Embed Size (px)
Citation preview

1
JOAN C. MASTERS, EDD, MBA, APRN, PMHNP-BCBELLARMINE UNIVERSITY
LOUISVILLE [email protected]
KENTUCKY COALITION OF NURSE PRACTITIONERS AND NURSE MIDWIVES CONFERENCE
LEXINGTON, KYAPRIL 15 , 2014
Psychiatric Aspects of Movement Disorders for Nurse Practitioners

2
Abstract
Movement abnormalities are often comorbid with psychiatric disorders. A movement disorder may be a manifestation of a psychiatric disorder (i.e. psychogenic disorder), an adverse response to psychiatric treatment (e.g., drug-induced), or a distinct but co-occurring condition with a psychiatric disorder. In this presentation, an overview of the major movement disorders with psychiatric aspects, clinical pearls, and treatment caveats will be presented.

3
OBJECTIVES
At the completion of this presentation, participants will be able to:
Differentiate among psychogenic, treatment induced, and co-occurring movement and psychiatric disorders
Explain appropriate treatments for psychogenic, treatment induced, and co-occurring movement and psychiatric disorders

4Somatic Symptom Disorders
Challenging patient populationChronic, difficult to treatHigh utilizers of the healthcare systemRisksRepetitive, unnecessary diagnostic testingInvasive medical/surgical workupsIatrogenic illnessClinical GoalsCoordination of care with psychiatric consultationTreat medical illness fullyAvoid excess iatrogenic harm

5
Terminology
Psychogenic considered unsatisfactory (Used by clinicians but not usually with pts.)
More recently “functional”Replaces conversion DO, hysteria

6
PSYCHOGENIC MOVEMENT DISORDERS (PMD)
Not caused by structural neuro damageWide range of symptoms (tremors,
bradykinesia, myoclonus, tics, chorea, athetosis, ballism)
PMD often (~70%) accompanied by anxiety, depression, PDOs, substance abuse
Clinicians (not pts.!) tend to see “stress” as causative but that is overly simplistic

7
History
Somatoform DO Not included in DSM I and II but neurosis wasDSM-III: Neurosis too vague and too psychodynamicS&S needed a home: SomatoformDSM-IV: Medical symptoms had to be “unexplained”DSM 5 DX: “Somatic Symptoms and Related
Disorders“ replaces old "Somatoform Disorders“ Somatic symptom disorder (subsumes pain DO &
somatization DO) New: Illness anxiety disorder and Psychological
factors affecting other medical conditions

8
Why So Many Changes?
Overlapping previous diagnosesDifficult for non‐psychiatric clinicians to applyReduction of stigma↓ mind‐body dualismImplication that symptoms were not "real”DSM‐5 Changes:Reduction in the number of diagnosesFocus on positive symptomsRemoval of “medically unexplained
symptoms”

9
DSM 5
Lack of medical explanation≠Psychiatric Diagnosis

10
DSM-5: Somatoform DOs Now Somatic Symptom and Related DO
Somatic Symptom DisorderIllness Anxiety DisorderConversion Disorder (Functional
Neurological Symptom Disorder)Psychological Factors affecting other medicalconditionsFactitious DisorderGone: Hypochondrias, somatization disorder,
pain disorder, & undifferentiated somatoform disorder

11
Epidemiology PMD
Accurate data limited~ 30% of outpatients in neuro settings S&S not
caused by neuro disease ½ PMD & ½ out of proportion to disease As distressed and more disabled (Stone & Carson, 2011)
~ 1% - 9% neuro unit admissions unexplained motor symptoms (Hallett)
~ 25% MDO pts. some point could be dx with PMDOLarge hospital DC study, 2.6% DC DX somatoform
DO ~3.5% large specialty clinic (Sa)Tremor, dystonia, myoclonus, gait, Parkinson's, tics
In order of commonality; last two may reverse order

12
Clues A: History
General; DO specific clues with each DOAbrupt onset, static courseInconsistent over time (spontaneous
remissions and exacerbations)Multiple somatic C/OHealth care workerOnset typically 35 – 50 yoa

13
Clues A: History
Predisposing factors:Low SES, 60%-75% female, hx of abuse and neglect,
current mistreatment, modeling, perceived stress; not ↓IQ
Precipitating factors: Often a physical injury Perpetuating factors:Illness beliefs, secondary gain; anger at DX, diagnostic
uncertainty, involved in litigation/worker’s compCluster B traits- low self-directedness and high novelty
seeking(Hallett; Sa)

14
Clues B: Clinical
No single finding will clinch itMovements increase with attention and decease
with distractionInconsistent (amplitude, character, distribution,
selective disability)Paroxysmal movement DOAbn movements can be triggered or relieved with
odd or non physiological tx (e.g., use of tuning fork)
False weakness/false sensory CODeliberate slowness of movements

15
Clues B: Clinical
PMD don’t usually involve the fingers; MD doFunctional disability out of proportion to clinical
findingsMultiple symptoms attributable to multiple organ
systemsFixed dystonia (contracted limb)Excessive grimacing or sighingNon-anatomical sensory loss (stocking & glove
anesthesia)Movements are bizarre or multiple or hard to classifySelf-inflicted injuries(Sa)

16
Clues C: Pt. Response
Responds to placeboDoes not respond to appropriate medsAbn movements remit with psychotherapyPts deny/refuse psychogenic explanationUsually agreeable with pragmatic approach
of therapy, meds to treat depression & anxiety, and improving coping skills

17
Pt Challenges
Complicated and difficult diagnostically (can be done) and clinically (because often have other pathology)
Inaccurate historians compared to clinicians and to selves
One study: Only 22% of self-reported symptoms confirmed
Another: Only 61% of med unexplained symptoms and 43% of all symptoms reported by pt a year later
Prognosis guarded; Two-thirds same/worse at follow-up
(Hallett)

18
Assessment
Initially should focus on listing all physical S&S Can wait on depression and anxiety questions- can be
alienatingAsk about fatigue, pain, sleep disturbance,
dizziness, memory, concentration Helps rapport
Gradual onset associated with fatigueWhat is pt.'s understanding? Irreversibility and damage beliefs prognostic

19
Caveat
Clues are only that People with organic DO may also have these
presentationsUp to 30% of people with PMD found to have
an organic condition that could explain their S&S
Neuro DO can have unusual presentations

20
PMD Tremor
Common: 35% and 55% of PMDs in two large studies
More common in middle-age, femaleQuick onset and rapid progression are cluesVariable amplitude and frequency cluesPostural more than resting which is more
than actionOften all three- a clueOrganic do not dissipate with distraction

21
PMD Tremor
Entrainment a clue- pt asked to do a slow rhythmic or complex irregular pattern with uninvolved/other limb the tremor often changes to match contralateral movement
Arm(s) most common Usually continuous
But rarely fingersThen headThen legs
Usually not continuousSurprisingly little C/O fatigue

22
PMD: Dystonia
Sustained muscle contractionsTwisting, writhing movementsMD most likely to be dx as psychogenic when
not No bio marker
39% of PMDOYoung femalesAbrupt onsetLower limb, excessive pain, slowness,
non-anatomic sensory dysfunction

23
PMD Myoclonus
Brief, shock-like muscle contractions or sudden loss of tone (negative myoclonus)
~13%, 2 X women, M= 43 yoaWorse with stress and anxietyMost have a precipitating eventElectrophysiological testing can differentiate
organic from PMD (which is slower, inconsistent, variable)

24
PMD Myoclonus: Related Culturally-Mediated Disorders
Startle response: Jump, grimace, hunch shoulders, breathe faster
Nl: Habituate and relax on successive exposuresSome people (and dogs, cows, horses, mice, have
an exaggerated response; shout, flex arms and legs and fall to ground Hereditary hyperkplexia Don’t habituate with repeated exposure Defect of inhibitory glycine receptors
In humans and one mouse strain one amino acid coded incorrectly- chloride channel opens less frequently when exposed to NT glycine; glycine now ↓ effective in inhibiting neurons in brain stem and sc

25PMD Myoclonus: Related culturally-mediated Disorders
Jumping Frenchmen of Maine: Unusual, extreme startle response, often followed by echolalia, echopraxia, coprolalia, forced obedience (“Sit!”, “Jump!”)
Normal startle habituates, this does not-increasing complexity
Late 19th century; isolated lumberjacksSymptoms milder with ageMore intense with stress, anxiety, and the
more frequently startled

26
Normal Startle
Two components1st abrupt brief blink, grimace, them head &
neck movement, with flexion of upper limbs & trunk
Involuntary; normally habituates but exaggerates in hereditary hyperekplexia (mutations in glycine receptors) and in acquired hyperekplexia from brainstem disease

27
Normal Startle
2nd componentBegins at latencies overlapping with voluntary
reaction times2nd component longer in duration and subject to
voluntary elaboration, “orienting” to the stimulus- look toward, away, raising hands, vocalization (including coprolalia), dropping or throwing objects
Presentation varies with intense emotion/pleasureLatah/descendent of JF- startle fall in voluntary
reaction timesMay be linked to frontal lobe dysfunction

28
PMD Myoclonus: Related Culturally-Mediated Disorders
Tx: Eliminating intentionally startling and/or teasing can reduce/end episodes
Latah in Indonesia Most common, middle age women Often rage, anxiety, fear
Myriachit in Siberia“Ragin’ Cajuns” in LouisianaMore research needed

29
Strychnine Poisoning
Plant toxin; used by farmers to kill farm pests and by psychopaths
Antagonizes glycine at its receptorHigh doses almost eliminates glycine inhibition in sc
and brain stemUncontrollable seizures, unchecked muscle
contractions, paralysis of respiratory muscles, asphyxia
Agonizing death bc glycine not a NT at higher centers of brain so no cognitive or sensory impairment
Low protein binding so enters tissues quicklyDeath within 1-2 hoursLow doses a stimulant; 1992 Olympics

30
PMD Chorea/Ballism
Changes in definition of chorea have changed over time
Random fleeting movements that flow from one part of the body to another in an unpredictable way
Figidity, antsyBallism: Involuntary, irregular, violent
movements arm and shoulder, rt stroke or tumor, usually one side
Again, inconsistentExceedingly rare

31
PMD Tics
Rare (~3%- 6%) and little writtenHigh percentage have an “inner urge” to
perform tics In contrast to other organic do (e.g., TD,
dystonia) in which no desire

32
PMD Facial Spasm Dyskinesia Tics
Unusual (~2.4%) May be overlooked if more dramatic symptoms
presentMore in women, 30sUsually found secondary to another PMDDx: Abrupt onset, multiple somatization,
secondary gain, exacerbation with attention, reduction with distraction

33
PMD Parkinsonism
~10%-20% of PMDs Slightly more women than men (opposite in PD)Often occurs after injury or accidentTremor present at rest, often of dominant hand,
persists with change in posture and action, lack dampening of true PD rest tremor with a new posture or movement
Tremor decreases/disappears with distractionOpposite of true resting tremor of PD where
mental exercise elicits or intensifies the tremor

34
PMD Parkinsonism
Bizarre movements with mild stimulus of testing (falling backwards but not falling, flailing of arms)
Non-anatomical sensory loss“Baby” or foreign accent speechHandwriting irregular but no micrographia Classic abrupt onset, inconsistencies, alteration/
distraction, false neuro signsRigidity common, often with c/o pain Disability can be severeCan remit with psychotherapyDx imaging (PET, SPECT) can clarify

35
PMD Parkinsonism
High resource use, excessive consultation, surgeries, dx tests
Nigrostriatal dopamine system imaging flurodopa PET and betaCIT and I-isoflupane SPECT can dx
Abnormal in even very early PD and not in psychogenic movement DO
Baylor: Placebo test with cariodopa alone and tuning fork test (told vibration will change tremor)
Disclosed after

36
PMD Gait Disorders
Long hx in med literature↑ hx of misdx (fx turn out not to be)All ages, but caution dx in older people – often
have (real) problems in balance with exaggerated compensation RT fear of falling
More femaleAbnormalities often distinctivePsych hx relevantKey: Abrupt onset, inconsistent, incongruent,
multiple simultaneous symptoms (e.g., contractions, tremor, voice abnormalities, paralysis), or total remission for day or weeks

37
PMD Gait Disorders
Often exaggerated slowness – “walking through thick soup”
Exaggerated effort, exaggerated fatigue
Convulsive shaking, scissor walkingUneconomic postures including
camptocormia (“bent tree”)Knee bucking, pained affectMay have dramatic fluctuations over minutes
(rare in neuro DO)

38
PMD Gait Disorders
Dragging gait (see next slide)Tightrope walker’s gait (arms out)Crouching gait- close to ground BC fear
falling (but that requires more strength!)

39
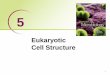
Example Functional Monoplegic Gait
Both cases, leg dragged at the hip. External or internal rotation of the hip or ankle inversion/eversion is common.

40
PMD Gait Disorders
Astasia-abasia Unstable, staggering way of standing and walking;
Uneconomical Normal limb power in bed but cannot stand or walk Constantly on the verge of falling, but always saves self Was most common conversion DO in WW I
Excellent example at http://www.youtube.com/watch?v=tdpvNObwEZo&list=PLz27Rlp3y6Xtfw83z3CfgeHhhuRIOZvBy&feature=player_detailpage (Harrison Video Library of Gait Disorders, # 4)
Observation/distraction may activate/suppressPrognosis can be good with short duration and acute
onsetIf ↑ 6 mos and secondary gain sets in prognosis
guarded

41
PMD Gait Disorders
Dx:Observe spontaneous gait and tandem heel toe walkingWilson’s disease and Huntington's disease most
frequent DO where incorrect dx of PMD made(Wilson's-autosomal recessive, cannot excrete copper,
accumulates liver, brain, kidneys)In addition to observation:Lab gait analysis: Software not yet where should beImaging
White matter disease (some nl in older)Dual task walking (Walking and cognitive task)
Abn in executive fx associated with reduced gait speed

42
PMD Tourette Syndrome
Tourette: Premonitory urge Suppressability- disappear during
voluntary movements Recognized as partially voluntary Relief following Tics nearly identical

43
PMD Tourette Syndrome
Tourette and pseudo tics: Abrupt onset Cessation with distraction Response to suggestion Waxing and waning course Dramatic resolution
Pseudo tics: Maximum disability at onset Increase with attention Variability BT tics Entrainment Uncommon

44
PMD Weakness
Female, mid-30s5/100,000Often co-morbid with fatigue & painMost common unilateral > one limb > both
LLMay report limb feels alien

45
Voluntary S&S: Factitious DO
Factitious: Intentional feigning or producing physical or psychological symptoms Severe form: Munchhausen's syndrome
Motivation is the sick roleNo external incentives (not for financial,
legal, or other gain)Poor prognosis

46
Voluntary S & S: Malingering
Not a psychiatric DOIntentional self-injury motivated by financial gain,
avoiding work, etc.Discrepancy between presentation and findingsRare, absurd, odd symptoms combinationsUncooperative with dx and tx recommendationsAntisocial PDOHx of different names*Possibly rationalMay clear up spontaneously with settlement or may
continue to keep up appearancesClinicians can be reluctant to diagnoses; insurance
companies less so

47
Voluntary S & S: Malingering
13% of patients in ED feign illnessSecondary gain most often food, shelter,
prescription drugs, financial gain, and avoidance of some responsibility
Red flags:Vague answers, professional language,
conditional threats, demanding certain meds, eagerly volunteers psychotic S&S, endorses both psychotic and cognitive S&S, overnight illness, no psychotic illness until ~late in life
BB article has good tools

48
DX PMD: “Here there be dragons”
Dx is very difficult and pitfalls aboundShould be done by a movement DO expert, not just a
neuro specialistDifferential includes entire spectrum, need wide and deep
experienceIncorrect dx of PMD subjects pts. to:
more stress more, expense missed opportunity for correct tx ASE of inappropriate rx stigma
Only 4% misdiagnosis (PMD incorrectly dx in organic condition)

49
DX PMD
Hospital admission could be usefulOnce correct dx, need to stop searchingSuggestion: Explaining to pt no serious disease
along with PT/OT, therapy, biofeedback Relatively benign approach
Placebo Legal and ethical issues, impugn autonomy
Damaging to pt-provider relationship when pt. finds out
Psychogenic dx should be made by neurology not psychiatry

50
Categories of Dx Certainty
Fahn and Williams-accepted standard1. Documented: Relieved with therapy, suggestion,
placebo, observed symptom free 2. Clinically established: Inconsistent, incongruent, with
definite psychogenic symptoms 1 &2 later “Clinically definite”3. Probable: Inconsistent/incongruent but that’s all, or
high likelihood of organicity but false neuro S&S, or likely organic but plethora of somatic complaints
4. Possible: Obvious emotional issues in someone with a movement DO that appears organic
May need revision; many patients have a “functional overlay” to PMDs

51
Patient Approach
Empathetic, with certainty, nonjudgmental, that do not believe they are “crazy”, confident of improvement
Neurobiological explanation; form of dystonia, myoclonus etc. without severe or permanent brain disease
Psych referral to aid in evaluation and coping with burden of illness
Psych should be adequately informed-do not want “nothing wrong” dx
No controlled trials so empirical approach

52
Prognosis
GuardedMany will have persistent disabilityResearch study, 66 PMD and 704 with PDPMD had more psychiatric DX, more severe
psychiatric illness, similarly poor QOL and disability despite younger age and shorter duration of illness
3 years after dx only 4/66 no longer had PMD but two of those had another somatoform DO
If no improvement with initial hospital evaluation recovery is rare
If legal/compensation issues present, seldom improvement until resolved but resolving many not help
(Sa)

53
Prognosis
Better prognosis if treated in a psychiatric setting than neuro setting
Illness beliefs & financial benefits stronger predictors of recovery than number of symptoms, disability, and distress
Better prognosis: Younger age, shorter duration, willing to accept psychological factors, believe reversibility, rapport with clinician, no other symptoms, presence of anxiety and depression, removal of stress, marriage or divorce
Poorer prognosis: Believe irreversible, PDO, anger at nonorganic dx, older age, sexual abuse, longer duration

54
Talking With Patients About the Dx
Difficulties: Pts. distress/fear:
Implication “on purpose”, wonder if worse dx being missed, convinced do not have a psych problem, shares negative ideas about psychogenic do, confirms worst fears,
Clinician: Non psych may be uninterested, may not know what
to make of it, may wonder if deliberate, reluctant to make dx and being wrong

55
Presenting the Dx
Explain what they haveHow the dx was madeExplain what they do not haveIndicate belief- (“I do not think you are making this up”)
Emphasize this is common (“I see many pts. . . “)Emphasize reversibility (“Because there is nothing wrong
with your brain, you have the potential to get better”)Emphasize self-help (“This is not your fault but there are
things you can do to help yourself get better”)Present the role of depression and anxiety (“Feeling
depressed/anxious will tend to make your symptoms worse”)

56
Presenting the Dx
Give written information- letter, handout, website
DC meds that indicate a not present disease Suggest antidepressants in context of
broader usePsychiatric referral in context of
management, not psychiatric illnessInvolve SO

57
Presenting the Dx
Controversy re core explanationPsychological explanation
May improve acceptance, makes connection BT symptoms & emotions, but may negatively affect relationship with pt
Functional explanation (“software” problem) Pt less likely to think perceived as “crazy”, better fit
with reversal potential but maybe too accommodating, too broad a term, may delay psych. Tx
“I don't know” Possibly accurate but creates ↑ doubt about clinician

58
Presenting the Dx
If pt hostile to a psych explanation then a functional explanation at start may be advisable
If pt taken seriously may be more amenable to a functional explanation first and over time a psych explanation

59
Presenting the Dx
Psychological explanation Speed acceptance- many pts suspect, Helps pt make that link if have not made
already No room for confusion May became angry but that may not be a
change

60
Presenting the Dx
ResourcesFunctional/dissociative neuro symptoms:www.neurosymptoms.orgNon-epileptic seizures www.nonepilepticattackes. OrgBritish, well-done

61
Psychotherapy
Psychotherapy seems logical but not enough research
Tx anxiety and depression if indicated. Meds, CBTPhysical therapy“This may be as much as can be done at
present – will need to work around it for now”

62
Local MDO Clinics
IU Dept. of Medicine, http://neurology.medicine.iu.edu/neurology-programs1/movement-disorders/
University of Cincinnati Gardner Center for Parkinson’s Disease and Movement Disorders in the UC Neuroscience Institute
http://ucgardnercenter.com/

63
Local MDO Clinics
Kentucky Neuroscience Institute movement Disorders Clinichttp://ukhealthcare.uky.edu/ky-neuro/movement/
Appointments and Info: 859-323-5661
Frazier Rehab Institute and the University of Louisville Division of Movement Disorders
http://www.kentuckyonehealth.org/movement-disorders-parkinson-disease-program502-582-7400

64
TREATMENT INDUCED MOVEMENT DISORDERS
Acute dystoniaAkathisiaPseudo-ParkinsonismTardive DyskinesiaNeuroleptic malignant syndromePundingSerotonin syndromeTremor

65
Pathophysiology
If D2 receptors blocked in nigrostraital pathway get movements resembling PD
Since nigostriatal pathway part of EP nervous system called EPS
Chronic blockade: Hyperkinetic movement DO known as tardive dyskinesia (TD)
D2 receptors upregulate (↑ in number) attempting to overcome drug-induced receptor blockade

66
EPS
“Inextricably linked” to antipsychoticsIssues:Mistaken for/worsen psych symptomsTroublesome SE from antiparkisinson medsSometimes irreversible, even lethalDisfiguring/stigmatizingNegatively affect compliance, relapse,
rehospitalization1988: Clozapine reported to be low on EPS,
sets off chain reaction of search for “atypicals”

67
Tardive Dyskinesia
Facial and tongue movementsGrimacing, tongue protrusion, constant chewingLimbs: Quick, jerky or choreiform (“dancing”) movements5% pts. on conventional antipsychotics develop every yearOlder-25% in first yearMay reverse if stopped soon enough by “resetting” of D2
receptors (either they decrease in # or become less sensitive)
↓With LT use, no reversibilityVulnerable? Early EPS ~2X risk of TDAfter 15 years, new risk lowTool: AIMS; http://www.cqaimh.org/pdf/tool_aims.pdf(Stahl)

69
Atypicals Also Risky for TD
TD study at CT CMHCAIMS & Glazer-Morgenstern criteria for dyskinesia every 6
month for 4 yearsTD risk with atypicals more than half that of conventional
when clozapine excluded or more than two-thirds risk when clozapine included
TD risk significantly higher for schizophrenia than affective DO pts
Olanzapine may be lower risk (but ziprasidone and aripirazole not included)
Clinicians should continue to monitor for tardive dyskinesia, and researchers should continue to pursue efforts to treat or prevent it
(Woods et al., 2010)

70
Acute Dystonia
Acute, frightening, painful, involuntary MDOBrief sustained or intermittent contractions of
antagonistic muscle groupsTwisting and repetitive movementsMost common: Head, jaw, eyes, mouthLeads to torticollis, retro/anterocollis, trismus
(lockjaw) Blepharospasm (eye spasms), tongue biting, protrusion
Not action or sensory dependentMore subtle: Muscle cramps, jaw tightness,
difficulty speaking/swallowing –may precede or be only S&S

71
Acute Dystonia
May get worse: Oculogyric crisis, dysarthria, dysphagia, respiratory stridor (if pharyngeal or laryngeal muscles affected)
Less common: Axial, truncal or limb involvement, camptocormia (marked flexion of thoracolumbar spine that abates in recumbent position), pleurothotonus (Pisa syndrome), opistotonus (head and lower limbs to bend backward and the trunk to arch forward)

72
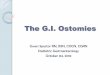
Anterocillis on upper L, Pisa syndrome on upper R, Trismus on lower R, camptocormia
on lower left, opistotonus middle

73
Acute Dystonia: DX
Earliest EPS; 95% first few days of tx or increase in med Last hours-days If med DC, resolves 24-48 hours 2%-5% patients overall but can go as high as 90% in young
men on IM meds From excessive compensatory dopaminergic activity or
dopamine antagonism??? ↑Risk: Young (rare ↑ 45), children ↑risk), male, AA, previous
rx, +family hx of dystonia, cocaine use, mood DO, hypocalcemia, hypoparathyroidism, hyperthyroidism, dehydration
Dose dependent: Very high/low higher risk; moderate doses OK If have weak dopamine antagonism and strong anticholinergic
effects then low dystonia Olanzapine, quetiapine, ~ clozapine

74
Acute Dystonia: DX
CATIE study: Older people with chronic schizophrenia given moderate doses of mid-potency FGA (e.g. perphenazine, loxipine) not at increased risk of dystonia
Young, high-risk pts., or if paranoid and want to avoid dystonia, then can give anticholinergic prophylactically
Respond 10”-20” to benztropine or diphenhydramine (IM, po; IV in emergency)

75
Acute Dystonia
Pt on L had taken metoclopramide (Reglan) for GI problems
Reglan now has a black box warning

76
Parkinsonism
Mimics PDBradykinesia, masked facies, reduced arm
swing, slowed activity initiation, soft speech, flexed posture, symmetrical resting/action tremors, rabbit syndrome (focal perioral tremor), bilateral & symmetrical rigidity of neck, trunk, limbs with cog-wheeling, ~sialorhea, postural or gait disturbances
Compared to dystonia, more common, more difficult to treat, can cause more disability, esp. in older people

77
Parkinsonism
Differential: Negative symptoms schizophrenia, psychomotor retardation, idiopathic PD
PD usually asymmetric, slow progression, autonomic dysregulation (orthostasis), anosmia; imaging will help
10%-15% pts. on FGAs50%-75% in a month, 90% in 3 months; also with
change/increase meds, WD of anticholinergicUsually reverses in days-weeks but may be months
or permanent (real PD?)Risk: Older age, female, family hx of PD, dementia,
HIV+, pre-existing extrapyramidal disease,

78
Parkinsonism
Tx with anticholinergics not as compelling as for dystonia
Risk of atropine toxicityPreferred: Lower dose, switch to lower risk
antipsychotic Anticholinergic or amantadineParkinsonism may worsen if
anticholinergic WD

79
Akathisia
More often affects lower limbsStill a problem with SGAs; hard to treatPts. C/O: Feels tense, anxious, restless, drawing in
of legs, feeling fidgetyObserve: Complex, semi-purposive, repetitive
movements, foot shuffling & tapping, shifting foot to foot, rocking, pacing running
Intolerable; associated with suicide and aggressionCan be fine within a few days of tx but usually
increase with duration; 50% within one month and 90% with 3 mos

80
Akathisia
20%-35% but as much as 75% in some FGA studies~Risk: Older age, female, negative symptoms,
cognitive dysfunction, iron deficiency, Parkinsonism, mood DO
SGAs may be less likely Close observation key; once +, discontinue,
reduce, or switch to less potent dopamine antagonist
TX: Beta-blocker (propranolol), anticholinergic (but ↑ effective if parkinsonism +), benzos, amantadine
5HT2A antagonist: Mirtazepine (equal to propranolol and better tolerated)

81
Akathisia
Differential: Includes drug intoxication and WD, neurogenerative DOs
Meds causing restlessness: SSRIs, CCBs, anti-emetics (metoclopramide), anti-vertigo meds
Resembles restless leg syndrome; dopamine agonist will worsen things
Need to differentiate from agitation and anxiety
Barnes Akathisia Scale https://outcometracker.org/library/BAS.pdf

82
Catatonia
Least recognized antipsychotic MDO but also rare
DO of speech, volition, movementS&S: Stupor, akinesia, mutismMust be differentiated from catatonia due to
schizophrenia and mood DO, neurodegenerative DOs, other brain DOs
Develops within hours-days of drug exposure and resolves as quickly when antipsychotic WD
May also develop when benzo or anticholinergic WD

83
Catatonia
Risk: Previous catatonia, high potency drugs; SGAs may be lower risk
TX: Benzodiazepines and ECTMust TX- can progress to NMS+Hx: Avoid antipsychotics (if possible)Patho may be drugs effects on dopamine
pathways in basal ganglia-thalmocortical circuits and GABA/glutamate pathways
May be genetic component

84
Neuroleptic Malignant Syndrome
Rare but potentially fatal rx resembling advanced parkinsonism and catatonia
Often mistaken for worsening psychosisDifferential: Whatever causes fever and
encephalopathy (CNS infection, heatstroke, serotonin syndrome, ETOH, sedative, or dopamine agonist WD; dopamine antagonists such as Reglan))
Can have rapid onset but usually within 1-2 weeks of med start
Most case resolve in 1-2 weeks

85
Neuroleptic Malignant Syndrome
FEVER mnemonic:
F – FeverE – EncephalopathyV – Vitals unstableE – Elevated enzymes – CPKR – Rigidity of muscles

86
Neuroleptic Malignant Syndrome
~0.02% patients, ~15% fatalDeath: Renal failure, DIC, PE, pneumonia, cardiac arrestRisk: Dehydration, cathexia, catatonia, previous episode, high IM doses of high potency medsMaybe: Multiple meds (antipsychotics, SSRIs, SNRI, Li)Treatment:
Symptom management (cooling, fluids)DC antipsychoticBromocriptine (Parlodel) - dopamine agonistDantrolene (Dantrium) - peripheral muscle relaxant

87
Punding
From Swedish slang for “block head”- psychostimulant abuse
“Compulsive hobbyism”Repetitive, complex, unproductive, excessive,
stereotyped motor behaviorPt has an irresistible urgeOften “meaningless” collecting and
arranging, may be RT a previous hobbyOften co-morbid sleep problems

88
Punding
Differential: Motor tics, OCD, impulse control DO, autism spectrum, frontal syndrome (will have lesions in frontotemporal region)
Unlike OCD, (a)not instigated by internal tension about whether to do, (b)not driven by fear or anxiety (e.g., locking doors, burglars or washing hands)
Dopaminergic drugs, levodopa (L-DOPA Not dose or duration related; idiosyncratic ~8% in PD patients
Amphetamine, cocaine abuse

89
Serotonin Syndrome
Potentially life-threateningAssociated with ↑ serotonergic activity in CNSSeen with therapeutic med use, increase in dose, drug
interactions (combo of two drugs most common reason), OD
S&S: Mental status changes (anxiety, agitated delirium, disorientation)
Autonomic hyperactivity (diaphoresis, tachycardia, hyperthermia, HTN, V, D), also dry mucous membranes, flushed skin, diaphoresis
Neuromuscular abnormalities: Tremor, muscle rigidity, myoclonus, hyperrefelxia, bilateral Babinski sign
Hyperrefelxia, *clonus, rigidity common & more pronounced in lower extremities

90
Serotonin Syndrome Drugs
SSRIs, SNRIs, TCAs, buspirone, trazodone
Triptans for migraine
Ecstasy, dextromethorphan, cocaine, hallucinogens (foxy methoxy, Syrian rue, LSD)
Carbamazepine, Valproic acid, lithium
Fentanyl, *meperidine, methadone, tramodol
Herbs: St. John’s wort, ginseng
Antiemetic: Metoclopromide
Antibiotic: Linezolide (Zyvox)Anti-Parkinson’s drug L-dopa; Pts should be asked for a complete list of drugs regularly
taken, including prescriptions, OTC, dietary supplements and recreational drugs before prescribing something new

91
Serotonin Syndrome
2002: 7,349 cases serotonin toxicity, 93 deaths2005: 118 deaths 85% MDs unaware of SSAll ages, probably under recognized, many case mildMajority in 24 hours, most within 6Intentional OD often more toxic (but less reliable)Worse with MAOI useAsk directly; tox screenClinical dx, no specific labsComplications: DIC, rhabdomyolysis, hemoglobinuria,
metabolic acidosis, ARDS, renal failure

92
Serotonin Syndrome
Hunter Toxicity Criteria Decision RulesHx taking serotoninergic agent Plus ONE of the following:Spontaneous clonusInduced clonus PLUS agitation or diaphoresisTremor Plus hyperreflexiaHypertonia PLUS temp ↑ & ocular clonus (slow
continuous horizontal eye movements)

93
Serotonin Syndrome Differential
NMS: But NMS has slow onset and resolution, SS rapid onset and (usually) rapid resolution; longer with LA agents
SS : Neuromuscular hyperactivity, NMS sluggish neuromuscular activity
Anticholinergic toxicity: Yes to ↑ temp, agitation, mental status changes, mydriasis, dry mucous membranes, urinary retention, ↓bowel sounds BUT muscle tone and reflexes are normal
Malignant hyperthermia: Susceptible, halogenated volatile anesthesia, depolarizing muscle relaxants (e.g., succinylcholine), severe muscle rigidity, tachycardia, ↑ temp, acidosis BUT no neuromuscular activation
Ditto for CNS infection

94
Serotonin Syndrome Management
DC serotonin drugsSupportive care: O2, IV fluids, cardiac monitoring,Sedation with benzodiazepines; should not be
restrained No butyrophenones (haloperidol, droperidol);
anticholinergic effect inhibits sweatingSerotonin antagonists in severely ill (Cyprohepadine;
histamine receptor antagonist)Hyperthermia: Critical to treat aggressively to avoid
complications may require paralysis, intubation
Do not use antipyretics; not due to alteration in hypothalamic temp set point

95
Serotonin Syndrome Management
Autonomic instability HTN: short acting agents (e.g., nitroprusside ) not LA
(e.g., propranolol)Hypotension- short acting agents
(epinephrine, norepinephrine) Avoid indirect agents (e.g., dopamine) bc
when monoanimine oxidase is inhibited epi and norepi production not controlled
Severe case need ICU

96
Libby Zion Case
Libby Zion-18 yo college freshmanNew York Hospital ED at night with temp 103.5“Jerky movements”, rx meperidine, Haldol, and restraintsTemp 107 next AMDies cardiac arrestPGY-2 had 40 patientsAccreditation Council Graduate Medical
Education

97
Co-occurring Movement Disorders: Tremor
Movement DO with tremor can worse with psychotropic drug tx Essential tremor and ataxias have action type tremors ET any age, equal in MF, autosomal dominant, variable
presentation, progressive, often ↓/stop in sleepMany antidepressants, antipsychotics, and mood
stabilizers/AEDsAlso immunosuppressant's, oncology meds (e.g..,
thalidomide and cytarabine), bronchodilators, and caffeine will worsen action tremors and should be used carefully
Also alcohol, nicotine, benzo WD

98
Drugs Causing Tremor
Cardiac (amiodarone 1/3 pts), procainamide, others)
Epinephrine and norepinephrineWeight loss medication (tiratricol)Too much levothyroxine Tetrabenazine, a medicine to treat excessive
movement disorderOther: Wilson’s disease(DO copper
metabolism) hyperthyroidism, pheochromocytoma

99
Drugs Causing Tremor
Bronchodilators (theophylline, albuterol)Immunosuppressant's (cyclosporine, 40% but mild,
tacrolimus- mostly liver transplant and RA pts. can be disabling)
Mood stabilizers (lithium-30%, Valproic, 25%, starts after 3 mos. Long acting form may help avoid)
Selective serotonin reuptake inhibitors (20%; starts after 2-3 months)
Tricyclic antidepressants ↑ 20%Certain antivirals (acyclovir, vidarabine)Weight loss medication (tiratricol)Tetrabenazine (to tx excessive movement disorder)

100
Drug-Induced Tremor Tx
Lab and imaging studies usually normalStop drugLower doseAdd propranolol if lowering dose or changing
med not feasible

101
Drug vs.PD
Drug-induced tremors: Both L & R side (but maybe not equally)
Usually face, hands, arms, eyelids; rarely lower bodyParkinson’s affects primarily one side May have shaky voice, nodding yes or noSymptoms stop when med stopped
Usually start within an hour of taking offending med May take months for tremor to subside – up to 18
Parkinson's chronic and progressiveNo brain degeneration; Parkinson’s causes brain
degeneration in a specific area↑ risk in older people, Hx renal or hepatic disease, medical or neuro
disease, women, HIV +, hx of dementia

102
References
Bear, M. F., Connors, B. W., Paradiso, M. A. (Eds.). (2007). Neuroscience: Exploring the brain. (3rd ed.). Baltimore: Lippincott.
Brady, M. C., Scher, L. M., & Newman, W. (2013). “I just saw Big Bird. He was 100 feet tall!” Malingering in the emergency room. Current Psychiatry, 33(12),33-39.
Brody, J. E. (2007. February 27). A mix of medicines that can be lethal. New York Times, Retrieved from http://www.nytimes.com/2007/02/27/health/27brody.html?_r=0
Brown,C. H. (2010). Drug-induced serotonin syndrome. US Pharmacist, 35(11), HS-16-HS-21. http://www.uspharmacist.com/content/d/feature/c/23707/

103
References
Caroff, S.A., Hurford, I.,Lybrand, J. & Campbell, E. C. (2011). Movement disorders induced by antipsychotic drugs: Implications of the CATIE Schizophrenia Trial. Neurologic Clinics, 29(1), 127–viii.
Hallett, M., Cloniger, C. R., Fahn, S. Janovic, J., Lang, A. E., & Yudovsky, S. C. (2005). Psychogenic movement disorders. Baltimore, MD: LWW.
Peluso, M. J., Lewis, S.W., Barnes T.R.E., & Jones, P. B. (2012). Extrapyramidal motor side-effects of first- and second-generation antipsychotic drugs. British Journal of Psychiatry, 200, 387-392.
Sa, D. S., Galvez-Jimenez, N., & Lang, A. E. (2011).Movement disorders. (3rd ed.). New York, NY: McGraw Hill.

104
References
Vorvick, L. J. (2012, July 15). Drug-induced tremor. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/article/000765.htm
Watts, R. L., Standaert, D. A., & Obeso, J. A. (2013, March12). Jumping Frenchmen of Maine. Retrieved from http://www.rarediseases.org/rare-disease-information/rare-diseases/byID/380/viewFullReport
Wint, C. (2012, July 20). Drug Induced Tremor. Retrieved from http://www.healthline.com/health/drug-induced-tremor#Symptoms
Woods, S.W., Morgenstern, H., Saksa, J. R., Walsh, B. C., Sullivan, M. C., Money, R., Hawkins, K. A.,Ralitza, V, et al. (2010). Incidence of tardive dyskinesia with atypical and conventional antipsychotic medications: Prospective cohort study. Journal of Clinical Psychiatry, 71(4), 463-474.