Embed Size (px)
Citation preview

at SciVerse ScienceDirect
Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8
Contents lists available
Journal of Cranio-Maxillo-Facial Surgery
journal homepage: www.jcmfs.com
Influence of kinesiologic tape on postoperative swelling, painand trismus after zygomatico-orbital fractures
Oliver Ristowa,b,*, Christoph Pautke b,c, Victoria Kehl d, Steffen Koerdt a,Katharina Schwärzler a, Lilian Hahnefeld a,b, Bettina Hohlweg-Majert e
a Ludwig-Maximilians Universität München (Dean: Prof. Dr. Dr. h. c. Wolfgang Gernet), Goethestr. 70, D-80336 Munich, GermanybMedizin & Aesthetik, Private Clinic for Oral and Maxillofacial and Plastic Surgery, Lenbachplatz 2a, D-80333 Munich, Germanyc Ludwig-Maximilians Universität München, Department of Oral and Maxillofacial Surgery (Chair: Prof. Dr. Dr. Michael Ehrenfeld), Lindwurmstr. 2a,D-80336 Munich, Germanyd Technische Universität München, Institute of Medical Statistics and Epidemiology (Chair: Prof. Dr. Klaus A. Kuhn), Ismaninger Straße 22,D-81675 Munich, Germanye Technische Universität Munich, Department of Oral and Maxillofacial Surgery (Chair: Prof. Dr. Dr. Klaus-Dietrich Wolff), Ismaninger Str. 22,D-81675 Munich, Germany
a r t i c l e i n f o
Article history:Paper received 21 December 2012Accepted 29 May 2013
Keywords:Kinesiologic tapeZygomatico-orbital fractureSwellingPainTrismusMorbidity
* Corresponding author. Medicine and AestheticsMaxillofacial and Plastic Surgery, Lenbachplatz 2a,Tel. þ49 89 5156 7963; fax þ49 89 5156 7964.
E-mail address: [email protected] (O
1010-5182/$ e see front matter � 2013 European Asshttp://dx.doi.org/10.1016/j.jcms.2013.05.043
Please cite this article in press as: Ristow O,orbital fractures, Journal of Cranio-Maxillo-F
a b s t r a c t
Surgical treatment of zygomatico-orbital (ZO) fractures is a common procedure in maxillofacial surgery.Often accompanied by pain, trismus and swelling, postoperative morbidity is a major disadvantage,affecting patients’ quality of life. The appliance of kinesiologic tape (KT) improves the blood and lymphflow, removing congestions of lymphatic fluid and haemorrhages. The aim of this study was to find out ifthe application of kinesiologic tape prevents or improves swelling, pain and trismus after zygomatico-orbital fracture surgery, improving patients’ postoperative quality of life.
A total of 30 patients were assigned for treatment of zygomatico-orbital fractures and were randomlydivided into treatment either with or without kinesiologic tape. Tape was applied directly after surgeryand maintained for at least 5 days postoperatively. Facial swelling was quantified using a five-linemeasurement at six specific time points. Pain and degree of mouth opening was measured. Patient’ssubjective feeling and satisfaction was queried.
The results of this study show that application of kinesiologic tape after zygomatico-orbital surgerysignificantly reduced the incidence of swelling with an earlier swelling maximum, and decreased themaximum turgidity for more than 60% during the first 2 days after surgery. Although, kinesiologic tapehas no significant influence on pain control and trismus, mouth opening increased earlier after operationin the kinesiologic tape group compared to the no-kinesiologic tape group. Furthermore, patients withkinesiologic tape felt significantly lower morbidity than those without kinesiologic tape. Thereforekinesiologic tape is a promising, simple, less traumatic, economical approach, which is free from adversereaction and improves patients’ quality of life.
� 2013 European Association for Cranio-Maxillo-Facial Surgery. Published by Elsevier Ltd. All rightsreserved.
1. Introduction
Midface fractures involving zygomatico-orbital (ZO) fractures arecommon inmaxillofacial surgery (Rogers et al., 2000, Erdmann et al.,2008, van den Bergh et al., 2012, Gassner et al., 2003, NaveenShankar et al., 2012). Often attended by pain, trismus and swelling,
, Private Clinic for Oral andD-80333 Munich, Germany.
. Ristow).
ociation for Cranio-Maxillo-Facial
et al., Influence of kinesiologiacial Surgery (2013), http://d
postoperative morbidity is a major disadvantage, affecting patients’quality of life (Miloro, 2004, Trivellato et al., 2011, Folkestad et al.,2006). Tissue reactions are thought to arise from the inflammatoryresponse as a direct and immediate consequence of the surgicalprocedure (Samad et al., 2001). Complications as haemorrhageemphysema or sepsis may occur (Trivellato et al., 2011). The adverseeffects of ZO surgery on life quality have been reported to beincreased in patients who experience swelling, pain and trismus. Itseems appropriate to study the causes and the effects of ZO fracturesmanaged by open reduction and rigid internal fixation at the presenttime, when economic factors are included in assessment of the
Surgery. Published by Elsevier Ltd. All rights reserved.
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e82
treatment. The break in social and professional activity of injuredindividuals and the scale of the problem indicates the necessity toreduce or eliminate these side effects, thus, improving patients’satisfaction after treatment of ZO surgery (Calderoni et al., 2011).
Several methods to control the immediate inflammatoryresponse associated with head and neck surgery have beendescribed and used, including the use of drugs such as analgesics(Kim et al., 2009, Aznar-Arasa et al., 2012; de Sousa Santos et al.,2012), corticosteroids (Markiewicz et al., 2008; Thoren et al.,2009), antibiotics (Knepil and Loukota, 2010; Andreasen et al.,2006) and proteolytic enzymes (Al-Khateeb and Nusair, 2008),laser application (Markovic and Todorovic, 2007, Roynesdal et al.,1993) or physical therapeutic methods like cryotherapy (Ranaet al., 2012) or manual lymph drainage (MLD) (Szolnoky et al.,2007). No single modality of management significantly preventsand/or significantly reduces the occurrence of swelling, pain andtrismus without potential undesirable side effects. Thereforefurther techniques for a better pain, swelling and trismus controlshould be developed for patients who undergo ZO surgery.
After its introduction in the 1970s, kinesiologic tape (KT) hasincreasingly become popular in the treatment of sport injuries anda variety of other conditions. There are several claims to the effectsof KT including supporting injured muscles and joints, relievingpain, and increasing blood and lymph flow in the injured area.However, there is still little evidence to support these claims andmuch more research is necessary (Williams et al., 2012; Morriset al., 2012). The use of KT in the management of lymphoedemais gaining popularity. The tape is similar inweight to the epidermis,and lifting the skin, KT improves the blood and lymph flow,removing congestions of lymphatic fluid or haemorrhages (Chouet al., 2012). By providing space, fluids are encouraged to movefrom areas of higher pressure towards the area of lower pressure,guided by the tape to the desired direction of drainage (Kase et al.,2003). Using this technique may be beneficial for postoperativetreatment after head and neck surgery, accelerating drainage oftissue reaction or haemorrhages.
The goal of this study was to find out if the application of KTprevents or improves swelling, pain and trismus after ZO surgery,improving patients’ postoperative quality of life.
2. Material and methods
2.1. Patients
Over a period of 12 months, 30 consecutive patients wererecruited and prospectively included in our monocentric, parallel-group, open label, randomized clinical trial. 14 female and 16male patients were enrolled (mean age and standard deviation,41.4 � 18.5 years; age range, 18e74 years). Based on the CONSORT2010 checklist for randomized, controlled, clinical trials (CochraneCollaboration, Manchester, UK) participants were randomized intotwo study groups: (i) KT group; (ii) no-KT group. Blinding andplacebo control were not possible due to the nature of the KT. In-clusion criteria were: zygomatico-orbital fracture, zygomatic-maxillary fracture involving orbital floor, indication for openreduction and internal fixation if necessary. Exclusion criteria wereisolated zygomatic arch fracture, sensitivities to tape, inflammatoryreactions after surgery, unwillingness to shave facial hair andknown allergies to medication used in the study.
2.2. Operation
All operations were performed by two board-certified andspecialized Oral and Maxillofacial Surgeons (BHM, CP) under gen-eral anaesthesia using nasal intubation. Surgery was performed in
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
sterile conditions following a standardized operation protocol andusing standardized approaches from the upper eyelid (blepharo-plasty approach), transconjunctival and transoral (if necessary). Thereduction of the zygoma was performed by transbuccal hookretraction. Internal fixation was achieved using miniplates (matrixmidface plating system, Synthes�, Switzerland). The orbital floorwas reconstructed using flexible and resorbable Ethisorb patches(Ethicon, Norderstedt, Germany). Mean operation duration variedfrom 45 to 60 min.
A single dose of antibiotics (Ampicillin/Sulbactam Kabi2000 mg/1000 mg) was given preoperatively. All patients stayed inhospital for at least 72 h after surgery. Patients received routinepostoperative instructions: Ice pack application for 6 h after sur-gery, alternating 30 min of application with 30 min of no applica-tion. All patients received the same postoperative analgesic drugtherapy of 1000mg Paracetamol (Perfalgan�) intravenously 2 timesper day for 3 days; and 600 mg Ibuprofen (Ibu-Ratiopharm�) orally(1st day: Ibuprofen 600 mg 3 times per day, 2nd day: Ibuprofen600 mg 2 times per day, 3rd day: Ibuprofen 600 mg 1 time per day,4th day: Ibuprofen 600 mg 1 time per day). There were no post-operative complications.
2.3. Taping
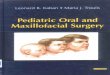
All taping procedures were performed by the same investigator(OR) a certified K-Taping therapist. Skin was cleaned and freed ofmoist and oils prior to application; if necessary the area wasshaved. All tape applications were performed using skin colouredK-Active Tape Classic�, 50 mm � 5 m (K-Active Europe GmbH�,Wiesthal, Germany). Tape length was individually measured forevery patient starting at the clavicle to the point of highestswelling. The tape was cut into three equal stripes (approximal1.5 cm wide). Tape endings were rounded down. The tape wascarefully removed from paper backing, trying to touch the adhe-sive as little as possible. The base was placed slightly above thelymph node area to which the drainage is being directed (supra-clavicular nodes). The patient was moved into a stretch position.Tails were placed on to the skin with slight tension (20%). Place-ment of the lymphatic stripes was directed at the appropriatelymphatic duct crossing the cervical, sub mental, mandibular,submandibular, preauricular and parotid nodes, crossing thezygomatic arch, reaching the infraorbital rim and frontozygomaticsuture surrounding the lower eye (Fig. 1). After application thetape was lightly rubbed to activate the medical grade acrylic ad-hesive. The tape was left for at least 5 days. Edges were trimmed iftape lifted before removal.
2.4. Measurements
All measurements were performed by one of the investigators(OR) at six specific time points (T): Pre-operative (T-1), Baseline(BL) ¼ directly after operation (T0), first (T1), second (T2), third(T3) and seventh (T4) postoperative day.
2.4.1. SwellingSwelling was assessed with a five-line measurement using a
standard plastic tape measure (accuracy �0.5 mm) placed in con-tact with the skin: (Line a) most posterior point tragus e mostlateral point lip commissure; (Line b) most posterior point tragus epogonium; (Line c) most posterior point tragus e lateral canthus ofthe eye; (Line d) lateral canthus of the eye e most inferior pointangle of the mandible; (Line e) most inferior point angle of themandibleemiddle of the nasal bone (Fig. 2). Marking endpoints forsubsequent tape measurements were drawn, using a fine water-proof felt tip pen.
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

Fig. 2. Five-line measurement. Note, segments endpoints were marked to ensure ac-curate measurements.
Fig. 1. Kinesio tape application from supraclavicular to the orbital rim surrounding theeye in a gradual wave. Tape stripes stimulate drainage of swelling and haematomafollowing the lymphatic duct.
O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 3
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
2.4.2. PainPain scores were assessed using a 10 level visual analogue scale
(VAS) of 100 mm, representing all pain sensations from none tomaximum; where 0 indicates no pain, 5 moderate pain and 10worst pain possible. Patients were asked to place a mark along theline that corresponded to the amount of pain they wereexperiencing.
2.4.3. TrismusMaximal mouth opening was recorded measuring the
maximum inter-incisal distance using callipers (Fig. 3).
2.4.4. Subjective feelingsAll patients of the KT and the no-KT group were asked to decide
how they evaluated their satisfaction and convenience: verysatisfied ¼ 1; satisfied ¼ 2; not satisfied ¼ 3. Furthermore, all pa-tients of the KT group were asked to decide whether they find thetape: not disturbing¼ 1, slightly disturbing¼ 2, very disturbing¼ 3;whether the tape is not¼ 1, slightly¼ 2, highly¼ 3 affecting them intheir movements.
2.5. Statistical analysis
All statistical analysis were performed using IBM SPSS Statisticssoftware (Version 20.0). In addition to the descriptive statistics, thestudy groups were compared with each other using the indepen-dent samples t-test for differences in means. The significance levelwas set at 5%. Primary endpoint of the study was increase ofswelling between T0 and T0 þ X. All other statistical tests weresecondary endpoints of the study and were performed in anexploratory manner. The 95% confidence intervals (CI) for meanswelling and VAS measurements were also calculated and dis-played in plots. Disturbance, movement and satisfaction weresummarized by time with percent patients in each category.
3. Results
3.1. Swelling
All swelling measurements were expressed as mean sum of allfive-line measurements (Line a through Line e) for all patients (incm) at the six specific measurement times (Fig. 4).
Mean sum of all five-line measurements for all patients showedno statistically significant difference pre-operatively (T-1) and
Fig. 3. Inter-incisal distance was measured using a calliper.
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

Table 2Reduction of swelling one day after maximal swelling (Tmax) comparing KT and theno-KT group for mean sum of all five-line measurements for all patients. Shown aremean values and standard deviation for the difference Tmaxþ1eTmax. Negativevalues indicate a reduction of swelling after Tmax. Although reduction is higher forthe KT compared to the no-KT group results are not significant (p > 0.05).
Mean sum swelling (cm) KT group no-KT group p-Value
Mean SD Mean SD
Tmaxþ1eTmax �2.1 1.4 �1.7 1.3 p > 0.05
Fig. 4. Mean sum and 95% CI of all five-line measurements for all patients comparingKT (black line) and no-KT group (grey line) at six specific measurement times (T-1: Pre-operative; T0: Baseline directly after operation; T1: first; T2: second; T3: third; T4:seventh postoperative day). Note, the statistically highly significant difference in in-crease of swelling (p < 0.001), maximum swelling (p ¼ 0.007), time of maximumswelling (p < 0.001) and reduction of swelling (p ¼ 0.005) comparing the KT and theno-KT group.
O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e84
directly after operation at baseline measurement (T0) comparingKT group (T-1: 62.1 cm � 3.8; T0: 66.0 cm � 3.9) and no-KT group(T-1: 63.5 cm � 4.3; T0: 65.8 cm � 3.7).
Comparing the increase of swelling between baseline (T0) andT1, T2, T3 after operation highly significant differences (p < 0.001)between the KT and the no-KT group were seen (Table 1).Comparing the KT and the no-KT group the different increases ofswelling between T0 and T2 and T0 and T3 were highly significant(p < 0.001). While patients in the no-KT group showed an increasein swelling on day two after surgery with mean sum of measure-ments of 2.2 cm � 1.6, those in the KT group had reduced swellingwith a mean of �1.9 cm � 3.1. The increase in swelling between T0and T1 showed no statistical significance (p > 0.05).
Maximal swelling was defined as the difference between themaximal mean sum of all five-line measurements for all patientsand the mean sum of all five-line measurements at baseline (T0).The extent of maximal swelling in the no-KT group was larger(2.7 cm � 1.3) than in the KT group (1.1 cm � 1.7). This differencewas statistically significant (p ¼ 0.007). Patients in the KT groupexperienced their maximal swelling very early (mean day 0.5,median day 0 (Tmax)) while patients in the no-KT group hadmaximum swelling on average on day two. This difference washighly statistically significant (p < 0.001).
For the reduction of swelling the pure differences of the meansum of all five-line measurements for all patients between Tmaxand one day after Tmax (Tmaxþ1) are displayed in Table 2. Since
Table 1Increase of swelling, comparing KT and the no-KT group. Mean sum of all five-linemeasurements for all patients. Shown are mean values and standard deviation forthe increase of swelling between baseline (T0) and T1, T2, T3. Note, that difference inincreases between T0 through T2 and T0 through T3 were highly significant(p < 0.001) comparing KT and the no-KT group.
Mean sum swelling (cm) KT group no-KT group p-Value
Mean SD Mean SD
T1eT0 (BL) �0.3 2.8 1.4 1.4 p > 0.05T2eT0 (BL) �1.9 3.1 2.2 1.6 p < 0.001T3eT0 (BL) �3.1 3.2 1.6 1.5 p < 0.001
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
patients in the KTgroup did not swell as much as patients in the no-KT group, their reduction is not significantly larger than in the no-KT group (p > 0.05).
Comparing the results for the mean sum of all five-line mea-surements for all patients one day after the maximal swelling(Tmax þ 1) with the initial swelling at baseline (T0), patients in theKT group had a swelling reduction which was �1.1 cm � 2.2 belowinitial swelling after operation (T0). The extent of swelling one dayafter the maximal swelling in the no-KT group still exceeded theinitial swelling of T0 by 1.0 cm � 1.4. This difference in swellingreduction was statistically significant (p ¼ 0.005).
3.2. Pain
Comparing the KT and the no-KT group results for pain scoresassessed using a 10 level visual analogue scale (VAS) are shown inFig. 5.
3.3. Trismus
Baseline mouth opening values did not differ significantly inboth groups. Comparing KT and no-KT group Table 3 shows thedifference between mean sum of all inter inter-incisal distancemeasurements at baseline and T1, T2, T3, T4 for all patients.Compared to the baseline there is an increase in mouth opening atT2, T3 and T4 for the KT group (0.19 cm � 0.68; 0.27 cm � 0.63;0.47 cm � 0.57) while the no-KT group is decreasing(�0.01 cm � 0.42, �0.18 cm � 0.55, �0.17 cm � 1.44). Results arenot statistically significant (p > 0.05).
3.4. Subjective feeling
Results of subjective feelings are shown as sum of all scores forall patients at the specific measurement times in percentage.Reviewing patients satisfaction showed almost no difference be-tween the KT and the no-KT group postoperatively (T0) and the dayafter the operation (T1) (Fig. 6). Two, three and four days afteroperation patients satisfaction is higher in the KT group (verysatisfied: T2: 60%; T3: 67%, T4: 73%; satisfied: T2: 40%, T3: 27%; T4:13%; not satisfied T2: 0%, T3: 7%, T4: 13%) than in the no-KT group(very satisfied: T2: 20%, T3: 27%, T4: 47%; satisfied: T2: 40%, T3: 40%,T4: 40%; not satisfied T2: 40%, T3: 33%; T4: 13%). Results for Sub-jective KT evaluation are shown in Fig. 7.
4. Discussion
ZO fractures account for a significant component of facialtrauma, affecting a young and economically active subset of thepopulation. Postoperative swelling, pain and trismus are commonevents after ZO surgery affecting the social and working life of thepatients (Calderoni et al., 2011, Trivellato et al., 2011).
There are many studies on the control of postoperative oedemain maxillofacial surgery. In third molar surgery, the use of laser is a
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

Fig. 5. Mean and 95% CI of VAS scores for all patients at six specific measurement times comparing KT (black error-bars) and the no-KT group (grey error-bars). Note, that for bothgroups patients scored moderate pain or less (VAS < 5). There was no statistically significant difference between the two groups at any time.
Table 3Increase of mouth opening after operation comparing KTand the no-KTgroup. Meansum of all inter-incisal distance measurements between baseline and T1, T2, T3, T4for all patients comparing KT and no-KT group.
Mean sum IID (cm) KT group no-KT group
Mean SD Mean SD
T1eT0 (BL) �0.05 0.63 �0.02 0.18T2eT0 (BL) 0.19 0.68 �0.01 0.42T3eT0 (BL) 0.27 0.63 �0.18 0.55T4eT0 (BL) 0.47 0.57 �0.17 1.44
Fig. 6. Satisfaction score for all patients in percentage at six specific measurementtimes comparing the KT group (panel A) and the no-KT group (panel B). Note, that ondays two, three and four after operation patient satisfaction was higher in the KT thanthe no-KT group.
O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 5
relatively new method reducing postoperative discomfort, espe-cially swelling (Osunde et al., 2011). It is believed that laser irra-diation induces an increase in number and diameter of lymphvessels, with a simultaneous decrease of blood vessel permeability.However, its use in midface surgery has not been investigated yet.Ice therapy is a simple, cheap, repeatable modality. Its therapeuticeffects are due to changes in blood flow, consequent vasocon-striction and reduced metabolism, therefore reducing bacterialgrowth. However, data concerning the effect of cryotherapy onswelling are controversial (Greenstein, 2007, Rana et al., 2011,2012).
Unfortunately, comparison of published drug studies is difficultbecause of the variability in parameters and methods used for eachstudy.
The use of steroids is common in oral and maxillofacial surgery(Assimes and Lessard, 1999). However, except for the use of steroidsafter third molar extraction (Buyukkurt et al., 2006; Grossi et al.,2007), little has been published about potential benefits aftermidfacial fracture treatment. Patients with ZO fractures usuallyhave swelling, pain and trismus before the operation, requiringlonger treatment than for the removal of thirdmolars. Therefore, tobenefit from steroid medication, patients with facial fracturesought to get higher doses than patients undergoing third molarsurgery.
The use of non-steroid anti-inflammatory drugs (NSAID) hasbeen investigated with regard to reducing pain and inflammation.In the current literature, it is apparent that the combination ofanother drug with an NSAID is often more effective in controllingpostoperative pain and swelling in head and neck surgery than aNSAID alone (Kim et al., 2009).
Although the use of antibiotics for the control on significantpostoperative swelling and haematoma after head and neck
Please cite this article in press as: Ristow O, et al., Influence of kinesiologic tape on postoperative swelling, pain and trismus after zygomatico-orbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://dx.doi.org/10.1016/j.jcms.2013.05.043

Fig. 7. Subjective KT evaluation score for all patients of the KT group (n ¼ 15) inpercentage. Shown is patient evaluation if they found the KT disturbing (panel A) and ifKT affected them in their movements (panel B).
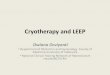
Fig. 8. Convolutions below the taped area caused by the elasticity of the applied tapesubsequently recoiling back to its original length following the application. It’sbelieved that these convolutions increase the interstitial space between the skin andunderlying connective tissue thus promote the follow of blood and lymphatic fluid.
O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e86
surgery is common, antibiotic therapy in ZO surgery is controver-sial. Knepil et al. highlight the low incidence of infections followingsurgery for ZO fractures (Knepil and Loukota, 2010). The in-vestigators think that avoiding a transoral approach allows for aclean operation, making prophylactic antibiotics unnecessary.
With any medication helping to reduce postoperative side ef-fects adverse effects and serious complications may follow.Emerging cases of drug allergies and drug-associated side effectsare focussing more attention on alternative methods.
In an initial study, Szolonoky et al. investigated the efficacy ofmanual lymph drainage (MLD) after third molar extraction. Usingreproducible facial measurement and a VAS pain scale, theydemonstrated that MLD promoted an improvement of lymph cir-culation and worked in an adjunctive role for a significant reduc-tion of postoperative swelling and pain (Szolnoky et al., 2007).
Although KT has been increasingly used in the rehabilitationprotocols and prevention of sport injuries, there is no clear evi-dence regarding potential mechanisms underlying the beneficialeffects of KT. While promising anecdotal reports and case studiesexist, there is a need for evidence-based studies with good
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
methodological quality showing beneficial clinical effects (Williamset al., 2012). KT has a potential influence on the reduction ofswelling and haemorrhage.
Studies performed on the treatment of neoplastic or cancerrelated lymphoedema, have no evidence-based significance (Chouet al., 2012, Tsai et al., 2009).
To the best of our knowledge clinical studies using KT forpostoperative management of swelling, pain and trismus after ZOsurgery have not been performed. The results of this study showthat the application of KT after ZO surgery has a significant influ-ence on tissue reaction and swelling with an average cost for uni-lateral taping below one Euro per patient. The primary endpoint,increase of swelling was significantly lower for the KT group thanthe no-KT group. After operation the maximum swelling usuallyoccurs 2nd to 3rd day after operation, which goes along with theresults of our control group. However, using KTmean peak swellingwas reached after 0.5 days with significant lower values comparedto the no-KT group. Furthermore, reduction of swelling was fasterin the KT group compared to the no-KT group, decreasing theswelling bymore than 60% during the first 2 days after surgery. Thismight be due to KT stretch capabilities, thickness and adhesionallowing approximating the quality of the skin. The material usedfor KT is an elastic cotton tape with a non-allergenic head sensitiveadhesive layer. KT has been designed to allow 30e40% longitudinalstretch. By extending and rotating the muscles the skin of the areato be treated is stretched. KT is than applied to the skinwith a slightstretch.When the body parts return to their starting points the tape
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e8 7
subsequently recoils back to its original length following theapplication. This creates a pulling force to the skin forming con-volutions below the taped area (Fig. 8). It is believed that theseconvolutions increase the interstitial space between the skin andunderlying connective tissue, thus promoting the flow of blood andlymphatic fluid. In the head neck region, as performed in this study,changes in the length of tissue and the tape are extreme around aflexed, extended or rotated joint. Major convolutions could berecognized. As proposed by Shim et al. in a pilot animal study theseemerging wrinkles are not only indenting, but also elevating theskin (Shim et al., 2003). These investigators propose a positive ef-fect on the formation of lymph by opening micro valves in theinitial lymphatic vessels, therefore generating appropriate dynamicpressure variation and sufficient periodic compression anddecompression of superficial and deep initial lymphatics.
According to some investigators KT facilitates the decrease ofpain by pressure reduction on nociceptors (Kase et al., 1996). In thisstudy no reduction of pain for the KT group compared to the no-KTgroup was demonstrated. Other studies performed (Gonzalez-Iglesias et al., 2009; Thelen et al., 2008) are in agreement withthese findings. The results of this study show patients scoredmoderate pain or less in both groups (VAS < 5) for all six specificmeasurement times. This might be due to the standardized anal-gesic drug therapy protocol which both study groups receivedpostoperatively and during their hospital admission. In order tomake an evidenced statement, further investigation needs to beperformed, eliminating the standardized analgesic and providingrescue drugs.
Using KT, patients mouth opening increases faster after theoperation than in the no-KT group. These results are as seen in oursubjective findings. Patients in the KT group had higher satisfactionafter operation compared to the no-KT group. This might bebecause the swelling resolves faster, taking the tension from theskin. In addition, KT effect detracts from pain and perception.Movement stresses KT, it only partially adjusts its length to that ofthe skin, and thus deforms the skin. This constant stimulus stim-ulates the skin and diverts patients’ recognition, but our studydesign was not designed to exclude possible placebo effects causedby the KT.
Although friction resulting from the elasticity of the tape couldcause skin irritation and some adhesives might provoke allergies tosome patients, we had no incidence of adverse reactions in ourstudy, but these reactions should be considered for different typesof tape. To the best of our knowledge, there are no reported cases ofsevere allergic reaction to KT application.
The assessment of facial volume reduction is one of the biggestobstacles for an objective and reliable demonstration of a usedmethod. Numerous methods have been tried, most of which areimprecise, complex, expensive or difficult to standardize (Bjornet al., 1954; Milles et al., 1985; Van Gool et al., 1975). To quantifythe changes in facial volume we used a modified method of linearmeasurements in our study. By applying a series of data points, weutilized defined landmarks covering the whole facial area of in-terest. By marking segments endpoints, great care was taken toalways measure the same distances. Measurements were onlycarried out by one of the investigators thus reducing unwantedmeasurement variance.
5. Conclusion
The use of KT appears promising, because it is simple to carryout, less traumatic, economical, can be performed everywhere inthe world, free from side effects on the body. Even when swellingpersists, KT gives patients the impression of a minor swellingdetracting them from their pain and morbidity. Further studies
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
have to be performed to find out if KT can reduce or replace theneed for additional medications such as the use of steroids.
Financial disclosureThere was no financial support for this study by any company.
All K-Active Tapes� used in this study were donated by the K-ActiveEurope GmbH.
Conflicts of interestWe declare that we have no conflicts of interest.
Acknowledgements
We thank the K-Active Europe GmbH for the donation of all K-Active Tapes� used in this study. This research project is part of thedoctoral thesis of Katharina Schwärzler.
References
Al-Khateeb TH, Nusair Y: Effect of the proteolytic enzyme serrapeptase on swelling,pain and trismus after surgical extraction of mandibular third molars. Int J OralMaxillofac Surg 37: 264e268, 2008
Andreasen JO, Jensen SS, Schwartz O, Hillerup Y: A systematic review of prophy-lactic antibiotics in the surgical treatment of maxillofacial fractures. J OralMaxillofac Surg 64: 1664e1668, 2006
Assimes TL, Lessard ML: The use of perioperative corticosteroids in craniomax-illofacial surgery. Plast Reconstr Surg 103: 313e321, 1999 quiz 322
Aznar-Arasa L, Harutunian K, Figueiredo R, Valmaseda-Castellon E, Gay-Escoda C:Effect of preoperative ibuprofen on pain and swelling after lower third molarremoval: a randomized controlled trial. Int J Oral Maxillofac Surg 41: 1005e1009, 2012
Bjorn H, Lundqvist C, Hjelmstrom P: A photogrammetric method of measuring thevolume of facial swellings. J Dent Res 33: 295e308, 1954
Buyukkurt MC, Gungormus M, Kaya O: The effect of a single dose prednisolone withand without diclofenac on pain, trismus, and swelling after removal ofmandibular third molars. J Oral Maxillofac Surg 64: 1761e1766, 2006
Calderoni DR, Guidi Mde C, Kharmandayan P, Nunes PH: Seven-year institutionalexperience in the surgical treatment of orbito-zygomatic fractures.J Craniomaxillofac Surg 39: 593e599, 2011
Chou YH, Li SH, Liao SF, Tang HW: Case report: manual lymphatic drainage andkinesio taping in the secondary malignant breast cancer-related lymphedemain an arm with arteriovenous (A-V) fistula for hemodialysis. Am J Hosp PalliatCare, 2012, PMID: 22879520. [Epub ahead of print].
de Sousa Santos JA, da Silva LC, de Santana Santos T, Menezes Junior LR, deAssuncao Oliveira AC, Brandao JR: Comparative study of tramadol combinedwith dexamethasone and diclofenac sodium in third-molar surgery.J Craniomaxillofac Surg 40: 694e700, 2012
Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D, et al:A retrospective analysis of facial fracture etiologies. Ann Plast Surg 60: 398e403, 2008
Folkestad L, Aberg-Bengtsson L, Granstrom G: Recovery from orbital floor fractures:a prospective study of patients’ and doctors’ experiences. Int J Oral MaxillofacSurg 35: 499e505, 2006
Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H: Cranio-maxillofacial trauma: a 10year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 31: 51e61, 2003
Gonzalez-Iglesias J, Fernandez-de-Las-Penas C, Cleland JA, Huijbregts P, Del RosarioGutierrez-Vega M: Short-term effects of cervical kinesio taping on pain andcervical range of motion in patients with acute whiplash injury: a randomizedclinical trial. J Orthop Sports Phys Ther 39: 515e521, 2009
Greenstein G: Therapeutic efficacy of cold therapy after intraoral surgical pro-cedures: a literature review. J Periodontol 78: 790e800, 2007
Grossi GB, Maiorana C, Garramone RA, Borgonovo A, Beretta M, Farronato D, et al:Effect of submucosal injection of dexamethasone on postoperative discomfortafter third molar surgery: a prospective study. J Oral Maxillofac Surg 65: 2218e2226, 2007
Kase K, Hashimoto T, Tomoki O: Development of kinesio taping perfect manual.Kinesio Taping Association, 1996
Kase K, Wallis J, Kase T: Clinical therapeutic applications of the kinesio tapingmethod, 2nd edn. Tokyo: Ken Ikai Co. Ltd., 2003
Kim K, Brar P, Jakubowski J, Kaltman S, Lopez E: The use of corticosteroids andnonsteroidal antiinflammatory medication for the management of pain andinflammation after third molar surgery: a review of the literature. Oral SurgOral Med Oral Pathol Oral Radiol Endod 107: 630e640, 2009
Knepil GJ, Loukota RA: Outcomes of prophylactic antibiotics following surgery forzygomatic bone fractures. J Craniomaxillofac Surg 38: 131e133, 2010
Markiewicz MR, Brady MF, Ding EL, Dodson TB: Corticosteroids reduce post-operative morbidity after third molar surgery: a systematic review and meta-analysis. J Oral Maxillofac Surg 66: 1881e1894, 2008
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043

O. Ristow et al. / Journal of Cranio-Maxillo-Facial Surgery xxx (2013) 1e88
Markovic A, Todorovic L: Effectiveness of dexamethasone and low-power laser inminimizing oedema after third molar surgery: a clinical trial. Int J Oral Max-illofac Surg 36: 226e229, 2007
Milles M, Desjardins PJ, Pawel HE: The facial plethysmograph: a new instrument tomeasure facial swelling volumetrically. J Oral Maxillofac Surg 43: 346e352,1985
Miloro M: Peterson’s principles of oral an maxillofacial surgery. Canada: BC DeckerInc, 2004
Morris D, Jones D, Ryan H, Ryan CG: The clinical effects of kinesio� tex taping: Asystematic review. Physiother Theory Pract 29(4): 259e270, 2013
Naveen Shankar A, Naveen Shankar V, Hegde N, Sharma, Prasad R: The pattern ofthe maxillofacial fractures e a multicentre retrospective study.J Craniomaxillofac Surg 40: 675e679, 2012
Osunde OD, Adebola RA, Omeje UK: Management of inflammatory complications inthird molar surgery: a review of the literature. Afr Health Sci 11: 530e537, 2011
Rana M, Gellrich NC, Ghassemi A, Gerressen M, Riediger D, Modabber A: Three-dimensional evaluation of postoperative swelling after third molar surgeryusing 2 different cooling therapy methods: a randomized observer-blind pro-spective study. J Oral Maxillofac Surg 69: 2092e2098, 2011
Rana M, Gellrich NC, von See C, Weiskopf C, Gerressen M, Ghassemi A, et al: 3Devaluation of postoperative swelling in treatment of bilateral mandibularfractures using 2 different cooling therapy methods: A randomized observerblind prospective study. J Craniomaxillofac Surg 41(1): e17e23, 2013
Rogers SN, Naylor R, Potter L, Magennis P: Three years’ experience of collaborativecare pathways on a maxillofacial ward. Br J Oral Maxillofac Surg 38: 132e137,2000
Roynesdal AK, Bjornland T, Barkvoll P, Haanaes HR: The effect of soft-laser appli-cation on postoperative pain and swelling. A double-blind, crossover study. Int JOral Maxillofac Surg 22: 242e245, 1993
Please cite this article in press as: Ristow O, et al., Influence of kinesiologiorbital fractures, Journal of Cranio-Maxillo-Facial Surgery (2013), http://d
Samad TA, Moore KA, Sapirstein A, Billet S, Allchorne A, Poole S, et al: Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory painhypersensitivity. Nature 410: 471e475, 2001
Shim JY, Lee HR, Lee DC: The use of elastic adhesive tape to promote lymphatic flowin the rabbit hind leg. Yonsei Med J 44: 1045e1052, 2003
Szolnoky G, Szendi-Horvath K, Seres L, Boda K, Kemeny L: Manual lymph drainageefficiently reduces postoperative facial swelling and discomfort after removal ofimpacted third molars. Lymphology 40: 138e142, 2007
Thelen MD, Dauber JA, Stoneman PD: The clinical efficacy of kinesio tape forshoulder pain: a randomized, double-blinded, clinical trial. J Orthop Sports PhysTher 38: 389e395, 2008
Thoren H, Snall J, Kormi E, Numminen L, Fah R, Iizuka T, et al: Does perioperativeglucocorticosteroid treatment correlate with disturbance in surgical woundhealing after treatment of facial fractures? A retrospective study. J Oral Max-illofac Surg 67: 1884e1888, 2009
Trivellato PF, Arnez MF, Sverzut CE, Trivellato AE: A retrospective study ofzygomatico-orbital complex and/or zygomatic arch fractures over a 71-monthperiod. Dent Traumatol 27: 135e142, 2011
Tsai HJ, Hung HC, Yang JL, Huang CS, Tsauo JY: Could kinesio tape replace thebandage in decongestive lymphatic therapy for breast-cancer-related lymphe-dema? A pilot study. Support Care Cancer 17: 1353e1360, 2009
van den Bergh B, Karagozoglu KH, Heymans MW, Forouzanfar T: Aetiology andincidence of maxillofacial trauma in Amsterdam: a retrospective analysis of 579patients. J Craniomaxillofac Surg 40: e165e169, 2012
Van Gool AV, Ten Bosch JJ, Boering G: A photographic method of assessing swellingfollowing third molar removal. Int J Oral Surg 4: 121e129, 1975
Williams S, Whatman C, Hume PA, Sheerin K: Kinesio taping in treatment andprevention of sports injuries: a meta-analysis of the evidence for its effective-ness. Sports Med 42: 153e164, 2012
c tape on postoperative swelling, pain and trismus after zygomatico-x.doi.org/10.1016/j.jcms.2013.05.043