Embed Size (px)
Citation preview

Michael Saper, DO, ATC, CSCSAssistant Professor, Orthopedics and Sports Medicine
Knee Osteochondritis Dissecans (OCD) in
the Pediatric and Adolescent Patient
Wall OCD Knee NonOperative 2015
Pediatric Sports Medicine Operative Challenges and Solutions: A Case Based Approach
AAOS 2015 Annual Meeting
Eric J Wall, MD, Cincinnati Children’s
Objectives
! Discuss the indications/contraindications for the non-operative treatment of knee
OCD
! Discuss the clinical and radiographic predictors of success for non-operative
treatment of knee OCD
! Describe the non-operative treatment methods of OCD of the knee
Should I Even Try Non-operative Treatment of Knee OCD?
! Success rates of non-operative treatment for OCD range from 50%-100%
! Will patients tolerate non-operative treatment?
! Should I go straight to surgery?
What Predicts Non-Operative Success?
! Patient Age: Open growth plates
! Lesion Size: Smaller is better
! Lesion Stability on MRI: Only stable lesions amenable for non-op treatment
! Blood Flow: Inconsistent data on vascular vs avascular
! Lesion Location (MFC, LFC, Patella, Trochlear Groove)
! Radiographic Sclerosis: More sclerosis is worse. (Ramirez A 2010)
! More bone in OCD Lesion: Perhaps
! Absence of Mechanical Symptoms: Perhaps
! Cyst Like Lesions: If < 1.3 mm in total length on MRI (Krause M 2013)
Stable MRI Unstable MRI
Predictive Model: Nomogram (Wall EJ 2008)
! Helps to individualize the specific success rate of non-operative treatment for each
patient
! Let’s parents choose non-operative vs operative treatment based on success rate
! How it works

Anatomy
• Cartilage covers the joint surface
at end of a bone.
• When healthy, allows:
• Range of motion
• Shock absorption
• Poor healing ability

What is OCD?
12/19/2017
7
Boundary
Boundary distinct
higher or lower density line separating parent from progeny
TJG
Juvenile OCD - Uniform Nomenclature – Credit ROCK group
Parent Bone
Progeny Bone
Fragmentation Fragmented >/= 2 pieces of bone
• Injury to the bone below the
cartilage
• Due to loss of blood supply from
repetitive trauma
• Risk for instability and disruption of
overlying cartilage
• May result in early arthritis
• Both knees in 25%
Can be a 3-4 procedure
problem

Treatment depends on….
• Stability of OCD lesion
• Fragment salvageable?
• Location
• Size
• Amount of bone
involvement

Cue Ball, Shadow
12/19/2017
12
TJG
Articular Surface Intact
-Not Marginated
-Wide open growth plates
Juvenile OCD
A
Articular Surface Intact
Marginated
B
Not Intact
C
TJG
Arthroscopic Evaluation
ROCK
Stable, Salvageable ProgenyCue Ball
Shadow
Immobile
TJG
Arthroscopic Evaluation
ROCK
Stable, Salvageable Progeny Locked Door mobile

Osteochondritis Dissecans – Locked Door
12/19/2017
12
TJG
Articular Surface Intact
-Not Marginated
-Wide open growth plates
Juvenile OCD
A
Articular Surface Intact
Marginated
B
Not Intact
C
TJG
Arthroscopic Evaluation
ROCK
Stable, Salvageable ProgenyCue Ball
Shadow
Immobile
TJG
Arthroscopic Evaluation
ROCK
Stable, Salvageable Progeny Locked Door mobile

Trap Door
12/19/2017
13
TJG
Unstable, Salvageable progeny:Trap Door
Crater with congruent flap
Crater with incongruent loose flap
That can be made congruent
Juvenile OCD
ROCK
mobile
TJG
Unstable, Unsalvageable progenyCrater with incongruent loose body that can not be made congruent
Crater with fagmented loose body
Crater without loose body
Juvenile OCD
ROCK
TJG
• Phase 1 (4-6 weeks)
– Immobilization – WBAT
• Phase 2 (6 weeks)
– No immobilization – ADL’s – PT
• Phase 3 (Lesion healed - absence of symptoms)
– Gradual/Supervised return to sport
OCD of the Knee
AlgorithmNonoperative Protocol
2010 AAOS Presentation – Unloader > Casting or Restriction
Kocher/Ganley/Micheli et al

Crater
12/19/2017
13
TJG
Unstable, Salvageable progeny:Trap Door
Crater with congruent flap
Crater with incongruent loose flap
That can be made congruent
Juvenile OCD
ROCK
mobile
TJG
Unstable, Unsalvageable progenyCrater with incongruent loose body that can not be made congruent
Crater with fagmented loose body
Crater without loose body
Juvenile OCD
ROCK
TJG
• Phase 1 (4-6 weeks)
– Immobilization – WBAT
• Phase 2 (6 weeks)
– No immobilization – ADL’s – PT
• Phase 3 (Lesion healed - absence of symptoms)
– Gradual/Supervised return to sport
OCD of the Knee
AlgorithmNonoperative Protocol
2010 AAOS Presentation – Unloader > Casting or Restriction
Kocher/Ganley/Micheli et al

Operative Treatment Options – Stable/Immobile Lesions
• Subchondral Bone Drilling
• ~1mm wire
• Drill into bone to stimulate healing
• ~85-90% healing at 4.5-5.5 months
12/18/2017
3
Isolated Drilling without additional procedures
• Isolated drilling for stable Lesions in those with significant growth remaining
• If closer to maturity, consider drilling + fixation, possible bone grafting
• For more advanced lesions, drilling in isolation is not enough
Stable/Immobile Lesions
Subchondral bone drilling options
Trans-articular drilling Retro-articular drilling
Drilling
• Trans-articular
– Visualize lesion / holes directly
– Ensures adequate coverage
• Retro-articular
– Doesn’t violate articular cartilage
– Fluoroscopy
• ROCK – RCT ongoing!
– Ben Heyworth CHB
– Trans vs retro MFC OCD lesions
12/18/2017
5
Subchondral Bone Drilling For OCD – Hyaline
Cartilage surface is normal
The C-arm is used to identify the OCD lesion. A guide pin is placed in the most inferior region of the lesion, to be used as a marking point for additional drilling
Medial Femoral Condyle
File name – Picture - Start of subchondral bone drilling video -
This 0.045 K-wire defines the Medial and posterior edge of the OCD lesion.This is placed with Guidance from the mini C-arm.
PCL Origin and Fibers
Medial Femoral Condyle
Notch Drilling Technique for OCD
File name – Picture - Notch Drilling Technique for OCD
Video - OCD Notch drilling
Video - OCD Notch drilling with Marker Pin

Operative Treatment Options – Unstable Lesions
• Fixation (open or arthroscopic)
• Salvageable cartilage
• Metal vs Bioabsorbable
• Biologic
• + Drilling
• Salvage
• Chondroplasty/Microfracture (drilling)/abrasion arthroplasty
• OATS
• OCA
• ACI
• + Bone grafting

Salvageable Unstable Lesions - Fixation
• No difference in outcomes
• Bioabsorbable implants (chondral dart, smart nail, biocompression
screw)
• No need to remove
• ? Cyst formation (with older technology)
• Metal screws
• May need removal 6-8 weeks (time varies depending on screw choice)
12/11/2017
4
Dallas, Texas
Treatment-Operative
15 year-old female
Dallas, Texas
Treatment-Operative
15 year-old female
Dallas, Texas
Treatment-Operative [salvage]
Microfracture
• Technically easy.
• Inexpensive.
• Gudas [2009]
– Microfracture vs. OATS
– Prospective, randomized.
– 41% failure in microfx at 4.2
yrs.
– 0% failure for OATS.

Arthroscopic Fixation with BioCompression Screws
(Preferred Technique)

Unsalvageable Lesions - Marrow Stimulation
• Small lesions (< 1-2 cm)
• Contained (cartilage walls all
around)
• Minimal bone loss
• Drill holes in the bone
• Forms a cartilage plug

Marrow Stimulation Plus Biocartilage
• Allograft cartilage
• Add PRP
• Scaffold
• Improves fill of defect
• Increased Type II collagen
• No outcome data
Introduction
Articular cartilage, also called hyaline cartilage,
is the tissue component that covers the joint
surface at the end of a bone. A joint typically
consists of two bones connected together with
the articular cartilage of each bone opposing
the other. When healthy, the cartilage allows our
joints to go through painless range-of-motion and
helps to provide shock absorption when weight-
bearing. When cartilage is damaged, this may
cause patient discomfort along with joint swelling,
which leads to decreased range-of-motion and
stiffness.
How is injured cartilage treated?
The physician will evaluate your symptoms and
perform a physical examination of the joint that
is causing you discomfort. The physician may
also elect to obtain an imaging study to further
evaluate your injury. Depending on the findings,
your physician may determine a surgical procedure
is warranted. When a cartilage lesion is identified,
your surgeon may recommend a microfracture
procedure, also known as bone marrow stimulation
technique. This procedure consists of debriding
the damaged cartilage until a border of healthy
cartilage is found. Small holes are then made in
the base of the defect providing access channels
for the underlying bone marrow cells to enter
and begin laying down reparative tissue.
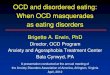
What is BioCartilage®?
BioCartilage is developed from allograft articular
cartilage. After going through a number of pro-
prietary processing steps, the result is a cartilage
extracellular matrix scaffold. BioCartilage contains
the extracellular matrix that is native to articular
cartilage, which includes scaffolding proteins and
additional cartilaginous growth factors. The small
particles are mixed with a blood solution that
comes from your own body in order to create
a paste-like consistency that can be applied over
a cartilage defect.
How does BioCartilage work?
BioCartilage functions as a tissue scaffold that
your body’s cells can attach to and produce
new reparative cartilage tissue in the defect site.
Your surgeon will clean the defect area, clearing
out damaged tissue and use this scaffold in
conjunction with microfracture as a way of
providing attachment sites for the bone marrow
cells. These cells will penetrate through the access
channels to aid in the healing process.
Microfracture procedure
BioCartilage Procedure in the Ankle
BioCartilage applied over defect
BioCartilage smoothed over defect
Completion of BioCartilage procedure
Microfracture procedure
BioCartilage Procedure in the Knee
BioCartilage applied over defect
BioCartilage smoothed over defect
Completion of BioCartilage procedure

Unsalvageable Lesions – Osteochondral Allograft
• Osteochondral Allograft
• Replaces bone and cartilage
• 88% good-excellent results at 10
years in adolescents
• Staged procedure ?
12/11/2017
6
Dallas, Texas
Treatment-Operative
Fresh Osteochondral Allograft• Replaces bone and
cartilage.
• Emmerson [2007]– 72% good-excellent at 7.7
yrs.
– Mean size 7.5 cm2.
– All had prior surgery.
• Murphy, Pennock, Bugbee[2014]– 88% good-excellent at 10
years in adolescents.
Dallas, Texas
Treatment-Operative
Fresh Osteochondral Allograft• Replaces bone and
cartilage.
• Emmerson [2007]– 72% good-excellent at 7.7
yrs.
– Mean size 7.5 cm2.
– All had prior surgery.
• Murphy, Pennock, Bugbee[2014]– 88% good-excellent at 10
years in adolescents.
Dallas, Texas
Summary
• Always assess alignment.
• Microfracture/Marrow Stimulation/Debridement does not
produce durable long-term results.
• Fixation with bone grafting is an option if cartilage is in good
condition and patient has growth remaining.
• Osteochondral allograft and ACI/MACI are good options for
large unsalvagable lesions.
12/11/2017
6
Dallas, Texas
Treatment-Operative
Fresh Osteochondral Allograft• Replaces bone and
cartilage.
• Emmerson [2007]– 72% good-excellent at 7.7
yrs.
– Mean size 7.5 cm2.
– All had prior surgery.
• Murphy, Pennock, Bugbee[2014]– 88% good-excellent at 10
years in adolescents.
Dallas, Texas
Treatment-Operative
Fresh Osteochondral Allograft• Replaces bone and
cartilage.
• Emmerson [2007]– 72% good-excellent at 7.7
yrs.
– Mean size 7.5 cm2.
– All had prior surgery.
• Murphy, Pennock, Bugbee[2014]– 88% good-excellent at 10
years in adolescents.
Dallas, Texas
Summary
• Always assess alignment.
• Microfracture/Marrow Stimulation/Debridement does not
produce durable long-term results.
• Fixation with bone grafting is an option if cartilage is in good
condition and patient has growth remaining.
• Osteochondral allograft and ACI/MACI are good options for
large unsalvagable lesions.

Operative Treatment Options – Unstable Lesions
• Bone grafting
• If significant bone loss or cystic changes at base of lesion
• Cancellous chips, DBM, autogenous local grafting (proximal tibia,
distal femur)

Rehabilitation and Return to Sports
• Weight-bearing depends on procedure
• From NWB to TTWB
• Encourage range-of-motion exercises
• Goal = full ROM by 6 weeks
• Increased loadbearing exercises at 3 months
• Return to sport at 6-9 months depending on sport

Conclusions
• Goals = remove diseased tissue, fill the defect, return to
sports
• Surgery generally results in improved elbow range-of-
motion and outcomes
• Low rate of complications
• Slow, progressive rehabilitation is key
• Return to sports (6-9 months)
Contact:
@DrMichaelSaper