Embed Size (px)
Citation preview

Kansas Heart and Stroke Collaborative
Overview and Update
April 26, 2017

The Kansas Heart & Stroke Collaborative
A Rural Clinically Integrated Network, focused on a care delivery and payment reform model to improve rural Kansans’ heart health and stroke outcomes and
reduce total cost of care for that population.
A CMMS Innovation Center HCIA2 Cooperative Award with The University of Kansas Hospital

Issues in Rural Kansas
• Inconsistent adoption of current evidenced based guidelines with Time Critical Diagnoses
• KS hospitals rarely performed Heart Cath within 90 minutes of First Medical Contact when patient transferred to them
• Less than 3% of eligible patients with ischemic stroke received thrombolytic therapy
• Higher mortality rates in rural Kansas
• Higher hospital readmissions in rural Kansas

1. CARE DELIVERY MODEL

Goal and Strategies
• “…to improve rural Kansans’ heart health and stroke outcomes and reduce total cost of care”
• Four strategies
1. Acute Care
2. Transitions of Care
3. Care Coordination and Patient Engagement
4. Population Health Management
5

KHSC Delivery of Care Model Strategies
Acute Care Focus
• Improve outcomes for heart attacks and stroke and reduce total cost of care.
– Evidence Based Guidelines and order set adoption after review/updates with local realities considered
– Telemedicine support to Critical Access Hospitals with Avera e-Emergency services
– Education Programs at local level engaging all community stakeholders

• Transitional Care Management (TCM) and Chronic Care Management (CCM) – Improve transitions of care and care coordination to
reduce readmissions – Billable services - part of sustainability plan
*Participating sites notify KHSC Hays Office when MI or Stroke patient transferred – TCM notified *TCM manager works with Discharge Planning at larger health system to engage patient in TCM upon discharge *TCM Manager hands patient off after 30 days to local Health Coach for CCM which includes a detailed assessment - includes screening for social determinants
KHSC Delivery of Care Model Strategies

KHSC Delivery of Care Model Strategies
Care Coordination Focus • Local “Health Coaches” identified, hired & trained
– Extension of local primary care system • Billable service to support infrastructure going forward
– Focus: Improve patient engagement/education and self-management skills and provide Chronic Care Management (CCM) • Efficiency of CCM improved with added technology -
Cerner’s HealtheCare module adopted August 2016
• Implemented Telehealth Coach capabilities August 2016

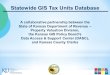
Health Coach Encounters
0 34 72 175 232 316 525
0 0 104 310
835
2,639
4,895
0 0 36 46 60 254
1,607
0
1,000
2,000
3,000
4,000
5,000
Q4 Q5 Q6 Q7 Q8 Q9 Q10
Growth in Health Coach Encounters by Encounter Type
In Person
Telephone
Electronic
Telehealth
Other

KHSC Delivery of Care Model Strategies
Population Health – Move to Clinical Care Focus
• Goal of KHSC is to reduce incidence and mortality of MI and Stroke – Risk stratification of population and focus on PI related
to hypertension, hyperlipidemia and tobacco cessation
– Technology to create Patient Registries and Performance Dashboards • Same Approach as Acute Care efforts in KHSC
– Implement best practices based on EB-Guidelines
– Work on clinical pathways,
– Work flow based on evidence based guidelines and team based care – involves the “medical neighborhood”, including public health

Findings 1. KHSC’s acute and ambulatory interventions are
succeeding – and KHSC participation is accelerating beyond expectations and new conditions being added
2. Developed KHSC Communications Committee to improve patient handoff’s and feedback loops
3. Partnered with all 20 EMS Services in EMS Region I to look at funding and training opportunities
4. KHSC model is improving quality, outcomes and lowering costs, as well as capturing new revenue
5. KHSC is sustainable - Opportunity to capitalize on shared savings revenue through the MSSP (Medicare Shared Savings Program) for sustainability

Current KHSC Participation
KHSC and/or KCIC Executed Agreements Received Overview and/or Expressed Interest KHSC Original Sites

Acute Care Progress Improving ----
Time to EKG
Time to EKG read Time CT Time to CT report Time to Thrombolytic
Time to Thrombolytic

Cardiac Measures Q10

Stroke Measures

Impact on Ischemic Stroke
• Baseline data showed <3% eligible received thrombolytic
• Through 10th Quarter
– 18% of eligible patients now receiving thrombolytic overall with 30% in Q10
– 50% of patients presenting outside of window for treatment
• Started out around 40%
• New studies demonstrating opportunities for interventions further out from onset

STEMI Success
• Previously found no STEMI getting to Cath Lab within 90 minutes from First Medical Contact
– Significant improvement in time to thrombolytic in those hospitals more than 1 hour from Cath Lab
– Increasing percentage of STEMI patients with Door In to Door Out at CAH of 30 minutes or less
• Includes both patients receiving thrombolytic or those transferred for primary Heart Cath
• Record so far is 13 minutes for primary Heart Cath!!

Expanded Clinical Interventions
• April 2016 - Introduced sepsis as additional time-critical diagnosis
– Data collection specific to sepsis completed and ongoing

Patient Safety Organization
• KHSC Identified need to engage in PI activities in protected environment
• Listed as Patient Safety Organization with AHRQ in December 2016
• Privilege and confidentiality protections beyond state peer review laws

Pursuing Performance Improvement
• Rural providers face challenges in adopting formal PI programs
• Leverage resources across participating communities
– KHSC Provides • Data extraction, normalization, analysis, and reporting, and
• Develop, implement, and monitor specific PI initiatives by site
• Secret to our success
– Local “classroom” approach
– Provide protocols, templates and assist with understanding their work flow

Public Health Opportunities in KHSC Findings
• More than 75% of patients with either MI or Stroke present to the ER by private care
– Seeing some improvement in Stroke in last quarter – 40%
– Awareness of signs and symptoms part of the education for communities
• Need for raising community awareness of Sepsis signs and symptoms and activating 911
– Early broad spectrum antibiotic significantly improves survival
• Awareness of Chronic Care Management services locally

Public Health Opportunities in KHSC Findings
Opportunities to Assist Clinics in community programs and alignment
• Areas of Population Health Focus in Clinics – Tobacco Cessation
• Starts with best practice of “asking” at each visit.
• Template created to collect information “assess” – saves provider time to get to “act”
– Treating Hypertension to Goal • Starts with proper BP measurement technique training for staff and patients.
• https://www.ama-assn.org/sites/default/files/media-browser/public/about-ama/iho-bp-proper-positioning-technique-english_0.pdf
– Treating high cholesterol to goal • Starts with decreased variation and simple approaches for patients;
• DASH Diet focused on portions, low salt and increasing servings of fruits and vegetables.
• https://www.nhlbi.nih.gov/files/docs/public/heart/hbp_low.pdf

2. IMPACT ON COST OF CARE

Medicare Claims Data Warehouse
• Claims data from ResDAC – All Part A and B claims for all traditional Medicare
beneficiaries residing in Kansas, 2007-2016
– Identifiable data, thus subject to restrictive data use agreement
• PL/pgSQL Database – Developed by PYA Analytics data scientists
– Decrypt, structure, and reconcile multiple data files
– Validated against 2014 LDS Standard Analytic Files (de-identified Medicare claims data)

Total Cost of Care • Average PBPM cost by primary diagnosis
• Compare pre-intervention (2014) and post-intervention (Q1 and Q2 2016)
– No adjustment for absolute amount of growth in national Medicare per capita expenditures
• Calculate for residents of communities in which original sites are located

AMI Episodes
Treatment in local community + transfer
• Inpatient services • Post-acute care • Related readmissions • Clinical lab services • Outpatient services
• Physician services • Independent outpatient
therapy • Other Part A and B
covered services
AMI-Related Discharge
Through 90 days post-discharge
-------------------------SERVICES INCLUDED -------------------------
Rx

Calculating Episodic Costs • Use CMS’ AMI episode definition + pre-admission
costs in home community
• Traditional Medicare beneficiaries residing in communities in which original sites located with AMI-related discharge during relevant time period
• Compare pre-intervention (2013) and post-intervention (Q1 and Q2 2016)
– No adjustment for absolute amount of growth in national Medicare per capita expenditures

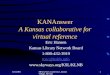
Reduction In Average AMI Episode Costs and Cases
2013 2016 (Q1 & Q2)
21% Cost Reduction
38% Case Reduction
$24,000
$ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $
$19,000
$ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $ $
(annualized)
56 episodes 91 episodes

Reduction In Total Cost of Care
$1,015 $1,091
$2,020
$1,428
$971 $1,085
$1,896
$1,512
Hyperlipidemia Hypertension STIA Tobacco
2014 2016
2.2% 0.3%
3.1%
2.9%

3. SUSTAINABILITY

Next Steps Kansas Clinical Improvement Collaborative • Moving to Medicare Shared Savings Program
– An ACO – no risk or Track 1 model that is part of sustainability plan for KHSC – required a new legal entity to move this direction
• New participating sites will be on boarded using the same model as KHSC. – Acute care focus on MI/Stroke/Sepsis and starting CHF May
2017 – Utilizing TCM and CCM services for appropriate patients – Current KHSC sites not pursuing MSSP with KCIC will
continue with activities but will have to support own TCM, CCM and technology.

The project described was supported by Funding Opportunity Number CMS-1C1-14-001 from the U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services. The contents provided are solely the responsibility of the authors and do not necessarily represent the official views of HHS or any of its agencies.