Embed Size (px)
Citation preview
www.elsevier.com/locate/braindev
Brain & Development 34 (2012) 605–608
Case report
Kawasaki disease-associated MERS: Pathological insights fromSPECT findings
Tatsuharu Sato ⇑, Yoko Ushiroda, Toshifumi Oyama, Akiko Nakatomi,Hideki Motomura, Hiroyuki Moriuchi
Department of Pediatrics, Nagasaki University Hospital, Nagasaki, Japan
Received 6 June 2011; received in revised form 6 September 2011; accepted 25 September 2011
Abstract
We report for the first time the single photon emission computed tomography (SPECT) findings of a patient with clinically mildencephalitis/encephalopathy with a reversible splenial lesion (MERS) associated with Kawasaki disease, which showed hypoperfu-sion of the bilateral cingulate gyri, thalamus, basal ganglia, brainstem, and cortex of the frontal lobes. These findings indicate thatthe pathogenesis of MERS is based on cerebral hypoperfusion due to vasculitis or cerebrovascular dehydration.� 2011 The Japanese Society of Child Neurology. Published by Elsevier B.V. All rights reserved.
Keywords: Clinically mild encephalitis/encephalopathy with a reversible splenial lesion (MERS); Kawasaki disease; Single photon emissioncomputed tomography (SPECT); Hyponatremia; Cerebral hypoperfusion
1. Introduction
Clinically mild encephalitis/encephalopathy with areversible splenial lesion (MERS) is a recently describedclinical-radiological entity characterized radiologicallyby the magnetic resonance imaging (MRI) findings of areversible isolated lesion with reduced diffusion in thesplenium of the corpus callosum and clinically by mildneurological symptoms and transient clinical course [1–3]. The neuropathological mechanism remains unknown.MERS has been associated with various infectious dis-eases [1,3,4], such as influenza A [5–7], mumps, measles,varicella, adenoviral infection, rotaviral gastroenteritis,Escherichia coli O-157 enteritis, and Salmonella enteriti-
dis infection, and therefore immunopathological condi-tions may also contribute to its development.
Kawasaki disease (KD) is a systemic vasculitis ofunknown etiology. Neurological complications of KD
0387-7604/$ - see front matter � 2011 The Japanese Society of Child Neuro
doi:10.1016/j.braindev.2011.09.015
⇑ Corresponding author. Address: Department of Pediatrics, Naga-saki University Hospital, 1-7-1 Sakamoto, Nagasaki 852-8501, Japan.
E-mail address: [email protected] (T. Sato).
are rare, with the exception of aseptic meningitis:encephalitis or encephalopathy has only rarely associ-ated with KD [8]. In this report, we present a case ofMERS associated with KD that was analyzed by singlephoton emission computed tomography (SPECT) inboth the acute and recovery phases. To the best of ourknowledge, this is the first report of MERS that was ableto be analyzed by SPECT, and the second report ofMERS associated with KD.
2. Case report
A previously healthy 7-year-old Japanese girl devel-oped right neck pain and high fever 2 days before admis-sion. She had an older brother with a history of KD. Onthe following day, she was seen by a neighboring pedia-trician who prescribed cefdinir, due to a positive groupA streptococcal antigen test for a pharyngeal swab. Onthe day of admission, she developed vomiting anddiarrhea and became somnolent, and she was referredto our hospital.
logy. Published by Elsevier B.V. All rights reserved.
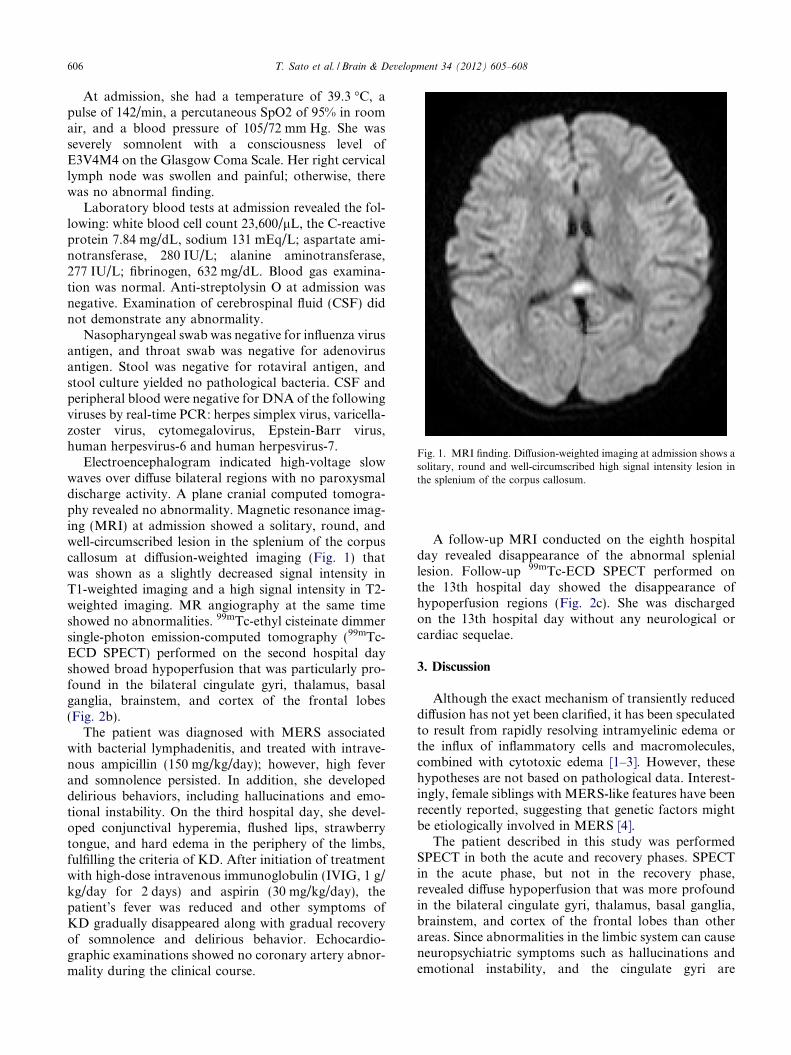
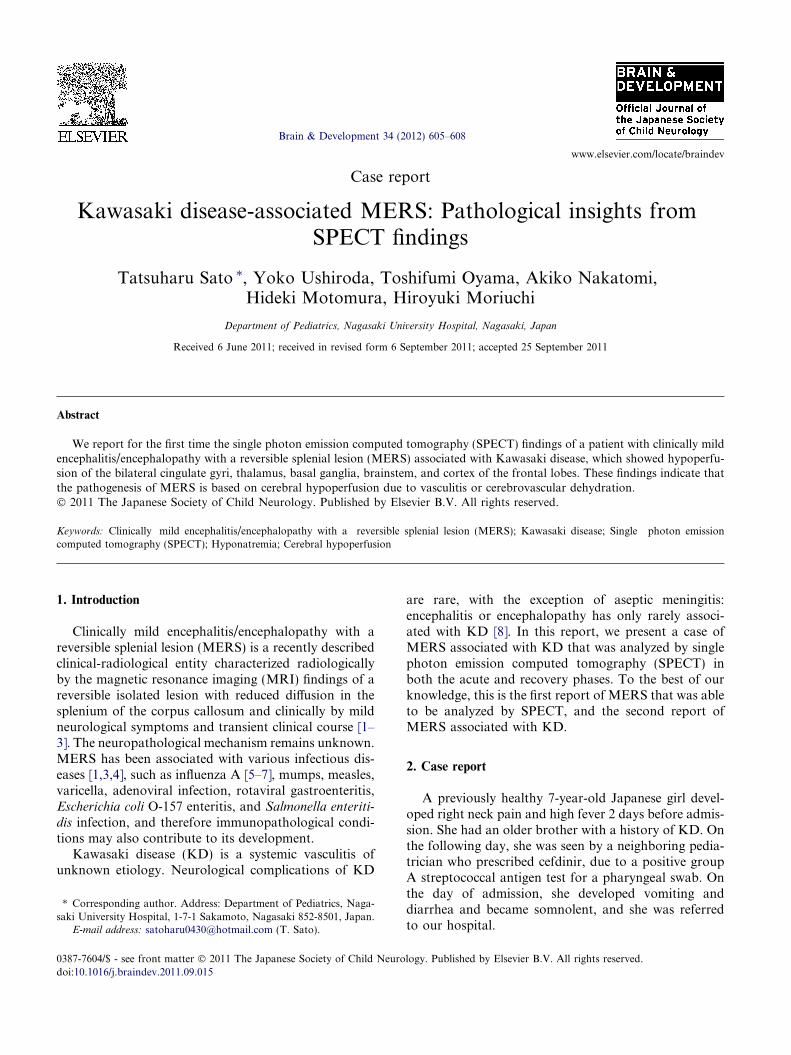
Fig. 1. MRI finding. Diffusion-weighted imaging at admission shows asolitary, round and well-circumscribed high signal intensity lesion inthe splenium of the corpus callosum.
606 T. Sato et al. / Brain & Development 34 (2012) 605–608
At admission, she had a temperature of 39.3 �C, apulse of 142/min, a percutaneous SpO2 of 95% in roomair, and a blood pressure of 105/72 mm Hg. She wasseverely somnolent with a consciousness level ofE3V4M4 on the Glasgow Coma Scale. Her right cervicallymph node was swollen and painful; otherwise, therewas no abnormal finding.
Laboratory blood tests at admission revealed the fol-lowing: white blood cell count 23,600/lL, the C-reactiveprotein 7.84 mg/dL, sodium 131 mEq/L; aspartate ami-notransferase, 280 IU/L; alanine aminotransferase,277 IU/L; fibrinogen, 632 mg/dL. Blood gas examina-tion was normal. Anti-streptolysin O at admission wasnegative. Examination of cerebrospinal fluid (CSF) didnot demonstrate any abnormality.
Nasopharyngeal swab was negative for influenza virusantigen, and throat swab was negative for adenovirusantigen. Stool was negative for rotaviral antigen, andstool culture yielded no pathological bacteria. CSF andperipheral blood were negative for DNA of the followingviruses by real-time PCR: herpes simplex virus, varicella-zoster virus, cytomegalovirus, Epstein-Barr virus,human herpesvirus-6 and human herpesvirus-7.
Electroencephalogram indicated high-voltage slowwaves over diffuse bilateral regions with no paroxysmaldischarge activity. A plane cranial computed tomogra-phy revealed no abnormality. Magnetic resonance imag-ing (MRI) at admission showed a solitary, round, andwell-circumscribed lesion in the splenium of the corpuscallosum at diffusion-weighted imaging (Fig. 1) thatwas shown as a slightly decreased signal intensity inT1-weighted imaging and a high signal intensity in T2-weighted imaging. MR angiography at the same timeshowed no abnormalities. 99mTc-ethyl cisteinate dimmersingle-photon emission-computed tomography (99mTc-ECD SPECT) performed on the second hospital dayshowed broad hypoperfusion that was particularly pro-found in the bilateral cingulate gyri, thalamus, basalganglia, brainstem, and cortex of the frontal lobes(Fig. 2b).
The patient was diagnosed with MERS associatedwith bacterial lymphadenitis, and treated with intrave-nous ampicillin (150 mg/kg/day); however, high feverand somnolence persisted. In addition, she developeddelirious behaviors, including hallucinations and emo-tional instability. On the third hospital day, she devel-oped conjunctival hyperemia, flushed lips, strawberrytongue, and hard edema in the periphery of the limbs,fulfilling the criteria of KD. After initiation of treatmentwith high-dose intravenous immunoglobulin (IVIG, 1 g/kg/day for 2 days) and aspirin (30 mg/kg/day), thepatient’s fever was reduced and other symptoms ofKD gradually disappeared along with gradual recoveryof somnolence and delirious behavior. Echocardio-graphic examinations showed no coronary artery abnor-mality during the clinical course.
A follow-up MRI conducted on the eighth hospitalday revealed disappearance of the abnormal spleniallesion. Follow-up 99mTc-ECD SPECT performed onthe 13th hospital day showed the disappearance ofhypoperfusion regions (Fig. 2c). She was dischargedon the 13th hospital day without any neurological orcardiac sequelae.
3. Discussion
Although the exact mechanism of transiently reduceddiffusion has not yet been clarified, it has been speculatedto result from rapidly resolving intramyelinic edema orthe influx of inflammatory cells and macromolecules,combined with cytotoxic edema [1–3]. However, thesehypotheses are not based on pathological data. Interest-ingly, female siblings with MERS-like features have beenrecently reported, suggesting that genetic factors mightbe etiologically involved in MERS [4].
The patient described in this study was performedSPECT in both the acute and recovery phases. SPECTin the acute phase, but not in the recovery phase,revealed diffuse hypoperfusion that was more profoundin the bilateral cingulate gyri, thalamus, basal ganglia,brainstem, and cortex of the frontal lobes than otherareas. Since abnormalities in the limbic system can causeneuropsychiatric symptoms such as hallucinations andemotional instability, and the cingulate gyri are
Fig. 2. 99mTc-ECD SPECT findings. (a) 99mTc-ECD SPECT on the second hospital day shows broad hypoperfusion. (b) Broad hypoperfusionshowed by (a) was particularly profound in the bilateral cingulate gyri, thalamus, basal ganglia, brainstem, and cortex of the frontal lobes. (c) 99mTc-ECD SPECT on the thirteenth hospital day shows the disappearance of hypoperfusion regions.
T. Sato et al. / Brain & Development 34 (2012) 605–608 607
integrated in the limbic system, clinical and radiologicalfindings would be compatible.
MERS is classified into types 1 and 2, both of whichexhibit an almost identical pathophysiology [9]. Whiletype 1 exhibits only splenial corpus callosum lesions,type 2 exhibits white matter lesions in addition to lesionsof the entire corpus callosum; however, the spleniallesion is always the last to disappear. While MRIdetected abnormality only in the splenium in thispatient, SPECT indicated hypoperfusion in areas withnormal MRI findings, some of which overlap withlesions involving MERS type 2. It is possible that suchhypoperfusion generally occurs in other MERS cases;however, it remains unknown why the splenial corpuscallosum is specifically involved.
Recently, KD associated with MERS in a 14-year-oldfemale was reported for the first time [8]. Ichiyama et al.[10] demonstrated that 6 of 21 KD patients had transientlocalized cerebral hypoperfusion on the SPECT in theacute stage, and speculated that cerebral vasculitis ledto the hypoperfusion [10]. In addition, Hikita et al.[11] performed SPECT for 22 KD patients includingfour with neurologic symptoms, and demonstratedlocalized hypoperfusion in all of the four with and other13 without neurologic symptoms. Interestingly, one ofthem had an abnormal high intensity area in the corpuscallosum in the diffusion-weighted imaging, although hisclinical and radiological findings were not compatiblewith those of MERS. Thus, it is possible that KD itselfoccasionally cause cerebral hypoperfusion. However, itis important to mention that while KD patients in the
previous studies showed only partial hypoperfusion withor without neurologic symptoms, the present study dem-onstrated diffuse hypoperfusion with no lateralization aswell as characteristic neuropsychiatric symptoms, imply-ing the different pathophysiological mechanism in thepresent patient.
KD may be complicated with cerebral vasculitis thatleads to hypoperfusion; however, a lack of abnormalfindings in the MR angiography did not support thishypothesis.
Another possibility is that cerebrovascular dehydra-tion with hyponatremia led to cerebral hypoperfusion.Recently, the association of MERS with hyponatremiahas been reported [12]. Hypotonic hyponatremia resultsin cerebral edema due to water that is allowed to enterinto the brain [12]. Hyponatremia, which is involved ina number of pathological processes, is frequentlyobserved in many viral infections and KD, as seen in thiscase study. Since the present patient also had hyponatre-mia at admission, it is also a likely explanation for cere-bral hypoperfusion, which results in brain edema,intramyelinic edema, or cytotoxic edema. Though themechanism remains to be determined, the present report,in addition to previous studies, may indicate that enceph-alopathic events must be taken into consideration whenKD patients develop even subtle neurological symptoms.
In conclusion, we herein reported the SPECT findingsof MERS associated with KD for the first time, andshowed evidence of diffuse cerebral hypoperfusion inthe neuropathogenesis in this patient. To clarify whetheror not this process is etiologically responsible for other

608 T. Sato et al. / Brain & Development 34 (2012) 605–608
MERS patients, further studies such as SPECT onMERS patients with or without KD are warranted.
Acknowledgment
We thank Masako Moriuchi for real-time PCR assays.
References
[1] Takanashi J. Two newly proposed infectious encephalitis/enceph-alopathy syndromes. Brain Dev 2009;31:521–8.
[2] Yeh IB, Tan LC, Sitoh YY. Reversible splenial lesion in clinicallymild encephalitis. Singapore Med J 2005;46:726–30.
[3] Tada H, Takanashi J, Barkovich AJ, et al. Clinically mildencephalitis/encephalopathy with a reversible splenial lesion.Neurology 2004;63:1854–8.
[4] Imamura T, Takanashi J, Yasugi J, Terada H, Nishimura A.Sisters with clinically mild encephalopathy with a reversiblesplenial lesion (MERS)-like features; familial MERS? J NeurolSci 2010;290:153–6.
[5] Ganapathy S, Ey EH, Wolfson BJ, Khan N. Transient isolatedlesion of splenium associated with clinically mild influenzaencephalitis. Pediatr Radiol 2008;38:1243–5.
[6] Matsubara K, Kodera M, Nigami H, Yura K, Fukaya T.Reversible splenial lesion in influenza virus encephalopathy.Pediatr Neurol 2007;37:431–4.
[7] Bulakbasi N, Kocaoglu M, Tayfun C, Uc�oz T. Transient spleniallesions of the corpus callosum in clinically mild influenza-associated encephalitis/encephalopathy. Am J Neuroradiol2006;27:1983–6.
[8] Itamura S, Kamada M, Nakagawa N. Kawasaki disease compli-cated with reversible splenial lesion and acute myocarditis. PediatrCardiol 2011;32:696–9.
[9] Takanashi J, Imamura A, Hayakawa F, Terada H. Difference inthe time course of splenial and white matter lesions in clinicallymild encephalitis/encephalopathy with a reversible splenial lesion(MERS). J Neurol Sci 2010;292:24–7.
[10] Ichiyama T, Nishikawa M, Hayashi T, Koga M, Tashiro N,Fukukawa S. Cerebral hypoperfusion during acute Kawasakidisease. Stroke 1998;29:1320–1.
[11] Hikita T, Kaminaga T, Wakita S, Ogita K, Ikemoto H, Fujii Y,et al. Regional cerebral blood flow abnormalities in patients withKawasaki disease. Clin Nucl Med 2011;36:643–9.
[12] Takanashi J, Tada H, Maeda M, Suzuki M, Terada H, BarkovichAJ. Encephalopathy with a reversible splenial lesion is associatedwith hyponatremia. Brain Dev 2009;31:217–20.

![MERS Legal FAQs[1] - Trillion Dollar FUBARtrilliondollarfubar.com/Court/Docs/MERS Legal.pdf · MERS LEGAL FAQs TABLE OF CONTENTS I. INTRODUCTION TO MERS ... Terms and Conditions,](https://img.pdfslide.us/doc/110x75/5ac313797f8b9a5c558b522c/mers-legal-faqs1-trillion-dollar-fuba-legalpdfmers-legal-faqs-table-of-contents.jpg)



























