Embed Size (px)
Citation preview

June Litmer, MS, CNS-BCSuzanne Brooks, MS, CNS-BC Teresa Ditmer, MS, CNS-BC
Sycamore Pain ManagementKettering Physician Network
1

Conflict of Interest
2

Objectives
Describe the pathophysiology of pain Discuss the concept of multimodal pain
management Identify indications for regional and
neuraxial analgesia
June Litmer, MS, [email protected]
3

Why do We Care About Pain? 1990s- Pain Became the 5th Vital Sign Effects of Uncontrolled Pain
Hypoventilation Increased myocardial stress Suppression of immune system
Focus became pain assessment and treatment with opioids.
Concept of pre-emptive, multimodal analgesia started to develop.
4
2000’s The Hospital Consumer Assessment of Healthcare
Providers and Systems survey (HCAHPS) started as the first national survey of patients' perspectives
The Score on questions related to Pain management is shown as a percentage of patients who reported that their pain was "Always" well controlled & hospital staff “did everything they could to help”
(CMS.gov)
5

Today Affordable Care Act of 2010 uses HCAHPS
scores to calculate payments to hospitals.
There is an estimated 76.5 million Americans (26%) with chronic pain, which makes this even more challenging. (American Pain Foundation, 2009)
Opioid-related adverse drug reactions following surgery – associated with significantly increased LOS and cost (Oderda, G. M. et al. 2007)
6

Pathophysiology of Pain Nociceptors
Nerve endings in the peripheral nervous system, muscle, fascia, blood vessels, joints, viscera, and dura
Receptors for painful stimuli A fibers- evoke sharp & aching pain
Fast pain
C fibers- evoke burning pain Slow pain that may be long-lasting
• (American Society of Pain Management Nurses Core Curriculum, 2012)
7

Activation of Nociceptors Pain is activated with injury.
Exchange of Na and K ions occurs at the cell membranes causing release of chemical messengers: Norepinephrine Epinephrine Substance P Glutamate Bradykinin Histamine Hydrogen ions Prostaglandins from the break down of
arachidonic acid by Cyclooxygenase (COX) Interleukins Tumor Necrosis Factor Serotonin (stimulates pain peripherally)
(Agitation and Pain in the Recovery Room February 6, 2012)8

Transduction:
Activation of nociceptors causes conversion of stimulus to electrical impulse
Na and Ca channels open causing depolarization of the nerve endings and release of the electrical signal.
Primary afferent fibers are stimulated and signal is carried to CNS
(Agitation and Pain in the Recovery Room February 6, 2012)
9

Transmission Pain is transmitted to dorsal horn
of spinal cord From the dorsal horn,
spinothalamic tracts carry signal up to the brain
Impulses reach thalmus & midbrain
(Agitation and Pain in the Recovery Room February 6, 2012) 10

Perception Pain perception occurs as the
nociceptive message is transmitted to the somatosensory cortex, parietal lobe, frontal lobe and limbic system
Stimulation of the limbic system produces the emotional reaction to pain
Hypothalma-pituitary-adrenal axis is stimulated & catecholamines are released- induce anxiety
Repeated stimulation of spinal cord causes the pain to intensify
(American Society of Pain Management Nurses Core Curriculum, 2012)
11

Modulation Body’s attempt to decrease pain When primary afferent fibers terminate in dorsal
horn, there is a release of neurotransmitters to block pain impulses: Gamma-aminobutyric acid (GABA) Neurotensin Acetylcholine Oxytocin Endogenous opioids
(American Society of Pain Management Nurses Core Curriculum, 2012)
12

Modulation Opioid Receptors - located in the dorsal horn at the end of
the afferent pain fibers- endogenous opioids binds to these to block painful stimulus Μ (mu) Κ (kappa) Δ (delta)
Midbrain activation causes fibers to modulate pain through descending pathway activation: Serotonin & Norepinephirine released & binds to the neurons
of descending analgesic tract When reuptake of norepinephrine and serotonin is inhibited, the
descending analgesic system is enhanced(American Society of Pain Management Nurses Core Curriculum, 2012)
13

Types of Pain Somatic – nociceptive activation of skin, SQ tissue,
bones, muscles and blood vessels Feels like sharp, aching, throbbing
Visceral- nociceptive activation of organs Feels like diffuse gnawing or cramping
Neuropathic- aberrant somatosensory processing in peripheral nervous system, can occur with injury or dysfunction of peripheral nervous system or CNS Feels like burning, shooting, stinging
(American Society of Pain Management Nurses Core Curriculum, 2012)
14

Chronic Pain- Central Sensitization
Can persist after acute injury is healed & peripheral input stops
Can expand beyond the site of the initial injury Increase excitability of neurons in the CNS
leading to abnormal sensing & spontaneous impulses
(American Society of Pain Management Nurses Core Curriculum, 2012)
15

• Multimodal pain management- Use of multiple agents that act at different regions of the pain pathway (Parvizi, J., Miller, A. G. , & Ganghi, K. 2011)
• Goal- Reduce doses of each medication, thereby reducing adverse effects
• NSAID’s, COX-2, & acetaminophen have an opioid dose sparing effect (American Society of Pain Management Nurses Core Curriculum, 2012, p. 257-258)
Multimodal Pain Management
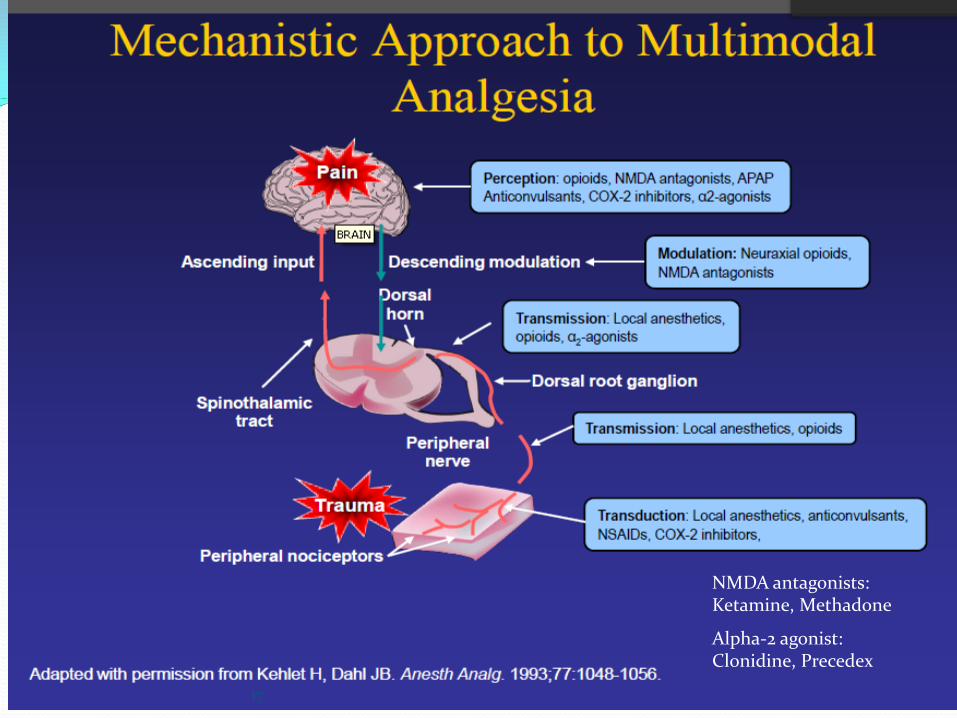
Alpha-2 agonist: Clonidine, Precedex
NMDA antagonists:Ketamine, Methadone
17
Anesthesiologists Task Force on Acute Pain Management
“The consultants and ASA members strongly agree that anesthesiologists who manage perioperative pain should use therapeutic options such as epidural or intrathecalopioids, systemic opioid PCA, and regional techniques after thoughtfully considering the risks and benefits for the individual patient.” (Anesthesiologists Task Force on Acute Pain Management, 2012
18

Spinal/Epidural Anesthesia Reduce deleterious
effects associated with general anesthesia
Meta-analysis demonstrated decreased mortality and morbidity after surgery
(Parvizi, J., Miller, A. G. , & Ganghi, K. 2011)
19

Epidural AnalgesiaIndications Advantages
Surgical Thoracotomy Total Joint Replacement AAA Resections Perineal Resections Major urology cases Amputations
Trauma Rib fractures
Chronic Pain Labor and C-Section
Improves Pain control GI function Peripheral circulation
Reduces Risk of postop MI Postop mortality Persistent pain syndrome
Meta-analysis demonstrated improved pain control, especially during early postop period (Parvizi, J., Miller, A. G. , & Ganghi, K. 2011)
(Sawhneym, M. August 2012) 20

Epidural Space Contains adipose tissue,
blood vessels, lymphatic vessels, and spinal nerves
The area of skin innervated by each spinal nerve is called a dermatome
The area of the body affected by the epidural infusion depends on where the tip of the epidural catheter is and what spinal nerves are affected.
(Sawhneym, M. August 2012)

Epidural Analgesia Epidural infusions usually combine local anesthetics
and opioids Local anesthetics bind to Na channels, block A-delta
and C nerve fibers to block pain transmission. Marcaine, Ropivacaine or Lidocaine are usually used.
Opioids given in the epidural space work by binding to opioid receptors in the dorsal horn of the spinal cord to block pain. Fentanyl is usually used because it is more lipophilic with a quicker onset but Dilaudid or Morphine can also be used.
(Sawhneym, M. August 2012)

Epidural AnalgesiaContraindications Adverse Effects
Anticoagulation Infection at site Systemic infection Increased ICP Coagulopathy Allergy to drugs Spinal deformity Neurological disorders Previous back surgery
(spinal fusion)
Pruritis Nausea & vomiting Urinary retention Decreased level of consciousness Respiratory depression Infection Headache Hematoma Sensory & motor deficits in dermatomes not
meant to be blocked Blocking sympathetic nerve fibers- bradycardia
& hypotension Blocking motor nerve fibers- muscle weakness
Local anesthetic toxicity can occur with vascular uptake Circumoral paresthesia, Tinnitus, distortion of
taste, irritability, tremor, seizures, & cardiac arrhythmias
(American Society of Anesthesiologists Task Force on Neuraxial Opioids 2009). 23

Nerve Blocks
Continuous or single-shot Continuous infusion provides superior
relief compared to single-shot Meta-analysis demonstrated significant
improvement in patients receiving peripheral nerve block compared to opioid analgesia alone.
)24

Nerve BlocksLocal anesthetics
Interscalene Supraclavicular Brachial Plexus Block Infraclavicular Brachial Plexus Block Axillary Brachial Plexus Block Celiac Plexus Block Transversus abdominis plane block Femoral Sciatic Fascia iliaca Saphenous (Adductor canal) Popliteal sciatic block Lumbar sympathetic block
(http://www.neuraxiom.com/)25

• Initial signs Severe drowsiness Light headedness Dizziness Anxiety Peri-oral numbness Metallic taste Blurred vision Tinnitus Disorientation
• Higher Dose Signs Initial CNS excitation followed by
CNS depression Muscle twitching Convulsions Unconsciousness Coma Respiratory depression Cardiac arrythmias Cardiac arrest
Local Anesthetic Toxicity
Treatment: Intralipid 20% 500 ml IV

Bupivacaine Bupivacaine levels reach maximum drug
concentration in 30-45 min. after injection followed by a decline in the next 3-6 hours Cost: $4-$13/vial
Exparel - Liposomal bupivacaine is bupivacaine loaded in multivesicular liposomes to increase duration Cost: $359/vial
Delays the peak plasma concentration by slow release from the liposome over a period of 72 hours Hu, D. et al. (2013)

Exparel 4 studies have examined pharmacokinetics
n= 253 Plasma levels demonstrated an initial peak within 1 hour
then a 2nd peak at 12-36 hours Adverse reactions- nausea, pyrexia, constipation,
peripheral edema, hypotension & vomiting Absorption is dependent on total dose, route and
amount of vasculature at the site Unknown to what extent plasma levels translate to pain
control Hu, D. et al. (2013)

Exparel Efficacy based on 5 phase II & III clinical trials
Inguinal hernia- Phase II trials vs. bupivacaine time to first dose of rescue pain med- not significantly different than
bupivacaine, pain scores were not significantly different
Total knee vs. bupivacaine Phase II trial- Pain scores not significantly different 0-96 hours Phase III trial- Pain scores not significantly different 0-72 hours
Hemorrhoidectomy vs. bupivacaine Phase II trial- Pain scores 0-72 hours significantly less than bupivicaine Phase III trial- not significantly different 0-96 hours
Breast Augmentation vs. bupivacaine Phase II trial- Pain scores not significantly different 0-96 hours Phase III trial- Pain scores not significantly different 0-96 hours
Hemorrhoidectomy vs. Placebo Phase III - significant difference 0-72 hours Phase III - significant difference 0-24 hours
Owen, R. T. (2013)

Exparel 7 studies comparing liposomal bupivacaine to bupivacaine with
epinephrine 631 patients receiving liposomal bupivacaine 446 patients receiving bupivacaine with epinephrine Inguinal hernia repair, total knee, hemorrhoidectomy, and breast
augmentation No difference in % patients avoiding opioid rescue Time to rescue medication slightly longer in liposomal
bupivacaine (9.3 vs. 6.4 hours, p<.05) 6/17 arms- liposomal dose exceeded FDA max dose of 266 mg,
4/11 remaining favored liposomal bupivacaine for 24 & 72 hour cumulative pain scores in hernia repair & hemorrhoidectomy (Noviasky, J. et al. 2014)
30

IV ACETAMINOPHENOFIRMEV• FDA approved November 2010• Site of Action : CNS
• Inhibition of prostaglandin synthesis• Higher peak levels compared with oral administration
• Avoids first pass metabolism• Clinical effect within 15 minutes• Peak effect within 1 hour• Duration 4-6 hours• Cost: oral $3/bottle, IV $35/dose
31
Ofirmev IV acetaminophen vs morphine & placebo- renal colic patients
N=165 RCT in ER-comparing single dose paracetamol to morphine and placebo- reduction in pain scores at 30 minutes was 43mm for paracetamol (p=.005), 40 mm for morphine, & 27 for placebo (Bektas, F. et al. 2009)
IV vs PO acetaminophen- hip fx patients N=75 prospective comparative study - significant reduction
(p<.005) in mean total IV morphine with IV paracetamol (6.5 mg) compared to oral paracetamol (21.8 mg) (Tsang, K. S., Page, J. & Mackenney, P. 2013)
IV vs PO acetaminophen- ICU patients N=77 total rescue medication was 21 % lower in IV group
(p=0.016) (Peterson, 2005)
32
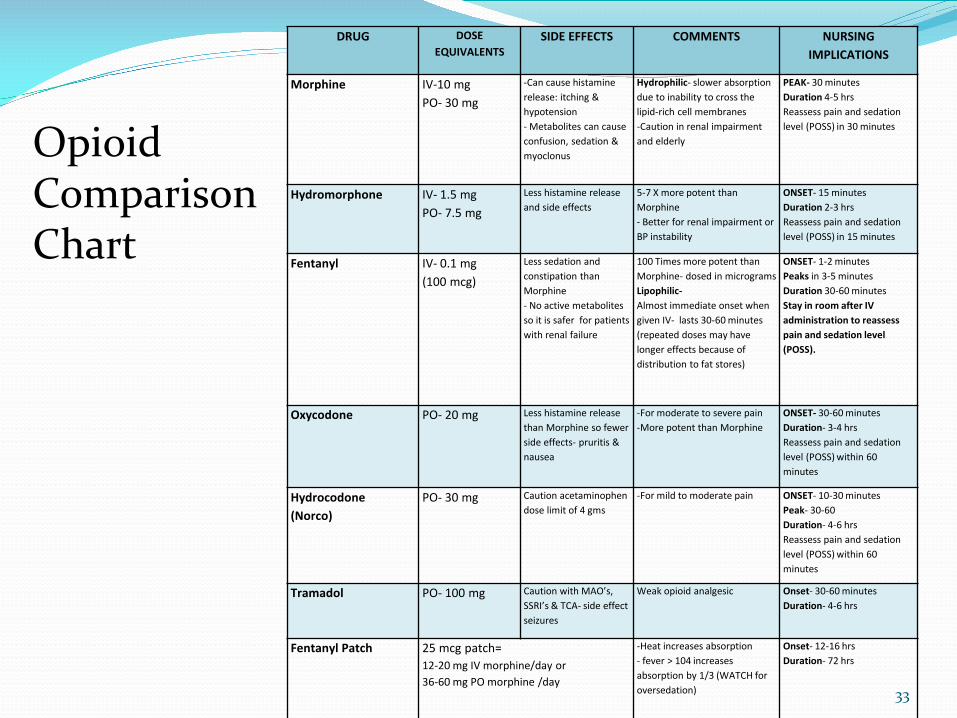
DRUG DOSE EQUIVALENTS
SIDE EFFECTS COMMENTS NURSING IMPLICATIONS
Morphine IV-10 mgPO- 30 mg
-Can cause histamine release: itching & hypotension - Metabolites can cause confusion, sedation & myoclonus
Hydrophilic- slower absorption due to inability to cross the lipid-rich cell membranes-Caution in renal impairment and elderly
PEAK- 30 minutesDuration 4-5 hrsReassess pain and sedation level (POSS) in 30 minutes
Hydromorphone IV- 1.5 mgPO- 7.5 mg
Less histamine release and side effects
5-7 X more potent than Morphine- Better for renal impairment or BP instability
ONSET- 15 minutesDuration 2-3 hrsReassess pain and sedation level (POSS) in 15 minutes
Fentanyl IV- 0.1 mg (100 mcg)
Less sedation and constipation than Morphine- No active metabolites so it is safer for patients with renal failure
100 Times more potent than Morphine- dosed in microgramsLipophilic-Almost immediate onset when given IV- lasts 30-60 minutes (repeated doses may have longer effects because of distribution to fat stores)
ONSET- 1-2 minutesPeaks in 3-5 minutesDuration 30-60 minutesStay in room after IV administration to reassess pain and sedation level (POSS).
Oxycodone PO- 20 mg Less histamine release than Morphine so fewer side effects- pruritis & nausea
-For moderate to severe pain-More potent than Morphine
ONSET- 30-60 minutesDuration- 3-4 hrsReassess pain and sedation level (POSS) within 60 minutes
Hydrocodone(Norco)
PO- 30 mg Caution acetaminophen dose limit of 4 gms
-For mild to moderate pain ONSET- 10-30 minutesPeak- 30-60Duration- 4-6 hrsReassess pain and sedation level (POSS) within 60 minutes
Tramadol PO- 100 mg Caution with MAO’s, SSRI’s & TCA- side effect seizures
Weak opioid analgesic Onset- 30-60 minutesDuration- 4-6 hrs
Fentanyl Patch 25 mcg patch= 12-20 mg IV morphine/day or 36-60 mg PO morphine /day
-Heat increases absorption- fever > 104 increases absorption by 1/3 (WATCH for oversedation)
Onset- 12-16 hrsDuration- 72 hrs
Opioid ComparisonChart
33
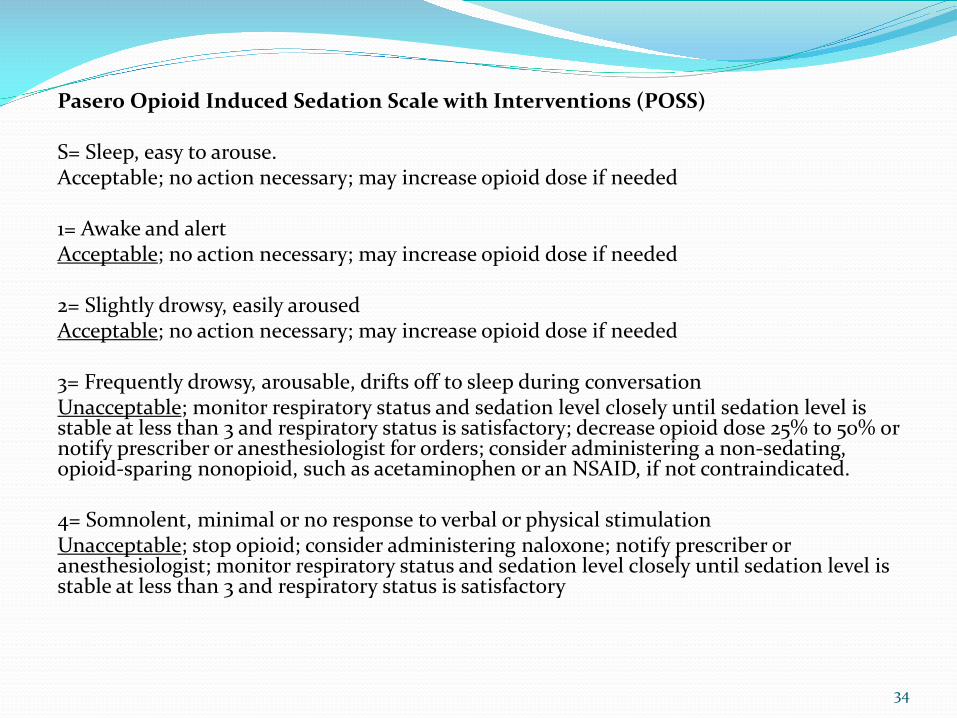
Pasero Opioid Induced Sedation Scale with Interventions (POSS)
S= Sleep, easy to arouse.Acceptable; no action necessary; may increase opioid dose if needed
1= Awake and alertAcceptable; no action necessary; may increase opioid dose if needed
2= Slightly drowsy, easily arousedAcceptable; no action necessary; may increase opioid dose if needed
3= Frequently drowsy, arousable, drifts off to sleep during conversationUnacceptable; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory; decrease opioid dose 25% to 50% or notify prescriber or anesthesiologist for orders; consider administering a non-sedating, opioid-sparing nonopioid, such as acetaminophen or an NSAID, if not contraindicated.
4= Somnolent, minimal or no response to verbal or physical stimulationUnacceptable; stop opioid; consider administering naloxone; notify prescriber or anesthesiologist; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory
34

CURRENT MULTIMODAL REGIMENFOR ORTHO SURGERY
PREOPERATIVE• Pregabalin• Celecoxib• Nerve Blocks
INTRAOPERATIVE• IV Acetaminophen (Ofirmev)• Opioids• NSAID• Exparel
PACU/Inpatient• Opiod• NSAID• Muscle Relaxants around the clock• Acetaminophen around the clock

References American Pain Foundation website (2009) American Society of Anesthesiologists Task Force on Neuraxial Opioids (2009). Practice
guidelines for the prevention, detection, and management of respiratory depression associated with neuraxial opioid administration. Anesthesiology, 110; 218-30
American Society of Anesthesiologists Task Force on Acute Pain Management, (2012). Practice Guidelines for Acute Pain Management in the Perioperative Setting. Anesthesiology, V 116, No 2. p248-273.
American Society of Pain Management Nurses Core Curriculum, 2012 Bektas, et al. (2009). Intravenous Paracetamol or Morphine for the treatment of renal colic: a
randomized, placebo-controlled trial. Annals of Emergency Medicine, Vol 54, No 4, p568-574. CMS.gov (2013) Hu, D. D., Onel, E., Singla, N., Kramer, W. G., Hadzic, A. (2013). Pharmacokinetic profile of
liposomal bupivacaine injection following a single administration at the surgical site. Clinical Drug Investigation, 33; 109-115.
Institute of Medicine (2010). Maund, E., McDaid, C., Rice, S., Wright, K., Jenkins, B., & Woolacott, N. (2011). Paracetamol
and selective and non-selective non-steroidal anti-inflammatory drugs for the reduction in morphine-related side-effects after major surgery: A systematic review. British Journal of Anaesthesia, 106(3), 292-7.
36
References Neligan, P. (February 6, 2012). Agitation and Pain in the Recovery Room Posted
http://anaesthesiawest .com/2012/02/06/agitation-and-pain-in-the-recovery-room-tutorial, retrieved Dec. 12, 2013
Neuraxiom, http://www.neuraxiom.com, retrieved September 7, 2014. Noviasky, J., Pierce, D. P., Whalen, K., Guharoy, R., Kildreth, K. (2014). Bupivacaine liposomal versus
bupivacaine comparative review. Hosp Pharm, 4996); 539-543. Odera, G. M. et al. (2007). Opioid related adverse drug events in surgical hospitalizations: impact on
costs and length of stay. Pharmacoeconomics, Volume 41. Owen, R. T., (2013). Bupivacaine liposome injectable suspension: a new approach to postsurgical pain.
Drugs of Today, 49 (8); 475-482. Parvizi, J., Miller, A. G. , & Ganghi, K. (2011). Multimodal pain management after total joint
arthroplasty. J bone Joint Surgery Am, 2011; 93:1075-84. Pettersson, P. H., Jakobsson, J., Owall, A. (2005). Intravenous acetaminophen reduced the use of
opioids compared with oral administration after coronary artery bypass grafting. J Cardiothor VascAnesth, 19: 306-309.
Sawhneym, M. (August 2012). Epidural analgesia, what nurses need to know. Nursing 2012, www.Nursing 2012.com.
Tsang, K. S., Page, J., Mackenney, P. (2013). Can intravenous Paracetamol reduce opioid use in preoperative hip fracture patients? Orthopedics, Vol 36, No 2 supplement, p.20-24.
37