Embed Size (px)
Citation preview
Version: Final Date: 30 10 17
GOVERNING BODY The THIRTY-FOURTH meeting of the Kingston Clinical Commissioning Group Governing Body will be held in public on Tuesday, 7th November 2017 in the Fraser Chapel, at The King’s Centre, Coppard Gardens, Chessington KT9 2EZ starting at 15:00hrs. Dr Naz Jivani Chair 1st November 2017
AGENDA Time Item
Attachment Action
DECLARATION OF INTERESTS: Members will be asked to declare any possible conflicts of interest at the start of the meeting that have not already been declared on the CCG Register. Members will also be asked to declare any awareness of Fraud or Bribery.
15:00 1 2
INTRODUCTIONS AND WELCOME APOLOGIES FOR ABSENCE: Nadeem Nayeem
15:05
3
MINUTES OF THE THIRTY-THIRD MEETING held on 5th September 2017
Att A
For Approval
15:10
4
MATTERS ARISING
5 QUESTION TIME: an opportunity for questions to be asked on items included in the agenda 15.20 15:25 15:30 15:40 15:50 16:00
6 7 8 9 10 11
CHAIR’S REPORT MANAGING DIRECTOR’S REPORT SOUTH WEST LONDON COMMISSIONING PRIORITIES – ANNUAL COMMISSIONING PLAN 2018-19 HEALTHY LONDON PARTNERSHIP KINGSTON & RICHMOND LOCAL TRANSFORMATION BOARD UPDATE RE-PROVISION OF CEDARS COMMUNITY & INPATIENT SERVICE UPDATE
Verbal Att B Att C Att D Att E Att F
For Information For Information For Information For Information For Information
Version: Final Date: 30 10 17
16:10 16:20 16:30 16:40
12 13 14 15 16 17
IVF / FERTILITY UPDATE KINGSTON CO-ORDINATED CARE SWL SUSTAINABILITY AND TRANSFORMATION PARTNERSHIP REFRESH COMMISSIONING
Integrated Governance Report [PM] Finance Report [YR] Council of Members Report [AG]
MINUTES FOR INFORMATION AND UPDATES FROM SUB COMMITTEES
Audit Committee Finance Committee Integrated Governance Committee Health & Well Being Board Primary Care Commissioning Committee
RECENT POLICIES APPROVED
Business travel and expenses policy
Att G Att H Att J Att K Att L Att M Att N Att O Att P Att Q Att R Att S
For Approval For Information For Information For Information For Information For Information
16:50 18 QUESTION TIME: an opportunity for questions to be asked on items not included in the agenda 19
DATE OF NEXT MEETING TO BE HELD IN PUBLIC: Tuesday, 10th Jan 2018 (3pm to 5pm) Venue: Kings Centre, Chessington
17:00 19 CLOSE To now resolve that the meeting is closed and the public be excluded from any Part 2 meeting because publicity would be prejudicial to the public interest by reason of the commercially sensitive or confidential nature of the business to be conducted in the second part of the agenda.
Items for discussion in Part 2:
Primary Care Mental Health Services Effective Commissioning Initiative SWL Commissioning Intentions Your Healthcare CIC contract South West London Performance Report
KINGSTON CCG MISSION & VALUES We want people to live longer, healthier lives Our vision is that the people of Kingston should be supported to look after themselves and those they care for; have access to high quality, joined up physical and mental health and care services when they need them; and we need to deliver better health outcomes within our budget
Version: Final Date: 30 10 17
Corporate Objectives for 2016-18
1. Better Health
We will seek to improve the quality, safety and effectiveness of healthcare services commissioned on behalf of the people of Kingston
We will take action to reduce inequalities in health outcomes in partnership with Public Health and other stakeholders
We will use choice and personal health budgets to give people control We will use local awareness and engagement campaigns to explain local health and social
care services in Kingston We will focus on local clinical priorities in addition to national programmes, including:
Diabetes/ obesity/ smoking/ falls/ anti-microbial resistance
2. Better Care
We will support the delivery of new models of care to secure sustainable health and care services which supports the delivery of the South West London Sustainability and Transformation Plan
We will improve out of hospital services for the local population working with primary care, social care, community & mental health providers and others
We will deliver the urgent/ emergency care and elective hospital care access targets for the people of Kingston
We will continue to develop and expand 7 day services for patients in all care settings We will focus on local clinical priorities in addition to national programmes, including:
Maternity/ Dementia/ Cancer/ Learning Disability/ Mental Health 3. Sustainability
We will implement our Estates and Digital Strategies We will develop and implement our new models of care (including Kingston Co-ordinated
Care) We will aim to deliver our 2016/17 financial plans including the achievement of Quality,
Innovation, Productivity and Prevention (QIPP) targets 4. Leadership
We will lead an innovative organisation, which creates and shapes services to meet the changing needs of the people of Kingston
Service change will be patient centred
We will ensure that there are effective arrangements for the oversight of the quality, effectiveness and safety of commissioned services
We will engage with the CCG workforce to develop their skills, reward excellence and make Kingston CCG an employer of choice
We will govern with transparency, comply with best practice and meet our statutory obligations
We will work in partnership with the Royal Borough of Kingston to develop the Kingston Commissioning Services and work towards integrating commissioning of services with the local authority
We will explore opportunities with neighbouring CCGs for collaboration in commissioning whilst delivering the Sustainability and Transformation Plans
Version: Draft A - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Minutes of the 33rd Meeting held on 5th September 2017
Agenda Item 3 Attachment
A Purpose (please indicate with X)
Approval/ Ratification
x Discussion / Comment
Information
Report Author: (name & job title)
Jo Dandridge, Governance & Business Lead
Presented by: (name & job title)
Dr Naz Jivani Chair, Governing Body
MINUTES OF THE THIRTY-THIRD MEETING OF THE GOVERNING BODY OF
KINGSTON CLINICAL COMMISSIONING GROUP HELD ON TUESDAY 5th SEPTEMBER 2017
KING’S CENTRE, CHESSINGTON PRESENT: David Knowles Vice Chair & Lay Member Dr Phil Moore Deputy Chair - Clinical Sarah Blow Accountable Officer, SWL Alliance James Murray Interim Chief Finance Officer, SWL Alliance Jim Smyllie Lay Member PPE Paul Gallagher Lay Member & Audit Chair Tonia Michaelides Managing Director, Kingston & Richmond CCGs Dr Gareth Hull GP Member Dr Naeem Iqbal GP Member Dr Pete Smith GP Member Nadeem Nayeem Secondary Care Specialist Kathryn Yates Nurse Member
MEMBERS IN Liz Meerabeau Kingston Healthwatch representative ATTENDANCE: Dr Atin Goel Council of Members Chair Yarlini Roberts Local Director of Finance, Kingston & Richmond CCGs Vicki Harvey-Piper Local Director Corporate Affairs & Governance Iona Liddington Public Health Representative Kathryn MacDermott Local Director of Primary Care & Planning, Kingston & Richmond CCGs Fergus Keegan Local Director of Quality, Kingston & Richmond CCGs
Version: Draft A - 2 Date: 30 10 17
Sue Lear Acting Deputy Director of Commissioning Andrea Knock Designated Nurse Safeguarding Children & Children Looked After (CLA) Jo Dandridge Governance & Business Lead
APOLOGIES: Dr Naz Jivani CCG Chair Dr Annette Pautz GP Member Julia Gosden Local Director of Commissioning Welcome and Introductions: Members of the public were welcomed to the thirty-second meeting of the Governing Body. The Chair also extended a welcome on behalf of the Governing Body to Liz Meerabeau as the new Kingston Healthwatch representative. Declarations of Interest relating to items on the agenda: Members were asked to declare any possible conflicts of interest that had not already been declared on the CCG Register. (All declarations of interest for Governing Body members are listed in the register available at each meeting and also published on our website)
Dr Phil Moore declared he was a partner at Central Surgery which provides the medical cover for the community beds currently located at Cedars Unit on the Tolworth Hospital site. Re-provision of these community beds was being discussed at item 17/56.
17/52 MINUTES OF THE THIRTY-SECOND MEETING HELD 4th JULY 2017
The minutes of the thirty-second meeting held on 4th July 2017 were agreed as an accurate record.
17/53 MATTERS ARISING None 17/54 QUESTION TIME
None.
17/55 MANAGING DIRECTOR’S REPORT This report highlighted items of interest to Governing Body members and the public including issues not contained within the substantive agenda. 55.1 Working within the South West London Alliance
Members noted that a review of governance arrangements for sub committee structures within Kingston and Richmond Local Delivery Unit had been completed in order to develop a streamlined decision making process, enable the benefits of a shared management team and to ensure governance is both efficient and effective across both organisations. Members were advised that Governing Body meetings and Primary Care Commissioning Committee meetings that are both held in public would be aligned and held on the first Tuesday of the month in each respective borough. Members noted that work continues to find a shared working location for the staff of both CCGs and a decision on this was expected soon. Options were being discussed in a Part 2 meeting.
Version: Draft A - 3 Date: 30 10 17
55.2 NHS England’s End of Year Assessment for Kingston CCG Members noted that the CCG had been rated as ‘good’ for 2016/17 in NHS England’s end of year Improvement and Assessment Framework (IAF). The rating was based on a set of three priority areas: cancer, mental health and dementia. The good rating was a positive result and reflected the position around the dementia key indicator target which it was hoped to improve upon going forward.
55.3 Healthy Workplace Charter Members noted that the CCG had been awarded ‘achievement’ level on the Healthy Workplace Charter. The award is based on a set of healthy workplace standards that organisations aspire to meet and if they do, they receive recognition for investing in the health and well being of their staff. Members were advised that the focus would now be on working towards the ‘excellence’ accreditation level to assure the CCG that it is doing everything possible to protect staff and support their health and well being.
55.4 Engagement Programme – Quality in Primary Care Members were advised that Kingston and Richmond CCGs were preparing to
launch a joint programme of engagement about the quality of general practice and community pharmacy services. The aim of the work is to develop a set of quality pledges for primary care. Over a period of four months, people of Kingston and Richmond will be asked what matters most to them when visiting their GP or local pharmacy. Views will also be sought from clinicians and staff working in local GP practices and pharmacies.
55.5 Kingston CCG’s Annual General Meeting
Members were informed of the CCG’s Annual General Meeting taking place on Tuesday, 12th September 2017 from 12.45pm to 2.45pm at the King’s Centre, Coppard Gardens, Chessington. The Governing Body NOTED the Managing Director’s Report.
17/56 RE-PROVISION OF KINGSTON COMMUNITY HOSPITAL BEDS Members received an update from Sue Lear, Acting Deputy Director of
Commissioning on the latest position with regard to re-provision of the community hospital beds currently located at the Cedars Unit on the Tolworth Hospital site.
At the July 2017 Governing Body meeting, the options for a short term solution to
move the 35 beds on the Tolworth Hospital site to a 25 bedded unit at Teddington Memorial Hospital and an enhanced home care based solution for the remaining 10 beds was supported.
Members noted that the move to Teddington Memorial is an interim short term
solution and the date of the move is yet to be confirmed between South West London & St George’s Mental Health NHS Trust and Your Healthcare Community Interest Company (CIC).
Members noted that Kingston CCG were committed to finding a permanent site for
the in-patient beds within the Kingston borough and discussions were underway with Your Healthcare CIC to develop a full options appraisal and enquiries were being
Version: Draft A - 4 Date: 30 10 17
made to NHS Property Services regarding the potential use of the ex Primary Care Support Services building on the Ewell Road in Surbiton.
Members were also advised that following the changes in Healthwatch Kingston,
which involved a significant increase in the number of Trustees on the Board, it was considered beneficial going forward for them to include the joint engagement plan within their work programme.
Discussion followed on the results of the recent bed audit that had been undertaken which determined that the optimum number of beds required was less than that being proposed. In response to a query as to whether audit would be carried out over the winter months, members noted that demand and capacity modelling had been done and with the pressures experienced within the system, resulted in demand for 15 more beds than there were currently within the system.
The Governing Body NOTED the contents of the report and would receive regular updates at future meetings.
17/57 CHOOSING WISELY
Members received a report on the feedback and recommendations from the engagement programme about proposed changes to prescribing, IVF and specialised fertility services. The governing body were being asked to consider the final report of the engagement exercise on Choosing Wisely which took place between 15th March 2017 to 14th July 2017. Members noted the pause that had taken place between 20th April 2017 and 8th June 2017 due to the General Election. The four areas of prescribing that had been the subject of the public engagement and under consideration by members were as follows:
Over the counter self care medication; Gluten Free foods; Vitamin D; and Baby milk
Members were advised that the changes being proposed for self care medication were for those conditions which would naturally get better by itself ie. coughs, colds, sprains and would therefore not apply to anti-inflammatory medication. Discussion followed on how constructive the public engagement had been and of the huge implications for the local pharmacists. It was agreed that a communications and engagement programme be developed to fully brief the pharmacists and the public Members were advised that those who had responded during the engagement exercise were, in the main supportive of the proposed changes to prescribing in Kingston. However, the strength of support varied on individual proposals and specific concerns were expressed across each of the prescribing-related proposals. The major concerns centred on patients and the public having insufficient information or knowledge about what actions they needed to take, the readiness of primary care to support these changes and concerns about vulnerable people
Version: Draft A - 5 Date: 30 10 17
Following lengthy consideration and debate, a decision was taken by Governing Body members, that the CCG will no longer support the routine NHS prescribing of the following products:
Prescriptions for gluten free food Prescriptions for vitamin D maintenance Prescriptions for medicines which are available over the counter
However, it was stressed by members that all decisions relating to prescribing still rests with the GP, who may decide, in specific cases, that it is not appropriate to follow the CCG guidelines.
Prescriptions for baby milk As part of the Choosing Wisely engagement, the option of reducing prescriptions for baby milks and specialist infant formula had also been considered. However, during the engagement exercise feedback was received from a number of sources about the complex nature of milk allergy. Members therefore agreed that the CCG will focus on developing improved guidelines and education for GPs and other healthcare professionals to advise when prescribing for baby milk is suitable or not. These resources will be developed with dieticians, other healthcare professionals and stakeholders including Allergy UK and will be supported with patient information.
IVF and specialised fertility services Members were reminded that no decisions had yet been taken regarding in vitro fertilisation (IVF) and intra-cytoplasmic sperm injection (ICSI) services following the views sought as part of the Choosing Wisely for Kingston engagement programme. Members noted that as a result of the feedback and further advice from the Assisted Conception Unit, an additional consideration had been identified, namely to review current eligibility criteria and review access to the fertility pathway. Members were also advised that Richmond CCG had already undertaken a full consultation process on the fertility pathway and found that the pathway could be revised to restrict access for those people where evidence would suggest there would be no benefit from fertility treatment based on the expected clinical outcomes. The governing body agreed that learning should be taken from the Richmond CCG consultation results and therefore agreed to support in principal, the option of retaining the current eligibility criteria and to review the fertility pathway. Further work on the revised fertility pathway would be taken forward during September and October and a report would be brought back to the next Governing Body meeting in November 2017.
17/58 SAFEGUARDING CHILDREN ANNUAL REPORT
Andrea Knock presented the 2016-17 Safeguarding Children Annual Report and the proposed work plan for 2017-18. The purpose of the report was to provide assurance that the safeguarding children’s arrangements are robust and that the organisation is meeting its statutory obligations. Members were advised that there were 142 children subject to a child protection plan. This number had reduced over the last year and is comparable to Kingston’s statistical neighbour but lower than the London and England national levels.
Version: Draft A - 6 Date: 30 10 17
Members discussed the challenges faced by GPs to attend case conferences as many are held within surgery time and securing cover is difficult. Also submission of reports by GPs had continued to be problematic. It was agreed to add this to the work plan as a key priority to take forward and to also explore the technology required to allow virtual attendance by GPs. A question was raised regarding Ellingham School which had lost circa £24k from their budget due to children requiring additional support not transferring with the appropriate paperwork. It was noted that although the assessment was not health related, this matter would be highlighted to social care colleagues.
A question was asked if it was thought there was a problem with grooming locally and in response it was noted that this was a national problem and there were separate Local Safeguarding Children Board sub groups which involved multiple agencies including the policy that looked at issues of child sexual exploitation and early intervention to divert any areas of concern. A question was raised regarding the ratio of foster parents to foster children in the borough and whether the local authority were doing any work to address the imbalance. In response, it was noted that there were 30 new families that had recently registered to be trained as foster parents and the CCG agreed to help to advertise the work of the local authority in recruiting foster parents. The Governing Body RECEIVED the 2016-17 Safeguarding Children Annual Report and proposed work plan for 2017-18 and expressed their thanks to Andrea Knock for all her work in this area.
17/59 COMMISSIONING 59.1 Integrated Governance Committee Report A report detailing issues discussed at the most recent Integrated Governance Committee meeting held in July 2017 had been circulated for information.
Members noted that the two main areas of concern continued to be the Dementia Diagnosis rate and A&E waiting times. Members were advised of the one Very High (red) rated risk on the Risk Register as follows:
Failure to deliver the 2016/17 South West London STP Objectives; Failure to plan effectively to implement STP objectives from 2017/18 onwards.
Members discussed the performance against the constitutional standards and
noted the following in particular:
A&E waiting times – Kingston Hospital have not met the standard of 95% on a monthly basis of patients spending less than 4 hours between arrival in the A&E department and admission, transfer for discharge. However, they were meeting the Sustainability and Transformation Fund trajectory to August 2017 of 89.6% with year to date performance to August 2017 of 90.79%.
Version: Draft A - 7 Date: 30 10 17
Members also noted that the Kingston, Richmond and Surrey A&E Delivery Board had refreshed its programme of work under the heading of the 8 pillars for improvement in Urgent & Emergency Care. Progress had been made in the last two months with the implementation of a Project Management Office to support the named leads for the 8 pillars.
Members were advised that Kingston has consistently shown better performance against the Red 2 and Category A targets and a forum across Kingston & Richmond had been introduced that would be responsible for developing a plan to reduce frequent callers to the London Ambulance Service. Members noted the variation year to date of non-elective admissions that had increased to 10.3% (from 9.2% from previous month). The two main underlying reasons were the delay to setting up the Kingston Co-ordinated Care locality team as part of the QIPP programme; and the increased level of admissions as a result of the new Clinical Decision Unit at Kingston hospital. The Governing Body NOTED the Performance Report.
59.2 Finance Report – Month 4
Members received the finance report for Month 4 (July 2017) and noted the following:
the CCG is on target to achieve its business rules for 2017/18 the CCG is forecast to meet its planned 0.5% in-year surplus of
£1,151k the acute position had worsened and reserves have been fully utilised
used to enable delivery of the surplus BPPC and cash targets were achieved in Month 4 QIPP savings are forecast to under achieve against plan, due to delays
in starting some of the QIPP schemes Acute Commissioning Members noted Kingston Hospital’s reported forecast position had worsened by £1.8m. Large variances had been reported in the areas of A&E, emergency, outpatient 1st and outpatient procedures. The overspend in outpatients largely related to ophthalmology. Non Acute Commissioning Members were advised that Better Care Fund draft plans had been drawn up following release of guidance and work was underway to produce a local plan for submission in September 2017. Members noted that CCG capital was received in Month 4 and IT will be purchased in line with the SWL IT strategy. QIPP Performance Members were advised that the medicines management scheme was currently in phase 1 of consultation and 17 medicines/category of medicines have been developed and approved. Another 6 are ready for approval and a
Version: Draft A - 8 Date: 30 10 17
further 4 in developed. The forecast outturn had been based on feedback from the prescribing team recognising the mid year effect and was therefore a pessimistic view.
59.3 Council of Members Report
Members received a report detailing items discussed at the most recent Council of Members meeting held on 11th July 2017. At the meeting, Elizabeth Brandill-Pepper attended to provide members with an update on Neuro Development services available across the borough; members received an update on the governance review undertaken to streamline the decision making process across Kingston and Richmond CCGs; and a primary care update was provided which included progress on the roll out of Kinesis and DXS. Mr Hooman Sherafat, Clinical Director of Ophthalmology at Kingston Hospital also provided members with an overview of referral patterns to ophthalmology together with feedback on ophthalmology A&E attendances. The Governing Body NOTED the Council of Members Report.
17/60 MINUTES FOR INFORMATION AND UPDATES FROM SUB COMMITTEES 60.1 Audit Committee Minutes of the Audit Committee meetings held on 24th April 2017 and 22nd May 2017 were received for information. 60.2 Finance Committee
Minutes of the Finance Committee meeting held on 26th June 2017 were received for information.
60.3 Integrated Governance Committee Minutes of the Integrated Governance Committee meeting held on 13th June 2017 were received for information.
60.4 Health & Well Being Board
Minutes of the Health & Well Being Board meeting held on 15th June 2017 were received for information.
60.5 Primary Care Commissioning Committee
Minutes of the Primary Care Commissioning Committee meeting held on 2nd May 2017 were received for information.
17/61 QUESTION TIME
An expression of thanks was given to the CCG for its funding of patients with diabetes and members were advised that the Diabetes Support Group had grown in strength and numbers and meetings were held on a monthly basis. The next meeting would take place on 19th September 2017 in the Education Centre at Kingston Hospital.
A plea was also made for GPs to refer patients in to the ‘Diabetes and your diet’, weekly exercise programme being held at Kingfisher Leisure Centre. The positive effects of the programme were seeing a reduction in patients needing medication.

Version: Draft A - 9 Date: 30 10 17
17/62 DATE OF NEXT MEETING TO BE HELD IN PUBLIC Tuesday 7th November 2017 Venue: King’s Centre, Chessington
Version: Final B - 1 Date: 31 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Managing Director’s Report
Agenda Item 7 Attachment
B
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Tonia Michaelides Managing Director, Kingston & Richmond CCGs
Presented by: (name & job title)
Tonia Michaelides, Managing Director, Kingston & Richmond CCGs
MANAGING DIRECTOR’S REPORT The following report highlights items of interest to Governing Body members and the public which are not discussed in detail in the rest of the agenda.
1. Effective Commissioning Initiative (ECI)
The six clinical commissioning groups (CCGs) in south west London (Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth) have agreed to establish a 'Committees in Common' to make decisions as a group of CCGs. In April 2017, the Committees in Common agreed that south west London CCGs would work together to develop a common version of the SWL Effective Commissioning Initiative (ECI) policy, ensuring alignment of existing clinical thresholds and common processes to monitor compliance with the policy. The original ECI policy had been in place since 2014 and is driven by the need to ensure that NHS funded treatments are evidenced-based, clinically effective and that access to a treatment in the south west London area is equal for patients with similar clinical need. All south west London CCG governing bodies approved the process for this common version to take place at their May 2017 governing body meetings. There was clinical and managerial representation to ensure CCG ownership of the revised clinical thresholds and compliance monitoring process. This work has progressed well and a final draft document will be discussed at the next Committees in Common, at 5-7pm on Thursday 16 November (at 120 The Broadway).
Version: Final B - 2 Date: 31 10 17
Once approved, the policy will go live across south west London from 2 January 2018. A coordinated programme of engagement with providers will take place leading up to this date.
2. Engagement programme – quality in primary care Work continues on Kingston and Richmond’s joint programme of engagement about the quality of general practice and community pharmacy. The aim of the work is to develop a set of quality pledges for primary care and patient responsibilities. The project will help the CCGs to understand what is important to patients, the public and primary care clinicians and staff and inform how we continue to implement our strategy to transform primary care. Our approach to engagement is where possible to build on existing local engagement arrangements and we will incorporate insight already gathered through, for example, the national GP survey, NHS South West London grassroots engagement activities, Health & Wellbeing Board listening events and Healthwatch feedback. To inform the project we are placing comments cards and boxes in GP practices, pharmacies and in some provider organisations. We are grateful for the support we have received from partners including the Councils, Healthwatch and other voluntary organisations to promote the project including our online survey. So far we have received 250 online survey response/cards; 67% from Richmond, 32% from Kingston and 1% living out of borough but have GP in either Kingston or Richmond. We are attending events and reaching out to local groups to ensure we are having conversations with different local communities and groups which include working with Achieving for Children to gather the views of children and young people, attending a carers’ discussion group, a BME older people’s group and a refugee action group and attending a health day for homeless people, Richmond’s Full of Life Fair and the Surbiton Festival. During November we will conduct a mid-project review to ensure our communication and engagement activities are effective and we will continue to identify events and forums for us to undertake patient and public involvement until January 2018. We plan to introduce the new primary care pledges in April 2018.
3. National Diabetes Audit 2016/17
For the second year running, Kingston CCG has achieved a 100% participation rate in the National Diabetes Audit.
This national audit measures the effectiveness of diabetes healthcare against NICE clinical guidelines and NICE quality standards, in England and Wales. The NDA collects and analyses data for use by a range of stakeholders to drive changes and improvements in the quality of services and health outcomes for people with diabetes.
This is a tremendous achievement and helps provide a sound basis from which we can work together to further improve diabetes care in Kingston. We expect the full findings of the audit to be published by NHS Digital in December.
Version: Final B - 3 Date: 31 10 17
4. Cancer awareness drop in session
Kingston CCG and Kingston Council will run a cancer awareness drop in session for the public on Thursday 16 November between 5pm – 7.30pm. This will take place at the YMCA, 49 Victoria Road, Surbiton.
Health, care, and voluntary sector partners in Kingston have recently produced a new cancer strategy that follows the patient journey. One of the key elements of the strategy is helping to prevent cancer and this event is designed to offer advice on cancer prevention. Those attending will be able to talk to representatives from Cancer Research UK, smoking cessation services, public health in Kingston, St George’s screening team, and voluntary sector partners.
5. Springfield University Hospital and Tolworth Hospital – development partner
announced David Bradley, Chief Executive of South West London and St George’s Mental Health NHS Trust has written to inform us that the trust has now completed the final stage of a 15 month procurement process to build two new state-of-the-art mental health hospitals at Springfield University Hospital and Tolworth Hospital. STEP (Kajima Partnerships and Sir Robert McAlpine Capital Ventures Ltd) has been selected as their preferred development partner and is now working with the trust to progress the estate modernisation programme to contract close. The announcement of preferred bidder marks a significant milestone, and enables the proposals to be finalised for a full business case to be submitted to government for approval - with the signing of contracts currently estimated to be in spring/summer 2018. At the same time, the trust is progressing the submission of detailed planning applications for the two hospital sites, which will form part of the government approvals processes. The estate modernisation programme will transform the way mental health services are delivered in south west London. The plans, once approved, will bring forward a range of benefits to service users and the local community with:
Two new state of the art mental health centres - replacing outdated facilities to provide patients with the best possible care
839 new homes - delivering high quality homes for the community in Tooting A new 32 acre public park - providing excellent outdoor space for the local
community A brand new primary school - investing in local children's future £5 million for local transport services - boosting transport links for local residents
Tonia Michaelides Managing Director of Kingston and Richmond CCGs
Version: Final C - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title South West London Commissioning Priorities – Annual Commissioning Plan
2018/19 Agenda Item 8 Attachment
C
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
x Information
Report Author: (name & job title)
Kath Cawley, Programme Office SWL Alliance
Presented by: (name & job title)
Jonathan Bates, Director of Commissioning Operations SWL Alliance
Summary and purpose of report The attached document outlines the proposed Commissioning Intentions across SWL for 2018/19. It is expected that the commissioning and contracting round for 2018/19 will be a refresh of the two year planning round, and therefore the Commissioning Intentions have been refreshed from those agreed for 2017/18-18/19. The Commissioning Intentions are a summation of local CCG and STP plans. During 2017/18, commissioners and providers have been involved in developing the Delivery Plans for Five Year Forward View for the four major clinical priorities detailed in the Five Year Forward View Next Steps:
- Urgent & Emergency Care; - Cancer; - Mental Health; and - Primary Care.
In addition, further work is underway across SWL to implement consistent models for Planned Care (currently focussing on MSK services and Effective Commissioning Initiative) and developing a Maternity Delivery Plan to respond to the Better Births national maternity recommendations. In addition to refreshing the Commissioning Intentions across all of SWL, this document also details the specific local Commissioning Intentions for each of the four Local Transformation Boards: Croydon, Kingston & Richmond, Merton & Wandsworth and Sutton. The Commissioning Intentions state the expected service changes across SWL in 2018/19 for the following:
Section 2 - Urgent and Emergency Care Section 3 - Primary Care Section 4 - Mental Health Section 5 - Cancer Section 6 - Planned Care Section 7 - Maternity Section 8 - Learning Disabilities Section 9 - Children and Young people Section 10 - Integrated Community Care
Version: Final C - 2 Date: 01 11 17
Section 11 - Further local priorities i. Croydon ii. Kingston & Richmond iii. Merton & Wandsworth iv. Sutton
CCGs in SWL would like to signal clear intent to move to payment mechanisms that better reflect the sharing of system risk and incentive in 2019/20. This will include introducing tariff flexibilities such as capped contracts, risk/gain shares, payment floors and other alternatives to Payment by Results where appropriate. Local systems will be supported to vary contracts in 2018/19 if they can move at pace to this approach. The commissioning intentions paper was sent to providers on the 29th September 2017 in accordance with the national timescale. Key sections for particular note The document is divided into two sections the first section details the SWL commissioning intentions across the joint priority areas; whereas the second section details the local priorities by local delivery units. Kingston and Richmond LDU priorities can be found on pages 17 – 19. Report recommendation Kingston CCG governing body is asked to note the contents of the paper. Financial and / or resource implications The local commissioning intentions detailed in section 11 sets out the financial context in which each system is operating and the level of QIPP savings currently envisaged to be required based on currently planning assumptions. This paper identifies the potential impact by point of delivery of the commissioning intentions but does not quantify these. This detailed work will be progressed over the next few months Key risks identified & mitigation A risk assessment has not yet been carried out, this would be developed specifically for individual areas. Equality and / or privacy impact analysis An equality impact analysis has not yet been carried out, this would be developed specifically for individual areas. Committees that have previously discussed / agreed the report and outcomes This has been discussed at the SWL Alliance Senior Management Team, SWL Directors of Commissioning and SWL Contract Delivery Group and locally to the joint Executive Management Team for Kingston and Richmond. Communication plan / stakeholder involvement / patient engagement This document has been sent to all SWL providers. Each of the individual five year forward view delivery plans (UEC, primary care, cancer, MH and maternity) seeks to improve quality of care and safety. Each sets out clear metrics against which
Version: Final C - 3 Date: 01 11 17
quality and safety performance are being assessed. CCGs should also have arrangements to share and discuss Commissioning Intentions with local stakeholders including patient groups and their representatives, including Healthwatch. Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
South West London
Commissioning Priorities
Annual Commissioning Plan
2018/19
Page 2 of 25
Contents 1. Introduction .......................................................................................................................................... 3
1.1. South west London update................................................................................................................ 3
1.2 SWL Commissioning Intentions 2018/19 ........................................................................................... 3
2. Urgent and Emergency Care (UEC) ....................................................................................................... 4
3. Primary Care ......................................................................................................................................... 5
4. Cancer ................................................................................................................................................... 5
5. Mental Health ....................................................................................................................................... 6
6. Planned Care ............................................................................................................................................. 7
6.1 St George’s NHS Foundation Trust ..................................................................................................... 7
6.2 Effective Commissioning Initiative (ECI) ............................................................................................. 8
6.3 Musculoskeletal Services (MSK) ......................................................................................................... 8
6.4 Ear, nose and throat (ENT) ................................................................................................................. 8
6.5 Advice and Guidance .......................................................................................................................... 8
7. Maternity .............................................................................................................................................. 9
8. Learning Disabilities ............................................................................................................................ 10
9. Children and young people ................................................................................................................ 10
10. Integrated community care ............................................................................................................ 11
11. Further local priorities .................................................................................................................... 13
11.1 Croydon .......................................................................................................................................... 13
11.2 Kingston & Richmond ..................................................................................................................... 17
11.3 Merton and Wandsworth ........................................................................................................... 20
11.4 Sutton ............................................................................................................................................. 23
Page 3 of 25
South West London Commissioning Priorities 2018/19
1. Introduction
1.1. South west London update
Commissioners and providers across South West London have come together in the South West London
Sustainability and Transformation Partnership. Our joint priorities for improving healthcare in South West
London shapes all that we do.
Our joint aim for South West London is set out below:
The Partnership has set the following strategic objectives:
Supporting people to stay well
Proactive, personalised care for people with long term conditions
Delivering the right care in the best place
Getting end of life care right
Transforming access to outpatient services
Getting the model of care right
The priorities set out in this Commissioning Plan support delivery of our Partnership’s aims and
objectives.
1.2 SWL Commissioning Intentions 2018/19
This document outlines the agreed Commissioning Intentions across SWL for 2018/19. Expectations for
the commissioning and contracting round for 2018/19 will be a refresh of the two year planning round,
and therefore the commissioning intentions have been refreshed from those agreed for 2017/18-18/19.
During 2017/18, commissioners and providers have been involved in developing the Delivery Plans for
Five Year Forward View for the four major clinical priorities detailed in the Five Year Forward View Next
Steps, including Urgent & Emergency Care, Cancer, Mental Health and Primary Care. In addition, further
work is underway across SWL to implement consistent models for Planned Care (currently focussing on
MSK services and Effective Commissioning Initiative); developing a Maternity Delivery Plan and
responding to the Better Births national maternity recommendations.
People need beater support to live healthy, active and independent lives for as long as
possible. This includes advice and support to help them stop getting ill and to help
them manage their condition themselves. Where people do get ill, we need to ensure
they are diagnosed and supported at an early stage.
Mental physical health issues go hand in hand. Mental health intervention can result
in better wellbeing and outcomes for patients with certain conditions. Patients with
long term conditions, like diabetes, medically unexplained symptoms and chronic pain
need better care and support, that takes into account their mental as well as physical
health needs.
Page 4 of 25
In addition to refreshing the Commissioning Intentions across all of SWL, this document also details the specific local Commissioning Intentions for each of the four Local Transformation Boards: Croydon, Kingston & Richmond, Merton & Wandsworth and Sutton. The Commissioning Intentions state the expected service changes across SWL in 2018/19 for the following:
Urgent and Emergency Care
Primary Care
Mental Health
Cancer
Planned Care
Maternity
Learning Disabilities
Integrated Community Care
Further local priorities o Croydon o Kingston & Richmond o Merton & Wandsworth o Sutton
CCGs in SWL would like to signal clear intent to move to payment mechanisms that better reflect the
sharing of system risk and incentive in 2019/20. This will include introducing tariff flexibilities such as
capped contracts, risk/gain shares, payment floors and other alternatives to Payment by Results where
appropriate. Local systems will be supported to vary contracts in 2018/19 if they can move at pace to this
approach.
2. Urgent and Emergency Care (UEC) The SWL UEC Delivery Plan 2017/18-18/19 details the priorities for delivery across SWL in line with the
national and London regional expectations for improving urgent and emergency care and getting A&E
performance back on track across SWL. Delivering timely access through the winter, as well as other
periods, remains a top priority. A&E Delivery Boards have worked collectively through the SWL UEC
Transformation & Delivery Boards to agree the collective delivery plan across 7 UEC pillars:
NHS 111 Online – support the local roll-out of NHS 111 Online across SWL, including procurement
of an online solution subject to pilot evaluation.
NHS 111 Calls – continue to increase the number of calls transferred to a clinician by March 2018
so that patients access the right care first time. Achieve direct booking from 111 to GP in and out
of hours by March 2019.
GP access – Continue to achieve 100% population coverage for evening and weekend
appointments and GP practices meeting the seven national standards by March 2019.
Urgent Treatment Centres – All urgent care facilities to be designated by March 18 (we currently
have 3 facilities where designation requires more work), and for designated UTCs to meet the
London specification by December 2019.
Ambulance – Continue to implement demand management plans with a reduction of Type 1 and
Type 2 conveyances to hospital by March 2019. Fully embed the Ambulance Response
Programme during 18/19.
Page 5 of 25
Hospitals – Deliver and sustain the 95% A&E 4 hour standard. Seek to achieve the 15 minute
ambulance handover standard at ED. Providers are expected to implement initiatives around
SAFER, Emergency Care Dataset and Early comprehensive geriatric assessment in time for Winter
17/18 as well as make progress towards implementing 14 hour-7 day a week Ambulatory Care
(adults and CYP).
Hospital to Home – A&E Delivery Boards and Local Transformation Boards will be expected to
make considerable improvements to reducing the number of CHC assessments in hospital (<15%
by March 18) and further work will be required to maintain this during 2018/19. All local systems
are expected to continue to implement the 8 High Impact Changes by March 2018 and continuing
into 2018/19.
3. Primary Care Primary care is fundamental to the delivery of effective healthcare, is important in tackling local health
needs and the things we know our local population want to see addressed. Our aim is to put primary
care on a sustainable footing for the future, while maintaining or improving the current quality of care.
Our work is informed by the London Strategic Commissioning Framework and the GPFV, and focuses on
localised general practice (list based care) that is underpinned by quality and consistency of care. Our
intentions are:
• Continue to support provider development through supporting implementation of the 10 high impact actions in General Practice to release time for care.
• Development of primary care at scale initiatives as part of integrated locality teams. • Develop new roles in primary care and initiatives to support recruitment and retention of the
primary care workforce. • Increase access to primary care through delivery of the extended access specification. • Improve the use of technology in primary care such as online consultations. • Development of estates through delivery of ETTF initiatives. • Revised primary care contracts to support implementation of the General Practice Forward View
and strategic commissioning framework. • Achieving national requirements in relation to peer review and support to practices in making
high quality referrals. All CCGs have been conducting their PMS reviews and are on track for contract start date of 1st April 2018. Further details are in section 11.
4. Cancer SWL commissioners and providers are working in conjunction with RM Partners Cancer Vanguard to
implement the Cancer Delivery Plan across SWL and NWL STPs. The vision is to achieve world-class cancer
outcomes for the population by 2020/21. Cancer transformation funding is now secured and being
released to help implement the delivery plan.
The Delivery Plan focuses on 3 major pillars:
Early Diagnosis – significantly improving survival, experience and quality of life through earlier
diagnosis and treatment. This will be achieved through:
o Ensure delivery of all the access standards set out in the NHS constitution.
Page 6 of 25
o Continue to achieve and maintain the NHS Constitution 62 day cancer standard, including
by securing adequate diagnostic capacity, and the other NHS Constitution cancer
standards.
o Improving targeted screening (particularly bowel screening) and early diagnosis
interventions through reducing variation in primary care to tackle health inequalities,
deliver better access to services and outcomes. This includes raising patient awareness
and acting on symptoms of cancer. Providers have already made progress to achieve 40%
of first attendances by day 7.
o Work across all acute providers to deliver sustainable waiting times to access diagnostics
and treatment through delivery of new pathways, (including “straight to test”), reviewing
PRL processes and improving MDT arrangements.
o Complete implementation across all providers of the Prostate and lung best practice
pathway: Providers to complete actions as set out in the SWL Cancer Performance
Improvement Plan.
o Undertake review of head and neck pathway to optimise care.
o All providers to continue to drive improvements in PTL management and MDT resources,
including delivery of 38 day trajectory, to support whole system delivery.
o All providers to continue to complete root cause analysis and share learning from 62 day
breaches.
Recovery Package – Improve the quality of life for people living with and beyond cancer, defining
cancer as a long term condition and ensuring it is managed as such across health and social care.
This will be achieved through:
o Ensuring all elements of the Recovery Package are commissioned, including Health
Needs Assessments (HNAs), completion of treatment summaries and completion of
holistic cancer care reviews in the community.
Stratified Follow-up – Ensure stratified follow-up pathways are in place to appropriately see
patients, with a focus on breast and prostate. This will be achieved through:
o Implementing primary care-led follow-up for stable prostate cancer patients. Planning is
underway to implement the primary care led model by Autumn 2017/18 and fully embed
the model by the end 17/18 and into 18/19.
5. Mental Health Our ambitions within mental health are to implement the SW London Mental Health Delivery Plan,
aligned to the Mental Health Forward View, and deliver the transformation of MH services across SWL.
Key initiatives for 2018/19 include:
Phased implementation of a SW London specialist perinatal community mental health team that meets Royal College of Psychiatry and London Clinical Network recommendations
Implementation of CAMHS transformation plans, including:
Page 7 of 25
o improving access to ensure that approximately 2,000 additional CYP receive NHS-funded community support per year (approximate calculation of SWL share of FYFV ambition)
o Review the designated SWL Eating Disorder Service to ensure that the requirements of the Access and Waiting Time Standards are met
o Develop and implement plans to increase numbers of CAMHS workforce to meet national target of 1,700 additional clinicians by 2020
o Commission SWL Neuro developmental pathway for children with ASD/ ADHD by April 2018
o Improve access to crisis response for children and young people o Develop provision post needs assessment for specialist CAMHS services
Complete a demand and capacity review of community mental health services, including Crisis Resolution Home Treatment Teams; LTBs will make decisions locally about how to address findings from the review
Review the community mental health crisis pathway improvements from 16/17 and 17/18 and take forward any recommendations or changes arising
Deliver psychiatric liaison services which meet Core 24 standards in all acute hospitals from April 2018
Implementation of local suicide prevention strategies and action plans; plans to be produced by December 2017
Increase access to psychological therapies across the population, including targeting Long Term Conditions and pathways, such as diabetes and MSK
Improve the physical health interventions offered to people with SMI
Increase the numbers of people receiving a timely dementia diagnosis, and ensuring they receive best practice interventions following diagnosis
Contribute to the South London forensic mental health service pilot
Implement recommendations from London wide work on Health Based Places of Safety and the section 136 pathway
Develop and implement local plans to increase the numbers within the mental health workforce, in line with national ambitions
In addition to the above, we will be working to improve prevention and early intervention around mental
health services, and to make progress on the integration of physical and mental health services as a
common theme running across all our work (including specialist mental health services). Working in
partnership with CCGs, our plans will support delivery of key local priorities:
Supporting primary care to manage and prevent admissions
Reducing lengths of stay and improving discharge processes, enabling more care to be delivered in the community
Reviewing step-down rehab services
6. Planned Care
6.1 St George’s NHS Foundation Trust
As St George’s Trust impacts on all of the SWL CCGs, and faces particular performance challenges, we
will work in partnership with the Trust and other local providers, to address the planned care access
issues at St George’s Hospital and Queen Mary’s Hospital Roehampton, seeking to ensure patients have
timely access to care.
Page 8 of 25
6.2 Effective Commissioning Initiative (ECI)
SWL CCGs are collaborating increasingly to ensure that variation is reduced for clinical threshold for
procedures with limited clinical effectiveness. As part of this collaboration joint clinical thresholds (version
2.0) are being developed and agreed in 17/18. To ensure adherence, a joint prior approval system went
live in July 17 for all six CCGs, developed in collaboration with providers to ensure their effectiveness. SWL
CCGs are expecting approximately 20,000 procedures per annum to go through the Prior Approval
System. During 2018/19, providers are expected to continue embedding internal processes to send Prior
Approval requests for relevant procedures.
6.3 Musculoskeletal Services (MSK)
SWL CCGs have agreed a shared direction of travel for Musculoskeletal (MSK) services (Physiotherapy,
Pain Management, Rheumatology and Trauma/Orthopaedics). The goal is to achieve an integrated MSK
Single Point of Access with clinical assessment triage by the end of 2017/18. There is agreement to achieve
as much commonality as possible in terms of specification and delivery.
6.4 Ear, nose and throat (ENT)
SWL CCGs will work with providers during the second half of 2017/18 to discuss a networked approach
to secondary and tertiary ENT provision in order to provide consistency of access and pathway across
the sector.
6.5 Advice and Guidance
Evidence suggests that up to 65% of patients attending outpatient specialty clinics are discharged
without the need for treatment. This can waste patient’s time and money. Evidence also shows that
many of the unnecessary referrals can be avoided when GPs have ready access to expert clinical advice,
including real time information.
‘Advice and Guidance’ is a tool that supports GP decision making. It is a key component of ‘best
practice’ referral management strategy. It allows one clinician to seek advice from another before
making a decision about the best treatment for a patient.
South West London CCGs currently commission advice and guidance services, (Kinesis and e-referral),
which directly links GPs to local hospital consultant for rapid access to expert advice about their
patients’ condition.
Benefits:
Patient - ensures that the right care and services are offered at the right time and it gives the
patient confidence that their needs are being quickly assessed by clinical specialists.
GP – support in making the right decisions for ‘when and how to treat and when to refer’ their
patient to hospital
Hospital - ensures that only patients that need their services are seen by the specialist, helping
to reduce demand on hospital services
By using advice and guidance, we have reduced unnecessary outpatient appointments and improved
financial efficiency. For every 100 patients that the GP has sought advice and guidance for their
condition, we have evidence that 45 (45%) first outpatient appointments were avoided.
Page 9 of 25
Currently, our GPs can receive advice and guidance from 37 different specialties across two local trusts.
We want to maximise the benefits of using advice and guidance across the whole system. Our aim is to
extend advice and guidance to all suitable specialties and in all our local trusts by October 2018.
6.6 Other areas of focus
SWL CCGs expect to transform the approach to Planned Care and Long term conditions through a phased
transformation programme which aims to:
• Embed and promote health and wellbeing and empowers patients to take control of their health
through self-care, self-management and shared decision making.
• Shifting care out of hospital, integrating and bringing it closer to patients through the speciality
working groups.
• Workforce development across the system through education and up skilling.
• Development of Primary Care to manage demand, variation and capacity whilst improving patient
care.
7. Maternity South West London will provide consistently high quality healthcare to women and families, delivered by
a skilled workforce that is confident in supporting both low and high risk women to have safe, healthy
births. Women and families will be empowered to make informed choice of where they receive their
antenatal care and preferred place of birth, increasing the availability of home births and midwifery led
care. Providers will continue to deliver safe and sustainable care for women and babies who need
obstetric-led and specialist care. Women and families will be able to access personalised antenatal,
intrapartum and postnatal care, as well as improved access to additional support where required such as
high quality and responsive perinatal mental health services.
During 2017/18, SWL Trusts and CCGs have participated in the Maternity Choice and Personalisation
Pioneer, funded by NHS England. Personal Maternity Care Budgets (PMCBs) are currently being piloted
by midwifery teams in each Trust across SWL, with each Trust recruiting 25 women in the pilot. “My
Maternity Journey in SW London” is a booklet that has been developed to support women to make
informed choices about their maternity care. It contains information on the Local Maternity Offer across
SWL Trusts for antenatal, place of birth and postnatal care. It also includes questions to support
personalised care planning. There will be an end of pilot evaluation by end 2017/18. It is anticipated that
during 2018/19, “My Maternity Journey in SWL” is further developed into a single point of access for
maternity services and rolled out across SW London.
The SWL Maternity Network evolved into the SWL Local Maternity System (LMS) from April 2017, in line
with expectations from NHS England for LMS’s to be established across each STP footprint. The LMS is
developing its delivery plan in line with the Better Births national maternity review recommendations by
end October. The draft priorities agreed for 2017/18 and onwards are as follows:
• Personalisation and Choice - Complete the pilot and evaluation of “My Maternity Journey in SW
London” (Personal Maternity Care Budgets) by end 2017/18. Preparing women and their
families for pregnancy and parenthood through consistent antenatal education and up-to-date,
Page 10 of 25
evidence-based information through to the postnatal stage of the maternity pathway including
supporting women to access perinatal mental health services. Women are provided with
individualised care, with a focus on their needs and preferences, and supported to develop
personalised care plans.
• Continuity of Carer – All Trusts are developing plans for roll-out of continuity of midwifery carer
from 17/18 onwards. This will ensure continuity of midwifery carer throughout the pathway
(initially with a focus on antenatal and postnatal care), contributing to better clinical outcomes
and improved patient experience. Continuity of Carer will have a strong emphasis on promoting
midwifery led care and normal birth for low risk pregnancies.
• Improving safety of maternity services – Reduce the rate of stillbirth, neonatal and maternal
deaths and the number of brain injuries occurring during or soon after birth, in line with the
national “halve it” ambition by 2030. This will be achieved through improving learning from
incidents and implementing a single Maternity quality and performance framework and
dashboard across SWL. This also means providing care which meets the clinical quality
standards for all women and their babies, including maintaining safe midwifery and obstetric
staffing levels.
• Improving access to and quality of postnatal care and perinatal mental health services –
working across providers to level up the quality of postnatal care and availability and access to
community-based perinatal mental health support. It is anticipated that funding will be
available to support the increased access to perinatal mental health in 18/19.
8. Learning Disabilities The South West London Transforming Care Partnership’s (TCP) plan aims to support people with a
learning disability and/or autism, who display behaviour that challenges, including mental health, to have
the same life chances as other people, and to live as independently as possible, with the right support
from mainstream health and care services.
We will achieve this through:
Implementing the National Service Model across SWL
Developing intensive support and crisis management mechanisms in a community setting
Ensuring comprehensive dynamic risk registers are in place, covering adults and children, and that the registers are proactively used to manage people at risk of admission
Through regular meetings between NHSE Specialised Commissioning, CCG commissioners and the TCP, create robust person centred plans to discharge identified in-patients from mental health institutions and delivery the TCP trajectory
Embedding the voice of the service users, their families/carer into the programme and incorporating feedback into the work
Ensuring the workforce in the community are appropriately trained and supported, particularly with regard to roll out of Positive Behavioural Support approaches
9. Children and young people
Our commissioning will focus on early intervention and prevention and to ensure that children are seen in the most appropriate settings as close to home as possible
Page 11 of 25
Strengthening community based support for children and young people for physical and mental health;
Strengthening the provision of CAMHS including reviewing the SWL Neurodevelopmental pathway;
Providing case management and co-ordination for children with complex needs;
Rapid response in primary and community settings;
Enhanced hospital front door assessment and streaming to reduce the need for admission; and
Continue to work towards the achievement of the London CYP Acute Care Standards.
10. Integrated community care A key aim of the SWL STP is to ensure that people receive the right care in the best setting, and that people can remain in their home wherever possible, which is what they tell us they want. Local Transformation Boards are driving the production of local plans to transform health and care services and deliver this objective. These plans will be locally tailored but have some common core elements which have been agreed at SWL level. Adults with frailty and complex care needs
Across South West London this patient population use and need a diverse range of health, social care
and voluntary services. They require and use services from multiple agencies, public and private sector
providers, often around the clock, for multiple contacts, sometimes several times a day.
There are a range of national and regionally initiated programmes that strive to improve and transform
service satisfaction, experience, safety, quality and efficiency for patients and carers. SWL
commissioners and providers, working in partnership, are strategically aligning and evaluating service
delivery for this patient population, using national and regional guidelines, evidence and quality
standards.
Services are locally commissioned, planned and delivered, based on local demography and population
need. Each local delivery group has a strategically aligned, delivery plan that is locally planned, designed
and delivered against strategic themes. These themes or service principles promote person centred
care, risk stratification, collaborative multidisciplinary pathways and networks and the promotion of
cross organisational and geographical boundaries and digital technologies to share information.
These programmes comprise: Enhancing Care in Care Homes (National Vanguard) including specific
schemes such as rolling out the red bag, Continuing Health Care and End of Life Care. They are closely
aligned with locality teams and intermediate care.
Locality teams As part of delivering an enhanced offer to support adults to receive treatment, support and care to enable them to remain at home, SWL will establish a network of MDT locality teams at an LDU level. The locality teams will be centred around primary care and responsible for managing the care of at least 50k people in a geographical area (around a group of practices). They will build on existing community based health and social care infrastructure to establish integrated teams. While working collaboratively teams will operate using a single point of contact and named care co-ordinator model, carrying out care planning and review in partnership with patients to improve patient experience and outcome and reduce unscheduled care needs. The focus is on enabling people to stay well.
Page 12 of 25
Establish locality based MDTs managing populations of at least 50,000; risk stratification and cross system working to proactively manage identified cohort in the community
Embedding effective care planning processes within the locality team, including integrated care plans, personalised outcomes and regular MDT reviews
Integrated intermediate and crisis care
A significant number of people are admitted to hospital because they have experienced a change in their health and/or social situation. While it is acknowledged that a proportion of these people will continue to require admission to an acute setting, a proportion could be supported in a non-acute setting. Additionally, a number of people could be discharged earlier from the acute setting with adequate support and management of risk.
To ensure patients receive appropriate care in the right setting, SWL’s intermediate care services will provide enhanced access and rapid response supported by multi-disciplinary teams
Anticipatory care plans are in place to support out of hours management of crisis
Timely access to advice and assessment to prevent hospital admissions including o rapid response assessment within two hours 7 days a week o real-time access to geriatrician advice o Geriatrician review available within 2 hours in ED
Rapid access to alternative services to prevent hospital admissions and enable timely discharge o Health and social care packages available within 4 hours 7 days a week, including access
to equipment o Step-up beds available to prevent hospital admission and step down beds? o 24-hour care packages can be delivered in patients’ own home where appropriate o Rapid response GPs have admitting rights to frailty wards
There is an integrated team responsible for planning discharges of patients with complex needs which includes community health and social care
A home First/Discharge to Assess approach is adhered to across all providers
11. Further local priorities
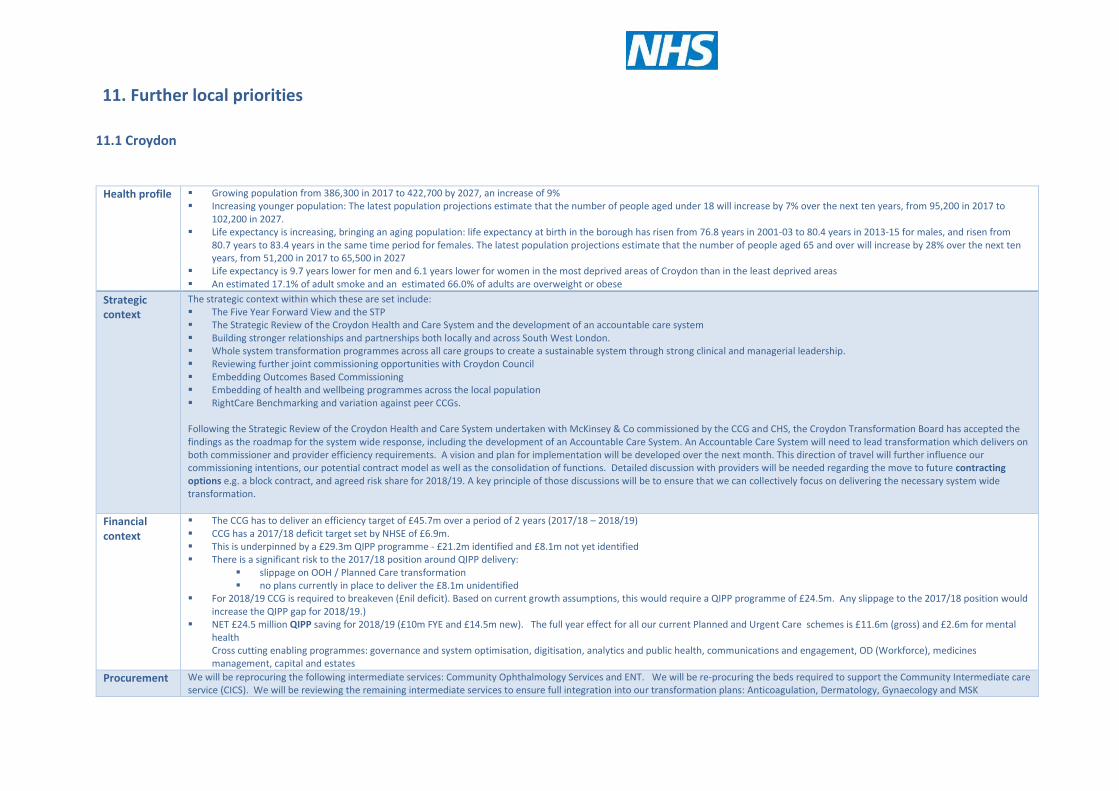
11.1 Croydon
Health profile Growing population from 386,300 in 2017 to 422,700 by 2027, an increase of 9% Increasing younger population: The latest population projections estimate that the number of people aged under 18 will increase by 7% over the next ten years, from 95,200 in 2017 to
102,200 in 2027. Life expectancy is increasing, bringing an aging population: life expectancy at birth in the borough has risen from 76.8 years in 2001-03 to 80.4 years in 2013-15 for males, and risen from
80.7 years to 83.4 years in the same time period for females. The latest population projections estimate that the number of people aged 65 and over will increase by 28% over the next ten years, from 51,200 in 2017 to 65,500 in 2027
Life expectancy is 9.7 years lower for men and 6.1 years lower for women in the most deprived areas of Croydon than in the least deprived areas An estimated 17.1% of adult smoke and an estimated 66.0% of adults are overweight or obese
Strategic context
The strategic context within which these are set include: The Five Year Forward View and the STP The Strategic Review of the Croydon Health and Care System and the development of an accountable care system Building stronger relationships and partnerships both locally and across South West London. Whole system transformation programmes across all care groups to create a sustainable system through strong clinical and managerial leadership. Reviewing further joint commissioning opportunities with Croydon Council Embedding Outcomes Based Commissioning Embedding of health and wellbeing programmes across the local population RightCare Benchmarking and variation against peer CCGs. Following the Strategic Review of the Croydon Health and Care System undertaken with McKinsey & Co commissioned by the CCG and CHS, the Croydon Transformation Board has accepted the findings as the roadmap for the system wide response, including the development of an Accountable Care System. An Accountable Care System will need to lead transformation which delivers on both commissioner and provider efficiency requirements. A vision and plan for implementation will be developed over the next month. This direction of travel will further influence our commissioning intentions, our potential contract model as well as the consolidation of functions. Detailed discussion with providers will be needed regarding the move to future contracting options e.g. a block contract, and agreed risk share for 2018/19. A key principle of those discussions will be to ensure that we can collectively focus on delivering the necessary system wide transformation.
Financial context
The CCG has to deliver an efficiency target of £45.7m over a period of 2 years (2017/18 – 2018/19) CCG has a 2017/18 deficit target set by NHSE of £6.9m. This is underpinned by a £29.3m QIPP programme - £21.2m identified and £8.1m not yet identified There is a significant risk to the 2017/18 position around QIPP delivery:
slippage on OOH / Planned Care transformation no plans currently in place to deliver the £8.1m unidentified
For 2018/19 CCG is required to breakeven (£nil deficit). Based on current growth assumptions, this would require a QIPP programme of £24.5m. Any slippage to the 2017/18 position would increase the QIPP gap for 2018/19.)
NET £24.5 million QIPP saving for 2018/19 (£10m FYE and £14.5m new). The full year effect for all our current Planned and Urgent Care schemes is £11.6m (gross) and £2.6m for mental health Cross cutting enabling programmes: governance and system optimisation, digitisation, analytics and public health, communications and engagement, OD (Workforce), medicines management, capital and estates
Procurement We will be reprocuring the following intermediate services: Community Ophthalmology Services and ENT. We will be re-procuring the beds required to support the Community Intermediate care service (CICS). We will be reviewing the remaining intermediate services to ensure full integration into our transformation plans: Anticoagulation, Dermatology, Gynaecology and MSK
Page 14 of 25
Croydon summary
Thro
ugh
an
am
bit
iou
s p
rogr
amm
e o
f in
no
vati
on
Thro
ugh
wo
rkin
g to
geth
er
wit
h t
he
div
ers
e c
om
mu
nit
ies
of
Cro
ydo
n a
nd
ou
r p
artn
ers
Thro
ugh
usi
ng
ou
r re
sou
rce
s w
ise
ly
We
will
tra
nsf
orm
hea
lth
care
to
hel
p p
eop
le lo
ok
afte
r th
em
selv
es a
nd
wh
en
pe
op
le n
eed
car
e
they
will
be
able
to
acc
ess
hig
h q
ual
ity
serv
ice
s
Cro
ydo
n L
DU
will
del
iver
….
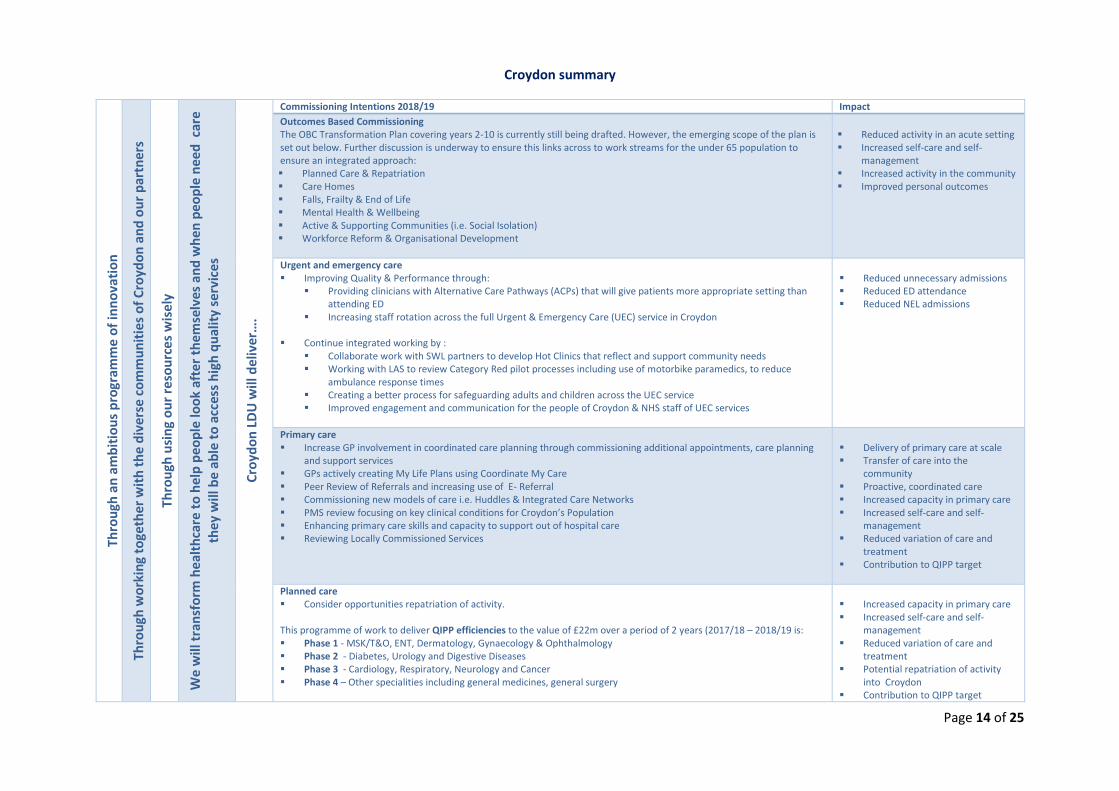
Commissioning Intentions 2018/19 Impact
Outcomes Based Commissioning The OBC Transformation Plan covering years 2-10 is currently still being drafted. However, the emerging scope of the plan is set out below. Further discussion is underway to ensure this links across to work streams for the under 65 population to ensure an integrated approach: Planned Care & Repatriation Care Homes Falls, Frailty & End of Life Mental Health & Wellbeing Active & Supporting Communities (i.e. Social Isolation) Workforce Reform & Organisational Development
Reduced activity in an acute setting Increased self-care and self-
management Increased activity in the community Improved personal outcomes
Urgent and emergency care Improving Quality & Performance through:
Providing clinicians with Alternative Care Pathways (ACPs) that will give patients more appropriate setting than attending ED
Increasing staff rotation across the full Urgent & Emergency Care (UEC) service in Croydon Continue integrated working by :
Collaborate work with SWL partners to develop Hot Clinics that reflect and support community needs Working with LAS to review Category Red pilot processes including use of motorbike paramedics, to reduce
ambulance response times Creating a better process for safeguarding adults and children across the UEC service Improved engagement and communication for the people of Croydon & NHS staff of UEC services
Reduced unnecessary admissions Reduced ED attendance Reduced NEL admissions
Primary care Increase GP involvement in coordinated care planning through commissioning additional appointments, care planning
and support services GPs actively creating My Life Plans using Coordinate My Care Peer Review of Referrals and increasing use of E- Referral Commissioning new models of care i.e. Huddles & Integrated Care Networks PMS review focusing on key clinical conditions for Croydon’s Population Enhancing primary care skills and capacity to support out of hospital care Reviewing Locally Commissioned Services
Delivery of primary care at scale Transfer of care into the
community Proactive, coordinated care Increased capacity in primary care Increased self-care and self-
management Reduced variation of care and
treatment Contribution to QIPP target
Planned care Consider opportunities repatriation of activity.
This programme of work to deliver QIPP efficiencies to the value of £22m over a period of 2 years (2017/18 – 2018/19 is: Phase 1 - MSK/T&O, ENT, Dermatology, Gynaecology & Ophthalmology Phase 2 - Diabetes, Urology and Digestive Diseases Phase 3 - Cardiology, Respiratory, Neurology and Cancer Phase 4 – Other specialities including general medicines, general surgery
Increased capacity in primary care Increased self-care and self-
management Reduced variation of care and
treatment Potential repatriation of activity
into Croydon Contribution to QIPP target
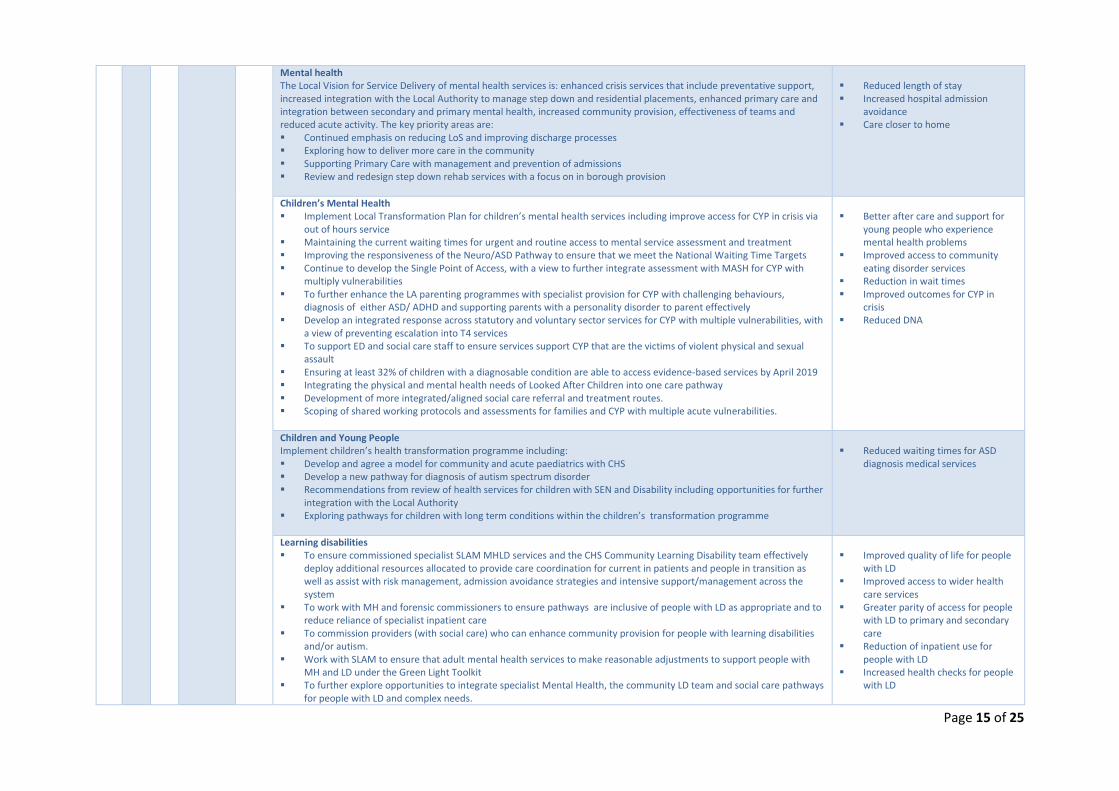
Page 15 of 25
Mental health The Local Vision for Service Delivery of mental health services is: enhanced crisis services that include preventative support, increased integration with the Local Authority to manage step down and residential placements, enhanced primary care and integration between secondary and primary mental health, increased community provision, effectiveness of teams and reduced acute activity. The key priority areas are: Continued emphasis on reducing LoS and improving discharge processes Exploring how to deliver more care in the community Supporting Primary Care with management and prevention of admissions Review and redesign step down rehab services with a focus on in borough provision
Reduced length of stay Increased hospital admission
avoidance Care closer to home
Children’s Mental Health Implement Local Transformation Plan for children’s mental health services including improve access for CYP in crisis via
out of hours service Maintaining the current waiting times for urgent and routine access to mental service assessment and treatment Improving the responsiveness of the Neuro/ASD Pathway to ensure that we meet the National Waiting Time Targets Continue to develop the Single Point of Access, with a view to further integrate assessment with MASH for CYP with
multiply vulnerabilities To further enhance the LA parenting programmes with specialist provision for CYP with challenging behaviours,
diagnosis of either ASD/ ADHD and supporting parents with a personality disorder to parent effectively Develop an integrated response across statutory and voluntary sector services for CYP with multiple vulnerabilities, with
a view of preventing escalation into T4 services To support ED and social care staff to ensure services support CYP that are the victims of violent physical and sexual
assault Ensuring at least 32% of children with a diagnosable condition are able to access evidence-based services by April 2019 Integrating the physical and mental health needs of Looked After Children into one care pathway Development of more integrated/aligned social care referral and treatment routes. Scoping of shared working protocols and assessments for families and CYP with multiple acute vulnerabilities.
Better after care and support for
young people who experience mental health problems
Improved access to community eating disorder services
Reduction in wait times Improved outcomes for CYP in
crisis Reduced DNA
Children and Young People Implement children’s health transformation programme including: Develop and agree a model for community and acute paediatrics with CHS Develop a new pathway for diagnosis of autism spectrum disorder Recommendations from review of health services for children with SEN and Disability including opportunities for further
integration with the Local Authority Exploring pathways for children with long term conditions within the children’s transformation programme
Reduced waiting times for ASD
diagnosis medical services
Learning disabilities To ensure commissioned specialist SLAM MHLD services and the CHS Community Learning Disability team effectively
deploy additional resources allocated to provide care coordination for current in patients and people in transition as well as assist with risk management, admission avoidance strategies and intensive support/management across the system
To work with MH and forensic commissioners to ensure pathways are inclusive of people with LD as appropriate and to reduce reliance of specialist inpatient care
To commission providers (with social care) who can enhance community provision for people with learning disabilities and/or autism.
Work with SLAM to ensure that adult mental health services to make reasonable adjustments to support people with MH and LD under the Green Light Toolkit
To further explore opportunities to integrate specialist Mental Health, the community LD team and social care pathways for people with LD and complex needs.
Improved quality of life for people
with LD Improved access to wider health
care services Greater parity of access for people
with LD to primary and secondary care
Reduction of inpatient use for people with LD
Increased health checks for people with LD
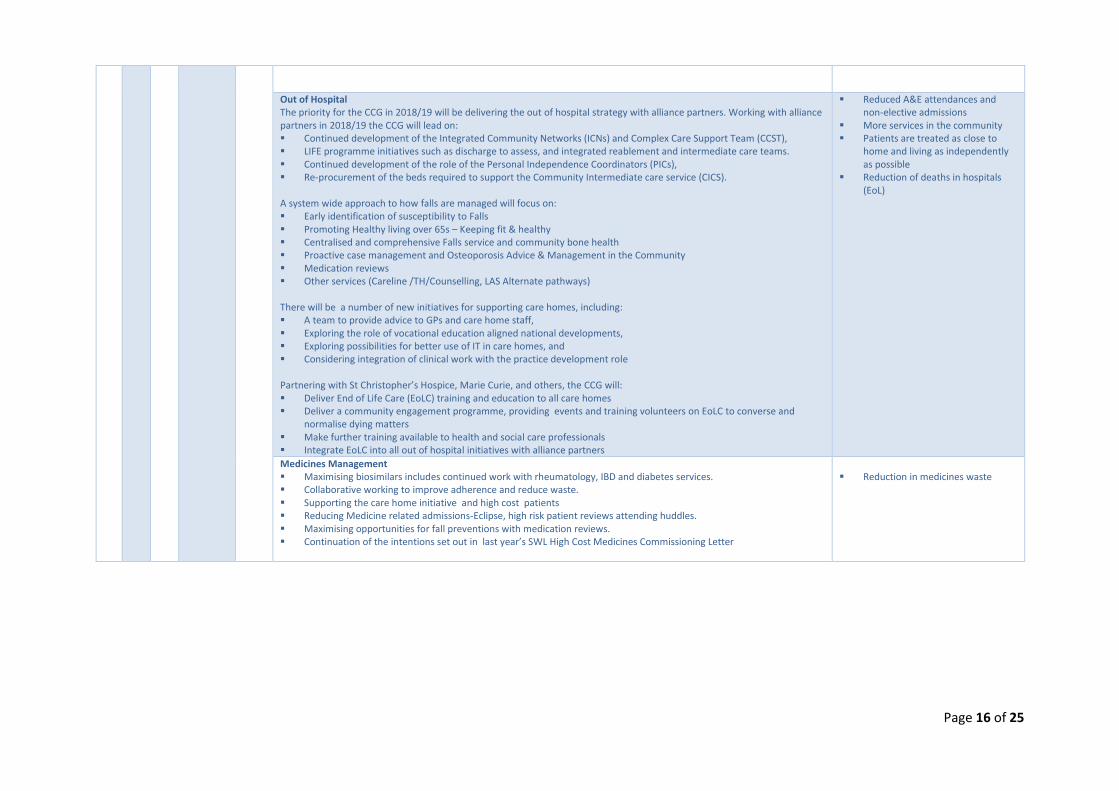
Page 16 of 25
Out of Hospital The priority for the CCG in 2018/19 will be delivering the out of hospital strategy with alliance partners. Working with alliance partners in 2018/19 the CCG will lead on: Continued development of the Integrated Community Networks (ICNs) and Complex Care Support Team (CCST), LIFE programme initiatives such as discharge to assess, and integrated reablement and intermediate care teams. Continued development of the role of the Personal Independence Coordinators (PICs), Re-procurement of the beds required to support the Community Intermediate care service (CICS). A system wide approach to how falls are managed will focus on: Early identification of susceptibility to Falls Promoting Healthy living over 65s – Keeping fit & healthy Centralised and comprehensive Falls service and community bone health Proactive case management and Osteoporosis Advice & Management in the Community Medication reviews Other services (Careline /TH/Counselling, LAS Alternate pathways) There will be a number of new initiatives for supporting care homes, including: A team to provide advice to GPs and care home staff, Exploring the role of vocational education aligned national developments, Exploring possibilities for better use of IT in care homes, and Considering integration of clinical work with the practice development role Partnering with St Christopher’s Hospice, Marie Curie, and others, the CCG will: Deliver End of Life Care (EoLC) training and education to all care homes Deliver a community engagement programme, providing events and training volunteers on EoLC to converse and
normalise dying matters Make further training available to health and social care professionals Integrate EoLC into all out of hospital initiatives with alliance partners
Reduced A&E attendances and non-elective admissions
More services in the community Patients are treated as close to
home and living as independently as possible
Reduction of deaths in hospitals (EoL)
Medicines Management Maximising biosimilars includes continued work with rheumatology, IBD and diabetes services. Collaborative working to improve adherence and reduce waste. Supporting the care home initiative and high cost patients Reducing Medicine related admissions-Eclipse, high risk patient reviews attending huddles. Maximising opportunities for fall preventions with medication reviews. Continuation of the intentions set out in last year’s SWL High Cost Medicines Commissioning Letter
Reduction in medicines waste
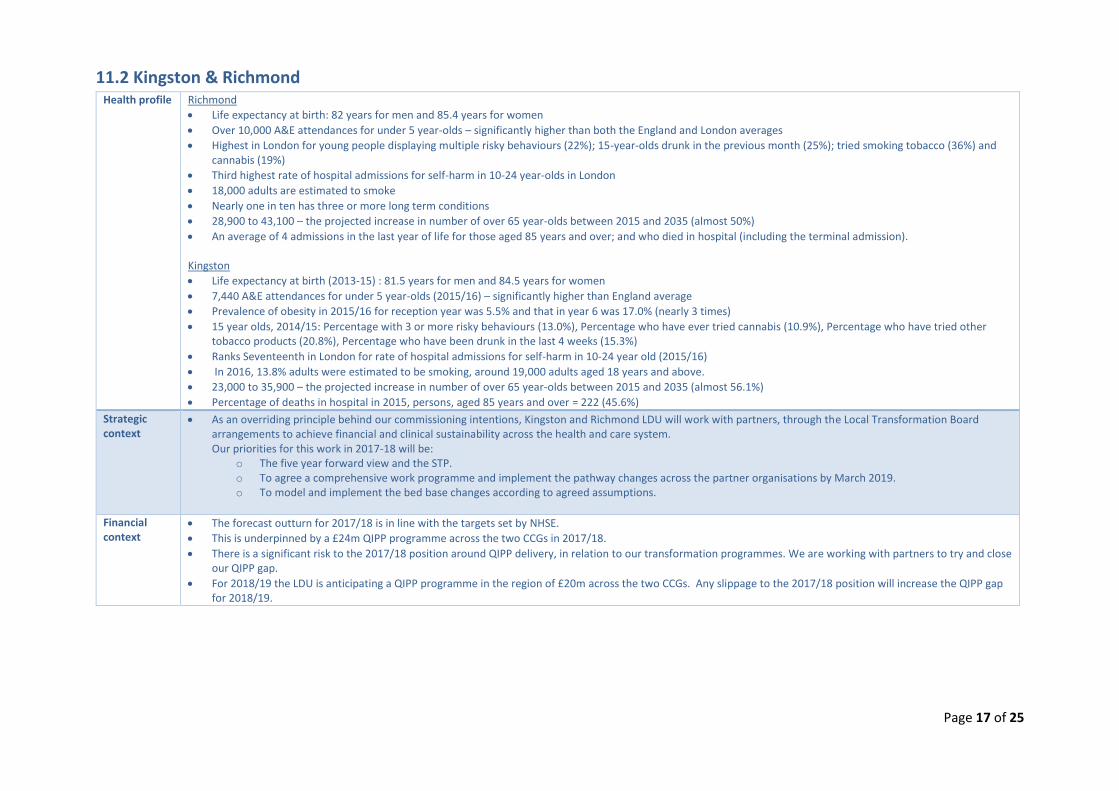
Page 17 of 25
11.2 Kingston & Richmond Health profile Richmond
Life expectancy at birth: 82 years for men and 85.4 years for women
Over 10,000 A&E attendances for under 5 year-olds – significantly higher than both the England and London averages
Highest in London for young people displaying multiple risky behaviours (22%); 15-year-olds drunk in the previous month (25%); tried smoking tobacco (36%) and cannabis (19%)
Third highest rate of hospital admissions for self-harm in 10-24 year-olds in London
18,000 adults are estimated to smoke
Nearly one in ten has three or more long term conditions
28,900 to 43,100 – the projected increase in number of over 65 year-olds between 2015 and 2035 (almost 50%)
An average of 4 admissions in the last year of life for those aged 85 years and over; and who died in hospital (including the terminal admission).
Kingston
Life expectancy at birth (2013-15) : 81.5 years for men and 84.5 years for women
7,440 A&E attendances for under 5 year-olds (2015/16) – significantly higher than England average
Prevalence of obesity in 2015/16 for reception year was 5.5% and that in year 6 was 17.0% (nearly 3 times)
15 year olds, 2014/15: Percentage with 3 or more risky behaviours (13.0%), Percentage who have ever tried cannabis (10.9%), Percentage who have tried other tobacco products (20.8%), Percentage who have been drunk in the last 4 weeks (15.3%)
Ranks Seventeenth in London for rate of hospital admissions for self-harm in 10-24 year old (2015/16)
In 2016, 13.8% adults were estimated to be smoking, around 19,000 adults aged 18 years and above.
23,000 to 35,900 – the projected increase in number of over 65 year-olds between 2015 and 2035 (almost 56.1%)
Percentage of deaths in hospital in 2015, persons, aged 85 years and over = 222 (45.6%)
Strategic context
As an overriding principle behind our commissioning intentions, Kingston and Richmond LDU will work with partners, through the Local Transformation Board arrangements to achieve financial and clinical sustainability across the health and care system. Our priorities for this work in 2017-18 will be:
o The five year forward view and the STP. o To agree a comprehensive work programme and implement the pathway changes across the partner organisations by March 2019. o To model and implement the bed base changes according to agreed assumptions.
Financial context
The forecast outturn for 2017/18 is in line with the targets set by NHSE.
This is underpinned by a £24m QIPP programme across the two CCGs in 2017/18.
There is a significant risk to the 2017/18 position around QIPP delivery, in relation to our transformation programmes. We are working with partners to try and close our QIPP gap.
For 2018/19 the LDU is anticipating a QIPP programme in the region of £20m across the two CCGs. Any slippage to the 2017/18 position will increase the QIPP gap for 2018/19.
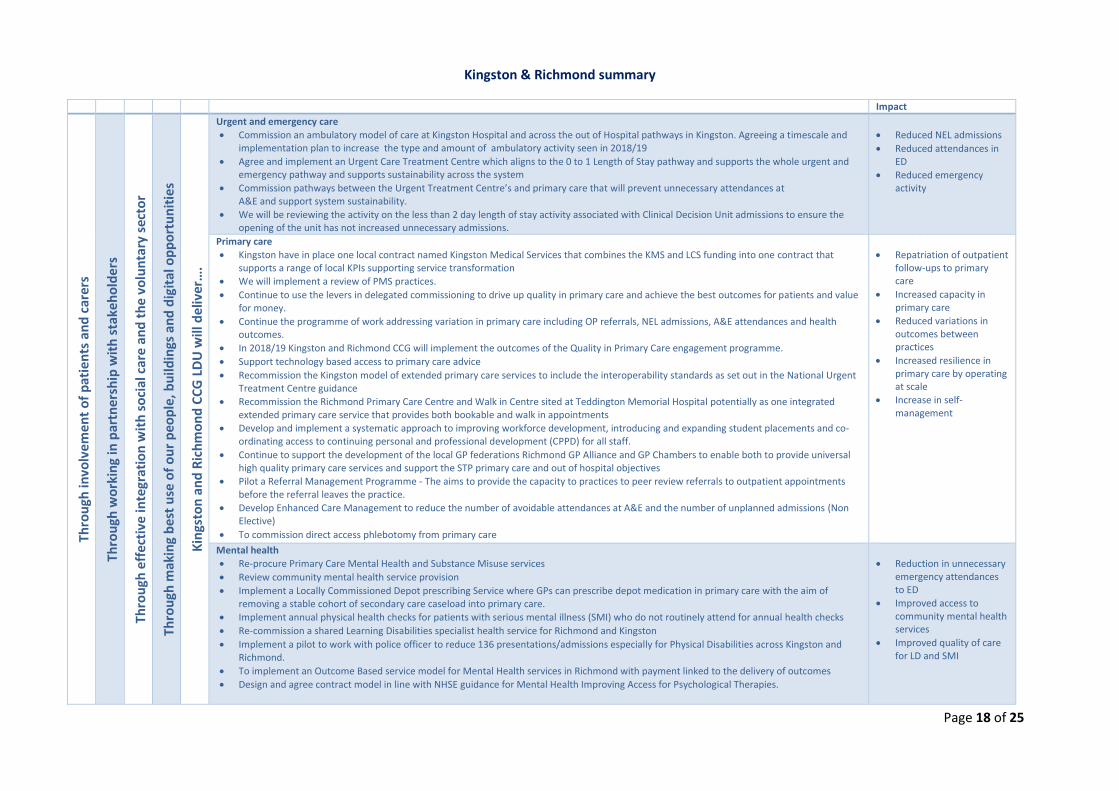
Page 18 of 25
Kingston & Richmond summary Impact
Thro
ugh
invo
lve
me
nt
of
pat
ien
ts a
nd
car
ers
Th
rou
gh w
ork
ing
in p
artn
ers
hip
wit
h s
take
ho
lde
rs
Thro
ugh
eff
ecti
ve in
tegr
atio
n w
ith
so
cial
car
e a
nd
th
e v
olu
nta
ry s
ecto
r
Thro
ugh
mak
ing
bes
t u
se o
f o
ur
peo
ple
, bu
ildin
gs a
nd
dig
ital
op
po
rtu
nit
ies
Kin
gsto
n a
nd
Ric
hm
on
d C
CG
LD
U w
ill d
eliv
er…
.
Urgent and emergency care
Commission an ambulatory model of care at Kingston Hospital and across the out of Hospital pathways in Kingston. Agreeing a timescale and implementation plan to increase the type and amount of ambulatory activity seen in 2018/19
Agree and implement an Urgent Care Treatment Centre which aligns to the 0 to 1 Length of Stay pathway and supports the whole urgent and emergency pathway and supports sustainability across the system
Commission pathways between the Urgent Treatment Centre’s and primary care that will prevent unnecessary attendances at A&E and support system sustainability.
We will be reviewing the activity on the less than 2 day length of stay activity associated with Clinical Decision Unit admissions to ensure the opening of the unit has not increased unnecessary admissions.
Reduced NEL admissions
Reduced attendances in ED
Reduced emergency activity
Primary care
Kingston have in place one local contract named Kingston Medical Services that combines the KMS and LCS funding into one contract that supports a range of local KPIs supporting service transformation
We will implement a review of PMS practices.
Continue to use the levers in delegated commissioning to drive up quality in primary care and achieve the best outcomes for patients and value for money.
Continue the programme of work addressing variation in primary care including OP referrals, NEL admissions, A&E attendances and health outcomes.
In 2018/19 Kingston and Richmond CCG will implement the outcomes of the Quality in Primary Care engagement programme.
Support technology based access to primary care advice
Recommission the Kingston model of extended primary care services to include the interoperability standards as set out in the National Urgent Treatment Centre guidance
Recommission the Richmond Primary Care Centre and Walk in Centre sited at Teddington Memorial Hospital potentially as one integrated extended primary care service that provides both bookable and walk in appointments
Develop and implement a systematic approach to improving workforce development, introducing and expanding student placements and co-ordinating access to continuing personal and professional development (CPPD) for all staff.
Continue to support the development of the local GP federations Richmond GP Alliance and GP Chambers to enable both to provide universal high quality primary care services and support the STP primary care and out of hospital objectives
Pilot a Referral Management Programme - The aims to provide the capacity to practices to peer review referrals to outpatient appointments before the referral leaves the practice.
Develop Enhanced Care Management to reduce the number of avoidable attendances at A&E and the number of unplanned admissions (Non Elective)
To commission direct access phlebotomy from primary care
Repatriation of outpatient follow-ups to primary care
Increased capacity in primary care
Reduced variations in outcomes between practices
Increased resilience in primary care by operating at scale
Increase in self-management
Mental health
Re-procure Primary Care Mental Health and Substance Misuse services
Review community mental health service provision
Implement a Locally Commissioned Depot prescribing Service where GPs can prescribe depot medication in primary care with the aim of removing a stable cohort of secondary care caseload into primary care.
Implement annual physical health checks for patients with serious mental illness (SMI) who do not routinely attend for annual health checks
Re-commission a shared Learning Disabilities specialist health service for Richmond and Kingston
Implement a pilot to work with police officer to reduce 136 presentations/admissions especially for Physical Disabilities across Kingston and Richmond.
To implement an Outcome Based service model for Mental Health services in Richmond with payment linked to the delivery of outcomes
Design and agree contract model in line with NHSE guidance for Mental Health Improving Access for Psychological Therapies.
Reduction in unnecessary emergency attendances to ED
Improved access to community mental health services
Improved quality of care for LD and SMI
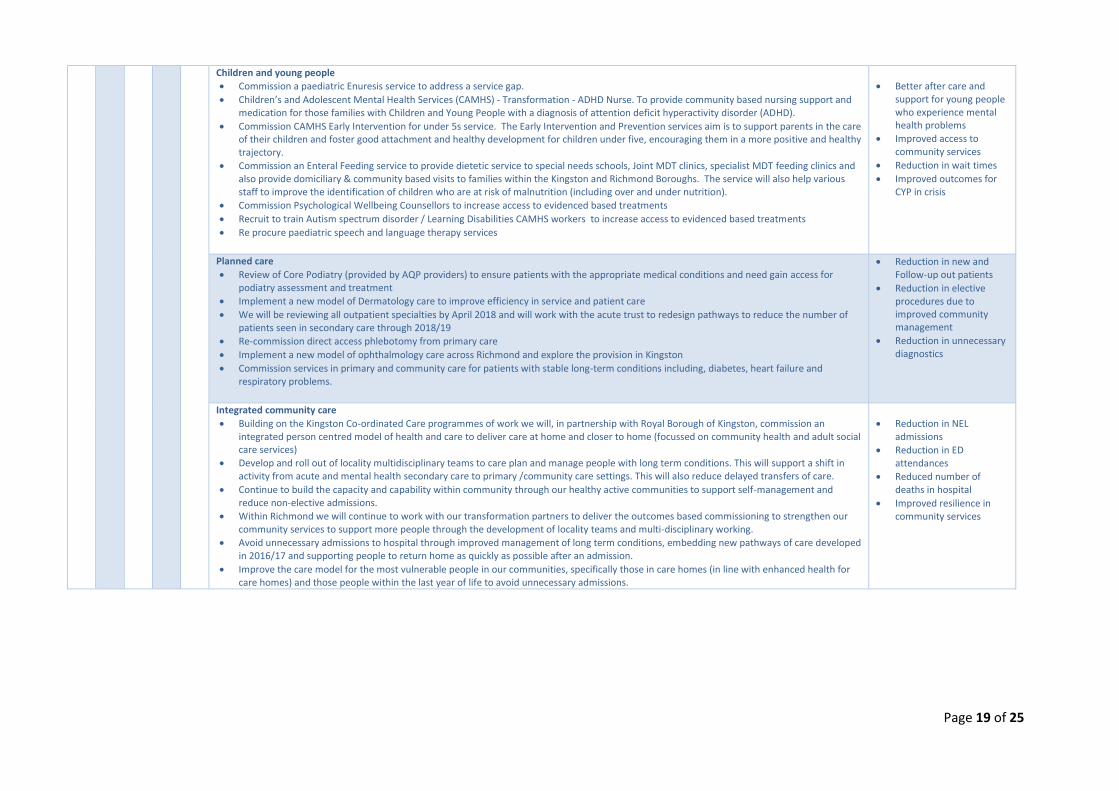
Page 19 of 25
Children and young people
Commission a paediatric Enuresis service to address a service gap.
Children’s and Adolescent Mental Health Services (CAMHS) - Transformation - ADHD Nurse. To provide community based nursing support and medication for those families with Children and Young People with a diagnosis of attention deficit hyperactivity disorder (ADHD).
Commission CAMHS Early Intervention for under 5s service. The Early Intervention and Prevention services aim is to support parents in the care of their children and foster good attachment and healthy development for children under five, encouraging them in a more positive and healthy trajectory.
Commission an Enteral Feeding service to provide dietetic service to special needs schools, Joint MDT clinics, specialist MDT feeding clinics and also provide domiciliary & community based visits to families within the Kingston and Richmond Boroughs. The service will also help various staff to improve the identification of children who are at risk of malnutrition (including over and under nutrition).
Commission Psychological Wellbeing Counsellors to increase access to evidenced based treatments
Recruit to train Autism spectrum disorder / Learning Disabilities CAMHS workers to increase access to evidenced based treatments
Re procure paediatric speech and language therapy services
Better after care and support for young people who experience mental health problems
Improved access to community services
Reduction in wait times
Improved outcomes for CYP in crisis
Planned care
Review of Core Podiatry (provided by AQP providers) to ensure patients with the appropriate medical conditions and need gain access for podiatry assessment and treatment
Implement a new model of Dermatology care to improve efficiency in service and patient care
We will be reviewing all outpatient specialties by April 2018 and will work with the acute trust to redesign pathways to reduce the number of patients seen in secondary care through 2018/19
Re-commission direct access phlebotomy from primary care
Implement a new model of ophthalmology care across Richmond and explore the provision in Kingston
Commission services in primary and community care for patients with stable long-term conditions including, diabetes, heart failure and respiratory problems.
Reduction in new and Follow-up out patients
Reduction in elective procedures due to improved community management
Reduction in unnecessary diagnostics
Integrated community care
Building on the Kingston Co-ordinated Care programmes of work we will, in partnership with Royal Borough of Kingston, commission an integrated person centred model of health and care to deliver care at home and closer to home (focussed on community health and adult social care services)
Develop and roll out of locality multidisciplinary teams to care plan and manage people with long term conditions. This will support a shift in activity from acute and mental health secondary care to primary /community care settings. This will also reduce delayed transfers of care.
Continue to build the capacity and capability within community through our healthy active communities to support self-management and reduce non-elective admissions.
Within Richmond we will continue to work with our transformation partners to deliver the outcomes based commissioning to strengthen our community services to support more people through the development of locality teams and multi-disciplinary working.
Avoid unnecessary admissions to hospital through improved management of long term conditions, embedding new pathways of care developed in 2016/17 and supporting people to return home as quickly as possible after an admission.
Improve the care model for the most vulnerable people in our communities, specifically those in care homes (in line with enhanced health for care homes) and those people within the last year of life to avoid unnecessary admissions.
Reduction in NEL admissions
Reduction in ED attendances
Reduced number of deaths in hospital
Improved resilience in community services
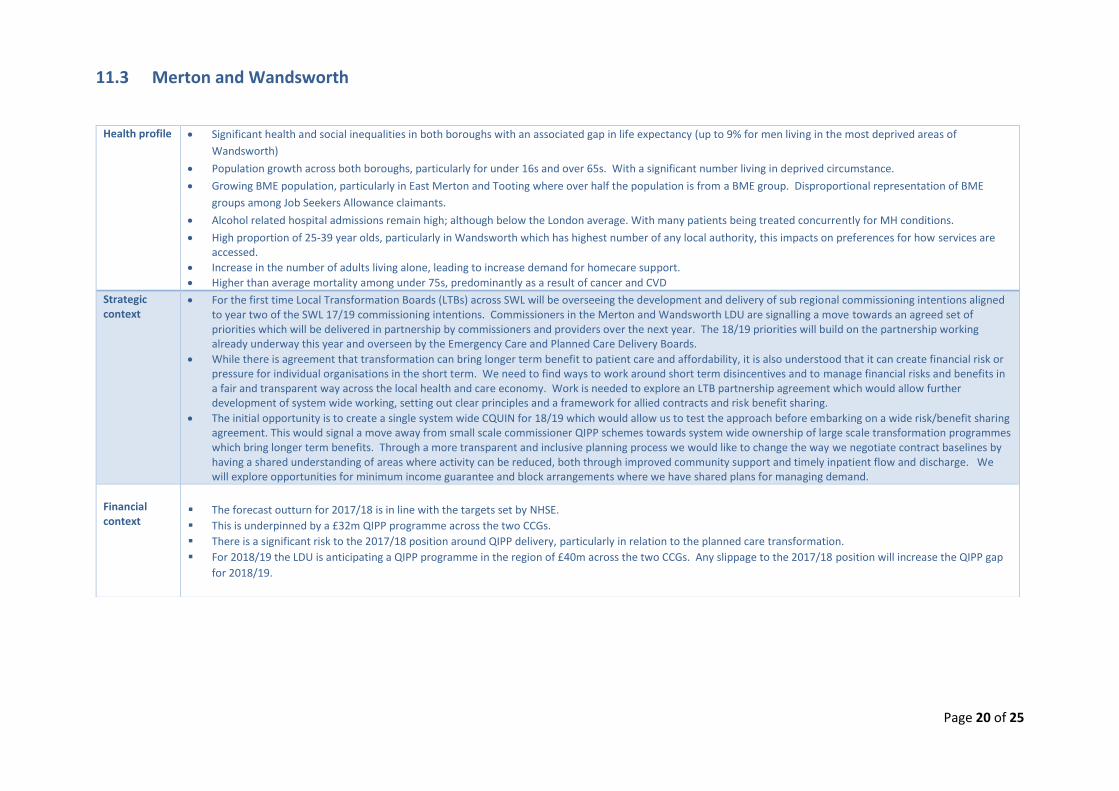
Page 20 of 25
11.3 Merton and Wandsworth
Health profile Significant health and social inequalities in both boroughs with an associated gap in life expectancy (up to 9% for men living in the most deprived areas of
Wandsworth)
Population growth across both boroughs, particularly for under 16s and over 65s. With a significant number living in deprived circumstance.
Growing BME population, particularly in East Merton and Tooting where over half the population is from a BME group. Disproportional representation of BME
groups among Job Seekers Allowance claimants.
Alcohol related hospital admissions remain high; although below the London average. With many patients being treated concurrently for MH conditions.
High proportion of 25-39 year olds, particularly in Wandsworth which has highest number of any local authority, this impacts on preferences for how services are accessed.
Increase in the number of adults living alone, leading to increase demand for homecare support.
Higher than average mortality among under 75s, predominantly as a result of cancer and CVD
Strategic context
For the first time Local Transformation Boards (LTBs) across SWL will be overseeing the development and delivery of sub regional commissioning intentions aligned to year two of the SWL 17/19 commissioning intentions. Commissioners in the Merton and Wandsworth LDU are signalling a move towards an agreed set of priorities which will be delivered in partnership by commissioners and providers over the next year. The 18/19 priorities will build on the partnership working already underway this year and overseen by the Emergency Care and Planned Care Delivery Boards.
While there is agreement that transformation can bring longer term benefit to patient care and affordability, it is also understood that it can create financial risk or pressure for individual organisations in the short term. We need to find ways to work around short term disincentives and to manage financial risks and benefits in a fair and transparent way across the local health and care economy. Work is needed to explore an LTB partnership agreement which would allow further development of system wide working, setting out clear principles and a framework for allied contracts and risk benefit sharing.
The initial opportunity is to create a single system wide CQUIN for 18/19 which would allow us to test the approach before embarking on a wide risk/benefit sharing agreement. This would signal a move away from small scale commissioner QIPP schemes towards system wide ownership of large scale transformation programmes which bring longer term benefits. Through a more transparent and inclusive planning process we would like to change the way we negotiate contract baselines by having a shared understanding of areas where activity can be reduced, both through improved community support and timely inpatient flow and discharge. We will explore opportunities for minimum income guarantee and block arrangements where we have shared plans for managing demand.
Financial context
The forecast outturn for 2017/18 is in line with the targets set by NHSE.
This is underpinned by a £32m QIPP programme across the two CCGs.
There is a significant risk to the 2017/18 position around QIPP delivery, particularly in relation to the planned care transformation.
For 2018/19 the LDU is anticipating a QIPP programme in the region of £40m across the two CCGs. Any slippage to the 2017/18 position will increase the QIPP gap
for 2018/19.
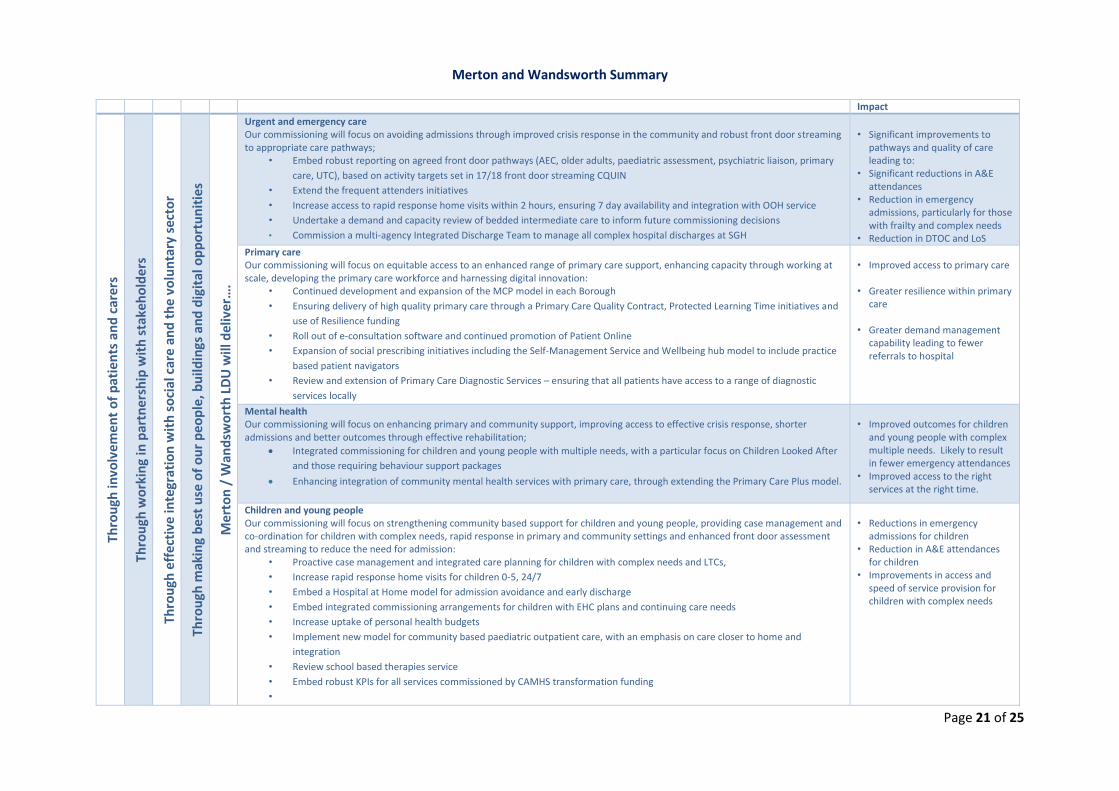
Page 21 of 25
Merton and Wandsworth Summary
Impact Th
rou
gh in
volv
em
en
t o
f p
atie
nts
an
d c
arer
s
Thro
ugh
wo
rkin
g in
par
tne
rsh
ip w
ith
sta
keh
old
ers
Thro
ugh
eff
ecti
ve in
tegr
atio
n w
ith
so
cial
car
e a
nd
th
e v
olu
nta
ry s
ecto
r
Thro
ugh
mak
ing
bes
t u
se o
f o
ur
peo
ple
, bu
ildin
gs a
nd
dig
ital
op
po
rtu
nit
ies
Mer
ton
/ W
and
swo
rth
LD
U w
ill d
eliv
er…
.
Urgent and emergency care Our commissioning will focus on avoiding admissions through improved crisis response in the community and robust front door streaming to appropriate care pathways;
• Embed robust reporting on agreed front door pathways (AEC, older adults, paediatric assessment, psychiatric liaison, primary
care, UTC), based on activity targets set in 17/18 front door streaming CQUIN
• Extend the frequent attenders initiatives
• Increase access to rapid response home visits within 2 hours, ensuring 7 day availability and integration with OOH service
• Undertake a demand and capacity review of bedded intermediate care to inform future commissioning decisions
• Commission a multi-agency Integrated Discharge Team to manage all complex hospital discharges at SGH
• Significant improvements to
pathways and quality of care leading to:
• Significant reductions in A&E attendances
• Reduction in emergency admissions, particularly for those with frailty and complex needs
• Reduction in DTOC and LoS
Primary care Our commissioning will focus on equitable access to an enhanced range of primary care support, enhancing capacity through working at scale, developing the primary care workforce and harnessing digital innovation:
• Continued development and expansion of the MCP model in each Borough
• Ensuring delivery of high quality primary care through a Primary Care Quality Contract, Protected Learning Time initiatives and
use of Resilience funding
• Roll out of e-consultation software and continued promotion of Patient Online
• Expansion of social prescribing initiatives including the Self-Management Service and Wellbeing hub model to include practice
based patient navigators
• Review and extension of Primary Care Diagnostic Services – ensuring that all patients have access to a range of diagnostic
services locally
• Improved access to primary care • Greater resilience within primary
care • Greater demand management
capability leading to fewer referrals to hospital
Mental health Our commissioning will focus on enhancing primary and community support, improving access to effective crisis response, shorter admissions and better outcomes through effective rehabilitation;
Integrated commissioning for children and young people with multiple needs, with a particular focus on Children Looked After
and those requiring behaviour support packages
Enhancing integration of community mental health services with primary care, through extending the Primary Care Plus model.
• Improved outcomes for children
and young people with complex multiple needs. Likely to result in fewer emergency attendances
• Improved access to the right services at the right time.
Children and young people Our commissioning will focus on strengthening community based support for children and young people, providing case management and co-ordination for children with complex needs, rapid response in primary and community settings and enhanced front door assessment and streaming to reduce the need for admission:
• Proactive case management and integrated care planning for children with complex needs and LTCs,
• Increase rapid response home visits for children 0-5, 24/7
• Embed a Hospital at Home model for admission avoidance and early discharge
• Embed integrated commissioning arrangements for children with EHC plans and continuing care needs
• Increase uptake of personal health budgets
• Implement new model for community based paediatric outpatient care, with an emphasis on care closer to home and
integration
• Review school based therapies service
• Embed robust KPIs for all services commissioned by CAMHS transformation funding
•
• Reductions in emergency
admissions for children • Reduction in A&E attendances
for children • Improvements in access and
speed of service provision for children with complex needs
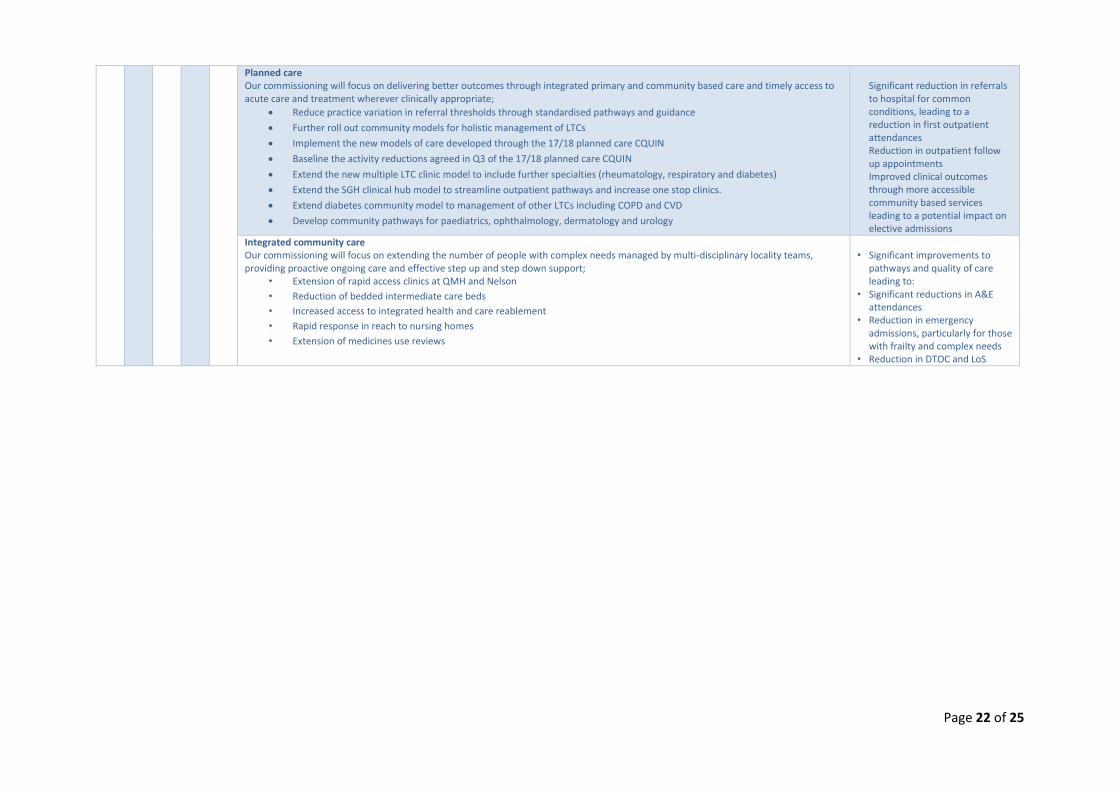
Page 22 of 25
Planned care Our commissioning will focus on delivering better outcomes through integrated primary and community based care and timely access to acute care and treatment wherever clinically appropriate;
Reduce practice variation in referral thresholds through standardised pathways and guidance
Further roll out community models for holistic management of LTCs
Implement the new models of care developed through the 17/18 planned care CQUIN
Baseline the activity reductions agreed in Q3 of the 17/18 planned care CQUIN
Extend the new multiple LTC clinic model to include further specialties (rheumatology, respiratory and diabetes)
Extend the SGH clinical hub model to streamline outpatient pathways and increase one stop clinics.
Extend diabetes community model to management of other LTCs including COPD and CVD
Develop community pathways for paediatrics, ophthalmology, dermatology and urology
Significant reduction in referrals to hospital for common conditions, leading to a reduction in first outpatient attendances Reduction in outpatient follow up appointments Improved clinical outcomes through more accessible community based services leading to a potential impact on elective admissions
Integrated community care Our commissioning will focus on extending the number of people with complex needs managed by multi-disciplinary locality teams, providing proactive ongoing care and effective step up and step down support;
• Extension of rapid access clinics at QMH and Nelson
• Reduction of bedded intermediate care beds
• Increased access to integrated health and care reablement
• Rapid response in reach to nursing homes
• Extension of medicines use reviews
• Significant improvements to
pathways and quality of care leading to:
• Significant reductions in A&E attendances
• Reduction in emergency admissions, particularly for those with frailty and complex needs
• Reduction in DTOC and LoS
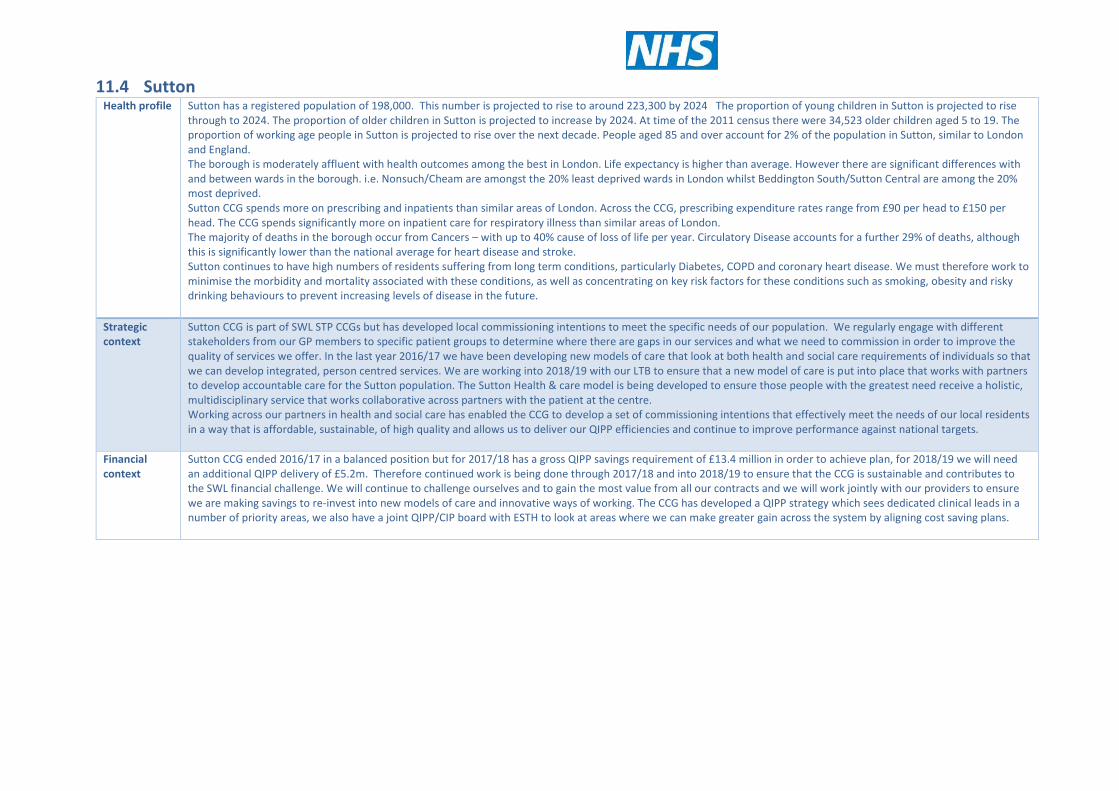
11.4 Sutton Health profile Sutton has a registered population of 198,000. This number is projected to rise to around 223,300 by 2024 The proportion of young children in Sutton is projected to rise
through to 2024. The proportion of older children in Sutton is projected to increase by 2024. At time of the 2011 census there were 34,523 older children aged 5 to 19. The proportion of working age people in Sutton is projected to rise over the next decade. People aged 85 and over account for 2% of the population in Sutton, similar to London and England. The borough is moderately affluent with health outcomes among the best in London. Life expectancy is higher than average. However there are significant differences with and between wards in the borough. i.e. Nonsuch/Cheam are amongst the 20% least deprived wards in London whilst Beddington South/Sutton Central are among the 20% most deprived. Sutton CCG spends more on prescribing and inpatients than similar areas of London. Across the CCG, prescribing expenditure rates range from £90 per head to £150 per head. The CCG spends significantly more on inpatient care for respiratory illness than similar areas of London. The majority of deaths in the borough occur from Cancers – with up to 40% cause of loss of life per year. Circulatory Disease accounts for a further 29% of deaths, although this is significantly lower than the national average for heart disease and stroke. Sutton continues to have high numbers of residents suffering from long term conditions, particularly Diabetes, COPD and coronary heart disease. We must therefore work to minimise the morbidity and mortality associated with these conditions, as well as concentrating on key risk factors for these conditions such as smoking, obesity and risky drinking behaviours to prevent increasing levels of disease in the future.
Strategic context
Sutton CCG is part of SWL STP CCGs but has developed local commissioning intentions to meet the specific needs of our population. We regularly engage with different stakeholders from our GP members to specific patient groups to determine where there are gaps in our services and what we need to commission in order to improve the quality of services we offer. In the last year 2016/17 we have been developing new models of care that look at both health and social care requirements of individuals so that we can develop integrated, person centred services. We are working into 2018/19 with our LTB to ensure that a new model of care is put into place that works with partners to develop accountable care for the Sutton population. The Sutton Health & care model is being developed to ensure those people with the greatest need receive a holistic, multidisciplinary service that works collaborative across partners with the patient at the centre. Working across our partners in health and social care has enabled the CCG to develop a set of commissioning intentions that effectively meet the needs of our local residents in a way that is affordable, sustainable, of high quality and allows us to deliver our QIPP efficiencies and continue to improve performance against national targets.
Financial context
Sutton CCG ended 2016/17 in a balanced position but for 2017/18 has a gross QIPP savings requirement of £13.4 million in order to achieve plan, for 2018/19 we will need an additional QIPP delivery of £5.2m. Therefore continued work is being done through 2017/18 and into 2018/19 to ensure that the CCG is sustainable and contributes to the SWL financial challenge. We will continue to challenge ourselves and to gain the most value from all our contracts and we will work jointly with our providers to ensure we are making savings to re-invest into new models of care and innovative ways of working. The CCG has developed a QIPP strategy which sees dedicated clinical leads in a number of priority areas, we also have a joint QIPP/CIP board with ESTH to look at areas where we can make greater gain across the system by aligning cost saving plans.
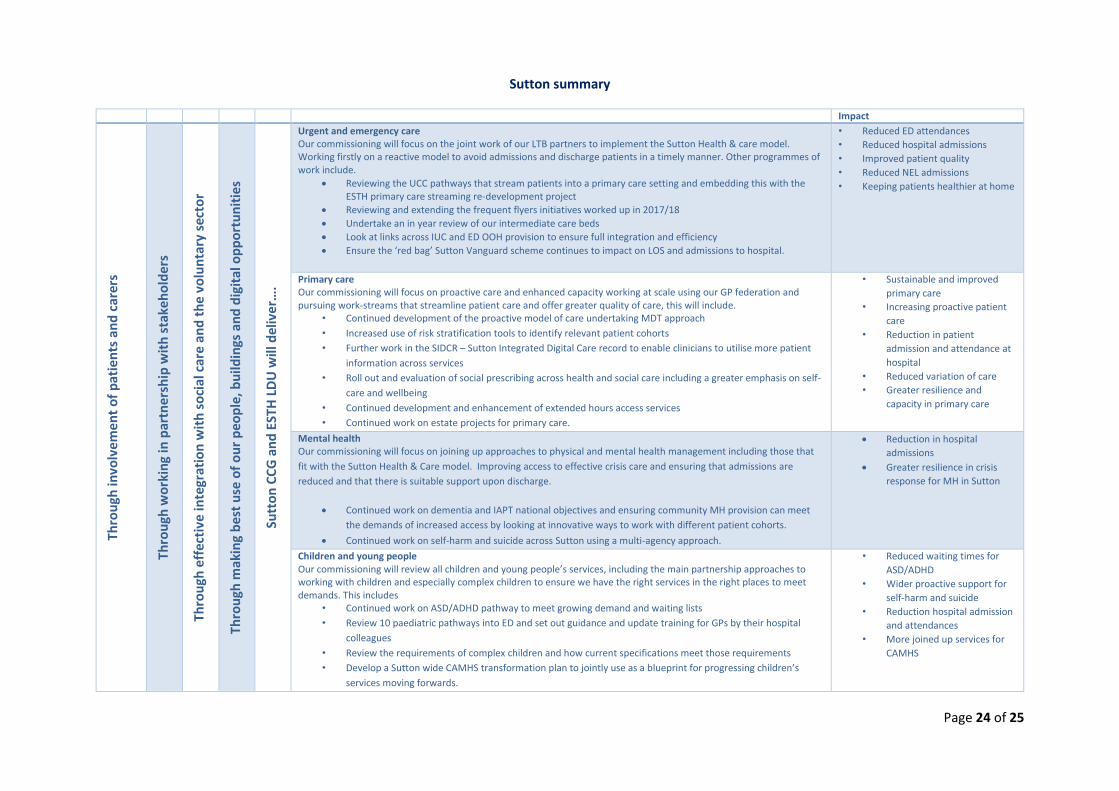
Page 24 of 25
Sutton summary
Impact Th
rou
gh in
volv
em
en
t o
f p
atie
nts
an
d c
arer
s
Thro
ugh
wo
rkin
g in
par
tne
rsh
ip w
ith
sta
keh
old
ers
Thro
ugh
eff
ecti
ve in
tegr
atio
n w
ith
so
cial
car
e a
nd
th
e v
olu
nta
ry s
ecto
r
Thro
ugh
mak
ing
bes
t u
se o
f o
ur
peo
ple
, bu
ildin
gs a
nd
dig
ital
op
po
rtu
nit
ies
Sutt
on
CC
G a
nd
EST
H L
DU
will
del
ive
r….
Urgent and emergency care Our commissioning will focus on the joint work of our LTB partners to implement the Sutton Health & care model. Working firstly on a reactive model to avoid admissions and discharge patients in a timely manner. Other programmes of work include.
Reviewing the UCC pathways that stream patients into a primary care setting and embedding this with the ESTH primary care streaming re-development project
Reviewing and extending the frequent flyers initiatives worked up in 2017/18
Undertake an in year review of our intermediate care beds
Look at links across IUC and ED OOH provision to ensure full integration and efficiency
Ensure the ‘red bag’ Sutton Vanguard scheme continues to impact on LOS and admissions to hospital.
• Reduced ED attendances
• Reduced hospital admissions
• Improved patient quality
• Reduced NEL admissions
• Keeping patients healthier at home
Primary care Our commissioning will focus on proactive care and enhanced capacity working at scale using our GP federation and pursuing work-streams that streamline patient care and offer greater quality of care, this will include.
• Continued development of the proactive model of care undertaking MDT approach
• Increased use of risk stratification tools to identify relevant patient cohorts
• Further work in the SIDCR – Sutton Integrated Digital Care record to enable clinicians to utilise more patient
information across services
• Roll out and evaluation of social prescribing across health and social care including a greater emphasis on self-
care and wellbeing
• Continued development and enhancement of extended hours access services
• Continued work on estate projects for primary care.
• Sustainable and improved
primary care
• Increasing proactive patient
care
• Reduction in patient
admission and attendance at
hospital
• Reduced variation of care
• Greater resilience and
capacity in primary care
Mental health Our commissioning will focus on joining up approaches to physical and mental health management including those that
fit with the Sutton Health & Care model. Improving access to effective crisis care and ensuring that admissions are
reduced and that there is suitable support upon discharge.
Continued work on dementia and IAPT national objectives and ensuring community MH provision can meet
the demands of increased access by looking at innovative ways to work with different patient cohorts.
Continued work on self-harm and suicide across Sutton using a multi-agency approach.
Reduction in hospital
admissions
Greater resilience in crisis
response for MH in Sutton
Children and young people Our commissioning will review all children and young people’s services, including the main partnership approaches to working with children and especially complex children to ensure we have the right services in the right places to meet demands. This includes
• Continued work on ASD/ADHD pathway to meet growing demand and waiting lists
• Review 10 paediatric pathways into ED and set out guidance and update training for GPs by their hospital
colleagues
• Review the requirements of complex children and how current specifications meet those requirements
• Develop a Sutton wide CAMHS transformation plan to jointly use as a blueprint for progressing children’s
services moving forwards.
• Reduced waiting times for
ASD/ADHD
• Wider proactive support for
self-harm and suicide
• Reduction hospital admission
and attendances
• More joined up services for
CAMHS
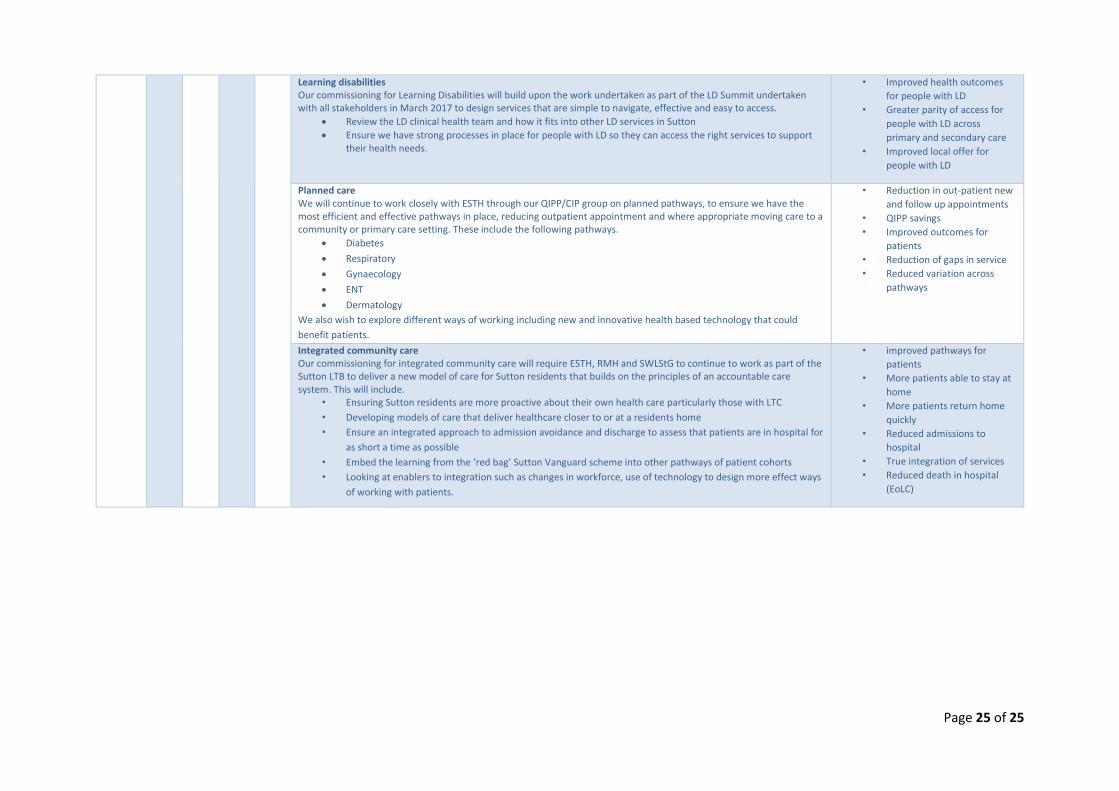
Page 25 of 25
Learning disabilities Our commissioning for Learning Disabilities will build upon the work undertaken as part of the LD Summit undertaken with all stakeholders in March 2017 to design services that are simple to navigate, effective and easy to access.
Review the LD clinical health team and how it fits into other LD services in Sutton
Ensure we have strong processes in place for people with LD so they can access the right services to support their health needs.
• Improved health outcomes
for people with LD
• Greater parity of access for
people with LD across
primary and secondary care
• Improved local offer for
people with LD
Planned care We will continue to work closely with ESTH through our QIPP/CIP group on planned pathways, to ensure we have the most efficient and effective pathways in place, reducing outpatient appointment and where appropriate moving care to a community or primary care setting. These include the following pathways.
Diabetes
Respiratory
Gynaecology
ENT
Dermatology
We also wish to explore different ways of working including new and innovative health based technology that could
benefit patients.
• Reduction in out-patient new
and follow up appointments
• QIPP savings
• Improved outcomes for
patients
• Reduction of gaps in service
• Reduced variation across
pathways
Integrated community care Our commissioning for integrated community care will require ESTH, RMH and SWLStG to continue to work as part of the Sutton LTB to deliver a new model of care for Sutton residents that builds on the principles of an accountable care system. This will include.
• Ensuring Sutton residents are more proactive about their own health care particularly those with LTC
• Developing models of care that deliver healthcare closer to or at a residents home
• Ensure an integrated approach to admission avoidance and discharge to assess that patients are in hospital for
as short a time as possible
• Embed the learning from the ‘red bag’ Sutton Vanguard scheme into other pathways of patient cohorts
• Looking at enablers to integration such as changes in workforce, use of technology to design more effect ways
of working with patients.
• improved pathways for
patients
• More patients able to stay at
home
• More patients return home
quickly
• Reduced admissions to
hospital
• True integration of services
• Reduced death in hospital
(EoLC)
Version: Final D - 1 Date: 31 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Healthy London Partnership Update
Agenda Item 9 Attachment
D
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Healthy London Partnership
Presented by: (name & job title)
Susan Harrison, Head of London Homeless Health Programme
Summary and purpose of report The purpose of the report is to give the Governing Body an overview of the following:
The role of HLP HLP’s achievements to date HLP’s relationship with CCGs and STPs What once for London looks like
Key sections for particular note The Governing Body is asked note the following sections:
Page 6 – Governance Section 2 – Highlights 2016/17
Report recommendation The Governing Body is asked to note the contents of the report. Financial and / or resource implications Kingston CCG contributed £255k in 2017/18. Contributions for 2018/19 are currently being reviewed. Key risks identified & mitigation If funding in future years is not secured, the initiatives being taken forward by HLP could be at risk.
Version: Final D - 2 Date: 31 10 17
Equality and / or privacy impact analysis HLP will complete equality and/or privacy impact analysis for each initiative it takes forward. Committees that have previously discussed / agreed the report and outcomes None. Communication plan / stakeholder involvement / patient engagement HLP has a comprehensive communication plan in place. Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? No. CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement

Supported by and delivering for:
London’s NHS organisations include all of London’s CCGs, NHS England and Health Education England
Healthy London Partnership
Working together to make London the healthiest city in the world
01
Transforming London’s health and care together
Introduction
2
Who are we?
Healthy London Partnership
3
Collaborative
Aspirational
Strategic
Innovative
• Formed in May 2015 as a collaboration between London’s 32 CCGs and NHS England (London Region)
• Funded annually by CCGs and NHS England (London Region)
• To deliver the Five Year Forward View and Better Health for London
• We work to deliver the things best done once for London
• We believe that collectively we can make London the healthiest global city in the world.
What do we do?
We work to deliver the changes best done once for London to make the vision of the NHS Five Year Forward View and Better Health for London a reality.
We also support the delivery of the sustainability and transformation plans in the five areas across London with strategic advice, resources and staff embedded in the areas. We:
• Work across London to deliver on national, London and local aspirations aiming to make London the healthiest city in the world
• Bring together political drive, academic research, clinical and managerial expertise, and delivery networks to make sure change is taken forward at every level
• Attract additional funding to London for transformation work – in 2017/18 London will benefit from up to £18 million of extra funding
• Horizon scan, summarise and share best practice, data and policy to make sure London’s health and care system has access to the most up to date information
• Bring together and facilitate London wide networks to build consistent guidelines and standards of care so all Londoners have access to the best possible health and care services
• Work on once for London projects where this is the most efficient and economic model for improving health and care for Londoners
• Facilitate evaluation and learning across the entire health and care system; benchmarking information and building capacity and capability for delivering change locally.
4
Why do we do it?
Health challenges affecting Londoners
5
• One-year cancer survival rates vary significantly across London, Londoners don’t know how to spot the signs and symptoms of cancer and screening uptake is low
• Children and young people in London have higher levels of mortality and serious illness and higher levels of childhood obesity than any other global city
• People with severe mental illness die 17 years earlier than the general population
• Only 14% of Londoners get the support they need in a mental health crisis
• London has the highest demand for child and adult mental health services in the country
• People who are homeless have a life expectancy of only 43-47 years, are more afflicted with mental ill health and are very high users of hospital services
• Three quarters of Londoners with several long term conditions say each condition is treated separately rather than holistically
• More than half of adults in London are overweight or obese and 1.8 million adult Londoners report they do less than 30 minutes moderately intense physical activity each week
• Only 50 per cent of Londoners think it’s easy to access GP services
• 500 lives could be saved if weekend care were the same as during the week
• Patients are still defaulting to A&E due to confusion in the current system
• NHS organisations in London can’t share patient records across artificial geographical boundaries
• Many qualified professionals leave London for a number of reasons including the high cost of living
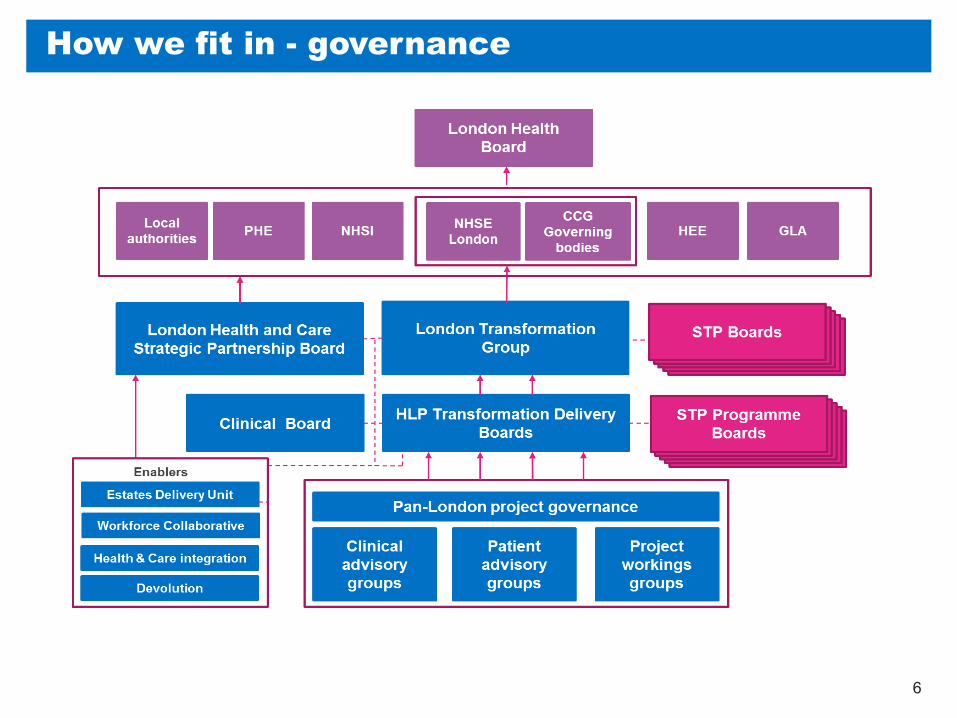
How we fit in - governance
6
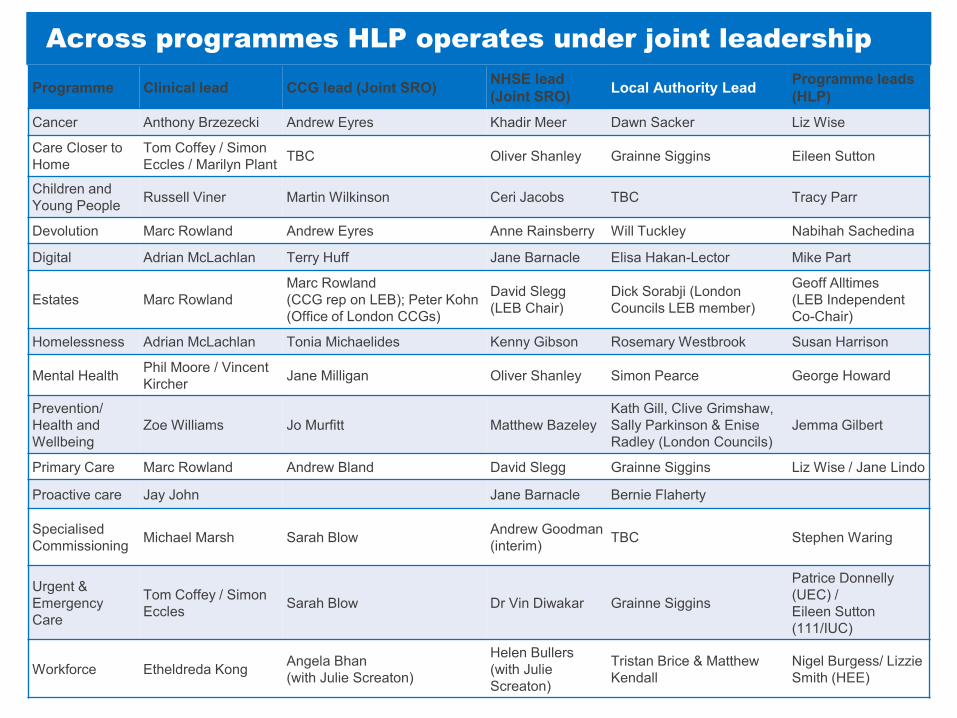
Across programmes HLP operates under joint leadership
7
Programme Clinical lead CCG lead (Joint SRO) NHSE lead (Joint SRO) Local Authority Lead Programme leads
(HLP)
Cancer Anthony Brzezecki Andrew Eyres Khadir Meer Dawn Sacker Liz Wise
Care Closer to Home
Tom Coffey / Simon Eccles / Marilyn Plant TBC Oliver Shanley Grainne Siggins Eileen Sutton
Children and Young People Russell Viner Martin Wilkinson Ceri Jacobs TBC Tracy Parr
Devolution Marc Rowland Andrew Eyres Anne Rainsberry Will Tuckley Nabihah Sachedina
Digital Adrian McLachlan Terry Huff Jane Barnacle Elisa Hakan-Lector Mike Part
Estates Marc Rowland Marc Rowland (CCG rep on LEB); Peter Kohn (Office of London CCGs)
David Slegg (LEB Chair)
Dick Sorabji (London Councils LEB member)
Geoff Alltimes (LEB Independent Co-Chair)
Homelessness Adrian McLachlan Tonia Michaelides Kenny Gibson Rosemary Westbrook Susan Harrison
Mental Health Phil Moore / Vincent Kircher Jane Milligan Oliver Shanley Simon Pearce George Howard
Prevention/ Health and Wellbeing
Zoe Williams Jo Murfitt Matthew Bazeley Kath Gill, Clive Grimshaw, Sally Parkinson & Enise Radley (London Councils)
Jemma Gilbert
Primary Care Marc Rowland Andrew Bland David Slegg Grainne Siggins Liz Wise / Jane Lindo
Proactive care Jay John Jane Barnacle Bernie Flaherty
Specialised Commissioning Michael Marsh Sarah Blow Andrew Goodman
(interim) TBC Stephen Waring
Urgent & Emergency Care
Tom Coffey / Simon Eccles Sarah Blow Dr Vin Diwakar Grainne Siggins
Patrice Donnelly (UEC) / Eileen Sutton (111/IUC)
Workforce Etheldreda Kong Angela Bhan (with Julie Screaton)
Helen Bullers (with Julie Screaton)
Tristan Brice & Matthew Kendall
Nigel Burgess/ Lizzie Smith (HEE)
Us and STPs
8
• Since we were established STPs have emerged as local ‘structures’ with a formal role in the delivery of transformation.
• In light of this, in June 2016 the London Transformation Group agreed an in-depth
review of activity needed to transform the whole system so the partnership could develop in the right direction.
• During engagement with stakeholders there was broad acknowledgement that a
transformation resource on a London level is beneficial and getting activity and the interface with STPs right was critical.
• Recommendation that three functions should be done on a London level:
• Healthy London Partnership to prioritise resources and activity to move from planning to delivery – bespoke plans and evidence were developed for each STP footprint to support planning
Horizon scanning function looking at new emerging
priorities
Products and support that are best done once for London
Embedded resource in STPs that links back to London level
work

How do we engage and involve Londoners?
9
02
Transforming London’s health and care together
Highlights 2016/17
10
Things we’ve made happen in 2016/17
11
• New technology we’ve led the development on and implemented means Londoners calling NHS 111 with care plans and crisis information can now be directed to a clinician who can see their information in real time helping them make the right clinical decision and making sure callers are referred to the right service, first time. The technology has already won several awards including the prestigious UK IT Industry Award for best use of cloud services.
• Mayor of London, Sadiq Khan launched London’s section 136 pathway and Health based Place of Safety specification, following extensive engagement across London’s crisis care system. Engagement with over 300 service users, mental health and acute trusts, LAS, local authorities and London’s three police forces. This resulted in formal endorsement from these agencies as well as the Royal College of Psychiatry and National Crisis Care Concordat.

Things we’ve made happen in 2016/17
12
• London has launched the first mental health dashboard in the world. This will help the health and care system improve mental health services for Londoners by having access to up to date information. The dashboard will help providers and commissioners benchmark performance and improve and transform services.
• 67% of children attending A&E could have been seen by a GP. London’s young people helped us design and launch a mobile app called NHS Go downloaded by over 40,000 people already, giving them targeted health information plus health advice and signposting to services.
• More than 40 NHS organisations and around 100,000 NHS employees in London took part in Healthy Living Week. Over 250 events took place across London, we led this with NHS Trusts and the London NHS Charities Group.
Highlights 16/17
13
• 220,000 Londoners now survive cancer. We have developed the pathway and tools for treating cancer as a long term condition in GP practices covering psycho-social and physical needs, the needs of carers and support for patients to improve their health and their experience of the NHS.
• Our Early Intervention in Psychosis team supported the mental health system with the new psychosis target and developed a range of materials to support GPs if they suspect someone may be experiencing a first episode of psychosis.
• Three children in every classroom has asthma. NHS services in London are working towards the aim of ‘no child dies from asthma’ by improving asthma care for all children and young people. The London Asthma Toolkit for GPs, pharmacists hospital clinicians, schools and parents officially launched at the British Thoracic Society’s winter symposium in December
• Our evaluation of a GP led service in Croydon for men with prostate cancer, showed that it is better value for money and improves the patient’s experience. Four areas in London (south east, south west, north central and north west) are now going to roll out this service which will benefit over 3,000 men.
• The Transforming Primary Care team have successfully negotiated with the national team on behalf of London’s CCGs to secure agreement to spend the allocated £25.4m of GP Access Monies this year (and next) to spread the offer across London to serve a greater population (9m patients) as opposed to national allocation for pilot areas only.
Highlights 16/17
14
• Homeless people are eight times more likely to go to A&E than other Londoners. 20,000 cards were sent out to homeless centres in London which along with the training we’ve designed for frontline staff means that people who are homeless or sleeping rough can use GP services when they need them rather than waiting until they are so ill they go to A&E.
• Through our partnership working, all 32 CCGs, all 33 borough councils, the Mayor of London, NHS England and Public Health England signed a London Health and Care Collaboration Agreement and London Devolution Agreement in 2015. This paves the way for central government and national bodies to devolve powers and funding to London to support local, sub-regional and London-wide transformation. In 2017, central government announced their commitment to a further London health and care devolution agreement.
• In a trial with professional football clubs like Spurs, Brentford and Fulham FC, 77 men who started off overweight or inactive lost a combined weight of 244kg via the Fanactiv project which we are now extending, showing how working locally where Londoners are is how you can bring about the biggest changes.
03
Transforming London’s health and care together
What does once for London
look like?
15
Case study: Mental health crisis care
Bringing an entire system together to improve care for the most vulnerable Londoners
16
Around 5,000 Londoners will be detained under section 136 and taken to one of London’s 20 health based places of safety or A&E each year. However, the care people receive when they are detained and the standards of these places of safety vary across London. It makes sense to take a once for London approach to improving care and so far we have:
• Developed a pan-London pathway for section 136
• Published a specification for health based place of safety sites
We are now working with CCGs, trusts and other key partners to implement the new model of care.
https://www.youtube.com/watch?v=um9fz2AubAk
Case study: Great Weight Debate
Mobilising partners and investment to make change happen on a London level?
17
Two out of five children starting secondary school are already overweight or obese.
We worked with the London Obesity Leadership Group, Public Health England, London Councils and borough obesity leads to raise awareness of childhood obesity and seek ideas from Londoners on what would help young people in London lead healthier lives.
The Great Weight Debate reached over half a million Londoners on social media, saw 3,900 people fill in our survey, nearly 2,000 people attend roadshows and culminated in 60 teenagers working through the issues at a Hackathon at City Hall, raising awareness of the issue of childhood obesity in London and creating a strategy for change in the London boroughs.
https://www.youtube.com/watch?v=sNTYwqWj5CI
Case study: Improving health of homeless people
Raising standards by pooling resources
18
Hundreds of people are homeless in London every night. They represent a small portion of the population and often move around London, experiencing varied care and outcomes – this is why we are taking a once for London approach to improving care.
After engaging with over 100 organisations and individuals, including every London CCG and more than 90 people with experience of homelessness: we have developed:
• Commissioning guide for CCGs
• Online training package for GP receptionists and practice managers
• ‘My right to access health services’ card for people who are homeless
https://www.youtube.com/watch?v=5QuBzaEUuh0
What next?
19
• Each STP has been assigned a lead from the partnership to work with, to provide support and ensure a clear route of communication and joined up working between the footprint area and London level.
• Joint membership across STP programme boards and partnership transformation delivery boards to also ensure clear communications and interface between London and boroughs.
• Embedded Healthy London Partnership staff working in STPs across a wide variety of programmes linking London level work with sector level work to support delivery.
• Supporting the Mayor of London's new citywide movement to improve mental health and wellbeing in the capital. Thrive LDN aims to encourage Londoners to step up to tackle mental health so that every person in London can live happier, healthier lives.
• Setting up the Urgent and Emergency Care Improvement Collaborative to work with staff and leaders across urgent and emergency care, and out of hospital care to define what the future support for improvement across London needs to address.
• Work is well underway on the London Health and Care Information Exchange which aims to join up NHS organisations across London. The exchange aims to give NHS clinicians secure access to real-time patient records and information.

05
Questions?
20
Version: Final E - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Kingston & Richmond Local Transformation Board (LTB) Update
Agenda Item 10 Attachment
E
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Tonia Michaelides, Managing Director, Kingston & Richmond CCGs
Presented by: (name & job title)
Tonia Michaelides, Managing Director, Kingston & Richmond CCGs
Summary and purpose of report The purpose of this report is to provide an update on the progress of the Kingston & Richmond Local Transformation Board with a focus on:
Membership Work to date Contribution to the SWL Sustainability and Transformation Partnership (STP) refresh
Key sections for particular note The Governing Body are asked to note the following sections:
Section 3 – Membership Section 4 – Governance Section 6 – SWL STP refresh
Report recommendation The Governing Body is asked to note the contents of the report and to agree the frequency of ongoing updates. Financial and / or resource implications There are resource implications to supporting the Local Transformation Board (LTB). These are currently being scoped. Key risks identified & mitigation
Version: Final E - 2 Date: 30 10 17
None outside the risks such as the financial challenge across the system going forward next year and the risks associated with delivery transformation at scale. Equality and / or privacy impact analysis Equality and privacy impact analysis will be completed for each LTB initiative as appropriate. Committees that have previously discussed / agreed the report and outcomes None. Communication plan / stakeholder involvement / patient engagement The LTB has a communication and PPI working group that is developing a communication plan. Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? No further assurance required. CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
Version: Final E - 3 Date: 30 10 17
Update on the Kingston and Richmond Local Transformation Board 1. Introduction
The South West London Sustainability and Transformation Partnership (STP) recognises that a local approach works best. The NHS is working jointly with Local Authorities and local people within boroughs to plan care based on people’s health and care needs. To achieve this ambition the SWL STP has established an approach to planning and developing care for health and care in the following partnership areas.
Kingston and Richmond Sutton Croydon Merton and Wandsworth
To support these partnership areas Local Transformation Boards (LTB) have been established. The purpose of this paper is to update the Governing Body on the establishment of the Kingston and Richmond LTB. 2. Purpose of the Kingston and Richmond Local Transformation Board
Kingston and Richmond LTB has been established to provide oversight and direction to the development of place-based level implementation plans which will deliver significant change in health and care systems. The LTB will expedite the design and delivery of these plans by bringing together key local organisations for agreement including contracting, reporting and financial issues. The responsibilities of the Transformation Board include;
Providing oversight of, and direction to, the local design and delivery of the SWL STP through local place- based implementation plans, and to be accountable to the SWL STP Programme Board for delivery.
Providing oversight of, and direction to, the delivery of the national ‘must do’s’ and the deliverables identified in the next steps of the NHS Five Year Forward View.
Bringing together local partners into one place, working collaboratively to expedite the delivery of the STP, which will be the responsibility of local place-based implementation plans.
Version: Final E - 4 Date: 30 10 17
3. Membership
The LTB has core representation at clinical and managerial level from CCGs, Local Authorities, Acute, Community Health, GP Federations, Healthwatch and Voluntary sector organisations. The full membership list of the Kingston and Richmond LTB is given on page 4 of the Terms of Reference which are attached as Appendix 1 of this report From December 2017 the LTB will be chaired by a GP commissioning leader. At the time of writing this paper the Chair has not been determined. 4. Governance
It is important to ensure that the LTB is appropriately reflected in the governance of the Kingston and Richmond system. Appendix 2 of this paper shows at a high level where the Local Transformation Board sits within the local governance structure. As the work plan of the LTB is developed the role of the LTB in decision making will need to be reviewed to ensure that it can support decision making at pace to expedite the delivery of the LTB’s transformation plans. 5. Work of the Kingston and Richmond Local Transformation Board to date
Below is a summary of the work completed by the LTB to date:
A refresh of the bed audit that took place in February 2016 to include all medical and community beds
Modelling is underway focussing on establishing how to achieve financial and clinical sustainability across the LTB
Developing a governance structure that incorporates all statutory organisations which will develop into a formal Memorandum of Understanding
Beginning to explore how Accountable Care could work across the Kingston and Richmond LTB.
In both Kingston and Richmond the locality model has been developed and is being rolled out across the 2 CCGs.
6. SWL STP Refresh
As part of the SWL STP refresh the Kingston and Richmond LTB will be focusing on developing the following areas:
Version: Final E - 5 Date: 30 10 17
The model for health and care across Kingston and Richmond The continued involvement of patients and residents The focus for the next 2 years to address the context and challenges across
Kingston and Richmond Metrics for success
7. Recommendation
The Governing Body is asked to note the contents of the report. Regular reports on the progress and work of the Kingston and Richmond LTB will be presented to future Governing Body meetings.
Page 1 of 7
GB 07 11 17
Att E1
Kingston Richmond and East Elmbridge Local Transformation
Board: Terms of Reference
(DRAFT)
Page 2 of 7
Document Creation
Document Revision History Revision date Author(s) Change summary Version
05/05/17 Tonia Michaelides Update of membership and alignment to SWL STP governance
0.2
Approvals
This document requires the following approvals before finalisation:
Name and position/group Date approved Version
K&R Local Transformation Board
Date Author(s) Role Version
04/01/17 Greg Penlington Asst. Dir., SWL Collaborative Commissioning 0.1
Page 3 of 7
Contents
1. Purpose and Remit .................................................................................... 4
2. Board Membership ................................................................................... 4
3. Responsibilities ......................................................................................... 5
4. Key Principles ............................................................................................ 5
5. Accountability ........................................................................................... 5
6. Meetings frequency .................................................................................. 6
7. Quoracy .................................................................................................... 6
8. Support ..................................................................................................... 6
9. Conflicts of interest ................................................................................... 6
10. Review of Terms of Reference .................................................................. 7
Page 4 of 7
1. Purpose and Remit
The Transformation Board has been established to drive forward the transformation of the health and social care system in Kingston Richmond and East Elmbridge through the local delivery of the South West London (SWL) Sustainability and Transformation Partnership (STP).
It will provide oversight and direction to the development of borough-level implementation plans which will deliver significant change in the health and care system. It will expedite the design and delivery of these plans by bringing together key local organisations in one place and facilitating key areas for agreement including contracting, reporting, and financial issues.
In doing so the Board will ensure the alignment of local plans for delivering transformation and the vision of the STP:
“We want people to live longer, healthier lives. Our vision is that local people should be supported to look after themselves and those they care for and have access to high quality, joined up physical and mental health and care services when they need them. We want to deliver better health outcomes within our budget.”
2. Board Membership
The Transformation Board shall be constituted from senior management or clinical representation from the following organisations:
Kingston Clinical Commissioning Group
Richmond Clinical Commissioning Group
Surrey Downs Clinical Commissioning Group – East Elmbridge Locality
Royal Borough of Kingston-Upon-Thames
London Borough of Richmond-Upon-Thames
Kingston Hospital NHS Foundation Trust
Richmond GP Federation
Kingston GP Federation
South West London and St. George’s Mental Health Trust
Hounslow and Richmond Community Healthcare NHS Trust
YourHealthcare CIC
Chelsea & Westminster Hospital NHS Foundation Trust
Richmond CVS
The Board will be chaired by a CCG GP commissioning leader and SRO for the delivery of the STP in Kingston and Richmond will be the Managing Director of Kingston and Richmond CCGs.
Organisations may send deputies with sufficient decision making powers, should the designated member not be available to ensure that each organisation is suitably represented.
Organisations will have their own local governance arrangements and Transformation Board members will be responsible for ensuring that this is used appropriate to support the Board in delivering its responsibilities.
Members from other organisations, from time to time, may be invited to further discussions in a particular area.
Page 5 of 7
NB: See Appendix A for full membership list
3. Responsibilities
The Kingsto, Richmond and East Elmbridge Local Transformation Board will:
Provide oversight of, and direction to, the local design and delivery of the SWL Sustainability and Transformation Partnership through local borough-based implementation plans, and be accountable to the SWL STP Programme Board for their delivery.
Provided oversight of, and provide direction to the delivery of the national `must dos` and the deliverables identified in the next steps of the NHS Five Year Forward View.
Through bringing together local partners into one place, work collaboratively to expedite the delivery of the STP, which will be the responsibility of local borough-based implementation plans. This includes agreeing:
- Borough-level implementation models;
- Priority areas around which all organisations will commit to achieve a transformed, improved and affordable service; and
- The financial and contractual elements that support the implementation of STP initiatives.
Ensure that risks identified by the Board are managed and notified as required to the individual organisational corporate risk registers, the SWL STP Programme Office, and the SWL STP Programme Board.
Report progress relating to planning, implementation and performance of STP initiatives to the STP Programme Office, as agreed by the STP Programme Board.
4. Key Principles
The key principles underlying the work of the Board will be that people in Kingston and Richmond will:
Be able to access greater preventative and early intervention support to enable them to become more independent and confident in managing their care
Experience greater delivery of joined-up care as a result of increased collaboration between acute, primary, community, mental health and voluntary sector providers in delivering care
Have a consistent quality of care regardless of their GP practice, and improve ability to access more specialised Primary Care services within the community
Be better supported in looking after themselves and staying healthy through greater involvement by the voluntary sector
Have access to improve technology that improves their ability to access necessary services, advice or information relevant for their needs
5. Accountability
The Transformation Board will be accountable to the SWL&SD Programme Board for the progress of its local transformation plans; the SRO for the Transformation Board will be a member of the Programme Board.
Page 6 of 7
Attached as Appendix 1 of this Terms of Reference is a diagram=ram that illustrates where the LTB sits within the local governance structure.
6. Meetings frequency
The Transformation Board will meet every month and will be held on the alternate first Thursday or Friday of the month. A schedule of meetings will be provided for all members of the group.
7. Quoracy
There is no formal requirement for this meeting to be quorate; however it is expected that representatives from organisations (or, where required, their deputies) will attend, and a register of attendance will be taken.
8. Support
Administrative support to the Board will be provided by the Kingston & Richmond CCGs Programme Management Office.
The agenda will be agreed with the Chair and shared, with appropriate supporting papers, at least 3 working days ahead of the meeting
Apologies will be sent in advance to the administrative support.
Notes and actions will be circulated within 3 working days of the meeting
Confidential information will be clearly marked and circulation restricted as necessary.
9. Conflicts of interest
A conflict of interest is where an individual has a direct or indirect pecuniary or non-pecuniary interest in a matter that is being discussed. These can be defined as follows:
A direct pecuniary interest is when an individual may financially benefit from a decision (for example moving services to them from an alternative provider).
An indirect pecuniary interest is when an individually may financially benefit from a decision though normally via a third party (for example where an individual is a partner, member or shareholder in an organisation that will benefit financially from the consequences of a reconfiguration decision).
A direct non-pecuniary interest is where an individual holds a non-remunerative or not-for profit interest in an organisation (for example, where an individual is a trustee of a voluntary provider that is bidding for a contract).
An indirect non-pecuniary interest is when individual may enjoy a qualitative benefit from the consequence of a decision which cannot be given a monetary value (for example, a reconfiguration of hospital services which might result in the closure of a busy clinic next door to an individual’s house).
In addition, where an individual is closely related to, or in a relationship, including friendship, with an individual in the above categories, this will constitute a conflict of interest.
Declarations of interests will be a standing item on the Transformation Board agenda. All members of the group must declare any interests that may arise as a result of this or any other matter being
Page 7 of 7
discussed. All interests will be recorded onto a register of interests held centrally by the Kingston CCG Governance Lead, as well as being recorded in the minutes of the meeting where the interest has been declared.
10. Review of Terms of Reference
The Transformation Board Terms of Reference will be reviewed every six months from the date of approval.
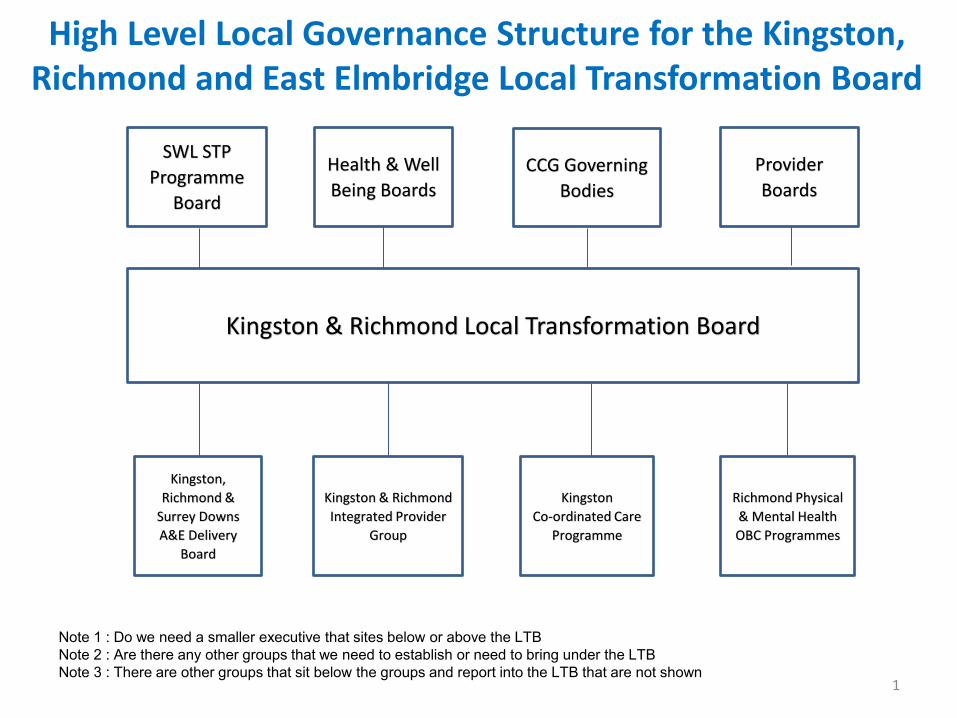
High Level Local Governance Structure for the Kingston, Richmond and East Elmbridge Local Transformation Board
1
Kingston
Co-ordinated Care
Programme
Kingston,
Richmond &
Surrey Downs
A&E Delivery
Board
Richmond Physical
& Mental Health
OBC Programmes
CCG Governing
Bodies
Kingston & Richmond
Integrated Provider
Group
Provider
Boards
Health & Well
Being Boards
Kingston & Richmond Local Transformation Board
SWL STP
Programme
Board
Note 1 : Do we need a smaller executive that sites below or above the LTB Note 2 : Are there any other groups that we need to establish or need to bring under the LTB Note 3 : There are other groups that sit below the groups and report into the LTB that are not shown
Version: Final F- 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Re-provision of Cedars Community and Inpatient Service
Agenda Item 11 Attachment
F
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Sue Lear, Acting Director of Commissioning
Presented by: (name & job title)
Sue Lear, Acting Director of Commissioning
Summary and purpose of report
At the July meeting the governing body supported plans for a temporary short term solution for the re-provision of 25 beds within a dedicated ward at Teddington Memorial Hospital. There will also be enhanced community care provision to support more people within their own homes to support the shortfall in beds.
This paper is presented to the Governing Body to provide an update on progress with the relocation from the Cedars Unit
Key sections for particular note This is a general update covering overarching arrangements, estates and staffing. Report recommendation The Governing Body is asked to note the contents of the report. Financial and / or resource implications There are no financial implications identified. Key risks identified & mitigation A full risk register will be developed by Your Healthcare CIC once a date for the service transfer is known. Equality and / or privacy impact analysis N/A
Version: Final F- 2 Date: 30 10 17
Committees that have previously discussed / agreed the report and outcomes N/A Communication plan / stakeholder involvement / patient engagement The CCG will be meeting with the communications lead at Your Healthcare CIC at the end of October 2017 to discuss their communications plan and to develop a joint engagement plan between the CCG and Your Healthcare in relation to the temporary move, and also to begin discussions about engagement planning around the long-term options Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
Update on the Cedars Unit Re-provision of Inpatient Beds
1.0 Background Your Healthcare CIC (YHC) currently operates a 1300sqm 35-bed facility, Cedars Community and In-Patient Service (Cedars) that provides sub-acute care and rehabilitation in step up and step down beds to prevent admission and support timely hospital discharge. Due to the South West London & St George’s Mental Health Trust (SWL&StG) redevelopment of the Tolworth site, YHC will need to relocate the above provision to another location. At the July meeting the governing body supported plans for a temporary short term solution for the re-provision of 25 beds within a dedicated ward at Teddington Memorial Hospital. There will also be enhanced community care provision to support more people within their own homes to support the shortfall in beds. 2.0 Purpose of the paper This paper is presented to provide an update to the governing body on progress. 3.0 Progress update Since the last update YHC have received formal notice from SWL& St Georges MH Trust solicitors, giving notice to terminate YHC contract on 13th April 2018. This means that YHC will have to have vacated the site by this date.
Version: Final F- 3 Date: 30 10 17
A project group has been established to manage the re-provision of the beds to the Teddington Memorial Hospital (TMH) site. The group meets regularly every 2-3 weeks with the first meeting on 3rd October 2017. YHC and Hounslow and Richmond Community Healthcare Trust (HRCH) have reached an agreement on the funding required to accommodate the beds at Teddington Memorial Hospital. TMH are working with their legal team to produce a lease for the required bed space.
3.1 Estate plans Space for an additional 4 beds is required on the ward area at TMH. The work required to provide this will take 4 weeks and will commence in November. Further service areas being discussed include pharmacy provision, medical supplies contract, potential use of the on-site gym, diagnostics and x-ray provision, along with the IT provision. The YHC project manager is liaising with the SWL facilities lead to develop plans for the decommissioning of the Cedars Unit. 3.2 Staff YHC have taken advice and can confirm that there is no requirement for a formal staff consultation due to the temporary nature of the move whilst permanent premises are secured. A number of communication approaches are being used to ensure that all staff are kept informed of plans and progress. This includes via email, written and verbal updates following the project group meetings. Face to face meetings between senior staff from YHC and HRCH are being held fortnightly to plan for the smooth transition to the new site. An open house event will be arranged for YHC staff to visit the TMH site.
4.0 Recommendation The governing body are asked to note the contents of the report
Version: Final G - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body meeting in public Date 7th November 2017 Report Title
IVF / Fertility Update Agenda Item 12 Attachment
G
Purpose (please indicate with X)
Approval/ Ratification
x Discussion / Comment
Information
Report Author: (name & job title)
Sue Lear Deputy Director of Commissioning
Presented by: (name & job title)
Sue Lear Deputy Director of Commissioning
Summary and purpose of report The CCG recently set out proposals for changing the access criteria for IVF/ICSI within the Choosing Wisely engagement. At the September 2017 Governing Body meeting it was decided that the criteria for access to IVF/ICSI in Kingston would not be changed. As an alternative measure an initial proposal from the consultants at the Assisted Conception Unit (ACU) has suggested changes in access to the fertility pathway, against clinical criteria where the evidence demonstrates a reduction in the successful outcome of fertility treatment Key sections for particular note The proposed fertility pathway section includes the initial criteria Next steps describes the process to be taken Report recommendation The governing body is asked to endorse the approach to jointly review the fertility pathway with the ACU and to consider changes to this pathway based on clinical expectations of successful conception. Financial and / or resource implications To be worked up once the pathway has been agreed Key risks identified & mitigation Risks will be identified once the pathway is agreed Equality and / or privacy impact analysis To be carried out once the pathway is agreed
Version: Final G - 2 Date: 30 10 17
Committees that have previously discussed / agreed the report and outcomes None Communication plan / stakeholder involvement / patient engagement To be developed Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? No CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
Version: Final G - 3 Date: 30 10 17
IVF /Fertility Update for NHS Kingston CCG Governing Body
1.0 Background
NHS Kingston CCG currently funds one fresh cycle and two frozen cycles of IVF/ICSI at the Assisted Conception Unit at Kingston Hospital for women up to their 40th birthday who have received a maximum of two previous self-funded cycles OR women aged 40 up to their 43rd birthday where they have had no previous self-funded cycles.
Although there is NICE Fertility Pathway guidance (CG156), many other CCGs have recently implemented changes to their local policies following local consultations and in effect, reduced the scope and availability of NHS funded specialist assisted conception services as part of their QIPP plans. Nationally, four CCGs do not routinely provide funding for IVF and ICSI for their local populations.
All but one CCG in London offers one cycle of IVF+/-ICSI (NHS Camden CCG offers three cycles). Only NHS Wandsworth CCG in London has extended the age range for treatment to 42 years. NHS Kingston CCG accepts referrals for women up to the age of 42 who have received no previous self-funded cycles. Nationally, a number of CCGs are reducing the provision of IVF cycles to one cycle in order to reduce expenditure or support an increase in the age range. Nationally there is also a variation in the number of frozen embryo transfers that are funded from unlimited down to no embryo transfers funded.
2.0 Proposal for change
The CCG recently set out proposals for changing the access criteria for IVF/ICSI within the Choosing Wisely engagement. At the September governing body it was decided that the criteria for access to IVF/ICSI in Kingston would not be changed. It was discussed whether; further work should be undertaken following a proposal by the clinical team at the Assisted Conception Unit (ACU) to explore the current fertility pathway and to consider the access to fertility services based on the anticipated successful clinical outcomes of fertility treatment. This paper is presented to the governing body to ask for endorsement to explore changes that could be made to the fertility pathway.
3.0 Fertility Pathway The initial proposal from the consultants at the Assisted Conception Unit has suggested changes in access to the fertility pathway, against clinical criteria that the evidence demonstrates reduces the successful outcome of fertility treatment. The initial suggested criteria are:
BMI less than 32 Age limit <42
Version: Final G - 4 Date: 30 10 17
The Assisted Conception Unit are also keen to work with the CCG to streamline the pathway for fertility investigations.
4.0 Next Steps If the governing body supports the re-design of the fertility pathway it is proposed that a clinical meeting is arranged between the ACU consultants and a CCG clinical lead to explore and agree the pathway. This would then be brought back to the governing body for sign off.
5.0 Recommendations
The governing body are asked to: Endorse the approach to jointly review the fertility pathway with the ACU and to consider changes to this pathway based on clinical expectations of successful conception.
Version: Final H - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing body in public Date 7 November 2017 Report Title
Kingston Coordinated Care Update
Agenda Item 13 Attachment H
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Sue Lear, Deputy Director of Commissioning
Presented by: (name & job title)
Sue Lear, Deputy Director of Commissioning
Summary and purpose of report To update the governing body on the development of the new locality model of care known as Kingston Coordinated Care. NHS Kingston CCG has been working with partner organisations to develop a new model of community care provision for the population of the Royal Borough of Kingston. The new model of care has been a multi-agency design piece underpinned by the ‘voice of the customer’ through public engagement to understand the changes required within the system to deliver desired outcomes. A formal provider alliance has been established through a memorandum of understanding between partner agencies. Key sections for particular note The section on the model of care describes the new way of working Progress to date on the 5 workstreams Report recommendation The governing body is asked to note the contents of the report. Financial and / or resource implications This paper does not cover financial or resource implications Key risks identified & mitigation Key risk is lack of impact of the model, this will be evaluated and monitored through the commissioner provider assurance group.
Version: Final H - 2 Date: 30 10 17
Equality and / or privacy impact analysis An equality impact analysis has not yet been carried out. Committees that have previously discussed / agreed the report and outcomes None Communication plan / stakeholder involvement / patient engagement Extensive patient engagement was carried out prior to the development of the new model of care. Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? None CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
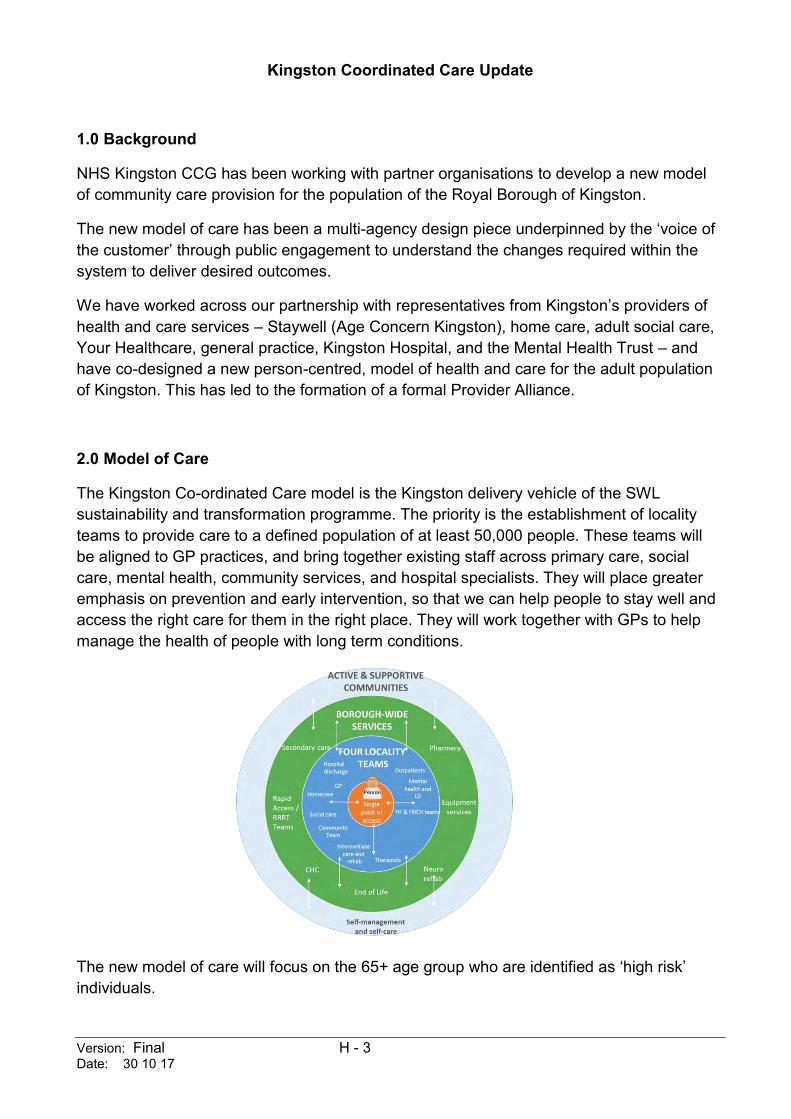
Version: Final H - 3 Date: 30 10 17
Kingston Coordinated Care Update
1.0 Background
NHS Kingston CCG has been working with partner organisations to develop a new model of community care provision for the population of the Royal Borough of Kingston.
The new model of care has been a multi-agency design piece underpinned by the ‘voice of the customer’ through public engagement to understand the changes required within the system to deliver desired outcomes.
We have worked across our partnership with representatives from Kingston’s providers of health and care services – Staywell (Age Concern Kingston), home care, adult social care, Your Healthcare, general practice, Kingston Hospital, and the Mental Health Trust – and have co-designed a new person-centred, model of health and care for the adult population of Kingston. This has led to the formation of a formal Provider Alliance.
2.0 Model of Care
The Kingston Co-ordinated Care model is the Kingston delivery vehicle of the SWL sustainability and transformation programme. The priority is the establishment of locality teams to provide care to a defined population of at least 50,000 people. These teams will be aligned to GP practices, and bring together existing staff across primary care, social care, mental health, community services, and hospital specialists. They will place greater emphasis on prevention and early intervention, so that we can help people to stay well and access the right care for them in the right place. They will work together with GPs to help manage the health of people with long term conditions.
The new model of care will focus on the 65+ age group who are identified as ‘high risk’ individuals.
Version: Final H - 4 Date: 30 10 17
Locality Teams will focus on the population most at risk of admission to hospital, and these patients will be identified through Risk Stratification via patient segmentation. When health care is delivered in a ‘one size fits all’ approach it is not reflective of individual needs. Patient segmentation offers an approach to ensure that service design is responsive to the local population. The model will enable people with complex health and social care needs to be reviewed and managed by a multi-disciplinary team (MDT) and care tailored to the individual’s needs.
3.0 Progress to date
Progress is reported against the 5 work-streams.
New Model of Care
First round of MDTs has taken place in New Malden
Task and Finish groups established for key deliverable areas of the locality model
Collaborative triage and screening function put in place, looking at further opportunities to reduce duplication and work together more closely. Early work has greatly reduced the level of people passed between Providers
Discussions on implementing well-being teams have commenced to gain committee approval for the establishment of wellbeing teams to deliver home care in Kingston
Patient segmentation has been limited as until recently ‘Sollis’ only contained GP and Acute Trust data. Therefore, detailed reporting from all providers is not possible until we add their data to ‘Sollis’ the process is now commencing to include social care data.
Contracting & Commissioning
A baseline data performance monitoring dashboard has been drafted and shared with the alliance
Implementation Plan from provider alliance - a revised version is being drafted by the alliance and will be shared with the commissioners
Establishing a collaboration model (AfC & ASC) for the delivery of the LD service
Preparing a report for Committee (September) on the future of dementia care in Kingston; site allocation awaited
Analysing the results of the ‘Thrive Kingston’ launch event and developing next steps
Kingston Care Record
IG sign off is awaited to enable the implementation of the Kingston Care Record which delivers combined Health and Social Care information in one place. This needs to then be tested to ensure that it will support the new ways of working.
Community, GP and Mental Health data feeds are live. GP and RBK Single Sign On (SSO) is live. RBK data feed – review of approach to service user consent
Version: Final H - 5 Date: 30 10 17
Active and Supportive Communities
The work to develop a social prescribing/community referral model for Kingston that augments clinical support and encourages people to be active and socially connected
Home Care Transformation
The Council has agreed to trial the establishment of Well-Being teams to deliver home care and support people to connect to the communities they live in. The Provider Alliance has agreed to trial an approach in the New Malden area to align with initial work around locality working, as Well-Being Teams need to be an integral element of those teams. A report was approved at Adults and Children's Committee to agree to the principle of establishing a limited trading company to implement well-being teams. A further report will go in February with the financial business plan and governance arrangements. In the meantime an initial small team will be recruited to establish how teams will work within the locality teams. An initial version of the ‘Home Care’ app has been demonstrated.
North and South locality teams set up and OT staff aligned to two teams. ‘Access’ set up and running, by moving ASC to co-locate with YH staff to do initial contact screening and triage for new people and crisis support. Referral forms to YH have been updated. A simplified form has been introduced for the access team so no longer need to complete additional assessments.
Collaborative Commissioning
The provider alliance has a signed memorandum of understanding that sits over the existing provider contracts in an umbrella arrangement for 2017-18, they have developed an implementation plan and an outcomes framework.
Monitoring
The provider alliance has developed a detailed implementation plan to be shared with commissioners.
Progress against implementation and evaluation of the MDT in New Malden will be monitored through regular established commissioner provider meetings. The lessons learnt from this pilot will inform the development of the model.
The impact of the new model of care will be reported back to the governing body and is regularly reported into the Kingston health and wellbeing board.
Version: Final J - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title SWL Sustainability and Transformation Partnership Refresh Agenda Item 14 Attachment J
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information X
Report Author: (name & job title)
Karen Broughton Director of Strategies and Programmes - SWL Sustainability and Transformation Partnership
Presented by: (name & job title)
Tonia Michaelides Managing Director – Kingston and Richmond CCGs
Summary and purpose of report The attached paper sets out the approach developed to support the refresh of the SWL Sustainability and Transformation Partnership (STP). The report outlines the reason for the refresh, the two stage approach that is being taken and the cycle for review and refresh going forward. Key sections for particular note The governing body are asked to note the following sections of the paper Slide 2 Explaining the reason for the refresh Slide 5-7 Outlines the approach the approach for the refresh Slide 9 Describes the plan going forward Report recommendation The Governing Body is asked to …note the contents of the report Financial and / or resource implications The SWL STP refresh is being completed using existing resources Key risks identified & mitigation No risks have been identified at the current time
Version: Final J - 2 Date: 01 11 17
Equality and / or privacy impact analysis Each STP initiative will have an equality and privacy impact analysis completed as appropriate. Committees that have previously discussed / agreed the report and outcomes None Communication plan / stakeholder involvement / patient engagement The SWL STP is developing a comprehensive communication and engagement plan Assurance No further assurance is required CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
South West London Sustainability and Transformation Partnership
Process for the STP Refresh 31 October 2017 Start well, live well, age well
Why are we doing a STP Refresh? • The perception of the SW London STP has been:
o Closure of hospitals
o Hospital bed reduction
o Stakeholders were not signed up to the financial analysis
• Reality far more than this:
o Prevention and early intervention
o Integrating with social care services
o Strengthened focus on locality teams made up of community, primary and social care
• To show the progress we have made for patients in South West London – the STP one year on
STP Refresh: the approach
• Empowering local leadership to drive health and social care improvement for local people: Croydon, Sutton, Merton + Wandsworth, Kingston + Richmond
• We are changing the conversation and the focus:
Not STP …but …local health and care partnerships Not SW London….but…local transformation boards areas
• Refreshed STP plan will now be locally focussed. It is not about creating something completely new, it is about sharing where we are and where we are going – pulling together all the things LTBs are working on. The aggregate of which will be our South West London joint health and care partnership plan.
• Key deliverables and will be turned into KPIs and expected outcomes so we can track our progress by LTB.
• Audience for local documents is informed stakeholders
The new narrative – tested locally/regionally
• A local approach works best for planning health and care
• Strengthen the focus on prevention and keeping people well – the greatest influences on our
health and wellbeing are factors such as education, employment, housing, healthy habits in our
communities and social connections
• The best bed is your own bed – lets keep people well and out of hospital
• Care is better when it is centred around a person, not an organisation. Clinicians and care workers
tell us this.
• Likely to mean changes to services locally - we are not proposing to close any hospitals, evolution
not revolution
• Involving people at local level will remain critical.
• We are not closing any hospitals. We will continue to need all our hospitals though we do not think
every hospital has to provide every service.
5 Start well, live well, age well
Stage one : November 2017
South West London STP one year on: our updated narrative, context and delivery so far
Stage Two : December 2017 – June 2018
Developing “Place Plans” for each of the four LTBs
We are taking a two stage approach to the STP refresh
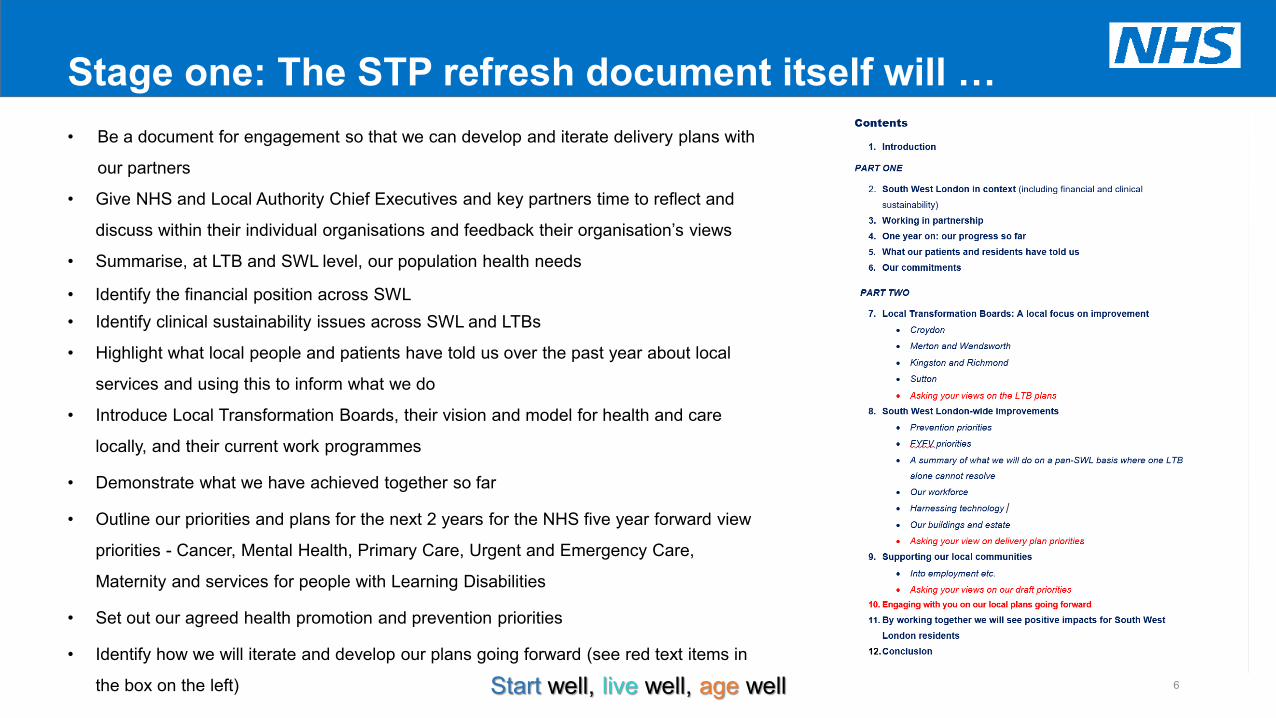
Stage one: The STP refresh document itself will … • Be a document for engagement so that we can develop and iterate delivery plans with
our partners
• Give NHS and Local Authority Chief Executives and key partners time to reflect and
discuss within their individual organisations and feedback their organisation’s views
• Summarise, at LTB and SWL level, our population health needs
• Identify the financial position across SWL • Identify clinical sustainability issues across SWL and LTBs
• Highlight what local people and patients have told us over the past year about local
services and using this to inform what we do
• Introduce Local Transformation Boards, their vision and model for health and care
locally, and their current work programmes
• Demonstrate what we have achieved together so far
• Outline our priorities and plans for the next 2 years for the NHS five year forward view
priorities - Cancer, Mental Health, Primary Care, Urgent and Emergency Care,
Maternity and services for people with Learning Disabilities
• Set out our agreed health promotion and prevention priorities
• Identify how we will iterate and develop our plans going forward (see red text items in
the box on the left)
6 Start well, live well, age well
Stage two: “Place Plans” will outline …
• The LTB’s vision for local health and care services
• Their model for health and care
• The local context and challenges they face, including any financial and clinical
sustainability issues
• Their priorities for the next 2 years to meet the health and care needs of their local
population, and plans to address financial and clinical sustainability
7 Start well, live well, age well
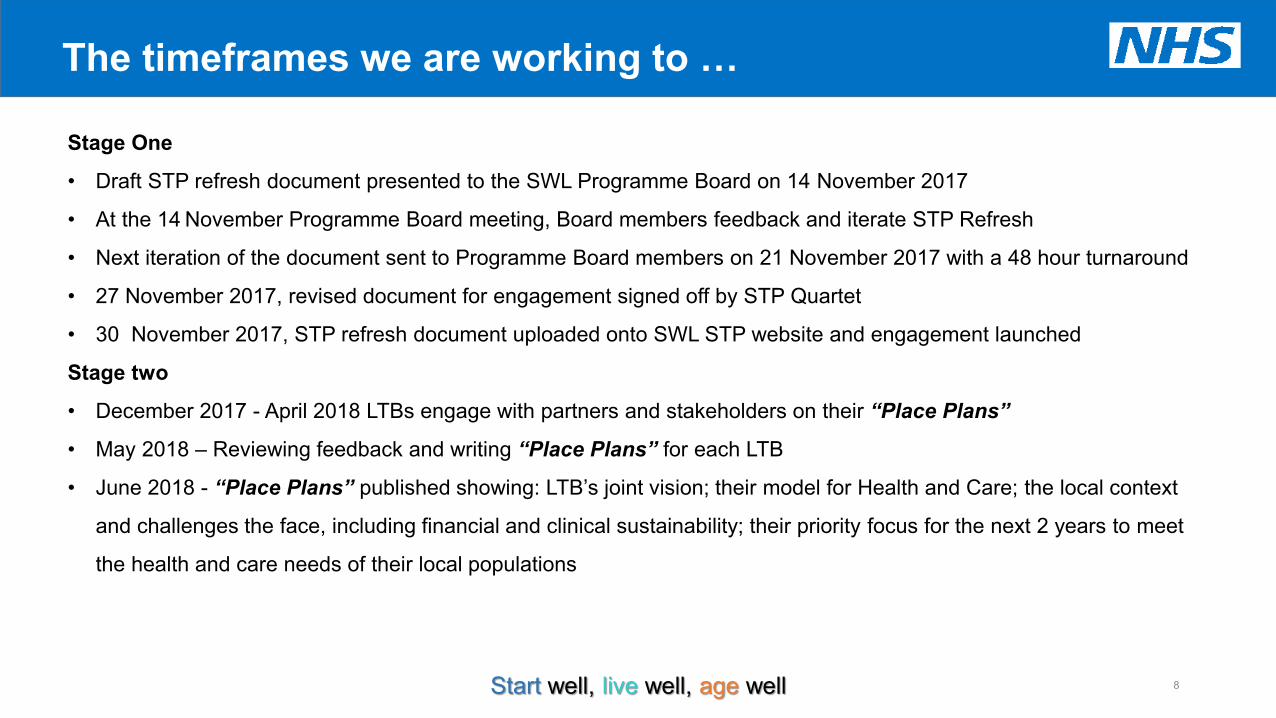
The timeframes we are working to …
8 Start well, live well, age well
Stage One
• Draft STP refresh document presented to the SWL Programme Board on 14 November 2017
• At the 14 November Programme Board meeting, Board members feedback and iterate STP Refresh
• Next iteration of the document sent to Programme Board members on 21 November 2017 with a 48 hour turnaround
• 27 November 2017, revised document for engagement signed off by STP Quartet
• 30 November 2017, STP refresh document uploaded onto SWL STP website and engagement launched
Stage two
• December 2017 - April 2018 LTBs engage with partners and stakeholders on their “Place Plans”
• May 2018 – Reviewing feedback and writing “Place Plans” for each LTB
• June 2018 - “Place Plans” published showing: LTB’s joint vision; their model for Health and Care; the local context
and challenges the face, including financial and clinical sustainability; their priority focus for the next 2 years to meet
the health and care needs of their local populations
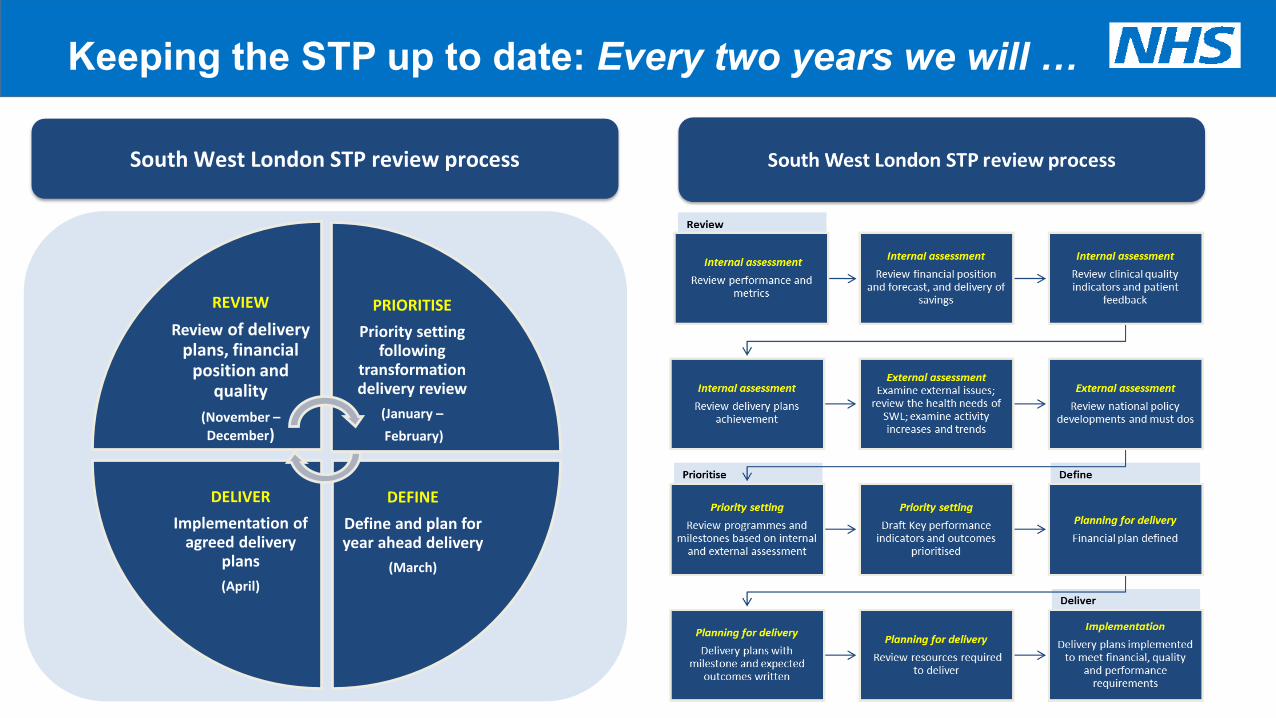
9
Keeping the STP up to date: Every two years we will …
REVIEW
Review of delivery plans, financial
position and quality
(November – December)
PRIORITISE
Priority setting following
transformation delivery review
(January –
February)
DEFINE
Define and plan for year ahead delivery
(March)
DELIVER
Implementation of agreed delivery
plans
(April)
South West London STP review process

Version: Final K - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017
Report Title Integrated Governance Report
Agenda Item 14 Attachment
K
Purpose (please indicate with X)
Approval/ Ratification Discussion /
Comment X Information X Report Author: (name & job title)
Brian Roberts Performance and Information Lead
Presented by: (name & job title)
Dr Phil Moore
Summary and purpose of report This report highlights issues and includes feedback from the 19th September 2017 and 17th October 2017 meeting of the Integrated Governance Committee, and contains a summary of the latest Performance Assurance Report. Key sections for particular note NHS England monitors the performance of CCGs using the following Constitutional Standards:
1. Dementia Diagnosis Rate 2. Referral to Treatment (18 Weeks) and Diagnostics 3. Access to Cancer Services 4. Mixed Sex Accommodation breaches 5. Mental Health/ Improving access to Psychological Therapies (IAPT) 6. Health Outcome Frameworks (MRSA and C Difficile Breaches) 7. Urgent Care (A&E and Ambulance Response Times) 8. Cancelled Operations
The performance scorecard focuses on these targets. The 2 main areas of concern are the Dementia Diagnosis rate and A&E waiting times. Report recommendation The Governing Body is asked to note this report. Financial and / or resource implications There is a financial implication regarding the 2017-2018 Quality Premium and QIPP Delivery. Key risks identified & mitigation As per report
Version: Final K - 2 Date: 30 10 17
Equality and / or privacy impact analysis Not applicable. Committees that have previously discussed / agreed the report and outcomes The Kingston CCG Integrated Governance Committee has previously discussed / agreed the report and outcomes. Communication plan / stakeholder involvement / patient engagement Not applicable. Assurance Not applicable. CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
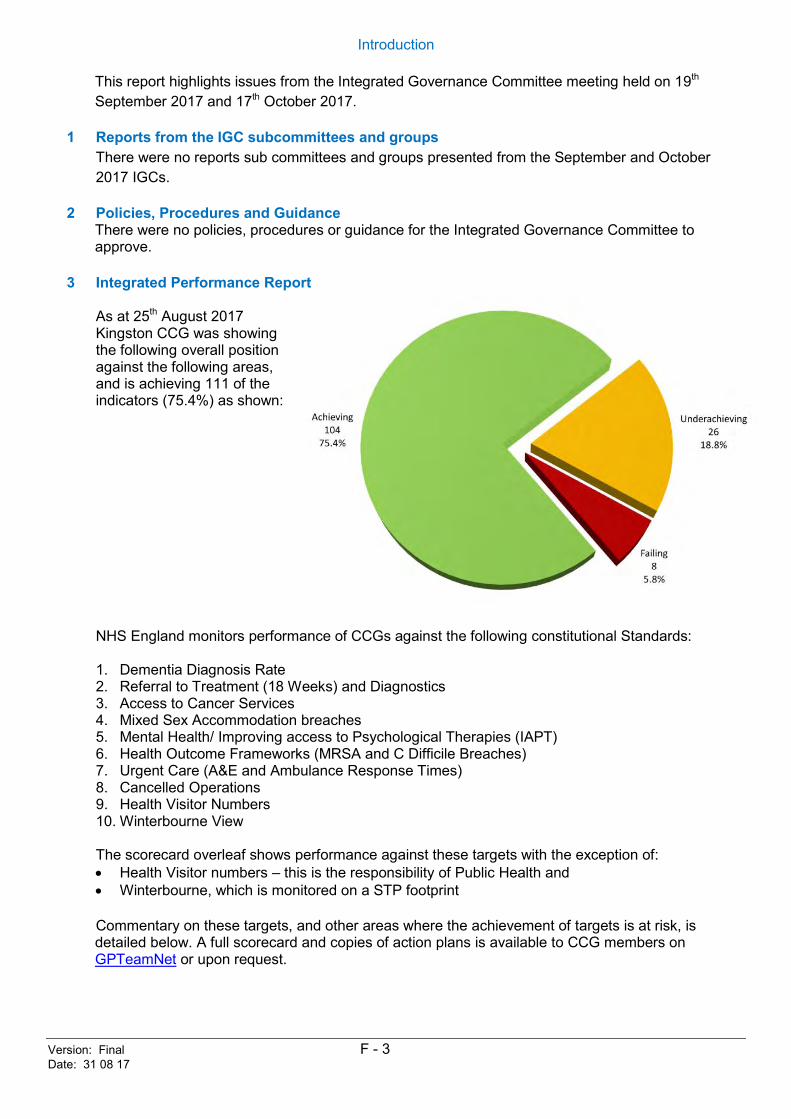
Version: Final F - 3 Date: 31 08 17
Introduction
This report highlights issues from the Integrated Governance Committee meeting held on 19th September 2017 and 17th October 2017.
1 Reports from the IGC subcommittees and groups There were no reports sub committees and groups presented from the September and October 2017 IGCs.
2 Policies, Procedures and Guidance There were no policies, procedures or guidance for the Integrated Governance Committee to approve.
3 Integrated Performance Report
As at 25th August 2017 Kingston CCG was showing the following overall position against the following areas, and is achieving 111 of the indicators (75.4%) as shown: NHS England monitors performance of CCGs against the following constitutional Standards: 1. Dementia Diagnosis Rate 2. Referral to Treatment (18 Weeks) and Diagnostics 3. Access to Cancer Services 4. Mixed Sex Accommodation breaches 5. Mental Health/ Improving access to Psychological Therapies (IAPT) 6. Health Outcome Frameworks (MRSA and C Difficile Breaches) 7. Urgent Care (A&E and Ambulance Response Times) 8. Cancelled Operations 9. Health Visitor Numbers 10. Winterbourne View
The scorecard overleaf shows performance against these targets with the exception of: Health Visitor numbers – this is the responsibility of Public Health and Winterbourne, which is monitored on a STP footprint Commentary on these targets, and other areas where the achievement of targets is at risk, is detailed below. A full scorecard and copies of action plans is available to CCG members on GPTeamNet or upon request.
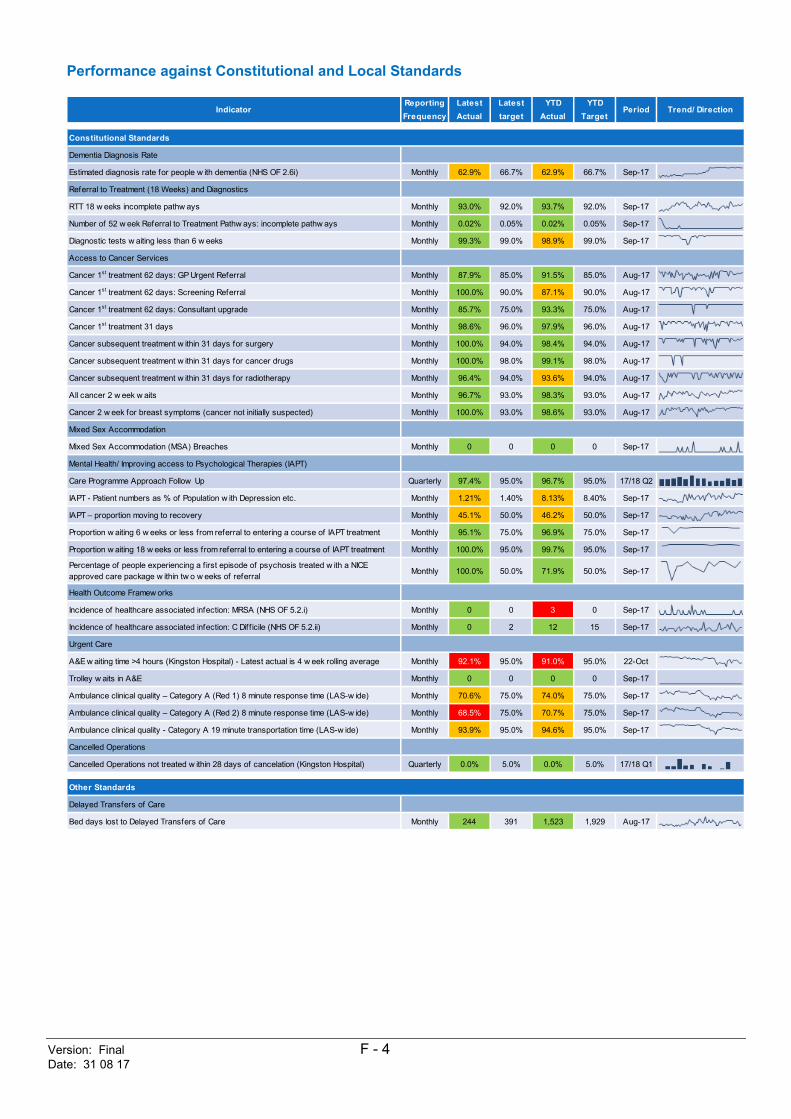
Version: Final F - 4 Date: 31 08 17
Performance against Constitutional and Local Standards
Reporting Latest Latest YTD YTDFrequency Actual target Actual Target
Constitutional Standards
Dementia Diagnosis Rate
Estimated diagnosis rate for people w ith dementia (NHS OF 2.6i) Monthly 62.9% 66.7% 62.9% 66.7% Sep-17
Referral to Treatment (18 Weeks) and Diagnostics
RTT 18 w eeks incomplete pathw ays Monthly 93.0% 92.0% 93.7% 92.0% Sep-17
Number of 52 w eek Referral to Treatment Pathw ays: incomplete pathw ays Monthly 0.02% 0.05% 0.02% 0.05% Sep-17
Diagnostic tests w aiting less than 6 w eeks Monthly 99.3% 99.0% 98.9% 99.0% Sep-17
Access to Cancer Services
Cancer 1st treatment 62 days: GP Urgent Referral Monthly 87.9% 85.0% 91.5% 85.0% Aug-17
Cancer 1st treatment 62 days: Screening Referral Monthly 100.0% 90.0% 87.1% 90.0% Aug-17
Cancer 1st treatment 62 days: Consultant upgrade Monthly 85.7% 75.0% 93.3% 75.0% Aug-17
Cancer 1st treatment 31 days Monthly 98.6% 96.0% 97.9% 96.0% Aug-17
Cancer subsequent treatment w ithin 31 days for surgery Monthly 100.0% 94.0% 98.4% 94.0% Aug-17
Cancer subsequent treatment w ithin 31 days for cancer drugs Monthly 100.0% 98.0% 99.1% 98.0% Aug-17
Cancer subsequent treatment w ithin 31 days for radiotherapy Monthly 96.4% 94.0% 93.6% 94.0% Aug-17
All cancer 2 w eek w aits Monthly 96.7% 93.0% 98.3% 93.0% Aug-17
Cancer 2 w eek for breast symptoms (cancer not initially suspected) Monthly 100.0% 93.0% 98.6% 93.0% Aug-17
Mixed Sex Accommodation
Mixed Sex Accommodation (MSA) Breaches Monthly 0 0 0 0 Sep-17
Mental Health/ Improving access to Psychological Therapies (IAPT)
Care Programme Approach Follow Up Quarterly 97.4% 95.0% 96.7% 95.0% 17/18 Q2
IAPT - Patient numbers as % of Population w ith Depression etc. Monthly 1.21% 1.40% 8.13% 8.40% Sep-17
IAPT – proportion moving to recovery Monthly 45.1% 50.0% 46.2% 50.0% Sep-17
Proportion w aiting 6 w eeks or less from referral to entering a course of IAPT treatment Monthly 95.1% 75.0% 96.9% 75.0% Sep-17
Proportion w aiting 18 w eeks or less from referral to entering a course of IAPT treatment Monthly 100.0% 95.0% 99.7% 95.0% Sep-17
Percentage of people experiencing a f irst episode of psychosis treated w ith a NICE approved care package w ithin tw o w eeks of referral Monthly 100.0% 50.0% 71.9% 50.0% Sep-17
Health Outcome Framew orks
Incidence of healthcare associated infection: MRSA (NHS OF 5.2.i) Monthly 0 0 3 0 Sep-17
Incidence of healthcare associated infection: C Diff icile (NHS OF 5.2.ii) Monthly 0 2 12 15 Sep-17
Urgent Care
A&E w aiting time >4 hours (Kingston Hospital) - Latest actual is 4 w eek rolling average Monthly 92.1% 95.0% 91.0% 95.0% 22-Oct
Trolley w aits in A&E Monthly 0 0 0 0 Sep-17
Ambulance clinical quality – Category A (Red 1) 8 minute response time (LAS-w ide) Monthly 70.6% 75.0% 74.0% 75.0% Sep-17
Ambulance clinical quality – Category A (Red 2) 8 minute response time (LAS-w ide) Monthly 68.5% 75.0% 70.7% 75.0% Sep-17
Ambulance clinical quality - Category A 19 minute transportation time (LAS-w ide) Monthly 93.9% 95.0% 94.6% 95.0% Sep-17
Cancelled Operations
Cancelled Operations not treated w ithin 28 days of cancelation (Kingston Hospital) Quarterly 0.0% 5.0% 0.0% 5.0% 17/18 Q1
Other Standards
Delayed Transfers of Care
Bed days lost to Delayed Transfers of Care Monthly 244 391 1,523 1,929 Aug-17
Indicator Period Trend/ Direction
Version: Final F - 5 Date: 31 08 17
3.1 Estimated diagnosis rate for people with dementia
Kingston CCG needs to both increase the current rate of diagnosis for dementia of 62.9% (as at 30th September 2017) to achieve the national target of 66.7% and to minimise the variation between practices. A recovery plan is in place achieve the 66.7% target within 2017-18, incorporating the following actions: Dementia information packs were circulated to every practice in Kingston CCG during May
17. The packs also highlight areas and actions that can be taken. Examples of this include advice on compiling a register for patients in their practice with Mild Cognitive Impairment (MCI) and to ensure these people are reviewed annually.
A dementia specialist nurse has been employed to visit the lowest performing practices initially and assess patients that have been identified with cognitive impairment to be included on the registers. She will then move on to support other practices that require support. The dementia specialist nurse commenced working two days per week on 22nd June 2017, and the dementia specialist nurse has met with the MAS and agreed a standard set of tools and templates with which to conduct the dementia screening reviews to ensure it dovetails with Memory assessment Service (MAS) assessment processes.
A dedicated clinician is assessing the cognition of patients in nursing homes and notify their GP of the diagnosis if found to have dementia.
A Mental Health KPI is being implemented which supports practices to increase their dementia diagnosis rate. Practices will receive a payment for either reaching or maintaining the rate above the threshold or making an improvement of 5% or more compared to their current performance. This KPI is due to be implemented across Kingston practices from November 2017.
3.2 Referral to Treatment (RTT) and Diagnostic Waits
Kingston CCG has achieved the incomplete RTT standard for June 2017 with performance of 93.0% against the 92% standard, and with year to date performance of 93.7%. Kingston CCG last missed the incomplete standard in July 2012. The 6 week diagnostics standard was achieved in September 2017 but the YTD position is 98.9% against the 99% standard. The majority of the breaches are in Audiology at St Georges (Queen Mary’s site), where there are data quality issues, rather than actual breaches. There are a range specific actions in place to increase performance at St Georges, and a monthly performance meeting has commenced, led by Wandsworth CCG.
3.3 Cancer Standards All the cancer standards were achieved for August 2017, with seven of the nine cancer standards have been met year to date. For 62 day waits resulting from a screening referral, YTD performance of 87.1% against the 90% standard has meant that the year to date the performance is below the threshold. This was as a result of 4 complex patients over 31 pathways, across several providers. The Radiotherapy (Subsequent) treatment standard is at 93.6% year to date against the 94% target. The breaches were all at the Royal Marsden, and relate mainly (6 of the 8 breaches over 125 pathways) to patient requested delays in treatment.
3.4 Mixed sex Accommodation Breaches There were no reported MSA breaches between April and September 2017.
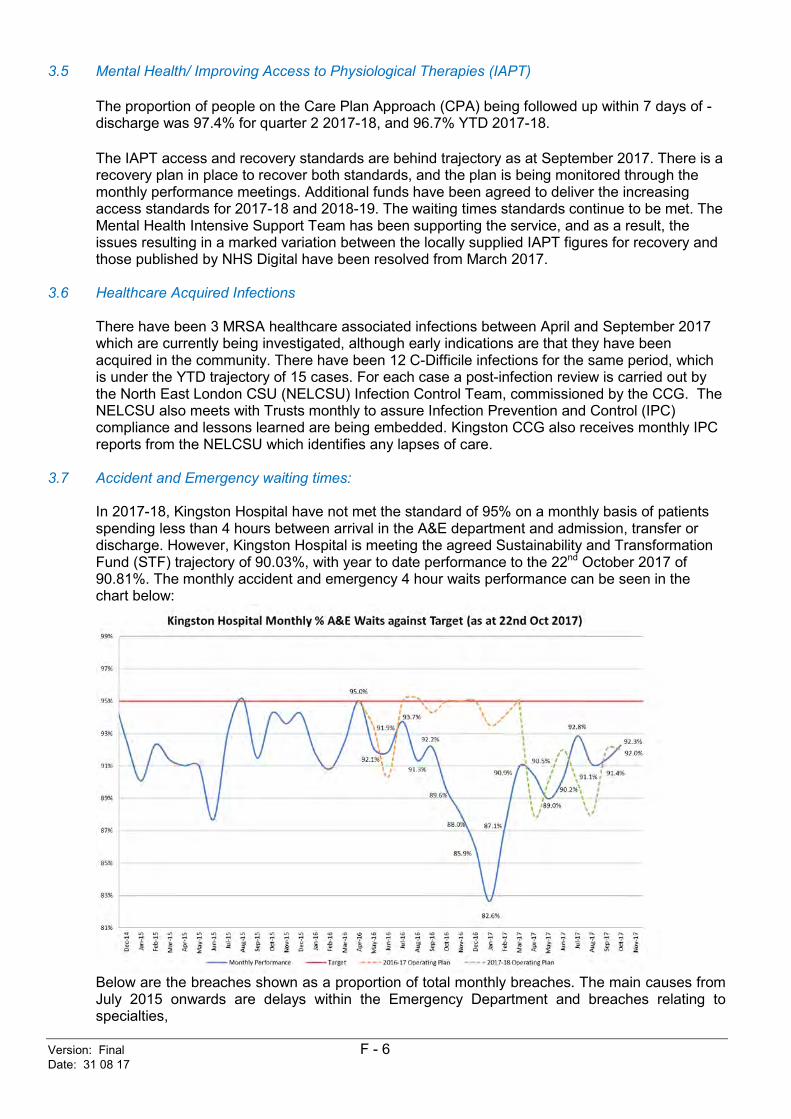
Version: Final F - 6 Date: 31 08 17
3.5 Mental Health/ Improving Access to Physiological Therapies (IAPT) The proportion of people on the Care Plan Approach (CPA) being followed up within 7 days of -discharge was 97.4% for quarter 2 2017-18, and 96.7% YTD 2017-18. The IAPT access and recovery standards are behind trajectory as at September 2017. There is a recovery plan in place to recover both standards, and the plan is being monitored through the monthly performance meetings. Additional funds have been agreed to deliver the increasing access standards for 2017-18 and 2018-19. The waiting times standards continue to be met. The Mental Health Intensive Support Team has been supporting the service, and as a result, the issues resulting in a marked variation between the locally supplied IAPT figures for recovery and those published by NHS Digital have been resolved from March 2017.
3.6 Healthcare Acquired Infections There have been 3 MRSA healthcare associated infections between April and September 2017 which are currently being investigated, although early indications are that they have been acquired in the community. There have been 12 C-Difficile infections for the same period, which is under the YTD trajectory of 15 cases. For each case a post-infection review is carried out by the North East London CSU (NELCSU) Infection Control Team, commissioned by the CCG. The NELCSU also meets with Trusts monthly to assure Infection Prevention and Control (IPC) compliance and lessons learned are being embedded. Kingston CCG also receives monthly IPC reports from the NELCSU which identifies any lapses of care.
3.7 Accident and Emergency waiting times: In 2017-18, Kingston Hospital have not met the standard of 95% on a monthly basis of patients spending less than 4 hours between arrival in the A&E department and admission, transfer or discharge. However, Kingston Hospital is meeting the agreed Sustainability and Transformation Fund (STF) trajectory of 90.03%, with year to date performance to the 22nd October 2017 of 90.81%. The monthly accident and emergency 4 hour waits performance can be seen in the chart below:
Below are the breaches shown as a proportion of total monthly breaches. The main causes from July 2015 onwards are delays within the Emergency Department and breaches relating to specialties,
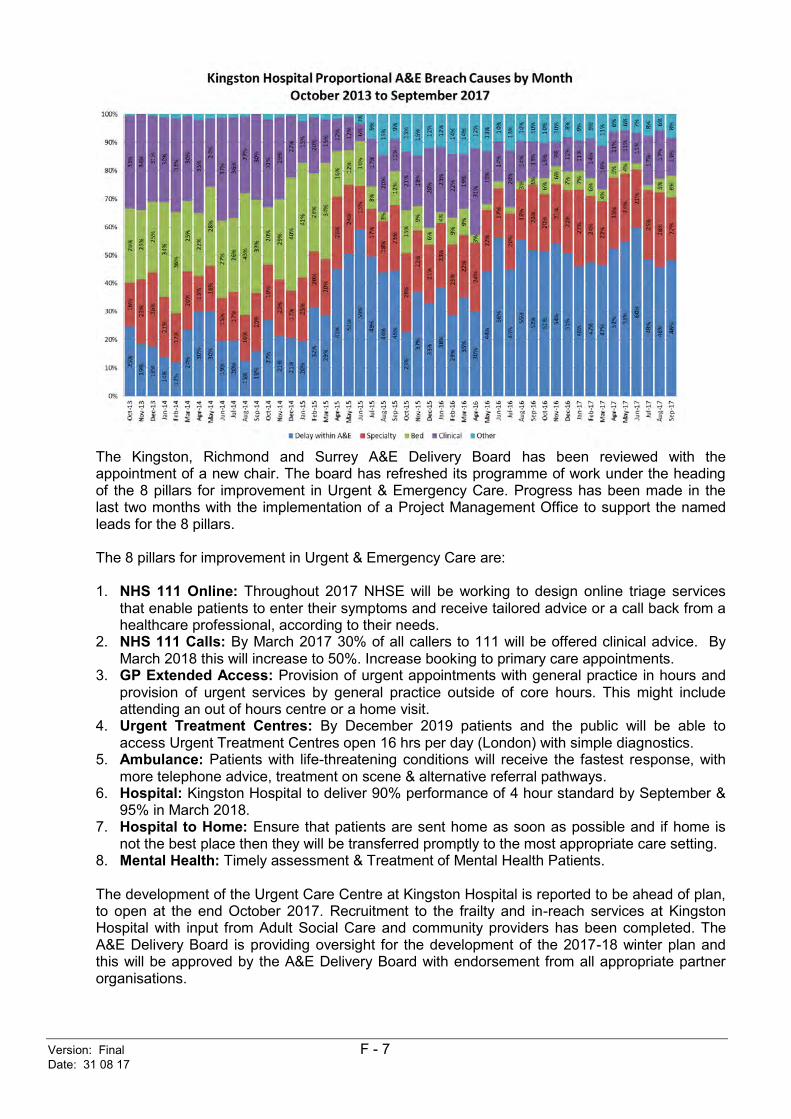
Version: Final F - 7 Date: 31 08 17
The Kingston, Richmond and Surrey A&E Delivery Board has been reviewed with the appointment of a new chair. The board has refreshed its programme of work under the heading of the 8 pillars for improvement in Urgent & Emergency Care. Progress has been made in the last two months with the implementation of a Project Management Office to support the named leads for the 8 pillars. The 8 pillars for improvement in Urgent & Emergency Care are: 1. NHS 111 Online: Throughout 2017 NHSE will be working to design online triage services
that enable patients to enter their symptoms and receive tailored advice or a call back from a healthcare professional, according to their needs.
2. NHS 111 Calls: By March 2017 30% of all callers to 111 will be offered clinical advice. By March 2018 this will increase to 50%. Increase booking to primary care appointments.
3. GP Extended Access: Provision of urgent appointments with general practice in hours and provision of urgent services by general practice outside of core hours. This might include attending an out of hours centre or a home visit.
4. Urgent Treatment Centres: By December 2019 patients and the public will be able to access Urgent Treatment Centres open 16 hrs per day (London) with simple diagnostics.
5. Ambulance: Patients with life-threatening conditions will receive the fastest response, with more telephone advice, treatment on scene & alternative referral pathways.
6. Hospital: Kingston Hospital to deliver 90% performance of 4 hour standard by September & 95% in March 2018.
7. Hospital to Home: Ensure that patients are sent home as soon as possible and if home is not the best place then they will be transferred promptly to the most appropriate care setting.
8. Mental Health: Timely assessment & Treatment of Mental Health Patients. The development of the Urgent Care Centre at Kingston Hospital is reported to be ahead of plan, to open at the end October 2017. Recruitment to the frailty and in-reach services at Kingston Hospital with input from Adult Social Care and community providers has been completed. The A&E Delivery Board is providing oversight for the development of the 2017-18 winter plan and this will be approved by the A&E Delivery Board with endorsement from all appropriate partner organisations.
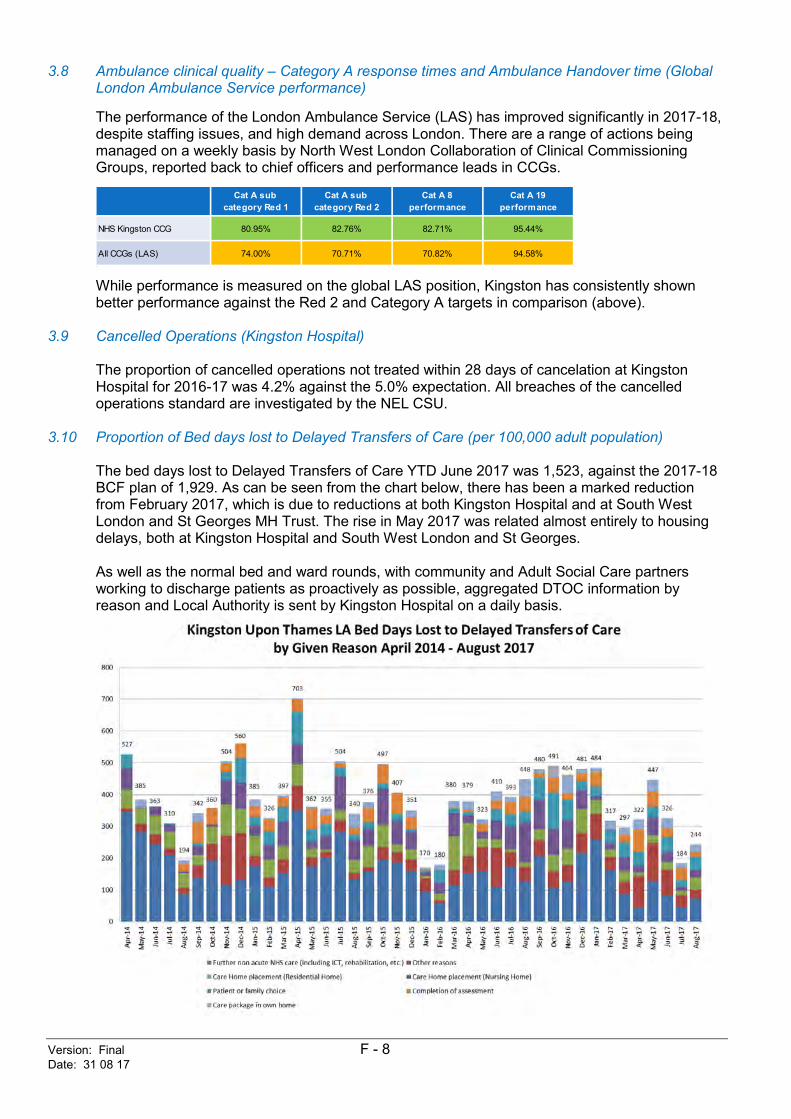
Version: Final F - 8 Date: 31 08 17
3.8 Ambulance clinical quality – Category A response times and Ambulance Handover time (Global London Ambulance Service performance)
The performance of the London Ambulance Service (LAS) has improved significantly in 2017-18, despite staffing issues, and high demand across London. There are a range of actions being managed on a weekly basis by North West London Collaboration of Clinical Commissioning Groups, reported back to chief officers and performance leads in CCGs.
While performance is measured on the global LAS position, Kingston has consistently shown better performance against the Red 2 and Category A targets in comparison (above).
3.9 Cancelled Operations (Kingston Hospital)
The proportion of cancelled operations not treated within 28 days of cancelation at Kingston Hospital for 2016-17 was 4.2% against the 5.0% expectation. All breaches of the cancelled operations standard are investigated by the NEL CSU.
3.10 Proportion of Bed days lost to Delayed Transfers of Care (per 100,000 adult population)
The bed days lost to Delayed Transfers of Care YTD June 2017 was 1,523, against the 2017-18 BCF plan of 1,929. As can be seen from the chart below, there has been a marked reduction from February 2017, which is due to reductions at both Kingston Hospital and at South West London and St Georges MH Trust. The rise in May 2017 was related almost entirely to housing delays, both at Kingston Hospital and South West London and St Georges. As well as the normal bed and ward rounds, with community and Adult Social Care partners working to discharge patients as proactively as possible, aggregated DTOC information by reason and Local Authority is sent by Kingston Hospital on a daily basis.
Cat A sub category Red 1
Cat A sub category Red 2
Cat A 8 performance
Cat A 19 performance
NHS Kingston CCG 80.95% 82.76% 82.71% 95.44%
All CCGs (LAS) 74.00% 70.71% 70.82% 94.58%
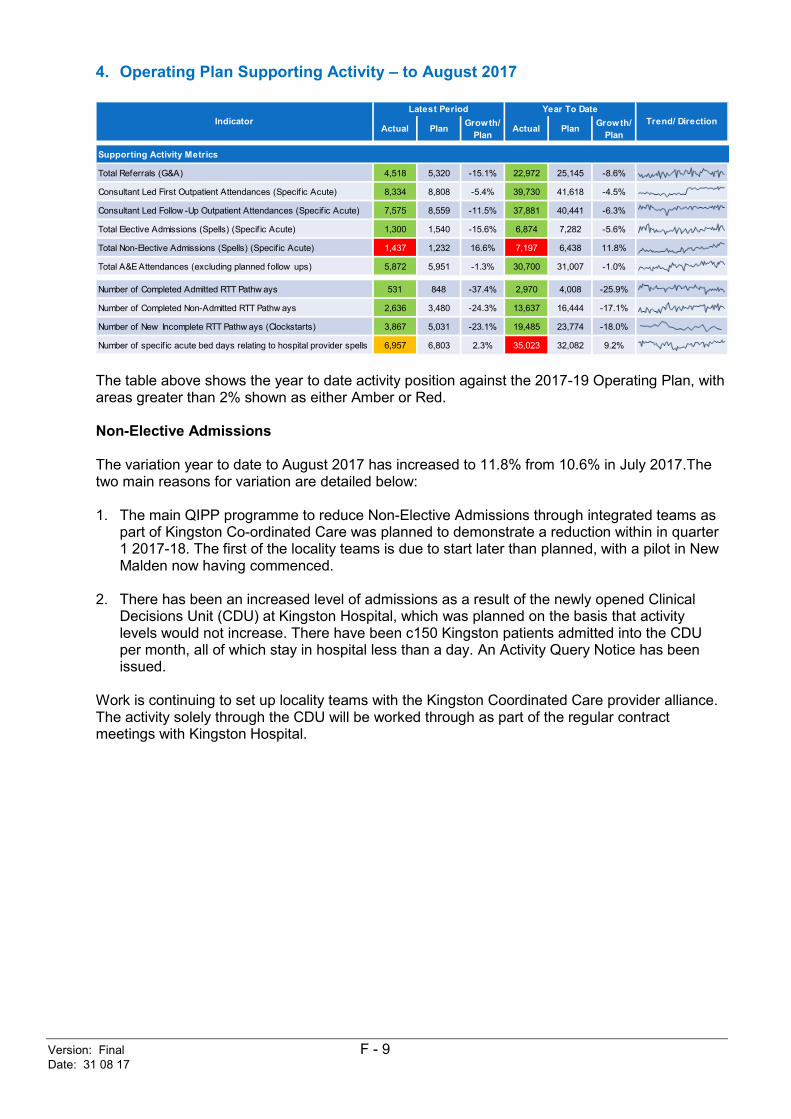
Version: Final F - 9 Date: 31 08 17
4. Operating Plan Supporting Activity – to August 2017
The table above shows the year to date activity position against the 2017-19 Operating Plan, with areas greater than 2% shown as either Amber or Red. Non-Elective Admissions The variation year to date to August 2017 has increased to 11.8% from 10.6% in July 2017.The two main reasons for variation are detailed below: 1. The main QIPP programme to reduce Non-Elective Admissions through integrated teams as
part of Kingston Co-ordinated Care was planned to demonstrate a reduction within in quarter 1 2017-18. The first of the locality teams is due to start later than planned, with a pilot in New Malden now having commenced.
2. There has been an increased level of admissions as a result of the newly opened Clinical Decisions Unit (CDU) at Kingston Hospital, which was planned on the basis that activity levels would not increase. There have been c150 Kingston patients admitted into the CDU per month, all of which stay in hospital less than a day. An Activity Query Notice has been issued.
Work is continuing to set up locality teams with the Kingston Coordinated Care provider alliance. The activity solely through the CDU will be worked through as part of the regular contract meetings with Kingston Hospital.
Actual Plan Growth/ Plan
Actual Plan Growth/ Plan
Supporting Activity Metrics
Total Referrals (G&A) 4,518 5,320 -15.1% 22,972 25,145 -8.6%
Consultant Led First Outpatient Attendances (Specif ic Acute) 8,334 8,808 -5.4% 39,730 41,618 -4.5%
Consultant Led Follow -Up Outpatient Attendances (Specif ic Acute) 7,575 8,559 -11.5% 37,881 40,441 -6.3%
Total Elective Admissions (Spells) (Specif ic Acute) 1,300 1,540 -15.6% 6,874 7,282 -5.6%
Total Non-Elective Admissions (Spells) (Specif ic Acute) 1,437 1,232 16.6% 7,197 6,438 11.8%
Total A&E Attendances (excluding planned follow ups) 5,872 5,951 -1.3% 30,700 31,007 -1.0%
Number of Completed Admitted RTT Pathw ays 531 848 -37.4% 2,970 4,008 -25.9%
Number of Completed Non-Admitted RTT Pathw ays 2,636 3,480 -24.3% 13,637 16,444 -17.1%
Number of New Incomplete RTT Pathw ays (Clockstarts) 3,867 5,031 -23.1% 19,485 23,774 -18.0%
Number of specif ic acute bed days relating to hospital provider spells 6,957 6,803 2.3% 35,023 32,082 9.2%
Indicator Trend/ DirectionLatest Period Year To Date

Version: Final F - 10 Date: 31 08 17
5. Draft Kingston CCG Quality Premium Forecast for 2017-18
Latest Latest YTD YTDActual target Actual Target
1. Cancers diagnosed at early stage
Demonstrate a 4% improvement in the proportion of cancers diagnosed at stages 1 and 2 in the 2017 calendar year compared to the 2016 calendar year, or achieve greater than 60% of all cancers that are diagnosed at stages 1 and 2 in the 2017 calendar year.
17% 54.5% 58.5% 54.5% 58.5% 2015 54.5% R 0.0%
2. Overall experience of making a GP appointment
Achieve a level of 85% of respondents w ho said they had a good experience of making an appointment, or a 3 percentage point increase from July 2017 publication on the percentage of respondents w ho said they had a good experience of making an appointment.
17% 68.9% 71.9% 68.9% 71.9% Jul-17 68.9% R 0.0%
Part a: To achieve the Quality Premium for this part, CCGs must ensure that in more than 80% of cases w ith a positive NHS CHC Checklist, the NHS CHC eligibility decision is made by the CCG w ithin 28 days from receipt of the Checklist (or other notif ication of potential eligibility)
8.5% 73.3% 80.0% 66.7% 80.0% 17/18 Q2 66.7% R 0.0%
Part b: To achieve the Quality Premium for this part, CCGs must ensure that less than 15% of all full NHS CHC assessments take place in an acute hospital setting.
8.5% 24.5% 15.0% 31.1% 15.0% 17/18 Q2 31.1% R 0.0%
Recovery rate of people accessing IAPT services identif ied as BAME; improvement of at least 5 percentage points or to same level as w hite British, w hichever is smaller. 4.6% 5.0% 5.8% 5.0% 16/17 Q4 5.8%
Proportion of people accessing IAPT services aged 65+; to increase to at least 50% of the proportion of adults aged 65+ in the local population or by at least 33%, w hichever is greater in 2017/18.
55.2% 50.0% 50.3% 50.0% 16/17 Q4 50.3%
i. 10% reduction (or greater) in all E coli BSI reported at CCG level based on 2016 performance data. 6.0% 2 7 37 45 Sep-17 74 G 6.0%
ii. collection and reporting of a core primary care data set for all E coli BSI inQ2-4 2017/18. 1.7%
iii. 10% reduction (or greater) in the Trimethoprim: Nitrofurantoin prescribing ratio based on CCG baseline data (June15-May16) for 2017/18. 3.8% 1.159 1.463 1.159 1.463 Jul-17 1.463 G 3.8%
iv. 10% reduction (or greater) in the number of trimethoprim items prescribed to patients aged 70 years or greater on baseline data (June15-May16) for 2017/18. 3.8% 3,175 3,332 3,175 3,332 Jul-17 3,332 G 3.8%
v. sustained reduction of inappropriate prescribing in primary care (maintain performance below England mean performance value of 2013-14). 1.7% 0.873 1.161 0.873 1.161 Jul-17 87.3% G 1.7%
6. Local Right Care measure
The percentage of patients w ith COPD w ho have had a review , undertaken by a healthcare professional, including an assessment of breathlessness using the Medical Research Council dyspnoea scale in the preceding 12 months (COPD003).
15% 84.1% 85.0% 87.1% 85.0% Aug-17 87.1% G 15.0%
100% 30.3%
Latest Latest YTD YTDActual target Actual Target
-25% 92.1% 95.0% 91.0% 95.0% 22-Oct 91.0% R -25.0%
-25% 93.0% 92.0% 93.7% 92.0% Sep-17 93.7% G 0.0%
-25% 87.9% 85.0% 91.5% 85.0% Aug-17 0.9 G 0.0%
-25% 70.6% 75.0% 74.0% 75.0% Sep-17 74.0% R -25.0%
-100% -50.0%
Forecast Quality Premium Percentage Achievement -15.2%
5. Reducing Gram Negative Bloodstream Infections (GNBSIs) and inappropriate antibiotic prescribing in at risk groups
Period Trend/ DirectionYear end forecast
17%
3. NHS Continuing Healthcare
4. Mental Health Menu: Equity of Access and outcomes in to IAPT services
Quality Premium Measures 2017-18Quality
Premium Percentage
Total Forecasted Adjustment against the NHS Constitution rights and Pledges
Total Forecasted Acheivement against the Quality Premium Measures
NHS Constitution rights and pledges Period R / GTrend/ DirectionYear end forecast
A&E w aiting time >4 hours (Kingston Hospital) - Latest actual is 4 w eek rolling average
Potential adjustment to Funding
Referral to Treatment (RTT) 18 w eeks incomplete pathw ays
Cancer 1st treatment 62 days: GP Urgent Referral
Ambulance clinical quality – Category A (Red 1) 8 minute response time (LAS-w ide)
Forecasted
adjustment to
Quality Premium % Forecast
R / G
R 0.0%
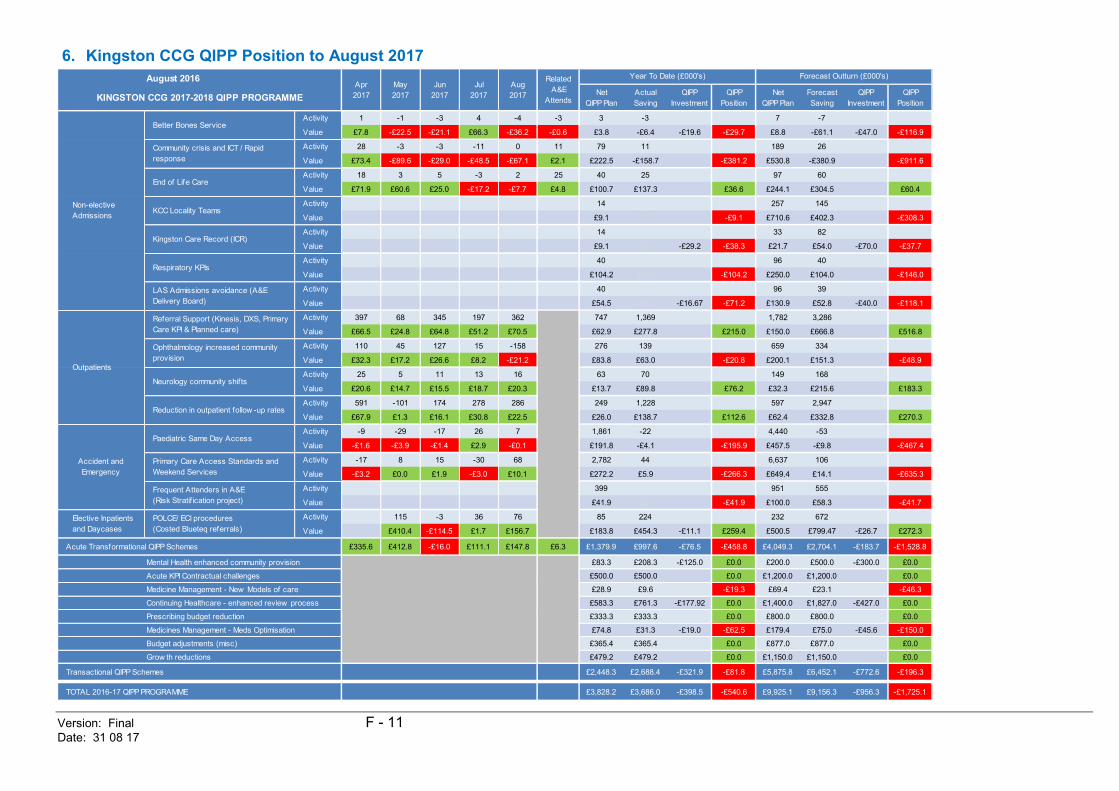
Version: Final F - 11 Date: 31 08 17
6. Kingston CCG QIPP Position to August 2017
August 2016Net
QIPP PlanActual Saving
QIPP Investment
QIPP Position
Net QIPP Plan
ForecastSaving
QIPP Investment
QIPP Position
Activity 1 -1 -3 4 -4 -3 3 -3 7 -7
Value £7.8 -£22.5 -£21.1 £66.3 -£36.2 -£0.6 £3.8 -£6.4 -£19.6 -£29.7 £8.8 -£61.1 -£47.0 -£116.9
Activity 28 -3 -3 -11 0 11 79 11 189 26
Value £73.4 -£89.6 -£29.0 -£48.5 -£67.1 £2.1 £222.5 -£158.7 -£381.2 £530.8 -£380.9 -£911.6
Activity 18 3 5 -3 2 25 40 25 97 60
Value £71.9 £60.6 £25.0 -£17.2 -£7.7 £4.8 £100.7 £137.3 £36.6 £244.1 £304.5 £60.4
Activity 14 0 257 145
Value £9.1 £0.0 -£9.1 £710.6 £402.3 -£308.3
Activity 14 0 33 82
Value £9.1 £0.0 -£29.2 -£38.3 £21.7 £54.0 -£70.0 -£37.7
Activity 40 0 96 40
Value £104.2 £0.0 -£104.2 £250.0 £104.0 -£146.0
Activity 40 0 96 39
Value £54.5 £0.0 -£16.67 -£71.2 £130.9 £52.8 -£40.0 -£118.1
Activity 397 68 345 197 362 747 1,369 1,782 3,286
Value £66.5 £24.8 £64.8 £51.2 £70.5 £62.9 £277.8 £215.0 £150.0 £666.8 £516.8
Activity 110 45 127 15 -158 276 139 659 334
Value £32.3 £17.2 £26.6 £8.2 -£21.2 £83.8 £63.0 -£20.8 £200.1 £151.3 -£48.9
Activity 25 5 11 13 16 63 70 149 168
Value £20.6 £14.7 £15.5 £18.7 £20.3 £13.7 £89.8 £76.2 £32.3 £215.6 £183.3
Activity 591 -101 174 278 286 249 1,228 597 2,947
Value £67.9 £1.3 £16.1 £30.8 £22.5 £26.0 £138.7 £112.6 £62.4 £332.8 £270.3
Activity -9 -29 -17 26 7 1,861 -22 4,440 -53
Value -£1.6 -£3.9 -£1.4 £2.9 -£0.1 £191.8 -£4.1 -£195.9 £457.5 -£9.8 -£467.4
Activity -17 8 15 -30 68 2,782 44 6,637 106
Value -£3.2 £0.0 £1.9 -£3.0 £10.1 £272.2 £5.9 -£266.3 £649.4 £14.1 -£635.3
Activity 399 0 951 555
Value £41.9 £0.0 -£41.9 £100.0 £58.3 -£41.7
Activity 115 -3 36 76 85 224 232 672
Value £410.4 -£114.5 £1.7 £156.7 £183.8 £454.3 -£11.1 £259.4 £500.5 £799.47 -£26.7 £272.3
Acute Transformational QIPP Schemes £335.6 £412.8 -£16.0 £111.1 £147.8 £6.3 £1,379.9 £997.6 -£76.5 -£458.8 £4,049.3 £2,704.1 -£183.7 -£1,528.8
Mental Health enhanced community provision £83.3 £208.3 -£125.0 £0.0 £200.0 £500.0 -£300.0 £0.0
Acute KPI Contractual challenges £500.0 £500.0 £0.0 £1,200.0 £1,200.0 £0.0
Medicine Management - New Models of care £28.9 £9.6 -£19.3 £69.4 £23.1 -£46.3
Continuing Healthcare - enhanced review process £583.3 £761.3 -£177.92 £0.0 £1,400.0 £1,827.0 -£427.0 £0.0
Prescribing budget reduction £333.3 £333.3 £0.0 £800.0 £800.0 £0.0
Medicines Management - Meds Optimisation £74.8 £31.3 -£19.0 -£62.5 £179.4 £75.0 -£45.6 -£150.0
Budget adjustments (misc) £365.4 £365.4 £0.0 £877.0 £877.0 £0.0
Grow th reductions £479.2 £479.2 £0.0 £1,150.0 £1,150.0 £0.0
Transactional QIPP Schemes £2,448.3 £2,688.4 -£321.9 -£81.8 £5,875.8 £6,452.1 -£772.6 -£196.3
TOTAL 2016-17 QIPP PROGRAMME £3,828.2 £3,686.0 -£398.5 -£540.6 £9,925.1 £9,156.3 -£956.3 -£1,725.1
May 2017
Apr 2017KINGSTON CCG 2017-2018 QIPP PROGRAMME
Aug 2017
Jul 2017
Reduction in outpatient follow -up rates
Ophthalmology increased community provision
Neurology community shifts
Paediatric Same Day Access
Community crisis and ICT / Rapid response
Kingston Care Record (ICR)
LAS Admissions avoidance (A&E Delivery Board)
Referral Support (Kinesis, DXS, Primary Care KPI & Planned care)
End of Life Care
Respiratory KPIs
KCC Locality Teams
Year To Date (£000's)Jun
2017
Forecast Outturn (£000's)Related A&E
Attends
Elective Inpatients and Daycases
POLCE/ ECI procedures(Costed Blueteq referrals)
Primary Care Access Standards and Weekend Services
Outpatients
Non-elective Admissions
Accident and Emergency
Frequent Attenders in A&E (Risk Stratif ication project)
Better Bones Service
Version: Final L - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Finance Report
Agenda Item 14 Attachment
L
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
X Information
Report Author: (name & job title)
Jenny Cheung, Management Accountant
Presented by: (name & job title)
Yarlini Roberts, Local Director of Finance
Summary and purpose of report The attached report details the CCG financial position as at the end of September 2017. Financial statements are included, along with monitoring reports of QIPP scheme achievements. Key sections for particular note Please note:
1. Finance Scorecard 2. Key Indicators 3. Summary Financial Position
Report recommendation The Governing Body is asked to note the finance report for September 2017. Financial and / or resource implications Please see main body of report. Key risks identified & mitigation Risks are detailed on page 3 of the finance report. Equality and / or privacy impact analysis n/a Committees that have previously discussed / agreed the report and outcomes Finance committee
Version: Final L - 2 Date: 30 10 17
Communication plan / stakeholder involvement / patient engagement n/a Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? No CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
KCCG Finance Report September 2017
Yarlini Roberts – Local Director of Finance
1 Produced by Finance September 2017
Contents
1. Finance Scorecard 2. Key Indicators 3. Summary Financial Position 4. Run Rate Analysis 5. Acute Commissioning 6. Non-Acute Commissioning 7. Primary Care 8. Running Costs 9. Underlying Position 10. Quality, Innovation, Productivity and Prevention programme (QIPP) 11. Financial Statements 12. Appendices
2 Produced by Finance September 2017
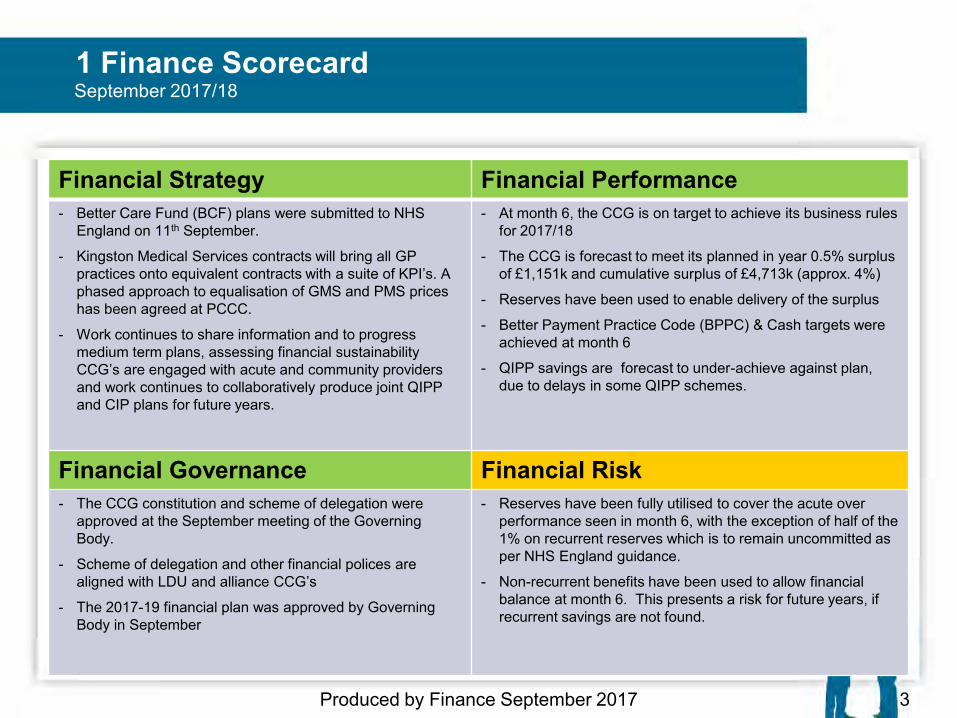
1 Finance Scorecard
3 Produced by Finance September 2017
Financial Strategy Financial Performance - Better Care Fund (BCF) plans were submitted to NHS
England on 11th September.
- Kingston Medical Services contracts will bring all GP practices onto equivalent contracts with a suite of KPI’s. A phased approach to equalisation of GMS and PMS prices has been agreed at PCCC.
- Work continues to share information and to progress medium term plans, assessing financial sustainability CCG’s are engaged with acute and community providers and work continues to collaboratively produce joint QIPP and CIP plans for future years.
- At month 6, the CCG is on target to achieve its business rules for 2017/18
- The CCG is forecast to meet its planned in year 0.5% surplus of £1,151k and cumulative surplus of £4,713k (approx. 4%)
- Reserves have been used to enable delivery of the surplus
- Better Payment Practice Code (BPPC) & Cash targets were achieved at month 6
- QIPP savings are forecast to under-achieve against plan, due to delays in some QIPP schemes.
Financial Governance Financial Risk - The CCG constitution and scheme of delegation were
approved at the September meeting of the Governing Body.
- Scheme of delegation and other financial polices are aligned with LDU and alliance CCG’s
- The 2017-19 financial plan was approved by Governing Body in September
- Reserves have been fully utilised to cover the acute over performance seen in month 6, with the exception of half of the 1% on recurrent reserves which is to remain uncommitted as per NHS England guidance.
- Non-recurrent benefits have been used to allow financial balance at month 6. This presents a risk for future years, if recurrent savings are not found.
September 2017/18
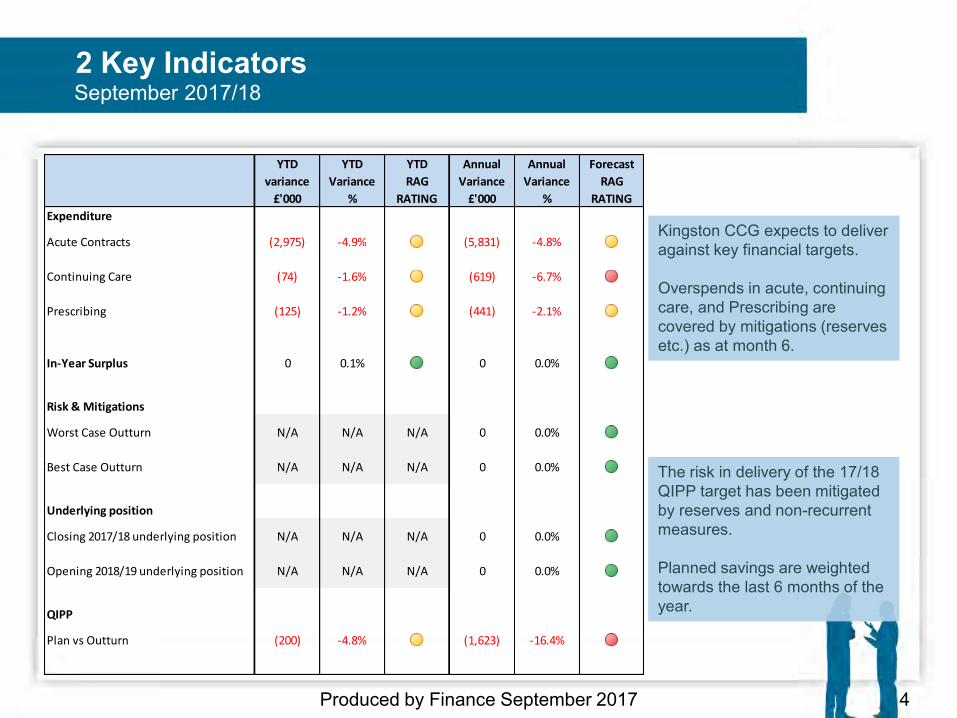
2 Key Indicators
Produced by Finance September 2017 4
September 2017/18
Kingston CCG expects to deliver against key financial targets. Overspends in acute, continuing care, and Prescribing are covered by mitigations (reserves etc.) as at month 6.
The risk in delivery of the 17/18 QIPP target has been mitigated by reserves and non-recurrent measures. Planned savings are weighted towards the last 6 months of the year.
YTD
variance
£'000
YTD
Variance
%
YTD
RAG
RATING
Annual
Variance
£'000
Annual
Variance
%
Forecast
RAG
RATING
Expenditure
Acute Contracts (2,975) -4.9% (5,831) -4.8%
Continuing Care (74) -1.6% (619) -6.7%
Prescribing (125) -1.2% (441) -2.1%
In-Year Surplus 0 0.1% 0 0.0%
Risk & Mitigations
Worst Case Outturn N/A N/A N/A 0 0.0%
Best Case Outturn N/A N/A N/A 0 0.0%
Underlying position
Closing 2017/18 underlying position N/A N/A N/A 0 0.0%
Opening 2018/19 underlying position N/A N/A N/A 0 0.0%
QIPP
Plan vs Outturn (200) -4.8% (1,623) -16.4%
3 Month 6 Summary
5 Produced by Finance September 2017
• The CCG expects to meet its planned in year 0.5% surplus of £1,151k. • Cash and Better Payment Practice Code (BPPC) targets were met in month 6
• Non-recurrent allocation of £30k has been received in month 6 for quarter 2
payment to Kingston Hospital to deliver the Faster Diagnosis standard. • The cost impact of Identification Rules (IR) is excluded from the acute
position. Analysis work is being carried out with NHSE specialised and it is anticipated that funding will be received to cover the shortfall.
• QIPP savings are forecast to under-achieve against plan, due to delays in
starting some QIPP schemes. Action plans are in development to improve performance.
• The CCG is using non-recurrent support to manage the forecast position,
enabling delivery of the planned in-year surplus of 0.5%.
September 2017/18
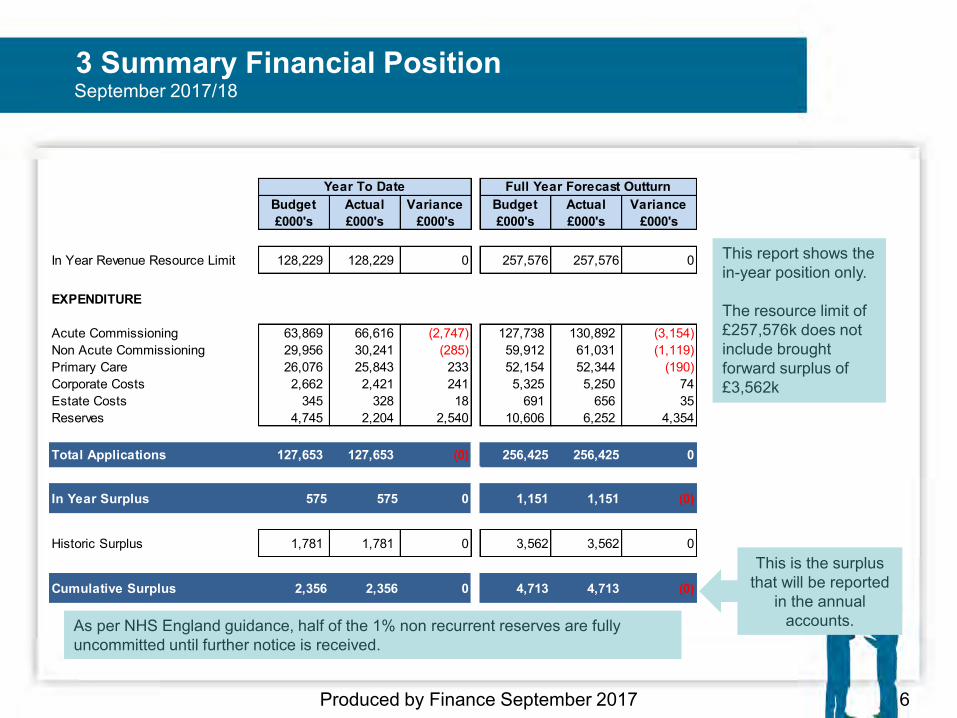
3 Summary Financial Position
6 Produced by Finance September 2017
This report shows the in-year position only. The resource limit of £257,576k does not include brought forward surplus of £3,562k
As per NHS England guidance, half of the 1% non recurrent reserves are fully uncommitted until further notice is received.
September 2017/18
This is the surplus that will be reported
in the annual accounts.
Budget Actual Variance Budget Actual Variance£000's £000's £000's £000's £000's £000's
In Year Revenue Resource Limit 128,229 128,229 0 257,576 257,576 0
EXPENDITURE
Acute Commissioning 63,869 66,616 (2,747) 127,738 130,892 (3,154)Non Acute Commissioning 29,956 30,241 (285) 59,912 61,031 (1,119)Primary Care 26,076 25,843 233 52,154 52,344 (190)Corporate Costs 2,662 2,421 241 5,325 5,250 74Estate Costs 345 328 18 691 656 35Reserves 4,745 2,204 2,540 10,606 6,252 4,354
Total Applications 127,653 127,653 (0) 256,425 256,425 0
In Year Surplus 575 575 0 1,151 1,151 (0)
Historic Surplus 1,781 1,781 0 3,562 3,562 0
Cumulative Surplus 2,356 2,356 0 4,713 4,713 (0)
Year To Date Full Year Forecast Outturn
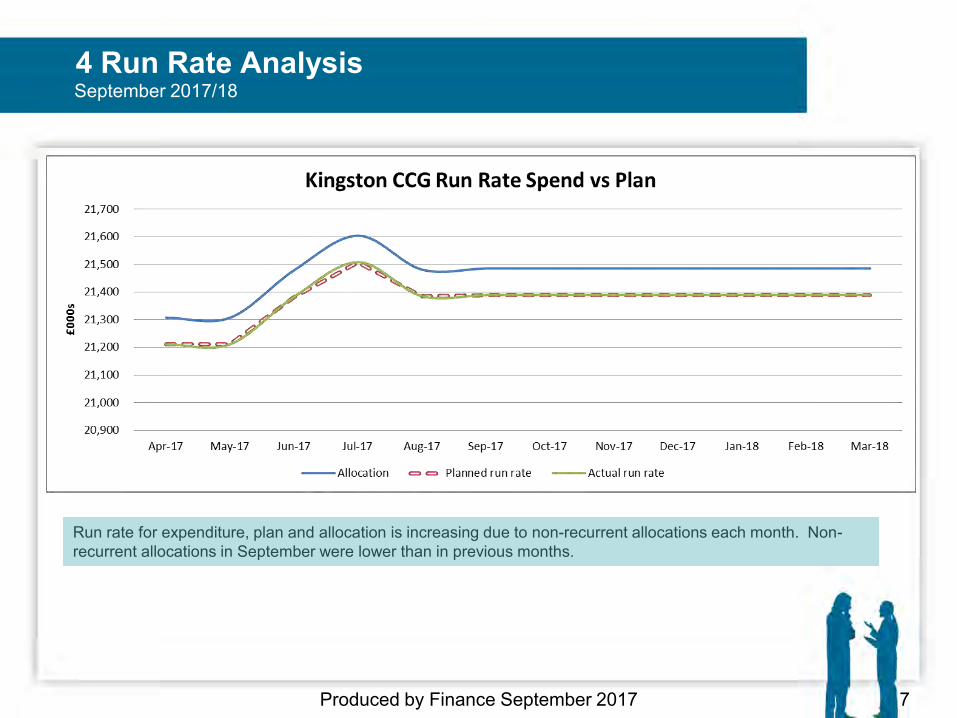
4 Run Rate Analysis
Produced by Finance September 2017 7
Run rate for expenditure, plan and allocation is increasing due to non-recurrent allocations each month. Non-recurrent allocations in September were lower than in previous months.
September 2017/18
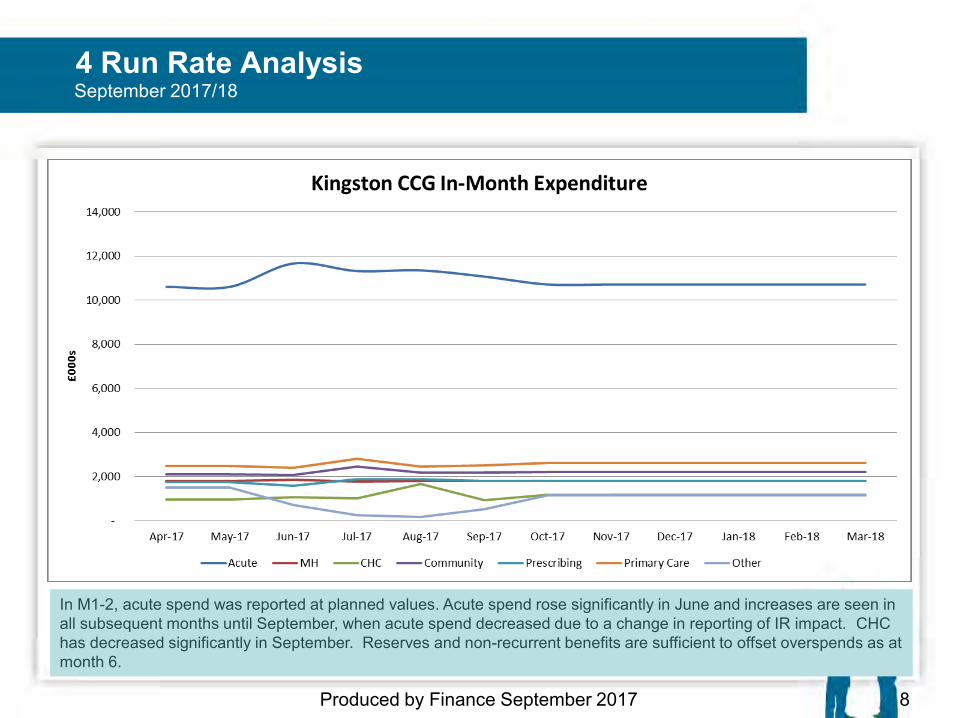
4 Run Rate Analysis
Produced by Finance September 2017 8
In M1-2, acute spend was reported at planned values. Acute spend rose significantly in June and increases are seen in all subsequent months until September, when acute spend decreased due to a change in reporting of IR impact. CHC has decreased significantly in September. Reserves and non-recurrent benefits are sufficient to offset overspends as at month 6.
September 2017/18
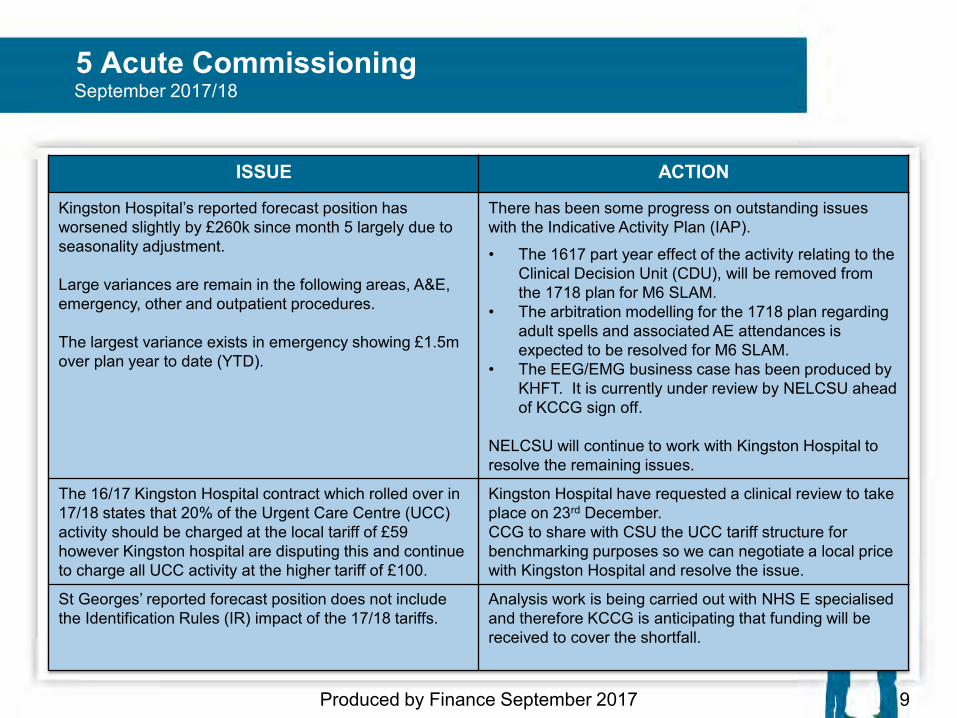
5 Acute Commissioning
Produced by Finance September 2017 9
September 2017/18
ISSUE ACTION
Kingston Hospital’s reported forecast position has worsened slightly by £260k since month 5 largely due to seasonality adjustment. Large variances are remain in the following areas, A&E, emergency, other and outpatient procedures. The largest variance exists in emergency showing £1.5m over plan year to date (YTD).
There has been some progress on outstanding issues with the Indicative Activity Plan (IAP).
• The 1617 part year effect of the activity relating to the Clinical Decision Unit (CDU), will be removed from the 1718 plan for M6 SLAM.
• The arbitration modelling for the 1718 plan regarding adult spells and associated AE attendances is expected to be resolved for M6 SLAM.
• The EEG/EMG business case has been produced by KHFT. It is currently under review by NELCSU ahead of KCCG sign off.
NELCSU will continue to work with Kingston Hospital to resolve the remaining issues.
The 16/17 Kingston Hospital contract which rolled over in 17/18 states that 20% of the Urgent Care Centre (UCC) activity should be charged at the local tariff of £59 however Kingston hospital are disputing this and continue to charge all UCC activity at the higher tariff of £100.
Kingston Hospital have requested a clinical review to take place on 23rd December. CCG to share with CSU the UCC tariff structure for benchmarking purposes so we can negotiate a local price with Kingston Hospital and resolve the issue.
St Georges’ reported forecast position does not include the Identification Rules (IR) impact of the 17/18 tariffs.
Analysis work is being carried out with NHS E specialised and therefore KCCG is anticipating that funding will be received to cover the shortfall.
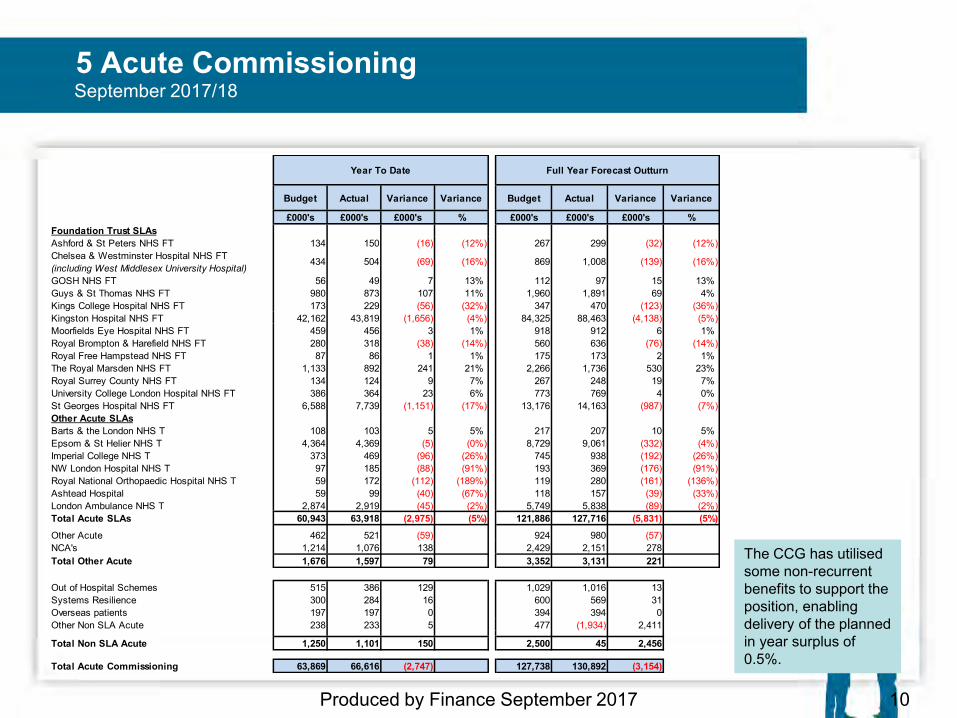
5 Acute Commissioning September 2017/18
10 Produced by Finance September 2017
The CCG has utilised some non-recurrent benefits to support the position, enabling delivery of the planned in year surplus of 0.5%.
Budget Actual Variance Variance Budget Actual Variance Variance
£000's £000's £000's % £000's £000's £000's %Foundation Trust SLAsAshford & St Peters NHS FT 134 150 (16) (12%) 267 299 (32) (12%)Chelsea & Westminster Hospital NHS FT(including West Middlesex University Hospital)
434 504 (69) (16%) 869 1,008 (139) (16%)
GOSH NHS FT 56 49 7 13% 112 97 15 13% Guys & St Thomas NHS FT 980 873 107 11% 1,960 1,891 69 4% Kings College Hospital NHS FT 173 229 (56) (32%) 347 470 (123) (36%)Kingston Hospital NHS FT 42,162 43,819 (1,656) (4%) 84,325 88,463 (4,138) (5%)Moorfields Eye Hospital NHS FT 459 456 3 1% 918 912 6 1% Royal Brompton & Harefield NHS FT 280 318 (38) (14%) 560 636 (76) (14%)Royal Free Hampstead NHS FT 87 86 1 1% 175 173 2 1% The Royal Marsden NHS FT 1,133 892 241 21% 2,266 1,736 530 23% Royal Surrey County NHS FT 134 124 9 7% 267 248 19 7% University College London Hospital NHS FT 386 364 23 6% 773 769 4 0% St Georges Hospital NHS FT 6,588 7,739 (1,151) (17%) 13,176 14,163 (987) (7%)Other Acute SLAsBarts & the London NHS T 108 103 5 5% 217 207 10 5% Epsom & St Helier NHS T 4,364 4,369 (5) (0%) 8,729 9,061 (332) (4%)Imperial College NHS T 373 469 (96) (26%) 745 938 (192) (26%)NW London Hospital NHS T 97 185 (88) (91%) 193 369 (176) (91%)Royal National Orthopaedic Hospital NHS T 59 172 (112) (189%) 119 280 (161) (136%)Ashtead Hospital 59 99 (40) (67%) 118 157 (39) (33%)London Ambulance NHS T 2,874 2,919 (45) (2%) 5,749 5,838 (89) (2%)Total Acute SLAs 60,943 63,918 (2,975) (5%) 121,886 127,716 (5,831) (5%)
Other Acute 462 521 (59) 924 980 (57)NCA's 1,214 1,076 138 2,429 2,151 278Total Other Acute 1,676 1,597 79 3,352 3,131 221
Out of Hospital Schemes 515 386 129 1,029 1,016 13Systems Resilience 300 284 16 600 569 31Overseas patients 197 197 0 394 394 0Other Non SLA Acute 238 233 5 477 (1,934) 2,411
Total Non SLA Acute 1,250 1,101 150 2,500 45 2,456
Total Acute Commissioning 63,869 66,616 (2,747) 127,738 130,892 (3,154)
Full Year Forecast OutturnYear To Date
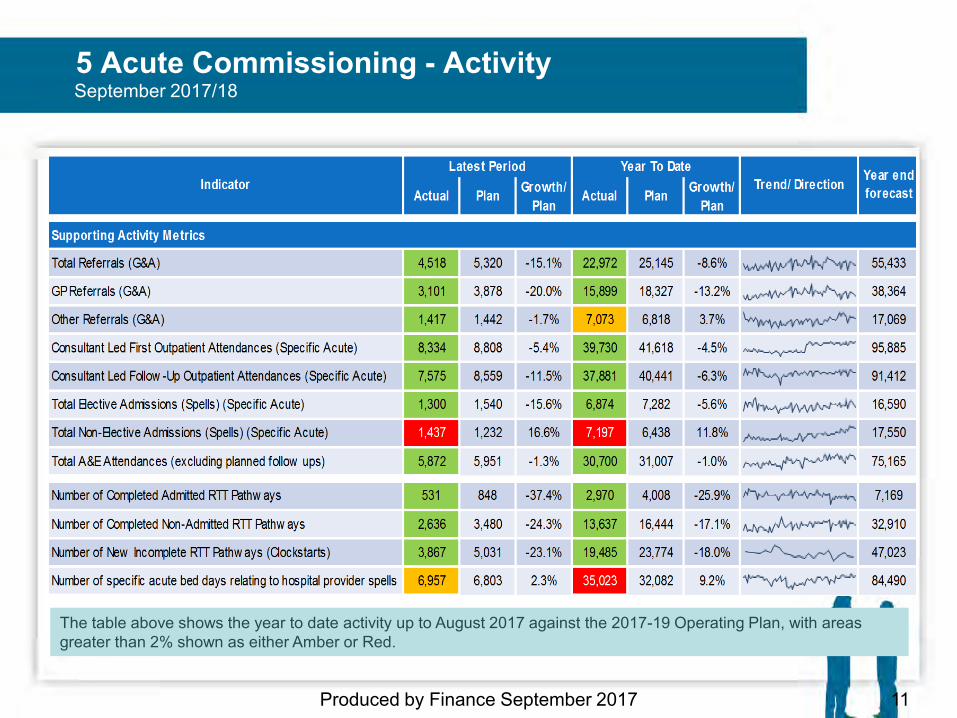
5 Acute Commissioning - Activity
Produced by Finance September 2017 11
September 2017/18
The table above shows the year to date activity up to August 2017 against the 2017-19 Operating Plan, with areas greater than 2% shown as either Amber or Red.
5 Acute Commissioning - Activity
Non-Elective Admissions The variation year to date in August 2017 has increased to 11.8% from 10.6% in July 2017.The two main reasons for variation are detailed below:
1. The main QIPP programme to reduce Non-Elective Admissions through integrated teams as part of Kingston Co-ordinated Care was planned to demonstrate a reduction within in quarter 1 2017-18. The first of the locality teams is due to start later than planned, with a pilot in New Malden due to complete soon.
2. There has been an increased level of admissions as a result of the newly opened Clinical Decisions Unit (CDU) at Kingston Hospital, which was planned on the basis that activity levels would not increase. There have been c150 Kingston patients admitted into the CDU per month, all of which stay in hospital less than a day. An Activity Query notice has been issued by the CCG to Kingston Hospital.
Work is continuing to set up locality teams with the Kingston Coordinated Care provider alliance. Issues with the CDU will be worked through as part of the regular contract meetings with Kingston Hospital.
Produced by Finance September 2017 12
September 2017/18
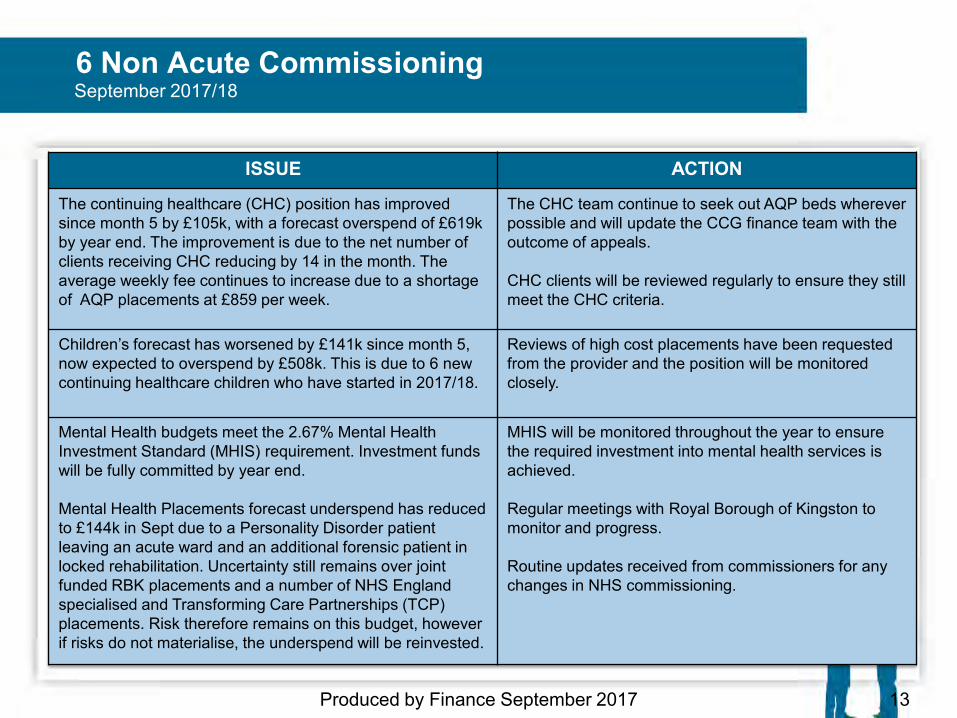
6 Non Acute Commissioning
Produced by Finance September 2017 13
September 2017/18
ISSUE ACTION
The continuing healthcare (CHC) position has improved since month 5 by £105k, with a forecast overspend of £619k by year end. The improvement is due to the net number of clients receiving CHC reducing by 14 in the month. The average weekly fee continues to increase due to a shortage of AQP placements at £859 per week.
The CHC team continue to seek out AQP beds wherever possible and will update the CCG finance team with the outcome of appeals. CHC clients will be reviewed regularly to ensure they still meet the CHC criteria.
Children’s forecast has worsened by £141k since month 5, now expected to overspend by £508k. This is due to 6 new continuing healthcare children who have started in 2017/18.
Reviews of high cost placements have been requested from the provider and the position will be monitored closely.
Mental Health budgets meet the 2.67% Mental Health Investment Standard (MHIS) requirement. Investment funds will be fully committed by year end. Mental Health Placements forecast underspend has reduced to £144k in Sept due to a Personality Disorder patient leaving an acute ward and an additional forensic patient in locked rehabilitation. Uncertainty still remains over joint funded RBK placements and a number of NHS England specialised and Transforming Care Partnerships (TCP) placements. Risk therefore remains on this budget, however if risks do not materialise, the underspend will be reinvested.
MHIS will be monitored throughout the year to ensure the required investment into mental health services is achieved. Regular meetings with Royal Borough of Kingston to monitor and progress. Routine updates received from commissioners for any changes in NHS commissioning.
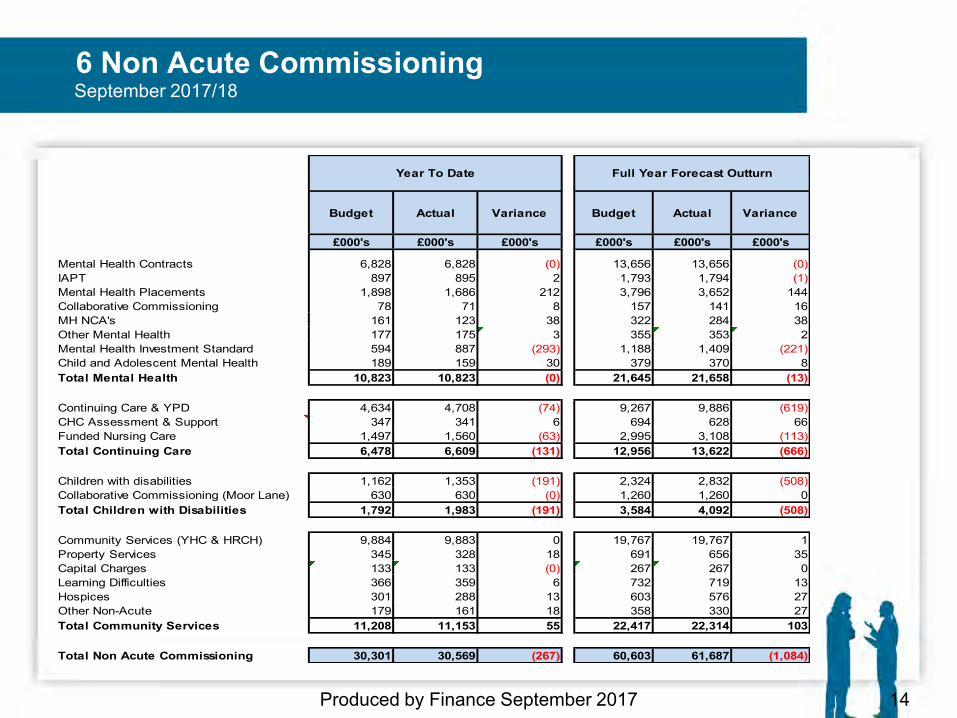
6 Non Acute Commissioning September 2017/18
14 Produced by Finance September 2017
Budget Actual Variance Budget Actual Variance
£000's £000's £000's £000's £000's £000's
Mental Health Contracts 6,828 6,828 (0) 13,656 13,656 (0)IAPT 897 895 2 1,793 1,794 (1)Mental Health Placements 1,898 1,686 212 3,796 3,652 144Collaborative Commissioning 78 71 8 157 141 16MH NCA's 161 123 38 322 284 38Other Mental Health 177 175 3 355 353 2Mental Health Investment Standard 594 887 (293) 1,188 1,409 (221)Child and Adolescent Mental Health 189 159 30 379 370 8Total Mental Health 10,823 10,823 (0) 21,645 21,658 (13)
Continuing Care & YPD 4,634 4,708 (74) 9,267 9,886 (619)CHC Assessment & Support 347 341 6 694 628 66Funded Nursing Care 1,497 1,560 (63) 2,995 3,108 (113)Total Continuing Care 6,478 6,609 (131) 12,956 13,622 (666)
Children with disabilities 1,162 1,353 (191) 2,324 2,832 (508)Collaborative Commissioning (Moor Lane) 630 630 (0) 1,260 1,260 0Total Children with Disabilities 1,792 1,983 (191) 3,584 4,092 (508)
Community Services (YHC & HRCH) 9,884 9,883 0 19,767 19,767 1Property Services 345 328 18 691 656 35Capital Charges 133 133 (0) 267 267 0Learning Difficulties 366 359 6 732 719 13Hospices 301 288 13 603 576 27Other Non-Acute 179 161 18 358 330 27Total Community Services 11,208 11,153 55 22,417 22,314 103
Total Non Acute Commissioning 30,301 30,569 (267) 60,603 61,687 (1,084)
Year To Date Full Year Forecast Outturn
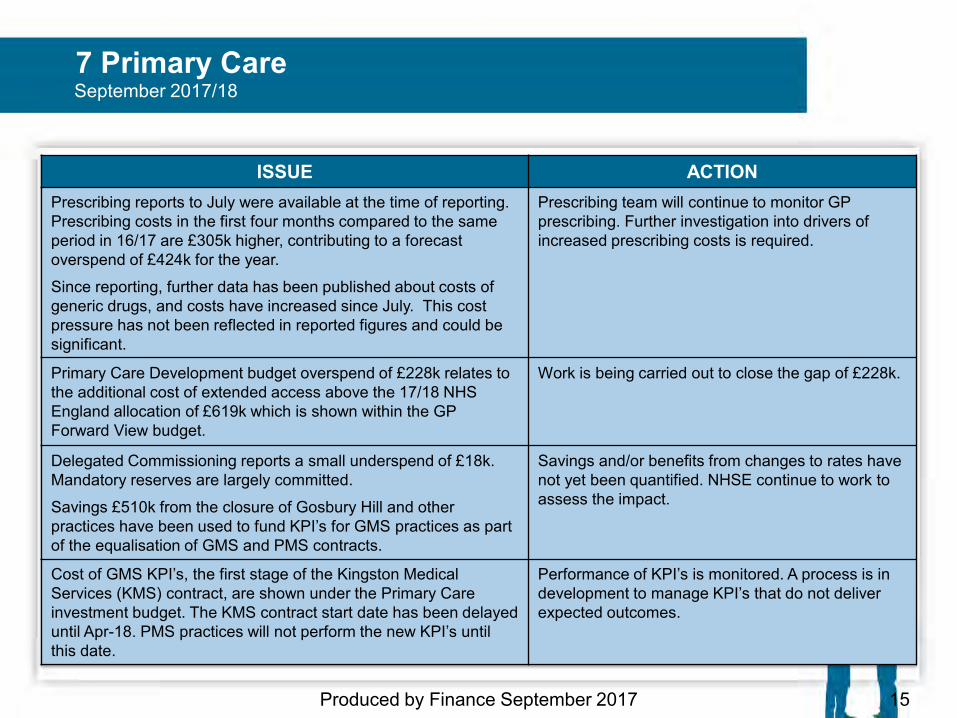
7 Primary Care
Produced by Finance September 2017 15
September 2017/18
ISSUE ACTION Prescribing reports to July were available at the time of reporting. Prescribing costs in the first four months compared to the same period in 16/17 are £305k higher, contributing to a forecast overspend of £424k for the year.
Since reporting, further data has been published about costs of generic drugs, and costs have increased since July. This cost pressure has not been reflected in reported figures and could be significant.
Prescribing team will continue to monitor GP prescribing. Further investigation into drivers of increased prescribing costs is required.
Primary Care Development budget overspend of £228k relates to the additional cost of extended access above the 17/18 NHS England allocation of £619k which is shown within the GP Forward View budget.
Work is being carried out to close the gap of £228k.
Delegated Commissioning reports a small underspend of £18k. Mandatory reserves are largely committed.
Savings £510k from the closure of Gosbury Hill and other practices have been used to fund KPI’s for GMS practices as part of the equalisation of GMS and PMS contracts.
Savings and/or benefits from changes to rates have not yet been quantified. NHSE continue to work to assess the impact.
Cost of GMS KPI’s, the first stage of the Kingston Medical Services (KMS) contract, are shown under the Primary Care investment budget. The KMS contract start date has been delayed until Apr-18. PMS practices will not perform the new KPI’s until this date.
Performance of KPI’s is monitored. A process is in development to manage KPI’s that do not deliver expected outcomes.
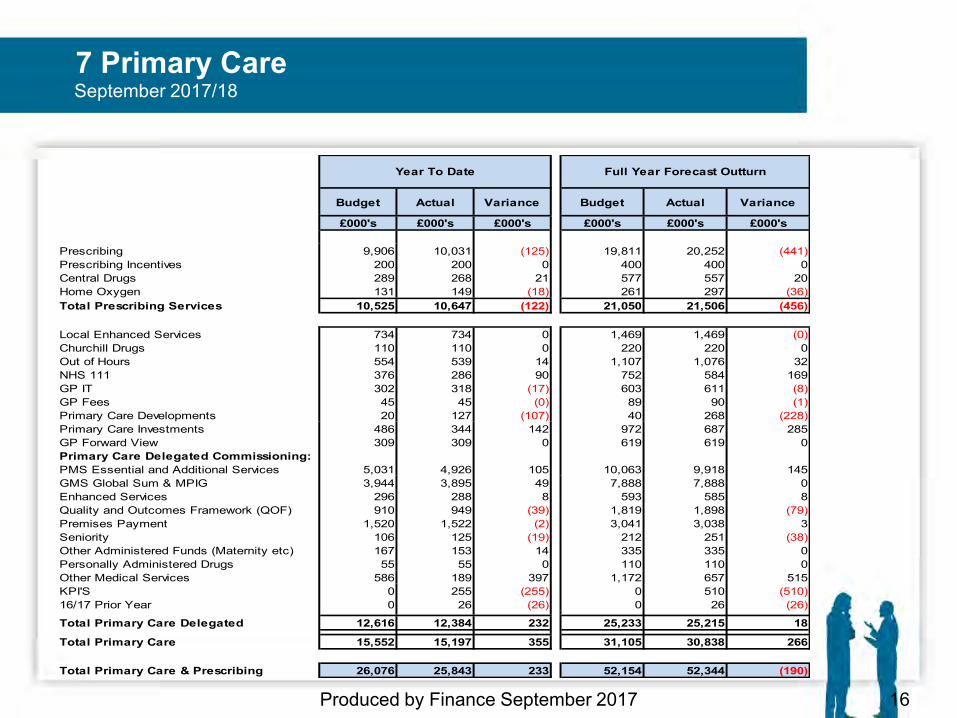
7 Primary Care
16 Produced by Finance September 2017
September 2017/18
Budget Actual Variance Budget Actual Variance
£000's £000's £000's £000's £000's £000's
Prescribing 9,906 10,031 (125) 19,811 20,252 (441)Prescribing Incentives 200 200 0 400 400 0Central Drugs 289 268 21 577 557 20Home Oxygen 131 149 (18) 261 297 (36)Total Prescribing Services 10,525 10,647 (122) 21,050 21,506 (456)
Local Enhanced Services 734 734 0 1,469 1,469 (0)Churchill Drugs 110 110 0 220 220 0Out of Hours 554 539 14 1,107 1,076 32NHS 111 376 286 90 752 584 169GP IT 302 318 (17) 603 611 (8)GP Fees 45 45 (0) 89 90 (1)Primary Care Developments 20 127 (107) 40 268 (228)Primary Care Investments 486 344 142 972 687 285GP Forward View 309 309 0 619 619 0Primary Care Delegated Commissioning:PMS Essential and Additional Services 5,031 4,926 105 10,063 9,918 145GMS Global Sum & MPIG 3,944 3,895 49 7,888 7,888 0Enhanced Services 296 288 8 593 585 8Quality and Outcomes Framework (QOF) 910 949 (39) 1,819 1,898 (79)Premises Payment 1,520 1,522 (2) 3,041 3,038 3Seniority 106 125 (19) 212 251 (38)Other Administered Funds (Maternity etc) 167 153 14 335 335 0Personally Administered Drugs 55 55 0 110 110 0Other Medical Services 586 189 397 1,172 657 515KPI'S 0 255 (255) 0 510 (510)16/17 Prior Year 0 26 (26) 0 26 (26)
Total Primary Care Delegated 12,616 12,384 232 25,233 25,215 18
Total Primary Care 15,552 15,197 355 31,105 30,838 266
Total Primary Care & Prescribing 26,076 25,843 233 52,154 52,344 (190)
Year To Date Full Year Forecast Outturn
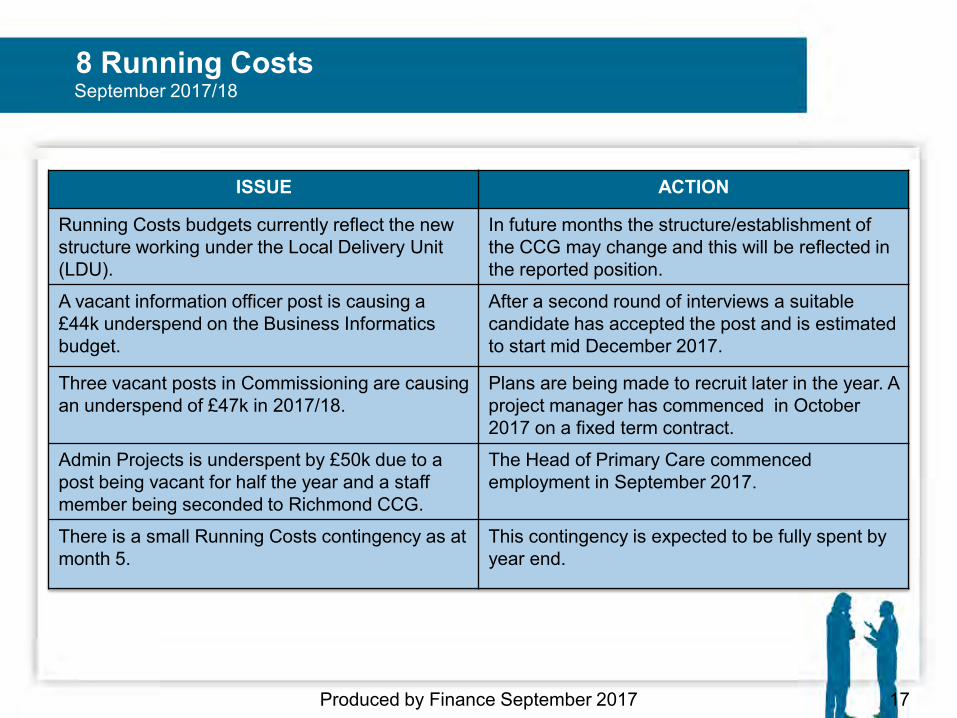
8 Running Costs
Produced by Finance September 2017 17
September 2017/18
ISSUE ACTION
Running Costs budgets currently reflect the new structure working under the Local Delivery Unit (LDU).
In future months the structure/establishment of the CCG may change and this will be reflected in the reported position.
A vacant information officer post is causing a £44k underspend on the Business Informatics budget.
After a second round of interviews a suitable candidate has accepted the post and is estimated to start mid December 2017.
Three vacant posts in Commissioning are causing an underspend of £47k in 2017/18.
Plans are being made to recruit later in the year. A project manager has commenced in October 2017 on a fixed term contract.
Admin Projects is underspent by £50k due to a post being vacant for half the year and a staff member being seconded to Richmond CCG.
The Head of Primary Care commenced employment in September 2017.
There is a small Running Costs contingency as at month 5.
This contingency is expected to be fully spent by year end.
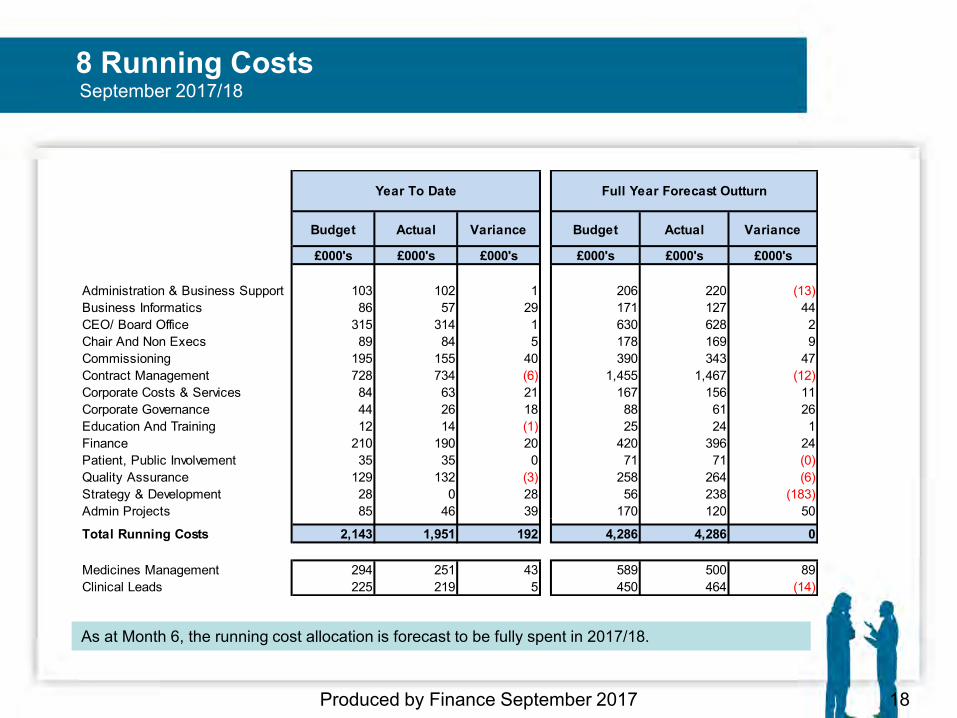
8 Running Costs
18 Produced by Finance September 2017
As at Month 6, the running cost allocation is forecast to be fully spent in 2017/18.
September 2017/18
Budget Actual Variance Budget Actual Variance
£000's £000's £000's £000's £000's £000's
Administration & Business Support 103 102 1 206 220 (13)Business Informatics 86 57 29 171 127 44CEO/ Board Office 315 314 1 630 628 2Chair And Non Execs 89 84 5 178 169 9Commissioning 195 155 40 390 343 47Contract Management 728 734 (6) 1,455 1,467 (12)Corporate Costs & Services 84 63 21 167 156 11Corporate Governance 44 26 18 88 61 26Education And Training 12 14 (1) 25 24 1Finance 210 190 20 420 396 24Patient, Public Involvement 35 35 0 71 71 (0)Quality Assurance 129 132 (3) 258 264 (6)Strategy & Development 28 0 28 56 238 (183)Admin Projects 85 46 39 170 120 50
Total Running Costs 2,143 1,951 192 4,286 4,286 0
Medicines Management 294 251 43 589 500 89Clinical Leads 225 219 5 450 464 (14)
Year To Date Full Year Forecast Outturn
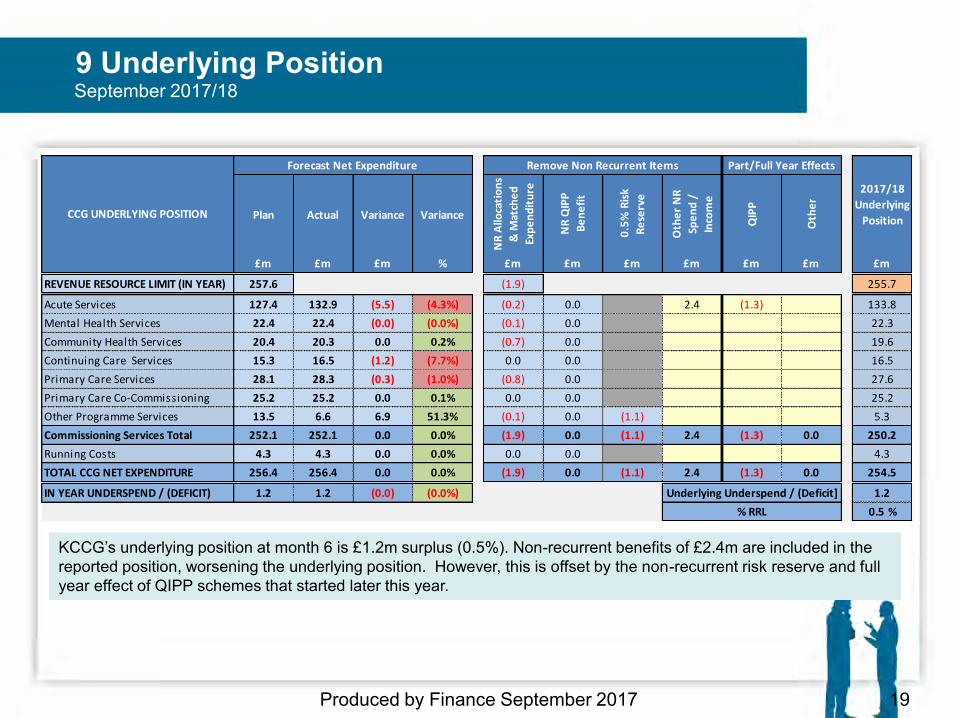
9 Underlying Position
Produced by Finance September 2017 19
KCCG’s underlying position at month 6 is £1.2m surplus (0.5%). Non-recurrent benefits of £2.4m are included in the reported position, worsening the underlying position. However, this is offset by the non-recurrent risk reserve and full year effect of QIPP schemes that started later this year.
September 2017/18
Plan Actual Variance Variance
NR
Allo
cati
on
s
& M
atch
ed
Exp
en
dit
ure
NR
QIP
P
Be
ne
fit
0.5
% R
isk
Re
serv
e
Oth
er
NR
Spe
nd
/
Inco
me
QIP
P
Oth
er
£m £m £m % £m £m £m £m £m £m £m
REVENUE RESOURCE LIMIT (IN YEAR) 257.6 (1.9) 255.7
Acute Services 127.4 132.9 (5.5) (4.3%) (0.2) 0.0 2.4 (1.3) 133.8
Mental Health Services 22.4 22.4 (0.0) (0.0%) (0.1) 0.0 22.3
Community Health Services 20.4 20.3 0.0 0.2% (0.7) 0.0 19.6
Continuing Care Services 15.3 16.5 (1.2) (7.7%) 0.0 0.0 16.5
Primary Care Services 28.1 28.3 (0.3) (1.0%) (0.8) 0.0 27.6
Primary Care Co-Commissioning 25.2 25.2 0.0 0.1% 0.0 0.0 25.2
Other Programme Services 13.5 6.6 6.9 51.3% (0.1) 0.0 (1.1) 5.3
Commissioning Services Total 252.1 252.1 0.0 0.0% (1.9) 0.0 (1.1) 2.4 (1.3) 0.0 250.2
Running Costs 4.3 4.3 0.0 0.0% 0.0 0.0 4.3
TOTAL CCG NET EXPENDITURE 256.4 256.4 0.0 0.0% (1.9) 0.0 (1.1) 2.4 (1.3) 0.0 254.5
IN YEAR UNDERSPEND / (DEFICIT) 1.2 1.2 (0.0) (0.0%) 1.2
0.5 %
Underlying Underspend / (Deficit]
% RRL
CCG UNDERLYING POSITION
Forecast Net Expenditure Remove Non Recurrent Items Part/Full Year Effects
2017/18
Underlying
Position
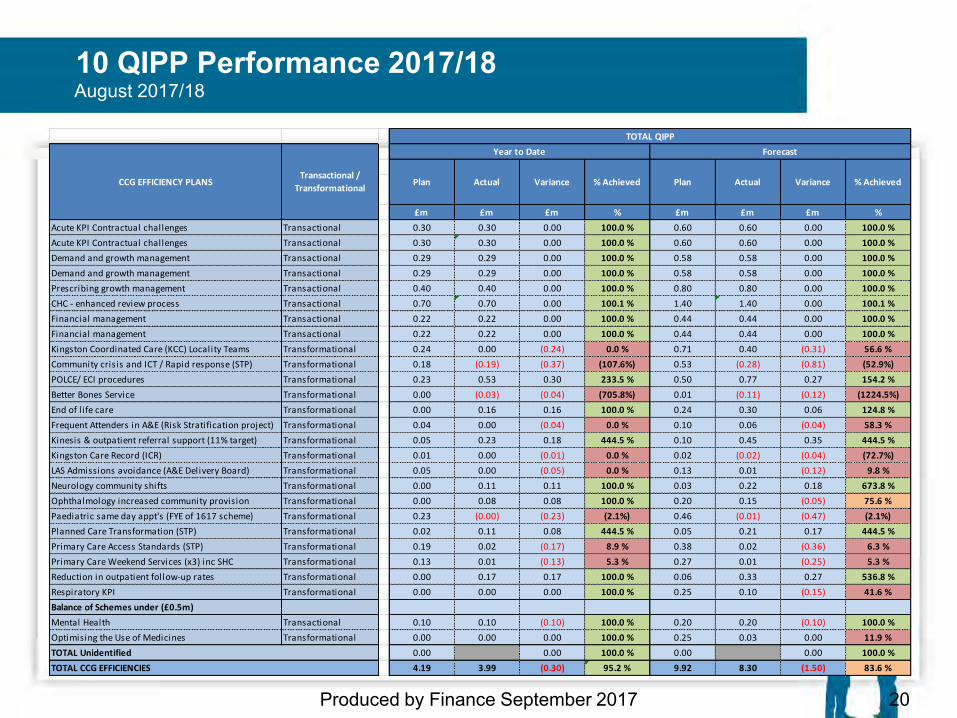
10 QIPP Performance 2017/18
20 Produced by Finance September 2017
August 2017/18
£m £m £m % £m £m £m %
Acute KPI Contractual challenges Transactional 0.30 0.30 0.00 100.0 % 0.60 0.60 0.00 100.0 %
Acute KPI Contractual challenges Transactional 0.30 0.30 0.00 100.0 % 0.60 0.60 0.00 100.0 %
Demand and growth management Transactional 0.29 0.29 0.00 100.0 % 0.58 0.58 0.00 100.0 %
Demand and growth management Transactional 0.29 0.29 0.00 100.0 % 0.58 0.58 0.00 100.0 %
Prescribing growth management Transactional 0.40 0.40 0.00 100.0 % 0.80 0.80 0.00 100.0 %
CHC - enhanced review process Transactional 0.70 0.70 0.00 100.1 % 1.40 1.40 0.00 100.1 %
Financial management Transactional 0.22 0.22 0.00 100.0 % 0.44 0.44 0.00 100.0 %
Financial management Transactional 0.22 0.22 0.00 100.0 % 0.44 0.44 0.00 100.0 %
Kingston Coordinated Care (KCC) Locality Teams Transformational 0.24 0.00 (0.24) 0.0 % 0.71 0.40 (0.31) 56.6 %
Community crisis and ICT / Rapid response (STP) Transformational 0.18 (0.19) (0.37) (107.6%) 0.53 (0.28) (0.81) (52.9%)
POLCE/ ECI procedures Transformational 0.23 0.53 0.30 233.5 % 0.50 0.77 0.27 154.2 %
Better Bones Service Transformational 0.00 (0.03) (0.04) (705.8%) 0.01 (0.11) (0.12) (1224.5%)
End of l ife care Transformational 0.00 0.16 0.16 100.0 % 0.24 0.30 0.06 124.8 %
Frequent Attenders in A&E (Risk Stratification project) Transformational 0.04 0.00 (0.04) 0.0 % 0.10 0.06 (0.04) 58.3 %
Kinesis & outpatient referral support (11% target) Transformational 0.05 0.23 0.18 444.5 % 0.10 0.45 0.35 444.5 %
Kingston Care Record (ICR) Transformational 0.01 0.00 (0.01) 0.0 % 0.02 (0.02) (0.04) (72.7%)
LAS Admissions avoidance (A&E Delivery Board) Transformational 0.05 0.00 (0.05) 0.0 % 0.13 0.01 (0.12) 9.8 %
Neurology community shifts Transformational 0.00 0.11 0.11 100.0 % 0.03 0.22 0.18 673.8 %
Ophthalmology increased community provision Transformational 0.00 0.08 0.08 100.0 % 0.20 0.15 (0.05) 75.6 %
Paediatric same day appt's (FYE of 1617 scheme) Transformational 0.23 (0.00) (0.23) (2.1%) 0.46 (0.01) (0.47) (2.1%)
Planned Care Transformation (STP) Transformational 0.02 0.11 0.08 444.5 % 0.05 0.21 0.17 444.5 %
Primary Care Access Standards (STP) Transformational 0.19 0.02 (0.17) 8.9 % 0.38 0.02 (0.36) 6.3 %
Primary Care Weekend Services (x3) inc SHC Transformational 0.13 0.01 (0.13) 5.3 % 0.27 0.01 (0.25) 5.3 %
Reduction in outpatient follow-up rates Transformational 0.00 0.17 0.17 100.0 % 0.06 0.33 0.27 536.8 %
Respiratory KPI Transformational 0.00 0.00 0.00 100.0 % 0.25 0.10 (0.15) 41.6 %
Balance of Schemes under (£0.5m)
Mental Health Transactional 0.10 0.10 (0.10) 100.0 % 0.20 0.20 (0.10) 100.0 %
Optimising the Use of Medicines Transformational 0.00 0.00 0.00 100.0 % 0.25 0.03 0.00 11.9 %
0.00 0.00 100.0 % 0.00 0.00 100.0 %
4.19 3.99 (0.30) 95.2 % 9.92 8.30 (1.50) 83.6 %
Transactional /
Transformational
TOTAL QIPP
Year to Date Forecast
Plan Actual Variance
TOTAL CCG EFFICIENCIES
% Achieved Plan Actual Variance % Achieved
TOTAL Unidentified
CCG EFFICIENCY PLANS
10 QIPP Performance 2017/18
21 Produced by Finance September 2017
August 2017/18
• The table on p22 reflects the forecasted Quality, Innovation, Productivity and Prevention (QIPP) position based on M1-5 data for all QIPP schemes.
• The overall QIPP forecast shows an expected under achievement of £1.5m based on savings seen year to date. 11 QIPP schemes are RAG rated red and forecast to under-achieve significantly against plan. Action plans are in development for all schemes that are expected to under-achieve against savings target.
• Kingston Coordinated Care (KCC) Locality Teams is forecast to achieve 56.6% of its planned target due to a delay in project roll out. The pilot phase is now complete and awaiting evaluation. The team are establishing commissioner provider meetings and as part of this will identify KPIs.
• Community crisis and ICT / Rapid response (STP) has not seen any savings, and is forecast to cost the CCG £0.28m. The poor performance was discussed at last contract review meeting. It was agreed to review emergency admissions and provide an updated plan to address the under achievement in this scheme
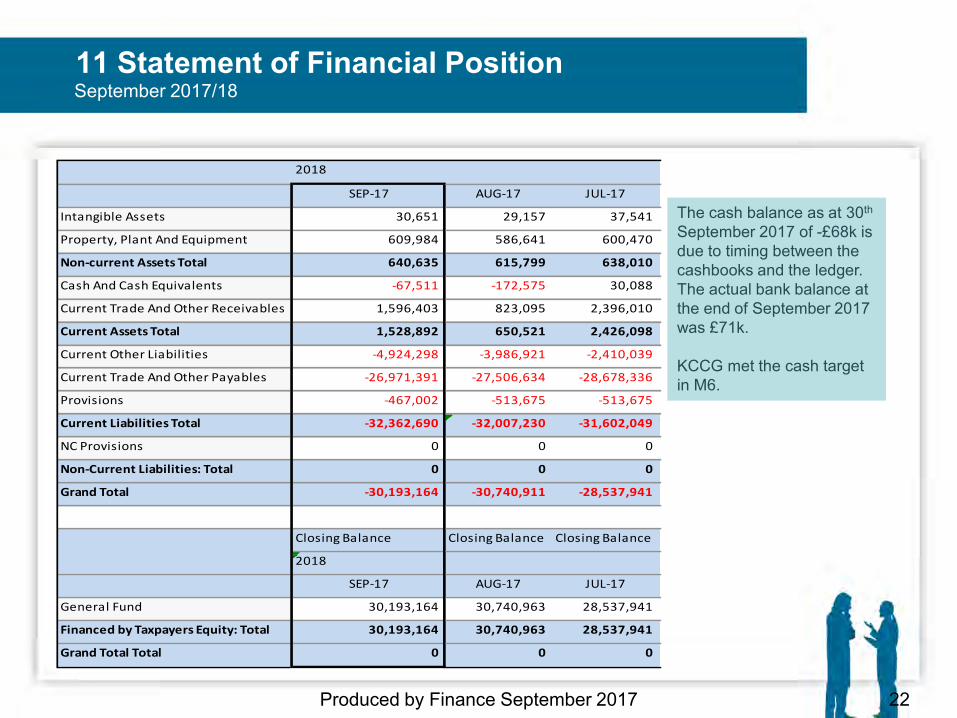
11 Statement of Financial Position
22 Produced by Finance September 2017
The cash balance as at 30th September 2017 of -£68k is due to timing between the cashbooks and the ledger. The actual bank balance at the end of September 2017 was £71k. KCCG met the cash target in M6.
September 2017/18
2018
SEP-17 AUG-17 JUL-17
Intangible Assets 30,651 29,157 37,541
Property, Plant And Equipment 609,984 586,641 600,470
Non-current Assets Total 640,635 615,799 638,010
Cash And Cash Equivalents -67,511 -172,575 30,088
Current Trade And Other Receivables 1,596,403 823,095 2,396,010
Current Assets Total 1,528,892 650,521 2,426,098
Current Other Liabilities -4,924,298 -3,986,921 -2,410,039
Current Trade And Other Payables -26,971,391 -27,506,634 -28,678,336
Provisions -467,002 -513,675 -513,675
Current Liabilities Total -32,362,690 -32,007,230 -31,602,049
NC Provisions 0 0 0
Non-Current Liabilities: Total 0 0 0
Grand Total -30,193,164 -30,740,911 -28,537,941
Closing Balance Closing Balance Closing Balance
2018
SEP-17 AUG-17 JUL-17
General Fund 30,193,164 30,740,963 28,537,941
Financed by Taxpayers Equity: Total 30,193,164 30,740,963 28,537,941
Grand Total Total 0 0 0
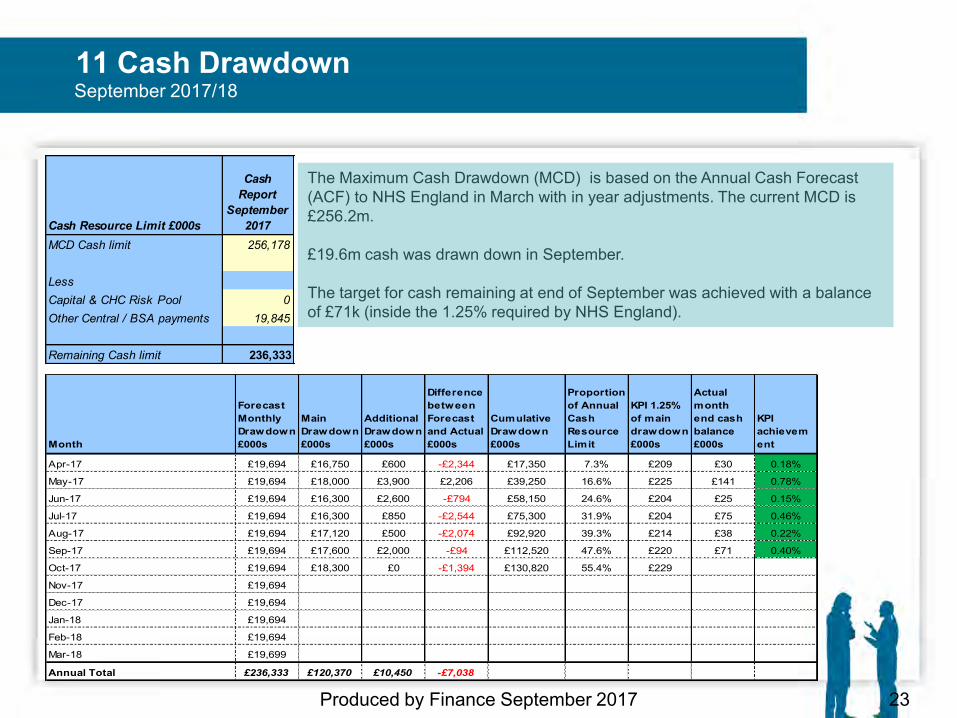
11 Cash Drawdown
23 Produced by Finance September 2017
September 2017/18
The Maximum Cash Drawdown (MCD) is based on the Annual Cash Forecast (ACF) to NHS England in March with in year adjustments. The current MCD is £256.2m. £19.6m cash was drawn down in September. The target for cash remaining at end of September was achieved with a balance of £71k (inside the 1.25% required by NHS England).
Cash Resource Limit £000s
Cash Report
September 2017
MCD Cash limit 256,178
LessCapital & CHC Risk Pool 0Other Central / BSA payments 19,845
Remaining Cash limit 236,333
Month
Forecast Monthly Drawdown £000s
Main Drawdown £000s
Additional Drawdown £000s
Difference between Forecast and Actual £000s
Cumulative Drawdown £000s
Proportion of Annual Cash Resource Limit
KPI 1.25% of main drawdown £000s
Actual month end cash balance £000s
KPI achievement
Apr-17 £19,694 £16,750 £600 -£2,344 £17,350 7.3% £209 £30 0.18%
May-17 £19,694 £18,000 £3,900 £2,206 £39,250 16.6% £225 £141 0.78%
Jun-17 £19,694 £16,300 £2,600 -£794 £58,150 24.6% £204 £25 0.15%
Jul-17 £19,694 £16,300 £850 -£2,544 £75,300 31.9% £204 £75 0.46%
Aug-17 £19,694 £17,120 £500 -£2,074 £92,920 39.3% £214 £38 0.22%
Sep-17 £19,694 £17,600 £2,000 -£94 £112,520 47.6% £220 £71 0.40%
Oct-17 £19,694 £18,300 £0 -£1,394 £130,820 55.4% £229
Nov-17 £19,694
Dec-17 £19,694
Jan-18 £19,694
Feb-18 £19,694
Mar-18 £19,699
Annual Total £236,333 £120,370 £10,450 -£7,038
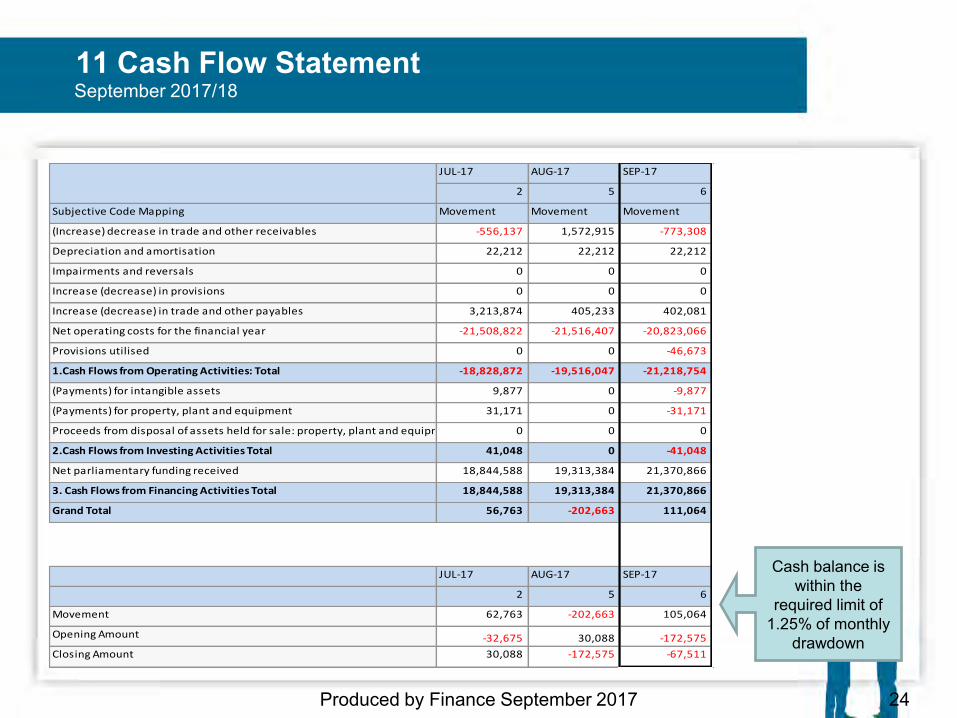
11 Cash Flow Statement
24 Produced by Finance September 2017
Cash balance is within the
required limit of 1.25% of monthly
drawdown
September 2017/18
JUL-17 AUG-17 SEP-17
2 5 6
Subjective Code Mapping Movement Movement Movement
(Increase) decrease in trade and other receivables -556,137 1,572,915 -773,308
Depreciation and amortisation 22,212 22,212 22,212
Impairments and reversals 0 0 0
Increase (decrease) in provisions 0 0 0
Increase (decrease) in trade and other payables 3,213,874 405,233 402,081
Net operating costs for the financial year -21,508,822 -21,516,407 -20,823,066
Provisions utilised 0 0 -46,673
1.Cash Flows from Operating Activities: Total -18,828,872 -19,516,047 -21,218,754
(Payments) for intangible assets 9,877 0 -9,877
(Payments) for property, plant and equipment 31,171 0 -31,171
Proceeds from disposal of assets held for sale: property, plant and equipment 0 0 0
2.Cash Flows from Investing Activities Total 41,048 0 -41,048
Net parliamentary funding received 18,844,588 19,313,384 21,370,866
3. Cash Flows from Financing Activities Total 18,844,588 19,313,384 21,370,866
Grand Total 56,763 -202,663 111,064
JUL-17 AUG-17 SEP-17
2 5 6
Movement 62,763 -202,663 105,064
Opening Amount -32,675 30,088 -172,575
Closing Amount 30,088 -172,575 -67,511
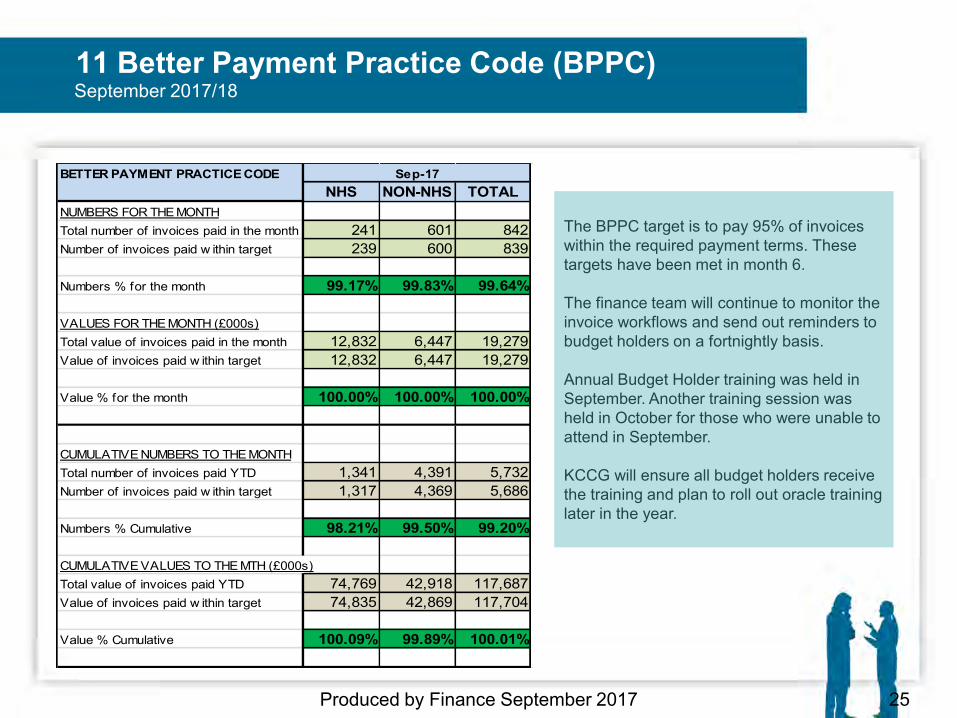
11 Better Payment Practice Code (BPPC)
25 Produced by Finance September 2017
The BPPC target is to pay 95% of invoices within the required payment terms. These targets have been met in month 6. The finance team will continue to monitor the invoice workflows and send out reminders to budget holders on a fortnightly basis. Annual Budget Holder training was held in September. Another training session was held in October for those who were unable to attend in September. KCCG will ensure all budget holders receive the training and plan to roll out oracle training later in the year.
September 2017/18
BETTER PAYMENT PRACTICE CODENHS NON-NHS TOTAL
NUMBERS FOR THE MONTHTotal number of invoices paid in the month 241 601 842Number of invoices paid w ithin target 239 600 839
Numbers % for the month 99.17% 99.83% 99.64%
VALUES FOR THE MONTH (£000s)Total value of invoices paid in the month 12,832 6,447 19,279Value of invoices paid w ithin target 12,832 6,447 19,279
Value % for the month 100.00% 100.00% 100.00%
CUMULATIVE NUMBERS TO THE MONTHTotal number of invoices paid YTD 1,341 4,391 5,732Number of invoices paid w ithin target 1,317 4,369 5,686
Numbers % Cumulative 98.21% 99.50% 99.20%
CUMULATIVE VALUES TO THE MTH (£000s)Total value of invoices paid YTD 74,769 42,918 117,687Value of invoices paid w ithin target 74,835 42,869 117,704
Value % Cumulative 100.09% 99.89% 100.01%
Sep-17
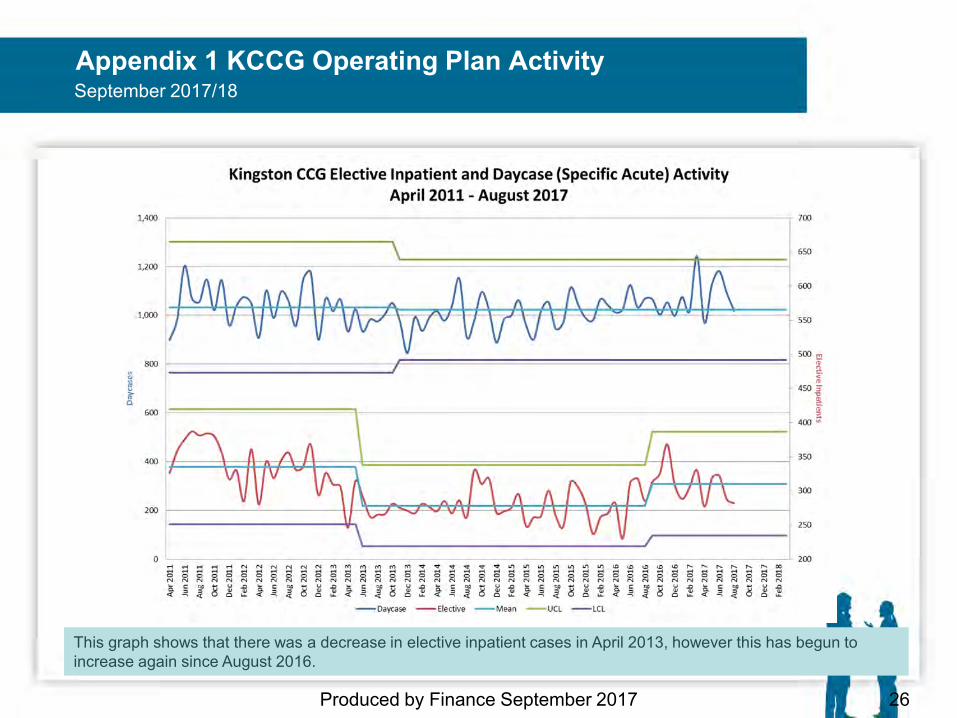
Appendix 1 KCCG Operating Plan Activity
Produced by Finance September 2017 26
September 2017/18
This graph shows that there was a decrease in elective inpatient cases in April 2013, however this has begun to increase again since August 2016.
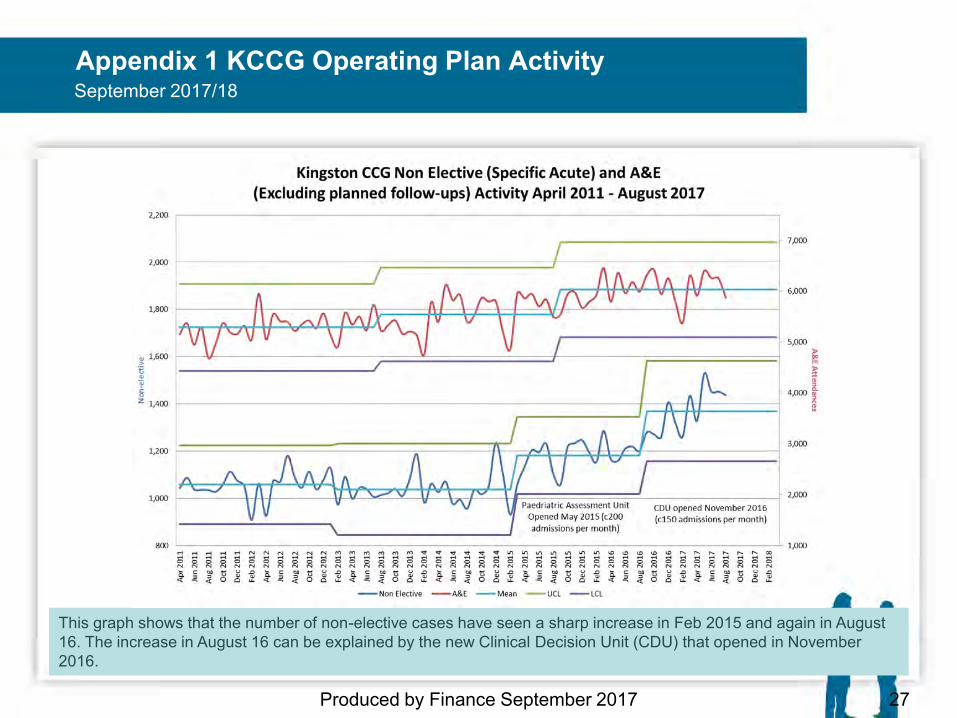
Appendix 1 KCCG Operating Plan Activity
Produced by Finance September 2017 27
September 2017/18
This graph shows that the number of non-elective cases have seen a sharp increase in Feb 2015 and again in August 16. The increase in August 16 can be explained by the new Clinical Decision Unit (CDU) that opened in November 2016.
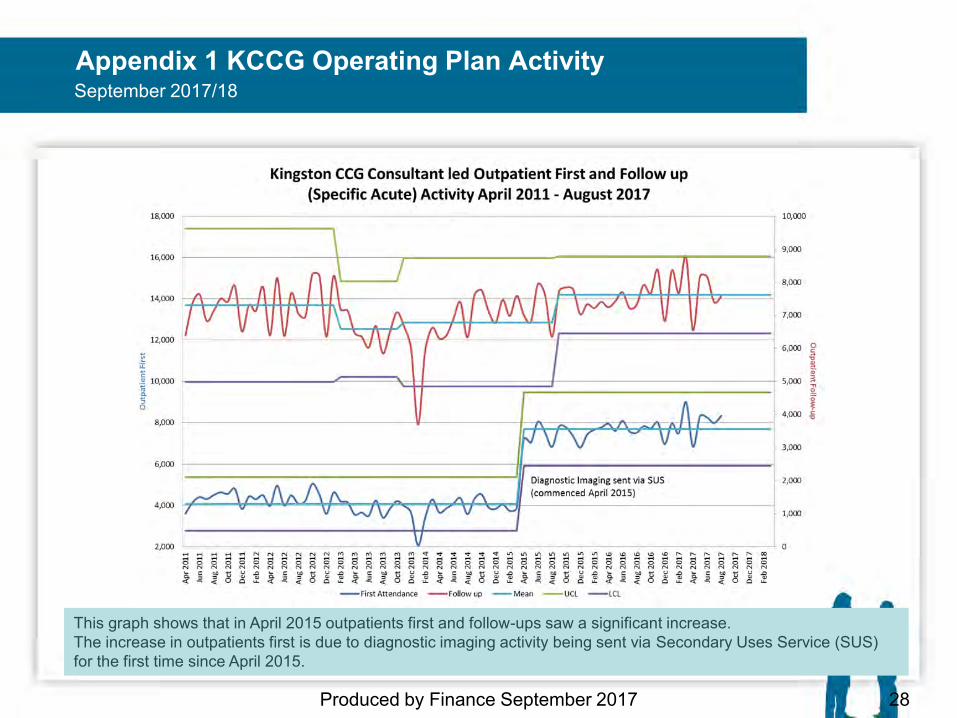
Appendix 1 KCCG Operating Plan Activity
Produced by Finance September 2017 28
September 2017/18
This graph shows that in April 2015 outpatients first and follow-ups saw a significant increase. The increase in outpatients first is due to diagnostic imaging activity being sent via Secondary Uses Service (SUS) for the first time since April 2015.
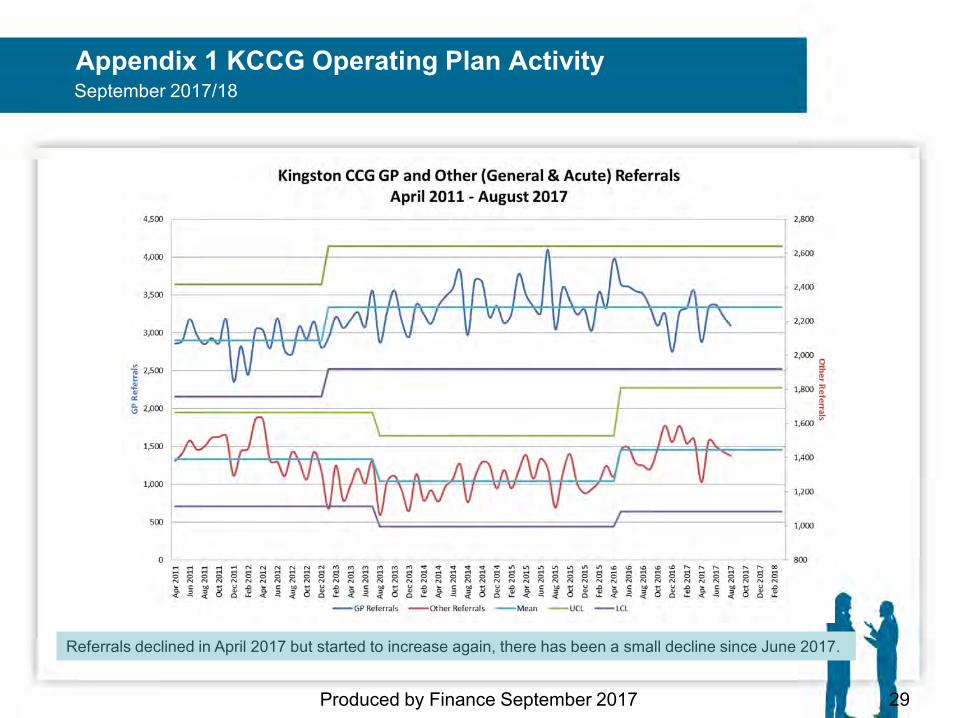
Appendix 1 KCCG Operating Plan Activity
Produced by Finance September 2017 29
September 2017/18
Referrals declined in April 2017 but started to increase again, there has been a small decline since June 2017.
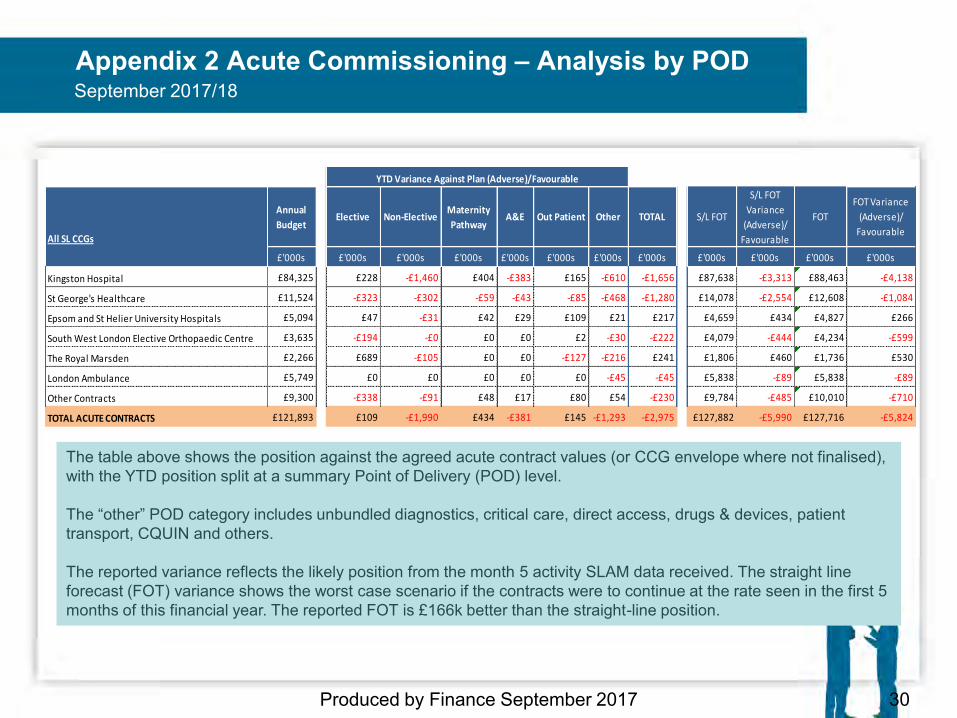
Appendix 2 Acute Commissioning – Analysis by POD
Produced by Finance September 2017 30
September 2017/18
The table above shows the position against the agreed acute contract values (or CCG envelope where not finalised), with the YTD position split at a summary Point of Delivery (POD) level. The “other” POD category includes unbundled diagnostics, critical care, direct access, drugs & devices, patient transport, CQUIN and others. The reported variance reflects the likely position from the month 5 activity SLAM data received. The straight line forecast (FOT) variance shows the worst case scenario if the contracts were to continue at the rate seen in the first 5 months of this financial year. The reported FOT is £166k better than the straight-line position.
All SL CCGs
Annual
BudgetElective Non-Elective
Maternity
PathwayA&E Out Patient Other TOTAL S/L FOT
S/L FOT
Variance
(Adverse)/
Favourable
FOT
FOT Variance
(Adverse)/
Favourable
£'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s £'000s
Kingston Hospital £84,325 £228 -£1,460 £404 -£383 £165 -£610 -£1,656 £87,638 -£3,313 £88,463 -£4,138
St George's Healthcare £11,524 -£323 -£302 -£59 -£43 -£85 -£468 -£1,280 £14,078 -£2,554 £12,608 -£1,084
Epsom and St Helier University Hospitals £5,094 £47 -£31 £42 £29 £109 £21 £217 £4,659 £434 £4,827 £266
South West London Elective Orthopaedic Centre £3,635 -£194 -£0 £0 £0 £2 -£30 -£222 £4,079 -£444 £4,234 -£599
The Royal Marsden £2,266 £689 -£105 £0 £0 -£127 -£216 £241 £1,806 £460 £1,736 £530
London Ambulance £5,749 £0 £0 £0 £0 £0 -£45 -£45 £5,838 -£89 £5,838 -£89
Other Contracts £9,300 -£338 -£91 £48 £17 £80 £54 -£230 £9,784 -£485 £10,010 -£710
TOTAL ACUTE CONTRACTS £121,893 £109 -£1,990 £434 -£381 £145 -£1,293 -£2,975 £127,882 -£5,990 £127,716 -£5,824
YTD Variance Against Plan (Adverse)/Favourable
Version: Final M - 1 Date: 30 10 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Council of Members Report
Agenda Item 14 Attachment
M
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Dr Atin Goel, Chair, Council of Members
Presented by: (name & job title)
Dr Atin Goel, Chair, Council of Members
Summary and purpose of report The Council of Members has met twice since the last Governing Body meeting, with good practice representation at both meetings. The first meeting was held on the 12th September 2017 and the appointment of Vice Chair for the Council of Members was confirmed as Dr Adel Kartas with effect from October 2017. Vicki Harvey-Piper, the Local Director of Corporate Affairs and Governance for Kingston and Richmond CCGs, also sought approval from members on the revisions to Kingston CCG’s Constitution to reflect the creation of the South West London Alliance. A demonstration was given of a newly created Excel workbook containing practice level referral information. Kathryn MacDermott, the Local Director of Primary Care and Planning for Kingston and Richmond CCGs also gave her regular update on primary care issues which included the list of new KPIs.
The second meeting was held on 10th October 2017 and Mr Alan Jones, Associate Medical Director at Kingston Hospital attended. A presentation was given by Nick Merrifield on Kingston Co-ordinated Care, and risk stratification KPI. Presentations were also given on Clinical Practice Research Datalink by Stuart Fordyce, MHRA; on Managing Clinical correspondence by India Peach; and on the Respiratory KPI by David Mphanza.
A primary care update was also provided by Kathryn MacDermott.
Key sections for particular note Our next meeting is being held on 14th November 2017 Report recommendation The Governing Body is asked to note the report.
Version: Final M - 2 Date: 30 10 17
Financial and / or resource implications None. Key risks identified & mitigation None. Equality and / or privacy impact analysis N/A. Committees that have previously discussed / agreed the report and outcomes Council of Members. Communication plan / stakeholder involvement / patient engagement Assurance Does the report need to be taken to any additional meetings for further assurance or ratification? No CORPORATE OBJECTIVES 2016-18 Please indicate below all the categories which the paper provides evidence for:
1. Better Health
2. Better Care
3. Sustainability
4. Leadership
5. Engagement
Version: Final N - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Audit Committee Minutes
Agenda Item 15 Attachment
N
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Paul Gallagher, Audit Committee Chair & Lay Member
Presented by: (name & job title)
Paul Gallagher Audit Committee Chair & Lay Member
MINUTES OF THE AUDIT COMMITTEE HELD ON MONDAY 24 JULY 2017
CONFERENCE ROOM, 3rd FLOOR, GUILDHALL 1 PRESENT: Jim Smyllie Lay Member David Knowles Lay Member Dr Annette Pautz Governing Body GP IN ATTENDANCE: Nick Atkinson RSM UK Lianna Parker-Carn LCFS RSM UK Gemma Higginson LCFS RSM UK Jenny Sinnott Head of Finance Andy Conlan Engagement Manager, Grant Thornton Dr Phil Moore Deputy Chair – Clinical Jo Dandridge Business Manager – Minutes APOLOGIES: Paul Gallagher (Chair) Lay Member Dr Naeem Iqbal Governing Body GP Yarlini Roberts Local Director of Finance Tonia Michaelides Managing Director, Kingston & Richmond CCGs Dr Naz Jivani Governing Body Chair James Murray Interim Chief Finance Officer, SWL Alliance Iain Murray Associate Director, Grant Thornton Vicki Harvey-Piper Local Director of Corporate Affairs & Governance Michael Mulligan SE CSU
Version: Final N - 2 Date: 01 11 17
17/40 Welcome and Introductions: Those present were welcomed to the meeting. 17/41 Minutes of the previous meetings: The Minutes of the last meeting held on Monday, 22nd May 2017 were agreed as an accurate record. 17/42 Declarations of any possible conflicts of interest arising:
There were no declarations. 17/43 Matters Arising None. 17/44 In Year Surplus Reporting
Members received a note which clarified the requirements for reporting financial performance for 2017/18. Members noted that from 2017/18 onwards, NHS England will begin reporting CCG financial performance on an in-year basis and therefore any in-year surplus or deficit would be calculated as the difference between the in-year allocation (plus any pre-approved surplus drawdown) and total expenditure. CCGs were being asked to adopt the same basis of reporting. Members also noted that CCGs are still required to comply with the business rules to maintain a cumulative surplus of the higher of 1% of (in-year) allocation or the amount brought forward from the previous year if higher. Compliance with this requirement will be tested through the planning process as normal. Members recommended that the move to in year surplus be discussed with the auditors during the year to ensure that they understand the change and are able to appropriate interpret this in the context of their testing of the CCG’s compliance with its statutory duties. The Audit Committee NOTED the in-year surplus reporting update..
17/45 External Audit
Andy Conlan, Engagement Manager from Grant Thornton presented a copy of the Annual Audit Letter for 2016/17. Members noted the statutory requirement for the Annual Audit Letter to be presented to the committee as it contained a summary of the key findings from the work that had been carried out by the auditors relating to Kingston CCG. The Audit Committee RECEIVED the Annual Audit Letter for 2016/17 and noted the unqualified opinion given on the CCG’s financial statements.
17/46 Internal Audit
Progress Report Members received a report detailing the audit assignments that had been completed since the last Audit Committee meeting and the impact of those findings. In particular members noted the latest two finalised reports were the Board Assurance Framework audit which received a ‘Substantial Assurance’ rating and the Conflicts of Interest audit which received a ‘Reasonable Assurance’ rating. The Executive Summary for each audit had been included within the Progress Report.
Version: Final N - 3 Date: 01 11 17
Members noted that the action for formal conflicts of interest training to be in place for staff in relation to the update NHS England Conflicts of Interest guidelines had since been removed as NHS England had not yet launched the training. Audit Tracker Members received a copy of the Internal Audit Action Tracker for information. Benchmarking Report Members received a copy of the NHS Benchmarking of internal audit findings for 2016/17 and found this to be a useful tool which detailed a comparison with last year’s assurance levels together with other NHS organisations. RSM Health Matters A copy of the most recent ‘Health Matters’ had been circulated for information. Members’ attention was drawn to the General Data Protection Regulation (GDPR) legislation coming into force in the UK in May 2018 and noted this will have ramifications for how information can be shared, and will need careful consideration alongside the drive for more digital solutions with the ever present growing threats around cyber security. It was agreed that the Governing Body needed assurance that robust controls would be put in place to prevent any breaches of lost or stolen data; that mandatory breach notification stipulation would be adhered to; and that internal processes for reporting and management of efficient and transparent communications with affected individuals/patients would be implemented.
17/47 LCFS LCFS Annual Report Members received for information a copy of the annual report which provided a summary against NHS Protect’s anti fraud standards, based upon the work performed in line with the agreed annual work plan for 2016/17. Progress Report Members received the LCFS work plan for 2017/18 for information and noted that the one referral made to LCFS was being actioned by way of an internal CCG investigation and therefore the case status was pending closure with no further action required. Fraud Spotlight Conflicts of Interest A copy of a briefing had been circulated for information which captured the key points of NHS England’s guidance to help organisations effectively manage conflicts of interest and provide safeguards for its staff. Notice Fraud – June 2017 A copy of the most recent Notice Fraud newsletter had been circulated for information.
Version: Final N - 4 Date: 01 11 17
17/48 Write-Offs
Jenny Sinnott advised members that the CCG had an outstanding credit note with Fairhome Care Group Ltd for -£11,973.75 in relation to an invoice raised in error for a mental health placement patient in May 2013. The credit note cancelled the invoice in full, however the invoice and credit note were not approved at the same time and only the invoice was approved. The CCG has no other invoices with the supplier to offset the credit against and the care home has since gone into liquidation. The CCG has been advised that there will be no financial return to any class of creditor from the insolvent liquidation of Fairhome Care Group Ltd, therefore members were being asked to approve that this debt is written off. The Audit Committee APPROVED the write off of bad debt with Fairhome Care Group Ltd.
17/49 Tender Waivers None.
17/50 Any Other Business None. 17/51 Date of next meeting Tuesday, 26th September 2017
Version: Final O1 - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Finance Committee Minutes
Agenda Item 15 Attachment
O1
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Presented by: (name & job title)
MINUTES OF THE FINANCE COMMITTEE HELD ON MONDAY 24th JULY 2017 3rd FLOOR CONFERENCE ROOM,
GUILDHALL 1, KINGSTON PRESENT: David Knowles Lay Member & Vice Chair Jim Smyllie Lay Member Phil Moore Governing Body GP Annette Pautz Governing Body GP Naz Jivani Governing Body Chair Jenny Sinnott Head of Finance IN ATTENDANCE: Ben Okoye Dep Director of Finance, NEL CSU Laura Winder NEL CSU Julia Gosden Director of Commissioning Jo Dandridge Business Manager - Minutes APOLOGIES: James Murray Chief Finance Officer, SWL Alliance Tonia Michaelides Managing Director Yarlini Roberts Local Director of Finance, K&R LDU Paul Gallagher Lay Member & Audit Chair 17/147 WELCOME AND APOLOGIES: Those present were welcomed to the meeting. 17/148 DECLARATIONS OF INTEREST: There were no declarations. 17/149 MINUTES OF THE LAST FINANCE COMMITTEE MEETING
The minutes of the last meeting held on Monday 26th June 2017 were agreed as an accurate record.
Version: Final O1 - 2 Date: 01 11 17
17/150 MATTERS ARISING
None.
17/151 FINANCE REPORT – MONTH 3 A copy of the Month 3 Finance Report had been circulated.
Members noted that the SWL estates and space utilisation strategy is under review, with potential implications for Kingston CCG properties. Members were also presented with a summary of the Month 3 position as follows:
CCG expects to meet its planned in year 0.5% surplus of £1,151k Cash targets and Better Payment Practice Code statistics were met in Month
3 Capital PIDs have been approved by NHS England CCG is marginally behind target for QIPP year to date but working towards full
delivery in 2017/18 Non-recurrent allocations of £706k and recurrent allocations of £5k were
received in Month 3 Acute Commissioning Members were advised that the year to date overspend in acute commissioning was currently £928k however at month 3 this overspend was mitigated through reserve utilisation. Members also noted the variation in elective admissions had reduced in May 2017 due to a marked increase against plan at St George’s and a smaller increase against plan at Kingston Hospital. The variation year to date in non-elective admissions had increased in May 2017 mainly due to the delay in set up of locality teams in the Kingston Co-ordinated Care provider alliance and the activity increases relating to the CDU at Kingston Hospital. Non Acute Commissioning Mental Health Members were informed that mental health placements were overspent by £46k due to invoicing for a patient’s hospital stay. The invoices are in dispute and additional evidence has been requested from the provider. Continuing Care Members were informed that the year to date continuing care position showed an underspend of £225k however this was not expected to continue throughout the year. The continuing care team will continue to review CHC clients to ensure they still meet the CHC criteria. Primary Care Members noted that prescribing costs were low in April 2017 compared to the previous 2 years spend hence the reported year to date underspend. However it was expected that by year end there will be an overspend of £74k if historic trends are applied.
Version: Final O1 - 3 Date: 01 11 17
Members were informed that GP IT is forecast to overspend by £11k, the cost pressure due to NHS England transferring Health & Social Care Network portal costs to the CCG which exceeds the allocation received in Month 3. Members were also advised that Primary Care Delegated commissioning budgets in Month 3 is reporting a cost pressure for QOF and Seniority. However overall costs are still forecast to be within budget/allocation. Risks and Mitigations A list of risks and mitigations of the 2017/18 reported position updated as at Month 3 had been submitted to NHS England. The risk adjusted control total is a surplus of £1.17m, the CCG is still able to deliver the 0.5% planned in year surplus. QIPP Performance Members were informed that of the 26 QIPP schemes identified for 2017/18, there were 8 of these schemes rated as red. The end of life care QIPP scheme is still being worked up, there had been an issue with project resource that had caused some delays to this starting. Neurology community shifts QIPP scheme is still in progress and a SWL wide project for neurology services that is being looked at by the planned care team. Ophthalmology increased community position is not expected to start until later in the year, limited project resource has been an issue on this project. The Finance Committee NOTED the Month 3 Finance Report.
17/152 NEL CSU INTEGRATED REPORT Members received the Month 2 consolidated view of Kingston’s CCG contracting performance for information
17/153 2017-19 FINANCIAL PLAN
Members received details of the 2017-19 financial plan for approval. Members noted the final version of the financial plan had been submitted to NHS England on 30th March 2017. A copy of the assurance feedback from NHS England recently received confirming that our financial plans were assured was tabled for information. The plan submitted reported meeting all business rules in both 2017-18 and 2018-19 as follows:
Delivery of an in-year 0.5% surplus in 2017/18 and in year breakeven in 2018/19;
Maintaining the 0.5% mandatory contingency reserve in both years; Maintaining the 1% non-recurrent reserve, with half remaining uncommitted; Meeting of the Mental Health Investment Standard requirement; Providing for the non-recurrent investment of £1.50/head for primary care in
both years; and QIPP savings required of £11.5m in 2017/18 and £8.7m in 2018/19.
Members of the Finance Committee expressed their thanks to the finance team for their hard work preparing the financial plan for 2017-19.
Version: Final O1 - 4 Date: 01 11 17
The Finance Committee APPROVED the 2017-19 Financial Plan. 17/154 QIPP
A copy of the 2017/18 QIPP dashboard for Month 3 had been circulated to members for information. The following ‘red’ rated QIPP areas were highlighted:
End of life care Medicines Management – new models of care and meds optimisation Neurology community shifts Ophthalmology increased community provision Planned care transformation Reduction in outpatient follow up rates Respiratory KPI
17/155 BUSINESS CASE Improving Access to Psychological Therapies (IAPT) Services in Kingston
A copy of an outline Business Case for the Kingston IAPT service requesting additional funding to meet the NHS England increased access performance targets was presented to members for approval. Members noted that the business case had been approved by the Delivery Group at its meeting on 20th June 2017 and they had requested a detailed implementation/action plan and data on the number of self-referrals both of which would be presented to the next Delivery Group meeting. Members discussed the issues with recruitment of staff for the service with the national drive that was underway and also requested that further work be done around interlinking long term conditions with the Expert Patient Programme. Members also raised the issue of needing a mechanism to ensure oversight of those patients that choose to self-refer into the service and this question would be raised at the next CQRG meeting.
The Finance Committee RATIFIED the business case and noted that the contract variation detail would be prepared separately for sign off by the Managing Director and Local Director of Finance.
17/156 CAPITAL PIDs
Members noted that as part of the financial planning process, the CCG submitted capital plans and bids to NHS England for approval by the London Capital Committee on 11th July 2017. Members received copies of the following 3 PIDS that had previously been reviewed and approved by the Delivery Group at their meeting on 20th June 2017:
Version: Final O1 - 5 Date: 01 11 17
Your Healthcare CIC IT rolling replacements
Members noted that as a CIC, Your Healthcare cannot bid for capital directly. Therefore the CCG would pass the capital grant to them on the understanding that there would be no financial consequences for commissioners resulting from the capital expenditure.
GP IT
Members noted that GP IT are assets held by NHS England. The CCG will procure the assets and recharge NHS England.
CCG IT rolling requirements Members noted that CCG IT rolling replacements are in line with the SWL IT strategic plans for integrated working. Depreciation costs are outlined in the PID. Support and maintenance costs would be covered under the current support contract until the end of the 3 year licensing agreement.
The Finance Committee APPROVED the planned capital expenditure as outlined in the above three PIDs. 17/157 TENDER WAIVER Kingston Care Record
Members received details of a tender waiver for retrospective approval by members and they were informed that due to capital approval received by the CCG late in December 2016 for the Kingston Care Record (KCR), and due to timescales quotes were not obtained even though the purchase was above £15k as per procurement and financial policies.
The value of the tender waiver was £215k. Members were not comfortable with a retrospective tender waiver. However, it was reported that the money spent with the software suppliers had enabled considerable progress with the programme over the last six months.
The Finance Committee APPROVED the Kingston Care Record Tender Waiver subject to a view from the Auditors that there could be no legal challenge.
17/158 ANY OTHER BUSINESS None. 17/159 DATE OF NEXT MEETING Tuesday, 26th September 2017 (1.30 – 3.00pm)
Future Meeting Dates: Tues 24th October 2017 (1.30-3.00pm) Tues 28th November 2017 (1.30-3.00pm) Tues 19th December 2017 (1.30-3.00pm)
Version: Final O2 - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Finance Committee Minutes
Agenda Item 15 Attachment
O2
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Presented by: (name & job title)
MINUTES OF THE FINANCE COMMITTEE HELD ON MONDAY 26th SEPTEMBER 2017 FRASER CHAPEL, THE KING’S CENTRE
CHESSINGTON PRESENT: David Knowles Lay Member & Vice Chair Jim Smyllie Lay Member Paul Gallagher Lay Member & Audit Chair Phil Moore Governing Body GP Annette Pautz Governing Body GP James Murray Chief Finance Officer, SWL Alliance Yarlini Roberts Local Director of Finance, K&R LDU Jenny Sinnott Head of Finance IN ATTENDANCE: Laura Winder NEL CSU Sue Lear Acting Deputy Director of
Commissioning Derek Hoddinott RBK Commissioning Consultant (items
10 and 11) Clare Woollett Governance & Business Support - Minutes APOLOGIES: Naz Jivani Governing Body Chair Tonia Michaelides Managing Director 17/160 WELCOME AND APOLOGIES: Those present were welcomed to the meeting. 17/161 DECLARATIONS OF INTEREST: There were no declarations.
Version: Final O2 - 2 Date: 01 11 17
17/162 MINUTES OF THE LAST FINANCE COMMITTEE MEETING The minutes of the last meeting held on Monday 24th July 2017 were agreed as an accurate record.
17/163 MATTERS ARISING
None.
17/164 TERMS OF REFERENCE The updated Terms of Reference were approved. 17/165 FINANCE REPORT – MONTH 5 A copy of the Month 5 Finance Report had been circulated.
Members noted that the Better Care Fund (BCF) plans were submitted to NHS England on the 11th September and that Kingston’s plan has been rated as strong.
Members were also presented with a summary of the Month 5 position as follows:
CCG is on target to achieve its business rules for 2017/18 CCG is forecast to meet its planned in year 0.5% surplus of £1,151k and
cumulative surplus of £4,713k Cash targets and Better Payment Practice Code statistics were met in Month
5 QIPP savings are forecast to under-achieve against plan due to delays in
implementation of some schemes Acute Commissioning Members were advised that both Kingston and St George’s Hospitals reported forecast positions had worsened since month 4 – Kingston by £2.4m and St George’s by £1.2m. With Kingston Hospital, large variances are reported in A&E, emergency and outpatients. The NEL CSU acute team are working with the hospital to resolve outstanding issues regarding arbitration, the Clinical Decision Unit (CDU), the impact of Identification Rules (IR) and Urgent Care Centre (UCC) charging. With St George’s Hospital, the worsening position is due to the impact of the Identification Rules being reported in month 5. There is an expectation that additional funding will be forthcoming from NHS England. Members noted the likely delay in the opening of the UCC at Kingston Hospital, which is due in October 2017 and acknowledged the risk that this may potentially increase activity and become an additional cost to the CCG. Currently, the CCG has had no sight of the service specification and pathways but NEL CSU is working on agreeing these with the hospital. Oversight of the project is being undertaken by the A&E Delivery Board. Members agreed that it was important that any new service provision took account of existing services in the system, both in the hospital and in primary care and the community.
Non Acute Commissioning Mental Health Members were informed that mental health placements are forecast to be underspent by £296k due to budgeting high cost placements not yet materialising. There remains a degree of uncertainty over joint funding RBK placements and a
Version: Final O2 - 3 Date: 01 11 17
number of NHS England specialised and TCP placements. These are subject to regular monitoring. Continuing Care Members were advised that the Continuing Healthcare (CHC) position has worsened since month 4 and is now reporting an overspend of £724k by year end. This is due to a continued increase in the average weekly fee and a significant increase in appeals. A working assumption has been made that circa 50% of these will be successful. There have been 6 new Children’s CHC cases in 2017/18 which has led to a forecast overspend of £367k. Primary Care Members noted that prescribing costs in Q1 of 2017/18 are £170k higher than in the same quarter of 2016/17 – this leads to a forecast overspend of £424k for the year. The increases are across a number of drug categories and analysis to investigate the causes is underway. It was also noted that CCGs have been notified that the reduction in category M prices (generic drugs) will not flow through to them but will be held over in an overall system reserve. Running costs Members noted that the running costs budgets currently reflect the new Local Delivery Unit (LDU) structure. Members requested that a report on the savings in running costs that were expected to result from the setting up of LDUs be provided by the Alliance. James Murray advised that work was in hand at an Alliance level to examine this among other issues and reports would be available in due course. Action: James Murray to provide report on cost savings that have resulted from the federation of CCGs into LDUs. QIPP Performance Members were informed that the overall QIPP position forecast shows an expected under achievement of £861k based on savings seen in year to date. It was noted that after the ‘Choosing Wisely’ engagement exercise, the CCG’s Governing Body had agreed to no longer support the routine prescribing of gluten free food, vitamin D maintenance and medicines which are available over the counter. Problematic QIPP schemes are community crisis and ICT/Rapid Response; paediatric same day access and primary care access and weekend services. All schemes are kept under review by the Delivery Group and consideration will be given to curtailing or stopping support for schemes that do not deliver the forecast quality improvements or savings. The Finance Committee NOTED the Month 5 Finance Report.
17/166 NEL CSU INTEGRATED REPORT Members received two Month 4 SWL CCG reports for information. These represent a reformatted approach which provides a comprehensive overview of contracting and finance activity and an additional report giving a STP and Trust wide view. Members were requested to provide any comments on the new format to [email protected] Initial feedback suggested that a key message summary would be a welcome addition.
Version: Final O2 - 4 Date: 01 11 17
17/167 UPDATE ON THE LOCAL TRANSFORMATION BOARD (LTB) Members were advised that the Local Director of Finance is now attending meetings of the LTB and that a finance sub-group has been established with representatives from the CCGs, Kingston Hospital, Your Healthcare and Hounslow and Richmond Community Healthcare. The sub-group’s remit also includes developing an estates strategy and looking at workforce transformation issues.
17/168 BUSINESS CASE
Respiratory KPI
A copy of the Business Case for the Kingston CCG and Kingston Hospital joint respiratory post was presented to members for approval. The objective of this joint funded post is to provide in-reach into the hospital to identify patients who could be referred to the CRIS team to be managed within the community – this will translate into supporting reductions in admissions and lengths of stay. Members noted that the business case had been approved in principle by the Delivery Group at its meeting on the 8th August 2017 subject to the necessary ratification by the Finance Committee. Members also noted that Kingston Hospital is looking at other Trusts which have introduced similar schemes to confirm the effectiveness of this approach. The Finance Committee RATIFIED the business case subject to the evidence of effectiveness being presented at the next meeting of the Delivery Group on the 17th October.
17/169 KCCG AND RBK JOINT FUNDING OF CARE PACKAGES
A copy of a proposal to regularise the arrangements for joint funding of care packages between the Royal Borough of Kingston (RBK) and KCCG was presented by Derek Hoddinott, RBK’s Commissioning Consultant. The proposal seeks to objectify the process of agreeing funding splits for placements to reduce delays and standardise and streamline the decision making process. It is based on a methodology already in use in other areas of the country and will be applied in circumstances where an individual has been deemed ineligible for continuing healthcare. The new arrangement would be run for 3 months and then be assessed and modified if required. Members sought clarity on (a) whether the proposal had received any clinical scrutiny through any of the CCG’s committees; and (b) whether there had been a material change in financial responsibility as a result of the arrangements where they have been operational for some time. It was agreed that the proposal would be discussed at Delivery Group on the 17th October and again at the next Finance Committee on the 24th October. In the meantime a request was made that some representative test cases be examined as per item (b) above. Action: Derek Hoddinott to attend October’s Delivery Group and provide examples of assessments under the new arrangements for scrutiny.
Version: Final O2 - 5 Date: 01 11 17
17/170 SECTION 75 AGREEMENT – KINGSTON CCG AND RBK
A copy of the summary cover sheet and Section 75 agreement for 2017/18 had previously been circulated to members. Queries were raised around the figures for Children’s Services and the figures for the accommodation charges for the Wellbeing Service, which have yet to be finalised. Members were assured that a strengthened Kingston Commissioning Board would provide oversight on the delivery of services.
Members agreed to delegate authority to the Chair to approve the Section 75 agreement subject to the satisfactory resolution of the outstanding financial issues. 17/171 ANY OTHER BUSINESS None. 17/172 DATE OF NEXT MEETING Tuesday, 24th October 2017 (1.30 – 3.00pm)
Future Meeting Dates: Tues 28th November 2017 (1.30-3.00pm) Tues 19th December 2017 (1.30-3.00pm)
Version: Final P - 1 Date: 01 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Integrated Governance Committee Minutes
Agenda Item 15 Attachment
P
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Presented by: (name & job title)
MINUTES OF THE INTEGRATED GOVERNANCE COMMITTEE HELD ON TUESDAY 19 SEPTEMBER 2017
IGC Members 25.4 16.5 13.6 11.7 8.8 19.9 17.10 14.11 12.12 2018 TBC TBC TBC
Phil Moore (chair) PM SA A A A
Fergus Keegan (deputy chair) FK A A A A
Sam Grant (minutes) SG A A A A
Nazim Jivani NJ SA A SA SA
Tonia Michaelides TM SA A SA SA
David Knowles DK SA DNA DNA SA
Naeem Iqbal NI A A A A
Pete Smith PS SA A A SA
Jim Smyllie JSm DNA DNA A SA
Paul Gallagher PG DNA DNA DNA DNA
Brian Roberts BR A A SA A
Vicki Harvey-Piper VHP A A SA DNA
Sue Lear SL SA
Laura Jackson LJ A A DNA SA
Kathryn Yates KY DNA SA A A
Version: Final P - 2 Date: 01 11 17
Sylvie Ford SF A DNA DNA DNA
Iona Lidington IL A A SA A
KEY: A = Attended, DNA = Did Not Attend, SA = Sent Apology, SD = Sent Deputy, NR = Not Required
Item Action
1. Welcome, apologies for absence and confirmation of quoracy The Chair welcomed the Integrated Governance Committee (IGC) members. Apologies were received from Nazim Jivani, Tonia Michaelides, David Knowles, Pete Smith, Jim Smyllie, Sue Lear and Laura Jackson. Peter Warburton (PW) attended the meeting to present item six and Lara Belling (LB) to present item eight.
2. Minutes of IGC held on 13 June 2017 and matters arising The minutes for the Integrated Governance Committee on 11 July 2017 were confirmed as a fair representation of the meeting. Action Log Please refer to the action log for all changes. Matters Arising No other matters noted.
3. Integrated Governance Exception Report BR gave on overview of the CCG performance for M4 2017/18, key points discussed are as follows
- Month on month dementia diagnosis rates have been increasing since March 2017. A clinical nurse specialist has been working with local care homes, evidence of this work will be seen in October 2017 performance data.
- Cancer targets: four complex breaches due to patient choice. - IAPT: access and recovery trajectory is currently not achieving target, funding
has been invested to increase access standards for 2017/18 to 2018/19. Patients that may relapse or experiencing delays with referrals are addressed at the Clinical Quality Review Group.
- There have been three MRSA healthcare associated infections between April and July 2017 which are currently being investigated, although early indications are that they have been acquired in the community. There have been two C-Difficile infections for the same period, which is under the YTD trajectory of 10 cases.
- In 2017-18, Kingston Hospital have not met the standard of 95% on a monthly basis of patients spending less than four hours between arrival in the A&E department and admission, transfer or discharge.
- The variation YTD in July 2017 has increased to 10.9% from 10.3% in June 2017: 2. There has been an increased level of admissions as a result of the newly opened Clinical Decisions Unit (CDU) at Kingston Hospital, which was planned on the basis that activity levels would not increase.
- The Kingston Cancer Strategy 2017 – 2022 has a range of actions in place related to increasing the uptake of screening which should impact the CCG meeting target of 58.8% for cancer diagnosed at early stages.
- The July 17 GP Patient Survey 69% stated good experience of making an appointment, although 83% of people were able to get an appointment, and 90% stated that the time of the appointment was convenient.
- The lead for Continuing Healthcare has developed the improvement action plan requested by NHSE and the SWL Alliance for Kingston and Richmond, and had identified a range of actions which will be implemented over the next quarter to achieve the required trajectory. This will remain an area of challenging performance give the scale of improvement required across the winter period. Equity of Access and outcomes in to IAPT services continues to be at monthly contract meetings with the provider.
Version: Final P - 3 Date: 01 11 17
Item Action 4. Q1 2017/18 Safeguarding Adults Report
PW gave an overview of safeguarding adult’s activity for Q1 2017/18, key points discussed noted below;
- Safeguarding Adults Board: PW Chairs the Kingston Safeguarding Adults Board Communication Sub-Group. They are leading on the redesign and update of the SAB web site to make this more accessible to the general public and user friendly. The group have developed a standard script for all partners to use when giving presentations and talks to voluntary and community groups. The local police have also requested training on MCA and DoLS and the training sub group partners will be providing this training.
- Safeguarding Adult Reviews (SARs): PW reported that a SAR has been called by the SAB board chair and SAR sub-group to investigate the death of a service user with care and support needs who died after being discharged to home from hospital. Issues have been identified in regards to the care pathway, missed information on medication administration and communication problems. An independent chair for the review is currently being sourced.
- Learning Disability Mortality Review (LeDeR): The CCG leads attended the London wide LeDeR steering group in August. Issues were raised and highlighted around the capacity of trained reviewers to complete allocated reviews. Across London since March 2017 there have been 83 notifications of deaths and so far only four reviews have been completed (one of which was from Richmond). Kingston currently has two reviews in progress and Richmond has had one notification in August, which is due to be allocated. A timescale for completion of reviews within four months from allocation date for completion for reviews has now been put in place. Now that a new Safeguarding Adults Lead has been appointed in Richmond CCG the safeguarding team can work together to share the work and complete current reviews.
- GP and Primary Care Training: A new revised bid has gone into NHSE Safeguarding Team for monies to support a training programme on MCA and DoLS for GPs and primary care staff across Kingston and Richmond.
5. Q1 2017/18 Safeguarding Children Report FK provided an overview of the safeguarding children’s activity for Richmond in Q1 2017/18. Central London Community Healthcare (CLCH) have been awarded the Richmond and Wandsworth Health Visiting Contract. The frontline staff from HRCH (previous provider of service) have been TUPE’d over to CLCH. Sexual health services are also now with CLCH. GP compliance with Case Conference report requests remains low at a 10% achievement this has been added to the organisations risk register for monitoring. PM questioned the process currently being used by social services, adding that this is an unreasonable expectation for GPs and highlighting it as a performance issue with GPs should be revised. Commentary on local providers:
Kingston Hospital are currently not recording their level one and two training figures.
CLCH recently reported 100% compliance with all levels of safeguarding training.
East London Foundation Trust (ELFT) IAPT services reported 49% achievement with safeguarding level three training – an action plan will be submitted to Sian Thomas, Designated Nurse Safeguard Children, Richmond CCG, and feedback will be included in the next quarterly report.
6. Integrated Performance Reporting Q1 2017/18 Medicines Optimisation
Version: Final P - 4 Date: 01 11 17
Item Action LB provided an outline of the performance and quality for Q1 2017/18, key points noted below:
- Unlike previous years, eligibility to receive MOIS funding is no longer dependent on the prescribing expenditure entry criteria. For 2017/18 the maximum entitlement payment scheme features three aspects; Achievement of Prescribing Budget Target, seven Medicines Optimisation Indicators and Polypharmacy Project.
- Quality Premium 2017/18: Reduction of inappropriate antibiotic prescribing for urinary tract infections (UTI) in primary care and sustained reduction of inappropriate antibiotic prescribing in primary care.
- LB reported that the SWL medicines optimisation work stream aims to save £10m across all six CCGs over 2016 – 2021. There have been delays in key components of the work streams will result in reduced savings.
- A number of components of the de-prescribing areas were considered to be ‘business as usual’ for standard Medicines Optimisation and were approved for implementation by the Kingston and Richmond Joint Governing Body Seminar held on 13 June 2017. However, a national consultation on the whole de-prescribing work stream may cause delays as the LMC has advised GP practices to wait until this has finished before implementing the recommendations of CCGs.
- There is currently reduced capacity within the Medicines Optimisation Team which is a risk to the delivery of the above work streams.
7. NICE Guidance Deep Dive Presentation
SG presented the Kingston and Richmond CCG Deep Dive into guidance from the National Institute for Health and Care Excellence. NICE’s role is to improve outcomes for people using the NHS and other public health and social care services by producing evidence based guidance and advice, development of quality standards and performance metrics as well as providing a range of information services. There are a number of classifications of guidance NICE publishes such as; guidelines which make evidence based recommendations on a range of areas, procedure guidelines recommending whether interventional procedures are effective and safe and standards which drive and measure quality improvements within a particular area of care. NICE have targeted updates and information pages online for general practice/primary care services. Clinical knowledge summaries provide practical recommendations to help general practice, NICE pathways can be utilised as quick reference for a particular topic and a tool to easily view all of NICE’s recommendations in one place. The NICE evidence series is an easy-to-use library of credible sources of health information and the monthly newsletter is a one-stop resource for the latest primary care news and guidance from NICE. The CCGs would recommend that individual practices sign up to the newsletter ensuring that the monthly updates can be disseminated throughout the practice. Action: SG and FK to discuss NICE Guidance monitoring to form part of the Primary Care Commissioning Committees. HRCH report their compliance with NICE guidance on a quarterly basis to the CCG. There have been no concerns or issues reported through the CQRG relating to compliance with NICE guidance. It is expected that Q2 Quality Report will evidence assessment of relevant NICE guidance from June 2017 to September 2017. Kingston Hospital also reports their compliance with NICE guidance on a quarterly basis to the CCGs. Again there have been no concerns or issues reported through the CQRG relating to compliance with NICE guidance. It is evident in reporting that the Trust continues to have difficulties working on the outstanding actions for partially compliant guidelines due to pressures on the team. SWLStG report their compliance with NICE Guidance through the annual Quality Account. Two particular audits noted is the implementation of NICE public health
SG/FK
Version: Final P - 5 Date: 01 11 17
Item Action guidance for the workplace and cardio metabolic assessment and treatment for people with psychosis. At this time it has not been possible to evidence reporting from Your Healthcare, Chelsea and Westminster Trust or St George’s Hospital on compliance with NICE Guidance. Kingston and Richmond CCGs will continue to work closely with the lead commissioners for our local acute, community and mental health providers to ensure that the services our patients access adhere to the quality standards and clinical guidance published by NICE. There may also be consideration of utilising existing methods of quality monitoring with providers to look at a requirement for formal reporting processes of compliance with NICE Guidance. A six monthly assurance report will be brought to the Quality, Safety & Performance Committee and Integrated Governance Committee including narrative on provider’s compliance with National Clinical Audits.
8. Kingston, Richmond and Surrey Downs Local A&E Delivery Board Winter Plan 2017/18 This paper was submitted for information purposes only.
9. Effective Commissioning Initiative Policy Development Version 2.0 progress update This paper was submitted for information purposes only.
10. Any other business No other business noted.
11. Date of Next Meeting Tuesday 17 October, Guildhall 1, Kingston.
Version: Final Q - 1 Date: 02 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Health & Well Being Board Minutes 14th September 2017
Agenda Item 15 Attachment
Q
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Presented by: (name & job title)
HEALTH AND WELLBEING BOARD
14 SEPTEMBER 2017 6:30 pm – 8:17 pm
Members of the Board Councillors: Councillors Kevin Davis (Co-Chair), Linsey Cottington, Tom Davies, Chris Hayes, Cathy Roberts, Hugh Scantlebury and Margaret Thompson* Representatives from Kingston CCG, Healthwatch and the Voluntary Sector: Dr Naz Jivani (Co- Chair), Dr Phil Moore, Dr Peter Smith*, Grahame Snelling* and Patricia Turner Council Officers (non voting): Rob Henderson*, Iona Lidington and Stephen Taylor* Advisory Members (non voting): Siobhan Clarke – Your Healthcare, Tonia Michaelides – Kingston CCG, Dr Mark Potter* – South West London and St George’s Mental Health Trust, Jane Wilson* – Kingston Hospital NHS Trust, Gwen Kennedy* – NHS England and Dr Anthony Hughes – Kingston GP Chambers
* Absent
12. QUESTIONS AND PUBLIC PARTICPATION
There were no questions from the public. 13. DECLARATIONS OF INTEREST
There were no declarations of interest.
Version: Final Q - 2 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES 14 SEPTEMBER 2017 14. APOLOGIES FOR ABSENCE AND ATTENDANCE OF SUBSTITUTE MEMBERS
Apologies were received from Councillor Margaret Thompson, Dr Pete Smith, Dr Mark Potter, Rob Henderson, Stephen Taylor and Jane Wilson. Stephen Bitti attended the meeting in an informal capacity on behalf of Grahame Snelling of Healthwatch.
15. MINUTES
The minutes of the meeting of the Board held on 15th June 2017 were approved and signed as a correct record.
16. DIRECTORS UPDATE Appendix A
The Board received updates from the Directors of Adult Social Care and Children’s Services, the Interim Director of Public Health and the Chief Officer of Kingston Clinical Commissioning Group, on a variety of issues. These included;
The successful launch of the Thrive Kingston Mental Health Strategy The commencement of work to update the Pharmaceutical Needs Assessment Discussions with the Joint Strategic Needs Assessment Working Group’s
members on a review of the processes and content of the Assessment The latest position in respect of the Kingston Coordinated Care programme
including Home Care Transformation, the New Model of Care, the Council and CCG’s joint commissioning arrangements, the Active and Supportive Communities project and the Kingston Care Record
The Community Sponsorship event hosted by the Council in July for people who may be interested in sponsoring refugees relocated to the Borough
A forthcoming table top exercise to test responses to a flu pandemic A two year pilot to improve cancer screening uptake in marginalised groups The roll out of Mental Health first aid train the trainer courses for staff working
with both adults and young people The progression of the new Self Care Kingston programme designed to
reduce pressure on services, including proposals for an event during national Self Care Week in November at which the Cancer Strategy for Kingston would be launched. Members endorsed details of the emerging Connect Well Kingston proposal, which
formed part of the Self Care programme. The intention was to co-design and implement new ways of working for frontline workers across the borough in order to provide a consistent training offer, improved community networks and champions providing early support and signposting. Service providers on the Board were asked to engage in the co-production of the model and nominate a lead for their respective organisations.
The Board also noted guidance from the Department for Education (DfE) which recommended that schools should consider the installation of automated external defibrillators (AEDs) on their premises. These were already widely available in Kingston in areas where a high footfall was expected and where higher risk physical activities were undertaken. It was emphasised, however, that the risk of out of hospital cardiac arrests in children and adolescents was very low and only a small proportion of these would take place on school grounds. AEDs could not be
Version: Final Q - 3 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES 14 SEPTEMBER 2017
considered a Public Access Defibrilator (PAD) because they would be unlikely to be available for use outside school hours and off the premises. Training for PAD use and CPR was of value both in the secondary school setting and the wider context and schools would be encouraged to take part in the British Heart Foundation’s ‘Restart a Heart’ campaign.
RESOLVED that –
1) The collective working approach in respect of the Connect Well Kingston proposals set out in paragraphs 32-36 of the agenda report be endorsed and service providers on the Board be asked to engage in the co-production of the model for Kingston and nominate a lead for their organisation; and 2) Schools be encouraged to participate in the British Heart Foundation’s ‘Restart a Heart’ campaign.
Voting – Unanimous 17. VERBAL UPDATES FROM KINGSTON VOLUNTARY ACTION AND HEALTHWATCH
KINGSTON
The Board received updates on the latest activity of Kingston Voluntary Action (KVA) and Healthwatch Kingston.
Patricia Turner reported that KVA was participating in the Macmillan social prescribing project steering group and had welcomed the new Social Prescribing worker as part of her induction. A new Active and Supportive Communities network had been established for voluntary organisations commissioned to deliver the outcomes of the Strategy as part of the Kingston Coordinated Care programme. The network, which had met for the first time in June, had developed a tool to assist pharmacists refer people directly to voluntary groups in order to reduce pressure on GPs and A&E. A number of voluntary organisations had attended the initial multidisciplinary team meetings in New Malden and Patricia Turner was herself now attending the Kingston and Richmond Local Transformation Board. The Health and Wellbeing network meeting the following week was due to look at means of supporting the CCG’s work on primary care. Stephen Bitti, the new manager of Healthwatch attending on behalf of Grahame Snelling, advised that the full complement of three members of staff were now in place and dealing with the logistics of establishing a new office. He was presently also engaged in meeting key stakeholders. In addition four new Trustees had been recruited.
18. SOUTH WEST LONDON SUSTAINABILITY AND Appendix B TRANSFORMATION PARTNERSHIP UPDATE
Tonia Michaelides, Managing Director of Kingston and Richmond Clinical Commissioning Groups, provided the Board with an update on the major work programmes of the South West London Sustainability and Transformation Partnership (previously the Sustainability and Transformation Plan). Members noted that a refresh of the STP strategy was being undertaken in order to move towards local planning and delivery to keep people healthy and out of hospital. Local Transformation Boards (LTBs) had been established for each Local Delivery Unit, the new structures continued to be embedded to lead the development and delivery of the new local health and care models and new leadership appointments and structures had been approved.
Version: Final Q - 4 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES 14 SEPTEMBER 2017
The Kingston and Richmond LTB, which brought together senior leaders from across the health and care system in both boroughs, had been meeting since January 2017 and its focus to date had been on reviewing progress of the development of the health and care model, its own workplan and initiation of work on how to develop an accountable care system. The Board was also informed that detailed implementation planning was underway in respect of 5 year Forward View programmes across South West London in urgent and emergency care, cancer, primary care and mental health. Further work continued in delivering common approaches to musculo-skeletal services and effective commissioning as well as agreement of a delivery plan for maternity services to meet the Better Births recommendations. Enabling digital, workforce and estates programmes were in place to support the transformation and the focus of communications and engagement was to be shifted into the individual LTB areas. It was anticipated that by the end of November 2017, when a refreshed strategy document was due to be published, local health and care systems would have reviewed feedback from engagement with residents, analysed local data and identified their main challenges. They would then be in a position to set out how they planned to work together to improve services and be clinically and financially sustainable going forward. Existing engagement activity would be further developed to ensure that local people were involved in the planning of services and there would be consultation on proposals for significant change. It was agreed that future updates to the Board would contain more information on Kingston specific activities and the implications for the local population.
19. CHILD DEATH OVERVIEW PANEL ANNUAL REPORT 2016-17 Appendix C Amanda Boodhoo and Sarah Bennet of the Local Safeguarding Childrens Board presented the 2016/17 annual report of the Child Death Overview Panel, a sub group of the Board which examined deaths in Kingston and Richmond with a view to understanding how and why children died and to develop interventions to prevent future deaths. Members noted that there had been a total of 16 child deaths in Kingston and 12 in Richmond during the course of the year. Some 62% of the Kingston children were from a White British ethnic background against a borough demographic of 67%. Eight of the deaths investigated were thought to have had modifiable factors. The main causes or categories of death overall were perinatal/neonatal events (11) and chromosomal, genetic and congenital anomalies (5). Most of the deaths had occurred in infants under 12 months of age. The Panel’s promotion of the availability of Government funding for defibrillators in schools was noted but it was recognised that the primary need was to reinforce messages of basic life support. Public access to defibrillators was now reasonably good but the training of young people in CPR techniques was likely to be of greater benefit. To this end the Council was promoting the British Heart Foundation’s ‘Restart a Heart’ campaign. Members of the Board requested that the Child Death Overview Panel’s updates be circulated directly to individual GPs rather than via Practices and also provided to Councillors.
Version: Final Q - 5 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES
14 SEPTEMBER 2017
20. LONDON MAYOR’S HEALTH INEQUALITIES STRATEGY - Appendix D CONSULTATION
The Board received a presentation on the Mayor of London’s proposed new London Health Inequalities Strategy and gave consideration to its implications for Kingston. Members noted that the Mayor was seeking to develop and implement a new strategy to reduce health inequalities in London between 2017 and 2027 in partnership with local authorities and the NHS. The draft document currently out for consultation contained five strategic priorities, namely; healthy children, healthy minds, healthy places, healthy communities and healthy habits. This aligned well with the actions contained in Kingston’s existing Joint Health and Wellbeing Strategy. Both the London wide and the local documents shared aims to support children and improve mental health and emphasised the importance of ill-health, community empowerment and reducing disadvantage. It was acknowledged that although Kingston was one of the least deprived unitary authorities in England with higher life expectancies for both men and women than the national and London norms, there remained substantial inequalities within the borough. Women living in the most deprived area of the borough were expected to live for 4.8 years less than those in the least deprived while for men the gap was 5.1 years. The significant cost of health inequalities to public services and the wider economy was also recognised. Members therefore gave consideration in brief break-out discussion sessions to the respective roles of individual members of the Board in reducing local health inequalities, how to align existing joint strategic plans in Kingston with the London wide priorities contained in the draft strategy and what needed to be in place across London to better enable local action in Kingston. Issues raised in the discussions included the opportunities for mental health created by the Prevention Concordat, the need for a national framework to reduce inequalities and for national, pan-London and local programmes to align and create synergy. It was recognised that the Mayor could only deliver through London boroughs – local was better in many respects – though his influence through the exercise of other functions was considerable. To this end the principles of the Strategy would need to be embedded in The London Plan, the spatial planning document due to be published in draft later in the year. Members also commented that it was important to focus on the wider determinants of health, which was where the most difference could be made. The detailed feedback from the break-out sessions would help shape both the response to the consultation and the development of local implementation plans. It was noted that partners would be able to draw on the Council’s consultation response in preparing their own submissions. RESOLVED that –
1) the five aims of the draft strategy, as described below and in paragraph 6 of the agenda report be endorsed; 2) the Director of Public Health be authorised to prepare a detailed consultation response in consultation with the Co-Chairs of the Board; and 3) local implementation plans be developed and submitted to the Board as appropriate after publication of the final London strategy. Voting – Unanimous
Version: Final Q - 6 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES 14 SEPTEMBER 2017
21. LONDON CRISIS PROGRAMME UPDATE - HEALTH BASED Appendix E PLACE OF SAFETY
The Board received details of pan London proposals to improve access to services for patients detained under Section 136 of the Mental Health Act. Members noted that there continued to be a disparity between care provision for people with mental health issues and those with physical problems. Service users were often denied access to Health based Places of Safety (for example hospitals), left in the back of Police cars and ambulances or transferred unnecessarily between A&E Departments and Mental Health Trusts due to a lack of integrated, holistic, care. Existing difficulties were likely to be compounded by forthcoming legislative changes which would reduce detention time from 72 to 24 hours and increase the scope of S136 which was likely to mean an increase in the number of people being detained. In order to mitigate these problems, and help ensure the crisis care system had sufficient capacity and processes in place to respond to the changes, the Healthy London Partnership had developed a new model of care which included:
a pan-London approach to care with individuals taken to the nearest place of safety and, if necessary following assessment, being transferred to their local mental health trust; transparency around capacity at Place of Safety sites and robust escalation processes when capacity was full; a dedicated 24/7 staffed service at Place of Safety sites; increased physical health competencies at Place of Safety sites to ensure unnecessary referrals to A&E departments and more timely, integrated care; and streamlined pathways between A&E Departments and Place of Safety sites for when individuals required more intensive physical health treatment
The existing local Health Based Place of Safety, at South West London and St George’s Hospital Mental Health Trust’s Springfield site was to be retained, thereby ensuring that the key components of the new arrangements would be met. Potential issues with travel times to the site from outer reaches of its catchment areas were acknowledged but it was emphasised that the site would not necessarily need to cater for all of South West London. Much of the population in Croydon, for example, tended to look to South East London provision. Mental Health STP programmes would lead on further engagement in their respective areas over the next six months to definitively establish the preferred options. The outcome of this consultation would be reported to the Board.
22. BETTER CARE FUND PLAN 2017-18 Appendix F
The Board retrospectively endorsed the Better Care Fund Plan for 2017/18 which had been submitted to NHS England just prior to the meeting. Members noted that the local vision for health and social care integration, which strongly aligned with the STP and sought to embed the principles of the Kingston Coordinated Care programme, was unchanged. There remained a commitment to the aims set out in the 2016/17 Plan, namely;
to support the development of active and supportive communities in which people were enabled to live healthy and well, independently within a thriving and resilient community, and
Version: Final Q - 7 Date: 02 11 17
ROYAL BOROUGH OF KINGSTON UPON THAMES
14 SEPTEMBER 2017
to develop customer centred care that supported people with complex needs to achieve the best possible quality of life and the goals that mattered to them with an increased focus on prevention, proactive care and self-reliance
Once again it was intended that these aims would be achieved by putting in place a customer centred approach, building resilience within communities with access to a variety of community support options and the design and implementation of a new model of simpler, streamlined, cost effective and integrated services. It was agreed that although the Plan was intended as a commissioning document there would be value in sharing its contents with providers, including Kingston hospital.
RESOLVED that –
the Better Care Fund Plan for 2017/18 attached at Annex 1 to the agenda be endorsed.
Voting – Unanimous
23. HEALTH OVERVIEW PANEL - MINUTES Appendix G
The minutes of the meeting of the Health Overview Panel held on 13th July 2017
were noted.
24. URGENT ITEMS AUTHORISED BY THE CHAIR There were no urgent items.
Signed…………………………………………………….Date………………… Co- Chair
Version: Final R - 1 Date: 02 11 17
Kingston Clinical Commissioning Group Report Summary
Meeting Title Governing Body in public Date 7th November 2017 Report Title Primary Care Commissioning Committee Minutes - 4th July 2017
Agenda Item 15 Attachment
R
Purpose (please indicate with X)
Approval/ Ratification
Discussion / Comment
Information x
Report Author: (name & job title)
Jo Dandridge, Governance & Business Lead
Presented by: (name & job title)
Jim Smyllie, Lay Member & PCCC Chair
Primary Care Commissioning Committee Meeting In Public
Date: 4th July 2017 Time: 1pm to 3pm Location: Fraser Chapel, The Kings Centre, Chessington Members: Name Role Jim Smyllie Lay Member, PPE and Chair David Knowles Lay Member & Vice Chair Dr Graham Lewis Independent GP Advisor, Richmond CCG Tonia Michaelides Managing Director, Kingston & Richmond CCGs Yarlini Roberts Local Director of Finance, Kingston & Richmond CCGs Nadeem Nayeem Secondary Care Specialist Kathryn Yates Governing Body Nurse Member In Attendance Kathryn MacDermott Local Director of Primary Care & Planning Dr James Benton GMS Practicing Clinician Dr Naz Jivani Governing Body Chair & GP Dr Phil Moore Governing Body Deputy Chair, Clinical Dr Gareth Hull Governing Body GP Dr Naeem Iqbal Governing Body GP Dr Pete Smith Governing Body GP Dr Annette Pautz Chair of Council of Members Dr Julius Parker Surrey & Sussex LMC David Mphanza Primary Care Development Manager Jo Dandridge Business Manager (minute-taker)
Version: Final R - 2 Date: 02 11 17
Item No
Agenda Item Action
1 Chair’s Welcome The Chair welcomed members to the seventh meeting of the Kingston CCG Primary Care Commissioning Committee.
A note of thanks was recorded to Julie Pickering for her involvement as Health & Well Being Board representative on the committee, and wishing her well in her new role as Mayor of Kingston
A note of thanks was also recorded to Grahame Snelling for his commitment to the committee as Kingston Healthwatch representative.
2 Apologies for Absence Paul Gallagher, Lay Member and Audit Chair William Cunningham-Davis, NHS England Iona Liddington, RBK Public Health
3 Declarations of Interest The chair reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of Kingston CCG. Interests declared by members of the Primary Care Commissioning Committee are listed in the CCG’s Register of Interests. The Register is available either via the Business Manager or the CCG website at the following link: http://www.kingstonccg.nhs.uk/about-us/primary-care-commissioning-committee.htm Declarations of interest from Sub-Committees None declared Declaration of interest from today’s meeting Dr Phil Moore declared his interest as a Partner at Central Surgery who were taking on responsibility for Kingsdowne Surgery.
The Chair declared that the meeting was quorate.
Minutes & Reports 4 Minutes of the Last Meeting
The minutes of the last meeting held on 2nd May 2017 were agreed as an accurate record.
Version: Final R - 3 Date: 02 11 17
5 Primary Care Quality and Development Group (PCQDG) meeting
The committee received a report from the most recent meeting of the Primary Care Quality and Development Group held in June 2017 for information. It was agreed to include on the agenda for the next meeting a summary of the utilisation of all three Kingston’s extended primary care services for consideration. The committee approved the recommendation made by the Primary Care Quality and Development Group to close the Red Lion Road Alexandra Drive surgery.
Kathryn MacDermott
6 Report of the Locally Commissioned Services (LCS) Steering Group meeting The committee received a report from the most recent meeting of the LCS Steering Group held in May 2017 for information. Members noted that the commissioning of patient transport is still under review and work was being undertaken with Richmond CCG to explore what service could be commissioned once across Kingston and Richmond. The Chair of the LCS Steering Group had formally raised her concerns about the increased workload that arises from the number of shared care drugs for which GPs are now responsible and it was agreed this matter would be discussed at the August PCCC Seminar with a view to exploring options to address this matter.
Quality and Governance 7. Primary Care Delegated Commissioning Risk Log
The Risk Log had been circulated for information prior to the meeting. Members agreed to close the following risks:
Financial gap between primary care allocation and budget
£400K cost pressure in primary care budget CCG reputation with member practices, NHS England
and population as a result of additional responsibilities involved with delegated commissioning of primary care
Members noted the following new risk:
Practice changes – unplanned / poorly managed practice changes risk providing lower standard of
Version: Final R - 4 Date: 02 11 17
patient care. Members discussed the issues with the transfer of services from PCSS to Capita and concerns over the long term sustainability of a loss making service was questioned. William Cunningham-Davis agreed to take up this matter with NHS England and to find out what risk rating they had assigned to this issue. Members noted an improvement in the transfer of patient records to practices.
William Cunningham-Davis
8 CQC Updates The committee received an update on the CQC inspections and noted that all 27 practices including branch practices had now been inspected and had their reports published. The Primary Care Quality & Development Group works on behalf of the PCCC and monitors the reports in detail and supports practices to achieve the required compliance. Members noted that Kingsdowne Surgery had done a lot of work to address the issues raised by their CQC inspection and also that the patients of that surgery were transferring to Central Surgery which had received an overall ‘good’ rating by the CQC.
Strategy and Commissioning 9. Extended Primary Care Services
Extended primary care access highlight report The committee received a copy of the NHS England highlight report for May 2017 for information. Members noted that the extended primary care service was mostly used on weekday evenings. Concern was raised on the number of DNA’s that seemed to be increasing month on month. It was agreed to look into this and bring back further data broken down by date, site, clinician and health issue to the next meeting. Members were reminded that the main purpose for providing extended primary care access within Kingston was to take the pressure away from A&E and therefore it was questioned if there had been any improvements seen within the hospital. In response, initial data showed a reduction in A&E attendance of minors Communications Campaign Members stressed the importance of allowing the extended services the time to be fully embedded particularly with the unavoidable delay to the start of the publicity campaign due to purdah.
Kathryn MacDermott
Version: Final R - 5 Date: 02 11 17
It was noted that the addresses of the sites providing extended primary care access had not been included in the patient leaflet and therefore the receptionists making the appointments needed to inform the patients of the location. Following lengthy discussion on further additions and changes needed to the patient leaflet it was agreed to produce a revised version and an offer from the Chessington Residents Association to proof read the draft version was offered.
Kathryn MacDermott
9 GP Contract Updates Members noted that Kingsdowne Surgery had merged with the nearby Central Surgery based within Surbiton Health Centre on 1st July 2017 following the retirement of Dr Syed. Patients will be able to access GP services from both the Kingsdowne Surgery and Central Surgery sites up to the 30th September 2017 after which date, Kingsdowne Surgery would close permanently. Patients have been assured that their medical records will be securely shared with Central Surgery and there is no need for them to re-register.
Finance and Performance 10 Primary Care Budget Report – M2
Members received the Primary Care Budget Report for Month 2 and noted that due to limited data available at Month 2, primary care expenditure had been forecast at budget. Members were advised that provision of NHS Wi-Fi services is, from 1st April 2017, a mandatory requirement in the GPIT Operating Model. Members noted that the NHS Wi-Fi programme would cover implementation costs, running costs for 24 months from launch and an allocation to cover temporary local project management costs. Responsibility for funding Wi-Fi services after the first two years would be clarified. Members were advised that work is ongoing to identify further sources of funds to increase the Kingston Medical Services budget for 2017-18. It was agreed that further discussion would be held in the form of a PCCC Seminar in August to ensure appropriate governance was adhered to.
Dr Julius Parker Kathryn MacDermott
Questions from members of the public 11 None.
Any Other Business 12 None Date of Next Meeting 13 Tuesday, 3rd October 2017
3pm to 5pm Queen Anne Suite, Guildhall
Page 1 of 8
ATT. S
BUSINESS TRAVEL AND EXPENSES POLICY AND
PROCEDURES FOR KINGSTON & RICHMOND CCGs
Document Version: 1.0 Review: Matt Taylor-Lund Date Approved by Joint CCG EMT: Next Review: November 2018
Page 2 of 8
CCG Policy Reference: BTE/11/17
This policy has been approved by the joint Kingston & Richmond CCG executive management team and will have effect as of November 2017 Target audience Governing body members, committee members and all staff
working for both Kingston & Richmond CCGs Brief description
The purpose of this policy is to set NHS Kingston and Richmond Clinical Commissioning Groups’ (CCGs) position and procedures on business travel and associated expenses and to ensure that these expenses are claimed, in a consistent and reasonable manner. This policy applies to all members of staff, permanently or temporarily appointed to work for either CCG. Governing body members as office holders have separate terms and conditions.
Action Required
Following approval at the joint executive management team (on behalf of both CCGs’ governing bodies), the director of corporate affairs and governance will ensure that the requirements of this policy are raised at team meetings, and that the policy is made available to all staff on GPTeamNet and the intranet All managers will be required to read and acknowledge the policy.
Document Control
Policy Title: Business travel & expenses policy
Original Policy Author(s): Matt Taylor-Lund, Comms & OD Manager
Policy Owner: Vicki Harvey-Piper, Director of Corporate Affairs and Governance
Reviewed by: Sarah Patmore, HR business advisor
Consultation This policy was distributed to members of the ways of working group
File Location: GPTeamNet & intranet
Approval Body: Executive Management Team
Approval Date: 14/09/17
Document Review Control Information Version Date Reviewer Name(s) Comments
Page 3 of 8
1 Contents
1 Contents ............................................................................................................... 2
2 Introduction .......................................................................................................... 3
3 Qualifying conditions and procedure .................................................................... 3
4 Work base ............................................................................................................ 4
5 Work time ............................................................................................................. 4
6 Travel expenses ................................................................................................... 4
7 Subsistence expenses ......................................................................................... 6
8 Other relevant documents .................................................................................... 7
9 Equality and diversity statement ........................................................................... 7
10 Monitoring of policy .............................................................................................. 7
Page 4 of 8
2 INTRODUCTION
2.1 The purpose of this policy is to set NHS Kingston and Richmond Clinical Commissioning Groups (CCGs) position and procedures on business travel and associated expenses and to ensure that these expenses are claimed, in a consistent and reasonable manner. This policy applies to all members of staff, permanently or temporarily appointed to work for either CCG. Governing body members as office holders have separate terms and conditions.
2.3 This policy supersedes all other relevant policies under previous terms and conditions of employment held by individuals who have transferred into the CCG from other NHS organisations.
2.4 Funding used for expense claims, comes from the public purse and consideration should be given to the suitability and reasonableness of claims. All claims are subject to the Public Sector Expenses Review Act, 2009, which means claims may be subject to public scrutiny.
2.5 Where NHS Kingston CCG or NHS Richmond CCGs’ position is not addressed in this policy with regards to reimbursement of any business related travel or expenses reimbursement the terms and conditions set out in the NHS Terms and Conditions of Service Handbook will apply.
3 QUALIFYING CONDITIONS AND PROCEDURE
3.1 A general principle of reasonableness underlies the claiming and payment of all expenses. All members of staff have a responsibility to ensure that the costs to either CCG are kept to a minimum without unduly reducing the efficiency with which they carry out their duties. Staff are expected, wherever possible, to organise their working week to minimise travel time, costs and expenses.
3.2 Both CCGs recognise the impact travel can have on the environment and therefore acknowledges its role in maximising transport opportunities which both minimise carbon emissions and promote the most cost effective methods of transport to employees undertaking official CCG business. 3.3 All those responsible for making decisions regarding business trips, should take account of the following principles:
consideration should be given to the need for travel, versus other options such as telephone/conference calls or video-conferencing, whilst ensuring the delivery of both CCGs business aims
every attempt should be made to find central locations travel outside peak times is encouraged to reduce costs where meetings are held on Mondays, the start time should be such that
overnight stays are not necessary it is expected that travel and expense policy decisions will be based on cost
efficiency and value for money, therefore advance tickets should be purchased where possible and should include the use of pre purchased Oyster Cards
when travelling by public transport the most economical means of transport must be used, which in all but exceptional cases will not exceed the cost of
Page 5 of 8
standard class rail travel, bus travel or low cost airlines when travelling by air, economy class air travel should be booked, air travel
would not normally be appropriate for domestic trips, unless it is cheaper than a standard open rail ticket
3.4 Allowable travel expenses will only be reimbursed when supported by relevant documented evidence, including official receipts and entered on the Workforce system, which must be authorised by the line manager. 3.5 Interim contractors not set up on payroll should claim for allowable travel expenses in line with this policy via the agency they are employed with or alternatively via invoice if they are invoicing via their own registered company.
3.6 Claims should be submitted in a timely manner, within one calendar month of the expenditure being incurred. Staff must claim for reimbursement within three months of the expense/mileage incurring.
3.7 Claims should be approved in a timely manner by line managers, within one month of the claim being submitted.
3.8 Payments will only be made via payroll and will be paid each month after the expense has been incurred, subject to the claim being suitably authorised and received by the payroll provider prior to the cut-off date.
4 WORK BASE
4.1 A staff member’s normal work base, will be designated upon appointment. The designated work base is the location where normally the employee is required to operate for the majority of their working week. 4.2 Employees will be reimbursed for miles travelled in the performance of their duties, which are in excess of the home to agreed work base return journey. The miles eligible for reimbursement are those travelled from the agreed work base and return. Home to work mileage must be deducted from your business mileage.
4.3 There is no entitlement to claim mileage for the normal home to work or work to home journey. Inland Revenue does not class the journey between home or any other place attended for private purposes and work as business mileage.
5 WORK TIME
5.1 Normal home to work travel time is not classed as working time and therefore, does not count towards hours worked in a day. Business travel time, in excess of the normal home to work travel time, is designated as working time.
6 TRAVEL EXPENSES
6.1 Staff must ensure that they select the most reasonable and cost effective route for their journey. It is expected that journeys will be planned to take the shortest distance. If a particular journey is unusual, in terms of distance or purpose, the mode of travel and the anticipated mileage will be agreed between the staff member and line manager, before it starts.
Page 6 of 8
6.2 Travel should be on public transport except in the instance where the cost of using a private vehicle is less costly.
6.3 This section deals with the reimbursement of costs incurred by staff who, with the agreement of the CCG, use their own vehicles or pedal cycles, to make journeys in the performance of their duties. Full details can be found in the Terms and Conditions of Service Handbook.
6.4 When using their vehicles in the performance of their duties all staff must ensure they possess a valid driving licence, that their vehicle has a current Motoring Organisation Test (MOT) certificate and motor insurance which covers business travel and that evidence is shown to the line manager and recorded on an annual basis. They must also be fit to drive and drive safely and they must obey the relevant laws e.g. speed limits. The employee must inform their line manager if there is a change in status.
6.5 For journeys made directly from and returning to the normal work base, the claim will be for the actual mileage incurred (to the nearest full mile). Where it has not been possible to record the distance, reference can be made to internet sites that have route planning facilities. For any other journeys the employee should claim either the distance travelled or the mileage from the work base to the place visited. The lowest mileage should be claimed. Where a member of staff is either on call or having completed their normal working day is required by the CCG to return to work, then in such circumstances the journey can be recorded and claimed as starting from the employee’s home address.
6.6 Staff who use their vehicles to make journeys in the performance of their duties will be reimbursed their motoring costs at the appropriate rates.
6.7 Passenger allowance is per person per mile. With the exception of lease, pool or hire vehicle users, where other staff or members of the CCG are conveyed in the same vehicle on NHS business and their fares would otherwise be payable by the CCG, the passenger allowance is payable to the vehicle driver.
6.8 Attendance on training courses - additional travel costs incurred when attending courses, conferences or events at the employer’s instigation will be reimbursed at the standard rates when the manager agrees that travel costs should be reimbursed. Subject to the prior agreement of the employer, travel costs incurred when staff attend training courses or conferences and events, in circumstances when the attendance is not required by the employer, will be reimbursed at the reserve rate.
6.9 Other allowances - staff who necessarily incur charges in the performance of their duties, in relation to parking and tolls etc. shall be refunded these expenses on production of receipts. This does not include reimbursement of parking charges incurred as a result of attendance at the normal place of work.
6.10 Staff are personally liable for any excess parking charges or fines issued to them and neither CCGs will provide refunds.
Page 7 of 8
6.11 Pedal cyclists – staff who use pedal cycles to make journeys in the performance of their duties will be reimbursed for eligible miles travelled at the current rate of reimbursement.
6.12 Public transport - if a member of staff uses public transport for business purposes, the cost of bus fares and standard rail fares should be reimbursed.
6.13 Taxi/private hire car - on occasions, it may be necessary to use a taxi/private hire. For example where the cost of the taxi/private hire car is less than public transport; where multiple members of staff are attending the same meeting and the cost is less than taking public transport; or additional equipment is required at the meeting/event. Where this is identified, the employee must obtain written authorisation from their director. If authorisation is not obtained in advance as required, the employee will only be able to claim the cost of the cheapest form of public transport.
6.14 Air travel – if an employee is required to travel abroad for business purposes; economy class air travel should be booked and all flights should be approved by a director or the managing director. Air travel would not normally be appropriate for domestic trips, unless it is cheaper than a standard open rail ticket.
6.15 Where there is a compulsory change of base, either permanent or temporary, resulting in extra public transport costs for the employee, these extra costs will be reimbursed, subject to a maximum period of four years from the date of transfer.
7 SUBSISTENCE EXPENSES
7.1 Subsistence expenses will only be reimbursed for the necessary extra cost of meals (up to the maximum allowances stated in paragraph 7.3 and 7.4 below) over that which would have been spent at the employee’s place of work. As per the Handbook, the cost of alcohol is not claimable. 7.2 It is the personal responsibility of all staff to ensure claims for subsistence are accurate and legitimate. Where staff are uncertain of their eligibility to claim subsistence allowances, they should check with their line manager before incurring any actual costs.
7.3 Night subsistence – For staff who need to stay overnight in a hotel/guest house with the agreement of their manager, the overnight costs will be reimbursed as follows:
the actual receipted cost of bed and breakfast up to a maximum limit of £55 per night a meals allowance (excluding alcohol) to cover the cost of a main evening meal and one other meal up to a maximum of £25.00 per 24 hour period
Any overnight accommodation booked should be within reasonable distance, should the costs be in excess of the maximum limits stated above, the individual will need to meet the difference. There may be exceptional circumstances that may warrant a higher fee (for example, it is the only available hotel in the area), in these
Page 8 of 8
circumstances, authorisation should be sought from the line manager prior to booking.
8 OTHER RELEVANT DOCUMENTS
8.1 Policies relating to: Finance Code of requirements for staff Organisational change Disciplinary Counter fraud and anti-bribery Equal opportunities
9 EQUALITY AND DIVERSITY STATEMENT
9.1 Both CCGs are committed to ensuring that it treats its employees fairly, equitably and reasonably and that it does not discriminate against individuals or groups on the basis of their ethnic origin, physical or mental abilities, gender, age, religious beliefs or sexual orientation.
10 MONITORING OF THE POLICY
10.1 The policy will be reviewed bi-annually by the executive management team.





























