Embed Size (px)
Citation preview

Cases in Urological OncologyCases in Urological Oncology
Dr Manish Patel Dr Manish Patel MB.BS., MMed., FRACS, PhDMB.BS., MMed., FRACS, PhD
Urological Cancer SurgeonUrological Cancer Surgeon Westmead Public and Private HospitalWestmead Public and Private HospitalSenior Lecturer, University of SydneySenior Lecturer, University of Sydney
A Case of Bladder CancerA Case of Bladder Cancer
• Mr K.S. 63 year old man.
• Heavy smoker in the past.
• Father had bladder cancer
• Asymptomatic
Bladder Cancer Screening• Risk Factors for Bladder Cancer
– Smoking– Age– Radiation exposure– Previous urothelial carcinoma– Analgesics– Cyclophosphamide

Has Haematuria Screening Been Useful?• Only one good long term study
• Not randomised
• Men over age 50 years
• Daily home dipstick test for a week
• 16.4% of the population had haematuria investigated.
• 8.1% with haematuria had BC
• At 14 years no man with screen detected BC died.
• 20% of non screen detected BC had died

What Causes Haematuria?
• Upper Urinary Tract• Renal Cell Carcinoma• Urothelial cancer• Urolithiasis• Glomerular causes• Nephritis• AV Malformation• Renal infarction• Renal vein thrombosis• Polycystic kidneys
• Lower Urinary Tract• Urothelial cancer• Cystitis• BPH• Bladder stones• Prostate cancer• Prostatitis• Trauma• TB• Anticoagulation
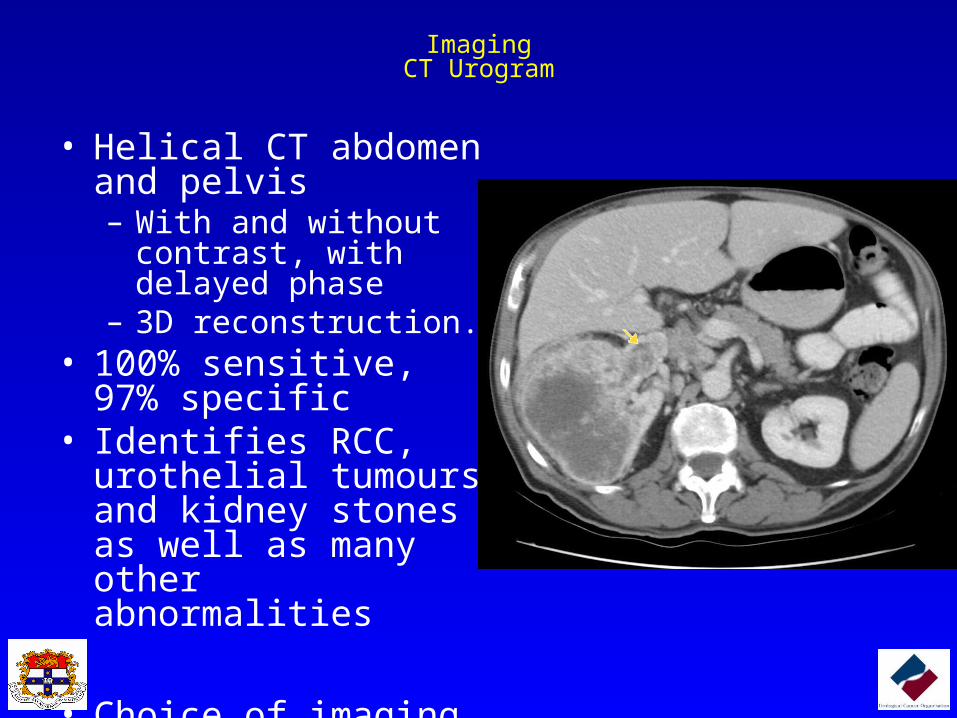
ImagingCT Urogram
• Helical CT abdomen and pelvis– With and without contrast,
with delayed phase– 3D reconstruction.
• 100% sensitive, 97% specific
• Identifies RCC, urothelial tumours and kidney stones as well as many other abnormalities
• Choice of imaging techniques

ImagingUrinary Tract Ultrasound
• Cheap, quick, non-invasive, no contrast
• Sensitivity 60-70%, specificity 90%
• Still inferior to CT.

ImagingIVP
• Intravenous contrast and tomograms
• Sensitivity 61%, specificifty 92%
• Expensive and time consuming
• Misses small renal lesions – need US as well

MacroscopicHaematuria
MicroscopicHaematuria
High Risk Low Risk
Exclude UTI (MSU)Urine cytology X3
Exclude UTI (MSU)Urine cytology X3
Upper Tract Imaging:CT Urogram orIVP + US
Upper Tract Imaging:US only.
Lower Tract Investigation:Cystoscopy (Flexible or Rigid)
Lower Tract Investigation:Cystoscopy (Flexible)
Dysmorphic cells onmicroscopy
NephrologistEvaluation
Algorithm for evaluation

Case
• Mr KS has
• Normal CT IVP
• Urine cytology: suspicious for malignancy
• Has cystoscopy

Cystoscopy
High Grade Urothelial Carcinoma Carcinoma in-situLamina Propria Invasion

Staging of Bladder CancerStaging of Bladder Cancer
Invasive
TisSuperficial
Superficially Invasive
CIS
T2
T3

What Next?• BCG treatment for 6 weeks- intravesically
– Eradicated CIS (70%)– Decreased recurrence and progression.
• Follow-up cystoscopy every 3 months for 2 years.

9 months later
• Muscle Invasive
• Staging CT, Bone scan normal.

A Case of Bladder CancerA Case of Bladder Cancer
Underwent:
Nerve-sparing cystoprostatectomy with neobladder formation and extended lymph node dissection.
• Continent at 6 weeks.• Erections at 5 months.• Voids normally with a
little straining.
Pouch
Ureters
Urethra
A Case of Bladder CancerA Case of Bladder Cancer Considerations in FollowUp
• Cancer Recurrence:– Regular urine cytology, CT scans abdomen and chest.
• Metabolic complications– Hypochloraemic hypokalaemic metabolic acidosis.
• Vitamin B12 and bile acids
• Urolithiasis
• Pyelonephritis
• Preservation of upper tracts.
• Potency
A Case of Prostate Cancer
• Mr J.B. 57 year old.
• Mild LUTS
• Hypertension
• Asks his G.P. for a test for prostate cancer?
• What should the G.P discuss with him?

2 New Randomised trails of screening
PLCO trial highly flawed30% were prescreened before entering the trial52% in control arm had screening85% only were screened in screening arm.

• 182,000 men aged 50-74
• Randomised to : PSA every 4 years or no screening.
• PSA cut-off 3.0ng/ml and DRE
• 16.2% tests were positive
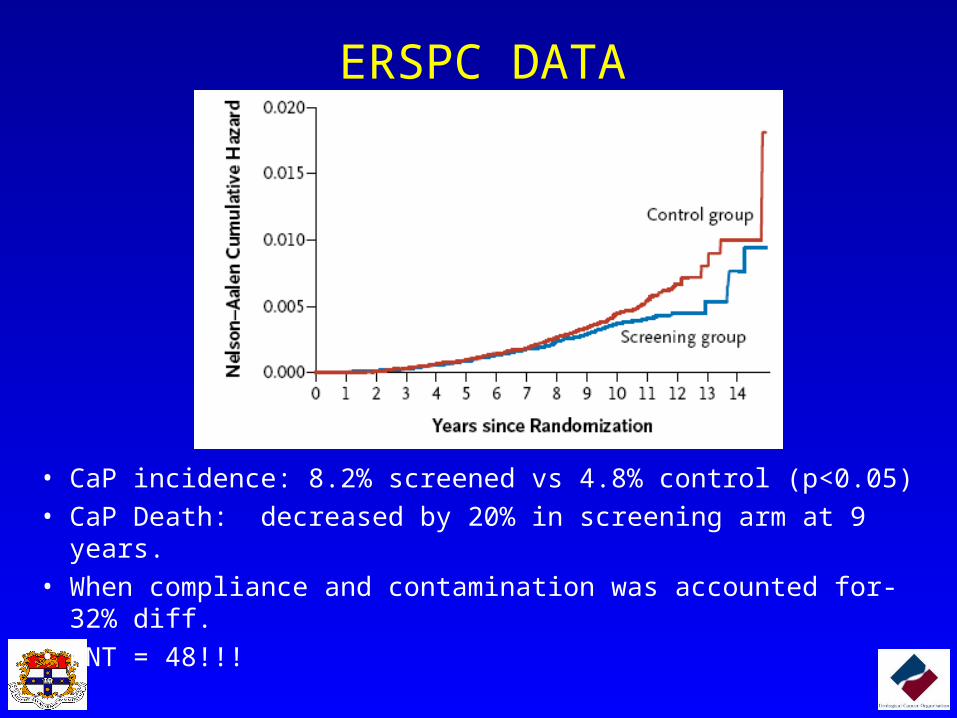
ERSPC DATA
• CaP incidence: 8.2% screened vs 4.8% control (p<0.05)
• CaP Death: decreased by 20% in screening arm at 9 years.
• When compliance and contamination was accounted for- 32% diff.
• NNT = 48!!!

• 20% reduction in death from CaP
•
Need to treat 48 men to save one.
Potential Benefits
SummaryPotential Harms
Need to discuss the individual benefits and risksof screening with all male patients 50-70years.

A Case of Prostate Cancer
PSA Test: 3.0 ng/ml, F/T 9%
Is this normal?AgeAge Median PSAMedian PSA Normal Normal
RangeRange
40-49 0.7ng/ml 0-2.5ng/ml
50-59 0.9ng/ml 0-3.5ng/ml
60-69 1.4ng/ml 0-4.5ng/ml
70+ 1.7g/ml 0-6.5ng/ml
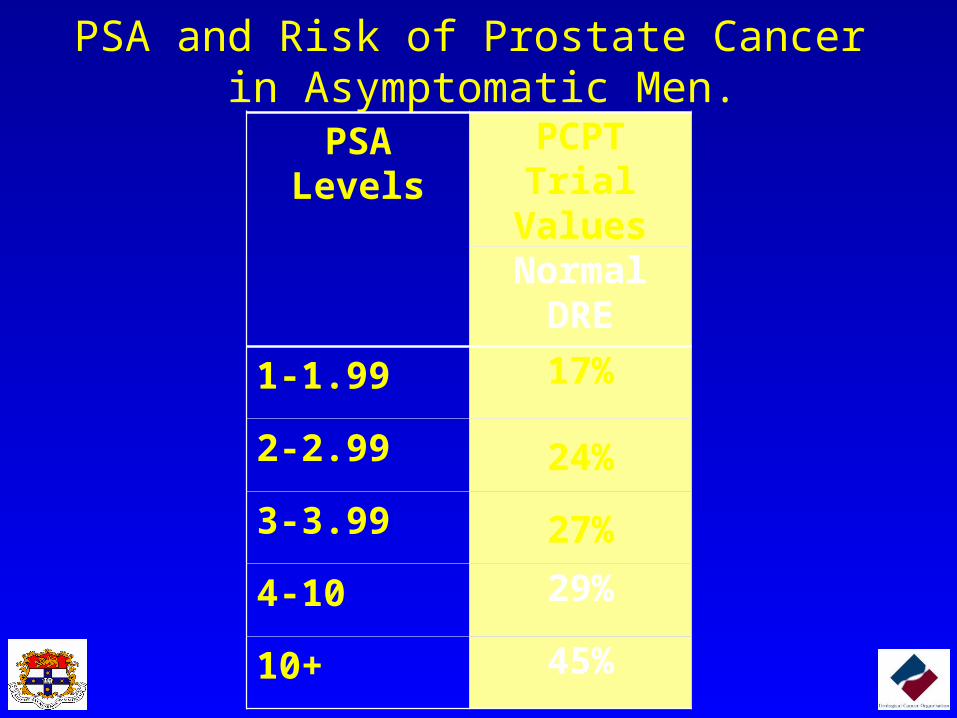
PSA and Risk of Prostate Cancer in Asymptomatic Men.
PSA Levels PCPT Trial Values
Normal DRE
1-1.99 17%
2-2.99 24%
3-3.99 27%
4-10 29%
10+ 45%
PSA Velocity• Needs to be calculated with at least 3 PSA values
– 15% variability day-day
• PSA velocity of >0.35ng/ml/year is abnormal.
• If PSA velocity is abnormal and PSA is above the median value – refer to urologist.

Free to Total (%) Does Help Specificity.
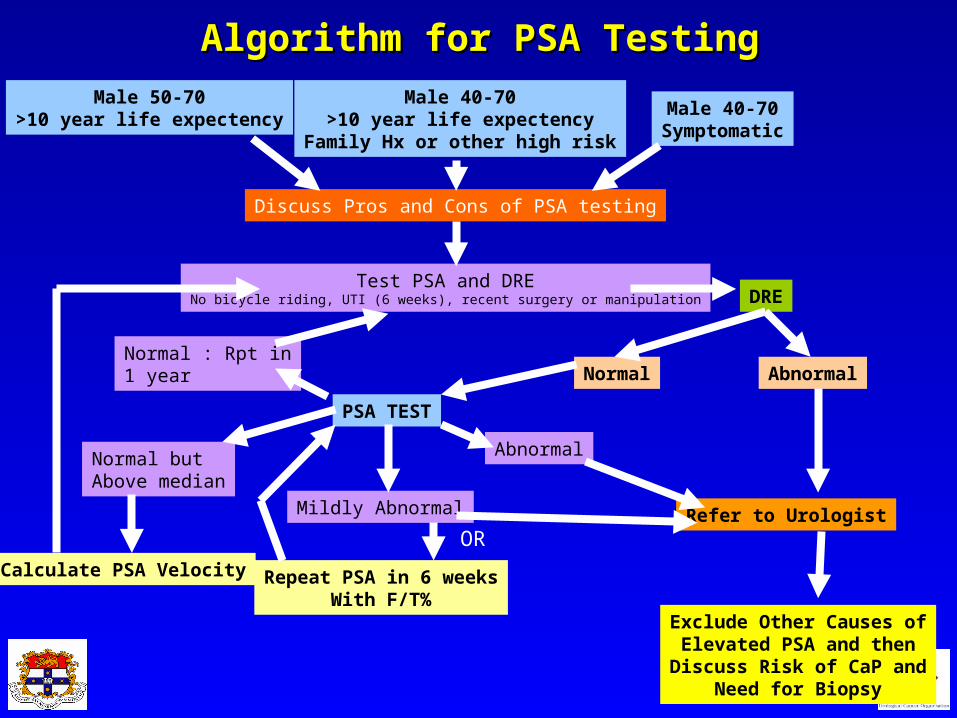
Male 50-70>10 year life expectency
Male 40-70>10 year life expectency
Family Hx or other high risk
Male 40-70Symptomatic
Discuss Pros and Cons of PSA testing
Test PSA and DRENo bicycle riding, UTI (6 weeks), recent surgery or manipulation DRE
AbnormalNormal
Refer to Urologist
Exclude Other Causes ofElevated PSA and then
Discuss Risk of CaP andNeed for Biopsy
PSA TEST
Abnormal
Mildly Abnormal
Normal but Above median
Repeat PSA in 6 weeksWith F/T%
Calculate PSA Velocity
OR
Algorithm for PSA TestingAlgorithm for PSA Testing
Normal : Rpt in1 year
A Case of Prostate Cancer• Mr J.B has an abnormal prostate exam. • He has a prostate biopsy
– 2% Lignocaine pudendal nerve block.
• Biopsy results:• Gleason Grade 3+3=6• In 6/12 cores involving 25%-50% of the cores.
• What are his options for treatment?

Treatment options for low risk CaP• Active surveillance
• Radical Prostatectomy– Open– Robotic
• Seed Brachytherapy (not HDR brachytherapy)
• External beam radiotherapy
• Experimental– HIFU– Cryothepy
A Case of Prostate CancerA Case of Prostate Cancer
• Pathology:– Adenocarcinoma, Gleason Grade 3+4– Extracapsular extension– Negative surgical margins.
• Follow-up:
• Continent @ 4weeks
• Potent @ 3 months
• No PSA recurrence at 2 years.
Questions