Embed Size (px)
Citation preview
![Page 1: Journal of Cardiology Cases - COnnecting REpositories · de pointes with solifenacin in an 81-year-old women. Br J Clin Pharmacol 2008;66:896–7. [10] Daubert GP, Mabasa VH, Leung](https://reader034.pdfslide.us/reader034/viewer/2022042413/5f2cbc8f3bf913100d55a5cf/html5/thumbnails/1.jpg)
C
Tc
TSa
b
c
a
ARRA
KTQSCI
I
sctnlwpfnioa
C
o
O3
1h
Journal of Cardiology Cases 9 (2014) 91–93
Contents lists available at www.sciencedirect.com
Journal of Cardiology Cases
journa l h om epage: www.elsev ier .com/ locate / j ccase
ase Report
orsade de pointes associated with the combination of solifenacin andlenbuterol for urinary incontinence
oru Kato (MD)a,∗, Taichi Adachi (MD)b, Kazuhiko Takano (MD)c, Toru Kamijima (MD)c,higeru Toyoda (MD, FJCC)c, Isao Taguchi (MD, FJCC)c, Teruo Inoue (MD, FJCC)c
Department of Clinical Research, National Hospital Organization Tochigi Medical Center, Utsunomiya, Tochigi, JapanDepartment of Cardiovascular Medicine, National Hospital Organization Tochigi Medical Center, Utsunomiya, Tochigi, JapanDepartment of Cardiovascular Medicine, Dokkyo Medical University, Mibu, Tochigi, Japan
r t i c l e i n f o
rticle history:eceived 20 June 2013eceived in revised form 8 October 2013ccepted 11 October 2013
eywords:
a b s t r a c t
A 79-year-old woman undergoing medical treatment with solifenacin and clenbuterol for urinary incon-tinence was admitted to our hospital because of recurrent syncope. Her syncope appeared one monthafter the doses of clenbuterol were increased. Torsade de pointes (TdP) was evident on her Holter electro-cardiogram at the time when she developed syncope. Ultimately, a cardioverter-defibrillator with dualchamber pacing capability was implanted. To our knowledge, this is the first report of TdP associated
orsade de pointesT prolongationolifenacinlenbuterol
mplantable cardioverter-defibrillator
with the combination of solifenacin and clenbuterol for urinary incontinence.<Learning objective: Urinary incontinence increases with age. Muscarinic receptor antagonists are con-sidered the mainstay of pharmacologic treatment for this condition. Some patients might be treatedwith a combination of a bladder selective muscarinic receptor antagonist solifenacin and a long-acting�2 adrenergic agonist clenbuterol. However, this combination therapy may cause torsade de pointes with
Jap
syncope.>© 2013
ntroduction
Torsade de pointes (TdP) occurs in several clinical settingsuch as drug treatment and inherited abnormalities of cardiac ionhannels and can be fatal. This condition is associated with ven-ricular action potential prolongation, which can be recognizedon-invasively on the electrocardiogram (ECG) by QT interval pro-
ongation. TdP may be caused by some non-cardiac drugs [1–3] asell as antiarrhythmic drugs [4]. Not only do drugs differ in theirotential to cause TdP, but also there are several other risk factorsor drug-induced TdP such as female sex, hypokalemia, hypomag-esemia, bradycardia, simultaneous administration of metabolic
nhibitors, and genetic factors [1,5–7]. Here, we report a rare casef TdP that appeared to be caused by the combination of solifenacinnd clenbuterol to treat urinary incontinence.
ase report
A 79-year-old woman was admitted to our hospital becausef recurrent syncope. She had been treated for two years with
∗ Corresponding author at: Department of Clinical Research, National Hospitalrganization Tochigi Medical Center, 1-10-37 Naka-Tomatsuri, Utsunomiya, Tochigi20-8580, Japan. Tel.: +81 286 22 5241; fax: +81 286 22 1011.
E-mail address: [email protected] (T. Kato).
878-5409/$ – see front matter © 2013 Japanese College of Cardiology. Published by Elsettp://dx.doi.org/10.1016/j.jccase.2013.10.009
anese College of Cardiology. Published by Elsevier Ltd. All rights reserved.
5 mg/day solifenacin in combination with 20 �g/day clenbuterolfor urinary incontinence. One year before admission, the dose ofsolifenacin was increased to 10 mg/day, and one month beforeadmission, the dose of clenbuterol was increased to 40 �g/day.After an increase in solifenacin dose from 5 to 10 mg/day, QTcinterval slightly increased from 419 ms to 428 ms. After an addi-tional increase in clenbuterol dose from 20 to 40 �g/day, more QTcprolongation was observed from 428 ms to 442 ms. Thereafter, shedeveloped recurrent syncope. At the time of admission, her 12-leadECG showed no P waves and a regular atrioventricular junctionalrhythm with QTc 442 ms (Fig. 1). Serum levels of electrolytes andhepatic function were normal, but her creatinine clearance wasslightly decreased. The echocardiogram showed no structural heartdisease. After hospitalization, the ECG monitor showed frequentpremature ventricular contractions (PVCs) with short runs. TdPwas evident on the Holter ECG at the time she developed syncope(Fig. 2). Just before the occurrence of TdP, the T wave was biphasic inshape with prolonged QTc interval to 560 ms (Fig. 2). We believedthat the increase in the dose of solifenacin and clenbuterol wasthe cause of TdP. Therefore, we discontinued these two medica-tions and prescribed amiodarone (100 mg; 12 h apart) for the first24 h. Thereafter, the ECG monitor showed a decrease in the fre-
quency of PVCs. Her heart rate decreased to 40/min, and to preventmore QTc prolongation, amioradone was discontinued. QTc intervaldecreased to 438 ms after withdrawing these drugs. She was at highrisk for sudden death, therefore, a cardioverter-defibrillator withvier Ltd. All rights reserved.
![Page 2: Journal of Cardiology Cases - COnnecting REpositories · de pointes with solifenacin in an 81-year-old women. Br J Clin Pharmacol 2008;66:896–7. [10] Daubert GP, Mabasa VH, Leung](https://reader034.pdfslide.us/reader034/viewer/2022042413/5f2cbc8f3bf913100d55a5cf/html5/thumbnails/2.jpg)
92 T. Kato et al. / Journal of Cardiology Cases 9 (2014) 91–93
and a
dtc
D
u
Fj(
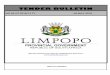
Fig. 1. The 12-lead electrocardiogram at the time of admission showed no P waves
ual chamber pacing capability was implanted. After the implan-ation of a cardioverter-defibrillator with dual chamber pacingapability, she was free from syncope.
iscussion
Solifenacin, a bladder-selective antimuscarinic drug, is widelysed for the treatment of urinary incontinence [8]. Solifenacin has
ig. 2. The Holter electrocardiogram showed torsade de pointes (TdP), at this time, she sudust before the occurrence of TdP was observed: TdP is induced by the short-long cardiacPVC). The initiating PVC appears after the T-wave peak of the last beat before the onset o
regular atrioventricular junctional rhythm with slight QTc prolongation (442 ms).
not been shown to have severe adverse cardiac effects, althoughanother antimuscarinic agent, telodiline, has been reported tocause QT prolongation and TdP [2,3,8]. However, Asajima et al.[9] reported a case of solifenacin-induced TdP associated with
QT prolongation. The case was an 81-year-old woman who wason 5 mg/day solifenacin when TdP appeared. Clenbuterol, a long-acting �2-adrenergic agonist, is also used for the treatment ofurinary incontinence. Clenbuterol also has not been reported todenly developed syncope for a few seconds. A short-long-short pattern of R–R cycles cycles followed by an initiating short-coupled premature ventricular contractionf TdP.
![Page 3: Journal of Cardiology Cases - COnnecting REpositories · de pointes with solifenacin in an 81-year-old women. Br J Clin Pharmacol 2008;66:896–7. [10] Daubert GP, Mabasa VH, Leung](https://reader034.pdfslide.us/reader034/viewer/2022042413/5f2cbc8f3bf913100d55a5cf/html5/thumbnails/3.jpg)
ardiolo
hta
fcwrccaoalCpsdnoo
Hpddfpbd
tn
M
taT
T. Kato et al. / Journal of C
ave severe cardiac adverse effects except for supraventricularachycardia and atrial fibrillation in a body builder who took ancute overdose [10].
The combination of solifenacin and clenbuterol is often usedor the treatment of urinary incontinence. In our case, syn-ope appeared after the doses of solifenacin and clenbuterolere increased from 5 to 10 mg/day and from 20 to 40 �g/day,
espectively. Based on previous reports, solifenacin rather thanlenbuterol might have been the drug responsible for TdP asso-iated with QT prolongation. However, a drug–drug interaction islso an important issue that should be considered. The metabolismf solifenacin occurs via CYP3A4 [8], so its combination with othergents that potentially inhibit CYP3A4 could increase solifenacinevels resulting in adverse effects. However, clenbuterol is not aYP3A4 inhibitor. Furthermore, no structural heart disease wasresent, serum electrolytes levels such as potassium and magne-ium and hepatic function were normal, and age and mild renalysfunction had no clinically relevant effects on the pharmacoki-etics of solifenacin. Therefore, we speculate that the combinationf solifenacin with clenbuterol had an impact on the developmentf TdP, although the exact mechanism is unknown.
In our case, amiodarone was effective in preventing TdP.owever, amiodarone induced bradycardia and might cause QTcrolongation with increasing the risk of TdP, so we were obliged toiscontinue amiodarone. After the implantation of a cardioverter-efibrillator with dual chamber pacing capability, she was freerom syncope. Although we did not investigate genetic factors andlasma drug concentrations in this case, these approaches woulde a sound strategy to evaluate the potential adverse effects of herrug therapy.
To our knowledge, this is the first report of TdP associated withhe combination of solifenacin and clenbuterol for urinary inconti-ence.
ultiple authorship
All authors of this paper listed have participated sufficiently inhe conception and design of the work, in the analysis of the data,nd in writing the manuscript to take public responsibility for it.
Kato and T Adachi designed the work. K Takano, T Kamijima, S
[
gy Cases 9 (2014) 91–93 93
Toyoda, and T Taguchi analyzed the data. T Kato and T Inoue wrotethe manuscript. All authors revised this manuscript.
Ethics standards
The institute’s ethical committee approved the access to thispatient’s records.
Conflict of interest
All authors disclose no financial and personal relationships withother people or organizations that could inappropriately influence(bias) the work.
Acknowledgments
None of the authors have potential conflicts to declare that couldinappropriately influence the results.
References
[1] Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med2004;350:1013–22.
[2] Cannolly MJ, Astridge PS, White EG, Morley CA, Cowan JC. Torsade de pointesventricular tachycardia and terodiline. Lancet 1991;33:344–5.
[3] McLeod AA, Thorogood S, Barnett S. Torsade de pointes complicating treatmentwith terodiline. BMJ 1991;302:1469.
[4] Waldo AL, Camm AJ, de Ruyder H, Friedman PL, MacNeil DJ, Pauls JF, Pitt B, PrattCM, Schwartz PJ, Veltri EP. Effect of d-sotalol on mortality in patients with leftventricular dysfunction after recent and remote myocardial infarction. Lancet1996;348:7–12.
[5] Dmochowski R, Staskin DR. The QT interval and antimuscarinic drugs. Curr UrolRep 2005;6:405–9.
[6] Takaya T, Okamoto M, Yodoi K, Hata K, Kijima Y, Nakajima H, Nishikawa Y, KitaT, Ito M, Seo T, Kawashima S. Torsades de Pointes with QT prolongation relatedto donepezil use. J Cardiol 2009;54:507–11.
[7] Gupta A, Lawrence AT, Krisnan K, Kavinsky CJ, Trohman RG. Current conceptsin the mechanisms and management of drug-induced QT prolongation andtorsade de pointes. Am Heart J 2007;153:891–9.
[8] Payne CK. Solifenacin in overactive bladder syndrome. Drugs 2006;66:175–90.[9] Asajima H, Sekiguchi Y, Matsushima S, Saito N, Saito T. QT prolongation and tor-
sade de pointes with solifenacin in an 81-year-old women. Br J Clin Pharmacol2008;66:896–7.
10] Daubert GP, Mabasa VH, Leung VW, Aaron C. Acute clenbuterol overdoseresulting in supraventricular tachycardia and atrial fibrillation. J Med Toxicol2007;3:56–60.





![Women’s Health Specialist Library · Sustained release oxybutynin transdermal patches, which release 3.9mg every 24 hours, have recently been launched in the UK [5,6,7]. Solifenacin](https://img.pdfslide.us/doc/110x75/5f5e427aea0ab4371b653ee0/womenas-health-specialist-library-sustained-release-oxybutynin-transdermal-patches.jpg)