Embed Size (px)
Citation preview

Kacy Aderhold, MSN, APRN-CNS, CMSRN

Promote and support healthy eating patterns ◦ Attain individualized glycemic, blood pressure, and lipid goals ◦ Achieve and maintain body weight goals ◦ Delay or prevent complications of diabetes
Emphasize a variety of nutrient dense foods in appropriate portion sizes
Address individual needs & barriers to change ◦ Culture ◦ Health literacy ◦ Access to healthy food ◦ Behavioral changes
Maintain pleasure of eating
Provide practical tools for day to day meal planning
(ADA, 2015)

“The goals of Medical Nutrition Therapy (MNT) in the hospital are to optimize glycemic control, to provide adequate calories to meet metabolic demands, and to create a discharge plan for follow-up care. The American Diabetes Association (ADA) does not endorse any single meal plan or specified percentages of macronutrients, and the term “ADA diet” should no longer be used. Current nutrition recommendations advise individualization based on treatment goals, physiologic parameters, and medication usage. Consistent carbohydrate meal plans are preferred by many hospitals since they facilitate matching the prandial insulin dose to the amount of carbohydrate consumed.” (ADA, 2011)


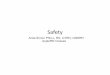
USDA, (2011) www.choosemyplate.gov
Balance calories Make ½ plate fruits &
vegetables Eat whole grains Switch to skim milk Avoid oversized portions Do not skip meals Eat about every 4 hours Choose food low in sodium Drink water instead of
sugary drinks
----------9 inches----------

Fruits: A serving of fruit is 1 small fresh fruit, 2 tbsp dried fruit, or ½ cup canned fruit or 4 oz unsweetened fruit juice
Vegetables: Choose nonstarchy vegetables, such as broccoli, carrots, cauliflower or green beans
Grains: Fill ¼ of the plate with a bread, cooked grain, or starchy vegetable such as corn, brown rice, or potatoes. Choose whole grains more often.
Dairy: Add 1 cup fat-free/low-fat milk or 2/3 cup fat-free/low-fat/light yogurt
Protein: Fill this ¼ of the plate with lean meat, poultry, or fish. If you choose a plant-based protein such as dried beans, consider the carbohydrate content as part of your total carbohydrate for the meal.


A healthy meal plan for patients with diabetes has foods from all major food groups (including carbs).
Carbohydrates raise blood glucose levels the most, but are an important part of a healthy meal plan.
Allows for variable intake and extra foods eaten between meals

Carbohydrates ◦ Have a significant effect on post-prandial blood glucose ◦ Equal amounts of carbs will have a similar impact on blood
glucose regardless of the source. ◦ Carbs are found in fruits, starchy vegetables, grains, milk,
yogurt, sweets, & sodas. ◦ Recommended carbs come from fruits, vegetables, whole
grains, legumes, and low-fat dairy
Fiber ◦ Adds bulk to meals and helps us feel fuller longer ◦ Beans, whole grains, brown rice, popcorn, nuts, baked
potato skin, berries, oatmeal, bran, vegetables ◦ If a food contains more than 5 gm of fiber, you can subtract
½ of the amount of fiber from the total grams of carbohydrate

15 grams of carbohydrate = 1 carb serving ◦ 1 cup milk (8oz) ◦ 1 small piece of fruit ◦ 1 slice of bread ◦ 1/3 cup cooked rice or pasta ◦ 4 oz. fruit juice or regular pop ◦ 2 small cookies
For most women, 45-60 grams of carbs (3-4 servings)
at each meal works well with 15 grams (1 serving) for snacks
For most men, 60-75 grams of carbs (4-5 servings) at each meal works well with 15-30 grams (1-2 servings) for snack
Carb Counting Video



Patients need to Look at 2 Things to Count Carbs
Serving Size or how many servings are in one bag/container
Total carbohydrates Remember you are teaching survival skills. The patient will need to follow up with a dietician after discharge.

If patients are carb counting, they need to know which foods to count. Typically, patients will need to count starchy carbs, fruits, milk, and sweets/desserts. Foods patients can consider “free” are proteins/meats, fats, and non-starchy vegetables like broccoli and spinach.
Remember you are teaching survival skills. The patient will need to follow up with a dietician after discharge.

Mealtime insulin is ordered as follows: 1 unit of Novolog (aspart) per 15 grams of carbohydrate with meals. The patient eats the following meal:
Ham Sandwich w/ mayo ____
Small banana ____
4 oz fruit juice ____
How much insulin would you give?
4 Units

Educate patient and family to report if anyone other than the patient ate anything on their tray.
Educate patient and family to report any extra food or beverages patient consumes.

When carb counting, don’t forget to include snacks and beverages.
Carb counting is not just for meal time.
Insulin must be given for these additional carbs in order to maintain euglycemia.
If only dosing for meals, BG fluctuations can occur.

Fat
◦ Limit saturated fat
◦ Fat has little effect on post prandial glucose
◦ Minimize trans fats to reduce risk of CV disease
◦ Two or more servings fish per week recommended
Cholesterol
◦ Limit cholesterol to less than 200 mg/day

Does not raise plasma glucose, but does stimulate insulin response
Should not be used to treat or prevent hypoglycemia
High protein diets generally not recommended

Chronic Kidney Disease ◦ Reduced protein diet may be beneficial for improving
kidney function in patients with kidney disease
Cardiovascular Disease ◦ Diets high in fruits, vegetables, whole grains, and nuts
may reduce risk.
Congestive Heart Failure ◦ Sodium less than 1500-2000 mg/day may reduce
symptoms
Hypertension ◦ 1500 mg/day sodium and a diet high in fruits,
vegetables, and low-fat dairy products lowers blood pressure

(Lustig, 2012)

Decreased appetite or no oral intake
Nausea/vomiting
Delayed meals/inconsistent meal timing
Inconsistent carbohydrate intake
Decreased activity level
Sudden interruption of either parenteral (TPN) or enteral (TF) nutrition.
Inadequate coordination of FSBS checks, meal tray delivery & insulin injections

NPO patients may still require basal insulin
Snacks are not mandatory for all patients-should be based on needs, preferences, medications

Provider who will manage DM after discharge
Assess need for HH or outpatient DM education ◦ Diagnosis
◦ SMBG & home goals
Information on consistent eating patterns
When & how to take BG lowering medications
Sick day management
Proper use & disposal of needles & syringes
(ADA, 2014)

ADA/ACC (2010). Choose to Live; Your Diabetes Survival Guide Ediba Diabetes Center of Excellence (2007). Diabetes Today: An update for health
care professionals. Moghissi, E., Korytkowski, M., DiNardo, M., Einhorn, D., Hellman, R., Hirsch, I.,
Inzucchi, S., Ismail-Beigi, F., Kirkman, S., & Ummpierrez, G., (2009). American association of clinical endocrinologists and american diabetes association consensus statement on inpatient glycemic control. Endocrine Practice, 15 (4). 1-17.
American Diabetes Association (2011). Clinical practice recommendations. Diabetes Care, 34 (1), S46
American Diabetes Association. Standards of Medical Care in Diabetes—2010 (Position Statement). Diabetes Care, 33(1), S11-S61
American Diabetes Association. Nutrition recommendations and interventions for diabetes. (Position Statement). (2008). Diabetes Care, 31(Suppl.1), S61-S78.
Gallagher Allred, C. R., Voss, A. C., Finn, S. C., & McCamish, M. A. (1996). Malnutrition and clinical outcomes: The case for medical nutrition therapy. Journal of the American Dietetic Association., 96(4), 361-369.
McKnight, K., and Carter, L. (2008). From trays to tube feedings: Overcoming the challenges of hospital nutrition and glycemic control. Diabetes Spectrum, 12(4), 233-240.