Embed Size (px)
Citation preview
9/26/17
1
IT'S NOT IN YOUR HEAD BIOLOGICAL RATIONALES OF PSYCHOLOGICAL TREATMENT FOR CHRONIC PAIN.
JILL FANCHER, PhD
DIRECTOR OF PAIN MANAGEMENT
NORTHWEST RETURN TO WORK
LYNNWOOD, WASHINGTON
DISCLOSURES
• Nothing to disclose
REASONS FOR PSYCH REFERRAL
• Coping
• Pain management
• Pain reduction
• Compliance/Adherence
• Associated depression/anxiety
9/26/17
2
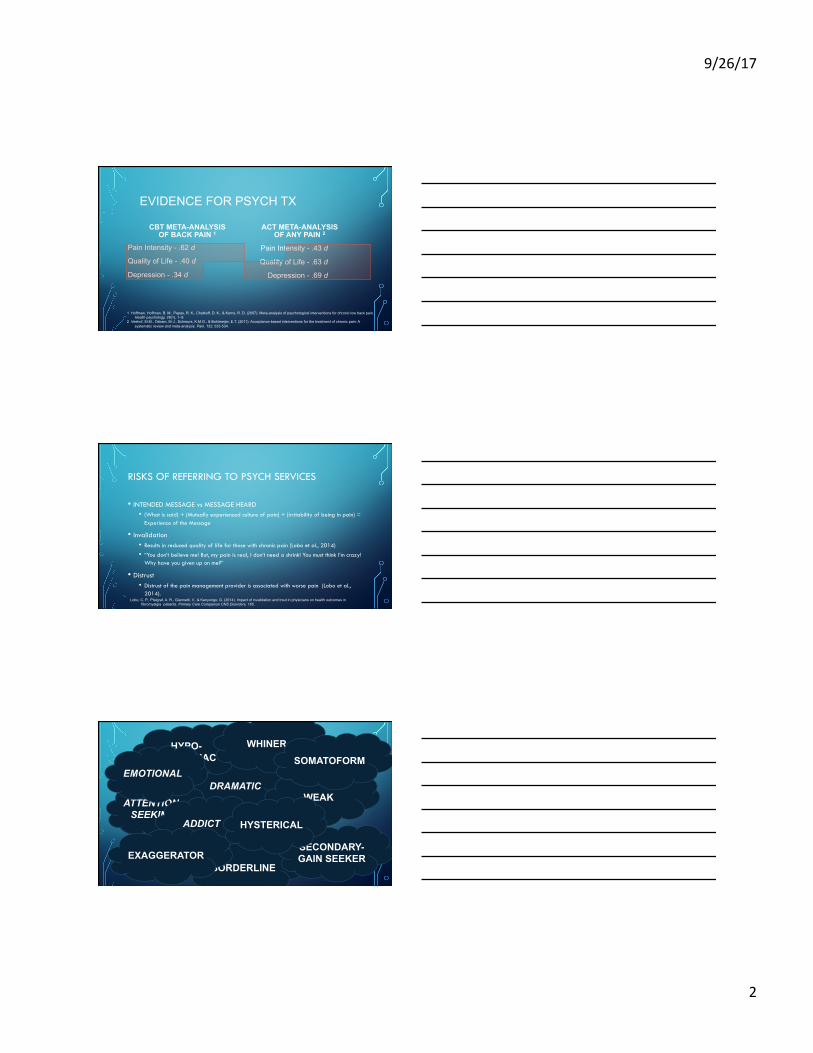
EVIDENCE FOR PSYCH TX
CBT META-ANALYSIS OF BACK PAIN 1
Pain Intensity - .62 d
Quality of Life - .40 d
Depression - .34 d
ACT META-ANALYSIS OF ANY PAIN 2
Pain Intensity - .43 d
Quality of Life - .63 d
Depression - .69 d
1 Hoffman, Hoffman, B. M., Papas, R. K., Chatkoff, D. K., & Kerns, R. D. (2007). Meta-analysis of psychological interventions for chronic low back pain. Health psychology, 26(1), 1–9.
2 Veehof, M.M., Oskam, M-J., Schreurs, K.M.G., & Bohlmeijer, E.T. (2011). Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain, 152, 533-534.
RISKS OF REFERRING TO PSYCH SERVICES
• INTENDED MESSAGE vs MESSAGE HEARD • (What is said) + (Mutually experienced culture of pain) + (irritability of being in pain) =
Experience of the Message
• Invalidation • Results in reduced quality of life for those with chronic pain (Lobo et al., 2014)
• “You don’t believe me! But, my pain is real, I don’t need a shrink! You must think I’m crazy! Why have you given up on me?”
• Distrust • Distrust of the pain management provider is associated with worse pain (Lobo et al.,
2014). Lobo, C. P., Pfalgraf, A. R., Giannetti, V., & Kanyongo, G. (2014). Impact of invalidation and trsut in physicians on health outcomes in
fibromyalgia patients. Primary Care Companion CNS Disorders, 165.
I’ve given up on you.
It isn’t real pain.
I can’t find any PHYSICAL reason why you are in this
much pain.
It can’t really be THAT bad!
It’s all in your head. DRAMATIC
ATTENTION-SEEKING
ADDICT
BORDERLINE
HYPO-CHONDRIAC
SECONDARY-GAIN SEEKER EXAGGERATOR
WHINER
WEAK
SOMATOFORM EMOTIONAL
HYSTERICAL
9/26/17
3
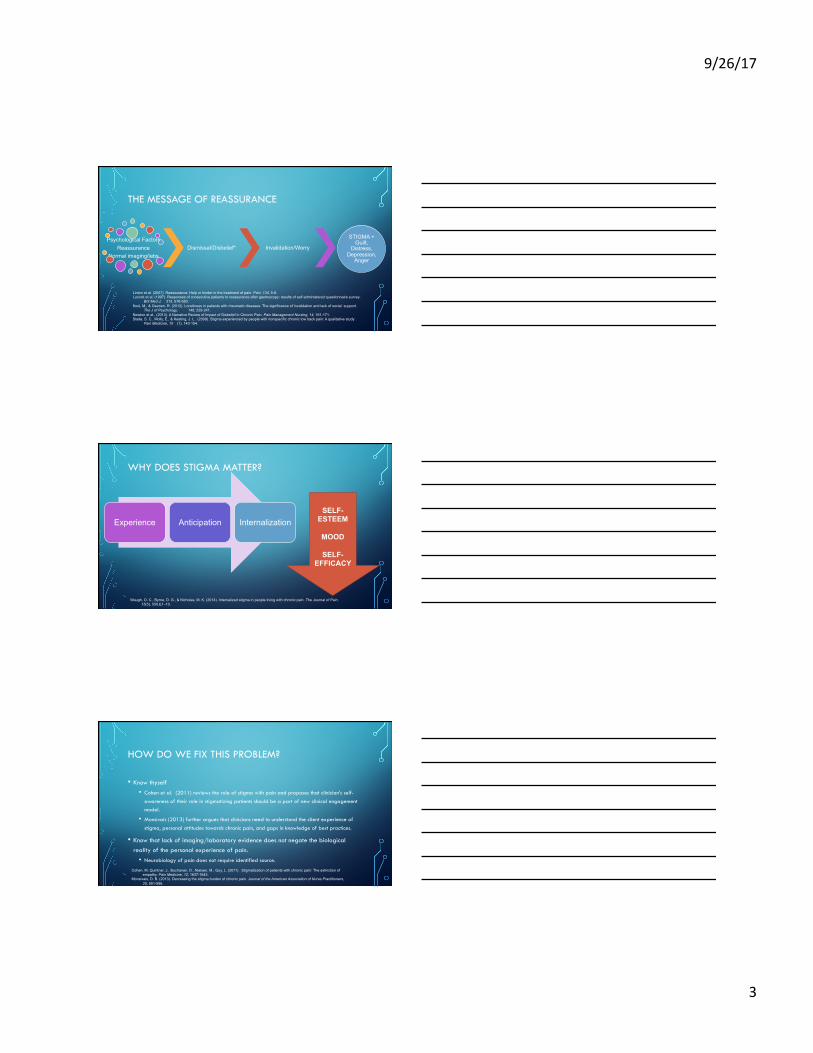
THE MESSAGE OF REASSURANCE
Psychological Factors Reassurance
Normal imaging/labs Dismissal/Disbelief* Invalidation/Worry
STIGMA + Guilt,
Distress, Depression,
Anger
Linton et al. (2007). Reassurance: Help or hinder in the treatment of pain. Pain, 134, 5-8. Lucock et al. (1997). Responses of consecutive patients to reassurance after gastroscopy: results of self administered questionnaire survey.
Brit Med J, 315, 576-580. Kool, M., & Geenen, R. (2012). Loneliness in patients with rheumatic diseases: The significance of invalidation and lack of social support.
The J of Psychology, 146, 229-241. Newton et al., (2013). A Narrative Review of Impact of Disbelief in Chronic Pain. Pain Management Nursing, 14, 161-171. Slade, S. C., Molly, E., & Keating, J. L. (2009). Stigma experienced by people with nonspecific chronic low back pain: A qualitative study .
Pain Medicine, 10 (1), 143-154.
WHY DOES STIGMA MATTER?
Experience Anticipation Internalization SELF-
ESTEEM
MOOD
SELF-EFFICACY
Waugh, O. C., Byrne, D. G., & Nicholas, M. K. (2014). Internalized stigma in people living with chronic pain. The Journal of Pain, 15(5), 550.E1–10.
HOW DO WE FIX THIS PROBLEM?
• Know thyself • Cohen et al. (2011) reviews the role of stigma with pain and proposes that clinician’s self-
awareness of their role in stigmatizing patients should be a part of new clinical engagement model.
• Monsivais (2013) further argues that clinicians need to understand the client experience of stigma, personal attitudes towards chronic pain, and gaps in knowledge of best practices.
• Know that lack of imaging/laboratory evidence does not negate the biological reality of the personal experience of pain.
• Neurobiology of pain does not require identified source.
Cohen, M, Quintner, J., Buchanan, D., Nielsen, M., Guy, L. (2011). Stigmatization of patients with chronic pain: The extinction of empathy. Pain Medicine, 12, 1637-1643.
Monsivais, D. B. (2013). Decreasing the stigma burden of chronic pain. Journal of the American Association of Nurse Practitioners, 25, 551-556.
9/26/17
4
• Validate the person’s experience
• Provides the rationale for treatments – even psychology
• DOUBLES Likelihood of ADHERENCE 1
• Reduces negative affect & worry1
• Pain biology education serves as its own intervention • Reducing pain, reducing worry, and improving physical functioning2
1 Linton et al. (2012). Painfully reassuring? The effects of validation on emotions and adherence in a pain test. European J of Pain, 16, 592-595. 2 Van oosterwijck, j., Meeus, M., Paul, L., De Schryver, M., Pascal, A., Lambrecht, L., & Nijs, J. (2013). Pain physiology education improves health status and
endogenous pain inhibition in fibromyalgia: A double-blind randomized controlled trial, Journal of Pain, 29(10), 873–882.
BIOLOGICAL EXPLANATIONS OF PAIN
VALIDATION
Thoughts, experiences, feelings are understandable and legitimate, regardless of whether you agree with the veracity of the claim.
”It must be frustrating to have so much pain, I wonder how you will be able to manage your activities.” 1
“A validating communication style seems to be beneficial for enhancing patient satisfaction, as well as diminishing negative affect and pain intensity ratings.” 2
1 Edmond, S. N., & Keefe, F. J. (2015). Validating pain communication: Current state of the science. Pain, 156, 215-219. 2 Vangronsveld KL, & Linton SJ. (2012). The effect of validating and invalidating communication on satisfaction, pain and affect in nurses suffering from low
back pain during a semistructured interview. European J of Pain, 16, 239-246.
BIOLOGICAL EXPLANATIONS OF PAIN • Simple, straightforward, includes full experience
• Provider fear of not being 100% accurate
• Practice metaphors • Pain is like a wild animal
• Tissues and spray bottles
• Resources • Eliot Krane’s Ted Talk: https://www.ted.com/talks/elliot_krane_the_mystery_of_chronic_pain
• Animation of Acute Pain, Salience, Distraction, and Chronic Pain: https://ed.ted.com/lessons/how-does-your-brain-respond-to-pain-karen-d-davis
• How Pain Works: Acute and Persistent Pain https://masteringpaininstitute.com/how-pain-works/
9/26/17
5
BIOLOGICAL EXPLANATIONS OF SPECIFIC PAIN MANAGEMENT STRATEGIES
• Worry Management
• Distraction
• Mindfulness
• Progressive Muscle Relaxation
• And MANY MORE!
BIOLOGICAL EXPLANATIONS OF WORRY MANAGEMENT
PROVIDER LEVEL KNOWLEDGE
• Not amplifying inflammatory interleukins
CONSUMER LEVEL LANGUAGE
• Worry may increase inflammation in the body for hours, so we want to stop anything that will make inflammation worse.
Darnall, B., Aickin, M, & Zwickey, H. (2010). Pilot study of inflammatory responses following a negative imaginal focus in persons with chronic pain: analysis by sex/gender, Gender Medicine, 7(3), 247-260.
BIOLOGICAL EXPLANATIONS OF DISTRACTION
PROVIDER LEVEL KNOWLEDGE
• Distraction correlated with activation of the PAG and top-down inhibitory.
• These have been associated with the endogenous opioid.
CONSUMER LEVEL LANGUAGE
• Pain naturally grabs your attention, that is its job.
• Redirecting attention can help your body to release its own natural pain medicine and opioids, in your body.
Tracey, I., Ploghaus, A., Gati, J. S., Clare, S., Smith, S., Menon, R. S., & Mathews, P.M. (2002). Imaging attentional modulation of pain in the periaqueductal gray in humans, The Journal of Neuroscience, 22(7), 2748-2752.
Valet, M., Sprenger, T., Boecker, H., Willoch, F., Rummeny, E., Conrad, B., Erhard, P., & Tolle, T. R. (2004). Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain--an fmri analysis. Pain, 109(3), 399–408.
Wiech, K., Ploner, M., & Tracey, I. (2008). Neurocognitive aspects of pain perception. Trends in Cognitive Sciences, 12, 306-313.
9/26/17
6
BIOLOGICAL EXPLANATIONS OF MINDFULNESS
PROVIDER LEVEL KNOWLEDGE • Mindfulness training reduces thalamic
activation and may provide a limbic gating mechanism for changes in the intensity and suffering associated with pain.1
• Further, there is evidence that analgesia produced by mindfulness is NOT mediated by endogenous opioids.2
CONSUMER LEVEL LANGUAGE
• Changes how your brain listens to the alarm signals and can now listen to the different aspects of the sensations like pressure, intensity, without feeling so overwhelmed by the pain.
1 Zeidan, F., Martucci, K. T., Kraft, R. A, gordon, N. S., Mchaffie, J. G., & Coghill, R. C. (2011). Brain mechanisms supporting the modulation of pain by mindfulness meditation. The Journal of Neuroscience, 31(14), 5540–8.
2 Zeidan, F., Adler-neal, A. L., Wells, R. E., Stagnaro, E., May, L. M., Eisenach, J. C., McHaffie, J. C., & Coghill, R. C. (2016). Mindfulness-meditation-based pain relief is not mediated by endogenous opioids. The Journal of Neuroscience, 36(11), 3391– 3397.
BIOLOGICAL EXPLANATIONS OF PROGRESSIVE MUSCLE RELAXATION
PROVIDER LEVEL KNOWLEDGE
• EMG studies show that it reduces muscle tension similarly to biofeedback.
CONSUMER LEVEL LANGUAGE
• Your muscles get tense and guard areas of your body that feel painful. This muscle guarding will cause its own pain. We can reduce this tension telling those muscles first to tighten, then they can release more fully.
Sime, W. E., & DeGood, D. E. (1977). Effect of EMG Biofeedback and Progressive Muscle Relaxation Training on Awareness of Frontalis Muscle Tension. Psychophysiology, 14, 522-530.
APPROPRIATE USE WITH DIFFERENT POPULATIONS
• Health Literacy • Sperber et al (2013) noted that those with lowest health literacy had the strongest effects from a
telephone support group for OA. • SHOW don’t just TELL
• Education level • Talking “over” someone and patronization • The engineer
• Treating other pain providers
• Non-English speaking and psycho-ed through interpretation • “Mindfulness”
Sperber, N. R., Bosworth, H. B., Coffman, C. J., Lindquist, J. H., Oddone, E. Z., Weinberger, M., & Allen, K. D. (2013). Differences in osteoarthritis self-management support intervention outcomes according to race and health literacy. Health Education Research, 28 (3), 502-511.
9/26/17
7
THANK YOU!
Any questions?
Contact information:
Jill Fancher, PhD
www.nwrtw.com
MasteringPainInstitute.com