Embed Size (px)
Citation preview

I’ve just been diagnosed with CML.Could you answer my questions?
Sameer TulpuleRoyal Hallamshire Hospital
Sheffield


What now?
Leukemia Can be cured

Fast Facts
• Rare disease 1 to 1.5 new cases per 100,000 population per year
• Rare in young adults under 19 years
• Not inherited – cannot pass down to kids

How did I get it?
• In almost all cases there are no identifiable predisposing
causes
• Radiation is the only clearly established external factor
predisposing to development of CML
• Benzene is implicated only on an anecdotal basis

What is CML
Wang et al. Genes Chromosomes Cancer. 2001;32:97 Wang et al. Genes Chromosomes Cancer. 2001;32:97

Diagnostic Considerations in Chronic Myeloid Leukemia
Karyotyping in CML
1) Allows for the diagnosis of CML2) Requires a bone marrow aspirate for optimal metaphases
Demonstrating the presence of the t(9;22) or its gene product is absolutely essential in diagnosing a patient with CML

FISH in CML
Red → Bcr probeGreen → Abl Probe
Yellow → fusion of Bcr and Abl
Ch 9 Ch 22
Bcr- Ch 22
Abl – Ch 9
Bcr-Abl Fusion

Diagnostic Considerations in Chronic Myeloid Leukemia
Bcr-Abl
Bcr
Abl
cDNAQuantitative RT-PCR
for Bcr-Abl in CML
1) Allows for the diagnosis of CML2) Does not require a bone marrow aspirate for optimal results3) Can quantify the amount of disease

Disease Diagnosis and Monitoring in CML
Test Target Tissue Sensitivity (%)* Use
Cytogenetics Ph chromosome BM 1-10 ▪ Confirm diagnosis of CML▪ Evaluate karyotypic abnormalities other than Ph chromosome (ie, clonal evolution)
FISH Juxtaposition of bcr and abl
PB/BM 0.5-5 ▪ Confirm diagnosis of CML▪ Routine monitoring of cytogenetic response in clinically stable patients▪ Routine measurement of MRD
RT-PCR bcr-abl mRNA PB/BM 0.0001-0.001 ▪ Routine measurement of MRD▪ Determine the breakpoints of the fusion genes
*Number of leukemic cells detectable per 100 cells.
BM = bone marrow; FISH = fluorescence in situ hybridization; PB = peripheral blood;MRD = minimal residual disease; RT-PCR = reverse transcriptase polymerase chain reaction.
Wang et al. Genes Chromosomes Cancer. 2001;32:97

Normal Bcr-Abl Signaling*
• The kinase domain activates a substrate protein, eg, PI3 kinase, by phosphorylation
• This activated substrate initiates a signaling cascade culminating in cell proliferation and survival
PP P
ADP P
P
PP P
ATP
SIGNALING
Bcr-Abl
Substrate
Effector
ADP = adenosine diphosphate; ATP = adenosine triphosphate; P = phosphate.Savage and Antman. N Engl J Med. 2002;346:683Scheijen and Griffin. Oncogene. 2002;21:3314.

Imatinib Mesylate: Mechanism of Action*
• Imatinib mesylate occupies the ATP binding pocket of the Abl kinase domain
• This prevents substrate phosphorylation and signaling
• A lack of signaling inhibits proliferation and survival
P
PP P
ATP
SIGNALING
Imatinib mesylate
Bcr-Abl
Savage and Antman. N Engl J Med. 2002;346:683.

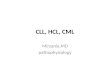
IRIS 8-Year UpdateOverall Survival (Intent-to-Treat) – Imatinib Arm
Estimated overall survival at 8 years
was 85% (93%, considering only
CML related deaths)
0
10
20
30
40
50
60
70
80
90
100
Alive,%
0 12 24 36 48 60 72 84 96 108
Months Since Randomization
Survival: deaths associated with CML
Overall Survival
% A
live

Most Common Adverse Events (by 5 Years)
All Grade AEs Patients, %
Grade 3/4 AE’s Patients %
Superficial Edema 60 2
Nausea 50 1
Muscle cramps 49 2
Musculoskeletal pain 47 5
Diarrhea 45 3
Rash/skin problems 40 3
Fatigue 39 2
Headache 37 <1
Abdominal pain 37 4
Joint pain 31 3
IRIS Study: Most Frequently Reported AEs
• Only Serious Adverse Events (SAEs) were collected after 2005
• Grade 3/4 adverse events decreased in incidence after years 1-2IRIS 8 year update
Imatinib is a Safe Drug....

How often do I need tests

Definitions of Treatment Response
Level of Response Definition
Complete hematological responseNormal CBC and differential, no extramedullary disease
Major cytogenetic response 0-35% Ph-positive metaphases*
- Partial cytogenetic response 1%-35% Ph-positive metaphases*
- Complete cytogenetic response 0% Ph-positive metaphases*
Major molecular response≥ 3-log reduction of BCR-ABL mRNA from baseline
Complete molecular remission Negativity by RT-PCR
* Cytogenetic response is based on analysis of at least 20 metaphases
Deininger, 2005; National Comprehensive Cancer Network, 2007.

Do I need repeated Bone marrows?
• Usually only at diagnosis
• No
• Part of trial
• If there is loss of response

CML – Phases of Disease
Phase Characteristics
Chronic Phase
• Indolent course, often asymptomatic and found incidentally on routine physical exam
• Predominance of mature white blood cells• Approximately 90% of patients are diagnosed at this stage• Median survival is 4–7 years (pre-tyrosine kinase inhibitor [TKI] therapy)
AcceleratedPhase
• Transition generally occurs over a period of 1 year or more. Duration is 6 months to 1 year
• Associated with progressive leukocytosis, thrombocytosis or thrombocytopenia, basophilia, increased blasts, splenomegaly, fever, bone pain
• Clonal evolution may be present
Blast Phase
• Lasts only a few months – survival is poor if untreated• Associated with increasing blasts (>20%), progressive splenomegaly despite treatment, and clonal evolution
National Comprehensive Cancer Network, 2007; National Cancer Institute, 2007; Calabretta & Perrotti, 2004; Cortes et al., 2006.

Summary
• Rare disease
• Potentially curable disease
• Good long term survival
• Imatinib has a good safety profile