Embed Size (px)
Citation preview
Journal ReadingJournal Reading
2005-12-022005-12-02Presented by Dr.Presented by Dr. 陳志榮陳志榮
An Illustrated Consensus on the ClassificatiAn Illustrated Consensus on the Classification of Pancreatic Intraepithelial Neoplasia aon of Pancreatic Intraepithelial Neoplasia and Intraductal Papillary Mucinous Neoplasnd Intraductal Papillary Mucinous Neoplas
mm
Original articleOriginal article
Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Hruban RH, Takaori K, Klimstra DS, Adsay NV, Albores-Saavedra J, Biankin AV, Biankin SA, Compton C, FukusSaavedra J, Biankin AV, Biankin SA, Compton C, Fukushima N, Furukawa T, Goggins M, Kato Y, Kloppel G, Lonhima N, Furukawa T, Goggins M, Kato Y, Kloppel G, Longnecker DS, Luttges J, Maitra A, Offerhaus GJ, Shimizu gnecker DS, Luttges J, Maitra A, Offerhaus GJ, Shimizu
M, Yonezawa S.M, Yonezawa S.
Am J Surg Pathol. 2004 Aug;28(8):977-87.Am J Surg Pathol. 2004 Aug;28(8):977-87.
IntroductionIntroduction
• Identification and treatment of pre-invasive lesiIdentification and treatment of pre-invasive lesions in the ducts of the pancreas is important.ons in the ducts of the pancreas is important.
• Noninvasive precursors: Noninvasive precursors: (1) Pancreatic intraepithelial neoplasm (PanINs)(1) Pancreatic intraepithelial neoplasm (PanINs)(2) Intraductal papillary mucinous neoplasm (IPM(2) Intraductal papillary mucinous neoplasm (IPM
N)N)(3) Mucinous cystic neoplasm(3) Mucinous cystic neoplasm the first two lack the internationally accepted nthe first two lack the internationally accepted n
omenclature and diagnostic criteria.omenclature and diagnostic criteria.
IntroductionIntroduction
• Pancreatic intraepithelial neoplasia (PaPancreatic intraepithelial neoplasia (PanIN): first proposed in 1994. nIN): first proposed in 1994.
• Developed at a National Cancer InstitutDeveloped at a National Cancer Institute in 1999.e in 1999.
• Progression model for pancreatic neoplProgression model for pancreatic neoplasia:asia:
a series of molecular analysesa series of molecular analyses
IntraductionIntraduction
IntroductionIntroduction
IntroductionIntroduction
• Papillomatosis of pancreatic duct: case rPapillomatosis of pancreatic duct: case report in 1936eport in 1936
• A series of intraductal neoplasm of pancrA series of intraductal neoplasm of pancreas: byOhhashi et al in 1982.eas: byOhhashi et al in 1982.
• Intraductal papillary mucinous neoplasm Intraductal papillary mucinous neoplasm (IPMN): introduced by Sessa et al in 1994.(IPMN): introduced by Sessa et al in 1994.
• A progression model for IPMNs: a growinA progression model for IPMNs: a growing body of molecular and clinical evidence.g body of molecular and clinical evidence.
IntroductionIntroduction
IntroductionIntroduction
IntroductionIntroduction
• 2002, Nagoyo, Japan: PanIN and IPMN s2002, Nagoyo, Japan: PanIN and IPMN should be revised and clarifiedhould be revised and clarified
• 2003, The Johns Hopkins Hospital: 2003, The Johns Hopkins Hospital: (1) Characteristics of PanIN and IPMN (1) Characteristics of PanIN and IPMN (2) Ambiguities in the previous classification system(2) Ambiguities in the previous classification system
ss(3) Revised definition(3) Revised definition
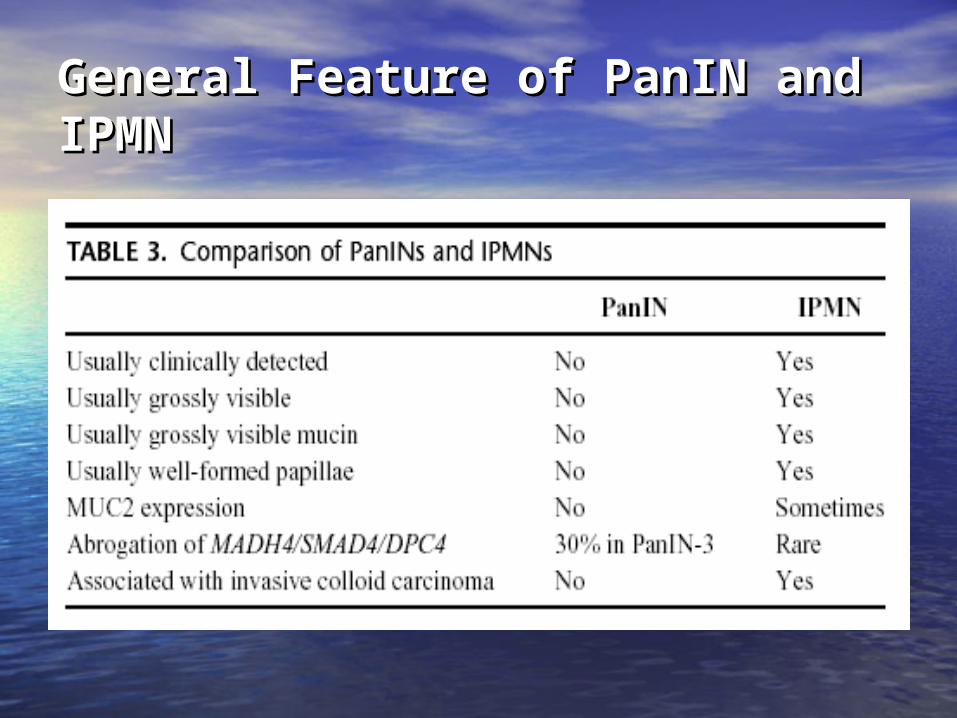
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• PanIN/L-1A and PanIN-1B: common incidentPanIN/L-1A and PanIN-1B: common incidental findingal finding
• Higher-grade PanIN: more often associated Higher-grade PanIN: more often associated with an invasive cancer.with an invasive cancer.
(1)(1) PanIN-1 lesions: 40% of adult pancreas withoPanIN-1 lesions: 40% of adult pancreas without cancer (PanIN-3 lesions are seen in <5% of ut cancer (PanIN-3 lesions are seen in <5% of such pancreas)such pancreas)
(2) PanIN-3: 30%~50% of pancreas with invasive(2) PanIN-3: 30%~50% of pancreas with invasive ductal carcinoma.ductal carcinoma.
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• Higher grade of PanIN: can be a precursors of iHigher grade of PanIN: can be a precursors of invasive carcinoma nvasive carcinoma
(1) Same genetic alterations in invasive ductal ca(1) Same genetic alterations in invasive ductal carcinoma and PanINs: KRAS2, TP53/p53, CDKN2rcinoma and PanINs: KRAS2, TP53/p53, CDKN2A/p16, and MADH4/SMAD4/DPC4 genesA/p16, and MADH4/SMAD4/DPC4 genes
(2) Continum of intraductal neoplastic progressi(2) Continum of intraductal neoplastic progression: greater numbers of genetic alteration in hion: greater numbers of genetic alteration in higher-grade PanIN lesions. gher-grade PanIN lesions.
General Feature of PanIN and IPMGeneral Feature of PanIN and IPMNN• IPMN: IPMN: (1) Typical radiographically identifiable ductal dilatat(1) Typical radiographically identifiable ductal dilatat
ion:ion: (a) Main duct type: main pancreatic ducts(a) Main duct type: main pancreatic ducts (b) Branch duct type: secondary ducts (b) Branch duct type: secondary ducts (c) Mixed type: both(c) Mixed type: both(2) Associated with an invasive adenocarcinoma: part(2) Associated with an invasive adenocarcinoma: part
icular main duct type.icular main duct type. (a) Colloid (mucinous noncystic) carcinoma:(a) Colloid (mucinous noncystic) carcinoma: approximately one half approximately one half (b) Conventional tubular adenocarcinoma: (b) Conventional tubular adenocarcinoma: the most of remainderthe most of remainder
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• IPMN: can be a precursors of invasive cIPMN: can be a precursors of invasive carcinomaarcinoma
(1)(1)Same genetic alterations in conventionSame genetic alterations in conventionalal
ductal adenocarcinoma: KRAS2, TP53/pductal adenocarcinoma: KRAS2, TP53/p53, and CDKN2A/p16 genes.53, and CDKN2A/p16 genes.
General Feature of PanIN and IPMGeneral Feature of PanIN and IPMNN(2)(2) Frequencies and stage of neoplastic progression : differFrequencies and stage of neoplastic progression : differ from PanIN.from PanIN. (a) CDKN2A/p16 gene, may be inactivated through(a) CDKN2A/p16 gene, may be inactivated through aberrant DNA methylationaberrant DNA methylation.. (b) IPMNs with carcinoma in situ: microsatellite(b) IPMNs with carcinoma in situ: microsatellite instability (-), high telomerase activity (+), and COX-2instability (-), high telomerase activity (+), and COX-2 expression (+).expression (+). (c) IPMNs: one third with inactived Peutz-Jeghers gene(c) IPMNs: one third with inactived Peutz-Jeghers gene STK11/LKB1 ( some patients with Peutz-JeghersSTK11/LKB1 ( some patients with Peutz-Jeghers syndrome develop IPMNs ).syndrome develop IPMNs ). (d) IPMNs: rare abnormalities in the MADH4/SMAD4/DPC4 ge(d) IPMNs: rare abnormalities in the MADH4/SMAD4/DPC4 ge
ne, in contrast to ductal adenocarcinomas and PanIN-3 lesine, in contrast to ductal adenocarcinomas and PanIN-3 lesions.(~30%)ons.(~30%)
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• Surgical resection: treatment of choice fSurgical resection: treatment of choice for most IPMNsor most IPMNs
• IPMNs resected before the developmenIPMNs resected before the development of invasive carcinoma are highly curabt of invasive carcinoma are highly curable.le.
• The prognosis is worse once invasive caThe prognosis is worse once invasive carcinoma develops: rcinoma develops: colloid type of invasicolloid type of invasive carcinoma has better prognosis than ve carcinoma has better prognosis than tubular type of invasive carcinoma.tubular type of invasive carcinoma.
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• Immunohistochemistry: MUC proteins Immunohistochemistry: MUC proteins (1) MUC2 : expressed in many IPMNs.(1) MUC2 : expressed in many IPMNs.
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• PanINs and IPMNs share many fundamental fePanINs and IPMNs share many fundamental features:atures:
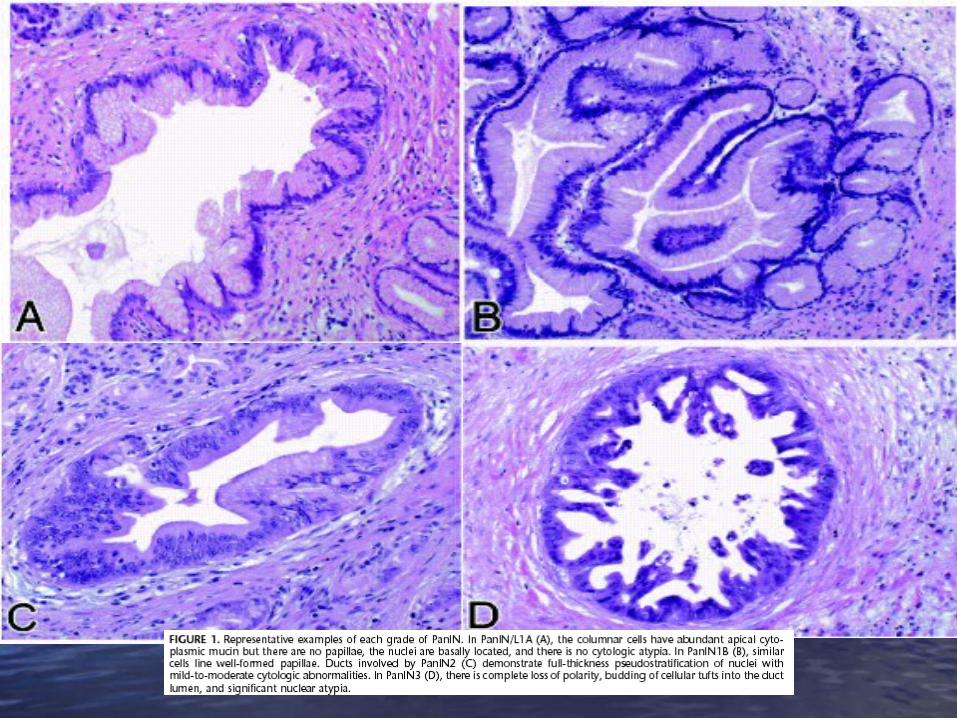
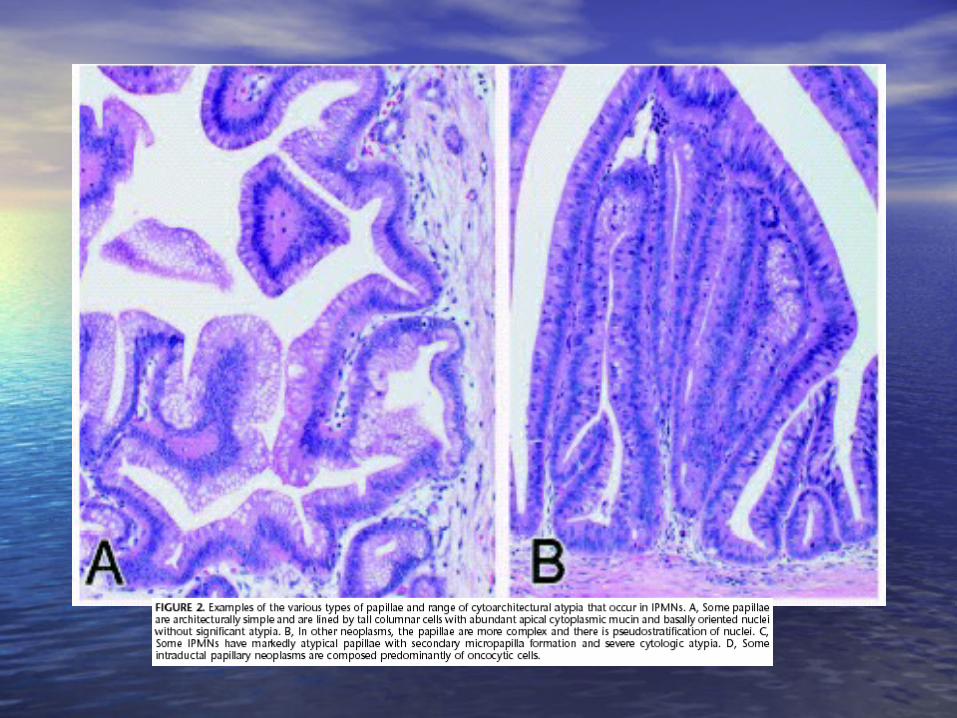
(1) Intraductal growth(1) Intraductal growth(2) Columnar, mucin- producing cells(2) Columnar, mucin- producing cells(3) Flat or papillae(3) Flat or papillae(4) A range of cytologic and architectural atypia(4) A range of cytologic and architectural atypia(5) Precursors to invasive adenocarcinoma(5) Precursors to invasive adenocarcinoma(6) Sequentially accumulate similar genetic(6) Sequentially accumulate similar genetic alterations with increasing cytoarchitectural atypia.alterations with increasing cytoarchitectural atypia.
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
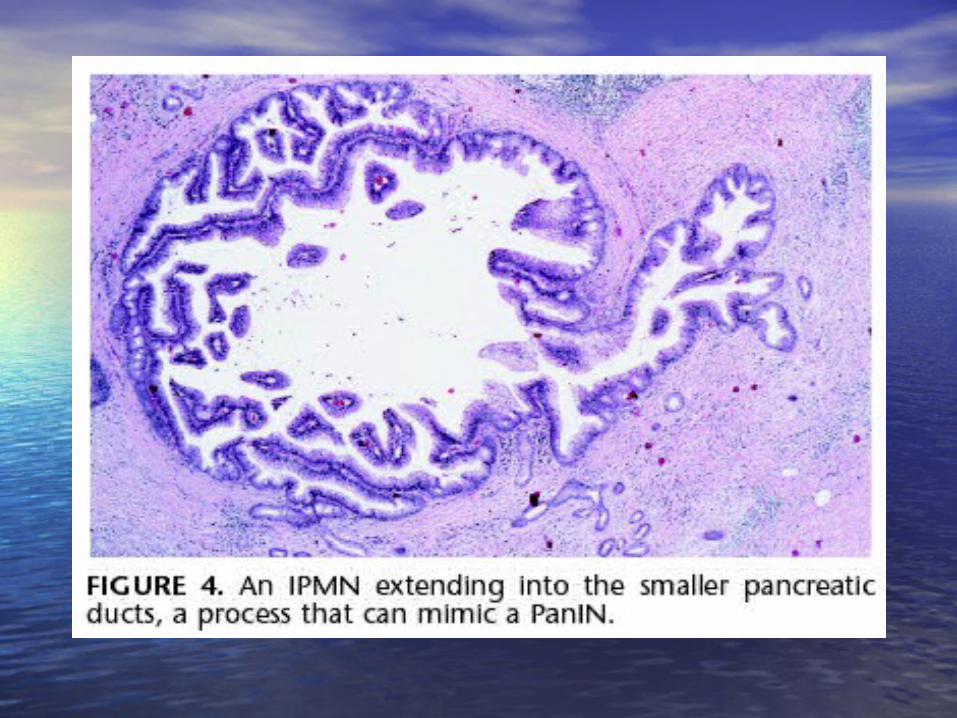
• Sometimes, intraductal neoplasm may be Sometimes, intraductal neoplasm may be almost impossible to classify almost impossible to classify by morpholoby morphology alone.gy alone.
(1) PanIN: typical arise in the smaller ducts,(1) PanIN: typical arise in the smaller ducts, may involve the large ductsmay involve the large ducts(2) IPMNs: usually involve the larger ducts,(2) IPMNs: usually involve the larger ducts, may involve small ductsmay involve small ducts
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
• Despite this overlap, there are abundant Despite this overlap, there are abundant data suggesting that PanINs and IPMNs rdata suggesting that PanINs and IPMNs represent epresent two separate classes of intradutwo separate classes of intraductal neoplasia of pancreasctal neoplasia of pancreas..
General Feature of PanIN and IPMNGeneral Feature of PanIN and IPMN
Ambiguities in the Previous Classification Ambiguities in the Previous Classification SystemsSystems
• The size of involved duct: The size of involved duct: (1) Size: the only factor used to distinguish between PanINs and IP(1) Size: the only factor used to distinguish between PanINs and IP
MNs in the previous classification systemMNs in the previous classification system(2) Some IPMNs involve the branch ducts and can be <1 cm, and still (2) Some IPMNs involve the branch ducts and can be <1 cm, and still
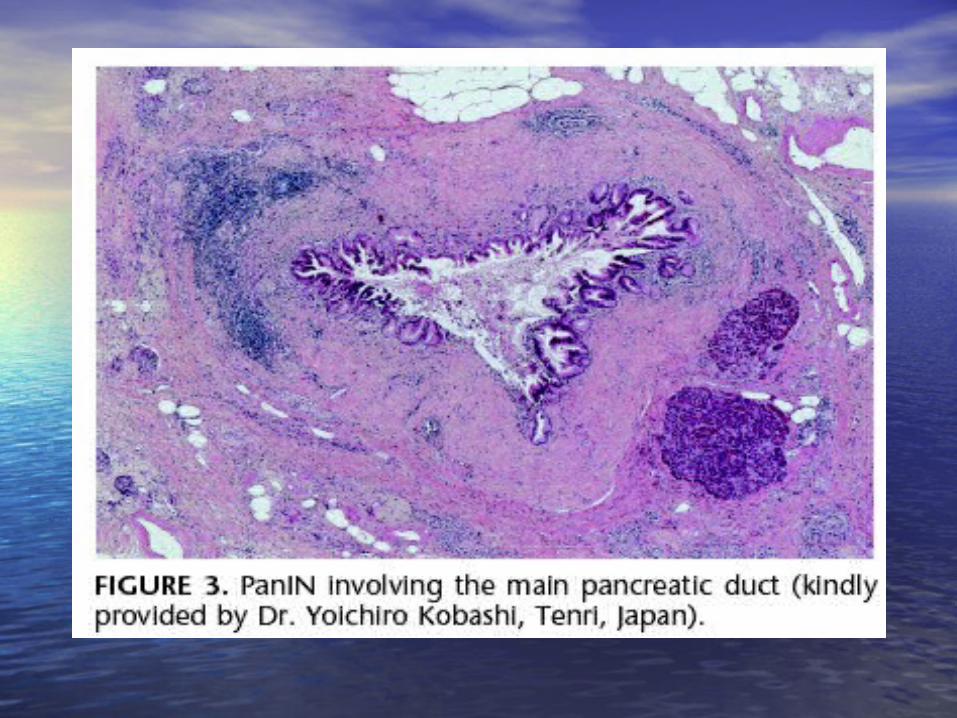
other IPMNs extend into the smallest caliber pancreatic ducts other IPMNs extend into the smallest caliber pancreatic ducts (3) Some PanINs can involve the main pancreatic duct and ducts in(3) Some PanINs can involve the main pancreatic duct and ducts in
volved with PanINs can be large due to secondary dilatation frovolved with PanINs can be large due to secondary dilatation from an obstructing mass or stricture m an obstructing mass or stricture
New definitions were needed that encompass these possibilities.New definitions were needed that encompass these possibilities.
Ambiguities in the Previous Classification Ambiguities in the Previous Classification SystemsSystems
• Measurement of involved duct: no specific gMeasurement of involved duct: no specific guidelines:uidelines:
(1)(1) The anatomic terms are particularly hard to The anatomic terms are particularly hard to apply to histological sections.apply to histological sections.
(2)(2) Extent of ductal dilatation often is difficult to Extent of ductal dilatation often is difficult to establish based on the diameter of the duct: iestablish based on the diameter of the duct: impossible to determine the original caliber ompossible to determine the original caliber of an involved ductf an involved duct
Ambiguities in the Previous Classification Ambiguities in the Previous Classification SystemsSystems
• Reproducible criteria: the previous classiReproducible criteria: the previous classification system failed to provide to distification system failed to provide to distinguish between retention cysts and IPMnguish between retention cysts and IPMNs.Ns.
• ““Cancerization of the duct”: a histologCancerization of the duct”: a histologic finding to be distinguished from PanIic finding to be distinguished from PanIN, N,
Ambiguities in the Previous Classification Ambiguities in the Previous Classification SystemsSystems
• Reactive change:Reactive change:(1)(1)Previous classification system : againsPrevious classification system : agains
t diagnosing PanIN in the setting of inflt diagnosing PanIN in the setting of inflammationammation
(2)(2) Now recognized that PanIN lesions caNow recognized that PanIN lesions can, and often do, occur in the setting of n, and often do, occur in the setting of chronic pancreatitis.chronic pancreatitis.
Ambiguities in the Previous Classification Ambiguities in the Previous Classification SystemsSystems
• Complex lesins: multiple lesions are present in a singlComplex lesins: multiple lesions are present in a single pancreas.e pancreas.
• Limits of radiologic detection: the use of radiologic deLimits of radiologic detection: the use of radiologic detectability in the definitions of PanINs and IPMNs shoutectability in the definitions of PanINs and IPMNs should be abandonedld be abandoned
Ambiguities in the Previous Ambiguities in the Previous Classification SystemsClassification Systems
• It was recognized that the current gradiIt was recognized that the current grading systems for PanINs (PanIN-1, PanIN-2,ng systems for PanINs (PanIN-1, PanIN-2, and PanIN-3) and IPMNs (IPMN adenom and PanIN-3) and IPMNs (IPMN adenoma, IPMN borderline, IPMN carcinoma in sia, IPMN borderline, IPMN carcinoma in situ) lack interobserver reproducibility. tu) lack interobserver reproducibility.
• A better consensus on the features definA better consensus on the features defining each grade is needed.ing each grade is needed.
Ambiguities in the Previous Ambiguities in the Previous Classification SystemsClassification Systems
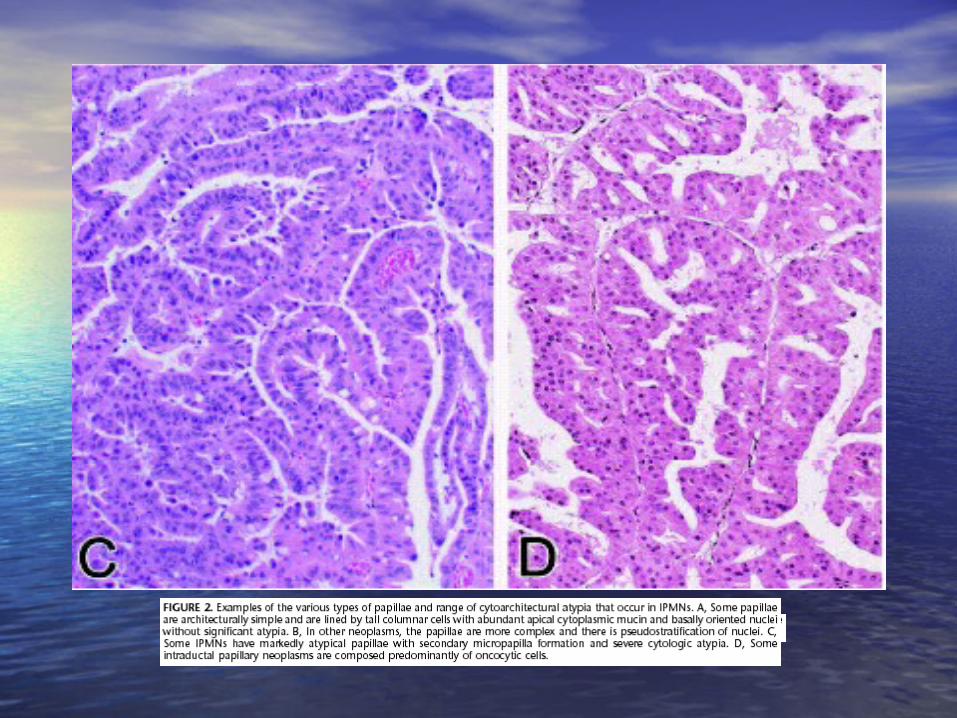
• It was acknowledged that different histoIt was acknowledged that different histologic types of papillae may occur in IPMlogic types of papillae may occur in IPMNs and that criteria and designations for Ns and that criteria and designations for each different type need to be better defeach different type need to be better defined.ined.
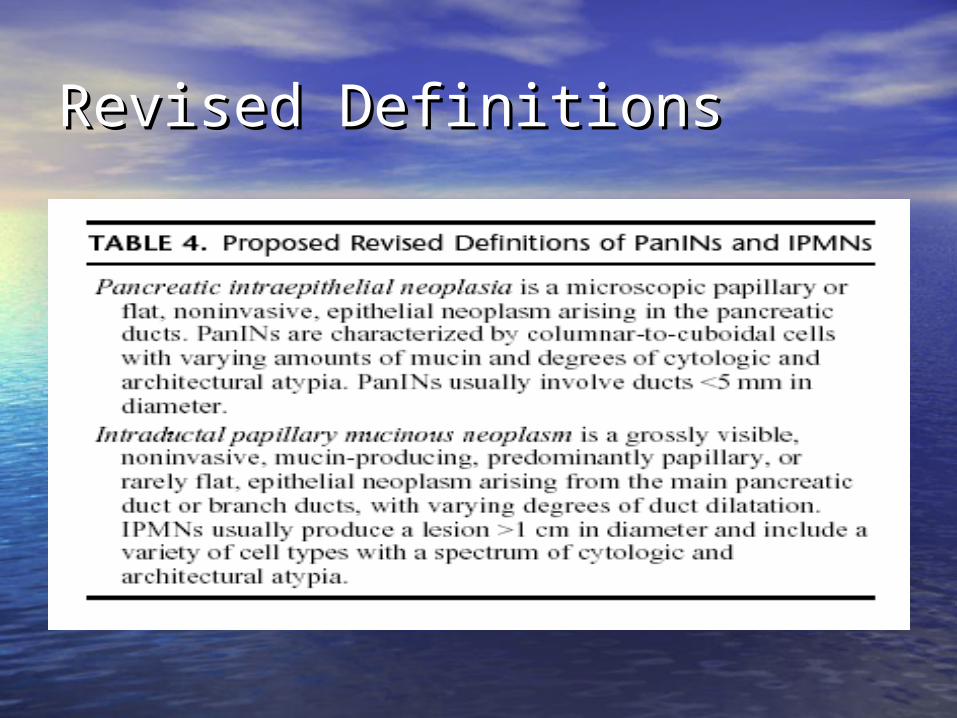
Revised DefinitionsRevised Definitions
Guidelines for Evaluation of PanINsGuidelines for Evaluation of PanINs
• Size: Size: (1) <5mm: cross sectioned diameter: from base(1) <5mm: cross sectioned diameter: from base
ment membrane to basement membrane.ment membrane to basement membrane.(2) >5mm: carefully examination of multiple sect(2) >5mm: carefully examination of multiple sect
ions of the pancreatic ductsions of the pancreatic ducts• Neoplasms: Neoplasms: (1)(1)Not mean to suggest the lesion need clinical Not mean to suggest the lesion need clinical
treatment.treatment.(2) Clonal proliferation with alterations in cance(2) Clonal proliferation with alterations in cance
r-related genes.r-related genes.
Guidelines for Evaluation of PanINsGuidelines for Evaluation of PanINs
• PanINs-1 and -2 :PanINs-1 and -2 :(1)(1)Typically incidental findings Typically incidental findings (2)(2)Unproved clinical significance.Unproved clinical significance.• PanIN-3: PanIN-3: (1)(1)Thought to have clinical significance:Thought to have clinical significance: (a) Potential to progress to invasive carcinoma(a) Potential to progress to invasive carcinoma (b) Information regarding progression is limited(b) Information regarding progression is limited• Difference with IPMN: when PanIN involving the main pancreatic Difference with IPMN: when PanIN involving the main pancreatic
duct duct (1) Papillae in PanINs: usually are not as tall and complex as those i(1) Papillae in PanINs: usually are not as tall and complex as those i
n IPMNs. n IPMNs. (2) Abundant luminal mucin production is a feature of IPMNs.(2) Abundant luminal mucin production is a feature of IPMNs.(3) MUC2 expression is a specific but relatively insensitive marker of (3) MUC2 expression is a specific but relatively insensitive marker of
an IPMN and is generally not present in PanINs.an IPMN and is generally not present in PanINs.
Guidelines for Evaluation of PanINsGuidelines for Evaluation of PanINs
• If multiple distinct PanINs in a single panIf multiple distinct PanINs in a single pancreas: creas:
(1) Graded separately (1) Graded separately (2) Many prefer to list the range and/or(2) Many prefer to list the range and/or the highest grade of PanIN present.the highest grade of PanIN present.
Guidelines for Evaluation of PanINsGuidelines for Evaluation of PanINs
• Reactive epithelial changes from PanINs:Reactive epithelial changes from PanINs:(1) A heterogeneous cell population (1) A heterogeneous cell population (2) Prominent nucleoli(2) Prominent nucleoli(3) Intraepithelial inflammatory cells, particularly neutro(3) Intraepithelial inflammatory cells, particularly neutro
philsphils should all suggest a reactive processshould all suggest a reactive process. .
In general, it is agreed that one should be conservativIn general, it is agreed that one should be conservative in categorizing a lesion as a PanIN in the setting of ine in categorizing a lesion as a PanIN in the setting of inflammation. flammation.
Guidelines for Evaluation of PanINsGuidelines for Evaluation of PanINs
• ““Cancerization of the ducts,” and can occur either Cancerization of the ducts,” and can occur either as direct continuity of invasive carcinoma. as direct continuity of invasive carcinoma.
(1) These processes should be distinguished from PanIN-(1) These processes should be distinguished from PanIN-3. 3.
(2) Suggest secondary ductal involvement: (2) Suggest secondary ductal involvement: (a) An abrupt transition from markedly atypical to(a) An abrupt transition from markedly atypical to normal-appearing epithelium normal-appearing epithelium (b) Continuity of the involved duct with invasive (b) Continuity of the involved duct with invasive carcinomacarcinoma
Guidelines for Evaluation of IPMNsGuidelines for Evaluation of IPMNs
• Entirely submitted for histologic examinEntirely submitted for histologic examination:ation:
The associated invasive cancer is the moThe associated invasive cancer is the most important determinant of prognosis fst important determinant of prognosis for patients with an IPMN. or patients with an IPMN.
Guidelines for Evaluation of IPMNsGuidelines for Evaluation of IPMNs
• Differential diagnosis of IPMNs:Differential diagnosis of IPMNs:(1) PanINs: If both PanINs and an IPMN are present in a single pancr(1) PanINs: If both PanINs and an IPMN are present in a single pancr
eas, efforts should be made to separate these lesions using the aeas, efforts should be made to separate these lesions using the above-mentioned criteria. bove-mentioned criteria.
(2) Mucinous cystic neoplasm:(2) Mucinous cystic neoplasm: (a) The presence of ovarian-type stroma (a) The presence of ovarian-type stroma (b) The absence of ductal involvement(b) The absence of ductal involvement(3) Retention cysts: (3) Retention cysts: (a) Flat, or at most very low papillary, epithelium.(a) Flat, or at most very low papillary, epithelium. (b) Epithelial atypia is minimal in retention cysts(b) Epithelial atypia is minimal in retention cysts (c) Usually unilocular.(c) Usually unilocular.
Guidelines for Evaluation of IPMNsGuidelines for Evaluation of IPMNs
• Involvement what kind of ducts?Involvement what kind of ducts?(1) (1) Main duct type ? branch duct type? Or mixed type?Main duct type ? branch duct type? Or mixed type? Branch duct-type IPMNs are usually confined to the heBranch duct-type IPMNs are usually confined to the he
ad/tail of the pancreas, they tend to occur at a youngead/tail of the pancreas, they tend to occur at a younger age, and they less often are associated with an invasir age, and they less often are associated with an invasive cancer than main duct type IPMNsve cancer than main duct type IPMNs
(2) Efforts should be made, radiographically or at the tim(2) Efforts should be made, radiographically or at the time of gross examination of resected specimens, to detee of gross examination of resected specimens, to determine if an IPMN involves the main pancreatic duct or rmine if an IPMN involves the main pancreatic duct or a branch duct.a branch duct.
Issues Requiring Further Issues Requiring Further StudyStudy• Neoplasm ? Lesion? Hyperplasia?Neoplasm ? Lesion? Hyperplasia?(1) These entities with the modifying term “lesion” (“(1) These entities with the modifying term “lesion” (“
PanIN/L-1A”) to acknowledge that the neoplastic natPanIN/L-1A”) to acknowledge that the neoplastic nature of many cases of PanIN-1A has not been unambigure of many cases of PanIN-1A has not been unambiguously established.uously established.
(2) Similarly, the Japanese classification system for IPM(2) Similarly, the Japanese classification system for IPMNs includes “Intraductal papillary mucinous tumor -hNs includes “Intraductal papillary mucinous tumor -hyperplasia”for histologically low-grade structures wityperplasia”for histologically low-grade structures without atypia. hout atypia.
(3) Additional study is needed to identify reproducible cr(3) Additional study is needed to identify reproducible criteria to distinguish hyperplastic lesions from low-graiteria to distinguish hyperplastic lesions from low-grade neoplasms.de neoplasms.
Issues Requiring Further Issues Requiring Further StudyStudy• Reproducible criteria?Reproducible criteria?(1) Morphometric evidence that a two-tier system (low-g(1) Morphometric evidence that a two-tier system (low-g
rade/high-grade) may be more reproducible. rade/high-grade) may be more reproducible. (2) It was the consensus of the group that further genetic (2) It was the consensus of the group that further genetic
and morphologic studies should be conducted to refinand morphologic studies should be conducted to refine the histologic grading of PanINs and IPMNs. e the histologic grading of PanINs and IPMNs.
Issues Requiring Further Issues Requiring Further StudyStudy• Histologic classification of IPMN:Histologic classification of IPMN:(1) Morphologically, IPMNs may have a variety of different cytoarchi(1) Morphologically, IPMNs may have a variety of different cytoarchi
tectural features even in different regions of a single neoplasm. tectural features even in different regions of a single neoplasm. (2) Some separate IPMNs into clear-, dark-, and compact-cell types (2) Some separate IPMNs into clear-, dark-, and compact-cell types
based on the density of the cytoplasm and the shape of the epithbased on the density of the cytoplasm and the shape of the epithelial cells, and the expression patterns of MUC1, MUC2, and MUCelial cells, and the expression patterns of MUC1, MUC2, and MUC5AC5AC
(3) It also has been proposed that IPMNs should be subdivided into (3) It also has been proposed that IPMNs should be subdivided into gastrointestinal, pancreaticobiliary, and oncocytic subtypes. It wgastrointestinal, pancreaticobiliary, and oncocytic subtypes. It was the consensus of the group that further clinical, genetic, and as the consensus of the group that further clinical, genetic, and morphologic studies are needed to refine the histologic classificamorphologic studies are needed to refine the histologic classification of IPMNs.tion of IPMNs.
Issues Requiring Further Issues Requiring Further StudyStudy• Finally, some of the group speculated on the interesting possibiliFinally, some of the group speculated on the interesting possibili
ty that some IPMNs may begin as PanINs that then progress alonty that some IPMNs may begin as PanINs that then progress along a different pathway of neoplasia than conventional pancreatic g a different pathway of neoplasia than conventional pancreatic ductal adenocarcinoma. ductal adenocarcinoma.
Conclusion Conclusion
• IPMNs and PanINs are important precursors to invasivIPMNs and PanINs are important precursors to invasive adenocarcinoma of the pancreas. It is our hope that e adenocarcinoma of the pancreas. It is our hope that the proposed revised definitions and diagnostic guidethe proposed revised definitions and diagnostic guidelines presented will help advance the study of these lelines presented will help advance the study of these lesions such that genesis of pancreatic cancer will be elsions such that genesis of pancreatic cancer will be elucidated and that pancreatic cancer, one of the most ucidated and that pancreatic cancer, one of the most dreadful diseases of humankind, can one day be treatdreadful diseases of humankind, can one day be treated at the preinvasive stage.ed at the preinvasive stage.


![(Endometrial Intraepithelial Neoplasia): Improved Criteria ... · Endometrial intraepithelial neoplasia [EIN] EIN Reproducibility UsubutumA et al Modern Pathol25: 877-884, 2012. Questionaire,](https://img.pdfslide.us/doc/110x75/6053ec04465f250d537d95f4/endometrial-intraepithelial-neoplasia-improved-criteria-endometrial-intraepithelial.jpg)