Embed Size (px)
Citation preview

Journal of Medical Genetics 1988, 25, 819-826
Reproductive behaviour and consistent patterns ofabnormality in offspring of Vietnam veteransBARBARA FIELD AND CHARLES KERRFrom the Departments of Paediatrics (Westmead Centre) and Preventive and Social Medicine, University ofSydney, New South Wales, Australia.
SUMMARY In view of the persistent claim of Australian Vietnam veterans that their health andthat of their children were adversely affected, aspects of reproductive behaviour and thedistribution of disease and disability in family units were investigated in a sample of Tasmanianveterans and another group chosen for comparison of selected characteristics. One third ofveterans reported serious health problems and their reproductive behaviour differed with moremarital breakdowns, increased use of reproductive alternatives, and more complications ofpregnancy. Patterns of malformation and disease among veterans' children involvedpredominantly the central nervous, skeletal, and cardiovascular systems. A similar pattern wasdetected on review of the three other major investigations on veterans' offspring in the USA andAustralia. Although plausible mechanisms remain unknown, the evidence from all availablestudies supports a causal contribution to defects in veterans' children from a paternally mediatedgenetic effect.
Vietnam veterans have claimed consistently that warservice produced adverse effects on their health.Symptoms they describe closely resemble thoseobserved in veterans of the first and second worldwars which are usually categorised as 'post-stressneurosis'. However, Vietnam veterans are unique inclaiming that war service affected their reproductivepatterns and health of their offspring. Such consequ-ences have been ascribed to the use in Vietnam ofthe defoliant, Agent Orange. However, no definiteassociation has been detected between exposure ofmilitary personnel and increase in congenital mal-formations among their offspring. 1 Majorepidemiological investigations on the reproductiveoutcome of Vietnam veterans exposed to AgentOrange have been the US Air Force Ranch HandProject (Ranch Hand2),2 the Centre for DiseaseControl Study (CDC), and the Australian Govern-ment's Veterans Study (AVS).4 Yet doubts remainabout the negative conclusions of these retrospec-tive studies and there are additional uncertaintiesabout the existence of male transmission of chemi-cally induced fetal detriment. We agree with Hatchand Stein5 that epidemiological methods havereached the limits of resolving any consequences ofdefoliant exposure on reproductive events. Never-
Received for publication 20 August 1987.Revised version accepted for publication 7 March 1988.
819
theless, claims persist that veterans experiencedserious reproductive problems. In Australia, thematter has not been clarified by a Royal Commis-sion which rejected any association between Viet-nam service and birth abnormalities and whosetreatment of scientific evidence has been criticised.6We have examined two aspects which have not
been previously addressed: the reproductive be-haviour of Vietnam veterans and the patterns ofdisease and disability among their children.
Material and methods
We did not consider that a formal case control studyof parents and children would provide sufficientinformation to address our research objectives.Accordingly we constructed an analytical approachcentred on family structure and interactions. Thestudy was based on information provided by familiesliving in Tasmania, an island state to the south of theAustralian mainland, with an area of 68 300 km2and a population of 390 000 in 1977.A total of 1395 Tasmanian servicemen was offi-
cially listed as having served in Vietnam between1965 and 1972; 705 men were conscripts and 690served in the regular army. The majority werestationed at Nui Dat in Phuoc Toy Province. Theterm of duty was up to 12 months for conscripts andlonger for some regular army personnel.
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from

Barbara Field and Charles Kerr
Veterans were asked to nominate for comparativepurposes a family living in the same suburb or area
with a father of similar age to the veteran andcontaining children. This sample was required toidentify any significant discrepancies in demo-graphic, social, reproductive, and general healthvariables between the families of veterans and thoseof similarly aged men with children who lived in thesame locality. Such descriptive data are not avail-able in Australia, and although it was recognisedthat the method of selecting a comparison group
may introduce a sample bias, this risk was minimisedby the wide range of variables being investigatedand the veteran being informed only in generalterms about a study into 'family health' until he hadnominated a comparison family. Interviews with 281comparison families were completed. Some couldnot be contacted, others declined to provide in-formation. Some veterans did not know of a familywhich met the requirements and others did not wishto nominate one.A questionnaire covering 22 aspects of reproduc-
tion and child health was completed on veteran andcomparison families by telephone interview. Addi-tional information was obtained on veterans' serviceexperience in Vietnam, family history of disease,and the fathers' exposure to chemicals in civilianlife.
All major medical problems and stillbirths inchildren were confirmed or clarified by the attend-ing physician. Samples of veterans and members ofcomparison families were examined to determinewhether each group was similar in basic characteris-tics.
Analysis of the type of health problems inveterans' children was then carried out. Interactionsbetween parental characteristics and reproductivebehaviour and the patterns of disease amongoffspring were analysed by assessing the number offamilies reporting an adverse outcome, the totalnumber of children, and the first born children.Parental characteristics were examined in 47 fami-lies which contained 53 children who had died or
who were surviving with a major illness or malig-nancy.
Results
A total of 436 veterans was located by telephone.Twenty-three did not wish to participate, 18 hadcompleted their families before service in Vietnam,38 had not had children, and 357 conceived one or
more children since completion of service, a total of832 children.
Thirteen of these families had one or more
children born before service, a total of 52 children.
There were 281 families in the comparison groupand they contained 726 children, 11 born before1965. There was no difference between the Vietnamveteran and comparison groups (table 1) in thefollowing respects: fathers' and mothers' ages andsocial class, parental age at marriage or at the birthof the first child, use of contraception, difficulty inconceiving, or the number of families reporting oneor more miscarriages. Nor were differences detectedin the average number of children per family, themale/female ratio, and birth weight below 2500 g ofliving children. However, the comparison familiesreported more occupational exposure to chemicals(p<001) and a greater but less significant frequencyof disease among relatives other than parents andoffspring (OO5>p>0.01).The veterans' families reported more health
problems in both father and mother, more maritalbreakdown and use of reproductive alternatives(adoption, AID, and IVF, not significant), andmore frequent complications of pregnancy(p<0-01). The veterans' reproductive outcome con-
TABLE 1 Comparison ofcharacteristics of veteran andnon-veteran groups
Parents Veteran Non-veteran(n=357) (n=281)
Father's age 37-3 37 NSMother's age 34-6 34-62 NSFather's age at marriage 24-1 23-8 NSMother's age at marriage 21.4 21.4 NSFather's age at birth
of first child 26-5 26-0 NSMother's age at birth
of first child 23-7 23-6 NSUse of contraception 280 225 NSDifficulty conceiving 89 43 NSMiscarriages 103 74 NSAverage number of children 2-5 2-9 NSFather's health problems 123 12 <0-01Mother's health problems 18 2 <0-01Marital breakdown 32 6 <0-01Reproductive alternatives 5 1 NSOccupational exposure to
chemicals 61 64 <0-01Family history of disease 63 66 <0-05Complications of pregnancy 141 46 <0-01
Children Veteran Non-veteran(832 cases) (726 cases)
Fetal loss Definite 199 108 <0-01Suspected 26 8
Adopted 17 2 NS(12 families) (1 family)
Birth weight <2500 g 48 27 NS37 Not known 13 Not known
Deaths 33 11 <0-01Major disease 39 3 <0-01Malignancy 4 0 NSMinor abnormality 137 41 <0-01Health problems 308 145 <0-01Learning problems 83 20 <0-01Behaviour problems 65 12 <0-01Sensory and other problems 66 37 <0-01
820
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from

Reproductive behaviour and consistent patterns of abnormality in offspring of Vietnam veterans
tained a greater fetal loss, more stillbirths andneonatal, infant, and child deaths, and more chil-dren with major and minor abnormalities, tumours,
TABLE 2 Deaths and major health problems in childrenof Vietnam veterans.
Gestation Sex Year ofdeath
StillbirthsIntrauterine deathIntrauterine deathHydrocephalus, Down's syndromeIntrauterine deathHydrocephalusCerebral teratomaIntrauterine deathIntrauterine deathIntrauterine deathIntrauterine deathIntrauterine death
Neonatal deathsCerebral haemorrhageSpina bifida, omphalocelePrematurity, hydropsPrematurityPrematurity, septicaemiaPrematurity, hyaline membrane
disease, intraventricularhaemorrhage
Hydrocephalus, cleft palate, fusedcervical vertebrae
Cervical meningomyeloceleCongenital heart disease, joint
deformitiesCongenital heart disease, joint
deformitiesCongenital heart disease, joint
deformities, cataractCerebrocostomandibular syndrome
Infant deathsCot deathCongenital heart disease, scoliosisDown's syndrome, congenital heart
disease, renal hypoplasiaDown's syndrome, congenital heart
disease
Child deathsAnoxic brain damageAnoxic brain damageMultiple cranial and vertebral
malformations, epilepsyWerdnig-Hoffmann syndromeDegenerative neurological diseaseDrowning
Surviving children
Central nervous systemMeningomyelocele, hydrocephalusCerebral arteriovenous
malformationPorencephalic cystDegenerative neurological diseaseThalamic tumour
SkeletalShort femur, absent fibulaAmputation deformity of fingersScoliosis (progressive)
OtherMosaic Down's syndromeDiabetes
34 wk31 wk41 wk22 wk40 wk40 wk26 wk32 wk39 wk26 wk40 wk
FFFFFF
IndeterminateFM
M
M
I d M
1 h Indeterminate15 h F2 h F4 d M
1 d
I hId
4d
3d
14 d3 wk
2 mth3 mth
4 mth
6 mth
20 mth7y
5y1Iy8y5y
*, t, t refer to sibs identified in three families.
1970197019711971197219721973
chronic health problems, and learning, behavioural,sensory, and other relatively minor problems(p<001). Details are given in tables 2 and 3. Healthproblems of children from the non-veteran compan-son group are listed in tables 4 and 5.The average age of the 357 veterans with children
was 37-3 years at the time of interview. The averageage of their wives was 34*6 years. Only 53 of theveterans were less than 20 years old on embarkation
TABLE 3 Relatively minor health problems in children ofVietnam veterans.
Sex
1973 Neurological1973 Epilepsy1973 Epilepsy, cerebral palsy1974 Epilepsy, short stature
Epilepsy, hyperactivity
1970 Clonus hyperreflexia, hyperactivity1971 Ataxia, 6th nerve palsy1972 Megalencephaly, learning problems1973 Muscular hypotonia1974 Facial palsy
M 1974
M 1977M 1980
Ft 1975
Ft 1977
Ft 1984M 1983
M 1979F 1973
M 1970
F 1970
F* 1972F 1972
Ft 1970Mt 1974Ft 1971M 1971
Date ofbirth
3M, IFM
M
M
F
M
M
M
M
2F
M
M
M
M
F
2F
10M, 14F
iF, 1MM
F
10M, 8F
SkeletalSpina bifida occulta, ureteric refluxDeformity of chest wall and ribsPigeon chestOsgood-Schlatter diseaseScheuermann diseaseSacral dimpleHypoplastic jawPalatal hypoplasiaTalipes
CardiacPatent ductus arteriosusPulmonary stenosisMitral valve prolapseBenign cardiac murmur
SkinHaemangioma
Mid-frontalUpper lipAnus
Strawberry haemangiomaFaceArm
Vascular hamartomaMultiple pigmented naeviFacial pigmentationIchthyosisGiant hairy naevus
Lipoblastoma
F 1973 Other
Hemia
F 1972 Single inguinalF 1971 Bilateral inguinalFt 1979 UmbilicalM 1975 Umbilical and inguinal
Hydrocele, undescended testesHeterochromia iridis
M 1979 Enamel dysplasiaF 1975 Breast deformityF 1969 Anus malformation
Darwinian tuberclesCataracts
F 1975 Colour blindnessF 1976 Strabismus
Ear deformity
M
FM
FM
M
2M, IF2FM
FF
15M. IOF5M, IFIM, 3F2M12MM
M
FM
2MM
4M15M, 9F2M
821
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from
Barbara Field and Charles Kerr
for Vietnam. Ninety were regular soldiers and 28served for more than 12 months. The majority werein Vietnam for less than one year. Two hundred andfour men had duties in jungle areas, 130 were solelyin administrative posts, and 23 had served in bothsituations.A total of 214 was based solely in Nui Dat (jungle
base), 63 were in Saigon or Vung Tau (urban ornon-jungle areas), and the remaining 80 served inboth situations. Fifty-three men were privates, 227
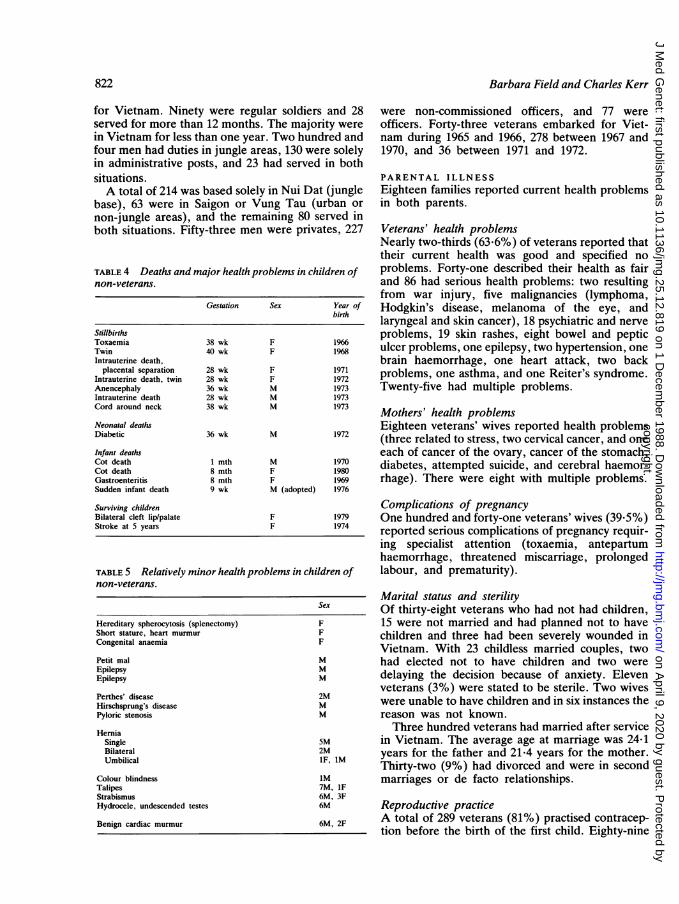
TABLE 4 Deaths and major health problems in children ofnon-veterans.
Gestation Sex Year ofbirth
StillbirthsToxaemia 38 wk F 1966Twin 40 wk F 1968Intrauterine death,
placental separation 28 wk F 1971Intrauterine death, twin 28 wk F 1972Anencephaly 36 wk M 1973Intrauterine death 28 wk M 1973Cord around neck 38 wk M 1973
Neonatal deathsDiabetic 36 wk M 1972
Infant deathsCot death 1 mth M 1970Cot death 8 mth F 1980Gastroenteritis 8 mth F 1969Sudden infant death 9 wk M (adopted) 1976
Surviving childrenBilateral cleft lip/palate F 1979Stroke at 5 years F 1974
TABLE 5 Relatively minor health problems in children ofnon-veterans.
Hereditary spherocytosis (splenectomy)Short stature, heart murmur
Congenital anaemia
Petit malEpilepsyEpilepsy
Perthes' diseaseHirschsprung's diseasePyloric stenosis
HerniaSingleBilateralUmbilical
Colour blindnessTalipesStrabismusHydrocele, undescended testes
Benign cardiac murmur
were non-commissioned officers, and 77 wereofficers. Forty-three veterans embarked for Viet-nam during 1965 and 1966, 278 between 1967 and1970, and 36 between 1971 and 1972.
PARENTAL ILLNESSEighteen families reported current health problemsin both parents.
Veterans' health problemsNearly two-thirds (63.6%) of veterans reported thattheir current health was good and specified noproblems. Forty-one described their health as fairand 86 had serious health problems: two resultingfrom war injury, five malignancies (lymphoma,Hodgkin's disease, melanoma of the eye, andlaryngeal and skin cancer), 18 psychiatric and nerveproblems, 19 skin rashes, eight bowel and pepticulcer problems, one epilepsy, two hypertension, onebrain haemorrhage, one heart attack, two backproblems, one asthma, and one Reiter's syndrome.Twenty-five had multiple problems.
Mothers' health problemsEighteen veterans' wives reported health problems(three related to stress, two cervical cancer, and oneeach of cancer of the ovary, cancer of the stomach,diabetes, attempted suicide, and cerebral haemor-rhage). There were eight with multiple problems.
Complications of pregnancyOne hundred and forty-one veterans' wives (39.5%)reported serious complications of pregnancy requir-ing specialist attention (toxaemia, antepartumhaemorrhage, threatened miscarriage, prolongedlabour, and prematurity).
Marital status and sterilitySex Of thirty-eight veterans who had not had children,F 15 were not married and had planned not to haveF children and three had been severely wounded inF
Vietnam. With 23 childless married couples, twoM had elected not to have children and two wereMM delaying the decision because of anxiety. Eleven
veterans (3%) were stated to be sterile. Two wivesM were unable to have children and in six instances theM reason was not known.
Three hundred veterans had married after serviceSM in Vietnam. The average age at marriage was 24-12M years for the father and 21-4 years for the mother.iF, IM Thirty-two (9%) had divorced and were in secondiM marriages or de facto relationships.7M, IF6M, 3F6M Reproductive practice6M, 2F A total of 289 veterans (81%) practised contracep-
tion before the birth of the first child. Eighty-nine
822
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from

Reproductive behaviour and consistent patterns ofabnormality in offspring of Vietnam veterans
(25%) reported difficulty in conceiving. There were19 adopted children in 12 families; three pregnancieswere achieved by AID and two by IVF.One hundred and three (30%) families reported
one or more miscarriages, three reported oneectopic pregnancy, and one a hydatidiform mole.The total number of miscarriages reported was 195definite and 26 suspected, that is, 21-3% of concep-tions resulted in fetal loss before 20 weeks.One hundred and seventy-five men had their first
child within three years of return from service. Theaverage age of the father at the birth of the first childwas 26-5 years and of the mother 23*7 years. Naturalchildren per family averaged 2-5, but for veteransparticipating in the study the average was 2-1.
CHARACTERISTICS OF VETERANS' CHILDREN
General featuresYears of birth ranged from 1966 to 1984 with a peakin 1974. Sixty percent of children were born between1972 and 1977. The total male/female ratio was1:1*02 (for first births it was 1-03:1). A birth weightless than 2500 g was recorded in 48 survivingchildren but was not known for an additional 37, 13of whom were premature and died.
Nearly half (46%) of veterans' children were
reported as having no health problems or learning orbehavioural difficulties.
Child mortality and health problems in survivingchildrenThree of 52 children born before the father's servicein Vietnam had died during the neonatal period(two because of prematurity, one with interstitialpneumonitis). One surviving female was physicallyhandicapped because of birth trauma.
Thirty-three (4%) of 832 children born after thefather's service in Vietnam had died. Causes ofdeath and other details are shown in table 2.Eleven offspring were stillborn, 12 died within
one month, and 10 between two months and eightyears. The sex ratio was 17 females: 14 males andtwo were of indeterminate sex.
Prematurity was associated with death in 10instances. An abnormality of the central nervoussystem was recorded in 16 cases. The skeleton andheart were affected in 10 instances. One death wasthe result of drowning and another was recorded ascot death.Reported health problems have been divided
arbitrarily into major (life threatening or seriouslydisabling) in table 2 and relatively minor in table 3.
Five children had major central nervous system
TABLE 6 Interaction between parental characteristics, reproduction, and children's health status.
Paternal Maternal Father Regular National Years Site Jungle Lowest Yearill ill <20 y army service of of duty rank embark-health health entry service service ation
Vietnam
Parental characteristicsMiscarriage - - - t -Problems conceiving - - - - - - - - -Pregnancy complication tContraception - §Stillbirths - - t - - - - - -Major disease - - t - - - tMalignancies -
Total: Stillbirths - - t - - - -Major diseaseMalignancies
Birth weight <2500 g - - tMinor malformations 1 t -- - - -
2 t3 _
Health problems 1 t2 t3 t
Behavioural problems 1 t t2 t t3 t t
Learning problems 1 - - - - - -
2 t3 _
Sensory problems 123
*p<O- 1.tp<001.tp<0-02.§p<0-05.
1 No of families.2 Total children.3 First child born after Vietnam.
823
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from

Barbara Field and Charles Kerr
disease and seven were reported to have epilepsy ofsufficient severity to warrant anticonvulsant ther-apy. Three children had a major skeletal deformityand there were 57 instances of minor abnormalitiesranging from spina bifida occulta to flexion de-formity of the toe. Of 13 dermatological conditions,six were of vascular origin. Of four tumours, threewere of embryonic cell origin (cerebral teratoma,vascular hamartoma, and a recurrent lipoblas-toma).There were 10 instances of congenital heart
disease of which six proved fatal. They wereatrioventricular canal defects (two), truncus arter-iosus plus an aortic valve defect, coarctation of theaorta, and ventricular septal defect with patentductus. Of the four who survived, two had patentductus and one each pulmonary valve stenosis andmitral valve prolapse.Four instances of chromosomal defect were iden-
tified: two with trisomy 21, a ring C chromosome(all dead), and one female surviving with mosaictrisomy 21. One stillborn male with hydrocephaluswas said to resemble trisomy 21.Three hundred and eight children (37%) were
reported to have continuing health problems.Learning difficulties were frequent (83 children) aswere behavioural and emotional problems (65 chil-dren).A number of families had multiple problems. For
example, in one family the parents had a stillbornfemale and female twins who both died after anoxicbrain damage at birth. In another family, threefemales died respectively at three, four, and 14 dayswith skeletal and cardiac malformations. One veter-an had a daughter with multiple malformations,epilepsy, and mental retardation who died aged fiveand a son from another marriage who died at 20months with central nervous system disease des-cribed as Werdnig-Hoffmann syndrome. Both hiswives had experienced multiple miscarriages.
INTERACTIONS BETWEEN PARENTALCHARACTERISTICS, REPRODUCTION, AND
CHILDREN S HEALTH STATUSParental health problems correlated with reproduc-tive and child health problems (table 6) and moststrongly with minor malformations, health, be-havioural, and learning problems in children, andalso with problems in conceiving and complicationsof pregnancy. Cross correlations existed betweenpaternal ill health and maternal ill health, jungleduties in Vietnam, and regular army status. Thelatter status, as opposed to being conscripted fornational service, correlated with miscarriages infamilies and with major disease among offspring.Other associations are recorded in table 6.
DiscussionThere is no dispute that the Vietnam war and thepublic response in Western countries which suppliedarmed forces were profoundly disturbing for someveterans. Relatively larger burdens of ill health werereported by Tasmanian veterans, their wives, andoffspring than a comparison group with similardemographic and social characteristics. It is notclear how representative the Tasmanian group wereof all Australian Vietnam veterans. There seemslittle likelihood that the sample was biased towardsover-ascertainment of those with personal or fami-lial health problems because the veterans wereselected from an official alphabetical list and not ongrounds of ill health, concern about children, ormembership of the Australian Vietnam Veterans'Association. On the other hand, the mode ofselection, via telephone to those with a fixedresidence, may have given some selective preferenceto those with a relatively greater socioeconomic anddomestic stability.
This selection mode applied also to the compari-son group who were unlikely to have had a biaseddistribution of problems although relatively minorabnormalities may have been under-representedowing to lower anxiety levels among the group.More than one-third of veterans in this study
reported that they had a serious health problem.Origins of this load remain unclear but to someextent may reflect the adverse consequences ofVietnam service or some exposure to specificharmful agents. Whatever the causes, health prob-lems of veterans affected the lifestyle, coping, andparenting skills in some families and indirectlycontributed to illness or problems in children.
Reproductive practice was modified in severalways. Some men did not marry and reproduce eitherby choice or because of ill health or anxiety andstress and the publicity surrounding them. Somechose to adopt children or use alternative methodssuch as AID or IVF.
Others married immediately on return and begantheir families against a background of high riskfactors for perinatal loss, with superimposed factorsof combat stress, health and psychiatric problems,and socioeconomic difficulties. Marital breakdownwas frequent.
Nearly half the men in this study had their firstchild within three years of return from Vietnam,although contraception was generally used beforethe first child was conceived. Sterility in the male,difficulty in conceiving, and miscarriage withinfamilies did not differ from non-veteran or Austra-lian population rates. There was, however, a higherproportion of conceptions which resulted in fetalloss before 20 weeks.
824
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from
Reproductive behaviour and consistent patterns ofabnormality in offspring of Vietnam veterans
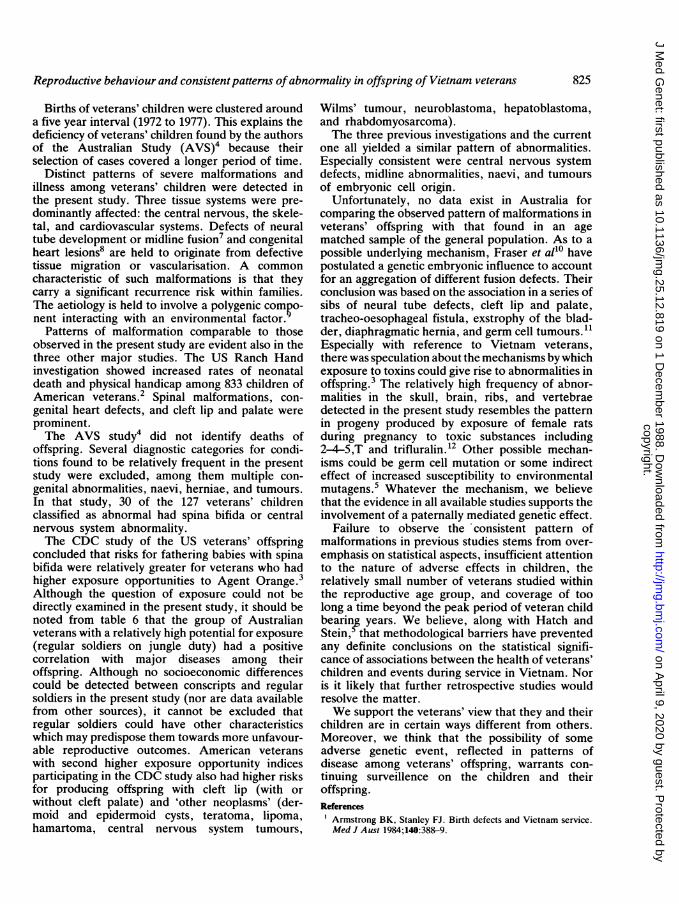
Births of veterans' children were clustered arounda five year interval (1972 to 1977). This explains thedeficiency of veterans' children found by the authorsof the Australian Study (AVS)4 because theirselection of cases covered a longer period of time.
Distinct patterns of severe malformations andillness among veterans' children were detected inthe present study. Three tissue systems were pre-dominantly affected: the central nervous, the skele-tal, and cardiovascular systems. Defects of neuraltube development or midline fusion7 and congenitalheart lesions8 are held to originate from defectivetissue migration or vascularisation. A commoncharacteristic of such malformations is that theycarry a significant recurrence risk within families.The aetiology is held to involve a polygenic compo-nent interacting with an environmental factor.
Patterns of malformation comparable to thoseobserved in the present study are evident also in thethree other major studies. The US Ranch Handinvestigation showed increased rates of neonataldeath and physical handicap among 833 children ofAmerican veterans.2 Spinal malformations, con-genital heart defects, and cleft lip and palate wereprominent.The AVS study4 did not identify deaths of
offspring. Several diagnostic categories for condi-tions found to be relatively frequent in the presentstudy were excluded, among them multiple con-genital abnormalities, naevi, herniae, and tumours.In that study, 30 of the 127 veterans' childrenclassified as abnormal had spina bifida or centralnervous system abnormality.The CDC study of the US veterans' offspring
concluded that risks for fathering babies with spinabifida were relatively greater for veterans who hadhigher exposure opportunities to Agent Orange.3Although the question of exposure could not bedirectly examined in the present study, it should benoted from table 6 that the group of Australianveterans with a relatively high potential for exposure(regular soldiers on jungle duty) had a positivecorrelation with major diseases among theiroffspring. Although no socioeconomic differencescould be detected between conscripts and regularsoldiers in the present study (nor are data availablefrom other sources), it cannot be excluded thatregular soldiers could have other characteristicswhich may predispose them towards more unfavour-able reproductive outcomes. American veteranswith second higher exposure opportunity indicesparticipating in the CDC study also had higher risksfor producing offspring with cleft lip (with orwithout cleft palate) and 'other neoplasms' (der-moid and epidermoid cysts, teratoma, lipoma,hamartoma, central nervous system tumours,
Wilms' tumour, neuroblastoma, hepatoblastoma,and rhabdomyosarcoma).The three previous investigations and the current
one all yielded a similar pattern of abnormalities.Especially consistent were central nervous systemdefects, midline abnormalities, naevi, and tumoursof embryonic cell origin.
Unfortunately, no data exist in Australia forcomparing the observed pattern of malformations inveterans' offspring with that found in an agematched sample of the general population. As to apossible underlying mechanism, Fraser et allo havepostulated a genetic embryonic influence to accountfor an aggregation of different fusion defects. Theirconclusion was based on the association in a series ofsibs of neural tube defects, cleft lip and palate,tracheo-oesophageal fistula, exstrophy of the blad-der, diaphragmatic hernia, and germ cell tumours.11Especially with reference to Vietnam veterans,there was speculation about the mechanisms by whichexposure to toxins could give rise to abnormalities inoffspring.3 The relatively high frequency of abnor-malities in the skull, brain, ribs, and vertebraedetected in the present study resembles the patternin progeny produced by exposure of female ratsduring pregnancy to toxic substances including2-4-5,T and trifluralin.12 Other possible mechan-isms could be germ cell mutation or some indirecteffect of increased susceptibility to environmentalmutagens.5 Whatever the mechanism, we believethat the evidence in all available studies supports theinvolvement of a paternally mediated genetic effect.
Failure to observe the consistent pattern ofmalformations in previous studies stems from over-emphasis on statistical aspects, insufficient attentionto the nature of adverse effects in children, therelatively small number of veterans studied withinthe reproductive age group, and coverage of toolong a time beyond the peak period of veteran childbearin,g years. We believe, along with Hatch andStein, that methodological barriers have preventedany definite conclusions on the statistical signifi-cance of associations between the health of veterans'children and events during service in Vietnam. Noris it likely that further retrospective studies wouldresolve the matter.We support the veterans' view that they and their
children are in certain ways different from others.Moreover, we think that the possibility of someadverse genetic event, reflected in patterns ofdisease among veterans' offspring, warrants con-tinuing surveillence on the children and theiroffspring.References
Armstrong BK, Stanley FJ. Birth defects and Vietnam service.Med J Aust 1984;140:388-9.
825
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from

Barbara Field and Charles Kerr
2 Lathrop GD, Wolfe WH, Albanese RA, Moynahan PM.Project Ranch Hand 11. An epidemiologic investigation of healtheffects in Air Force personnel following exposure to herbicides.San Antonio, Texas: Aerospace Medical Division, 1984.Erickson JD, Mulinarei J, McClain PW, et al. Vietnam veterans'risks for fathering babies with birth defects. JAMA1984;252:903-12.
4 Donovan JW, Adena MA, Rose G, Batistutta D. Case controlstudy of congenital anomalies and Vietnam service. Canberra:Australian Government Publishing Services, 1983.Hatch MC, Stein ZA. Agent Orange and risks to reproduction.The limits of epidemiology. Teratogenesis Carcinog Mutagen1986;6:185-202.
6 Humphrey GF. Scientists and Royal Commissions. Search1986;17:63-4.
7Opitz J, Gilbert EF. CNS anomalies and the midline as adevelopmental field. Am J Med Genet 1982;12:443-55.
8Clark E. Mechanisms in the pathogenesis of congenital heartdefects. Proc Greenwood Genetic Center 1985;4:80.
Carter CO. Multifactorial inheritance revisited. Proceedings ofthe Third International Conference on Congenital Malforma-tions, The Hague, Netherlands, 1969. New York: ExcerptaMedica Foundation, 1970: 227-32.
'° Fraser FC, Czeizel A, Hanson C. Increased frequency of neuraltube defects in sibs of children with other malformations. Lancet1982;ii: 144-5.Birch M. Anencephaly in stillborn sibs of children with germ celltumours. Lancet 1980;i:1257.
12 Beck SC. Assessment of adult skeletons to detect prenatalexposure to 2-4-5,T or trifluralin in mice. Teratology1981 ;23:33-55.
Correspondence and requests for reprints to Profes-sor C B Kerr, Department of Public Health,University of Sydney, Sydney, NSW 2006, Austra-lia.
826
copyright. on A
pril 9, 2020 by guest. Protected by
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.25.12.819 on 1 D
ecember 1988. D
ownloaded from





























