Embed Size (px)
Citation preview

Case Conference
June 22, 2009Rivera, Rivere, Robosa, Rodas, Rodriguez, Rogelio, Roque, Ruanto, Sabalvaro
Section D Group 1
Patient Information
• J.D., 49 y/o, Male • Married • Filipino, Roman Catholic • Jeepney driver

Chief Complaint
ABDOMINAL PAIN

History of Present Illness
ADMISSION

Past Medical History
• No hypertension, diabetes, or asthma
• No previous surgeries or transfusions

Family History
(‐) asthma, DM, hypertension

Personal and Social History
• Smoker, 40 pack years • Occasional alcoholic beverage
drinker • Diet: mixed • Denies illicit drug use

Review of Systems • No fever, no weight loss, no weakness, no anorexia • No rashes, no increased pigmentation • No visual dysfunction, no redness, no itchiness, no eye
pain, excessive lacrimation • No deafness, no tinnitus, no aural discharge • No epistaxis, no nasal discharge • No gum bleeding, no throat soreness • No dyspnea, no shortness of breath, no chest pain, no
palpitations • No diarrhea, no constipation, no nausea, no vomiting, no
heartburn, (+) melena • No dysuria, hematuria, incontinence • No limitation of movements, joint pains and swelling of
joints • No heat or cold intolerance, no polyphagia, polydipsia,
polyuria • No convulsions, no headache, no sleep disturbances

Physical Exam
• General – conscious, coherent, not in
cardiorespiratory distress • Vital Signs: – BP: 140/90 mmHg – PR = 90 bpm, regular – RR = 22 cpm – T = 37.6 C • Skin – Warm, moist – no active dermatoses

Physical Exam
• HEENT – pink palpebral conjunctivae, anicteric scelrae, no
nasoaural discharge, moist buccal mucosa, tonsils not enlarged,
nonhyperemic posterior pharyngeal walls – Supple neck, no palpable cervical lymph nodes, thyroid
not enlarged • Thorax – symmetric chest expansion, (‐) retractions, resonant on both lung fields, equal and clear breath sounds • Cardiovascular Adynamic precordium, AB 5th LICS MCL, apex S1>S2,
base S2>S1, (‐) murmurs

Physical Exam
• Abdomen – Flat, no scars or striae, NABS, tympanitic upon
percussion, Traube’s space not obliterated, (+) direct and
rebound tenderness in upper abdominal region with guarding
(‐)Rovsing’s sign, (‐) psoas sign • DRE: – no skin tags seen, tight sphincteric tone, smooth
rectal mucosa, (‐) palpated masses, (‐) pararectal
tenderness, brown stool on tactating finger

Physical Exam
• Extremities – Pulses were full and equal, no cyanosis, no edema, no limitation of movement in all extremities were noted. • Neurological Examination – Conscious, coherent, oriented to 3 spheres – Cranial nerves: pupils 2‐3 mm ERTL, EOMs full and equal, V1V2V3 intact, can clench teeth, can raise eyebrows, can close eyes tightly, can smile, can frown, can puff cheeks,
no facial asymmetry, no hearing loss, can turn head from side to side with resistance, can shrug shoulders, tongue midline on protrusion.

Physical Exam
• Neurologic Exam – Motor: MMT of 5/5 on all
extremities – Cerebellar: can do FTNT & APST – DTR’s: ++ on all extremities – No sensory deficit – (‐) Babinski – (‐) nuchal rigidity

Salient Features
49 y/o, Male, jeepney driver (+) melena Generalized, persistent, severe, non-
radiating epigastric pain, 9/10 (+) direct and rebound tenderness in
upper abdominal region with guarding – BP: 140/90 mmHg – RR = 22 cpm Smoker, 40 pack years

Assessment
ACUTE ABDOMEN SECONDARY TO
PERFORATED VISCUS SECONDARY TO
PUD

Differential Diagnosis

PUD
Gastric ulcer Duodenal ulcer Erosive gastritis Zollinger- Ellison Syndrome Gastrointestinal tumors
Gastric ulcer
Majority of GUs can be attributed to either H. pylori infection or NSAID induced mucosal damage
Type I - located near the angularis incisura on the lesser curvature, close to the border between the antrum and the body of the stomach. These patients usually have normal or decreased acid secretion.

Gastric ulcer
Type II - associated with active or quiescent duodenal ulcer disease
Type III - prepyloric Type IV- near the gastroesophageal
junction, and acid secretion is normal or below normal
Type V- any location, associated with NSAID use

Duodenal ulcer
Acid secretory abnormalities that is also caused by H. pylori infection
Bicarbonate secretion is significantly reduced in patients with DU
Role of NSAIDS in inducing mucosal damage

Erosive gastritis
caused by many factors, including infection, injury, certain drugs, and disorders of the immune system.
involves both inflammation and wearing away of the stomach lining.
results from irritants such as drugs, especially aspirin and other nonsteroidal anti-inflammatory drugs
Painless upper GI bleeding in ICU setting

Zollinger- Ellison Syndrome
increased levels of the hormone gastrin are produced, causing the stomach to produce excess hydrochloric acid
a tumor (gastrinoma) of the duodenum or pancreas producing the hormone gastrin. Gastrin then causes an excessive production of acid which can lead to peptic ulcers in almost 95% of patients.

Gastrointestinal tumors
one of the most common mesenchymal tumors of the gastrointestinal tract
Patients present with trouble swallowing, gastrointestinal hemorrhage or metastases

Pathogenesis

Pathophysiology
H. pylori and NSAID induced injury account for the majority of DUs and GUs.
Caused by mild gastric acid hypersecretion resulting from (1) increased release of gastrin due to the
stimulation of a. antral G cells by cytokines released by inflammatory cells b. diminished production of somatostatin by D cells, both resulting from H. pylori infection
(2) an exaggerated acid response to gastrin due to an increased parietal cell mass resulting from gastrin stimulation

H. pylori and Ulcer Formation H. pylori infection is virtually always
associated with a chronic active gastritis The particular end result of H. Pylori
infection is determined by a complex interplay between bacterial and host factors

H. pylori and Ulcer Formation

Bacterial Factors
HP is able to facilitate gastric residence, induce mucosal injury, and avoid host defense
Urease allows the bacteria to reside in the acidic stomach and generates NH3 which can damage epithelial cells
produce surface factors that are chemotactic for neutrophils and monocytes which further contribute to injury
Proteases and phospholipases break down the glycoprotein lipid complex of the mucus gel and reduces the efficacy of the first line of mucosal defense
Adhesins are expressed to facilitate attachment

Host Factors
Inflammatory response to H. pylori includes recruitment of neutrophils, lymphocytes (T and B), macrophages, and plasma cells
Pathogens lead to injury by binding to class II MHC molecules expressed in gastric epithelial cells, leading to apoptosis
Elevated concentrations of multiple cytokines contribute to the mucosal and systemic humoral response that further compounds cell injury

Summary of potential mechanisms by which H. pylori may lead to gastric secretory abnormalities.

NSAIDs Induced Ulcer Formation
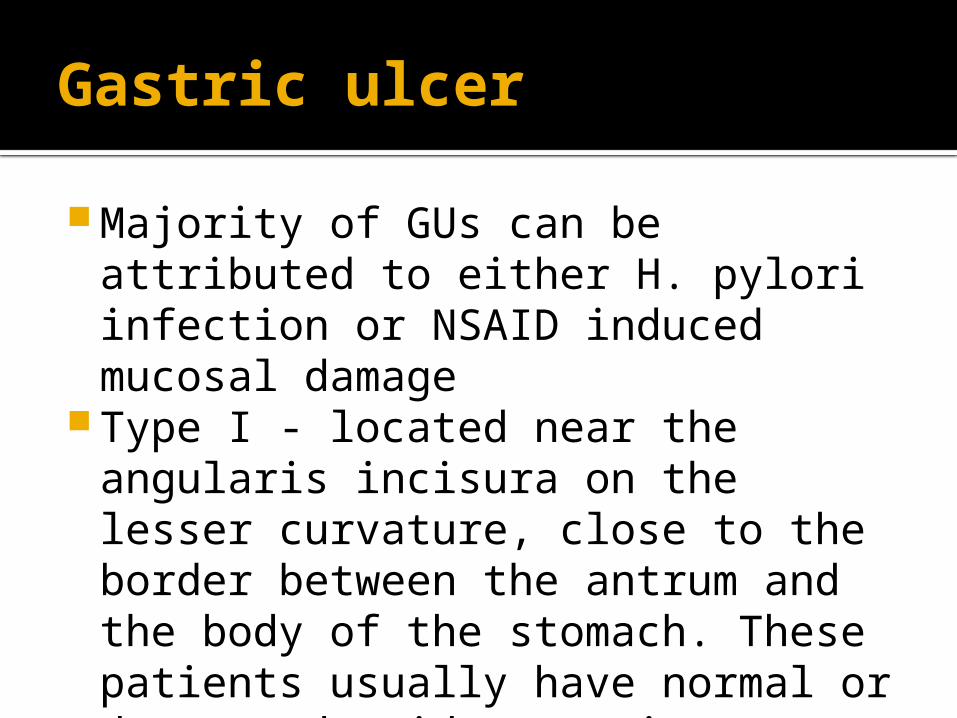
PGs play a critical role in maintaining gastroduodenal mucosal integrity and repair
Interruption of PG synthesis can impair mucosal defense and repair, thus facilitating mucosal injury
Mechanisms by which NSAIDs may induce mucosal injury.

Risk Factors
Smoking Decreases both gastroduodenal
prostaglandin production and pancreaticoduodenal bicarbonate production
Impairs blood flow and healing Alcoholism
Not been proved to directly cause peptic ulceration, but alcoholic cirrhosis is associated with an increased incidence of peptic ulcers

Symptomatology

Abdominal Pain
Gnawing characteristically peptic ulcer disease
Epigastric pain Location of duodenum
Acid-induced activation of chemical receptors in the duodenum
Enhanced duodenal sensitivity to bile acids and pepsin
Altered gastroduodenal motility

Relieved by Antacids
Final common pathway to ulcer formation is peptic acid injury of the gastroduodenal mucosal barrier

Aggravated by heavy meal intake
Classically associated with gastric ulcers
Possibly due to increased acid secretion during digestion
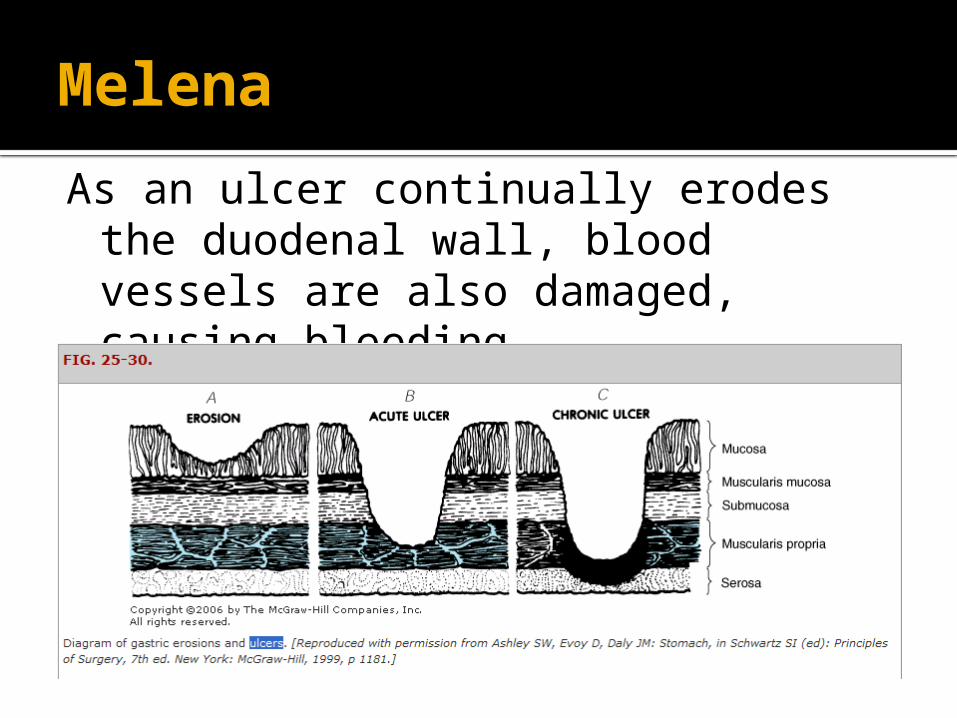
Melena
As an ulcer continually erodes the duodenal wall, blood vessels are also damaged, causing bleeding.

Melena
Tarry stools – Upper GI Bleeding can be confirmed by
nasogastric aspiration Principal indication for surgery
http://nyp.org/health/stomach-duodenal-ulcers.html

High BP
To compensate for the blood loss so as to not compromise circulation

Relatively high temperature
Chemical infection due to release of enzymes

LABORATORY FINDINGS

CBCDate 05/14/09 Ref. RangeINTHGB: 136 120-170 NHCT: 0.41 0.37-0.54 NPlatelet: 332 150 – 450
NWBC: 12.7 4.5 – 10.00 HIGHNeut: 0.83 0.50 – 0.70 HIGHLymph: 0.17 0.20 – 0.40LOW

UrinalysisDate 05/14/09Color : Dark yellowTransparency: Sl. TurbidpH: 6.0Sp. Gravity: 1.020Albumin: NegativeSugar : ++RBC: 0-3/hpfWBC : 0-3/hpf

Sodium and Potassium
Date 05/14/09 Ref. RangeINT
Sodium 136 137-147N
Potassium 3.5 3.5-5.1N

Serum amylase and lipase
Date 05/14/09 Ref. Range
INTAmylase 65.0 10-130 IU/L NLipase 31.8 13-60 IU/L N

RADIOLOGY

12-L ECG
NORMAL

CHEST X-RAY• There is a linear lucency noted in the subdiaphragmatic area suggestive ofPneumoperitoneum
• Suspicious infiltrates are seen in the right apex and right infraclavicular area.
• The heart is not enlarged
• The right hemidiaphragm is slightly elevated
• Sulci are intact

Medical and Surgical Management

Medical Management
Reduce acid output Increase mucosal protection Eliminate infectious agents
Acid-reducing medications Antacids –
Aluminum hydroxide Calcium carbonate Magnesium hydroxide Sodium bicarbonate
H2-receptor antagonists Competitively blocking binding of histamine to H2
receptors Cimetidine,famotidine,nizatidine,ranitidine
Proton pump inhibitors Omeprazole,lansoprazole Binds to H/K ATPase suppressing secretion of hydrogen
ions into the gastric lumen

Cytoprotective agents
Sucralfate Impairs HCl and prevents degradation of
mucus by pepsin Colloidal Bismuth
inhibit activity of pepsin, increase mucus secretion and interact with proteins in necrotic mucosal tissue

Treatment of Infectious Agents
Amoxicillin Bismuth compounds Clarithromycin Metronidazole Tetracycline
Sulperazone(sulbactam+cefoperazone)
Cefoperazone –3rd gen. cephalosporins Inhibits the bacterial cell wall synthesis,
and Sulbactam – acts as a beta-
lactamase inhibitor, to increase the antibacterial activity of cefoperazone against beta-lactamase producing organisms

Surgical Management
Indications for Surgery: Hemorrhage Perforation Obstruction Intractibility
Emergency exploratory laparotomy Primary repair with omental buttress

Acute abdomen secondary to perforated viscus secondary to PUD
Perforation Typically seen in anterior wall of the
duodenal bulb. Classic presentation is sudden severe
epigastric pain that rapidly spreads Generalized boardlike rigidity of the
abdomen

PreOperative Management
Optimize condition of patient Nasogastric tube placed Fluid resuscitation and hydration Pre-op monitoring Antibiotics Screening of other condition that will
interfere with treatment
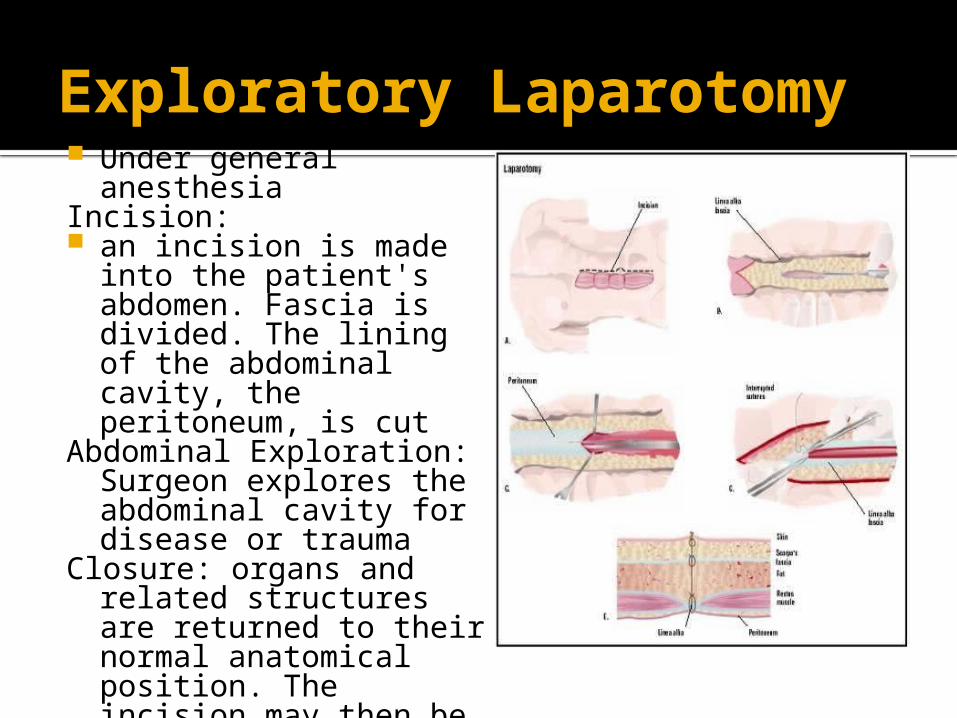
Exploratory Laparotomy Under general
anesthesia Incision: an incision is made into
the patient's abdomen. Fascia is divided. The lining of the abdominal cavity, the peritoneum, is cut
Abdominal Exploration: Surgeon explores the abdominal cavity for disease or trauma
Closure: organs and related structures are returned to their normal anatomical position. The incision may then be sutured (stitched closed).

Omental Patch
Sutures are placed across the perforation
And a piece of omentum is placed on top of the perforation
Sutures are securely tied to entrap the omentum as a plug
Post Operative Management NGT maintained Hydration continued – D5 NR IV Antibiotics
Pantoprazole 40mg/IV OD Sulperazone 1.5g/IV q8 hrs

Follow up Plan
Continue medications at home Continue daily wound care Resume moderate daily activities Follow up after a week or earlier if
any problem arises Advise patient to avoid skipping
meals and take small but frequent meals
.

JOURNAL PRESENTATION
Diagnostic, Treatment, Harm, Prognosis

Diagnosis of Helicobacter pylori infection using urease rapid test in patients with bleeding duodenal ulcer: influence of endoscopic signs and simultaneous corporal and antral biopsiesM. Castro Fernández, D. Sánchez Muñoz, E. García Díaz, M. V. Galán Jurado and C. Rodríguez AlonsoService of Digestive Diseases. Hospital Universitario de Valme. Sevilla. Spain
1130-0108/2004/96/9/599-605REVISTA ESPAÑOLA DE ENFERMEDADES DIGESTIVASCopyright © 2004 ARÁN EDICIONES, S. L.
REV ESP ENFERM DIG (Madrid)Vol. 96. N.° 9, pp. 599-605, 2004Recibido: 16-10-03.Aceptado: 27-01-04.Correspondencia: Manuel Castro Fernández. Servicio de Aparato Digestivo(9ª planta izda.). Hospital Universitario de Valme. Ctra. de Cádiz, s/n.41014 Sevilla. e-mail: [email protected]

Introduction: the sensitivity of invasive diagnostic methodsfor Helicobacter pylori (H. pylori) infection, particularly of ureaserapid test, is decreased in cases of gastroduodenal ulcer andupper gastrointestinal bleeding.
ABSTRACT

Objectives: to assess the influence of blood in the stomach or recent bleeding endoscopic signs in the diagnostic sensitivity of urease rapid test among patients with bleeding duodenal ulcer, as well as the influence of simultaneously collected corporal and antral biopsy samples.

Patients and methods: 120 patients, 85 male and 35 female,with
an average age of 62 (18-88) years, who were admitted to our Hospital due to bleeding duodenal ulcer and who received an endoscopic diagnosis within 24 hours of admission were included.
None of the patients had been under treatment with non-steroideal antiinflammatory drugs, proton-pump inhibitors or antimicrobial drugs in the two weeks prior to the bleeding event, and none had received eradicating therapy for H. pylori. In this group of selected patients an H. pylori infection rate nearing 100% was assumed.

H. pylori infection was ruled out using antral biopsy (69 cases) or both antral and fundic biopsies (51cases) for urease rapid testing (Jatrox®-H.p.-Test). Patients were classified in three groups according to their endoscopic bleeding signs: a) presence of blood in the stomach or recent bleeding ulcer(21 cases); b) ulcer showing non-recent bleeding signs (38 cases);and c) ulcer without bleeding signs (61 cases).
The sensitivity of the urease rapid test was
compared between patient groups.
Similarly,urease test results with an antral biopsy sample were compared in 100 patients with non-bleeding duodenal ulcer.

Results: urease test was positive in 93% of patients with
nonbleeding duodenal ulcer, and in 83% of patients with upper gastrointestinal bleeding, which reached statistical significance (p = 0.019).
This test was positive in 82.6% of patients with
an antral biopsy, and in 82.3% of patients with combined antral and fundic biopsies.
In group A, urease test was positive in 90.5% of patients; in group B, it was positive in 89.5% of patients, and in group C, the test turned positive in 75.4% of patients. Statistical differences were only reached when patients in group C were compared to patients in groups A and B together (p = 0.037).

Conclusions: 1. The presence of either blood in the
stomach or recent bleeding endoscopic signs appeared not to be the conditioning factor for the decreased sensitivity of urease test among patients with bleeding duodenal ulcer.
2. The decreased sensitivity of this test in patients with upper gastrointestinal bleeding is more evident during the resolution stage, and it does not seem to occur because of H. pylori migration from the antrum to the corporal gastric region.

LAPAROSCOPIC REPAIR FOR PERFORATED PEPTIC ULCERA Randomized Controlled Trial
Wing T. Siu, MBChB (HK), FRCSEd (Gen),* Heng T. Leong, MBBS (HK), FRCSEd,* Bonita K. B. Law, MBChB (HK), FRCSEd (Gen),* Chun H. Chau, MBBS (Jinan), LMCHK (HK), FRCSEd (Gen),* Anthony C. N. Li, MBBS (HK), FRCSEd,* Kai H. Fung, MBBS (HK), FRCR (UK),† Yuk P. Tai, MBBS (Lond), FRCSEd, and * Michael K. W. Li, MBBS (Lond), MRCS (Eng.), LRCP(Eng.), FRCS (Eng.), FRCSEd*
From the Departments of *Surgery and †Diagnostic Radiology, Pamela Youde Nethersole Eastern Hospital, Chai Wan,Hong Kong, SAR, China
OBJECTIVETo compare the results of open versus laparoscopic repair for perforated peptic ulcers.
SUMMARY BACKGROUND DATA Omental patch repair with peritoneal lavage is the mainstay of treatment for perforated peptic ulcers in many institutions.
Laparoscopic repair has been used to treat perforated peptic ulcers since 1990, but few randomized studies have been carried out to compare open versus laparoscopic procedures.

METHODS
• A Gastrografin meal was performed 48 to 72 hours after surgery to document sealing of the perforation.




CONCLUSION Laparoscopic repair of perforated peptic ulcer is a safe and reliable procedure.
It was associated with a shorter operating time, less postoperative pain, reduced chest complications, a shorter postoperative hospital stay, and earlier return to normal daily activities than the conventional open repair.

Laparoscopic repair of perforated peptic ulcerA meta-analysisH. LauDepartment of Surgery, University of Hong Kong Medical Center, Tung Wah Hospital, 12 Po Yan Street, Sheung Wan, Hong Kong, China
Received: 14 October 2003/Accepted: 7 January 2003/Online publication: 12 May 2004

To compare the safety and efficacy of open and laparoscopic repair of perforated peptic ulcer in an evidence-based approach using meta-analytical techniques
OBJECTIVE
SUMMARY BACKGROUND DATA• Although laparoscopic repair combines the
principles of open repair with the advantages of minimal access surgery, it has not been widely accepted by general surgeons

Literature search: Search of electronic databases, including MEDLINE and EMBASE between January 1990 and December 2002
Inclusion criteria: All prospective randomized trials or case–control studies that compared the outcomes of laparoscopic and open repair of perforated peptic ulcer were included. For the laparoscopic treatment group, only patients who underwent laparoscopic suture repair were recruited
Data extraction: Standardized data abstract form
Data pooling and statistics: An effect size for the outcome parameter of individual studies was calculated by the odds ratio (OR). The effect sizes of all trials were tested for heterogeneity by Q Statistics. A qualitative review of the outcome data was performed when a formal meta-analysis was not feasible. Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS, Chicago, IL,USA) software program and Comprehensive Meta-analysis
All reports (13) were critically appraised with respect to their methodology and outcome
METHODS

RESULTS
Meta-analyses demonstrated a significant reduction in the wound infection rate after laparoscopic repair, as compared with open repair, but a significantly higher reoperation rate was observed after laparoscopic repair.
Factors considered in the comparison of laparoscopic and open surgery were as follows:
Length of operation ConversionPostoperative painPostoperative complicationsReoperationMortalityLength of hospital stayRecovery variables

Length of operation: Five studies demonstrated a significantly longer operative time for laparoscopic repair
Conversion: Reported rates of conversion to open repair ranged from 0% to 29.1%
Postoperative pain: A postoperative assessment of pain score consistently showed a lower pain score after laparoscopic repair than after open repair
Postoperative complications: Chest infection was the most common postoperative morbidity. Naesgaard et al. in their retrospective study, demonstrated a significantly higher incidence of chest infection in the laparoscopic group. But subsequent meta-analyses showed a lower overall chest infection rate after laparoscopic repair
Wound infection was the next most common morbidity after open repair of perforated peptic ulcer. Subsequent meta-analyses proved that laparoscopic repair conferred a significant reduction in wound infection rate, as compared with open repair.

Leakage was more common after laparoscopic repair than after open repair. Intraabdominal collection was more prevalent after laparoscopic repair than after open repair. Most of the studies demonstrated a higher incidence of intraabdominal collection or abscess formation after laparoscopic repair.
Reoperation: The overall reoperation rate was 3.7% (n = 11) for laparoscopic repair (n = 294) and 1.9% (n = 7) for open repair (n = 364). Leakage was the chief reason for reoperation. Subsequent meta-analyses found a significantly lower reoperation rate after open repair.
Mortality None of the mortality was attributed directly to the adoption of laparoscopic repair. The subsequent pooled estimate of the overall mortality favored laparoscopic repair.
Length of hospital stay All the studies showed that the length of hospital stay after laparoscopic repair was either shorter than or equal to that associated with open repair.
Recovery variables: Only Katkhouda et al. showed significantly earlier resumption of the normal diet after laparoscopic repair. Siu et al. found that patients returned to normal activities after laparoscopic repair within an average of 10 ± 6.9 days, which was significantly earlier than the return of those who underwent open repair (26 ± 15.1 days).

DISCUSSION
The rationale for the sutureless technique is both to simplify the procedure and to shorten the operative time. However, sutureless repair using a plug of gelatin sponge with fibrin glue has not gained wide acceptance because of its associated higher leakage rate, particularly if the ulcer is larger than 5 mm in diameter.
One main drawback of laparoscopic repair was the increase in operating time.
Another disadvantage of laparoscopic repair was a significantly increased reoperation rate, which was a consequence of postoperative leakage. The higher incidence of leakage after laparoscopic repair may be attributable in part to a faulty technique of laparoscopic closure. Furthermore, the higher incidence of intraabdominal collection was secondary to inadequate lavage and suctioning of the peritoneal cavity. Perfection and standardization of the laparoscopic technique for the repair of perforated ulcer is therefore necessary.

CONCLUSION
Laparoscopic repair is effective and superior to open repair in terms of early postoperative outcomes including pain, wound infection, and functional recovery.
However, the relative benefits of the laparoscopic approach must be weighted against the increased risk of mortality, which can be reliably predicted by preoperative assessment of Boey’s risk factors and the APACHE II score. It is therefore of paramount importance that patients be selected carefully for the laparoscopic approach. Patients who have one or more of Boey’s risk factors are therefore less suitable for laparoscopic surgery.
Other relative contraindications for laparoscopic repair include the concomitant presence of other ulcer complications such as bleeding and obstruction, large perforation, technical difficulty, previous upper abdominal operations, and serious associated cardiopulmonary diseases.

Meta-analyses of the 13 recruited trials demonstrated that laparoscopic repair was associated with a significantly lower wound infection rate. Laparoscopic repair of perforated peptic ulcer also was associated with reduced postoperative pain and diminished analgesic consumption.
Currently, the main drawbacks of laparoscopic repair are a longer operation and a higher reoperation rate. Both laparoscopic and open repairs of perforated peptic ulcer, being complementary to each other, have their roles in the management of perforated peptic ulcer.
**Boey’s risk factors: concurrent major medical illness, preoperative shock, and delayed presentation of more than 24 hours

Randomized Clinical Trial of Laparoscopic Versus Open Repair of the Perforated Peptic Ulcer: The LAMA Trial
Mariëtta J. O. E. Bertleff, 1 Jens A. Halm,2 Willem A. Bemelman,3 Arie C. van der Ham,4 Erwin van der Harst,5 Hok I. Oei,6 J. F. Smulders,7 E. W. Steyerberg,8 and Johan F. Lange2

OBJECTIVETo evaluate whether laparoscopic closure of a PPU is as safe as conventional open correction.
SUMMARY BACKGROUND DATA
Laparoscopic surgery has become popular during the last decade mainly because it is associated with fewer postoperative complications than the conventional open approach.
It remains unclear, however, if this benefit is observed after laparoscopic correction of perforated peptic ulcer (PPU).

METHODS


RESULTS
Operating time was significantly longer in the laparoscopy group (75 min versus 50 min), which is comparable to reports in the literature [3, 10]
Laparoscopic correction of PPU causes less postoperative pain [6, 12, 17, 18]

Open repair > Laparascopic

Open repair > laparascopic

CONCLUSION
Results of the LAMA trial confirm the results of other trials that laparoscopic correction of PPU is safe, feasible for the experienced laparoscopic surgeon, and causes less postoperative pain.
Operating time was longer in the laparoscopic group and there was no difference in length of hospital stay or incidence of postoperative complications.

APPENDIX