Embed Size (px)
Citation preview

9/3/2019
1
Moving the ICU to the ED to Improve Patient Outcomes: Focus on ARDS,
Sepsis and PEMarin H. Kollef, MD
Professor of Medicine
Virginia E. and Sam J. Golman Chair in
Respiratory Intensive Care Medicine
Washington University School of Medicine
St. Louis, Missouri
Conflicts of Interest
Academy of Infection ManagementAllerganAridisMerckShinogi
Timing is Crucial in the ED! - Do not Delay Fluids/Antibiotics/Pressors/Optimal Vent Settings

9/3/2019
2
Background: Mechanical Ventilation in the ED
Easter B, Fischer C, Fisher J. Amer J Em Med. 2012;30:1183-1188
Common: 300,000 annually
Deadly: 25% mortality
Pulmonary complications: high
incidenceFuller BM, et al. Acad Emerg Med 2013. Fuller BM, et al. Chest 2015.Dettmer MR, et al. J Crit Care 2015.Mikkelsen ME, et al. Shock 2013.
IMPROVE Study Group. N Engl J Med 2013; 369: 428-43 7.
Neto AS, Cardoso SO, et al. JAMA 2012;308(16):1651-1659
Lung-Protective Ventilation in At-Risk Patients
Preliminary Data- Lung Protection Uncommon
Fuller BM, Mohr NM , Dettmer M. Acad Emerg Med. 201 3 ; 20: 659-669.
Fuller BM, et al. CHEST 2015; 148(2): 365-374.

9/3/2019
3
Study Objectives
Evaluate the effectiveness of an ED-based lung-protective mechanical ventilation protocol on reducing the incidence of pulmonary complications including progression to ARDS
Design and SubjectsSingle-center, quasi-experimental before (2009-2013) - after (2015-2016) study
Population: mechanically ventilated adult ED patients
Primary Outcome: ARDS + VAC
Design
n=1,192 n=513
Fuller BM, et al. BMJ Open 2016; 6e010991.

9/3/2019
4
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.
Pre-intervention
Group (n= 1,192)
Intervention
Group (n= 513)
P value
Age (yr) 60.4 (21.1) 58.0 (24.0) <0.001
Male, n (%) 628 (52.7) 303 (59.0) 0.02
Caucasian
African-American
Other
478 (40.1)
698 (58.6)
16 (1.3)
232 (45.2)
280 (54.6)
1 (0.2)
0.05
0.13
0.03
Comorbidities, n (%)
Diabetes
Cirrhosis
CHF
Dialysis
COPD
Immunosuppression
Alcohol abuse
HIV/AIDS
427 (35.8)
84 (7.0)
289 (24.2)
95 (8.0)
304 (25.5)
95 (8.0)
177 (14.8)
29 (2.4)
166 (32.4)
41 (8.0)
115 (22.4)
43 (8.4)
122 (23.8)
66 (12.9)
76 (14.8)
6 (1.2)
0.17
0.49
0.31
0.77
0.45
0.01
0.99
0.09
Height (in) 67.1 (4.1) 67.9 (3.9) <0.001
Weight (kg) 84.7 (30.6) 83.9 (26.5) 0.68
BMI 29.3 (10.7) 28.2 (8.8) 0.07
Temperature (Celsius) 36.9 (1.1) 36.5 (1.2) <0.001
Mean arterial pressure 87.3 (22.5) 84.0 (41.6) 0.34
Lactate 2.2 (1.4-3.9) 3.0 (1.6-5.2) <0.001
APACHE II* 14.0 (8.0) 17.0 (13.0) <0.001
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.
Results- Ventilator Settings
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.

9/3/2019
5
Results- Tidal Volume
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.
Results- Clinical Outcomes
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.
Results- Clinical OutcomesPropensity-
matched
Fuller BM, et al. Ann Emerg Med. 2017;70:406-418.

9/3/2019
6
Baseline characteristics Preintervention (n= 186) Intervention Group (n= 43) P value
Age (yr) 57.7 (50.9-71.9) 57.5 (43.5-66.3) 0.14
Male, n (%) 106 (57.0) 28 (65.1) 0.33
Race, n (%)
Caucasian
African-American
Other
97 (52.2)
86 (46.2)
3 (1.6)
22 (51.2)
22 (51.2)
0 (0.0)
0.91
0.56
0.40
BMI 29.9 (11.0) 30.5 (13.4) 0.30
MAP 79.3 (20.9) 75.0 (36.0) 0.30
Lactate 3.0 (1.9-6.0) 4.7 (2.3-7.9) 0.06
APACHE II 17.1 (5.5) 23.7 (7.8) <0.01
SOFA 6.0 (4-8) 8.0 (4-9) 0.02
Reason for mechanical ventilation, n (%)
Medical
Trauma
Other
129 (69.4)
20 (10.8)
37 (19.9)
33 (83.7)
5 (11.6)
5 (11.6)
0.34
0.87
0.21
Sepsis, n (%) 101 (54.3) 30 (69.7) 0.17
Intravenous fluids in ED (liters) 2.5 (2.0) 1.7 (1.6) 0.15
Blood products, n (%) 33 (17.7) 10 (23.3) 0.40
Central venous catheter, n (%) 89 (47.8) 22 (51.2) 0.70
Antibiotics, n (%) 96 (51.6) 29 (67.4) 0.11
Vasopressor infusion, n (%) 69 (37.1) 24 (55.8) 0.02
Fuller BM, et al. Crit Care Med 2017;45:645-652.
Fuller BM, et al. Crit Care Med 2017;45:645-652.
Pre-Intervention
group (n= 186)
Intervention group (n= 43)
Adjusted Odds Ratio or Between-Group Difference
(95% CI)
P value
Mortality, n(%) 102 (54.8)
17 (39.5)
0.38 (0.17 - 0.83)
0.02
Secondary outcomes (days)Ventilator-freeICU-freeHospital-free
7.7 (9.9)7.2 (9.4)4.0 (6.3)
11.6 (10.8)9.1 (9.2)5.7 (7.7)
0.010.180.13

9/3/2019
7
Septic shock: persisting hypotension; requiring vasopressors to maintain MAP ≥65 mm Hg; lactate level >2 mmol/L despite adequate volumes
Singer M, et a. JAMA 2016;315:801-810.
Shankar-Hari M, et al. JAMA 2016;315:775-87.

9/3/2019
8
Increased Mortality With Inadequate Antibiotic Therapy in Infections Requiring ICU Admission
ICU=intensive care unit.
Site of infection includes bloodstream, lung, wound, gastrointestinal tract, urinary tract, and miscellaneous (includes peritoneal infection, meningitis, endocarditis, and infections of the skin and fascia).
Kollef MH. Chest 1999;115:462-474.
Hosp
ital M
ort
ality
(%
)
0
10
20
30
40
60
All Cause
P<.001
Infection Related
P<.001
Mortality Type
Inadequate antimicrobial treatment
Adequate antimicrobial treatment
5052%
24%
42%
18%
655 (32.8%) infected169 (25.8%) inappropriate treatmentN = 2000
Park SY, et al. Int J Antimicrob Agents 2018; doi:10. 1016/j.ijantimicag.2017.10.018
• 146 patients with CRABC bacteraemic pneumonia
• 128 (87.7%) patients were treated in the ICU
• 110 (75.3%) had VAP
• 42 (28.8%) received appropriate empirical therapy
Liu VX, et al. AJRCCM 2017;196:856-863.35,000 randomly selected sepsis inpatients 21 emergency depart ments 2010-2013 Northern CA.

9/3/2019
9
In multivariable model, each hour of time to complete 3-hour bundle a/w
higher mortality
(OR, 1.04; 95%CI, 1.02 to 1.05; P<0.001)
Seymour CW, et al. NEJM 2017; 376:2235-2244.
Alam N, et al. Lancet Respir Med 2018;6:40-50.
• Ceftriaxone 2 g vs. Placebo in ambulance• Netherlands• 75% of bacteria staph, strep, E. coli
JAMA. 2014;311(13):1308-1316.
Mortality Severe Sepsis and Septic Shock in Australia and New Zealand, 2000-2012

9/3/2019
10
Rivers E et al. N Engl J Med 2001;345:1368-1377.
Rivers E et al. N Engl J Med 2001;345:1368-1377.
Standard Therapy EGDTMortality: 46.5% 30.5%
P = 0.009
The PRISM Investigators. N Engl J Med 2017;376:2223-2234.

9/3/2019
11
The PRISM Investigators. N Engl J Med 2017;376:2223-2234.
EGDT Cont EGDT Cont EGDT Cont EGDT ContLactate 7.7 6.9 4.8 5.0 6.7 6.6 7.0 6.8ScvO2 48.6% 49.2% - - 76% - 74% -
Death 30.5% 45.5% 21% 18.9% 18.6% 18.8% 29.5% 29.2%
Rivers PROCESS ARISE ProMISe
Are The Patients the Same?
NO!
Holst LB et al. N Engl J Med 2014;371:1381-1391.
Blood Hemoglobin Levels in Patients in the ICU at Baseline and after Randomization

9/3/2019
12
Time to Death and Relative Risk of Death at 90 Days
Holst LB et al. N Engl J Med 2014;371:1381-1391.
Caironi P et al. N Engl J Med 2014;370:1412-1421.
Albumin through D 28 and Net Fluid through D 7
Caironi P et al. N Engl J Med 2014;370:1412-1421.
Probability Survival from Randomization through Day 90

9/3/2019
13
Asfar P et al. N Engl J Med 2014;370:1583-1593.
MAP during the 5-Day Study Period
De Backer D et al. N Engl J Med 2010;362:779-789.
Norepinephrine Shortage US Hospitals 2011
Vail E, et al. JAMA 2017 Apr 11;317(14):1433-1442.

9/3/2019
14
Early Vasopressin v Norepinephrine: Kidney Failure in Septic Shock
Gordon AC, et al. JAMA. 2016;316:509-518.
Khanna A et al. N Engl J Med 2017. DOI: 10.1056/NEJMoa1704154

9/3/2019
15
Khanna A et al. N Engl J Med 2017. DOI: 10.1056/NEJMoa1704154
Volbeda M et al. Intensive Care Med 2015;41:1220-123 4.
CortocosteroidsIn Septic Shock
CHEST 2016 149, 209-219DOI: (10.1378/chest.15-1733)
Corticosteroids Severe CAP

9/3/2019
16
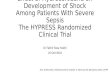
JAMA. 2016;316(17):1775-1785. doi:10.1001/jama.2016.14799
JAMA 2016;316(17):1775-1785
Continuous infusion 200 mg HCT 5 d followed by dose tapering until d 11
Effect of Hydrocortisone on Development of Shock Among Patients With Severe Sepsis -The HYPRESS Trial
Venkatesh B, et al. N Engl J Med 2018; 378:797-808. Annane D, et al. N Engl J Med 2018; 378:809-81 8.
Hydrocortisone 50-mg IV q 6 hours/fludrocortisone 5 0-µg poContinuous infusion hydrocortisone 200 mg per day
Adjunctive Corticosteroids for Septic Shock

9/3/2019
17
Mean Daily Fluid Balance
Mil
lili
ters
Day
†
†
†
†
†
*†
*†
*†* *
Survivors
Nonsurvivors
Murphy CV et al. Chest 2009;136:102-109.
Cumulative Daily Fluid Balance
Mil
lili
ters
Day
††
†
†
*† * **
*
Nonsurvivors
Survivors
Murphy CV et al. Chest 2009;136:102-109.
Optimizing the Ebb and Flow Phases
Adequate Fluid Resuscitation
Conservative Fluid Management
+
+
-
+
+
-
-
-
n=93 n=31 n=53 n=35
P < 0.001
Murphy CV et al. Chest 2009;136:102-109.

9/3/2019
18
Zambia: 6-hour sepsis protocol emphasizing IVFs, va sopressors, and RBCs in the ED for patients with septic shock
Andrews B, et al. JAMA 2017;318:1233-1240.
Shackelford SA, et al. JAMA 2017 Oct 24;318:1581-15 91.
Hoste EA, et al. British Journal of Anaesthesia 201 4;113: 740–747.
Four Phases of Intravenous Fluid Therapy

9/3/2019
19
Traditional Methods for Detection of BSI
Gram Stain
18 – 24 h
Hours to Days
Subculture
Organism identification
and susceptibility
testing
Traditional Methods for Detection of BSI
Accurate but slow!
Ideal Diagnostic Tool for Sepsis

9/3/2019
20
Vazquez C, Kollef MH. Clin Infect Dis 2018.
Acinetobacter spp.
EET = effective empiric therapyIET = ineffective empiric therapyRDDT = rapid diagnostic directed treatment
Douglas I. Curr Opin Infect Dis 2016;29:197-204.
Timing of Microbiologic Diagnostics
BiofireCuretis

9/3/2019
21
PERTPE Response Team
Rodriguez-Lopez J, et al. Semin Respir Crit Care Med 2017;38:51-55.
Rodriguez-Lopez J, et al. Semin Respir Crit Care Med 2017;38:51-55.
Mean 9.22 6.31 6.86 4.4 12,219 16,843 13.38 15.07
SD 16.09 7.44 9.35 5.05 20,957 25,242
Pvalue
.004 .006 .12 .72
Control PERT Control PERT Control PERT Control PERT
Hospital LOS ICU LOS Direct Cost Mort ality
Xenos ES, et al. J Vasc Surg 2018;67:e13-e14.
U Kentucky Lexington PERT Experience

9/3/2019
22
Thank you!