Embed Size (px)
Citation preview

J Head Trauma RehabilVol. 20, No. 3, pp. 257–269c© 2005 Lippincott Williams & Wilkins, Inc.
Risk of PosthospitalizationMortality Among Persons WithTraumatic Brain Injury, SouthCarolina 1999–2001
Anbesaw Wolde Selassie, DrPH; Melissa Lee McCarthy,MS, ScD; Pamela Lynn Ferguson, PhD, RN;Jianmin Tian, MSPH; Jean A. Langlois, ScD, MPH
Traumatic brain injury (TBI) negatively impacts long-term survival. However, little is known aboutthe likelihood of death within the first year following hospital discharge. This study examinedmortality among a representative sample of 3679 persons within 1 year of being discharged fromany of 62 acute care hospitals in South Carolina following TBI and identified the factors associatedwith early death using a multivariable Cox proportional hazards model. The mortality experience ofthe cohort was also compared with that of the general population by using standardized mortalityratios for selected causes of death by age, adjusted for race and sex. Key words: follow-up study,mortality rate, risk ratio, standardized mortality ratio, survival rate, traumatic brain injury
BACKGROUND
In 2001, injuries were the fourth leadingcause of death in the United States.1 Traumatic
From the Department of Biostatistics,Bioinformatics, and Epidemiology, MedicalUniversity of South Carolina, Charleston, SC (DrsSelassie and Ferguson); Department of EmergencyMedicine, The Johns Hopkins University School ofMedicine, Baltimore, Md (Dr McCarthy); Division ofBiostatistics and Health GIS, Public Health Statisticsand Information System, South CarolinaDepartment of Health and Environmental Control,Charleston, SC (Mr Tian); and National Center forInjury Prevention and Control, Centers for DiseaseControl and Prevention, Atlanta, Ga (Dr Langlois).
This study was funded by cooperative agreementU17/CCU421926 from the National Center for InjuryPrevention and Control, The Centers for Disease Con-trol and Prevention.
The Issue Editors sincerely thank Wesley Rutland-Brown, the Assistant to the Editor, for his invaluablehelp with this manuscript.
Corresponding author: Anbesaw Selassie, DrPH, De-partment of Biostatistics, Bioinformatics, and Epidemi-ology, Medical University of South Carolina, 135 Can-non Street, PO Box 250835, Charleston, SC 29425(e-mail: [email protected]).
brain injuries (TBIs) are associated with onethird of all injury-related deaths2—because ofthe brain being the most common anatomicsite involved in death from trauma.3–5 Of the230,000 persons hospitalized with a TBI eachyear, 5.6% will die during their hospital stay.6
Less well known, however, is the impact ofTBI on life expectancy among those who sur-vive the acute injury.
Follow-up studies suggest that personswho experience a TBI have shortened lifeexpectancies.7–15 In one study, in which ap-proximately 1200 World War I veterans werefollowed for up to 50 years postinjury, re-searchers concluded that veterans who hadsustained a head injury had a 4-year shorterlife expectancy, on average, than the un-wounded veterans.13 However, a study of acohort of 1127 Vietnam veterans with braininjury revealed that although excess mortal-ity occurred during the first 3 years postin-jury, veterans who survived longer had alife expectancy similar to that of the generalpopulation.10 More recently, researchers fol-lowed 2320 Californians who received statemedical services for long-term, TBI-associated
257

258 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
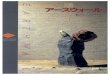
Figure 1. Eligibility criteria and sampling strategy of study cohort.
disability and documented a 3-fold excessmortality risk in the study cohort up to 10years postinjury compared with the generalpopulation.7
Although most studies have found thatTBI negatively impacts long-term survival, thestudies have examined only specific studypopulations and not a representative sampleof persons with TBI. Furthermore, almost allof the past studies have focused on long-termmortality (ie, ≥1 year postinjury) as opposedto early mortality (ie, deaths that occur dur-ing the first year postinjury). The purpose ofthis report is to document mortality within15 months of hospital discharge for a repre-sentative sample of 3679 persons who weretreated for TBI at acute care hospitals in SouthCarolina and to identify factors associatedwith early death.
METHODS
Data for this study were collected as partof the South Carolina Traumatic Brain InjuryFollow-Up Registry (SCTBIFR). The SCTBIFR
is a population-based cohort study designedto document the short- and mid-term healthconsequences of persons hospitalized with aTBI.
Study population and setting
South Carolina residents aged 15 years orolder who sustained a TBI and were dis-charged from any of the 62 acute care, non-federal hospitals in the state from January 1,1999, through December 31, 2001, were eli-gible for the study (Fig 1). Using the South Car-olina hospital discharge data as the samplingframe, 6583 TBI-related hospitalizations wereidentified using the Center for Disease Con-trol and Prevention’s (CDC) case definitionsand sampling guidance.16,17 A 2-stage strat-ified random sampling procedure was usedto select cases based on hospital size andTBI severity. To achieve a final sample of ap-proximately 1300 persons per year, 75% ofcases were first randomly selected based onhospital size. Among those initially selected,67% of those with a severe TBI (AIS [Abbrevi-ated Injury Scale] ≥ 3) and 33% with a mild

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 259
TBI were then randomly selected, resultingin a final sample of 3950 TBI cases over the3-year study period. The SCTBIFR excluded271 cases who were either (1) non-Englishspeaking (n = 21), (2) nonresidents of SouthCarolina (n = 113), (3) prisoners (n = 77), or(4) medically unable to complete the follow-up interview (n = 60).
Data sources
Medical record, hospital discharge, anddeath-certificate data were used. The medicalrecords of all patients selected for participa-tion were reviewed by accredited health infor-mation specialists prior to the first interviewto confirm the TBI diagnosis and to abstractcontact information for follow-up.
The statewide hospital discharge data pro-vided all demographic information and up to10 International Classification of Diseases,9th Revision, Clinical Modification (ICD-9-CM) discharge diagnosis codes.18 To rate theseverity of all injuries sustained, the ICDMAP-90 software was used to convert hospitaldischarge ICD-9-CM diagnosis codes into AISscores.19 The AIS, one of the most widely usedanatomic measures of injury severity,20,21 isused to classify each injury according to thetype of injury and to assign a severity ratingranging from 1 (minor) to 6 (unsurvivable) ac-cording to its associated threat to life.22 Forthis study, the severity of the TBI was de-termined by the maximum ICD/AIS score ofthe head region; TBI was classified as eithermild (head AIS = 2), moderate (head AIS =3), or severe (head AIS ≥4). A major associ-ated injury was defined as an injury to an AISbody region other than the head (eg, chest,abdomen, and extremities) with a maximumICD/AIS severity rating of ≥2. ICD-9-CM di-agnosis codes were also used to identify thepresence of comorbid conditions using a co-morbidity scale developed for administrativedata.23
Finally, multiple cause-of-death data(MCDD) were obtained from the Division ofVital Records at the South Carolina Depart-ment of Health and Environmental Control(SCDHEC) for persons who died during the
follow-up period. The MCDD file includesinformation regarding personal identifiers,causes of death, and timing of death for allSouth Carolina residents who die. The under-lying cause of death and up to 20 contributingcauses of death are coded according to theInternational Classification of Diseases,10th Revision (ICD-10) for all study years.24
Procedures
This study was reviewed and approvedby the Institutional Review Boards (IRBs) ofboth the Medical University of South Car-olina and the CDC. Approximately 1 year (±3months) after discharge from a TBI-relatedhospitalization, project personnel attemptedto contact all patients to conduct a telephoneinterview. When information was obtained in-dicating that a patient had not survived (eg, afamily member told the study personnel aboutthe death or the US Postal Service returnedthe study letter because the person had died),study personnel confirmed the death throughthe Social Security Death Index (SSDI).
A list of patients confirmed to be deadthrough the SSDI (as well as those not ableto be located) was submitted to the Divisionof Vital Records at SCDHEC. This list waslinked to the MCDD database using the de-ceased patient’s social security number, dateof birth, and first 4 letters of the last name.For those patients with an unknown socialsecurity number (n = 18), the date of birthand the first 4 letters of the last name andaddress were used. Of patients confirmeddead by the SSDI, 93% were linked to theMCDD database. The deaths of 5 additionalpatients who had previously not been locatedby study personnel were discovered when theMCDD database was merged with the studylist. Therefore, death certificate informationwas obtained for 94% of all known deathsthat occurred among study patients within 15months of hospital discharge.
Deaths were classified as either TBI-related(ie, underlying cause of death was an ex-ternal cause of injury [E code] and aTBI diagnosis was listed as a contributingcause), other injury–related (ie, E code was

260 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
underlying cause of death but TBI diagno-sis was not listed as a contributing cause),or noninjury-related (ie, underlying causeof death was not an E code) using CDCdefinitions.2,25
Analysis
Patient and injury characteristics betweenthe decedents and survivors were comparedusing a chi-square test statistic. The relation-ship between death and different risk factorswas examined as a function of time usingsurvival analysis techniques. The dependentvariable (survival time) was defined as time(days) between hospital discharge and death.Those who were alive at the 15th monthwere treated as censored observations. Vari-ables evaluated as risk factors included age,sex, race, comorbid conditions, type of insur-ance, location of residence, TBI severity, thepresence of a major associated injury(s), andtrauma center level of the hospital that pro-vided inpatient care (Table 1). Kaplan-Meierestimates of the cumulative proportion ofdeaths were computed for each risk factor.A log-rank test was used to test the homo-geneity of survival curves across TBI severitycategories. Possible interaction effects wereevaluated using Breslow-Day test of homo-geneity and Wald chi-square test statistics.26
Test statistics with P values of <.05 were con-sidered significant.
To estimate the combined effect of mul-tiple risk factors on deaths that occurredwithin 15 months of hospital discharge, aCox proportional hazards regression modelwas used. This model assumes that the haz-ard ratio when comparing any 2 specificationsof predictors is constant over time.27 Theproportional hazard assumption was testedwith the goodness-of-fit chi-square test, whichcompares the observed and expected sur-vival probabilities, and by graphical means us-ing the log–log Kaplan-Meier curves.27 Confi-dence intervals (95% CIs) for the hazard ratioswere calculated from the corresponding co-variance estimates and standard errors.28
Finally, the mortality experience of thestudy cohort was compared with the gen-
eral population using standardized mortalityratios (SMRs), defined as the ratio of observeddeaths to the expected number of deaths.Age, sex, and race-adjusted overall and cause-specific death rates for the US populationfor 2000 (the midpoint of our study period)were used to compute the expected numberof deaths.29 Cause-specific SMRs were calcu-lated for unintentional injuries (ICD-10: V01–X59, Y85–Y86), diseases of the heart (ICD-10: I00–I09, I11, I13, I20–I51), malignantneoplasms (ICD-10: C00–C97), cerebrovascu-lar diseases (ICD-10: I61–I64, I67), and allother diseases or injuries according to theNational Center for Health Statistics (NCHS)categories.30 For the SMRs, 95% CIs werecalculated by assuming that the observednumber of deaths followed a standard Pois-son distribution, with the mean and vari-ance being equal to the expected number ofdeaths estimated according to the referencepopulation.31
RESULTS
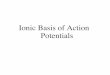
Of the 3679 eligible patients selected forparticipation, 3371 were alive (91.6%) and308 (8.4%) were deceased within 15 monthsof hospital discharge. Of the 308 deaths, 23%were injury-related, either TBI-related (17%)or other injury–related (6%). The mediannumber of days from hospital discharge untildeath was 93 (range, 1–453 days). Of the TBI-related deaths, 63% occurred within the first3 months of discharge compared with 47% ofnoninjury-related deaths. Estimated survivalcurves of the study cohort varied significantlydepending on the severity of the TBI (log-ranktest, P < .0001) (Fig 2).
Significant differences in the study popula-tion by survival status were observed within15 months postdischarge (Table 1). Dece-dents were more likely to be older, female, in-sured by Medicare, have more comorbidities,and have sustained a severe TBI than were sur-vivors (P < .001). In contrast, patients whowere alive at the end of the follow-up pe-riod were more likely to be white, from a ru-ral area, to have associated injuries, and to

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 261
Table 1. Percentage distribution of patient and injury characteristics within 15 months of aTBI-related hospital discharge,∗ by survival status
Total Deceased AliveCharacteristic (N = 3679) (N = 308) (N = 3371) P value
Age at time of injury, y <.00115–34 38.2 3.6 41.435–54 29.2 15.9 30.455–74 15.9 20.8 15.4≥75 16.7 59.7 12.8
Sex <.001Male 65.2 53.6 66.2Female 34.8 46.4 33.8
Race <.001White 71.2 81.8 70.3Non-white 28.8 18.2 29.7
Comorbid conditions <.001None 55.3 16.9 58.91 24.6 29.2 24.22 12.2 25.7 11.03 or more 7.9 28.3 6.0
Insurance status <.001Commercial 39.8 15.9 42.0Medicare/government 27.9 75.3 23.6Medicaid 7.6 2.9 8.1Uninsured 24.7 5.8 26.4
Place of residence .03Urban 60.9 66.6 60.4Rural 39.1 33.4 39.6
TBI severity† <.001Mild (ICD/AIS 1–2) 40.2 25.3 41.5Moderate (ICD/AIS 3) 17.5 14.0 17.8Severe (ICD/AIS ≥4) 42.4 60.7 40.7
Major associated injury to otherbody region <.001
None 58.9 73.4 57.61–2 body regions 35.9 25.0 36.9≥3 body regions 5.2 1.6 5.5
Trauma center level <.001Level 1 47.0 34.1 48.2Level 2 14.9 13.6 15.0Level 3 23.3 29.2 22.8Not a trauma center 14.8 23.1 14.0
∗One-year follow-up status determined 9–15 months postinjury.†ICDMAP-90 software was used to convert hospital discharge ICD-9-CM diagnosis codes into AIS scores.
have been treated at a Level 1 trauma center(P < .05).
The Cox proportional hazards regressionmodel was used to determine variables
associated with death (Table 2). Age was themost significant predictor of death; the olderthe injured patient, the higher the likelihoodof early mortality. Furthermore, a significant

262 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
Fig
ure
2.E
stim
ated
surv
ival
curv
eso
fth
eT
BI
coh
ort
stra
tifi
edb
yse
veri
tyo
fb
rain
inju
ry.

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 263
Table 2. Adjusted hazard ratios of mortality within 15 months of a TBI-related hospital discharge
Characteristic Hazard ratio∗ 95% CI†
Age and sex (years) (vs males aged 15–34 years)Males ≥75 14.34 6.24–32.94Females ≥75 9.12 3.95–21.05Males 55–74 5.41 2.37–12.37Females 55–74 4.25 1.78–10.17Males 35–54 2.97 1.33–6.64Females 35–54 6.29 2.72–14.53Females 15–34 0.64 0.14–3.04
Non–white race (vs white) 0.96 0.70–1.32Comorbid conditions (vs none)
≥3 3.95 2.66–5.872 2.60 1.76–3.831 1.82 1.25–2.64
Insurance status (vs commercial)Medicare/government 1.64 1.08–2.49Medicaid 1.14 0.55–2.38Uninsured 0.67 0.37–1.21
Urban residence (vs rural) 1.28 0.99–1.67TBI severity (vs mild)‡
Severe ICD/AIS ≥4 1.79 1.34–2.40Moderate ICD/AIS 3 1.39 0.93–2.08
Associated injury of AIS ≥ 2 (vs TBI only)≥3 or more body regions 0.81 0.29–2.251–2 body regions 1.13 0.84–1.50
Trauma center level (vs not a trauma center)Level 1 0.56 0.39–0.78Level 2 0.49 0.33–0.74Level 3 0.67 0.48–0.94
∗The Cox proportional hazards model was calculated on 288 patients’ cases for which the exact date of death wasdetermined.†Reference group is in parentheses for each covariate; confidence intervals (CIs) that do not include “1” are statisticallysignificant.‡ICDMAP-90 software was used to convert hospital discharge ICD-9-CM diagnosis codes into AIS scores.
interaction effect was noted between ageand sex on mortality. For all age groups (ex-cept persons aged 35–54 years), males weremore likely to die than females. Among pa-tients 35 to 54 years of age, females were6.3 times (95% CI, 2.7–14.5) and males were3.0 times (95% CI, 1.3–6.6) more likely todie than males aged 15 to 34 years, the ref-erence group (Table 2). Among patients aged35 to 54 years, females were more likely to diefrom noninjury-related conditions (68%) com-pared to males (36%), whereas for all other
age groups, the proportion of deaths causedby noninjury-related conditions was approxi-mately the same for both sexes.
The presence of comorbid conditions sig-nificantly influenced the likelihood of death.Patients with 3 or more comorbidities were4.0 times (95% CI, 2.7–5.9) more likely to diewithin the first year after injury comparedwith patients with no comorbidities. Of thosewho died within 15 months of hospital dis-charge, 48% had a cardiac-related comorbidity(eg, cardiac arrhythmia and congestive heart

264 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
Table 3. Standardized mortality ratios (SMRs) for selected causes of death, by age∗
Observed ExpectedAge (years) Cause of death deaths deaths SMR 95% CI†
15–34 Cancer 0 0.1 0.0 −Heart disease 1 0.8 12.2 0.0–47.9Unintentional injury 5 0.5 9.5 3.0–19.7Cerebrovascular diseases 0 0.0 0.0 −Other causes 4 0.7 5.4 1.4–12.0All causes‡ 11 1.5 7.5 3.7–12.6
35–54 Cancer 4 0.9 4.4 1.1–9.8Heart disease 5 0.7 7.2 2.3–15.0Unintentional injury 19 0.4 48.7 29.3–73.0Cerebrovascular diseases 2 0.1 16.7 1.6–47.9Other causes 14 1.4 9.8 5.4–15.7All causes‡ 49 3.5 13.9 10.3–18.0
55–74 Cancer 11 3.4 3.2 1.6–5.4Heart disease 11 2.7 4.1 2.0–6.9Unintentional injury 9 0.2 41.6 18.8–73.1Cerebrovascular diseases 7 0.5 14.7 5.8–27.6Other causes 23 3.0 7.7 4.9–11.2All causes‡ 64 9.8 6.5 5.0–8.2
≥75 Cancer 16 9.2 1.7 1.0–2.7Heart disease 33 18.0 1.8 1.3–2.5Unintentional injury 28 0.9 31.4 20.8–44.1Cerebrovascular diseases 27 4.7 5.7 3.8–8.1Other causes 69 19.0 3.6 2.8–4.6All causes‡ 184 51.8 3.6 3.1–4.1
All Cancer 31 10.2 3.1 2.1–4.2Heart disease 50 13.5 3.7 2.8–4.8Unintentional injury 61 1.7 36.3 27.8–46.0Cerebrovascular diseases 36 3.1 11.7 8.2–15.9Other causes 110 15.5 7.1 5.8–8.5All causes‡ 308 43.5 7.1 6.3–7.9
∗Rates are adjusted for race and sex.†Confidence intervals (CIs) that do not include “1” are statistically significant.‡The category of “All causes” includes 20 deaths where information on causes was not available.
failure); 29% had hypertension; 21% had afluid and electrolyte imbalance; 13% had can-cer; 11% had anemia, diabetes, or chronic ob-structive pulmonary disease; and 8% had apsychiatric condition.
The severity of the TBI, type of insurance,and level of trauma center within the hospi-tal that provided the acute medical care were
also significant determinants of death within15 months of hospital discharge. Patients whosustained severe TBI were 1.8 times (95%CI, 1.3–2.4) more likely to die postdischargecompared with those experiencing mild TBI.Those insured by Medicare were 1.6 times(95% CI, 1.1–2.5) more likely to die thanpatients covered by commercial insurance.

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 265
Being treated at a higher level trauma centerhad a protective effect on mortality. For ex-ample, patients who were treated at traumacenters that provide the most comprehensivetrauma care (ie, Level 1 centers) were 44%(95% CI, 0.4–0.8) less likely to die during thefollow-up period than those treated at hospi-tals that do not have a trauma center. Persons75 years of age or older had the highest mor-tality and were less likely to be treated at atrauma center than younger patients, regard-less of the severity of the TBI.
The SMRs of the study sample were deter-mined for selected causes of death (Table 3).Compared with the general US population,the study cohort experienced a 7-fold excessrisk of death overall (SMR = 7.1; 95% CI,6.3–7.9) within 15 months of hospital dis-charge. Unintentional injury deaths were themost frequent cause of death and were asso-ciated with a 36-fold excess risk of early death(SMR = 36.3; 95% CI, 27.8–46.0). The excessmortality risk for unintentional injury deathswas significant for all age groups, although itwas highest for persons aged 35 to 54 years. In67% of these unintentional injury deaths, thecause of death listed in the death certificatewas the same as the cause of injury noted dur-ing the initial hospitalization. Of the 61 per-sons who died from unintentional injury, 49(80%) had TBI listed on their death certificatesas a contributing cause of death. An additional6 decedents died from intentional injuries—3from suicide and 3 from assault. The study co-hort also experienced excess mortality risksfrom cerebrovascular diseases, heart diseases,and cancer, but these excess risks were smalland were not significant across all age groups.
DISCUSSION
This large, population-based cohort of per-sons in South Carolina hospitalized with a TBIexperienced considerable excess mortalitycompared with the US population within 15months of hospital discharge. To our knowl-edge, this is the first comprehensive mortalitystudy of a statewide representative sample ofUS civilians who sustained a TBI. Results from
this study indicate that several factors wereassociated with death within 15 months ofhospital discharge, including age, sex, thepresence of comorbidities, TBI severity, typeof insurance, and the type of hospital that pro-vided acute medical treatment. The leadingcause of death in the study cohort was un-intentional injuries; TBI was listed as a con-tributing cause in 80% of the unintentional in-jury deaths. In summary, TBI negatively im-pacted the survival of a significant proportionof the study sample during the 15 months fol-lowing hospital discharge.
Our results suggest that the causes for theexcess mortality experienced by the cohortare multifactorial. Older age was strongly as-sociated with death following hospital dis-charge. This finding is consistent with anotherfollow-up study of general trauma patients andwith numerous in-hospital trauma mortalitystudies.32–37 Elderly patients who are injuredmay have a harder time regaining their prein-jury level of health and avoiding complica-tions compared to younger patients.38–40 Thisfinding suggests that more resources shouldbe devoted to developing and implementingacute and postacute care interventions thatrestore preinjury function to patients withTBI as soon after injury as possible. In ad-dition, clinicians should monitor elderly pa-tients more closely during the postacute pe-riod since they are at increased risk of deathfollowing a TBI.
With the exception of persons 35 to 54years of age, males in the study cohortwere more likely to die after TBI hospital-ization than were females; the overall higherdeath rate for males with TBI is consistentwith the mortality patterns of the generalUS population.41 However, among personsaged 35 to 54 years, the death rate was high-est among females. The only difference be-tween this age group and the others was thecause of death. Specifically, females aged 35to 54 years were more likely to die from anoninjury-related condition compared withmales, but no specific noninjury-related con-dition was associated with most deaths amongfemales in this age group. This effect measure

266 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
modification between age and sex on deathfollowing hospital discharge warrants furtherinvestigation.
Underlying disease also contributed tothe excess mortality in our study cohort.The more comorbidities documented dur-ing the index hospitalization, the greater thelikelihood of death following discharge. Otherstudies also have noted a significant associa-tion between the presence of comorbiditiesand mortality during hospitalization34,39,42,43
and after hospital discharge.32,40 This findingemphasizes the importance of adopting pro-cesses of care that optimize concurrent treat-ment of injuries and associated medical prob-lems during both the acute and rehabilitativestages.32,44
In our study, the severity of the TBI alsoinfluenced the likelihood of death follow-ing hospital discharge. Although other stud-ies have noted an association between in-hospital mortality and the severity of theTBI,33,35–37,45–48 this study extends this findingto the early, postacute care phase. TBI seque-lae, such as decreased mobility and impairedcognitive function, contribute to decreasedsurvival following hospital discharge and aremore likely to occur among the more severelyinjured.15
Patients covered by Medicare or other gov-ernment insurance were more likely to diewithin 15 months of hospital discharge com-pared with those covered by commercial in-surance. Of the patients categorized as havinggovernmental insurance, 97% were coveredby Medicare; 16% of Medicare patients wereunder 60 years of age and thus were likely in-sured by Medicare because of disability ratherthan age. Medicare insurance could either rep-resent a surrogate measure of disability or ad-ditional comorbidity that was underreportedin the hospital discharge data. In either case,this finding supports the conclusion that un-derlying disease has a negative impact on sur-vival following a TBI.
Finally, patients who were treated at hos-pitals with trauma centers were significantlyless likely to die within 15 months of hospi-tal discharge compared with patients treated
at hospitals without trauma centers. Althoughseveral studies have documented the benefi-cial effects of trauma centers on in-hospitalmortality,49–51 our results are the first to sug-gest that patients treated in hospitals withtrauma centers may also have better post-discharge survival outcomes compared withthose receiving care at hospitals withouttrauma centers. These results should be inter-preted with caution, however, because refer-ral patterns varied between the different typesof hospitals. For example, elderly patientswere significantly less likely to be treatedat a designated trauma center compared toyounger patients, regardless of TBI severity.
The TBI cohort experienced not onlyexcess mortality caused by injury, but in-creased risk for death from cerebrovasculardiseases (SMR = 11.7). However, most deathsattributed to a nontraumatic hemorrhagemay have actually resulted from traumatichemorrhage (ie, the index TBI). Of the 36cerebrovascular deaths, 12 were caused bynontraumatic subdural, intracerebral, or in-tracranial hemorrhage, and all but 1 deceasedpatient had a traumatic hemorrhage docu-mented in the hospital discharge file. Mostlikely, these deaths were inaccurately codedon the death certificate, which implies that aneven greater proportion of the deaths mighthave been caused by the index TBI. Unlikeother studies, we did not find excess mor-tality risks associated with seizures, respira-tory infections, choking and suffocation, orsuicide.7,52 The length of follow-up and thedifferences in study populations may accountfor variation in the causes of excess mortalitybetween our cohort and others.
Limitations
The results of this study must be consid-ered in the context of the following limita-tions. First, we were unable to obtain multi-ple cause-of-death information on 6% of thedecedents. This potential bias should be min-imal, however, because of the small num-ber of unlinked deaths; in addition, a com-parison of the characteristics of the linkedand unlinked deaths revealed no significant

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 267
differences between the 2 groups. Second,our mortality rate of 8.4% may be conserva-tive given that 22% of the study sample couldnot be located within 15 months of hospitaldischarge. However, because only 5 additionaldeaths were discovered when the list of pa-tients who were not located was merged withthe MCDD database and because the char-acteristics of those not located were similarto those located alive, most of the patientswho were not located likely were alive at theend of the follow-up period. Third, the mor-tality information gathered for our study wasbased on data recorded on the death certifi-cate, a source that could have yielded inac-curate data. However, because mortality infor-mation was collected using death certificatesfor both the study cohort and the general pop-ulation, this data source likely had a minimaleffect on results. Fourth, we were unable tocontrol for the effect of lifestyle or behavioralcharacteristics (eg, smoking status and alco-hol use) on death after hospital discharge. Ifpersons who sustain a TBI practice more un-healthy behaviors (either before or after theinjury) than the general population, some ofthe excess mortality we found could resultfrom factors not measured. Finally, becauseour study results are limited to patients hospi-
talized with TBI, they cannot be generalizedto those treated on an outpatient basis or tothose untreated. Likewise, whether the find-ings can be generalized to other states is un-known, because the study involved data fromthe residents of only one state.
CONCLUSIONS
This study provides valuable informationabout the risk of death within 15 monthsof hospital discharge for a large, representa-tive sample of patients discharged followingTBI. After hospital discharge, most patientsare expected to convalesce and recover fromtheir injuries. However, this study found thatthe TBI continues to be life-threatening, es-pecially to those who are already more vul-nerable (ie, the elderly, those with a severeTBI, or those with associated medical con-ditions). Given the high death rate within15 months of hospital discharge, healthcareproviders should carefully monitor the healthand well-being of these patients during thepostacute care period. Improved methods ofcare must be developed and implemented tominimize the late effects of TBI and to maxi-mize the opportunity for full recovery amongall patients with TBI.
REFERENCES
1. Anderson RN, Smith BL. Deaths: leading causes for2001. Natl Vital Stat Rep. 2003;52(9):1–85.
2. Sosin DM, Sniezek JE, Waxweiler RJ. Trends in deathassociated with traumatic brain injury, 1979 through1992: success and failure. JAMA. 1995;273(22):1778–1780.
3. Sauaia A, Moore FA, Moore EE, et al. Epidemiol-ogy of trauma deaths: a reassessment. J Trauma.1995;38(2):185–193.
4. Shackford SR, Mackersie RC, Holbrook TL, et al.The epidemiology of traumatic death—a population-based analysis. Arch Surg. 1993;128:571–575.
5. Baker CC, Oppenheimer L, Stephens B, Lewis FR,Trunkey DD. Epidemiology of trauma deaths. Am JSurg. 1980;140(1):144–150.
6. Centers for Disease Control and Prevention, NationalCenter for Injury Prevention and Control. TraumaticBrain Injury in the United States: A Report to
Congress. Atlanta, Ga: US Dept of Health and Hu-man Services, Centers for Disease Control and Pre-vention, National Center for Injury Prevention andControl; 1999.
7. Shavelle RM, Strauss D, Whyte J, Day SM, Yu YL. Long-term causes of death after traumatic brain injury. AmJ Phys Med Rehabil. 2001;80:510–516.
8. Baguley I, Slewa-Younan S, Lazarus R, Green A. Long-term mortality trends in patients with traumaticbrain injury. Brain Inj. 2000;14(6):505–512.
9. Strauss DJ, Shavelle RM, Anderson TW. Long-termsurvival of children and adolescents after traumaticbrain injury. Arch Phys Med Rehabil. 1998;79:1095–1100.
10. Rish BL, Dillon JD, Weiss GH. Mortality followingpenetrating craniocerebral injuries: an analysis of thedeaths in the Vietnam Head Injury Registry popula-tion. J Neurosurg. 1983;59:775–780.

268 JOURNAL OF HEAD TRAUMA REHABILITATION/MAY–JUNE 2005
11. Weiss GH, Caveness WF, Einsiedel-Lechtape H,McNeel ML. Life expectancy and causes of death in agroup of head-injured veterans of World War I. ArchNeurol. 1982;39:741–743.
12. Lewin W, Marshall TF, Roberts AH. Long-termoutcome after severe head injury. Br Med J.1979;2:1533–1538.
13. Walker AE, Leuchs HK, Lechtape-Gruter H, Cave-ness WF, Kretschman C. Life expectancy of head in-jured men with and without epilepsy. Arch Neurol.1971;24:95–100.
14. Fahy TJ, Irving MH, Millac P. Severe head injuries—asix-year follow-up. Lancet. 1967;2:475–479.
15. Harrison-Felix C, Whiteneck G, DeVivo M, HammondFM, Jha A. Mortality following rehabilitation in theTraumatic Brain Injury Model Systems of Care. Neu-roRehabilitation. 2004;19:45–54.
16. Thurman DJ, Sniezek JE, Johnson D, Greenspan A,Smith SM. Guidelines for Surveillance of CentralNervous System Injury. Atlanta, Ga: US Dept ofHealth and Human Services, Centers for Disease Con-trol and Prevention, National Center for Injury Pre-vention and Control; 1995.
17. Butler JA, Langlois JA. Central Nervous SystemInjury Surveillance Annual Data SubmissionStandards—2000. Atlanta, Ga: US Dept of Healthand Human Services, Centers for Disease Controland Prevention, National Center for Injury Preven-tion and Control; 2001.
18. International Classification of Diseases, 9th Revi-sion, Clinical Modification (ICD-9-CM). 4th ed. SaltLake City, Utah: Medicode; 1993.
19. MacKenzie EJ, Steinwachs DM, Shankar B. Classifyingtrauma severity based on hospital discharge diagno-sis: validation of an ICD-9-CM to AIS-85 conversiontable. Med Care. 1989;27(4):412–422.
20. MacKenzie EJ. Injury severity scales: overview anddirections for future research. Am J Emerg Med.1984;2(6):537–549.
21. Sacco WJ, MacKenzie EJ, Champion HR, Davis EG,Buckman RF. Comparison of alternative methods forassessing injury severity based on anatomic descrip-tors. J Trauma. 1999;47(3):441–446.
22. Committee on Injury Scaling. The Abbreviated In-jury Scale 1990 Revision. Des Plaines, Il: Associationfor the Advancement of Automotive Medicine; 1990.
23. Elixhauser A, Steiner C, Harris DR, Coffey RM. Co-morbidity measures for use with administrative data.Med Care. 1998;36(1):8–27.
24. World Health Organization. International StatisticalClassification of Diseases and Related Health Prob-lems, 10th Revision. Geneva, Switzerland: WorldHealth Organization; 2004.
25. Adekoya N, Thurman DJ, White DD, Webb KW.Surveillance for traumatic brain injury deaths—United States, 1989–1998. MMWR Morb MortalWkly Rep. 2002;51(SS-10):1–16.
26. Allison PD. Estimating and Comparing Survival
Curves With Proc Lifetest: Survival Analysis. Cary,NC: SAS Institute; 1995:29–40.
27. Kleinbaum DG. Evaluating the ProportionalHazards Assumption: Survival Analysis—A Self-Learning Text. New York, NY: Springer-Verlag;1996:133–152.
28. Woodward M. The Cox Proportional Hazard Model:Epidemiology. Study Design and Analysis. Boca Ra-ton, Fla: Chapman and Hall/CRC Press; 1999:534–544.
29. US Census Bureau. Unpublished estimates of theJuly 1, 2000, United States population, by age, sex,race, and Hispanic origin: 1990-based estimates.2001. Available at: http://www.census.gov/popest/estimates.php. Accessed October 19, 2004.
30. Anderson RN. Deaths: leading causes for 2000. NatlVital Stat Rep. 2002;50(16):1–85.
31. Vandenbroucke JP. A shortcut method for calculatingthe 95 percent confidence interval of the standard-ized mortality ratio. Am J Epidemiol. 1982;115:303–304.
32. Olson CJ, Brand D, Mullins RJ, Harrahill M, TrunkeyDD. Time to death of hospitalized injured patients asa measure of quality of care. J Trauma. 2003;55:45–52.
33. Mosenthal AC, Lavery RF, Addis M, et al. Isolatedtraumatic brain injury: age is an independent pre-dictor of mortality and early outcome. J Trauma.2002;52(5):907–911.
34. Grossman MD, Miller D, Scaff DW, Arcona S. When isan elder old? Effect of preexisting conditions on mor-tality in geriatric trauma. J Trauma. 2002;52(2):242–246.
35. Peek-Asa C, McArthur D, Hovda D, Kraus J. Early pre-dictors of mortality in penetrating compared withclosed brain injury. Brain Inj. 2001;15(9):801–810.
36. Kraus JF, Peek-Asa C, McArthur D. The independenteffect of gender on outcomes following traumaticbrain injury: a preliminary investigation. NeurosurgFocus. 2000;8(1):1–9.
37. Conroy C, Kraus JF. Survival after brain injury. Neu-roepidemiology. 1988;7:13–22.
38. McGwin G Jr, Melton SM, May AK, Rue LW. Long-term survival in the elderly after trauma. J Trauma.2000;49:470–476.
39. Perdue PW, Watts DD, Kaufmann CR, Trask AL. Dif-ferences in mortality between elderly and youngeradult trauma patients: geriatric status increases riskof delayed death. J Trauma. 1998;45(4):805–810.
40. Gubler KD, Davis R, Koepsell T, Soderberg R, MaierRV, Rivara FP. Long-term survival of elderly trauma pa-tients. Arch Surg. 1997;132:1010–1014.
41. Arias E, Anderson RN, Kung H, Murphy SL, KochanekKD. Deaths: final Data for 2001. Natl Vital Stat Rep.2003;52(3):1–115.
42. Sacco WJ, Copes WS, Bain LW Jr, et al. Effect of prein-jury illness on trauma patient survival outcome. JTrauma. 1993;35(4):538–543.

Risk of Posthospitalization Mortality Among Persons With Traumatic Brain Injury 269
43. Morris JA Jr, MacKenzie EJ, Edelstein SL. The ef-fect of preexisting conditions on mortality in traumapatients. JAMA. 1990;263(14):1942–1946.
44. Mullins RJ, Mann NC, Hedges JR, et al. Adequacy ofhospital discharge status as a measure of outcomeamong injured patients. JAMA. 1998;279(21):1727–1731.
45. Susman M, DiRusso SM, Sullivan T, et al. Trau-matic brain injury in the elderly: increased mortalityand worse functional outcome at discharge despitelower injury severity. J Trauma. 2002;53(2):219–224.
46. Gennarelli TA, Champion HR, Copes WS, SaccoWJ. Comparison of mortality, morbidity, and sever-ity of 59,713 head injured patients with 114,447patients with extracranial injuries. J Trauma.1994;37(6):962–968.
47. Tiret L, Hausherr E, Thicoipe M, et al. The epidemi-ology of head trauma in Aquitaine (France), 1986: a
community-based study of hospital admissions anddeaths. Int J Epidemiol. 1990;19(1):133–140.
48. Champion HR, Copes WS, Buyer D, Flanagan ME,Bain L, Sacco WJ. Major trauma in geriatric patients.Am J Public Health. 1989;79(9):1278–1282.
49. Nathens AB, Jurkovich GJ, Cummings P, RivaraFP, Maier RV. The effect of organized systems oftrauma care on motor vehicle crash mortality. JAMA.2000;283(15):1990–1994.
50. Mullins RJ, Mann NC. Population-based researchassessing the effectiveness of trauma systems. JTrauma. 1999;47(3, Suppl):S59–S66.
51. Mullins RJ, Veum-Stone J, Helfand M, et al. Out-come of hospitalized injured patients after institu-tion of a trauma system in an urban area. JAMA.1994;271(24):1919–1924.
52. Teasdale TW, Engberg AW. Suicide after traumaticbrain injury: a population study. J Neurol NeurosurgPsychiatry. 2001;71:436–440.