-
n engl j med 371;21 nejm.org November 20, 20142018 n engl j med
371;21 nejm.org November 20, 20142018
Pr esen tation of C a se
Dr. Nicholas A. Morris (Neurology): An 18-year-old woman was
admitted to this hos-pital because of fever, pharyngitis, facial
swelling, and diplopia.
The patient had been well until 2 weeks before the current
admission, when a headache and sore throat developed, without a
fever. On evaluation at her physi-cians office, a rapid test for
streptococcal pharyngitis was negative, and she re-turned home.
During the next 2 days, throat pain persisted and oral intake
de-creased. She was admitted to the observation unit of another
hospital because of dehydration, weakness, and fevers, with a
temperature as high as 39.4C. A chest radiograph was normal.
The patient reportedly had a white-cell count of less than 2000
per cubic mil-limeter, positive tests for IgG and IgM antibodies to
EpsteinBarr virus (EBV)spe-cific viral capsid antigen and
antibodies to EBV nuclear antigen, and negative tests for
heterophile antibodies, influenza A and B viruses, and IgM and IgG
antibodies to cytomegalovirus (CMV). A pharyngeal culture grew
group C streptococcus. Cultures of the blood and urine were
sterile. A diagnosis of infectious mononucle-osis with possible
bacterial superinfection was made. Intravenous fluids were
ad-ministered, and her condition improved. On day 2, treatment with
erythromycin was begun and she was discharged home.
Nine days before the current admission, trismus, pain on opening
the mouth, and swelling on the right side of the face and jaw
developed. The patient returned to the emergency department of the
same hospital; parotitis was diagnosed, and ibuprofen was
administered. Pain persisted on the right side of the jaw and was
associated with temperatures as high as 38.3C and swelling and
erythema of the right parotid gland and face.
Six days before the current admission, the patient was seen at a
second hospital; prednisone and narcotic analgesic agents were
administered, and massage of the parotid gland was performed. She
returned home. Fevers persisted, and edema of the right lateral
side of the face and neck worsened. Three days later, she was seen
by her physician and was admitted to the second hospital. Computed
tomography (CT) of the head and neck reportedly revealed no
evidence of retropharyngeal or periton-
From the Departments of Medicine (K.R.O.), Pediatrics (K.R.O.),
Radiology (J.M.J.), and Pathology (J.A.B.) and the Center for
Global Health (K.R.O.), Massachusetts General Hospital; the
Departments of Medicine (K.R.O.), Pediatrics (K.R.O.), Radiology
(J.M.J.), and Pathology (J.A.B.), Harvard Medical School; and the
Department of Ophthalmology (S.K.F.), Massachusetts Eye and Ear
Infirmary all in Boston.
N Engl J Med 2014;371:2018-27.DOI:
10.1056/NEJMcpc1310001Copyright 2014 Massachusetts Medical
Society.
Founded by Richard C. Cabot Eric S. Rosenberg, M.D., Editor
Nancy Lee Harris, M.D., Editor JoAnne O. Shepard, M.D., Associate
Editor Alice M. Cort, M.D., Associate Editor Sally H. Ebeling,
Assistant Editor Emily K. McDonald, Assistant Editor
Case 36-2014: An 18-Year-Old Woman with Fever, Pharyngitis, and
Double Vision
Kristian R. Olson, M.D., M.P.H., Suzanne K. Freitag, M.D., Jason
M. Johnson, M.D., and John A. Branda, M.D.
Case Records of the Massachusetts General Hospital
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 2014 2019
Case Records of the Massachusetts Gener al Hospital
sillar abscesses. Trimethoprimsulfamethoxazole, clindamycin, and
intravenous fluids were ad-ministered.
Two days before the current admission, swell-ing of the right
eyelids and horizontal diplopia developed. On evaluation, there was
decreased abduction of the right eye. Imaging studies were
obtained.
Dr. Jason M. Johnson: Magnetic resonance imag-ing (MRI) of the
head and neck, performed with and without the administration of
contrast ma-terial, revealed a multiloculated, rim-enhancing fluid
collection in the right parotid gland and inflammation of the
masticator space. There was linear enhancement of the pachymeninges
in the right temporal region, a finding that raised con-cern about
meningitis. Diffusion-weighted im-ages obtained at the level of the
parotid gland showed findings consistent with an abscess. There was
an irregularity of the right cavernous sinus, without definite
thrombosis. A subperios-teal abscess in the right orbit was also
identified.
Dr. Morris: The patient was transferred to a third hospital. On
examination, she was alert and communicative. The vital signs and
oxygen satu-ration were normal. There was diffuse swelling of the
right preauricular and periorbital areas, mild trismus, bilateral
cervical submental and submandibular lymphadenopathy (greater on
the right side than on the left), and preauricular and
postauricular lymphadenopathy on the right side. White plaque was
seen on the gingivobuccal sul-cus and anterior tongue, which was
painful when scraped. The right Stensens duct was tender on firm
compression, with no fluid discharge. On neurologic examination,
the right eye had medial deviation, with an inability to abduct
past the mid-line. The patient had mild difficulty with tan-dem
walking. The general and neurologic ex-aminations were otherwise
normal. The activated partial-thromboplastin time, red-cell
indexes, and results of renal-function tests were normal, as were
levels of electrolytes, magnesium, globulin, angiotensin-converting
enzyme, and IgG, IgA, and IgM. Tests for heterophile antibodies,
antibodies to human immunodeficiency virus (HIV) types 1 and 2, and
HIV nucleic acid were negative; other test results are shown in
Table 1. Urinalysis re-vealed trace protein, 3+ glucose, and 2+
urobi-linogen, along with squamous epithelial cells and bacteria,
findings suggestive of contamination.
Dr. Johnson: MRI of the head, orbits, face, and
neck, performed with and without the adminis-tration of contrast
material (Fig. 1), reportedly revealed changes consistent with
multiple lobu-lated abscesses in the right parotid gland, with
extensive inflammation surrounding the gland that involved the
muscles of mastication, as well as a small subperiosteal abscess
along the right lateral orbital wall, dural enhancement along the
right temporal lobe, and enhancement along the cavernous sinus;
these findings were again not thought to constitute definite
evidence of throm-bosis. Changes consistent with extensive
peri-odontal disease were also seen. Vancomycin, meropenem, and
clindamycin were administered. Ultrasound-guided percutaneous
fine-needle as-piration of fluid collected in the parotid gland was
performed, and the aspirate was cultured. The following day, CT of
the sinuses, performed with the administration of contrast
material, re-portedly revealed preseptal swelling of the right eye
extending to the temporal fossa, subperios-
VariableReference Range,
AdultsOn Admission to
Third Hospital
Hematocrit (%) 3648 28.0
Hemoglobin (g/dl) 11.516.4 9.8
Whitecell count (per mm3) 400010,000 8290
Differential count (%)
Neutrophils 4876 80.6
Lymphocytes 1841 11.3
Monocytes 4.011.0 7.7
Basophils 01.5 0.4
Platelet count (per mm3) 150,000450,000 119,000
Prothrombin time (sec) 12.214.6 15.8
Prothrombintime international normalized ratio
0.91.1 1.2
Glucose (mg/dl) 70100 173
Glycated hemoglobin (%) 4.25.8 5.9
Total protein (g/dl) 6.48.3 5.9
Albumin (g/dl) 3.55.2 2.3
Calcium (mg/dl) 8.810.7 7.9
Phosphorus (mg/dl) 2.44.3 3.3
* To convert the values for glucose to millimoles per liter,
multiply by 0.05551. To convert the values for calcium to
millimoles per liter, multiply by 0.250. To convert the values for
phosphorus to millimoles per liter, multiply by 0.3229.
Reference values are affected by many variables, including the
patient population and the laboratory methods used. The reference
ranges are those used at the third hospital.
Table 1. Laboratory Data.*
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 20142020
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
teal enhancement adjacent to the right lateral rectus muscle,
and heterogeneous enhancement and enlargement of the right parotid
gland; there was no substantial improvement in the appear-ance of
the orbital or parotid abnormalities as compared with the previous
imaging studies.
Dr. Morris: The patient was transferred to Mas-sachusetts Eye
and Ear Infirmary, which is af-filiated with this hospital.
Medications on transfer included vancomycin, meropenem,
clindamycin, trimethoprimsulfamethoxazole, and enoxaparin, as well
as an albuterol inhaler, lorazepam, oxy-
codone, ibuprofen, and acetaminophen, as need-ed. She reported
having fatigue and double vision, without headache, pain in her eye
or throat, or pain with eye movements. She had a history of
dysmenorrhea, for which she took norethindrone acetate and ethinyl
estradiol oral contraceptives, and asthma. She was allergic to
penicillins, which had caused urticaria, and was possibly allergic
to cephalosporins. She lived with her family and attended high
school. She did not smoke, drink alcohol, or use illicit drugs, and
she had had no travel-related exposures.
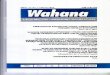
Figure 1. MRI Scans of the Head and Neck.
T1weighted images of the head and neck were obtained after the
administration of contrast material. A coronal image of the head
shows temporal pachymeningeal enhancement and subtle leptomeningeal
enhancement, findings suggestive of basilar and temporal meningitis
(Panel A, arrows). A coronal fatsaturated image (Panel B) and an
axial diffusionweighted image (Panel C) show changes consistent
with abscess formation in the right parotid gland (arrows). Axial
and coronal fatsaturated images (Panels D and E, respectively) show
changes consistent with a subperiosteal abscess in the right orbit
(arrows).
A B C
ED
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 2014 2021
Case Records of the Massachusetts Gener al Hospital
On examination, the patient was somnolent but arousable. The
vital signs were normal, as was the oxygen saturation while she was
breath-ing ambient air. The right parotid gland, face, and neck
were swollen, with marked periorbital edema of the right eyelid,
minimal erythema and tenderness, and no palpable fluctuance; the
right eye had 1+ lateral clear chemosis (Fig. 2). The right parotid
gland was tender. There was a whitish plaque on the inner aspect of
the right buccal mucosa, which was tender and had no obvious
abscesses. The patient was able to swal-low oral secretions. A
systolic murmur, grade 1 out of 6, was heard at the left lower
sternal border. There was bilateral submandibular lymphade-nopathy,
greater on the right side than on the left. On neurologic
examination, visual acuity was 20/30 in the right eye and 20/20 in
the left. In the right eye, supraduction was limited by 50%,
abduction was slightly limited, and infraduction and adduction were
normal; the left eye had normal motility, with splinting on upgaze.
Other cranial-nerve functions (excluding smell, which was not
tested) and the remainder of the general and neurologic
examinations were normal.
Diagnostic procedures were performed, and the patient was
admitted to this hospital.
Differ en ti a l Di agnosis
Dr. Kristian R. Olson: This patient is a previously healthy
18-year-old woman whose illness began with a sore throat and
progressed to include fe-ver, facial swelling, and a deficit on
abduction of the right eye. Fourteen days before this admis-sion,
the patient had a sore throat and headache; at this time, her
presentation was consistent with acute pharyngitis, a diagnosis
that accounts for 6% of all outpatient visits in the United
States.1
Pharyngitis
Over the ensuing 2 days, a high temperature de-veloped, throat
pain persisted, and oral intake decreased, resulting in the
patients first hospi-talization. My differential diagnosis at this
point includes infectious pharyngitis, which can be caused by such
viruses as rhinovirus, coxsackie-virus, and adenovirus.
Mononucleosis-like illness-es, including EBV, CMV, and acute HIV
infections, should be considered together, because it is not
possible to distinguish among these infections clinically.2
Although testing for heterophile anti-
bodies was negative, only 25% of patients with EBV infection
have detectable heterophile antibod-ies in the first week, and 10%
never have these antibodies.3 This patients EBV-specific antibody
profile provides evidence of recent EBV infection; however, the
fulminant nature of her illness is not consistent with this
diagnosis alone. Serologic testing for CMV was negative. Testing
for HIV antibodies and HIV RNA (viral load) was negative, and there
was no history of sexual activity or other risk factors that would
raise concern about acute HIV infection.
An initial throat culture grew group C strep-tococcus; infection
with this organism can be clinically indistinguishable from group A
strep-tococcal infection.4 I suspect that this is un-
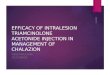
Figure 2. Photographs of the Patients Eye.
On presentation to the Massachusetts Eye and Ear Infirmary, the
patient had periorbital erythema and edema surrounding the right
eye (Panel A) and conjunctival injection and chemosis (Panel B).
Photographs are courtesy of Dr. John B. Miller.
A
B
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 20142022
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
likely to be the sole cause of this patients ill-ness, because
her condition worsened despite treatment with erythromycin. That
she was suf-ficiently dehydrated to warrant admission may be an
early indication that her condition is more serious than a typical
pharyngitis.
Swelling of the Parotid Gland
During the 6-day period between the patients first and second
hospital evaluations, swelling of her face and trismus developed,
and the fevers persisted. She sought medical attention twice and
was treated with ibuprofen, systemic gluco-corticoids, and
narcotics before being again ad-mitted to the hospital. During this
period, there were several potential clues; perhaps the most
important was the development of swelling of the parotid gland. A
number of noninfectious causes may result in enlargement of the
parotid gland, including Sjgrens syndrome, which may be manifested
unilaterally but is not usually as-sociated with pain or fevers.
Heerfordts syn-drome is a variant of sarcoidosis that is
mani-fested by fevers and occasionally by facial-nerve palsy;
however, only a minority of patients pres-ent with painful swelling
of the parotid gland, and it is usually bilateral. Mumps is a cause
of infectious parotitis that has frequently been overlooked since
the introduction of the vaccine in 1967. Mumps causes unilateral
swelling of the parotid gland in 10% of cases and has resulted in
several outbreaks in North America, including an outbreak involving
teenagers who had re-ceived two doses of the vaccine.5 However,
mumps typically resolves within 10 days in the absence of
treatment, which is not consistent with the clinical deterioration
seen in this case.
Does this patient have a peritonsillar or retro-pharyngeal
abscess or Ludwigs angina? There are no typical findings, such as a
change in vo-cal quality, difficulty swallowing, or persistent
oropharyngeal pain, and CT did not reveal evi-dence of these
conditions. Therefore, these are unlikely causes of the patients
illness.
Given the patients pharyngitis, edema of the right side of the
face, and persistent fevers, I must consider the diagnosis of
Lemierres syndrome (i.e., the constellation of symptoms and signs
that arise in the weeks following a painful throat infection).
Diagnostic criteria include a history of anginal illness of the
oropharynx within the preceding 4 weeks, evidence of metastatic
le-
sions in the lungs or another remote site, and evidence of
internal-jugular-vein thrombophlebi-tis or isolation of
Fusobacterium necrophorum from the blood or another sterile
site.6
Does this patients illness meet the criteria for Lemierres
syndrome? A second MRI study shows inflammation of the muscles of
mastica-tion and lobulated abscesses in the parotid gland, as well
as a subperiostial abscess in the right orbit indicating metastatic
infection. The facial swelling and chemosis could be caused by
throm-bophlebitis in the carotid sheath and nearby vasculature.
Inflammation in the periorbital struc-tures, parotid gland, and
adjacent structures can result from extension of an infectious or
inflam-matory process of the lateral pharyngeal space (Fig. 3). In
addition, the patients age is consis-tent with this diagnosis,
because the median age at onset is 19 years.6 Approximately 6% of
patients have intracranial complications, which would also meet the
definition of distant (metastatic) infection.
The administration of antibiotic agents may have decreased the
likelihood of establishing a microbiologic diagnosis; however,
negative cul-tures increase the likelihood of the presence of an
organism such as fusobacterium, a fastidious anaerobe that may
require an incubation period of 5 to 8 days before detection.
Clindamycin and meropenem would both be expected to provide
adequate antibacterial coverage, but it is impor-tant to recognize
that the symptoms of Lemierres syndrome may progress despite
adequate antibi-otic therapy.
Deficit on Abduction of the Right Eye
How does a deficit on ocular abduction help to explain the
pathophysiology of the syndrome seen in this patient? To further
define this pro-cess, it is important to understand ocular
anat-omy, especially the structures along the pathway of the
abducens nerve, which controls ocular abduction. The abducens nerve
runs just lateral to the sphenoid, pierces the dura, and continues
forward between the dura and the apex of the petrous bone.7 The
nerve makes a sharp angle and enters the cavernous sinus before
piercing the orbit and the deep surface of the lateral rectus
muscle. In this case, there were no intraparen-chymal deficits
involving the pons or abducens nucleus on imaging. However, there
was dural enhancement, inflammation of the lateral rectus
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 2014 2023
Case Records of the Massachusetts Gener al Hospital
Figure 3. Anatomical Features of Laterally Invasive Pharyngeal
Infection.
The parapharyngeal space has an inverted triangular shape and is
bound medially by the pharyngeal wall, superiorly by the base of
the skull, laterally by the deep lobe of the parotid gland and
mandibular ramus, and inferiorly by the hyoid bone. The thick arrow
shows the likely route of infection from the site of initial
invasion to the carotid sheath. The thin arrows show the
interaction between lymphatic and vascular contents of the carotid
sheath and those of the orbital and facial structures. Either
hematogenous or lymphatic spread of fusobacterium is thought to
result in metastatic infection. Septic lymph may cause perivascular
inflammation and luminal thrombosis.
Parotid gland
Hyoid bone
Lymph node
Lateral rectus muscle
Abducens nerve
Base of skull (sphenoid bone)
Pharyngeal wall (route of initial invasion)
Mandibular ramus
Facial artery
Facial vein
Externaljugular vein
Posterior facial vein
Reflected sternocleidomastoid
muscle
Parapharyngeal space
Base of skull
Front view
Parotid gland
Mandible
Hyoid bone
Pharyngeal wall
Internaljugular vein
Vagus nerve
Internalcarotid artery
Deepcervical nodes
Commoncarotid artery
Carotid sheath
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 20142024
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
muscle, and possible cavernous-sinus involvement. Paralysis of
the lateral rectal muscle due to or-bital impingement, inflammation
of the muscle itself, or involvement of the peripheral abducens
nerve may have resulted in the deficit.
Sarcoidosis, myasthenia gravis, or the Miller Fischer syndrome
(a variant of the GuillainBarr syndrome) may cause a unilateral
deficit on ocu-lar abduction. However, in this patient, the
rap-idly progressive symptoms and associated fevers point toward
infectious causes. Mycobacterium tu-berculosis may cause
inflammation of the parotid gland, involvement of the basilar
meninges, and isolated abducens-nerve palsies. However, it is
highly unusual for M. tuberculosis infection to have such a
fulminant course, and this patient had no known exposure history.
Gradenigos syndrome, characterized by the triad of otorrhea,
retro-or-bital pain, and palsy of the lateral rectus muscle, is
caused by petrosal osteomyelitis associated with suppurative otitis
media and mastoiditis. In this case, however, Gradenigos syndrome
is an unlikely diagnosis, since the patient did not have a history
of auricular pain consistent with chron-ic otitis media, and the
imaging studies did not indicate mastoiditis or petrous
osteomyelitis.
A diagnosis of EBV mononucleosis alone is not consistent with
the fulminant and progres-sive disease course in this case;
however, it is important to note that serologic testing did
pro-vide evidence of recent primary EBV infection. The detection of
IgM antibodies to EBV-specific viral capsid antigen is virtually
diagnostic of primary infection,8 and the presence of IgG
an-tibodies to EBV-specific viral capsid antigen and to EBV nuclear
antigen indicates that the onset of infection occurred at least 3
weeks earlier. Although it is normal to find fusobacterium in the
oral cavity, the bacteria may become patho-genic after an
oropharyngeal infection.9 Approxi-mately 10% of cases of invasive
fusobacterium infection are preceded by EBV infection.10
Finally, it is necessary to rule out the diagno-sis of bulimia
nervosa in an 18-year-old woman with marked hypoalbuminemia,
radiographic findings suggestive of poor dentition, and
inflam-mation of the parotid gland. However, in patients with
bulimia nervosa, swelling of the parotid gland is normally painless
and bilateral, and den-tal findings usually include diffuse enamel
loss and caries. Furthermore, the serum albumin level is usually
normal in patients with eating disorders, even in those who are
severely mal-
nourished.11 Hypoalbuminemia is frequently a marker of critical
illness and has been described in patients with Lemierres
syndrome.
My leading diagnosis in this case is Lemierres syndrome due to
an invasive fusobacterium in-fection that developed shortly after
primary EBV mononucleosis. The diagnosis of Lemierres syn-drome can
be confirmed on the basis of either definitive evidence of
thrombophlebitis or a cul-ture growing fusobacterium.
Dr. Eric S. Rosenberg (Pathology): Dr. Sen and Dr. Freitag,
would you tell us your clinical impres-sions when you initially
evaluated this patient?
Dr. Pritha Sen (Infectious Diseases): On the basis of the
clinical history, physical examina-tion, and radiographic findings,
our impression was that this patient had an acute pharyngitis that
led to a suppurative infection of the parotid gland. Furthermore,
we thought that this infec-tion extended along the vasculature
originating in the parotid gland to the right inferotemporal dural
space and to the subperiosteal space of the superior lateral orbit,
causing abscess formation, and that an abscess in the subperiosteal
space of the right lateral orbit caused the cranial-nerve deficit.
Given the pharyngitis and evidence of infection involving the
parotid gland, lateral or-bit, and dura, we were concerned about
oral and odontogenic sources of infection of the head and deep
neck. Consequently, we chose to administer vancomycin, meropenem,
and clindamycin, anti-microbial agents directed against
gram-positive, oral gram-negative, and anaerobic organisms that can
penetrate the central nervous system. All cultures were sterile at
the time of our initial evaluation and there was no clear evidence
of thrombosis of the vasculature of the head and neck, but on the
basis of the patients presenta-tion, we suspected Lemierres
syndrome due to F. necrophorum. Our recommendations included
expedited ophthalmologic evaluation for surgi-cal drainage of the
right subperiosteal lateral orbital abscess and otolaryngologic
evaluation of the abscesses in the parotid gland. Given our concern
about Lemierres syndrome or a similar disorder, we also recommended
additional im-aging studies of the head and neck to evaluate the
patient for jugular-vein thrombosis and cav-ernous-sinus
thrombosis.
Dr. Suzanne K. Freitag: On initial consultation with the
ophthalmic plastic surgery service, we noted that the patients
right eye had decreased visual acuity, a deficit on abduction, and
perior-
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 2014 2025
Case Records of the Massachusetts Gener al Hospital
bital edema, erythema, and tenderness. Given these findings, in
conjunction with the findings on imaging studies and her worsening
clinical course, we made the decision to proceed with urgent
drainage of the orbital abscess. A supero-lateral orbitotomy was
performed through a crease of the right upper eyelid. The
subperios-teal dissection yielded a small amount of green purulent
material, which was cultured.
Clinic a l Di agnosis
Lemierres syndrome, complicated by an orbital abscess.
Dr . K r is ti a n R . Ol sons Di agnosis
Lemierres syndrome due to Fusobacterium nec-rophorum.
Pathol o gic a l Discussion
Dr. John A. Branda: The diagnostic procedures in-cluded
collection of specimens from several sites for routine aerobic and
anaerobic bacterial culture. F. necrophorum, a highly pleomorphic
gram-nega-tive rod, was isolated from the anaerobic compo-nent of
two blood cultures (two of four bottles), an aspirate of the
parotid-gland abscess, and a sample of the orbital fluid.
Monomicrobial in-fection with F. necrophorum is frequently seen in
patients with Lemierres syndrome.6
On the basis of the patients clinical presenta-tion and the
usual pathogenesis of Lemierres syndrome,12 it is likely that the
initial site of in-fection in this case was the pharynx. There is
evi-dence that EBV mononucleosis and group C strep-tococcal
pharyngitis are independent risk factors for the development of
pharyngeal F. necrophorum infection.6,12,13 Both a recent EBV
infection and a group C streptococcal infection were reported in
this patient, and it is possible that these infec-tions predisposed
her to the invasive F. necropho-rum infection that ultimately
developed.
Hospi ta l Cour se
Dr. Emily B. Rubin (Pediatrics): After the patient un-derwent
drainage of the subperiosteal abscess, she was admitted to the
pediatrics department of this hospital. On the night of admission,
she
had periorbital swelling of the left eye, increas-ing facial
pain, and worsening right lateral gaze palsy. Because of the rapid
development of these symptoms, we performed additional imaging
studies.
Dr. Johnson: CT angiography and venography were performed,
followed by MRI of the head, neck, and orbits, with and without the
adminis-tration of contrast material (Fig. 4). These stud-ies
revealed extensive thrombophlebitis of the right facial vein. There
was also extensive bilat-eral arteritis of the intracranial
internal carotid arteries, including a small mural thrombus in the
right cavernous carotid artery. Postoperative changes in the right
orbit and cavernous-sinus thrombophlebitis were also present. There
was persistent basilar and temporal meningitis on the right
side.
Dr. Rubin: Because of the severe narrowing of the carotid
arteries that was seen on these imag-ing studies, the patient was
transferred to the pediatric intensive care unit, where she
received anticoagulant and antiplatelet therapy. She had a good
response to the treatment. Repeat imaging of the head showed
several small infarcts dis-tributed in the right middle cerebral
artery, and it was unclear whether the cause of the infarcts was
embolic or ischemic. Despite these findings, the patient had no
neurologic deficits other than an inability to abduct her right
eye. She was transferred back to the pediatrics inpatient ser-vice
on day 9 and was discharged on day 15; medications at discharge
included vancomycin (intravenous), meropenem, low-molecular-weight
heparin (dalteparin sodium), and aspirin. Five days later, she was
readmitted with fever and a rash, which were thought to be caused
by the antibiotics, and she was transitioned to clindamy-cin. On
discharge from the hospital, she was taking warfarin. Imaging of
the head that was performed 3 months after her initial admission
showed an expected evolution of the infarcts of the right middle
cerebral artery and no sequelae of the carotid arteritis. The
warfarin was discon-tinued after 4 months.
Dr. John B. Miller (Ophthalmology): After the patient was
discharged, she was referred to the pediatric ophthalmology
department for man-agement of her diplopia associated with
persis-tent palsy of the right sixth cranial nerve. After 7 weeks
and with minimal improvement, the decision was made to inject 5
units of botulinum
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 20142026
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
toxin in order to weaken the right medial rectus muscle.14 This
immediately improved her ocular alignment in primary gaze. Four
weeks later, she had full extraocular motility, and the diplopia
had resolved.
Fina l Di agnosis
Lemierres syndrome caused by Fusobacterium necrophorum, with
cavernous-sinus thrombophle-
bitis, carotid-artery thromboarteritis, and abscess-es of the
parotid gland and subperiosteal orbit.
Presented at the Medical Case Conference.Dr. Olson reports
receiving grant support through his institution
from Vodafone Foundation and the Omidyar Network. No other
potential conflict of interest relevant to this article was
reported.
Disclosure forms provided by the authors are available with the
full text of this article at NEJM.org.
We thank Dr. Michael H. Lev (Radiology, Massachusetts Gen-eral
Hospital) and Dr. John B. Miller (Ophthalmology, Massa-chusetts Eye
and Ear Infirmary) for their contributions to this article.
Figure 4. Additional Imaging Studies of the Head and Neck.
CT angiography and venography of the head and neck, as well as
MRI of the head and neck (with and without the administration of
contrast material), performed on the current admission, revealed
findings suggestive of extensive thrombophlebitis of the right
facial vein, cavernoussinus thrombophlebitis, and bilateral
arteritis. A curved, multiplanar, reformatted image of the neck
shows extensive thrombophlebitis of the right facial vein (Panel A,
arrows). An axial T2weighted image shows hyperintense material in
the orifices of the facial vein (Panel B, arrow), a finding
consistent with thrombus. A coronal T1weighted, fatsaturated image
(obtained after the administration of contrast material) shows
bilateral cavernoussinus thrombophlebitis (Panel C, arrows) and
findings suggestive of basilar and temporal meningitis. An axial
T1weighted, fatsaturated image (obtained after the administration
of contrast material) shows evidence of bilateral arteritis,
including abnormal enhancement of the petrous internal carotid
arteries (Panel D, arrow). An axial image obtained at the level of
the right cavernous internal carotid artery shows evidence of
arteritis, as well as a focus of thrombus along the vessel wall
(Panel E, arrow). An axial image shows cavernoussinus
thrombophlebitis, which is greater on the right side than on the
left (Panel F, arrows).
A B C
E FD
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.
-
n engl j med 371;21 nejm.org November 20, 2014 2027
Case Records of the Massachusetts Gener al Hospital
References1. Alcaide ML, Bisno AL. Pharyngitis and epiglottitis.
Infect Dis Clin North Am 2007; 21: 449-69.2. Hurt C, Tammaro D.
Diagnostic eval-uation of mononucleosis-like illnesses. Am J Med
2007; 120(10): 911.e1-8.3. Hunt DP, Thabet A, Rosenberg ES. Case
Records of the Massachusetts Gen-eral Hospital (Case 29-2010). N
Engl J Med 2010; 363: 1266-74.4. Shah M, Centor RM, Jennings M.
Se-vere acute pharyngitis caused by group C streptococcus. J Gen
Intern Med 2007; 22: 272-4.5. Update: mumps outbreak New York and
New Jersey, June 2009January 2010. MMWR Morb Mortal Wkly Rep 2010;
59: 125-9.6. Riordan T. Human infection with Fu-
sobacterium necrophorum (Necrobacillo-sis), with a focus on
Lemierres syndrome. Clin Microbiol Rev 2007; 20: 622-59.7.
Wilson-Pauwels L, Akesson EJ, Stew-ard PA. Cranial nerves: anatomy
and clin-ical comments. Philadelphia: B.C. Decker, 1988.8.
Luzuriaga K, Sullivan JL. Infectious mononucleosis. N Engl J Med
2010; 362: 1993-2000.9. Smith GR, Wallace LM, Noakes DE.
Experimental observations on the patho-genesis of necrobacillosis.
Epidemiol In-fect 1990; 104: 73-8.10. Ramirez S, Hild TG, Rudolph
CN, et al. Increased diagnosis of Lemierre syn-drome and other
Fusobacterium necroph-orum infections at a Childrens Hospital.
Pediatrics 2003; 112(5): e380.
11. Winston AP. The clinical biochemis-try of anorexia nervosa.
Ann Clin Bio-chem 2012; 49: 132-43.12. Kuppalli K, Livorsi D,
Talati NJ, Os-born M. Lemierres syndrome due to Fu-sobacterium
necrophorum. Lancet Infect Dis 2012; 12: 808-15.13. Jensen A,
Hagelskjaer Kristensen L, Prag J. Detection of Fusobacterium
nec-rophorum subsp. funduliforme in tonsil-litis in young adults by
real-time PCR. Clin Microbiol Infect 2007; 13: 695-701.14. Scott
AB. Botulinum toxin injection of eye muscles to correct strabismus.
Trans Am Ophthalmol Soc 1981; 79: 734-70.Copyright 2014
Massachusetts Medical Society.
Lantern SLideS Updated: CompLete powerpoint SLide SetS from the
CLiniCopathoLogiCaL ConferenCeS
Any reader of the Journal who uses the Case Records of the
Massachusetts General Hospital as a teaching exercise or reference
material is now eligible to receive a complete set of PowerPoint
slides, including digital images, with identifying legends, shown
at the live Clinicopathological Conference (CPC) that is the basis
of the Case Record. This slide set contains all of the images from
the CPC, not only those published in the Journal. Radiographic,
neurologic, and cardiac studies, gross specimens, and
photomicrographs, as well as unpublished text slides, tables, and
diagrams, are included. Every year 40 sets are produced, averaging
50-60 slides per set. Each set is supplied on a compact disc and is
mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets
may be purchased for $50 each. Application forms for the current
subscription year, which began in January, may be obtained from the
Lantern Slides Service, Department of Pathology, Massachusetts
General Hospital, Boston, MA 02114 (telephone 617-726-2974) or
e-mail [email protected].
The New England Journal of Medicine Downloaded from nejm.org on
January 27, 2015. For personal use only. No other uses without
permission.
Copyright 2014 Massachusetts Medical Society. All rights
reserved.