Embed Size (px)
DESCRIPTION
bedah
Citation preview

lable at ScienceDirect
International Journal of Surgery 19 (2015) 61e66
Contents lists avai
International Journal of Surgery
journal homepage: www.journal-surgery.net
Original research
Laparoscopic assisted versus open gastric pull-up followingthoracoscopic esophagectomy: A cohort study
Hiroyuki Daiko*, Takeo FujitaDepartment of Surgery, National Cancer Center Hospital East, Chiba, Japan
h i g h l i g h t s
� This study evaluated a feasibility of laparoscopically assisted gastric pull-up (LAG) following thoracoscopic esophagectomy (TE).� LAG was compared with open laparotomy gastric pull-up (OLG) following TE.� No significant difference was found between two groups in the technical and oncological outcomes.� LAG following TE was feasible in patient with thoracic esophageal cancer.
a r t i c l e i n f o
Article history:Received 6 November 2013Received in revised form23 March 2015Accepted 9 April 2015Available online 15 May 2015
Keywords:Thoracoscopic surgeryLaparoscopic surgeryEsophageal cancer
* Corresponding author. Department of Surgery, NaEast, 6-5-1 Kashiwanoha, Kashiwa, Chiba 277-8577, J
E-mail address: [email protected] (H. Daiko)
http://dx.doi.org/10.1016/j.ijsu.2015.04.0401743-9191/© 2015 The Authors. Published by Elseviercreativecommons.org/licenses/by-nc-sa/4.0/).
a b s t r a c t
Background: Thoracolaparoscopic esophagectomy (TLE) is a type of minimally invasive esophagectomy(MIE) for esophageal cancer which consists of thoracoscopic resection and laparoscopic reconstruction.The aim of the present study was to evaluate the technical and oncological feasibility of alimentary tractreconstruction with laparoscopically assisted gastric pull-up (LAG) following thoracoscopic esoph-agectomy in the prone position (TSEP) in comparison with reconstruction with open laparotomy gastricpull-up (OLG) following TSEP, to establish TLE with extended lymph node dissection as a standardoperation for esophageal cancer.Methods: Sixty-four patients with esophageal cancer underwent TSEP with 3-field lymphadenectomyfrom 2008 through 2010: for reconstruction after TSEP, 31 patients underwent LAG, and 33 patientsunderwent OLG. We retrospectively evaluated the technical and oncological feasibility of TLE with 3-fieldlymphadenectomy and compared surgical outcomes after reconstruction with OLG and that with LAG.Results: TLE with 3-field lymphadenectomy was successfully completed in 30 of 31 (97%) patients, andno surgery-related postoperative deaths occurred. No significant difference was found between LAG andOLG in the mean number of dissected abdominal lymph nodes, amount of blood loss, incidence ofpostoperative complications, mean postoperative hospital stay, restoration rate of respiratory function, orrate of complete resection or locoregional control, but the mean duration of abdominal procedures wassignificantly longer with LAG than with OLG.Conclusion: This study demonstrates that the quality and safety of surgery and the oncological effec-tiveness of LAG for esophageal cancer. TLE consisting of LAG following TSEP with extended lymph-nodedissection is a feasible surgical technique for thoracic esophageal carcinoma.© 2015 The Authors. Published by Elsevier Ltd on behalf of IJS Publishing Group Limited. This is an open
access article under the CC BY-NC-SA license (http://creativecommons.org/licenses/by-nc-sa/4.0/).
1. Introduction
Surgical resection is the standard treatment for carcinoma of thethoracic esophagus. However, the procedure is a complex; involvesthe cervical, thoracic, and abdominal fields; and includes
tional Cancer Center Hospitalapan..
Ltd on behalf of IJS Publishing Gr
thoracotomy or laparotomy or both. Accordingly, resection of car-cinomas of the thoracic esophagus can be associated with signifi-cant morbidity and mortality and a delay in return to preoperativeactivity levels. Thoracolaparoscopic esophagectomy (TLE) is a typeof minimally invasive esophagectomy (MIE) for esophageal cancerwhich comprises both thoracoscopic resection and laparoscopicreconstruction. Such an MIE can produce less morbidity than openoperations and allows a quicker return to normal function [1]. Wehave assessed the technical and oncological feasibility of
oup Limited. This is an open access article under the CC BY-NC-SA license (http://

H. Daiko, T. Fujita / International Journal of Surgery 19 (2015) 61e6662
thoracoscopic resection and thoracoscopic esophagectomy in theprone position (TSEP) in comparisonwith open thoracotomy for thetreatment of carcinoma of the esophagus [2].
Regardless of tumor location, nodal metastasis is often wide-spread in the 3 operative fields. In one series, the rates of abdominallymph-node metastasis from tumors in the upper, middle, andlower thirds of the thorax were 10%, 74%, and 40%, respectively [3].Both the open and laparoscopic approaches are associated with asignificant incidence of reconstruction-related complications.Anastomotic leakage is a leading cause of operative mortality andremains responsible for approximately one-third of operativedeaths [4]. For these reasons, the method of alimentary tractreconstruction is of particular importance in determining periop-erative outcomes and the oncological completeness of resection.However, the laparoscopic approach for reconstruction andabdominal lymph-node dissection has not, to our knowledge, beenreported, and its technical and oncological feasibility has not beenevaluated in comparison with open laparotomy.
The aim of the present study was to evaluate the technical andoncological feasibility of alimentary tract reconstruction with lap-aroscopically assisted gastric pull-up (LAG) following TSEP incomparison with open laparotomy gastric pull-up (OLG) followingTSEP, to establish TLE with extended lymph node dissection as astandard operation for esophageal cancer.
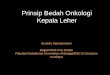
Fig. 1. Port placement and skin incisions. Filled circle, Filled circle: 5-mm port; filledsquare: 12-mm port. Dotted line is additional minilaparotomy 3e4 cm in diameter.
2. Materials and methods
2.1. Patients population
Since September 2008, previously untreated clinical stage Iesophageal cancer has been treated with TSEP and 3-field lymph-node dissection at the National Cancer Center Hospital East. Wehave previously reported the oncological feasibility of TSEP with3-field lymph node dissection for clinical stage I esophagealcancer [2]. Since April 2010, the indications for TSEP with 3-fieldlymph node dissection have been expanded to include clinicalstages T1 to T3 without metastasis to thoracic lymph nodes, andreconstruction with LAG after esophagectomy has been per-formed for patients without metastasis to abdominal lymphnodes. From September 2008 through June 2011, TSEP with 3-field lymph node dissection was performed for 64 patients: 33of these patients underwent gastric reconstruction with OLG viathe posterior mediastinal route, and 31 patients without metas-tasis to abdominal lymph nodes underwent LAG via the retro-mediastinal route.
All patients were evaluated and underwent disease staging withpreoperative computed tomographic scans of the neck, chest, andabdomen; barium swallow examination; endoscopy with biopsy;and ultrasonography of the neck. Endoscopic ultrasonography wasperformed to confirm the presence of submucosal cancer, when thetumor was suspected to not be restricted to themucosa. Indicationsfor definitive operationwith extended lymph-node dissectionweresubmucosal cancer and mucosal cancer with circumferentialspread, for which endoscopic mucosal resection is not indicated.
Comprehensive evaluations of cardiac and respiratory functionsshowed that all patients could tolerate anesthesia and operation.Before surgery and just before discharge after surgery, respiratoryfunction was assessed with spirometry, including determinationsof vital capacity (VC), percent predicted vital capacity (%VC), forcedvital capacity (FVC), forced expiratory volume in 1 s (FEV1.0), andFEV1.0 as a percentage of FVC (FEV1.0%). Informed consent wasobtained from all patients. Clinical and pathological staging wasbased on the 1997 TNM classification of the International UnionAgainst Cancer.
2.2. Statistical analysis
Survival timewasmeasured from the date of surgery until deathor the most recent follow-up examination. Length of survival wasdetermined with the KaplaneMeier method, and the log-rank testwas used for comparisons. The x [2] test and Fisher's exact proba-bility test were used for comparing percentages. A p-value of lessthan 0.05 was considered to indicate significance. All analyses wereperformed with the IBM SPSS Statistics software package (IBMCorp., Armonk, NY).
2.3. Surgery
The operation consists of 3 stages, as previously described indetail [2]. Stage 1 involves the thoracic field and includes TSEP andthorascopic mediastinal lymph-node dissection through 4 or 5ports. Stage 2 involves the abdominal field and includes gastricmobilization and abdominal lymph-node dissection with openlaparotomy or the laparoscopic approach. Stage 3 involves thecervical field and includes anastomosis and cervical lymph-nodedissection.
2.4. Stage 1: thoracic stage (TSEP)
After intubation, the patient is placed in the prone position uponoperative beanbags with a blocking balloon in the right mainbronchus for single-lung ventilation.
The port positions are as follows (Fig. 1). Port I is 12-mm bluntport in the 4th intercostal space (ICS) on the posterior axillary line.Port II, placed under thoracoscopic guidance, is a 12-mm port in the5th ICS on the anterior axillary line. Port III is a 12-mm port in the3rd ICS on the midaxillary line. Port IV is a 5-mm port in the 8th or9th ICS on the midaxillary line to insert a camera for procedures ofthe middle-to-lower mediastinum. Port V is a 5-mm port in the 5thICS just under the angle of the scapula to insert a camera for pro-cedures of the upper mediastinum. Carbon dioxide is insufflated ata pressure of 8 mm Hg to expand the mediastinum.

Table 1Clinical and pathological characteristics of TSEP with 3-field lymph node dissectionaccording to method of gastric pull-up.
Total OLG LAG P Value
Number of Patients 64 33 31Sex 0.71male/female 56/8 28/5 28/3
Age, years 0.45Median (range) 66 (49e78) 65 (49e76) 66 (49e78)Location of tumors 0.01Upper thorax 7 7 0Middle thorax 23 14 9Lower thorax 34 12 22
Clinical T status 0.001cT1 45 30 15cT2 6 1 5cT3 13 2 11
Clinical N status 1.0cN0 60 31 29cN1 4 2 2
Clinical stage 0.002I 43 29 14IIA/IIB 16/3 2/1 14/2III 2 1 1
Pathological T status 0.002pT1 46 28 18pT2 7 4 3pT3 11 10
Pathological N status 0.035pN0 45 27 18pN1 19 6 13
Pathological stage 0.05I 37 24 13IIA/IIB 6/12 2/6 4/6III 6 0 6IVA 3 1 2
OLG: open laparotomy gastric pull-up.LAG: laparoscopically assisted gastric pull-up.
H. Daiko, T. Fujita / International Journal of Surgery 19 (2015) 61e66 63
2.5. Thoracoscopic mobilization of the middle-to-lower esophagus
The middle-to-lower esophagus is circumferentially mobilizedfrom the descending aorta, pericardium, and the left mediastinalpleura from below the arch of the azygos vein to the diaphragmatichiatus. Mobilization of the middle-to-lower esophagus was ach-ieved through en-bloc lymph-node dissection including the middlemediastinal nodes (subcarinal, bilateral main bronchial, and themiddle paraesophageal lymph nodes) and the lower mediastinalnodes (lower thoracic paraesophageal, posterior mediastinal, andsupradiaphragmatic lymph nodes).
2.6. Thoracoscopic mobilization of the upper esophagus
Mobilization of the upper esophagus was achieved through en-bloc lymph-node dissection including the upper mediastinal nodes(upper thoracic paraesophageal lymph nodes and thoracic para-tracheal lymph nodes, including the bilateral recurrent laryngealnerve nodes and infra-aortic arch nodes). Themost important pointfor lymph-node dissection around the recurrent laryngeal nerve isto keep the nerve under tension. The right recurrent laryngealnerve can be kept tense by taping the right vagus nerve with vesselloops. On the left side, retraction of the upper third of esophaguscreates tension on the left recurrent laryngeal nerve through itsesophageal branch. Moreover, retracting the esophagus leftwardand dorsally by pulling the tape extrathoracically and by retractingthe trachea rightward and ventrally provides better visualizationand clearance of the left recurrent laryngeal nerve and lymph nodesaround the nerve and simplifies lymph nodes dissection withoutinjuring the left recurrent laryngeal nerve.
2.7. Stage 2: abdominal stage; LAG
After the thoracic esophagus is mobilized with dissection oflymph nodes in the upper-to-lower mediastinum, the patient isplaced in the supine position and receives bilateral-lung ventila-tion. The port positions are as follows (Fig. 1). A 12-mm camerablunt port is created below the umbilicus, and carbon dioxide isinsufflated at a pressure of 12 mmHg to expand the abdomen. Fourother ports (two 12-mm ports and two 5-mm ports) are insertedunder laparoscopic guidance. Under laparoscopic guidance, thegastrocolic ligament is first divided along the border of the trans-verse colon using ultrasonic shears (Harmonic Scalpel; EthiconEndo-Surgery Inc., Cincinnati, OH, USA). The greater omentum iscompletely preserved because of the arcade of right and left gas-troepiploic veins and arteries. The entire greater omentum ismobilized from transverse colon until the inferior portion of thespleen, and the root of the left gastroepiploic vein and artery areisolated and sealed with ultrasonic shears. The division of thegreater omentum is continued toward the hilum of the spleen, andthe gastrosplenic ligament, including the short gastric vein andartery, is divided until the upper pole of the spleen by means ofultrasonic shears. The adipose tissue, including lymph nodes alongthe celiac artery and left gastric artery, is dissected, and the leftgastric vein and artery are exposed and divided with ultrasonicshears and clips. After the lesser omentum is sealed and resectedalong the liver edge up to the esophagogastric junction, theabdominal esophagus is mobilized, and the thoracic esophagusincluding the primary tumor is removed through the thoracic inlet.We also partially divide the left crus and anterior diaphragm toallow easy passage of the gastric specimen and tube through thehiatus and to prevent gastric outlet obstruction. After gastricmobilization has been achieved, a 3- to 4-cm minilaparotomy ismade by cranially extending the camera port below the umbilicus.Through this minilaparotomy, the mobilized stomach is pulled out
of the peritoneal cavity, and a gastric tube is created with a linearstapler.
2.8. Open laparotomy
An upper abdominal incision 30 cm in diameter is made fromxiphoid process to above the umbilicus. Gastric mobilization andlymph node dissection are performed as in LAG.
2.9. Stage 3: cervical stage
The procedures in the cervical field include anastomosis andcervical lymph-node dissection. The cervical lymph nodescomprise the supraclavicular and cervical paraesophageal lymphnodes. The alimentary tract was restored with reconstruction of thestomach through a mediastinal route in 64 patients. Anastomosesin all patients were performed in an end-to-end manner withGambee's method and hand-sewing at the neck.
3. Results
3.1. Clinical and pathological characteristics of TSEP with 3-fieldlymph node dissection according to method of gastric pull-up
Of the patients who underwent TSEP with 3-field lymph nodedissection, those who underwent LAG had more advanced disease,as indicated by clinical and pathological stages (Table 1), than didpatients who underwent OLG.

H. Daiko, T. Fujita / International Journal of Surgery 19 (2015) 61e6664
3.2. Surgical outcomes of TSEP with 3-field lymph node dissectionaccording to method of gastric pull-up
Conversion to an open thoracotomy procedurewas required in 3patients (5%); however, conversion to open laparotomy was notrequired. Eventually, microscopically complete resection (R0) waspossible in 32 of 33 (97%) patients undergoing TLE with 3-fieldlymph node dissection. The mean number of lymph nodes har-vested in the abdomen, the amount of blood loss in the abdomen,and the rate of complete resection (R0) did not differ significantlybetween patients undergoing OLG and those undergoing LAG.However, the total duration of all procedures, the duration of thethoracic phase, and the duration of the abdominal phase weregreater in patients undergoing LGA (Table 2).
3.3. Postoperative course and complications of TSEP with 3-fieldlymph node dissection according to method of gastric pull-up
The incidence of postoperative morbidity was 36% in patientsundergoing OLG and 32% in patients undergoing LAG. The rate ofcomplications did not differ significantly between the patientgroups. No in-hospital deaths occurred in either group (Table 3).
Table 2Surgical outcomes of TSEP with 3-field lymph node dissection according to method of g
Total O
Number of Patients 64 3Conversion to open procedure
to thoracotomy 3 2to laparotomy 0
Operation time (minutes)Mean (range)Total 409 (297e569) 3Thoracic phase 217 (123e325) 2Abdominal phase 161 (90e248) 1
Amount of blood loss (ml)Mean (range)Total 396 (28e4225) 4Thoracic phase 157 (5e4138) 2Abdominal phase 238 (1e1131) 2
Number of dissected lymph nodesMean (range)Total 57 (20e88) 5Thoracic phase 24 (6e44) 2Abdomen 15 (5e31) 1
Completeness of resectionR0 63 3R1 1 1
OLG: open laparotomy gastric pull-up.LAG: laparoscopic assisted gastric pull-up.
Table 3Postoperative course and complications of TSEP with 3-field lymph node dissection acco
Total
Number of Patients 64Deaths 0Morbidity: number of cases (%) 22 (34)Pneumonia 0Recurrent laryngeal nerve palsy 9 (14)Anastomotic leakage 10 (16)Surgical site infection 5 (9)Chylothorax 3 (5)
Postoperative hospital stay, daysMean (range) 20 (10e76)
OLG: open laparotomy gastric pull-up.LAG: laparoscopic assisted gastric pull-up.
3.4. Restoration rate of respiratory function between before andafter operation
The rate of restoration of spirometric variables (VC, %VC, FVC,FEV1.0 and FEV1.0%) to preoperative levels did not differ signifi-cantly between patients undergoing OLG and those undergoingLAG (Table 4).
3.5. Pattern of first failure of TSEP with 3-field lymph nodedissection according to method of gastric pull-up
Disease recurred in 3 of 33 patients who underwent OLG and in4 of 33 patients who underwent LAG. The rate of recurrence did notdiffer significantly between the patient groups. In particular,recurrence in the abdominal field was not detected in any patient(Table 5).
4. Discussion
Surgical therapy has traditionally been considered the optimaltreatment for esophageal cancer in terms of locoregional controland long-term survival [5]. In the treatment of esophageal cancer,
astric pull-up.
LG LAG P Value
3 31
1 1.00
90 (297e480) 429 (308e569) 0.00933 (147e325) 200 (123e256) 0.00631 (90e235) 194 (145e248) 0.0001
98 (28e4225) 286 (50e1183) 0.1350 (5e4138) 59 (8e263) 0.1549 (40e618) 227 (1e1131) 0.71
7 (26e88) 58 (20e85) 0.773 (7e39) 25 (6e44) 0.245 (5e31) 15 (5e29) 0.56
1.02 31
0
rding to method of gastric pull-up.
OLG LAG P Value
33 310 012 (36) 10 (32) 0.800 06 (18) 3 (10) 0.484 (12) 6 (19) 0.505 (15) 0 0.051 (3) 2 (6) 0.61
19 (13e51) 20 (10e76) 0.76

Table 4Restoration rate of respiratory function between before and after operation according to method of gastric pull-up.
Before OLG after Restoration rate Before LAG after Restoration rate P Value
VC (L) 3.3 ± 0.7 2.4 ± 0.7 72.3 ± 14.0 3.5 ± 0.6 2.6 ± 0.6 74.7 ± 11.0 0.51%VC 97.5 ± 17.4 71.0 ± 15.6 73.2 ± 14.5 110.9 ± 17.2 81.3 ± 16.1 73.5 ± 10.4 0.93FVC (L) 3.2 ± 0.7 2.3 ± 0.6 73.1 ± 14.5 3.5 ± 0.6 2.6 ± 0.6 73.3 ± 10.4 0.93FEV1.0 (L) 2.4 ± 0.6 1.8 ± 0.5 72.1 ± 14.2 2.7 ± 0.4 2.0 ± 0.5 72.4 ± 14.0 0.94FEV1.0% 77.0 ± 6.1 75.0 ± 15.4 97.3 ± 8.3 75.3 ± 9.0 77.0 ± 13.2 131.5 ± 172.0 0.37
OLG: open laparotomy gastric pull-up.LAG: laparoscopic assisted gastric pull-up.
Table 5Pattern of first failure of TSEP with 3-field lymph node dissection according tomethod of gastric pull-up.
Total OLG LAG P Value
Number of Patients 64 33 31Median follow-up time, days 601 784 412Pattern of recurrence: n 7 3 4 0.70Locoreginal 2 2 0Thorax 2 2 0Abdomen 0 0 0
Distant 4 0 4Both 1 1 0
OLG: open laparotomy gastric pull-up.LAG: laparoscopic assisted gastric pull-up.
H. Daiko, T. Fujita / International Journal of Surgery 19 (2015) 61e66 65
the trauma and invasiveness associated with esophagectomy aregreater than those of other surgical interventions. The significanttrauma associated with thoracotomy or laparotomy or both is a keydisadvantage and induces a pronounced systemic inflammatoryresponse [6]. The conventional open surgical procedure, whichincludes thoracotomy, laparotomy, or both, is associated with sig-nificant morbidity and mortality and a delay in return to the pre-operative level of activity [7,8]. Recently, a type of MIE foresophageal cancer including thoracoscopic procedures or laparo-scopic procedures or both has been performed and its surgicalbenefits have been assessed. Several studies of thoracoscopic MIEhave been performed. Several different techniques for thoraco-scopic MIE have been described and have been found to be equal toopen thoracotomy in terms of technical and oncological feasibility.Furthermore, thorascopic surgery has the advantages of shorterintensive care unit stays and hospital stays after surgery, a weakersystemic inflammatory response, less blood loss, and lower rates ofsurgical site infection, blood transfusion, and postoperative com-plications, especially pulmonary complications [9e20].
Two different surgical positions are used for procedures in thethoracic stage: the left lateral decubitus position and the proneposition. First described by Cuschieri and colleagues in 1994, TSEPhas attracted attention as a potentially less-invasive procedure [21].Recent reports on the use of TSEP have stimulated new interest in itand have described short-term perioperative outcomes[2,9,14,16,20,22,23]. Because of the effects of gravity with the pa-tient in the prone position, the esophagus is well-visualized,dissection is simpler because the esophagus falls anteriorly fromits normal position, the lungs and heart require no retraction, andblood pools outside the operative field [2,14,22]. Moreover, with thepatient in the prone position, neither a skilled assistant surgeon noran endoscopist is required [2]. The technical and oncologicalfeasibility of TSEP has been confirmed to be equal to that of openthoracotomy [2,9,14,16,20]. However, these reports demonstratingthe advantages of TSEP did not evaluate its technical and onco-logical feasibility for abdominal surgical procedures. Surgery foresophageal cancer consists of thoracic, abdominal, and cervicalphases, and an MIE for esophageal cancer is TLE, which consists ofthoracoscopic resection and laparoscopic reconstruction. Moreover,
the abdominal phase is of particular importance for the perioper-ative outcome and oncological completeness of resection.
In the present study, we have demonstrated the technical andoncological feasibility of LAG in comparison with conventionalopen abdominal procedures for esophageal cancer. We found nosignificant differences between LAG and OLG in the mean numberof dissected abdominal lymph nodes, volume of blood loss, inci-dence of postoperative complications, mean postoperative hospitalstay, restoration rate of respiratory function, or rate of completeresection or locoregional control, but the mean duration ofabdominal procedurewas significantly longer for LAG than for OLG.
Pulmonary function is suppressed after abdominal surgerybecause of diaphragmatic dysfunction and postoperative pain.Several randomized trials have demonstrated that FVC and FEV1.0value are suppressed less after laparoscopic cholecystectomy thanafter open procedures [24e26]. However, Kitano et al. have re-ported that the suppression of FVC differs significantly betweenlaparoscopically assisted distal gastrectomy and open distal gas-trectomy but that the suppression of FEV1.0 does not [27]. More-over, Stage et al. have found no significant difference in pulmonaryfunction between a laparoscopic colectomy and open colectomy[28]. Whether laparoscopic surgery or open surgery causes greatersuppression of pulmonary function remains controversial. There-fore, a studywith a large number of cases is necessary to investigatethe effects of laparoscopic surgery and open surgery on pulmonaryfunction.
A previous study has demonstrated the safety and oncologicalfeasibility of throacoscopic MIE but did not assess the technical andoncological feasibility of LAG compared with conventional openabdominal procedures for esophageal cancer [2]. The presentreport is, to our knowledge, the first to demonstrate the technicaland oncological feasibility of alimentary tract reconstruction withLAG following TSEP and extended lymph-node dissection foresophageal cancer. The safety and oncological effectiveness ofreconstruction with LAG following TSEP are comparable to those ofreconstruction with OLG. For these reasons, we believe TLE con-sisting of TSEP followed by LAG has the potential to become astandard surgical treatment and the ultimate minimally invasivesurgery for esophageal cancer.
This study demonstrates that the quality and safety of surgeryand the oncological effectiveness of LAG for esophageal cancer. Weconclude that TLE, consisting of TSEP followed by LAG withextended lymph node dissection, is a feasible surgical technique forthoracic esophageal carcinoma.
Conflict of interest
None.
References
[1] J.D. Luketich, M. Alvelo-Rivera, P.O. Buenaventura, N.A. Christie,J.S. McCaughan, V.R. Litle, et al., Minimally invasive esophagectomy: outcomesin 222 patients, Ann. Surg. 238 (2003) 486e494 discussion 94e5.

H. Daiko, T. Fujita / International Journal of Surgery 19 (2015) 61e6666
[2] H. Daiko, M. Nishimura, A pilot study of the technical and oncologic feasibilityof thoracoscopic esophagectomy with extended lymph node dissection in theprone position for clinical stage I thoracic esophageal carcinoma, Surg. Endosc.26 (2012) 673e680.
[3] H. Akiyama, M. Tsurumaru, H. Udagawa, Y. Kajiyama, Radical lymph nodedissection for cancer of the thoracic esophagus, Ann. Surg. 220 (1994)364e372 discussion 72e3.
[4] J.D. Urschel, Esophagogastric anastomotic leaks: the importance of gastricischemia and therapeutic applications of gastric conditioning, J. Invest. Surg.11 (1998) 245e250.
[5] C. Mariette, G. Piessen, J.P. Triboulet, Therapeutic strategies in oesophagealcarcinoma: role of surgery and other modalities, Lancet Oncol. 8 (2007)545e553.
[6] N. Ni Choileain, H.P. Redmond, Cell response to surgery, Arch. Surg. 141 (2006)1132e1140.
[7] M.B. Orringer, B. Marshall, M.D. Iannettoni, Transhiatal esophagectomy: clin-ical experience and refinements, Ann. Surg. 230 (1999) 392e400 discussion00e3.
[8] R. Rindani, C.J. Martin, M.R. Cox, Transhiatal versus Ivor-Lewis oesophagec-tomy: is there a difference? Aust. N. Z. J. Surg. 69 (1999) 187e194.
[9] U. Zingg, A. McQuinn, D. DiValentino, A.J. Esterman, J.R. Bessell,S.K. Thompson, et al., Minimally invasive versus open esophagectomy forpatients with esophageal cancer, Ann. Thorac. Surg. 87 (2009) 911e919.
[10] T.H. Pham, K.A. Perry, J.P. Dolan, P. Schipper, M. Sukumar, B.C. Sheppard, et al.,Comparison of perioperative outcomes after combined thoracoscopic-laparoscopic esophagectomy and open Ivor-Lewis esophagectomy, Am. J.Surg. 199 (2010) 594e598.
[11] S. Law, M. Fok, K.M. Chu, J. Wong, Thoracoscopic esophagectomy for esoph-ageal cancer, Surgery 122 (1997) 8e14.
[12] S. Taguchi, H. Osugi, M. Higashino, T. Tokuhara, N. Takada, M. Takemura, et al.,Comparison of three-field esophagectomy for esophageal cancer incorpo-rating open or thoracoscopic thoracotomy, Surg. Endosc. 17 (2003)1445e1450.
[13] T. Shiraishi, K. Kawahara, T. Shirakusa, S. Yamamoto, T. Maekawa, Risk anal-ysis in resection of thoracic esophageal cancer in the era of endoscopic sur-gery, Ann. Thorac. Surg. 81 (2006) 1083e1089.
[14] T. Fabian, J.T. Martin, A.A. McKelvey, J.A. Federico, Minimally invasiveesophagectomy: a teaching hospital's first year experience, Dis. Esophagus 21(2008) 220e225.
[15] R. Parameswaran, D. Veeramootoo, R. Krishnadas, M. Cooper, R. Berrisford,S. Wajed, Comparative experience of open and minimally invasive esoph-agogastric resection, World J. Surg. 33 (2009) 1868e1875.
[16] B.M. Smithers, D.C. Gotley, I. Martin, J.M. Thomas, Comparison of the out-comes between open and minimally invasive esophagectomy, Ann. Surg. 245
(2007) 232e240.[17] Y. Kinjo, N. Kurita, F. Nakamura, H. Okabe, E. Tanaka, Y. Kataoka, et al.,
Effectiveness of combined thoracoscopic-laparoscopic esophagectomy: com-parison of postoperative complications and midterm oncological outcomes inpatients with esophageal cancer, Surg. Endosc. 26 (2012) 381e390.
[18] N.T. Nguyen, P. Roberts, D.M. Follette, R. Rivers, B.M. Wolfe, Thoracoscopic andlaparoscopic esophagectomy for benign and malignant disease: lessonslearned from 46 consecutive procedures, J. Am. Coll. Surg. 197 (2003)902e913.
[19] S. Sihag, C.D. Wright, J.C. Wain, H.A. Gaissert, M. Lanuti, J.S. Allan, et al.,Comparison of perioperative outcomes following open versus minimallyinvasive Ivor Lewis oesophagectomy at a single, high-volume centre, Eur. J.Cardiothorac. Surg. 42 (2012) 430e437.
[20] H. Tsujimoto, R. Takahata, S. Nomura, Y. Yaguchi, I. Kumano, Y. Matsumoto, etal., Video-assisted thoracoscopic surgery for esophageal cancer attenuatespostoperative systemic responses and pulmonary complications, Surgery 151(2012) 667e673.
[21] A. Cuschieri, Thoracoscopic subtotal oesophagectomy, Endosc. Surg. AlliedTechnol. 2 (1994) 21e25.
[22] C. Palanivelu, A. Prakash, R. Senthilkumar, P. Senthilnathan, R. Parthasarathi,P.S. Rajan, et al., Minimally invasive esophagectomy: thoracoscopic mobili-zation of the esophagus and mediastinal lymphadenectomy in prone posi-tioneexperience of 130 patients, J. Am. Coll. Surg. 203 (2006) 7e16.
[23] H. Noshiro, H. Iwasaki, K. Kobayashi, A. Uchiyama, Y. Miyasaka, T. Masatsugu,et al., Lymphadenectomy along the left recurrent laryngeal nerve by a mini-mally invasive esophagectomy in the prone position for thoracic esophagealcancer, Surg. Endosc. 24 (2010) 2965e2973.
[24] P.R. Schauer, J. Luna, A.A. Ghiatas, M.E. Glen, J.M. Warren, K.R. Sirinek, Pul-monary function after laparoscopic cholecystectomy, Surgery 114 (1993)389e397 discussion 97e9.
[25] A.J. McMahon, J.N. Baxter, G. Kenny, P.J. O'Dwyer, Ventilatory and blood gaschanges during laparoscopic and open cholecystectomy, Br. J. Surg. 80 (1993)1252e1254.
[26] R.C. Frazee, J.W. Roberts, G.C. Okeson, R.E. Symmonds, S.K. Snyder,J.C. Hendricks, et al., Open versus laparoscopic cholecystectomy. A comparisonof postoperative pulmonary function, Ann. Surg. 213 (1991) 651e653 dis-cussion 53e4.
[27] S. Kitano, N. Shiraishi, K. Fujii, K. Yasuda, M. Inomata, Y. Adachi, A randomizedcontrolled trial comparing open vs laparoscopy-assisted distal gastrectomyfor the treatment of early gastric cancer: an interim report, Surgery 131(2002) S306eS311.
[28] J.G. Stage, S. Schulze, P. Moller, H. Overgaard, M. Andersen, V.B. Rebsdorf-Pedersen, et al., Prospective randomized study of laparoscopic versus opencolonic resection for adenocarcinoma, Br. J. Surg. 84 (1997) 391e396.