Embed Size (px)
Citation preview

Treatment with Hydrocortisone and Fludrocortisone in Septic Shock
• Prospective, R, P-C, D-B trial, n = 300
• 19 ICUs in France, 10/95 – 2/99
• Relative adrenal insufficiency defined as response of 9ug/dl or less on ACTH stim test
• Randomization within 8 hrs of septic shock
• Hydrocortisone 50mg IV q 6 hours, and fludrocortisone 50 mcg via NG daily, 7 days
• Outcome measure: 28-day survival in non-responders to ACTH stimulation test.
Annane D et al. JAMA August 2002;288:862-871

Treatment with Hydrocortisone and Fludrocortisone in Septic Shock
• 229 pts with adrenal insufficiency (76.6%)• Median time to vasopressor withdrawal in
patients with adrenal insufficiency:– 7 days in corticosteroid group
– 10 days in placebo group
– HR 1.91 (95% CI, 1.29-2.84, p = 0.001)
• Adverse Events:– No significant differences between groups
Annane D et al. JAMA August 2002;288:862-871

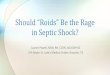
Treatment with Hydrocortisone and Fludrocortisone in Non-responders
Annane D et al. JAMA August 2002;288:862-871
Variable Placebo Steroids Adjusted OR (95% CI) P value
# pts 115 114
28-day mortality 73 (63%) 60 (53%) 0.54
(0.31-0.97) .04
ICU mortality 81 (70%) 66 (58%) 0.50
(0.28-0.89) .02
Hospital mortality 83 (72%) 70 (61%) 0.53
(0.29-0.96) .04
1-year mortality 88 (77%) 77 (68%) 0.57
(0.31-1.04) .07

Treatment with Hydrocortisone and Fludrocortisone in Septic Shock
• Conclusion:
• A 7-day treatment with low dose of hydrocortisone and fludrocortisonesignificantly reduced the risk of death in patients with septic shock and relative adrenal insufficiency without increasing adverse events.
Annane D et al. JAMA August 2002;288:862-871

Adrenal Insufficiency in Septic Shock• Prospective observational study (n=66)
• University of Hawaii, Surgical ICU
• Thyrotropin and baseline cortisol levels were obtained at 3 am
• Cortrosyn stimulation test (250 mcg), 1-hr cortisol level
• Mean age was 62 (19) years, Mean APACHE II score 21(5)
• Mortality 22.7%
• Adrenal insufficiency present in 65.1% of patients
• 12% incidence of simultaneous hypothyroidism and adrenal insufficiency
HO HC et al. Arch Surg. 2004 Nov;139(11):1199-203





Which patients will benefit from steroids?
• “Relative Adrenal Insufficiency Syndrome”
• Deficiencies in current measurement strategies:– Total (free plus protein-bound) cortisol is measured– Free Cortisol concentrations may be more accurate
• “Rapid hemodynamic improvement of catecholamine-dependent patients after the administration of low-dose corticosteroids still seems the best available clue to diagnosis.”
Ligtenberg JJ, Zijlstra JG. Curr Opin Crit Care 2004 Dec;10(6):456-60

Surviving Sepsis Guidelines - 2004
Crit Care Med 2004;32(3):858-873

Surviving Sepsis Guidelines

Surviving Sepsis Guidelines

Sepsis Resuscitation Bundle
• The Severe Sepsis Resuscitation Bundledescribes seven tasks that should begin immediately, but must be accomplished within the first 6 hours of presentation for patients with severe sepsis or septic shock.
• Some items may not be completed if the clinical conditions described in the bundle do not prevail in a particular case, but clinicians must assess for them.
• The goal is to perform all indicated tasks 100 percent of the time within the first 6 hours of identification of severe sepsis.

Sepsis Resuscitation BundleChanges targeted for Improvement:
• Serum Lactate Measured
• Blood Cultures Obtained Prior to Antibiotic Administration
• Improve Time to Broad-Spectrum Antibiotics
• Treat Hypotension and/or Elevated Lactate with Fluids
• Apply Vasopressors for Ongoing Hypotension
• Maintain Adequate Central Venous Pressure
• Maintain Adequate Central Venous Oxygen Saturation

Sepsis Resuscitation Bundle1. Serum lactate measured
2. Blood cultures obtained prior to antibiotic administration
3. From the time of presentation, broad-spectrum antibiotics administered within 3hrs for ED admissions and 1hr for non-ED ICU admissions
4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): 1. Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid
equivalent)2. Apply vasopressors for hypotension not responding to initial
fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg
5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dl):
1. Achieve central venous pressure (CVP) of > 8 mm Hg2. Achieve central venous oxygen saturation (ScvO2) of > 70%3. *Mixed venous oxygen saturation (SvO2) > 65 percent is an
acceptable alternative.

Sepsis Management Bundle
• The Sepsis Management Bundle lists four management goals.
• Efforts to accomplish these tasks should also begin immediately, but these items may be completed within twenty-four hours of presentation for patients with severe sepsis or septic shock.
http://www.ihi.org/IHI/Topics/CriticalCare/Sepsis

Sepsis Management Bundle1. Low-dose steroids administered for septic shock in
accordance with a standardized ICU policy
2. Drotrecogin alfa (activated) administered in accordance with a standardized ICU policy
3. Glucose control maintained > lower limit of normal, but < 150 mg/dl (8.3 mmol/L)
4. Inspiratory plateau pressures maintained < 30 cm H2O for mechanically ventilated patients
http://www.survivingsepsis.orghttp://www.ihi.org/IHI/Topics/CriticalCare/Sepsis

CORTICUS Trial – Charles Sprung MD• Prospective, randomized DB multi-center trial
– 52 European ICUs
• n=500 (3/02-11/05)– Planned 800 to give 80% power to detect 10% reduction in mortality,
difficult to enroll due to high use of steroids prior to enrollment (in ED) due to SCC Guidelines
– 65% surgical patients– 40% abdominal sepsis– 25% pulmonary sepsis
• Inclusion Criteria: SIRS ≥ 2, infection suspicion, shock and organ dysfunction (Severe Sepsis definition)
• Exclusion Criteria: Steroids, Immunosuppression
ESICM September 27, 2006, Barcelona

Sepsis: Defining a Disease Sepsis: Defining a Disease ContinuumContinuum
Bone et al. Bone et al. Chest.Chest. 1992;101:1644; Wheeler and Bernard. 1992;101:1644; Wheeler and Bernard. N N EnglEngl J MedJ Med. 1999;340:207. . 1999;340:207.
SepsisSepsisSIRSSIRSInfection/Infection/TraumaTrauma Severe SepsisSevere Sepsis
Sepsis with ≥1 sign of organ failure
Cardiovascular (refractory hypotension)
RenalRespiratoryHepaticHematologicCNSMetabolic acidosis
ShockShock

CORTICUS Trial – Charles Sprung MD• Outcome Measures:• Primary outcome measure:
– Decreased 28-day mortality in non-responders to ACTH (> 9 mcg/dl rise)
• Secondary outcome measures: – ICU mortality– Hospital mortality– Organ failure
• To evaluate accuracy of ACTH testing
ESICM September 27, 2006, Barcelona

CORTICUS Trial• All patients underwent ACTH Stimulation test
• Mass spec vs. hospital-based assay
• ACTH (250 mcg) stimulation test (by mass spec)– 51% responders– 49% non-responders
• Hydrocortisone vs. Placebo – 50 mg IV q6h x 5d– 50 mg BID x 3d (days 6-8)– 50 mg qD x 3 d (days 9-11)
ESICM September 27, 2006, Barcelona

CORTICUS Trial• No difference in 28-day all-
cause mortality
• ↑ mortality in Non-responders
• Earlier shock resolution in steroid group in total cohort, not in NR
– Reversal of shock 80% vs. 74.6%– Median time to reverse shock (all
patients) 3.1 days vs. 5.7 days, p=0.003)
– Median time to reverse shock (nonresponders) 3.7 vs. 6 days (p=0.005)
– ICU polyneuropathy 1% vs. 2% (NS)
– Hyperglycemia 84% vs. 72% (NS) ESICM September 27, 2006, Barcelona
All-cause 28-day Mortality
Steroids Placebo
Total 33.5% 31.0%
Responders 28.8% 27.7%
Nonresponders 37.6% 35.2%

CORTICUS Trial• Significant reduction in placebo group mortality
compared to Ananne study (63% vs. 31%)
• Different patient population– more abdominal sepsis– more surgical patients– less pneumonia
• Central diagnostic testing for cortisols by Mass Spec, identified most clinical cortisol assays are not accurate
ESICM September 27, 2006, Barcelona

Surviving Sepsis Guidelines - 2007H. Corticosteroids
1. We recommend intravenous hydrocortisone at 200 mg/day for 7 days in four divided doses or by continuous infusion be given only to adult septic shock patients with a SBP < 90 mmHg persisting for at least one hour despite appropriate fluid resuscitation and aggressive vasopressor therapy (vasopressor-unresponsive). (1B)
2. We suggest hydrocortisone not be given to adult septic shock patients if blood pressure is adequate (SBP > 90 mmHg) with appropriate fluid resuscitation and aggressive vasopressor therapy (vasopressor-responsive). (2B)

Surviving Sepsis Guidelines - 2007Rationale:
One French multi-center, randomized, controlled trial (RCT) of patients in vasopressor-unresponsive septic shock (hypotension despite fluid resuscitation and vasopressors) showed a significant shock reversal and reduction of mortality rate in patients with relative adrenal insufficiency (defined as post-adrenocorticotropichormone [ACTH] cortisol increase 9 ug/dL or less) (66).
Two additional smaller RCTs also showed significant effects on shock reversal with steroid therapy(67,68). However, a large, more recent European multicenter trial (CORTICUS), which has been presented in abstract form but not yet published under peer review, failed to show a mortality benefit with steroid therapy (69). CORTICUS did show a faster resolution of septic shock in patients who received steroids. The use of the ACTH test (responders and non-responders) did not discriminate this effect. Importantly, unlike the French trial which only enrolled patients with vasopressor-unresponsive shock, the CORTICUS study included patients with septic shock, regardless of how the BP responded to vasopressors.

Surviving Sepsis Guidelines - 20073. We suggest the ACTH stimulation test is not used to identify the subset
of adults with septic shock who should receive hydrocortisone. (2B)Rationale. Although one study suggested those who did not respond to
ACTH with a brisk surge in cortisol (<9 µg/dL increase in cortisol 30-60 mins post-ACTH administration) were more likely to benefit from steroids than those who did respond (intact adrenal axis defined as a >9 µg/dLincrease in cortisol 30-60 mins post-ACTH administration), the overall trial population appeared to benefit regardless of ACTH result, and the observation of a potential interaction between steroid use and ACTH test was not statistically significant. Furthermore, there was no evidence of this distinction between responders and non-responders in a recent multicenter trial (69). Additionally, comparisons of different immunoassays for measurement of cortisol show a high variation in serum from septic shock patients but not in healthy controls. When compared to an FDA-approved immunoassay (Electrochemoluminescence Immunoassay of Roche Diagnostics[SBB1] ), cortisol immunoassays may over- or underestimate the actual cortisol level, affecting the assignment of patients to responders or non-responders.

Surviving Sepsis Guidelines - 20074. We suggest that patients with septic shock should not
receive dexamethasone. (2B)
Rationale. Although often proposed for use until an ACTH stimulation test can be administered, we no longer suggest an ACTH test in this clinical situation (see #3 above). Furthermore, dexamethasone can lead to immediate and prolonged suppression of the HPA axis after administration.

Surviving Sepsis Guidelines - 2007
5. We suggest the addition of fludrocortisone 50 µg PO qdif hydrocortisone is not available and the steroid that is substituted has no significant mineralocorticoid activity. Fludrocortisone is considered optional if hydrocortisone is used. (2C)
Rationale. One study added 50 μg of fludrocortisone orally (66). Since hydrocortisone has intrinsic mineralcorticoidactivity, there is controversy as to whether fludrocortisoneshould be added.

Surviving Sepsis Guidelines - 2007
6. We suggest clinicians wean steroid therapy once the septic shock has resolved. (2D)
Rationale. There has been no comparative study between a fixed duration and clinically guided regimen. Two RCTsused a fixed duration protocol for treatment (66,68), and in one RCT, therapy was decreased after shock resolution and discontinued after 6 days (67). One study showed hemodynamic and immunologic rebound effects after abrupt cessation of corticosteroids (70).

Surviving Sepsis Guidelines - 20077. We recommend doses of corticosteroids comparable to >300 mg
hydrocortisone daily are not to be used in severe sepsis or septic shock for the purpose of treating septic shock. (1A)
Rationale. Two randomized prospective clinical trials and two meta-analyses concluded that for therapy of severe sepsis or septic shock, high-dose corticosteroid therapy is ineffective or harmful (71-74). There may be reasons to maintain higher doses of corticosteroid for medical conditions other than septic shock.
7A. We suggest clinicians wean steroid therapy once the septic shock has resolved.
Grade 2D
Rationale. There has been no comparative study between a fixed duration and clinically guided regimen, or between tapering and abrupt cessation of steroids. Three RCTs used a fixed duration protocol for treatment (66,68,69), and in two RCTs, therapy was decreased after shock resolution (67,75). In four RCTs steroids were tapered over several days (67-69, 75), and in two RCTs (66, 76) steroids were withdrawn abruptly. One cross-over study showed hemodynamic and immunologic rebound effects after abrupt cessation of corticosteroids (70). It remains uncertain whether tapering (69) or no tapering (66) of steroids affected outcome.

Surviving Sepsis Guidelines - 2007
8. We recommend corticosteroids are not to be administered for the treatment of sepsis in the absence of shock. There is, however, no contraindication to continuing maintenance steroid therapy or to using stress does steroids if the patient’s history of corticosteroid administration or the patient’s endocrine history warrants. (1D)
Rationale. There are no studies documenting that stress doses of steroids improve the outcome of sepsis in the absence of shock unless the patient requires stress dose replacement due to a prior history of steroid therapy or adrenal dysfunction.