Embed Size (px)
Citation preview

1
Management of CML patients treated with TKI:
the place of molecular monitoring
Antwerp, December 13th 2011
C. Graux
CHU Mont-Godinne
MolecularDiagnostic.be
Third Scientific Meeting Molecular Diagnostics.be
CML: definition
t(9;22)
CML epidemiology
• CML accounts for 14% of all leukemias
• The incidence is 1.6 per 100.000 /year
+/- 200 new cases/ year in Belgium
1 CML = 2 AML = 3 MM = 12 NHL = 37 CLL
Increases with age (median 67 y)
• Male predominance : 1.4/1
• The only known risk factor is ionizing radiations (high doses)
Exposure to atomic bomb in Nagasaki and Hiroshima induced CML
• Symptoms
- Fatigue, anorexia, weight loss
• Clinical examination
- Splenomegaly
• Biology
- Hyperleucocytosis
- Circulating bone marrow myeloid precursors (left shift)
- Increased basophilia
- Thrombocytosis
• Cytogenetics : t(9;22) = Philadelphia (Ph) chromosome
• Molecular biology: BCR-ABL1
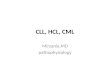
CML diagnosis
Normal Chronic phase of CML
CML: peripheral blood smear Cytogenetic abnormality of CML
1 2 3 4 5
6 7 8 10 119 12
13 14 15 16 17 18
19 20 21 22 x Y
Ph chromosome

2
Ph chromosome and BCR-ABL1 gene
BCR-ABL1
ABL1
Chimeric protein
with tyrosinekinase activity
22
BCR
Ph (or 22q-)
9 9 q+
P210 BCR-ABL1
P190 BCR-ABL1
Chromosome 9
BCR
Chromosome 22
ABL1
Exons
Introns
CML Breakpoints
ALL Breakpoint
t(9;22) translocation BCR-ABL1 gene structure
BCR-ABL1: types of transcripts
m-bcr≈ 55 kd
M-bcr≈ 2,9 kb
µ-bcr
1a
1b
a3
a2
Multiplex-PCR for BCR-ABL1 transcripts
BCR
BCR-ABL1
Constitutively activated tyrosine kinase
Bcr-Abl1 signal transduction pathways
Adapted from Pasternak G et al. J Cancer Res Clin Oncol. 1998;124:643-660
BCR-ABL1
BCL-2MYC
GRB2 CRKL CBL (p120CBL)
RAS
RAF-MEK-MAPK cascade
JAK/STATs
Paxillin
PI3 kinase
Actin
DNA repair
AKT
Regulates cell cycle progression and differentiation Inhibition of apoptosis
Adhesion
Adhesion
Clinical evolution : CML phases
Chronic phase
Variable
Accelerated phase
Median time
6–9 months
Blastic crisis
Median survival
3–6 months
Advanced phases

3
What are the therapeutic goals in CML?
Disappearance of the symptoms
Modify the natural evolution of the disease � blastic phase
Cure
Criteria for response to R/
Hematologic response
Complete
- Platelet count < 450 x 109/L
- WBC count < 10 x 109/L
- Differential: no immature granulocyte
- Basophils < 5%
- Non palpable spleen
Cytogenetic response
Complete (CCgR) = No Ph+ metaphases
Partial (PCgR) = 1-35% Ph+ metaphases
Minor = 36-65% Ph+ metaphases
Minimal = 66-95% Ph+ metaphases
None = > 95% Ph+ metaphases
Molecular response
Allogeneic SCT
Nati
on
al M
arr
ow
Do
no
r P
rog
ram
(N
MD
P)
ov
erv
iew
slid
e p
rese
nta
tio
n.
Av
ailab
le a
t h
ttp
://w
ww
.marr
ow
.org
/NM
DP
/SL
IDE
SE
T/s
ld031.h
tm#slid
e.
Acce
sse
d 1
7 J
un
e 2
002.
Survival by disease stage, June 2001, based on transplants 1987 – Feb 2001.
P P = .0001= .0001
The only known cure but is associated with high
morbidity and mortality rates in CML
Interferon α
Guilhot F et al. N Engl J Med. 1997;337:223-229.
0.0 12 24 36 48 60
Major cytogenetic responseP
rop
ort
ion
su
rviv
ing
1.0
Minor or no response
P < .001
Months after treatment with IFN-αααα
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Chemotherapy
• Oral cytotoxic agents
– Hydroxyurea
– Busulfan
• Hematological responses in up to 90% of patients
• Major cytogenetic responses are rare (1%–5%)1-4
• Palliative care: no effect on disease progression
1. The Italian Cooperative Study Group on Chronic Myeloid Leukemia. N Engl J Med. 1994;330:820-825.2. Hehlmann R et al. Blood. 1994;84:4064-4077.3. Allan NC et al. Lancet. 1995;345:1392-1397.4. Ohnishi K et al. Blood. 1995;86:906-916.
BCR-ABL1: the ideal target for
molecular therapy
• Present in the majority of patients with CML (95%)
• The cause of the disease
• Necessary for the initiation of the disease (primary event)
• ABL1 is non essential for normal cellular functions
- Abl1 neg mice are viable
� Imatinib targets BCR-ABL1

4
Mechanism of action of Imatinib
Goldman JM, Melo JV. N Engl J Med. 344 :1084-1086
IRIS Study
S
Imatinib
IFN-a + Ara-C
R Cross-over
IF:· Loss of MCyR or CHR· Increasing WBC count
· Intolerance of treatment· Failure to achieve MCyR
Progression· Death· Accelerated phase or blast crisis· Loss of MCR or CHR· Increasing WBC count
S = screeningR = randomisation
Imatinib versus IFN-α + Ara-C1106 patients enrolled from June 2000 to January 2001
Complete hematological responses
94%
55%
Imatinib
IFN-αααα + Ara-C0
10
20
30
40
50
60
70
80
90
100
Months Since Randomisation
0 3 6 9 12 15 18 21
% R
esp
on
din
g
Major cytogenetic responses
Imatinib
IFN-αααα + Ara-C0
10
20
30
40
50
60
70
80
90
100
Months Since Randomisation
0 3 6 9 12 15 18 21
% R
esp
on
din
g
83%
20%
Superiority of Imatinib to IFN-α + Ara-C
IRIS Study : Summary of the 12-Month Data
CHR = complete haematological response; MCR = major cytogenetic response; PD = progressive disease; AP = accelerated phase; BC = blast crisis.
94
55
83
20
1,58,7
0,7
23
0
20
40
60
80
100
CHR MCyR PD to AP/BC Intolerance
Imatinib
IFN- + Ara-Cαααα
Baccarani, M. et al. Blood 2006;108:1809-1820
Is CCyR the best surrogate endpoint?

5
Progression to AP/BP
IRIS study
Towards cure under TKI?
Is MMR the best surrogate endpoint?
• No proven effect on survival…
• Variability of the assay…
• Data on benefit of MMR based on good responders…
But …
– MMR = very low progression rate
– Loss of MMR signals relapse/progression
– Early MMR predicts complete molecular response � cure?
– MMR underscores the basic oncology principle that less disease is better
� Less is probably more
Molecular monitoring: difficulties
• RQ-PCR is technically challenging
• Issues concerning comparability of results between centres
� International standardisation of molecular monitoring for
CML to enable testing laboratories to accurately mesure key
therapeutic molecular milestones in CML (MMR and CMR)
International scale for BCR-ABL1
• Historically (IRIS trial; 2000), the mean BCR-ABL1 levels of 30
CML patients was defined as 100% in each of the three
participating laboratories using BCR as a control
• The value corresponding to MMR in each laboratory has been
defined as 0,1% (reduction of 3 log from IRIS baseline)
• International Scale (IS) fixed to these key points
MMR is defined as ≤ 0,1%IS = - 3 log reduction of BCR-ABL1 from IRIS standardised baseline , NOT 3 log reduction from individual pretreatment levels
The absolute and not the relative amount is important
International scale for BCR-ABL1

6
Second generation TKI
• Nilotinib vs. Imatinib in CML-CP (ENESTnd Trial, NEJM 2010, Lancet, 2011)
– More frequent and faster MMR
– Decreased progression to accelerated or blastic phase
– More frequent CMR � room for cure?
• Dasatinib vs. Imatinib in CML-CP (NEJM 2010)
– More CCyR
– More frequent and faster MMR
Effect on long term outcome?
Nilotinib vs. Imatinib in CML-CP (ENESTnd Trial)
BCR-ABL1 kinase domain mutants
• Are associated with various degrees of TKI insensitivity
• Select resistant clones = most important mechanism of
resistance
• Can precede or accompany progression to advanced-phase
disease
� KD mutations above a certain level should be identified as
early as possible to reconsider the therapeutic strategyMartinelli. The Hematology Journal, 2005
≅≅≅≅ 90 KD mutations known to date
BCR-ABL1 kinase domain mutants
0
500
1000
1500
2000
2500
3000
ma
tern
al
+ I
L3
bcr-
ab
l w
t
M2
37I
M2
44V
L2
48V
G2
50
A
G2
50E
G2
50V
Q2
52H
Y2
53H
E2
55D
E2
55K
E2
55V
E2
55R
E2
75K
E27
6G
E2
81K
K2
85N
E2
92K
F3
11V
T31
5I
F3
17C
F31
7L
F3
17V
D3
25N
S34
8L
M3
51
T
E3
55
A
E35
5G
F3
59C
F3
59V
A3
80
S
L38
7F
M38
8L
F4
68S
IC50
(n
M)
on
pro
life
rati
on
Gleevec
AMN107
Activity of Nilotinib on Imatinib-Resistant
BCR-ABL1 Mutants
72-hour proliferation assay with BCR-ABL–expressing Ba/F3 cells (ATPLite; Perkin Elmer). Trough levels at a dose of 400 mg twice daily (BID) (1.7 µM) exceed the IC50 determined in vitro for 32/33 BCR-ABL mutants (exception T315I)
Weisberg et al. Br J Cancer. 2006;94:1765.
Spectrum of Kinase Inhibition for Imatinib and Novel Compounds
Melo J, Hematology 2009

7
Time Optimal
response
Suboptimal
response
Failure Warnings
Diagnosis N/A N/A N/A High riskCCA/Ph+
3 months CHR, at least MinorCgR
No CgR Less than CHR N/A
6 months At least PCgR Less than PCgR No CgR N/A
12 months CCgR PCgR Less than PCgR Less than MMR
18 months MMR Less than MMR Less than CCgR N/A
Any time (duringtreatment)
Stable or improvingMMR
Loss of MMR Mutations (IM-sensit)
Loss of CHR, loss of CCgR, mutations (IM-insensit)CCA/Ph+
Increase in transcriptlevelsCCA/Ph-
New recommendations 2010 are marked in red.
Management of CMLRecommendations from the European LeukemiaNet Conclusion
The next step is
- to better define CMR (EUTOS project)
- to identify patients cohorts not relapsing after TKI
withdrawal