Embed Size (px)
Citation preview

1Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Telithromycin-Associated Telithromycin-Associated HepatotoxicityHepatotoxicity
Telithromycin-Associated Telithromycin-Associated HepatotoxicityHepatotoxicity
Allen Brinker, MD, MSEpidemiology Team Leader
Division of Drug Risk Evaluation (DDRE)
Office of Surveillance and Epidemiology (OSE)
Allen Brinker, MD, MSEpidemiology Team Leader
Division of Drug Risk Evaluation (DDRE)
Office of Surveillance and Epidemiology (OSE)

2Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Telithromycin-Associated Acute Liver Failure Telithromycin-Associated Acute Liver Failure (ALF) and Clinically Significant Liver Injury(ALF) and Clinically Significant Liver Injury
Telithromycin-Associated Acute Liver Failure Telithromycin-Associated Acute Liver Failure (ALF) and Clinically Significant Liver Injury(ALF) and Clinically Significant Liver Injury
• Outline of Speakers– Allen Brinker, MD (FDA)
• Case material / DDRE signal assessment– Leonard Seeff, MD
• Expert Consultant for FDA• Principles of ALF causality assessment
– William Lee, MD• Expert Consultant for FDA• Telithromycin ALF causality assessment
• Outline of Speakers– Allen Brinker, MD (FDA)
• Case material / DDRE signal assessment– Leonard Seeff, MD
• Expert Consultant for FDA• Principles of ALF causality assessment
– William Lee, MD• Expert Consultant for FDA• Telithromycin ALF causality assessment

3Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Telithromycin-Associated ALFTelithromycin-Associated ALFOverviewOverview
Telithromycin-Associated ALFTelithromycin-Associated ALFOverviewOverview
• Summarize DDRE review• Methods
– spontaneous adverse event (MedWatch) reports
• Analysis of cases• Pharmacoepidemiology
• Reporting rates• Two supporting ALF reporting rate analyses• Telithromycin ALF reporting rate analysis
• Conclusions and status as of September 2006
• Summarize DDRE review• Methods
– spontaneous adverse event (MedWatch) reports
• Analysis of cases• Pharmacoepidemiology
• Reporting rates• Two supporting ALF reporting rate analyses• Telithromycin ALF reporting rate analysis
• Conclusions and status as of September 2006

4Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Summary of DDRE AnalysisSummary of DDRE AnalysisTelithromycin-Associated ALFTelithromycin-Associated ALFSummary of DDRE AnalysisSummary of DDRE Analysis
Telithromycin-Associated ALFTelithromycin-Associated ALF
• Spectrum of injury• Per FDA review, 12 cases of telithromycin-
associated ALF “clinically remarkable”– Short time-to-onset (median 4 days)
• One case following first dose– Profound hepatic injury– 4 deaths
• 1 transplant– Patients appeared healthy and with few
confounding factors
• Spectrum of injury• Per FDA review, 12 cases of telithromycin-
associated ALF “clinically remarkable”– Short time-to-onset (median 4 days)
• One case following first dose– Profound hepatic injury– 4 deaths
• 1 transplant– Patients appeared healthy and with few
confounding factors

5Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Summary of DDRE AnalysisSummary of DDRE AnalysisTelithromycin-Associated ALFTelithromycin-Associated ALFSummary of DDRE AnalysisSummary of DDRE Analysis
Telithromycin-Associated ALFTelithromycin-Associated ALF
• Reporting rate for telithromycin-associated ALF similar ALF reporting rates for selected comparators (moxi-, gatifloxacin) given variation inherent in spontaneous adverse event reporting
• Reporting rate for telithromycin-associated ALF similar ALF reporting rates for selected comparators (moxi-, gatifloxacin) given variation inherent in spontaneous adverse event reporting

6Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Summary of DDRE AnalysisSummary of DDRE AnalysisTelithromycin-Associated ALFTelithromycin-Associated ALFSummary of DDRE AnalysisSummary of DDRE Analysis
Telithromycin-Associated ALFTelithromycin-Associated ALF
• Recommended regulatory actions consistent with actions advanced for the fluoroquinolones
• Review of this analysis included
• DDRE recommendations realized with addition of WARNING for ALF within approved labeling for telithromycin - June 2006
• Recommended regulatory actions consistent with actions advanced for the fluoroquinolones
• Review of this analysis included
• DDRE recommendations realized with addition of WARNING for ALF within approved labeling for telithromycin - June 2006

7Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Summary of DDRE AnalysisSummary of DDRE AnalysisTelithromycin-Associated ALFTelithromycin-Associated ALFSummary of DDRE AnalysisSummary of DDRE Analysis
Telithromycin-Associated ALFTelithromycin-Associated ALF
• Set a reporting rate level (bar) for further regulatory action for telithromycin– based on experience with trovafloxacin-
associated ALF• Review of this analysis included
• Set a reporting rate level (bar) for further regulatory action for telithromycin– based on experience with trovafloxacin-
associated ALF• Review of this analysis included

8Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
MethodsMethods
Spontaneous Adverse Event ReportsSpontaneous Adverse Event Reports
MethodsMethods
Spontaneous Adverse Event ReportsSpontaneous Adverse Event Reports

9Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Spontaneous Adverse Event ReportsSpontaneous Adverse Event Reports Spontaneous Adverse Event ReportsSpontaneous Adverse Event Reports
• “MedWatch reports”
• Designed to detect– Rare– Serious– Unexpected
• Substantial variation in quality and information report to report
• “MedWatch reports”
• Designed to detect– Rare– Serious– Unexpected
• Substantial variation in quality and information report to report

10Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Spontaneous Adverse Event ReportsSpontaneous Adverse Event ReportsSpontaneous Adverse Event ReportsSpontaneous Adverse Event Reports
• Fraction of incident adverse events attributable to a selected drug AND reported is unknown
• Estimates of 1% to 10% commonly cited– These are likely to be overestimates– Assume variation between products
• Fraction of incident adverse events attributable to a selected drug AND reported is unknown
• Estimates of 1% to 10% commonly cited– These are likely to be overestimates– Assume variation between products

11Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Spontaneous Adverse Event ReportsSpontaneous Adverse Event ReportsSpontaneous Adverse Event ReportsSpontaneous Adverse Event Reports
• Three DDRE reviews of antibiotic-associated ALF– Separated in time and by authors
• Utilized generally similar case definitions– Totality of information could not exclude
telithromycin as a factor in liver injury• Typical for FDA case series
– Inclusion “case” criteria– Exclusion “confounding” criteria
• Three DDRE reviews of antibiotic-associated ALF– Separated in time and by authors
• Utilized generally similar case definitions– Totality of information could not exclude
telithromycin as a factor in liver injury• Typical for FDA case series
– Inclusion “case” criteria– Exclusion “confounding” criteria
12Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE review of telithromycin-Associated DDRE review of telithromycin-Associated ALFALF
DDRE review of telithromycin-Associated DDRE review of telithromycin-Associated ALFALF
• Conducted January - May 2006
– Ron Wassel and Allen Brinker
– Telithromycin market appearance - July 2004
• Conducted January - May 2006
– Ron Wassel and Allen Brinker
– Telithromycin market appearance - July 2004
13Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Ongoing review– Initial review (June 2005)
• Continued monitoring– Annals of Internal Medicine
• January 2006• Three patients who experienced serious
liver toxicity following administration of telithromycin
– Concern for hepatotoxicity observed in controlled clinical trials
• Ongoing review– Initial review (June 2005)
• Continued monitoring– Annals of Internal Medicine
• January 2006• Three patients who experienced serious
liver toxicity following administration of telithromycin
– Concern for hepatotoxicity observed in controlled clinical trials
14Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Identified cases of:
– Acute Liver Failure (ALF)
– Acute Serious Liver Injury (ASLI)
• Identified cases of:
– Acute Liver Failure (ALF)
– Acute Serious Liver Injury (ASLI)

15Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE review of telithromycin-DDRE review of telithromycin-associated ALFassociated ALF
DDRE review of telithromycin-DDRE review of telithromycin-associated ALFassociated ALF
• Acute Liver Failure (ALF) defined as a report describing:– diagnosis of acute “liver failure,” or– acute and severe liver injury with
encephalopathy, or– liver transplant following acute illness, or– death in the setting of acute severe liver
injury
• Acute Liver Failure (ALF) defined as a report describing:– diagnosis of acute “liver failure,” or– acute and severe liver injury with
encephalopathy, or– liver transplant following acute illness, or– death in the setting of acute severe liver
injury

16Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Acute Serious Liver Injury (ASLI) defined as a report of:– hepatic transaminase elevations, or– hyperbilirubinemia, or– clinical jaundice
• leading to hospitalization
• Acute Serious Liver Injury (ASLI) defined as a report of:– hepatic transaminase elevations, or– hyperbilirubinemia, or– clinical jaundice
• leading to hospitalization
17Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Exclusion criteria included:– “Hearsay” reports– Infectious hepatitis– Sepsis– Pancreatitis– Rhabdomyolysis– Cancer– Selected concomitant therapies
• Exclusion criteria included:– “Hearsay” reports– Infectious hepatitis– Sepsis– Pancreatitis– Rhabdomyolysis– Cancer– Selected concomitant therapies

18Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• 110 unduplicated, domestic reports of liver injury in association with telithromycin
• Excluded 31 as confounded or hearsay reports
• Excluded 44 as minor liver injury• 23 cases of Acute Serious Liver Injury• 12 cases of Acute Liver Failure
• 110 unduplicated, domestic reports of liver injury in association with telithromycin
• Excluded 31 as confounded or hearsay reports
• Excluded 44 as minor liver injury• 23 cases of Acute Serious Liver Injury• 12 cases of Acute Liver Failure

19Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Causality assessment project– 2 FDA + 3 expert consultants– Review of 109 unduplicated, domestic reports
of liver injury with telithromycin by Seeff• 38 cases as very likely, possible or probable• 12 cases “ALF” or “ASLI” per DDRE review• 3 cases from DILIN network
– Reviewed 53 cases in total
• Causality assessment project– 2 FDA + 3 expert consultants– Review of 109 unduplicated, domestic reports
of liver injury with telithromycin by Seeff• 38 cases as very likely, possible or probable• 12 cases “ALF” or “ASLI” per DDRE review• 3 cases from DILIN network
– Reviewed 53 cases in total
20Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
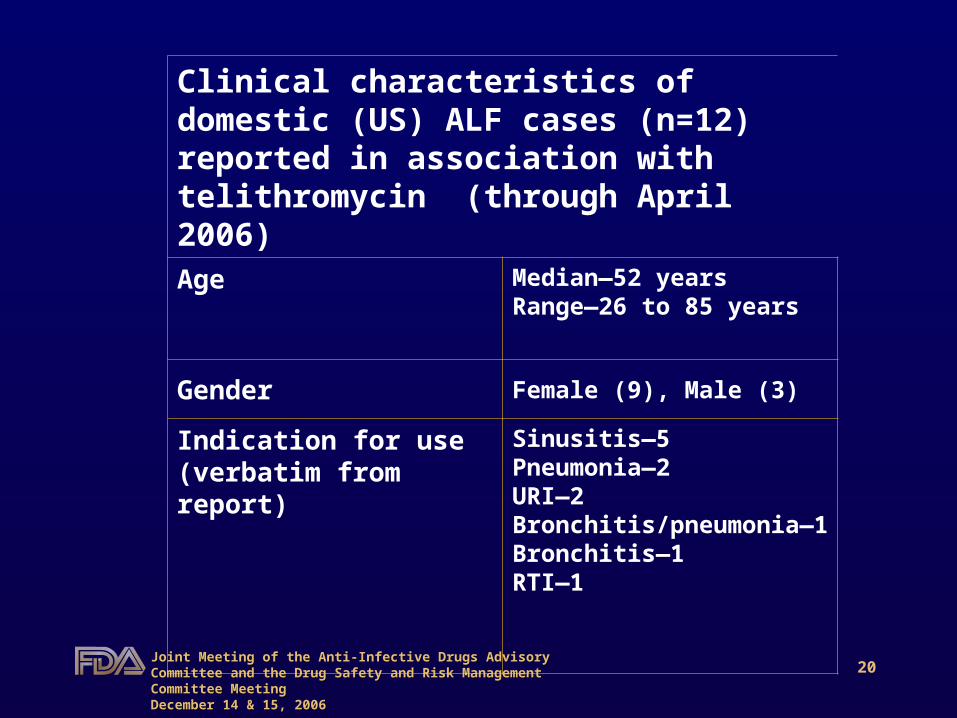
Clinical characteristics of domestic (US) ALF cases (n=12) reported in association with telithromycin (through April 2006)
Age Median—52 yearsRange—26 to 85 years
Gender Female (9), Male (3)
Indication for use (verbatim from report)
Sinusitis—5Pneumonia—2URI—2Bronchitis/pneumonia—1Bronchitis—1RTI—1

21Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Clinical characteristics of domestic (US) ALF cases (n=12) reported in association with telithromycin through April 2006.
continued
Latency (time to onset of symptoms from initiation of treatment)
Median—4 days Range—1 to 20 days
Jaundice reported at Dx 8
Highest reported bilirubin (mg/dL) Median—18.3Range—1.7 to 24.3
Highest reported AST (IU/L) Median—3638Range—812 to 34,423
Highest reported ALT (IU/L) Median—2489Range—833 to 19,888
Death / transplant 4 / 1

DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
AERS # 4892304-3 51 year old female(North Carolina)
PMHx-Non significant; Current meds-ASA, MVit, Vit Eno prior hx of liver diseasesocial drinker (up to 2-3 glasses wine/day)
Received telithromycin after presentation to her PCP with 2 wk h/o symptoms c/w URI. Developed icterus and elevated liver enzymes, bilirubin, and PT 7 days after initiation of therapy with telithromycin; alk phos only mildly elevated. Negative for hepatitis A, B, and C. Abdominal US that showed a small, echogenic liver with ascites. One month later bili increased; listed for liver transplant. Subsequently pt readmitted with systemic symptoms and underwent liver transplant. Explanted liver was small and remarkable for massive necrosis on histologic examination.
**As published within: Clay KD, Hanson JS, Pope SD, et al. Brief communication: severe hepatotoxicity of telithromycin: three case reports and literature review. Ann Intern Med 2006;144(6):415-20.
AERS # 4892304-3 51 year old female(North Carolina)
PMHx-Non significant; Current meds-ASA, MVit, Vit Eno prior hx of liver diseasesocial drinker (up to 2-3 glasses wine/day)
Received telithromycin after presentation to her PCP with 2 wk h/o symptoms c/w URI. Developed icterus and elevated liver enzymes, bilirubin, and PT 7 days after initiation of therapy with telithromycin; alk phos only mildly elevated. Negative for hepatitis A, B, and C. Abdominal US that showed a small, echogenic liver with ascites. One month later bili increased; listed for liver transplant. Subsequently pt readmitted with systemic symptoms and underwent liver transplant. Explanted liver was small and remarkable for massive necrosis on histologic examination.
**As published within: Clay KD, Hanson JS, Pope SD, et al. Brief communication: severe hepatotoxicity of telithromycin: three case reports and literature review. Ann Intern Med 2006;144(6):415-20.
23Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
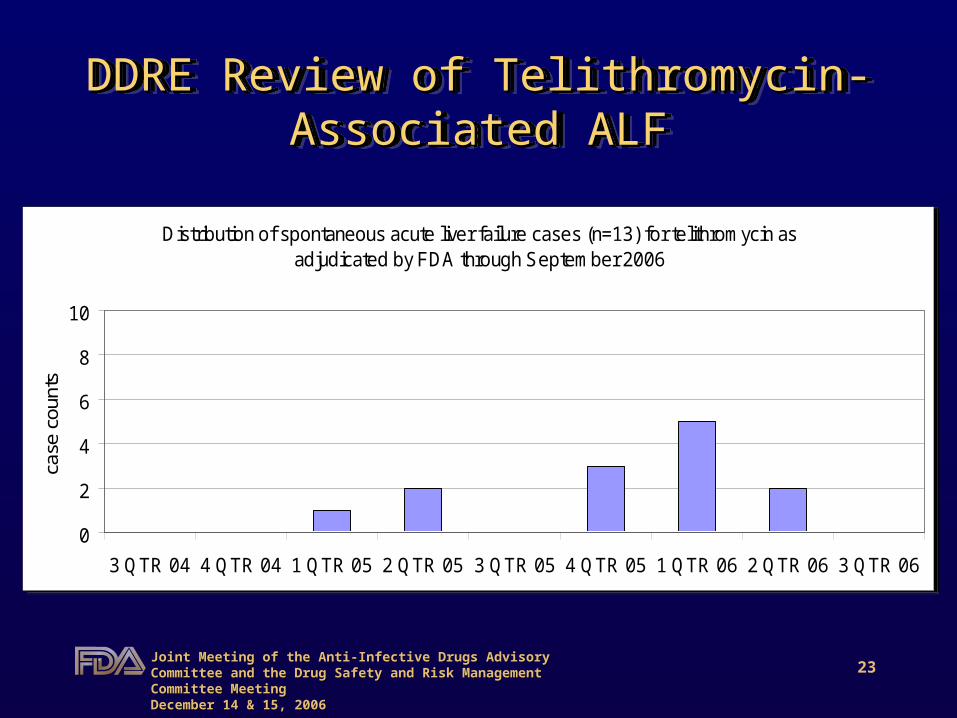
Distribution of spontaneous acute liver failure cases (n=13) for telithromycin as adjudicated by FDA through September 2006
0
2
4
6
8
10
3 QTR 04 4 QTR 04 1 QTR 05 2 QTR 05 3 QTR 05 4 QTR 05 1 QTR 06 2 QTR 06 3 QTR 06
case
cou
nts
Distribution of spontaneous acute liver failure cases (n=13) for telithromycin as adjudicated by FDA through September 2006
0
2
4
6
8
10
3 QTR 04 4 QTR 04 1 QTR 05 2 QTR 05 3 QTR 05 4 QTR 05 1 QTR 06 2 QTR 06 3 QTR 06
case
cou
nts
24Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Case material sufficient for addition of serious liver injury including ALF to telithromycin label
• What is risk compared to similar agents?– Reporting rates
• Two supporting analyses
• Case material sufficient for addition of serious liver injury including ALF to telithromycin label
• What is risk compared to similar agents?– Reporting rates
• Two supporting analyses

25Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
PharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiology
• Reporting rates
– Drug-against-drug comparisons– Observed versus expected comparisons
• Reporting rates
– Drug-against-drug comparisons– Observed versus expected comparisons

26Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
PharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiology
• Reporting rates calculated as:
Spontaneous cases of selected event-----------------------------------------------------------
exposure or utilization
– Expressed as:• Cases per million Rx, per 10 million Rx• Incidence density (cases per unit person-
time)– Typically restricted to cases that arise during
oral (ambulatory) therapy.
• Reporting rates calculated as:
Spontaneous cases of selected event-----------------------------------------------------------
exposure or utilization
– Expressed as:• Cases per million Rx, per 10 million Rx• Incidence density (cases per unit person-
time)– Typically restricted to cases that arise during
oral (ambulatory) therapy.

27Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
PharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiology
• Spontaneous reports data offer limited insight into population risk
• Reporting rates are not incidence rates• Have been used in addition to other data
to support previous regulatory actions by the agency
• Large differences in reporting rate ratios may support differential in risk
• Spontaneous reports data offer limited insight into population risk
• Reporting rates are not incidence rates• Have been used in addition to other data
to support previous regulatory actions by the agency
• Large differences in reporting rate ratios may support differential in risk

28Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
PharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiologyPharmacoepidemiology
• Drug-against-drug reporting rate comparisons require very similar drug products
– time on market
• Assumption that reporting practices are similar for similar drug products over the observed reporting period.
• Drug-against-drug reporting rate comparisons require very similar drug products
– time on market
• Assumption that reporting practices are similar for similar drug products over the observed reporting period.

29Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Relevant Case Studies Including Relevant Case Studies Including Reporting Rate Comparisons and Reporting Rate Comparisons and
Regulatory RecommendationsRegulatory Recommendations
Relevant Case Studies Including Relevant Case Studies Including Reporting Rate Comparisons and Reporting Rate Comparisons and
Regulatory RecommendationsRegulatory Recommendations
• ALF in association with trovafloxacin
• ALF in association with moxifloxacin, gatifloxacin, and levofloxacin
• ALF in association with trovafloxacin
• ALF in association with moxifloxacin, gatifloxacin, and levofloxacin

30Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
• July 1999– David Graham and Sarah Singer
• Analysis included drug-against-drug reporting rate comparisons– trovafloxacin– levofloxacin
• July 1999– David Graham and Sarah Singer
• Analysis included drug-against-drug reporting rate comparisons– trovafloxacin– levofloxacin

ALF in Association with Trovafloxacin: ALF in Association with Trovafloxacin: Reporting Rate AnalysisReporting Rate Analysis
ALF in Association with Trovafloxacin: ALF in Association with Trovafloxacin: Reporting Rate AnalysisReporting Rate Analysis
DrugUS market
appear-ance
UScases
Onset median (days)
Rxs*(in
millions)
Reportingrate
(per 10 million Rx)
LevoJan 1997 1 --- 6.868 1.5
TrovaJan1998 12 25 2.073 58
*IMS Health, National Prescription Audit Plus™, Years 1997 and 1998, Hardcopy book.
32Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
• Absolute ratio in case counts– 12:1
• Adjusted ratio in case counts(reporting rate ratio)– 39:1
• Absolute ratio in case counts– 12:1
• Adjusted ratio in case counts(reporting rate ratio)– 39:1
33Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
Acute Liver Failure in Association with Acute Liver Failure in Association with TrovafloxacinTrovafloxacin
• Regulatory action: June 1999
• Trovafloxacin restricted to initial therapy for in-hospital use for treatment of life and limb-threatening infections
• Regulatory action: June 1999
• Trovafloxacin restricted to initial therapy for in-hospital use for treatment of life and limb-threatening infections
34Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Failure in Association with Acute Liver Failure in Association with Moxifloxacin, Gatifloxacin, and LevofloxacinMoxifloxacin, Gatifloxacin, and Levofloxacin
Acute Liver Failure in Association with Acute Liver Failure in Association with Moxifloxacin, Gatifloxacin, and LevofloxacinMoxifloxacin, Gatifloxacin, and Levofloxacin
• August 2004– Sarah Singer and Allen Brinker
• Analysis included drug-against-drug reporting rate comparisons– levofloxacin– moxifloxacin– gatifloxacin
• August 2004– Sarah Singer and Allen Brinker
• Analysis included drug-against-drug reporting rate comparisons– levofloxacin– moxifloxacin– gatifloxacin

ALF with Moxi-, Gati-, and Levofloxacin:ALF with Moxi-, Gati-, and Levofloxacin:Reporting Rate ComparisonReporting Rate Comparison
ALF with Moxi-, Gati-, and Levofloxacin:ALF with Moxi-, Gati-, and Levofloxacin:Reporting Rate ComparisonReporting Rate Comparison
DrugUS
market appear-
ance
USCases
Onsetmedian(days)
Rxs*(millions)
Reporting rate
(cases per 10 mil Rx)
Levo Jan1997
12 7.0 57.436 2.1
Gati Dec 1999 6 4.0 10.068 6.0
Moxi Dec 1999 5 2.5 7.563 6.6
IMS Health, National Prescription Audit Plus™, Years 1997 through September 2003, extracted July 2004.

36Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Failure in Association with Acute Liver Failure in Association with Moxifloxacin, Moxifloxacin, Gatifloxacin, and , and
Levofloxacin Levofloxacin
Acute Liver Failure in Association with Acute Liver Failure in Association with Moxifloxacin, Moxifloxacin, Gatifloxacin, and , and
Levofloxacin Levofloxacin
• Absolute ratio in case counts• About 2:1
• Adjusted ratio in case counts(reporting rate ratio)
• About 3:1
• Absolute ratio in case counts• About 2:1
• Adjusted ratio in case counts(reporting rate ratio)
• About 3:1
37Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Acute Liver Acute Liver Failure in Association with in Association with Moxifloxacin, Gatifloxacin, and Moxifloxacin, Gatifloxacin, and
Levofloxacin Levofloxacin
Acute Liver Acute Liver Failure in Association with in Association with Moxifloxacin, Gatifloxacin, and Moxifloxacin, Gatifloxacin, and
Levofloxacin Levofloxacin
• Observed ALF reporting rates for these three agents appeared similar
• DDRE recommended addition of ALF as a WARNING within product labeling for all fluoroquinolones
• Observed ALF reporting rates for these three agents appeared similar
• DDRE recommended addition of ALF as a WARNING within product labeling for all fluoroquinolones

Telithromycin-Associated ALF:Telithromycin-Associated ALF:Reporting Rate ComparisonReporting Rate Comparison
Telithromycin-Associated ALF:Telithromycin-Associated ALF:Reporting Rate ComparisonReporting Rate Comparison
DrugUS market
appear-ance
USCases
OnsetMedian(days)
Rxs(in
millions)
Reporting rate
(Per 10 million Rx)
Gati Dec 99 6 4.0 10.068* 6.0
Moxi Dec 99 5 2.5 7.563* 6.6
Teli July 04 12(Apr 06)
4.0 5.198** 23
*IMS Health, National Prescription Audit Plus™, Years 1997 through September 2003, extracted July 2004.
**Verispan Vector One®:National, months May 2004-April 2006, extracted May 2006.

39Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Absolute ratio in case counts• About 2:1
• Adjusted ratio in case counts(reporting rate ratio)
• About 4:1 (April 2006)
• Absolute ratio in case counts• About 2:1
• Adjusted ratio in case counts(reporting rate ratio)
• About 4:1 (April 2006)

40Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Observed reporting rates generally similar
• Not consistent with trovafloxacin analysis– Absolute ratio of case count not ~12:1– Adjusted ratio of case count not ~39:1
• Recommended regulatory actions similar to that advanced for the recent ALF-FQ review
• Observed reporting rates generally similar
• Not consistent with trovafloxacin analysis– Absolute ratio of case count not ~12:1– Adjusted ratio of case count not ~39:1
• Recommended regulatory actions similar to that advanced for the recent ALF-FQ review
41Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• Also noted rising trend in the cumulative telithromycin-ALF reporting rate– 12 per 10 million Rx through Dec 2005– 17 per 10 million Rx through February
2006– 23 per 10 million Rx through April 2006
• Liver injury was a concern pre-approval– to be addressed within Study 3014
• Also noted rising trend in the cumulative telithromycin-ALF reporting rate– 12 per 10 million Rx through Dec 2005– 17 per 10 million Rx through February
2006– 23 per 10 million Rx through April 2006
• Liver injury was a concern pre-approval– to be addressed within Study 3014

42Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
• DDRE recommended a “bar” for further regulatory actions based on ALF-reporting rate for trovafloxacin (58 per 10 million Rx)
– Would not wait until:• Absolute ratio of case counts ~12:1, or• Adjusted ratio of case counts ~39:1
– As seen with ALF with trovafloxacin
• DDRE recommended a “bar” for further regulatory actions based on ALF-reporting rate for trovafloxacin (58 per 10 million Rx)
– Would not wait until:• Absolute ratio of case counts ~12:1, or• Adjusted ratio of case counts ~39:1
– As seen with ALF with trovafloxacin
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALF - UpdateAssociated ALF - Update
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALF - UpdateAssociated ALF - Update
• 13th case added in 2 QTR 06
• Reporting rate for telithromycin-associated ALF through September 2006 with:– 13 cases / 5,650,000 Rx*– 23 per 10 million Rx
• Unchanged from RR observed in April 2006
• 13th case added in 2 QTR 06
• Reporting rate for telithromycin-associated ALF through September 2006 with:– 13 cases / 5,650,000 Rx*– 23 per 10 million Rx
• Unchanged from RR observed in April 2006
*Verispan Vector One®:National, months May 2004-September 2006, extracted Nov 2006.

44Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
• Received completed studies last week (early December 2006)– Pharmetrics– i3 drug safety
• Review ongoing– Comments at this time preliminary
• Received completed studies last week (early December 2006)– Pharmetrics– i3 drug safety
• Review ongoing– Comments at this time preliminary
45Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
• Comments (preliminary)– Both studies appear underpowered for
both drug-associated ALF and serious liver injury
– Medical record validation required• Done in i3 study; not done in Pharmetrics
study
• Comments (preliminary)– Both studies appear underpowered for
both drug-associated ALF and serious liver injury
– Medical record validation required• Done in i3 study; not done in Pharmetrics
study
46Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
Sanofi-Aventis Population-Based Sanofi-Aventis Population-Based Epidemiology StudiesEpidemiology Studies
• Comments (preliminary)– The point estimate for severe liver injury
observed in the i3 study is consistent with an elevated risk for serious liver injury with telithromycin in comparison to clarithromycin.
– The finding in the i3 study of an elevated risk of serious liver injury with sequential use of telithromycin and clarithromycin
• deserves attention (further study) but based on 3 cases.
• Comments (preliminary)– The point estimate for severe liver injury
observed in the i3 study is consistent with an elevated risk for serious liver injury with telithromycin in comparison to clarithromycin.
– The finding in the i3 study of an elevated risk of serious liver injury with sequential use of telithromycin and clarithromycin
• deserves attention (further study) but based on 3 cases.

47Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
DDRE Review of Telithromycin-DDRE Review of Telithromycin-Associated ALFAssociated ALF
End ofPresentation
AcknowledgementsJenna Lyndly, RNRon Wassel, PharmDMelissa Truffa, PharmDMark Avigan, MD, CM
End ofPresentation
AcknowledgementsJenna Lyndly, RNRon Wassel, PharmDMelissa Truffa, PharmDMark Avigan, MD, CM

48Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Back-up SlidesBack-up SlidesBack-up SlidesBack-up Slides
Return to agenda

49Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Crude Assessment of Agreement on ALF Crude Assessment of Agreement on ALF “Case” Status between 3 Disparate DDRE “Case” Status between 3 Disparate DDRE
Reviews of Antibiotic-Associated ALFReviews of Antibiotic-Associated ALF
Crude Assessment of Agreement on ALF Crude Assessment of Agreement on ALF “Case” Status between 3 Disparate DDRE “Case” Status between 3 Disparate DDRE
Reviews of Antibiotic-Associated ALFReviews of Antibiotic-Associated ALF
Drug Crude count(“serious”)
“Cases” after review
Percent
Trova 115 14 12
Levo 107 19 18
Gati 55 9 16
Moxi 49 6 12
Teli 66 12 18

50Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
• Rx-based comparisons preferred by this reviewer as:– 1 Rx = 1 Pt (in most cases)– Time to onset falls within typical treatment
course for most cases• Rx-based reporting rates
– Absolute difference in case counts• About 2:1
– Adjusted difference (reporting rate ratio)• About 4:1
• Rx-based comparisons preferred by this reviewer as:– 1 Rx = 1 Pt (in most cases)– Time to onset falls within typical treatment
course for most cases• Rx-based reporting rates
– Absolute difference in case counts• About 2:1
– Adjusted difference (reporting rate ratio)• About 4:1

51Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
• Person-time reporting rates– Transformation based on typical treatment
courses of:• 10 days for moxifloxacin and gatifloxacin• 5 days for telithromycin
– Results in incidence density for moxi- or gati associated ALF of ~22 per million person years
– Results in incidence density for telithromycin-associated ALF of 168 per million person-years
• Background (expected) rate of idiosyncratic ALF in the general population ~1 per million person-years.
• Person-time reporting rates– Transformation based on typical treatment
courses of:• 10 days for moxifloxacin and gatifloxacin• 5 days for telithromycin
– Results in incidence density for moxi- or gati associated ALF of ~22 per million person years
– Results in incidence density for telithromycin-associated ALF of 168 per million person-years
• Background (expected) rate of idiosyncratic ALF in the general population ~1 per million person-years.
52Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
Rx Versus Person-Time Reporting Rx Versus Person-Time Reporting Rate ComparisonRate Comparison
• Person-time reporting rates– Absolute difference in case counts
• About 2:1 (unchanged)– Adjusted difference (incidence ratio)
• About 8:1 fold (increased from 4:1)• Trovafloxacin
– Absolute difference in case counts:• 12:1
– Adjusted difference (reporting rate ratio):• 39:1
• Person-time reporting rates– Absolute difference in case counts
• About 2:1 (unchanged)– Adjusted difference (incidence ratio)
• About 8:1 fold (increased from 4:1)• Trovafloxacin
– Absolute difference in case counts:• 12:1
– Adjusted difference (reporting rate ratio):• 39:1

53Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Joint Meeting of the Anti-Infective Drugs Advisory Committee and the Drug Safety and Risk Management Committee Meeting Drug Safety and Risk Management Committee Meeting December 14 & 15, 2006December 14 & 15, 2006
ReturnReturnReturnReturn
Return to agenda Return to agenda





























