICAL
BLADDER CANCER FAILURE TO LOCAL
TREATMENT
cT1+/-CIS
MUSCLE INVASIVE EARLY STAGE
cT2
MUSCLE INVASIVE LATE STAGE c T3-T4a +/- Hydronephrosis
pT0 – pT1 CIS pT2 -pT3 pN+pR+
pT4b
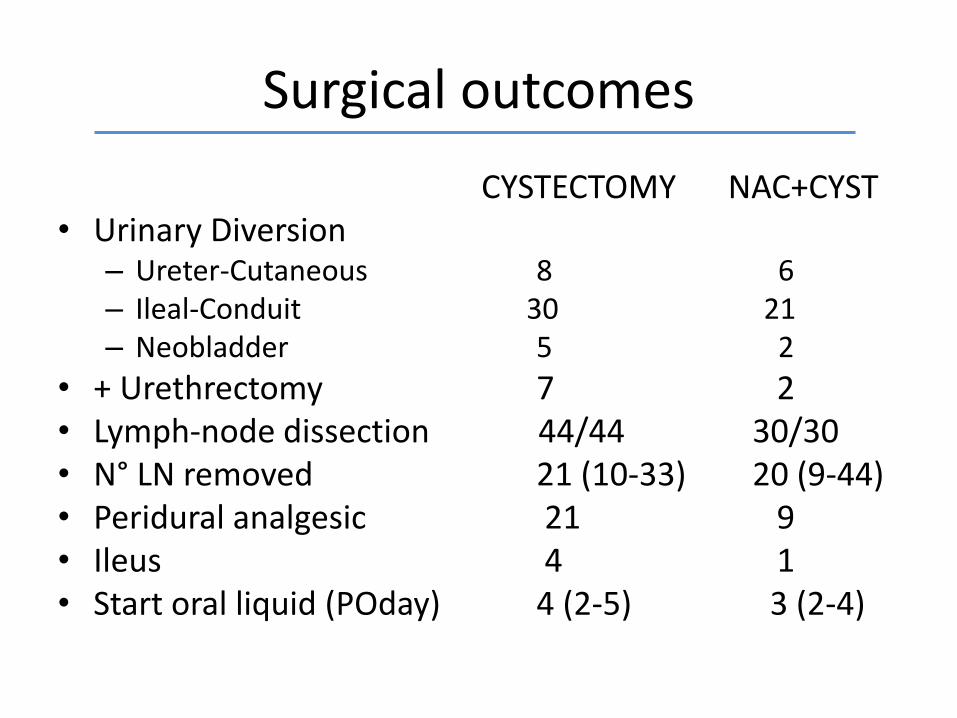
Surgical outcomes
CYSTECTOMY NAC+CYST• Urinary Diversion
– Ureter-Cutaneous 8 6– Ileal-Conduit 30 21– Neobladder 5 2
• + Urethrectomy 7 2• Lymph-node dissection 44/44 30/30• N° LN removed 21 (10-33) 20 (9-44)• Peridural analgesic 21 9• Ileus 4 1• Start oral liquid (POday) 4 (2-5) 3 (2-4)
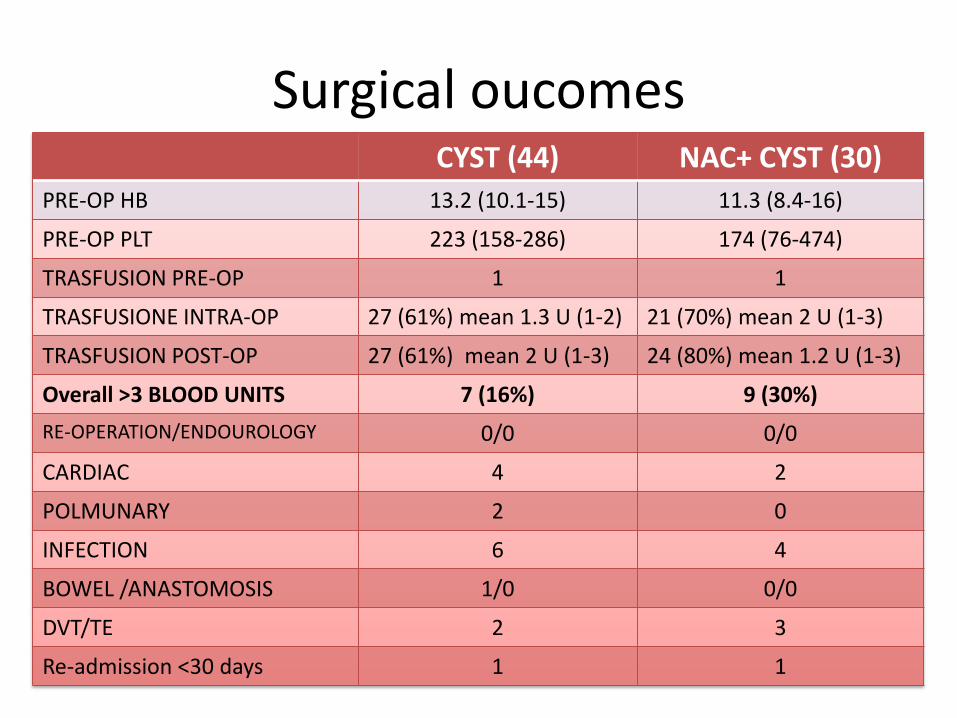
Surgical oucomesCYST (44) NAC+ CYST (30)
PRE-OP HB 13.2 (10.1-15) 11.3 (8.4-16)
PRE-OP PLT 223 (158-286) 174 (76-474)
TRASFUSION PRE-OP 1 1
TRASFUSIONE INTRA-OP 27 (61%) mean 1.3 U (1-2) 21 (70%) mean 2 U (1-3)
TRASFUSION POST-OP 27 (61%) mean 2 U (1-3) 24 (80%) mean 1.2 U (1-3)
Overall >3 BLOOD UNITS 7 (16%) 9 (30%)
RE-OPERATION/ENDOUROLOGY 0/0 0/0
CARDIAC 4 2
POLMUNARY 2 0
INFECTION 6 4
BOWEL /ANASTOMOSIS 1/0 0/0
DVT/TE 2 3
Re-admission <30 days 1 1
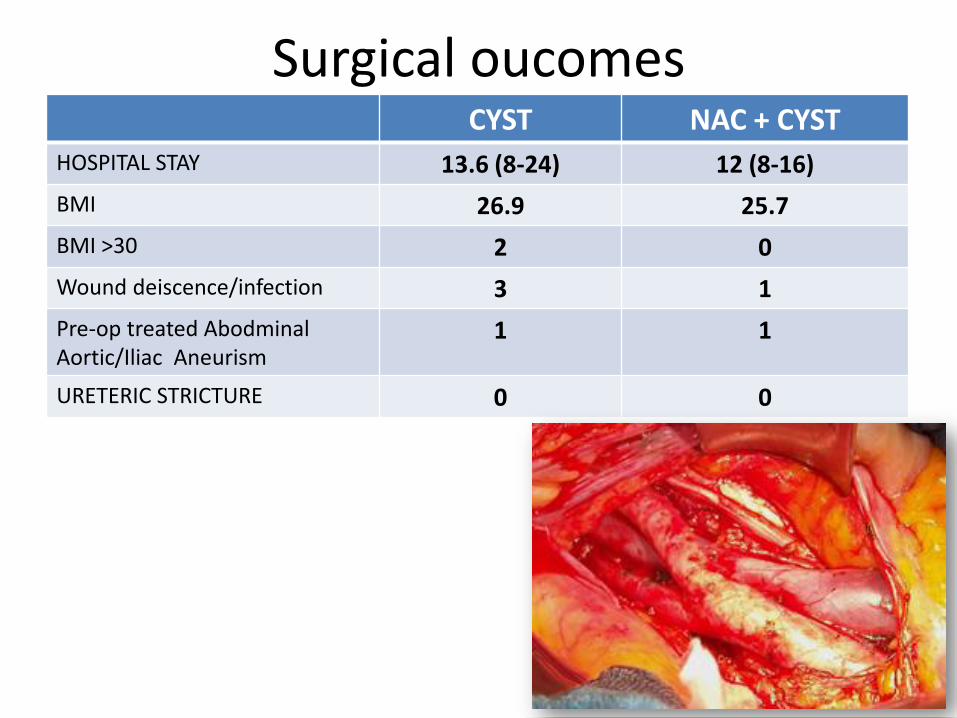
Surgical oucomesCYST NAC + CYST
HOSPITAL STAY 13.6 (8-24) 12 (8-16)
BMI 26.9 25.7
BMI >30 2 0
Wound deiscence/infection 3 1
Pre-op treated AbodminalAortic/Iliac Aneurism
1 1
URETERIC STRICTURE 0 0
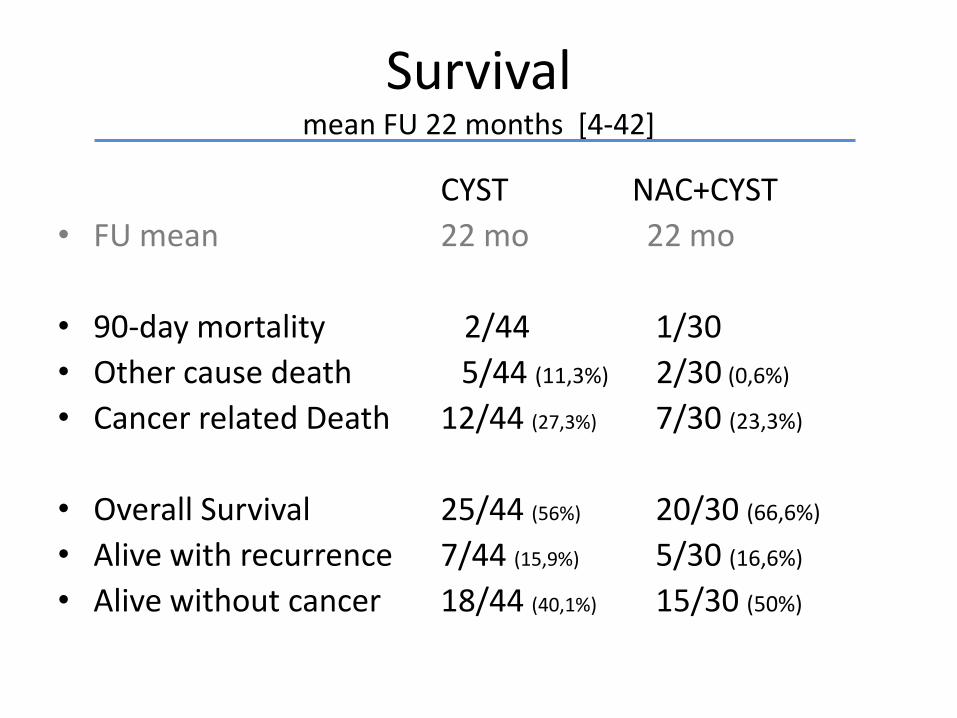
Survivalmean FU 22 months [4-42]
CYST NAC+CYST
• FU mean 22 mo 22 mo
• 90-day mortality 2/44 1/30
• Other cause death 5/44 (11,3%) 2/30 (0,6%)
• Cancer related Death 12/44 (27,3%) 7/30 (23,3%)
• Overall Survival 25/44 (56%) 20/30 (66,6%)
• Alive with recurrence 7/44 (15,9%) 5/30 (16,6%)
• Alive without cancer 18/44 (40,1%) 15/30 (50%)
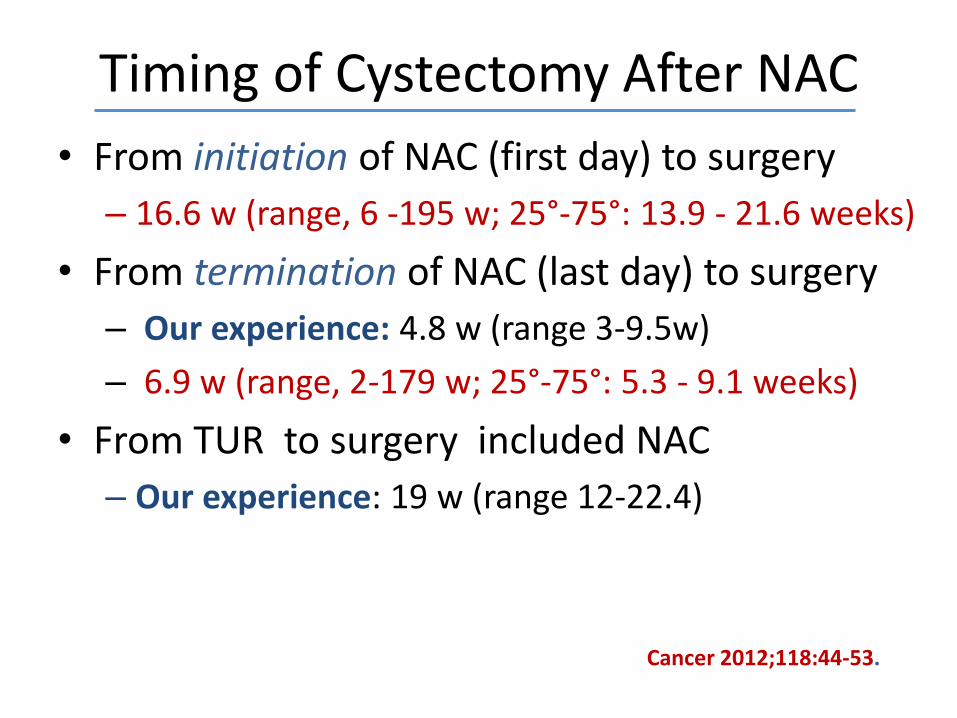
Timing of Cystectomy After NAC
• From initiation of NAC (first day) to surgery
– 16.6 w (range, 6 -195 w; 25°-75°: 13.9 - 21.6 weeks)
• From termination of NAC (last day) to surgery
– Our experience: 4.8 w (range 3-9.5w)
– 6.9 w (range, 2-179 w; 25°-75°: 5.3 - 9.1 weeks)
• From TUR to surgery included NAC
– Our experience: 19 w (range 12-22.4)
Cancer 2012;118:44-53.
• NAC time added
–12 w (10-16w)
• Improved scheduling in Operating Room
Timing of Cystectomy After NAC
CYSTECTOMY FOR BLADDER CANCER
NEO-ADJUVANT CHT
MUSCLE INVASIVE LATE STAGE T3-T4a +/-
Hydronephrosis
MUSCLE INVASIVE EARLY STAGE - T2
BLADDER CANCER FAILURE
TO LOCAL TREATMENT
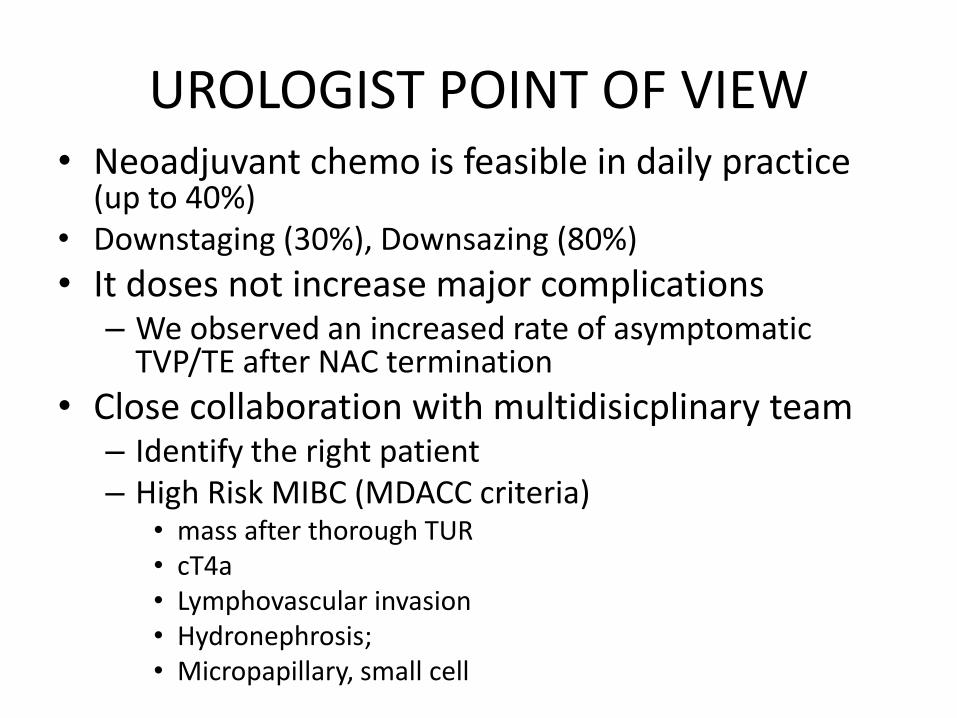
UROLOGIST POINT OF VIEW• Neoadjuvant chemo is feasible in daily practice
(up to 40%)• Downstaging (30%), Downsazing (80%)
• It doses not increase major complications– We observed an increased rate of asymptomatic
TVP/TE after NAC termination
• Close collaboration with multidisicplinary team– Identify the right patient– High Risk MIBC (MDACC criteria)
• mass after thorough TUR• cT4a• Lymphovascular invasion• Hydronephrosis;• Micropapillary, small cell