Embed Size (px)
DESCRIPTION
The Continuing Role of AIDS Drug Assistance Programs (ADAPs) As Health Insurance Coverage is Expanded by the Affordable Care Act ADAP Advocacy Association April 14, 2014. Jeffrey S. Crowley Distinguished Scholar/Program Director, National HIV/AIDS Initiative - PowerPoint PPT Presentation
Citation preview

Jeffrey S. CrowleyDistinguished Scholar/Program Director, National HIV/AIDS InitiativeO’Neill Institute for National and Global Health LawGeorgetown Law
The Continuing Role of AIDS Drug Assistance Programs (ADAPs) As Health Insurance Coverage is Expanded by the Affordable Care Act
ADAP Advocacy AssociationApril 14, 2014
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law

As we enter a new environment created by the Affordable Care Act, it is important to remember:• The Ryan White Program is likely to remain critically
necessary to the HIV response• The context in which Ryan White operates is changing,
and this creates new opportunities
The recent introduction of legislation to make changes to Ryan White has raised anew questions about when to reauthorize the program. For political, policy, and budgetary reasons, most people in the HIV community are not pushing for immediate changes to the program. The program was funded by Congress in early 2014 and can continue without an authorization. Instead of arguing about when, I believe the HIV community needs to continue educating policymakers and the public about the continued need for the program. And, we need to step out of our comfort zones to consider pragmatic changes to make the program maximally effective in the new health care landscape.
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
Ryan White Reauthorization will wait

Affordable Care Act (ACA) Overview
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1

Efforts to expand access to insurance coverage and reform how health services in the US are financed and delivered go back roughly a century
• Across the spectrum of health systems among developed nations, the US has the most market oriented system. The ACA maintains that market orientation
• Despite investing more than any other nation in terms of total health spending and per capita spending, the US health system performs poorly on many population-level metrics, and we face a major challenge of increasing costs . Also, we are witnessing continued erosion of the employer-sponsored market
• Roughly 16% of the US population, or about 50 million Americans are uninsured
• The US health system supports innovation and the highest quality care is often found here, yet we generally get less for our investment in terms of improved health than other nations
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1 The ACA responds to pressing national concerns

Expansions of coverage or services
• Medicaid: Coverage for childless adults
• Medicare: ADAP counts toward TrOOP
• Medicare: Closing the drug coverage gap
• Insurance protections for consumers: Lifetime limits and rescission on coverage
• Insurance protections for consumers: Pre-existing condition insurance plan (PCIP)
• Young adult dependent coverage
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1
Key ACA provisions have been in effect for a while

Prevention• Prevention and Public Health Fund
• Free prevention services and annual HIV screenings for women
Health system improvements• Medicaid: Health homes
• Medicaid: Increased payments for primary care
• Medicaid/Medicare: Integrated care for dual eligibles
• New investments in health centers and National Health Service Corps
• Health disparities data collection
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1
Key ACA provisions have been in effect for a while

Key provisions
• Individual requirement to have insurance
• Expanded Medicaid coverage
• Establishment of health insurance marketplaces
• Premium and cost sharing subsidies
• Guaranteed availability of coverage: prohibits pre-existing condition exclusions
• No annual limit on coverage
• Essential health benefits (EHBs) and essential community providers (ECPs)
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1
Most coverage expansions took effect on January 1st

ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1
Slight majority of HIV+ in states expanding Medicaid
Source: Kaiser Family Foundation.
Note: Roughly 45% of HIV+ are in states not expanding Medicaid. States not expanding are concentrated in the south, a region disproportionately impacted by HIV with a relatively weak health care and HIV care capacity.

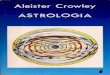
In care: Of the roughly 407,000 people with HIV between age 19-64 in care, roughly 70,000 are uninsured who could gain new coverage:
– With current 26 states expanding Medicaid: 26,560 gain Medicaid, 25,190 receive subsidized marketplace coverage, 17,980 have access to unsubsidized marketplace coverage.
– If all states expanded Medicaid: 46,910 gain Medicaid, 20,290 receive subsidized marketplace coverage, 2,520 have access to unsubsidized marketplace coverage.
Not in care: Of the roughly 700,000 people with HIV aged 19-64 not in care, if their insurance/income status mirrors those in care, approximately 124,000 could gain new coverage if all states expanded Medicaid.
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
1
How Many people with HIV Will Gain New Coverage?

Overview of the Ryan White
HIV/AIDS Program
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2

• Third largest source of financing for HIV care after Medicaid and Medicare. Roughly 500,000 people with HIV receive at least one service from Ryan White, some count on it for most of their care• FY 2012 federal funding level was $2.4 billion
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2Ryan White fills many roles

ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2
Biggest HIV discretionary program, yet smaller than Medicaid or Medicare

ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2
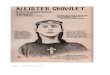
Federal Ryan White Funding (adjusted for inflation) and HIV Prevalence, 1991-2012
$-
$500
$1,000
$1,500
$2,000
$2,500
$3,000
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
Ryan White Funding, Current $Ryan White Funding, Constant 1991 $HIV/AIDS Prevalence
Funding Prevalence
SOURCE: Updating the Ryan White HIV/AIDS Program for a New Era: Key Issues and Questions for the Future, Kaiser Family Foundation, April 2013.NOTES: The Consumer Price Index (CPI) from the Bureau of Labor Statistics (BLS) was used to adjust for inflation. HIV prevalence data are estimates based on analysis of data from CDC. SOURCES: Funding amounts based on Kaiser Family Foundation analysis of data from OMB, CBJs, appropriations bills, and CRS; Prevalence based on data from CDC; U.S. Department of Labor, Bureau of Labor Statistics.

•
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2
The majority of Ryan White clients use it to supplement other forms of coverage

ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2
Ryan White currently pays for medical care and other critical support services

ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
2
Ryan White services are critical to engagement in care

The Future Role of ADAPs
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
3

• ADAP is the largest component of Ryan White. In FY2014, Congress appropriated $900 million in federal funds (a $14 million increase)
• Has been a high priority for the Obama Administration, as evidenced by consistent increases in the President’s budget and through emergency actions taken to direct supplement resources to the program
• In FY 2013, states contributed nearly $226 million to ADAPs, or about 11% of the total ADAP budget. Manufacturer rebates of nearly $900 million were paid back to states further extending the purchasing power of ADAP programs.
• In FY 2013, 72% of ADAP spending was on direct expenditures for prescription drugs
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
3
Key Facts about ADAPs

• Began implementing health reform more than a decade ago, to near universal access
• Changed how Ryan White funding was used in state, with greater share of resources shifting from paying for care to paying for:
– Insurance continuation– Co-payments– Support services to help engage people with HIV in care
and support adherence
• State has observed decline in new HIV diagnoses, high viral load suppression
• Attributes to the combination of expanded insurance coverage, ART access, and extensive HIV community care network including Ryan White providers
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
3
Massachusetts gives us hope
SOURCES: Cranston K et al. (2012). “Controlling the Massachusetts HIV Epidemic: Triangulated Measures of Care Access and HIV Incidence”,19th International AIDS Conference: Abstract no. TUPE212; Kevin Cranston, Personal communication, January 22, 2013.

• Massachusetts may foreshadow some of the anticipated changes to ADAPs with an increasing emphasis on payment for co-payments.
• Even after the ACA, there will remain a need for a program to pay for prescription drugs…for people with no other coverage, for non-covered medications, and for people who fall through the cracks such as during insurance transitions.
• Nonetheless, we make large investments in pharmaceuticals to get people with HIV to achieve and sustain effective viral suppression. As the treatment cascade shows, a variety of supports are often needed to help people access and gain the benefits of effective antiretroviral therapy.
• Funding for ADAP has been more robust than other parts of Ryan White. This is due to the central role of ART in HIV treatment, but also due to the unique collaboration between people with HIV, community advocates, ADAP program administrators, and industry. We all have a stake in maintaining this collaboration to keep all parties invested in strong ADAP programs.
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
3
How ADAPs support effective viral suppression may change

By maximizing the opportunities available to us, we are poised to make major progress at getting more Americans with HIV better supported in systems of care in ways that lead to much better population-level viral suppression.The ACA is an important opportunity. But, there will be challenges along the way.Some people may reasonably ask if we will still need the Ryan White Program after the ACA has expanded insurance coverage. We need to unequivocally and convincingly answer yes…But, as a community, we need to do the hard work of showing how we are changing the program to be maximally effective in the new environment.We cannot end the HIV epidemic in the United States if we do great things in New York, but infections explode in the South. And, we cannot end the epidemic if we keep infection rates falling for all groups, except for young gay men. We have a lot of work to do, but much progress is possible.
For the foreseeable future, the Ryan White HIV/AIDS Program and its AIDS Drug Assistance Program are essential to helping us move closer to ending the HIV epidemic in the United States.
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law
Parting thoughts…

Thank you!
ADAP Advocacy Association
Jeffrey S. CrowleyDistinguished Scholar/
Program Director, National HIV/AIDS Initiative
O’Neill InstituteGeorgetown Law