Embed Size (px)
Citation preview

Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Electromyography and Kinesiology
journal homepage: www.elsevier .com/locate / je lek in
Rigid and Elastic taping changes scapular kinematics and pain in subjectswith shoulder impingement syndrome; an experimental study
http://dx.doi.org/10.1016/j.jelekin.2014.07.0111050-6411/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author. Tel.: +44 1483689670.E-mail address: [email protected] (A.F. Shaheen).
1 Current affiliation.
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping changes scapular kinematics and pain in subjects with shoulder impinsyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.doi.org/10.1016/j.jelekin.2014.07.011
Aliah F. Shaheen a,b,⇑, Anthony M.J. Bull a, Caroline M. Alexander c
a Department of Bioengineering, Imperial College London, Royal School of Mines, South Kensington Campus, London SW7 2AZ, United Kingdomb Department of Mechanical Engineering Sciences, University of Surrey, Stag Hill campus, Guildford GU2 7XH, United Kingdom1
c Department of Physiotherapy, Imperial College Healthcare NHS Trust, Charing Cross Hospital, London W6 8RF, United Kingdom
a r t i c l e i n f o a b s t r a c t
Article history:Received 27 November 2013Received in revised form 14 April 2014Accepted 23 July 2014Available online xxxx
Keywords:ScapulaTapingShoulder impingementKinematicsPain
Rigid and Elastic scapular taping is used in physical rehabilitation of shoulder impingement syndrome(SIS). It is believed to reduce pain and normalise scapular movement patterns. However, there is insuffi-cient evidence to support its use.
The aim of the study was to investigate the effect of Rigid and Elastic taping techniques on the scapularkinematics and pain in patients with SIS.
Eleven patients with SIS participated in the study. They performed elevation and lowering of the arm inthe scapular and sagittal planes under three conditions: Baseline, Rigid taping and Elastic taping. Themovements of the thorax, humerus and scapula were tracked. Scapular displacements and scapulotho-racic joint rotations were calculated. Subjects used a visual analogue scale to rate the intensity of painat rest and during movements in both planes.
Both taping techniques externally rotated the scapula in sagittal plane movements (p < 0.05) andresulted in reduced pain. In the scapular plane, Elastic taping increased the scapular retraction(p < 0.05) and posterior displacement (p < 0.01), but neither of the taping techniques had an effect on painin this plane.
In conclusion, both taping techniques had an effect on scapular kinematics and pain in movementsoccurring in the sagittal plane. Elastic taping also affected scapular kinematics in scapular planemovements, but without the concomitant decrease in pain.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction
Shoulder impingement syndrome (SIS) accounts for the major-ity of reported shoulder complaints (van der Windt et al., 1996;Vecchio et al., 1995). The condition is associated with a reducedclearance of the soft tissues occupying the subacromial space asthe arm is elevated (Neer, 1972). Despite its high prevalence(Lo et al., 1990; Michener et al., 2003), the underlying aetiologyof the condition is still debated (Budoff et al., 1998; Fu et al.,1991; Jobe et al., 2000). Poor posture and abnormal scapularkinematics have been suggested as possible primary factors indeveloping SIS (Fu et al., 1991; Jobe et al., 2000) and also as second-ary observed phenomena of SIS (Kamkar et al., 1993). These pat-terns are also believed to exacerbate the condition by further
narrowing of the subacromial space (Kaya et al., 2011; Ludewigand Cook, 2000; Lukasiewicz et al., 1999).
Most of the physiotherapeutic rehabilitation programmes forSIS are designed to correct posture (Lewis et al., 2005b; Ludewigand Reynolds, 2009) and minimise the deviation of shoulder kine-matics from normality (Host, 1995; Kaya et al., 2011; Ludewig andReynolds, 2009). To this end, the application of tape is extensivelyused. Two types of tape of different elastic properties have beenused in shoulder rehabilitation; Rigid (Ackermann et al., 2002;Alexander et al., 2003; Cools et al., 2002; Host, 1995, Kalter et al.,2011; Lewis et al., 2005b, McConnell et al., 2011; Selkowitz et al.,2007; Smith et al., 2009) and Elastic taping techniques (Bradleyet al., 2009; Garcia-Muro et al., 2010; Hsu et al., 2009; Kaseand Kase, 2003; Kaya et al., 2011; Lin et al., 2011; Thelen et al.,2008).
The underlying mechanism of taping is also poorly understood.A number of hypotheses have been put forward to explain theeffects of taping; it has been suggested that taping alters muscleforce (Host, 1995; Morrissey, 2000), neuromuscular control
gement

2 A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx
(Alexander et al., 2008; Lin et al., 2011; Lohrer et al., 1999) and pro-prioception (Lin et al., 2011; Morrissey, 2000). One of the otherproposed theories suggests that taping achieves its effects via abiomechanical realignment of the joints (Bennell et al., 2000;Host, 1995; Lewis et al., 2005a) and restrictions to the joint rangeof motion (Bradley et al., 2009; McConnell et al., 2011). This poorunderstanding contributes to the variations in the taping tech-niques used by different clinicians. For example many applicationtechniques have been presented in the literature for the manage-ment of SIS alone (Host, 1995; Hsu et al., 2009; Kalter et al.,2011; Kaya et al., 2011; Lewis et al., 2005b; Selkowitz et al.,2007; Smith et al., 2009; Thelen et al., 2008).
The popularity of using taping with the shoulder is not sup-ported by sufficient scientific evidence. It is generally believed thattaping helps in reducing pain and normalising scapular kinematics,however, these claims are often based on anecdotal observations.Recent systematic reviews that investigated the effect of Elastictaping on musculoskeletal conditions highlight the shortage ofsupporting evidence (Mostafavifar et al., 2012; Williams et al.,2012). The reviews included small numbers (10 and 6 respectively)of studies covering a wide range of musculoskeletal joints andmany outcome measures including pain, range of motion, proprio-ception and muscle strength. As a result, it is still not possible toprove or discount any beneficial effects of taping (Mostafavifaret al., 2012; Williams et al., 2012).
In addition, few studies have investigated the effects of tapingon kinematics despite the association of altered scapular restingposition (Borstad, 2006) and kinematics (Ludewig and Reynolds,2009) with shoulder pathology. This is in part because of the diffi-culties involved in obtaining in-vivo measurements of the scapularmovement (Hill et al., 2007; Kontaxis et al., 2009). Recently, anumber of studies have developed methods to obtain scapularkinematics in-vivo with relatively high accuracies (Brochardet al., 2011; Prinold et al., 2011; Shaheen et al., 2011a,b; Warneret al., 2012).
One of these methods (Karduna et al., 2001) was utilised by Hsuet al. (2009) who investigated the effects of an Elastic tape appliedto envelope the lower trapezius muscle on shoulder kinematicsand muscle activity in a group of baseball players with SIS. Thestudy found that taping increased posterior tilt (approximately1�) in low humeral elevations in scapular plane movements.
Shaheen et al. (2013) also utilised a scapular tracking method(Shaheen et al., 2011b) to measure subtle changes in scapular kine-matics caused by Rigid taping. In the aforementioned study, tapingwas applied bilaterally in a non-symptomatic subject group accord-ing to the method described by Lewis et al. (2005b). The studyshowed that taping increased scapular external rotation, upwardrotation and posterior tilt compared to baseline measurements(Shaheen et al., 2013). The magnitudes of these alterations (3–6�)were significantly higher than those reported by Hsu et al. (2009).
The results of previous studies point towards a positive effect oftaping on scapular kinematics; the reported alterations arebelieved to reverse the effects of SIS on scapular kinematics andcan contribute to an increase in the subacromial space (Lewiset al., 2005a; Ludewig and Cook, 2000) thus possibly resulting inpain relief. However, both studies have obtained measurementsin either pain-free subjects or a pain-free state (Hsu et al., 2009),hence it is not possible to make any conclusions regarding theassociation of these alterations with pain relief.
In addition, the magnitudes as well as some of these alterations(scapular external and upward rotations) are different in the twostudies. This may be caused by differences in the subject groups,the measurement method or the different application techniques.To date, no studies have attempted to investigate the effects ofElastic and Rigid tape applications designed to treat the samesymptoms on a single subject group.
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
The aim of this study was to investigate the effects of taping onscapular kinematics and pain in patients with SIS when two differ-ent taping techniques designed for the management of SIS areused; a Rigid tape application and an Elastic tape application.
2. Method
2.1. Participants
Subjects were included in the study if they experienced pain inelevation of the shoulder and if they tested positive to at least 4 ofthe following tests: (1) Neer impingement sign (2) Hawkins sign(3) pain during supraspinatis empty can test (4) painful arcbetween 60� and 120� and (5) tenderness when palpating thegreater tuberosity of the humerus. Subjects were excluded if theyexperienced pain with cervical spinal tests, had a history of spinalor upper-limb fractures or had systemic illnesses. Subjects who fitthese criteria and consented to participating in the study signed aconsent sheet approved by Central London REC 4.
2.2. Intervention
2.2.1. Taping techniquesTwo taping techniques commonly used for SIS were applied.
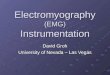
The first technique uses Rigid tape and is applied bilaterally(Lewis et al., 2005b). In the Rigid tape application, a combinationpack of zinc oxide tape and protective tapea was used. The protec-tive tape was applied first with no tension. To apply the Rigid tape,subjects placed their thoracic spine in a neutral position, the Rigidtape was applied bilaterally from the first to the twelfth thoracicvertebra (Fig. 1). Subjects were then asked to retract and depressthe scapula; this was demonstrated by the investigator. Rigid tapewas applied diagonally from the middle of the scapular spine to thetwelfth thoracic vertebra; this was also applied bilaterally.
The second taping technique used Elastic tapeb and was appliedon the symptomatic side only (Kase and Kase, 2003). Placing thearm in various positions before application of each strip, firstly, aY-strip was applied from the insertion to the origin of the supraspi-natus with no additional stretch, another Y-strip was applied fromthe insertion to the origin of the deltoid with no additional stretchand a final I-strip was applied from the coracoid process to the pos-terior deltoid with approximately 75% stretch and a downwardpressure (Fig. 1).
2.3. Outcome measures
2.3.1. Experimental setupA 10-camera motion capture systemc was used to track the tra-
jectories of reflective markers attached to the thorax, humerus andthe scapula locator (Shaheen et al., 2011b).
Subjects were asked to attend one laboratory session, the ses-sions lasted between 60 and 90 min. Subjects were seated on abackless stool with the feet at a comfortable width apart. Subjectsperformed three bilateral elevations and lowerings in the scapularand the sagittal planes at a comfortable pace; the order of planeswas randomised. During this session, movements were repeatedfor three conditions: Baseline, Rigid taping and Elastic taping. Sub-jects were allowed short breaks between conditions, the durationsof which were determined by the subjects. The markers were notremoved during these breaks.
Baseline measurements were always obtained at the start. Theorder of the Rigid and Elastic taping was randomised. Visual Ana-logue Scales (VAS) were used to assess the intensity of pain at restand during movements in the scapular and sagittal planes for thethree conditions. The scales were horizontal lines of 10 cm in
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

Fig. 1. A – Scapular Rigid taping technique applied bilaterally according to the method described by Lewis et al. (2005a,b). B – Scapular Elastic taping technique applied usingthe method described by Kase and Kase (2003).
A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx 3
length, where one end represented ‘‘No pain’’ and the other endrepresented ‘‘Maximum pain’’.
2.3.2. Scapular trackingMeasurements of the scapular movement in the symptomatic
shoulder were obtained using the method described by Shaheenet al. (2011a,b) (Shaheen et al., 2011b). The scapula locator: a tri-pod device with three pegs on the scapula acromial angle, inferiorangle and the root of the scapular spine was used to obtain thescapular measurements. An experienced observer used the scapulalocator to track the movement of the scapula during shoulderelevations and lowerings whilst keeping low pressures on the threescapular landmarks. Feedback on the pressures were displayed ona computer screen and used to ensure that that high pressures,which may influence the physiological movement of the scapulaare avoided (Shaheen et al., 2011b). The method provided a contin-uous measure of the scapular position and orientation duringmovement.
The inter-observer and intra-observer reliabilities of themethod have been assessed in previous studies (Shaheen et al.,2011a,b). The intra-observer errors of an experienced observerhave been reported to range from 1.7� to 2� for scapular internalrotation, 2.7–3� for scapular upward rotation and 1–1.5� forscapular tilt (Shaheen et al., 2011a).
2.4. Data analysis
Coordinate frames for the humerus, thorax and the scapulawere defined according to the ISB recommendations (Wu et al.,2005). Humerothoracic angles were calculated using Euler anglerotations in the sequence of x–z0–y00 abduction, flexion and axialrotation for elevations in the scapular plane and in the sequenceof z–x0–y00 flexion, abduction and axial rotation for elevations inthe sagittal plane (Kontaxis et al., 2009). Scapulothoracic rotationswere calculated in the sequence of y–x0–z00 internal rotation,upward rotation and tilt. Scapular displacements were computedusing the position of the acromial angle in the thoracic coordinateframe. Anterior displacements were measured using the displace-ment of the acromial angle in the positive direction of the x-axis
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
of the thoracic coordinate frame, scapular elevation was thedisplacement in the positive direction of the y-axis and scapularprotraction was the displacement in the positive direction of thez-axis (Hsu et al., 2009).
Two-factor repeated measures ANOVA tests were used to com-pare the measured scapulothoracic rotations and displacements.The first factor defined the testing condition: Baseline, Rigid tapingor Elastic taping and the second factor consisted of selected anglesof elevation: from 30� to 120� at 5� interval. A Bonferroni Posthoctest was used to find where the differences were.
Data obtained from VAS did not pass the normality check andhence non-parametric tests were used. Friedman’s related-samplestest was used to compare the pain VAS results between the threetesting conditions. Multiple related-samples Wilcoxon Signed Ranktests were conducted as a Posthoc test.
3. Results
Eleven subjects (8 males and 3 females) with confirmed SIS anda mean age of (45.7 ± 9.4) participated in the study. Subjects scoreda mean of 33.1 ± 7.4 on the Oxford Shoulder score (Dawson et al.,2009).
There were no significant differences in pain VAS between thethree conditions at rest; Baseline condition had a median of0.5 cm (max = 5 cm, min = 0 cm), Rigid taping had a median of0.5 cm (max = 2.9 cm, min = 0 cm) and Elastic taping had a medianof 0.8 cm (max = 8.7 cm and min = 0 cm).
3.1. Sagittal plane
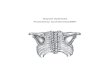
In the sagittal plane, differences were found for the scapularinternal rotation (p < 0.05) between the Rigid taping and Elastictaping conditions and the baseline measurements in sagittal planeelevation and lowering (Table 1). Rigid and Elastic taping tech-niques externally rotated the scapula in sagittal plane elevationby means of 3.4� and 2.7� and in sagittal plane lowering by 2.5�and 2.8�, respectively (Fig. 2). Neither of the taping techniquesaltered the scapular upward rotation. Rigid taping was found to
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

Table 1Results of the repeated ANOVA tests for scapulothoracuc rotations (Internal, upward and posterior tilt) and displacements (anterior, elevation, protraction) for arm elevation andlowering movements occurring in the sagittal and scapular planes.
Sagittal plane Scapular plane
Movement Parameter Taping Taping*Angle Movement Parameter Taping Taping*Angle(p-value) (p-value) (p-value) (p-value)
Elevation Scapular rotations Elevation Scapular rotationsInternal rotation 0.016* 0.512 Internal rotation 0.108 0.477Upward rotation 0.405 0.577 Upward rotation 0.057 0.134Posterior tilt 0.002** 0.874 Posterior tilt 0.130 0.766
Scapular displacements Scapular displacementsAnterior displacement 0.393 0.593 Anterior displacement 0.009** 0.315Scapular elevation 0.271 0.754 Scapular elevation 0.025* 0.082Scapular protraction 0.854 0.901 Scapular protraction 0.035* 0.031*
Lowering Scapular rotations Lowering Scapular rotationsInternal rotation 0.029* 0.169 Internal rotation 0.006** 0.300Upward rotation 0.142 0.169 Upward rotation 0.317 0.111Posterior tilt 0.000*** 0.196 Posterior tilt 0.008** 0.186
Scapular displacements Scapular displacementsAnterior displacement 0.479 0.423 Anterior displacement 0.008** 0.382Scapular elevation 0.301 0.412 Scapular elevation 0.011* 0.100Scapular protraction 0.454 0.451 Scapular protraction 0.153 0.058
* p < 0.05.** p < 0.01.
*** p < 0.001.
4 A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx
anteriorly tilt the scapula by a mean of 3.8� in elevation (p < 0.01)and 3.6� in lowering (p < 0.001) compared to the Baseline condi-tion. There were no significant differences between the Elasticand Baseline conditions for the scapular tilt (Fig. 2).
The Rigid and Elastic taping techniques did not have a significanteffect on scapular displacements (Table 1). Pain was significantlylower (p < 0.05) under the two taping conditions for movementsin the sagittal plane compared to the Baseline condition; the Base-line condition had a median of 5.2 cm (max = 7.5 cm, min = 0 cm),Rigid taping had a median of 2.4 cm (max = 8.9 cm, min = 0 cm)and Elastic taping had a median of 1.5 cm (max = 8.6 cm,min = 0 cm). Table 2 shows a summary of the number of subjectswith changes in their pain scores under the two taping conditions.
3.2. Scapular plane
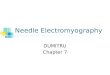
In scapular plane elevation, no significant differences in scapu-lar rotations were found between the taping conditions andBaseline. This was different to scapular plane lowering, wheredifferences in scapular internal rotation under the Elastic tapingcondition reached statistical significance (p < 0.01). Elastic tapingwas found to externally rotate the scapula by a mean of 4.6� inscapular plane lowering. Rigid taping was found to anteriorly tiltthe scapula in scapular plane lowering by a mean of 3.6� (Fig. 3).
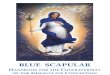
Elastic taping had a significant effect on the scapular position inscapular plane elevation and lowering (Fig. 4). In elevation, Elastictaping positioned the scapula in a more posterior (p < 0.01) andretracted (p < 0.05) position. The effect of Elastic taping on thescapular retraction were greater at mid and high elevation angleswhich is the reason for the significance in the interaction effectof Taping and Elevation Angle (p < 0.05, Table 1). In lowering, thescapula was also more posterior (p < 0.01) under the Elastic tapecondition. Rigid taping had no significant effect on the scapulardisplacements.
It is also interesting to note that although neither of the tapingtechniques were significantly different to the Baseline for the dis-placement in the superior-inferior direction (scapular elevationand depression), the two taping conditions differed from eachother (p < 0.05). While Rigid taping depressed the scapula, Elastic
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
taping caused a small elevation to the scapular position relativeto the thorax (Fig. 4).
There was no significant difference in pain between the threeconditions in scapular plane movements; Baseline had a medianof 4.6 cm (max = 10.0 cm, min = 0 cm), Rigid taping had a medianof 3.5 cm (max = 10.0 cm, min = 0 cm) and Elastic taping had amedian of 2.8 cm (max = 10.0, min = 0 cm). Table 2 shows a sum-mary of the number of subjects with changes in their pain scoresunder the two taping conditions.
4. Discussion
The results suggest that taping techniques have effects on scap-ular kinematics and pain, these effects are different for differentplanes of movement and they may be of different magnitudes forelevation and lowering in the same plane.
Both Rigid and Elastic taping techniques externally rotated thescapula in sagittal plane movements. In the scapular plane, onlyElastic taping significantly increased scapular external rotation inlowering. A number of studies have shown that patients with SIShave increased scapular internal rotation compared to a healthycontrol group (Hebert et al., 2002; Ludewig and Cook, 2000;Ludewig and Reynolds, 2009). The results in this study would sug-gest that both taping techniques help in reducing the scapularinternal rotation and therefore in normalising scapular kinematics.However, this is only consistent for movements occurring in thesagittal plane. Both taping techniques also resulted in a clinicallysignificant (Farrar et al., 2001) reduction in pain in sagittal planemovements (difference of more than 2 cm on the median of VASscores). Other studies that have investigated the effect of tapingon shoulder pain reported an increase in the pain-free range-of-motion but no change to the intensity of pain (Lewis et al.,2005a; Thelen et al., 2008).
Interestingly, Hebert et al. (2002) suggested the use of scapularinternal rotation as an indicator for the severity of SIS. The authorsalso suggested that rehabilitation protocols should focus on restor-ing scapular kinematics in the sagittal plane and particularly onrestoring scapular external rotation (Hebert et al., 2002). Thesesuggestions are in line with the findings of this study.
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

Elevation
Internal Rotation
Posterior Tilt
LoweringInternal Rotation
Posterior Tilt
* significant difference between Rigid Taping and Baseline difference between Elastic Taping and Baseline
* †
*
* †
*
†
Fig. 2. Means of scapulorthoracic rotations in sagittal plane movements affected by taping and 95% confidence intervals of the difference between measurements obtainedunder the Rigid and Elastic taping conditions Baseline measurements.
A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx 5
SIS has been associated with a decrease in scapular upwardrotation (Endo et al., 2001; Ludewig and Cook, 2000; Su et al.,2004) and posterior tilt (Endo et al., 2001; Lukasiewicz et al.,1999). The two taping techniques did not seem to have an effecton upward rotation. In addition, Rigid taping increased anteriortilt in sagittal plane movements. Although this suggests thatRigid taping exaggerates an already increased anterior tilt inpatients with SIS, the results may be caused by an angle calcu-lation artifact caused by thoracic extension. The reported scapu-lar rotations are calculated relative to a coordinate frame of thethorax which is defined relative to four bony landmarks on the
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
thorax (Wu et al., 2005) rather than a coordinate system basedon the thoracic spine alone. This means that an increase in thethorax extension angle may be falsely perceived as scapularanterior tilt. Indeed, one of the aims of the Rigid tape applicationtechnique is to extend the thoracic spine from a flexed startingposition (Lewis et al., 2005a). Calculating the rotations of thethoracic coordinate frame relative to a global frame revealed thatthe thorax extended by a range of 2–5�. Contrary to the resultsof this study; Hsu et al. (2009) found that Elastic taping signifi-cantly increased the scapular posterior tilt, but the magnitude ofchange was very small (approximately 1�) and it only occurred
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

Table 2Median, maximum and minimum VAS scores for Rigid and Elastic taping conditions in the sagittal and scapular plane movements. The table also shows the number of subjectswith VAS of less than 2 cm at baseline, the number of subjects with reduced and increased pain scores.
Sagittal plane Scapular planemovements movements
Rigid taping Elastic taping Rigid taping Elastic taping
Number of subjects with VAS < 2 cm at baseline 2 2Number of subjects with reduced paina 5 5 3 2Number of subjects with increased paina 0 0 0 1Median (cm) 2.4 1.5 3.5 2.5Maximum (cm) 8.9 8.6 10 10Minimum (cm) 0 0 0 0
a Pain reduction or increase is defined as a change of 2 cm or more on VAS.
Lowering
Internal Rotation
Posterior Tilt
* significant difference between Rigid Taping and Baseline
*
†
†
Fig. 3. Means of scapulothoracic rotations in scapular plane movements affected by taping and 95% confidence intervals of the difference between measurements obtainedunder the Rigid and Elastic taping conditions Baseline measurements.
6 A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx
in low elevation angles in scapular plane elevations (Hsu et al.,2009).
It is also interesting to note that although the Rigid taping appli-cation and the measurement method used in this study is directlycomparable to that of Shaheen et al. (2013), there are a number ofdifferences in the results of the two studies. Whilst Rigid tapingwas found to increase scapular external rotation in sagittal planeelevations in both studies, it was not found to have an effect onupward rotation in this study. Rigid taping was also found to havethe opposite effect on scapular tilt. This however may be due to thedifference in subjects’ posture in the two studies, the study ofShaheen et al. (2013) tested younger non-symptomatic volunteerswho may have had better postures and were therefore less affectedby the artifact caused by thoracic extension. Both studies howeverfound that changes in kinematics were only present in sagittalplane movements.
The Rigid taping technique employed in this study is alsobelieved to retract and depress the scapula (Lewis et al., 2005b).There is a trend which suggests that Rigid taping did depress thescapula in scapular plane movements. Although this change inkinematics did not reach statistical significance compared to the
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
baseline, it is interesting to note that Rigid taping did positionthe scapula in a more depressed position compared to the Elastictaping and that this difference was statistically significant. TheElastic taping technique on the other hand increased scapularretraction in scapular plane movement. This effect was significantin scapular plane elevation at mid and high elevation angles.Elastic taping also placed the scapula in a more posterior positionin scapular plane movements. However, these changes do not seemto relate to the intensity of pain during scapular plane movements.
The key alteration to scapular kinematics caused by taping isthe reduction in scapular internal rotation, this alteration occursmainly in the sagittal plane where a significantly reduced painwas also found. Thus, it is reasonable to suggest that the reductionin pain could be associated with the change in the scapular internalrotation. One possible mechanism by which this reduction of painoccurs is that an externally (less internally) rotated scapulaincreases the subacromial space and relieves pain caused bysoft-tissue impingement as illustrated in Fig. 5; this has also beensuggested in previous studies (Ludewig and Reynolds, 2009).
Interestingly, despite the differences in the type of tape (Rigidvs. Elastic) and how it is applied (Unilateral vs. Bilateral), the
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

Elevation
ScapularAnterior
displacement
ScapularElevation
Scapular Protraction
LoweringScapularAnterior
displacement
ScapularElevation
†
†
†
‡
‡
†‡
Fig. 4. Means of scapular displacements in scapular plane movements affected by taping and 95% confidence intervals of the difference between measurements obtainedunder the Rigid and Elastic taping conditions Baseline measurements.
A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx 7
effects of taping on scapular kinematics on the whole are similar.It is however interesting to note that 10 out 11 subjects pre-ferred the Elastic tape application, this was mainly due to therestriction to the range of movement of the thorax caused byRigid taping. Nonetheless, the effects on pain seen in this studydo not suggest a more beneficial effect of one taping techniqueover the other. In addition, although small differences were
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
found in the effects of the two taping techniques on scapularplane kinematics, these cannot be used to indicate an addedadvantage of a taping technique over the other due to theabsence of a concomitant effect on pain and the existing discrep-ancy in the literature with regards to the movements that tapingneeds to normalise in patients with SIS (Ludewig and Reynolds,2009).
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

No Tape
Subacromialspace
ExternalRotation
No Tape
ExternalRotation
With Tape
With Tape
Fig. 5. Both taping techniques externally rotated the scapula in sagittal plane movements. One possible mechanism that explains the reduction in pain is the subsequentincrease in the subacromial space caused by the external rotation of the scapula after taping.
8 A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx
4.1. Study limitations
The effects of scapular taping on muscular control or proprio-ception have not been investigated as part of this work and mayhave contributed to the pain reduction or to the observed changesin kinematics. In addition, the study only investigated immediateeffect of taping on kinematics. This set-up allowed a comparisonwhen subjects were experiencing the same level of pain at restand also reduced inter-session measurement errors. However,the long term effects of taping as well as the effects of couplingthese taping techniques to an exercise regime were notinvestigated.
There are also limitations associated with the measurementmethod used in this study. The study employed the scapular track-ing method proposed by Shaheen et al. (2011b). Although themethod has improved intra-observer reliability compared to otherscapula tracking methods, the method is still dependent on theability of the observer to correctly identify and track scapularlandmarks. It is however believed that errors introduced by theobserver would not have contributed to the differences shown bytaping, particularly as the significant changes caused by taping inkinematics were consistent across subjects as shown by the 95%confidence intervals shown in Figs. 2–4. Another limitation is theway that scapular displacements were quantified in this study.The method uses the position of the acromial angle relative tothe thorax coordinate system. These displacements are used toprovide a measure of the changes in the position of the scapuladue to taping but they may not be representative of true scapulo-thoracic translations.
Other factors that could have contributed to the variations inthe effects of taping on kinematics of different subjects includethe inconsistencies introduced by the taping application. Theeffects of these were assessed in a pilot study that looked at re-taping a non-symptomatic cohort using the same Rigid tape appli-cation technique, the results of the pilot study showed that therewere no significant differences in kinematics between the twoapplications (Villa, 2010).
5. Conclusions
Rigid and Elastic taping techniques reduce the scapular internalrotation in patients suffering from SIS. This effect corresponds witha reduction in the intensity of pain experienced by patients and isonly observed in movements in the sagittal plane. The Elastic tap-ing technique positions the scapula more posteriorly and increasescapular retraction in scapular plane movements; however thesealterations to kinematics did not have a corresponding effect onthe pain.
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
Suppliers
(a). Physio-med. Unit 13, Glossop Brook Business Park, SurreyStreet, Glossop, Derbyshire SK13 7AJ.
(b). Kinesio UK. Cobalt 3.1, Silverfox Way, Newcastle Upon Tyne,NE27 0QJ.
(c). Vicon. 14 Minns Business Park Oxford OX2 0JB.
Ethical approval
This research has been approved by Central London REC 4.
Conflict of interest
None declared.
Acknowledgement
This study was funded by Imperial College NHS HealthcareCharity.
References
Ackermann B, Adams R, Marshall E. The effect of scapula taping onelectromyographic activity and musical performance in professional violinists.Aust J Physiother 2002;48:197–203.
Alexander CM, McMullan M, Harrison PJ. What is the effect of taping along or acrossa muscle on motoneurone excitability? A study using triceps surae. Man Ther2008;13:57–62.
Alexander CM, Stynes S, Thomas A, Lewis J, Harrison PJ. Does tape facilitate orinhibit the lower fibres of trapezius? Manual Ther 2003;8:37–41.
Bennell K, Khan K, McKay H. The role of physiotherapy in the prevention andtreatment of osteoporosis. Manual Ther 2000;5:198–213.
Borstad JD. Resting position variables at the shoulder: evidence to support aposture-impairment association. Phys Ther 2006;86:549–57.
Bradley T, Baldwick C, Fischer D, Murrell GA. Effect of taping on the shoulders ofAustralian football players. Br J Sports Med 2009;43:735–8.
Brochard S, Lempereur M, Remy-Neris O. Double calibration: an accurate, reliableand easy-to-use method for 3D scapular motion analysis. J Biomech2011;44:751–4.
Budoff JE, Nirschl RP, Guidi EJ. Debridement of partial-thickness tears of the rotatorcuff without acromioplasty. Long-term follow-up and review of the literature. JBone Joint Surg Am 1998;80:733–48.
Cools AM, Witvrouw EE, Danneels LA, Cambier DC. Does taping influenceelectromyographic muscle activity in the scapular rotators in healthyshoulders? Man Ther 2002;7:154–62.
Dawson J, Rogers K, Fitzpatrick R, Carr A. The Oxford shoulder score revisited. ArchOrthop Trauma Surg 2009;129:119–23.
Endo K, Ikata T, Katoh S, Takeda Y. Radiographic assessment of scapular rotationaltilt in chronic shoulder impingement syndrome. J Orthop Sci 2001;6:3–10.
Farrar JT, Young JP, Lamoreaux L, Werth JL, Poole RM. Clinical importance of changesin chronic pain intensity measured on an 11-point numerical pain rating scale.Pain 2001;94:149–58.
Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome. A critical review. ClinOrthop Relat Res 1991:162–73.
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011

A.F. Shaheen et al. / Journal of Electromyography and Kinesiology xxx (2014) xxx–xxx 9
Garcia-Muro F, Rodriguez-Fernandez AL, Herrero-De-lucas A. Treatment ofmyofascial pain in the shoulder with Kinesio taping. A case report. Man Ther2010;15:292–5.
Hebert LJ, Moffet H, McFadyen BJ, Dionne CE. Scapular behavior in shoulderimpingement syndrome. Arch Phys Med Rehabil 2002;83:60–9.
Hill AM, Bull AM, Dallalana RJ, Wallace AL, Johnson GR. Glenohumeral motion:review of measurement techniques. Knee Surg Sports Traumatol Arthrosc2007;15:1137–43.
Host HH. Scapular taping in the treatment of anterior shoulder impingement. PhysTher 1995;75:803–12.
Hsu YH, Chen WY, Lin HC, Wang WT, Shih YF. The effects of taping on scapularkinematics and muscle performance in baseball players with shoulderimpingement syndrome. J Electromyogr Kinesiol 2009;19:1092–9.
Jobe CM, Coen MJ, Screnar P. Evaluation of impingement syndromes in theoverhead-throwing athlete. J Athl Train 2000;35:293–9.
Kalter J, Apeldoorn AT, Ostelo RW, Henschke N, Knol DL, Van Tulder MW. Tapingpatients with clinical signs of subacromial impingement syndrome: the designof a randomized controlled trial. BMC Musculoskelet Disord 2011;12:188.http://dx.doi.org/10.1186/1471-2474-12-188.
Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulderimpingement syndrome. J Orthop Sports Phys Ther 1993;17:212–24.
Karduna AR, McClure PW, Michener LA, Sennett B. Dynamic measurements ofthree-dimensional scapular kinematics: a validation study. J Biomech Eng2001;123:184–90.
Kase KW, Kase JT. Clinical therapeutic applications of the kinesio tapingmethod. Tokyo, Japan: Ken Ikai Co., Ltd.; 2003.
Kaya E, Zinnuroglu M, Tugcu I. Kinesio taping compared to physical therapymodalities for the treatment of shoulder impingement syndrome. ClinRheumatol 2011;30:201–7.
Kontaxis A, Cutti AG, Johnson GR, Veeger HE. A framework for the definition ofstandardized protocols for measuring upper-extremity kinematics. ClinBiomech (Bristol, Avon) 2009;24:246–53.
Lewis JS, Green A, Wright C. Subacromial impingement syndrome: the role ofposture and muscle imbalance. J Shoulder Elbow Surg 2005a;14:385–92.
Lewis JS, Wright C, Green A. Subacromial impingement syndrome: the effect ofchanging posture on shoulder range of movement. J Orthop Sports Phys Ther2005b;35:72–87.
Lin JJ, Hung CJ, Yang PL. The effects of scapular taping on electromyographic muscleactivity and proprioception feedback in healthy shoulders. J Orthop Res2011;29:53–7.
Lo YP, Hsu YC, Chan KM. Epidemiology of shoulder impingement in upper armsports events. Br J Sports Med 1990;24:173–7.
Lohrer H, Alt W, Gollhofer A. Neuromuscular properties and functional aspects oftaped ankles. Am J Sports Med 1999;27:69–75.
Ludewig PM, Cook TM. Alterations in shoulder kinematics and associated muscleactivity in people with symptoms of shoulder impingement. Phys Ther2000;80:276–91.
Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeraljoint pathologies. J Orthop Sports Phys Ther 2009;39:90–104.
Lukasiewicz AC, Mcclure P, Michener L, Pratt N, Sennett B. Comparison of 3-dimensional scapular position and orientation between subjects with andwithout shoulder impingement. J Orthop Sports Phys Ther 1999;29:574–83.discussion 584–6.
McConnell J, Donnelly C, Hamner S, Dunne J, Besier T. Effect of shoulder taping onmaximum shoulder external and internal rotation range in uninjured andpreviously injured overhead athletes during a seated throw. J Orthop Res2011;29:1406–11. http://dx.doi.org/10.1002/jor.21399.
Michener LA, Mcclure PW, Karduna AR. Anatomical and biomechanical mechanismsof subacromial impingement syndrome. Clin Biomech (Bristol, Avon)2003;18:369–79.
Morrissey D. Proprioceptive shoulder taping. J Bodywork Movement Ther2000;4:189–94.
Mostafavifar M, Wertz J, Borchers J. A systematic review of the effectiveness ofkinesio taping for musculoskeletal injury. Phys Sportsmed 2012;40:33–40.
Neer CS. Anterior acromioplasty for the chronic impingement syndrome in theshoulder a preliminary report. J Bone Joint Surg 1972;54:41–50.
Prinold JA, Shaheen AF, Bull AM. Skin-fixed scapula trackers: a comparison of twodynamic methods across a range of calibration positions. J Biomech2011;44:2004–7.
Selkowitz DM, Chaney C, Stuckey SJ, Vlad G. The effects of scapular taping on thesurface electromyographic signal amplitude of shoulder girdle muscles duringupper extremity elevation in individuals with suspected shoulder impingementsyndrome. J Orthop Sports Phys Ther 2007;37:694–702.
Shaheen AF, Alexander CM, Bull AM. Effects of attachment position and shoulderorientation during calibration on the accuracy of the acromial tracker. JBiomech 2011a;44:1410–3.
Shaheen AF, Alexander CM, Bull AM. Tracking the scapula using the scapula locatorwith and without feedback from pressure-sensors: a comparative study. JBiomech 2011b;44:1633–6.
Please cite this article in press as: Shaheen AF et al. Rigid and Elastic taping chasyndrome; an experimental study. J Electromyogr Kinesiol (2014), http://dx.do
Shaheen AF, Villa C, Lee YN, Bull AM, Alexander CM. Scapular taping alterskinematics in asymptomatic subjects. J Electromyogr Kinesiol 2013;23:326–33.
Smith M, Sparkes V, Busse M, Enright S. Upper and lower trapezius muscle activityin subjects with subacromial impingement symptoms: is there imbalance andcan taping change it? Phys Ther Sport 2009;10:45–50.
Su KP, Johnson MP, Gracely EJ, Karduna AR. Scapular rotation in swimmers with andwithout impingement syndrome: practice effects. Med Sci Sports Exerc2004;36:1117–23.
Thelen MD, Dauber JA, Stoneman PD. The clinical efficacy of kinesio tape forshoulder pain: a randomized, double-blinded, clinical trial. J Orthop Sports PhysTher 2008;38:389–95.
van der Windt DA, Koes BW, Boeke AJ, Deville W, de Jong BA, Bouter LM. Shoulderdisorders in general practice: prognostic indicators of outcome. Br J Gen Pract1996;46:519–23.
Vecchio P, Kavanagh R, Hazleman BL, King RH. Shoulder pain in a community-basedrheumatology clinic. Br J Rheumatol 1995;34:440–2.
Villa C. Does taping affect the motion of the scapula? MSc Imperial College London.2010.
Warner MB, Chappell PH, Stokes MJ. Measuring scapular kinematics during armlowering using the acromion marker cluster. Hum Mov Sci 2012;31:386–96.
Williams S, Whatman C, Hume PA, Sheerin K. Kinesio taping in treatment andprevention of sports injuries: a meta-analysis of the evidence for itseffectiveness. Sports Med 2012;42:153–64.
Wu G, van der Helm FC, Veeger HE, Makhsous M, van Roy P, Anglin C, et al. ISBrecommendation on definitions of joint coordinate systems of various joints forthe reporting of human joint motion–Part II: Shoulder, elbow, wrist and hand. JBiomech 2005;38:981–92.
Aliah F. Shaheen is a lecturer in Human MovementScience in the University of Surrey. Her researchinterests are in movement variability and inter-seg-mental coordination and its relation to function. Shecompleted her PhD in 2010 in Imperial College Lon-don; where she developed methods to accuratelytrack the movement of the scapula in-vivo. Sheworked as a postdoctoral researcher in the sameinstitution investigating the effect of scapular tapingtechniques on posture, kinematics and pain inasymptomatic subjects and subjects with shoulderimpingement syndrome.
Anthony M.J. Bull is Professor of MusculoskeletalMechanics at Imperial College London. His researchinterests are in how forces and deformations aretransmitted through the musculoskeletal system. Theapplications range from diseases of ageing, includingosteoarthritis, to high-level athletic performance andinjuries. Anthony leads the Royal British Legion Centrefor Blast Injury Studies, the Centre for Medical Engi-neering Solutions in Osteoarthritis, and the SportsInnovation Challenge, all multi-million pound fundedresearch activities at Imperial College. His adminis-trative roles include Head of Department of Bioen-gineering and Director of the Institute of BiomedicalEngineering.
Caroline M. Alexander is a NIHR Senior ClinicalLecturer at Imperial College Healthcare N.H.S. Trust.Her laboratory is situated within the clinical phys-iotherapy department. She obtained a doctorate inphysiology in 2002 in the field of reflex control ofshoulder girdle muscles. Her research interestsinclude the differences in motor control betweenhealthy people and people with musculoskeletalproblems as well as the effectiveness of physiother-apy.
nges scapular kinematics and pain in subjects with shoulder impingementi.org/10.1016/j.jelekin.2014.07.011