Embed Size (px)
Citation preview
CLINICAL STUDY
Is Uterine Artery Embolization for Patients withLarge Myomas Safe and Effective? A Retrospective
Comparative Study in 323 Patients
Hye Jeong Choi, MD, Gyeong Sik Jeon, MD, Man Deuk Kim, MD,Jong Tae Lee, MD, and Jung Hyun Yoon, MD
ABSTRACT
Purpose: To evaluate the effectiveness, safety, and complications of uterine artery embolization (UAE) in women with large fibroid
tumors.
Materials and Methods: From January 2005 to February 2011, 323 patients underwent UAE for symptomatic uterine leiomyomas
without adenomyosis and were included in this study. Patients were divided into two groups: those with a large tumor burden (group
1; n ¼ 63), defined as a dominant tumor with a longest axis of at least 10 cm or a uterine volume of at least 700 cm3; and the control
group (group 2; n ¼ 260). Tumor infarction and volume reduction were calculated based on magnetic resonance imaging findings.
Symptom status was assessed with a visual analog scale. Postprocedure complications and repeat interventions were recorded. The
data were analyzed with appropriate statistical tests.
Results: No significant differences were seen between the two groups in volume reduction of dominant tumors (46.5% in group 1 vs
52.0% in group 2; P ¼ .082) or percentage volume reduction of the uterus (40.7% in group 1 vs 36.3% in group 2; P ¼ .114). Also, no
significant differences were seen between the two groups regarding satisfaction scores at immediate or midterm follow-up (P ¼ .524
and P ¼ .497) or in the presence of procedure-related complications (P ¼ .193).
Conclusions: UAE outcomes in large fibroid tumors were comparable to those in smaller tumors, without an increased risk of
significant complications. Tumor size may not be a key factor in predicting successful outcomes of UAE.
ABBREVIATIONS
GnRH = gonadotropin-releasing hormone, UAE = uterine artery embolization
Uterine artery embolization (UAE) has been reported as a
safe and effective alternative to hysterectomy or myomec-
tomy for symptomatic fibroid tumors (1). UAE has
potential advantages versus surgical treatment, such as
preservation of the uterus, no complications regarding
general anesthesia or surgery, and low risk of blood loss
or transfusion (1,2). Also, the recovery time for daily
& SIR, 2013
J Vasc Interv Radiol 2013; 24:772–778
http://dx.doi.org/10.1016/j.jvir.2013.02.003
None of the authors have identified a conflict of interest.
From the Department of Radiology (H.J.C., G.S.J., J.T.L., J.H.Y.), CHA
Bundang Medical Center, CHA University, College of Medicine, 351 Yatap-
dong, Bundang-gu, Seongnam-si, Gyeonggi-do 463-712, Republic of Korea;
and Department of Radiology (M.D.K., J.H.Y.), Research Institute of Radi-
ological Science, Yonsei University College of Medicine, Seoul, Republic of
Korea. Received October 26, 2012: final revision received and accepted
February 8, 2013. Address correspondence to G.S.J.; E-mail:
activity is shorter than that associated with open hyster-
ectomy or myomectomy (3). Most patients who have
undergone UAE are highly satisfied (1), and multiple
factors are known to be associated with successful
outcomes of UAE.
There have been studies published reporting that treat-
ment failure is more likely to occur in patients with large
fibroid tumors (4,5). In addition, several reports have
described rare but serious complications shortly after
UAE for large tumors, such as uterine injury, sepsis, and
death (6,7). In a large, prospective study of the FIBROID
Registry reported by Goodwin et al (5), larger leiomyoma
size was associated with poorer outcome. That study (5)
was a prospective study that included a large number of
patients, but it evaluated only the change in clinical
symptoms before and after UAE, lacking side-by-side
comparison of tumor size with an objective imaging tool
such as magnetic resonance (MR) imaging. Recent studies
suggest that outcomes of UAE in patients with large

Volume 24 ’ Number 6 ’ June ’ 2013 773
leiomyomas are as good as in other patients, with com-
parable low risk of severe complications (8–11). However,
these studies with tumor size comparisons were performed
in small cohorts. Therefore, the purpose of the present
study was to evaluate the effectiveness, safety, and
complications of UAE when applied to fibroid tumors of
large volume in a larger study population.
MATERIALS AND METHODS
This retrospective study was approved by our institutional
review board, and the need for informed consent from
patients was waived. From January 2005 to February 2011
at a single institution, 579 patients were treated with UAE
for symptomatic fibroid tumors, adenomyosis, or both.
Because the adenomyosis component could affect the
outcome of embolization (12), 179 patients who had
adenomyosis were excluded. An additional 77 patients
were excluded because of the absence of MR imaging
(n ¼ 53) or loss to follow-up (n ¼ 24), leaving 323 patients
(mean age, 37.3 y; range, 19–51 y). Patient inclusion and
subclassification within the study population are summar-
ized in Figure 1. Group 1 included patients with a
dominant tumor with a longest axis of at least 10 cm or
a uterine volume of at least 700 cm3 (11,13). Group 2
included the remaining patients who did not fulfill the size
criteria of the large tumor burden group. Of the 323
patients, 63 (19.5%) were in group 1 and the remaining
260 (80.5%) were in group 2. Mean ages were not
significantly different between groups (group 1, 37.1
y � 5.6; group 2, 37.3 y � 5.6; P = .777; Table 1).
Figure 1. Patient enrollment flowchart. UFE ¼ uterine fibroidembolization.
Patients’ clinical information was obtained by retrospec-
tive review of medical records. Baseline clinical symptoms
were assessed in all patients via an oral questionnaire
before the UAE procedure. Uterine leiomyomas were
diagnosed based on clinical history, gynecologic and
physical examination, and MR imaging. Detailed informa-
tion regarding tumor position and exclusion of other pelvic
malignancy was confirmed on the MR imaging study
performed before the procedure.
MR ImagingPelvic MR imaging (MAGNETOM Sonata; Siemens,
Erlangen, Germany) was performed before UAE in all
patients on a 1.5-T system with a pelvic coil. MR imaging
protocols consisted of T2-weighted sequences of axial,
coronal, and sagittal planes, and axial T1-weighted fat-
saturated sequences. Contrast-enhanced MR imaging was
performed after intravenous infusion of 0.1 mmol/kg body
weight of gadolinium-based contrast agent (MultiHance;
Bracco, Milan, Italy) at a rate of 2 mL/s. Postcontrast fat-
saturated T1-weighted sequences of axial, coronal, and
sagittal planes were also obtained. The baseline MR
imaging features are summarized in Table 2. The most
common number of tumors per patient in group 1 (31 of
63; 49.2%) was one, compared with more than five in
group 2 (108 of 260; 41.5%).
All patients underwent follow-up MR imaging, and 284
patients had follow-up imaging within 3 months after the
UAE procedure. The remaining 39 patients had an interval
of 4–11 months from UAE until MR imaging. Additional
follow-up MR imaging was performed on an individual
basis.
Embolization ProceduresUAE was performed after selective catheterization of both
uterine arteries via unilateral approach. The primary
embolic agent was polyvinyl alcohol (PVA) particles
(Contour [Boston Scientific, Cork, Ireland] or PVA Foam
Embolization Particles [Cook, Bloomington, Indiana])
mixed with 60 mL of 1:1 saline solution/contrast agent
mixture. PVA particle size (ranging from 250 to 710 mm)
was decided according to the operator’s preference. Bilat-
eral UAE was performed in 317 patients, and unilateral
UAE was performed in six cases as a result of aplasia of
the contralateral uterine artery. In three of those cases,
contralateral ovarian arteries supplying the uterus were
embolized. Coil embolization (Tornado; Cook) was per-
formed in nine patients to avoid unintended embolization
of other branches such as rectal, ovarian, or cervical
branches, which originate from the uterine arteries. Embo-
lization was performed until there was sluggish blood flow
in the ascending portion of the uterine artery, usually
during 10 heart beats.
Technical success after the embolization procedure was
defined as occlusion or marked reduction of blood flow
in both uterine arteries. Successful embolization of only

Table 1 . Summary of Baseline Characteristics, Age, Previous Treatment, and Presenting Symptoms of the 323 Patients
Characteristic Large Tumor Group (n ¼ 63) Control Group (n ¼ 260) P Value
Mean age (y) � SD 37.1 � 5.6 37.3 � 5.6 .777
Previous treatment
Hormone therapy 10 (15.9) 5 (1.9) o .001
MR-guided focused US surgery 3 (4.8) 3 (1.2) .091
Myomectomy 2 (3.2) 15 (5.8) .542
More than two of the above 1 (1.6) 3 (1.2) .582
Presenting symptoms
Heavy bleeding* 59 (93.7) 247 (95.0) .752
Dysmenorrhea 51 (81.0) 174 (66.9) .033
Mass-related symptoms† 45 (71.4) 170 (65.4) .457
Values in parentheses are percentages.*Heavy bleeding; menorrhagia, dysfunctional uterine bleeding.†Mass-related symptoms; mass palpation, urinary frequency or urgency, constipation, back pain, pelvic heaviness, or prolapse-likesensation.
Table 2 . Baseline MR Imaging Findings
Characteristic Large Tumor Group (n ¼ 63) Control Group (n ¼ 260) P Value
Myomas per patient
1 31 (49.2%) 103 (39.6%) .002
2–5 4 (6.3%) 48 (18.5%) .021
4 5 26 (41.3%) 108 (41.5%) 4 .050
Extensive 2 (3.2%) 1 (0.4%) .098
Tumor burden
Dominant tumor diameter (cm) 10.7 � 2.5 6.2 � 1.7 o .001
Dominant tumor volume (cm3) 443.0 � 319.6 117.1 � 89.4 o .001
Uterine volume (cm3) 855.8 � 277.1 313.5 � 142.8 o .001
Values presented as means � SD where applicable. Values in parentheses are percentages.
Choi et al ’ JVIR774 ’ Safety and Effectiveness of UAE in Patients with Large Myomas
one artery was considered as a technical failure because
the aim of the procedure was to reduce blood flow
bilaterally.
ComplicationsComplications related to the procedures were classified
according to the guidelines established by the Society of
Interventional Radiology Standards of Practice Committee
(14). Minor complications were defined as those that
resulted in no sequelae; patients required nominal therapy
or a short hospital stay for observation (generally overnight).
Major complications were defined as those that resulted
in unplanned increase in the level of care, prolonged
hospitalization, permanent adverse sequelae, or death.
Clinical Follow-upClinical follow-up was completed at 1 and 3 months after
UAE, and patients were interviewed during these visits.
The enrolled patients were instructed to express their
symptomatic severity according to a 10-point visual analog
scale (with a score of 10 indicating the worst initial
symptoms and 0 indicating no symptoms). Midterm clinical
follow-up was defined as follow-up visits more than 12
months after UAE. Midterm follow-up was achieved via an
oral questionnaire at the time of the hospital visit or a phone
call that included questions about pregnancy, duration of
amenorrhea, newly developed or sustained symptoms,
additional treatment, and symptom score.
Data and Statistical AnalysisThe total volumes of the uterus and predominant tumors
were calculated based on the formula for a prolate ellipse
(length � width � height � 0.5233) before and after treat-
ment (15). Dominant tumor and overall tumor infarction
rate after UAE were decided based on the consensus of two
radiologists after individually estimating percentage
decrease of the enhancing portion of tumor between
baseline and follow-up MR images (16). Infarction of
more than 80% was considered sufficient (11).
An independent t test was used in the comparison of
continuous variables between group 1 and group 2. An w2
test or Fisher exact test was used in the comparison of
categoric variables between the two groups. Linear regres-
sion analysis was performed to determine the correlation of
symptom change on initial follow-up, dominant tumor size,
dominant tumor volume change, and initial uterus volume
with volume change. Statistical analyses were performed
with SPSS software (version 20; IBM, Armonk, New York).

Volume 24 ’ Number 6 ’ June ’ 2013 775
A probability value of less than 5% (ie, P o .05) was
considered significant.
RESULTS
Procedures and Outcomes of UAEA significantly greater number of vials of embolic agent
were used per procedure in group 1 (P o .001), and UAE
procedures required a significantly longer period of time in
group 1 (P ¼ .038; Table 3). Collateral supply of
leiomyomas was noted in 20 patients: five of the 63
patients in group 1 (7.9%) and 15 of the 260 patients in
group 2 (5.8%). Except in one case of supply from the
inferior mesenteric artery, all collateral vessels were
embolized.
Table 3 also summarizes outcomes of UAE in the
present study. Infarction rates of the dominant and overall
tumors on the initial follow-up MR images were 99.5% and
98.7%, respectively, in group 1 and 98.7% and 98.6%,
respectively, in group 2. An overall tumor infarction rate of
nearly 100% was seen on MR images in 57 patients
(90.5%) in group 1 and 234 patients (90.0%) in group
2 (P 4 .050). An overall tumor infarction rate of more
than 80% was achieved in 96.9% of patients (n ¼ 313),
and there was no significant difference between the two
groups: 95.2% (60 of 63) in group 1 and 97.3% (253 of
260) in group 2 (P ¼ .416).
There was no significant difference in the average
percentage volume reduction of dominant tumor between
the two groups: 46.5% in group 1 and 52.0% in group 2
(P ¼ .082). Also, volume reduction of the uterus did not
Table 3 . Procedures and Outcomes of Uterine Artery Embolization
Characteristics Large Tumor Gr
Technical success (n) 62 (98
Procedure time (min)* 49.0 � 1
Hospital stay (h) 62.21 �
No. of vials of embolic agent 3.6 � 1
Collateral supply 5 (7.9
Infarction rate (%)†
Dominant tumor
Mean 99.5
Range 83.0–1
Overall tumor
Mean 98.7
Range 71.9–1
Volume reduction of dominant tumor (%) 46.5 � 2
Volume reduction of uterus (%) 40.7 � 1
Short-term symptom score (initial; 10-‡) 3.1 � 2
Short-term duration (mo) 3.0 � 0
Midterm symptom score (initial; 10-‡) 1.9 � 2
Midterm duration (mo) 34.1 � 1
Values presented as means � SD where applicable. Values in pare*Procedure time is defined as the interval from injection of local a†Infarction rates were evaluated on initial follow-up MR imaging a‡Scores listed the difference from an initial score of 10.
show a significant difference between groups: 40.7% in
group 1 and 36.3% in group 2 (P ¼ .114; Fig 2).
Symptom score data obtained at 3-month follow-up visits
were available in 73.0% of patients in group 1 (46 of 63)
and 81.5% of patients in group 2 (212 of 260). There was no
statistical difference in the mean symptom score between
groups: 3.1 in group 1 and 3.6 in group 2 (P ¼ .137).
Follow-up duration of more than 12 months after UAE was
available in 243 patients, among whom 233 responded to
the questionnaires. Midterm satisfaction scores were 1.9 at
34.1 months follow-up in group 1 and 2.3 at 32.3 months
follow-up in group 2, where were not significantly different
(P ¼ .258; Table 3).
ComplicationsComplications associated with UAE procedures are sum-
marized in Table 4. Procedure-related complications
developed in 26 patients (8.0%). There were only two
cases of major complications. In one patient in group 1, the
tumor showed endocavitary transformation after the pro-
cedure, leading to subsequent myomectomy 3 months after
UAE. One patient in group 2 experienced unstable angina
immediately after UAE. There were no cases of permanent
amenorrhea in either group.
Elective hysterectomy after UAE was performed in 0.9%
of patients (n ¼ 2; one in each group; P ¼ .353) during the
mean follow-up period of 25.3 months. None of the patients
underwent emergency hysterectomy. Elective myomec-
tomy was performed in 12 cases in total (3.7%): five in
group 1 (7.9%) and seven in group 2 (2.7%; P ¼ .062). One
patient in group 1 underwent hysterectomy at 50 months
oup (n ¼ 63) Control Group (n ¼ 260) P Value
.4) 260 (100) .195
3.3 44.9 � 12.7 .038
36.9 57.17 � 25.7 .204
.4 2.2 � 0.7 o .001
) 15 (5.8) .560
.518
98.7
00 13.8–100
.918
98.6
00 29.0–100
1.6 52.0 � 25.6 .082
7.6 36.3 � 20.3 .114
.0 3.6 � 2.0 .137
.9 2.9 � 0.8 .524
.1 2.3 � 2.3 .258
6.4 32.3 � 15.4 .497
ntheses are percentages.nesthetic agent to removal of the sheath.fter procedures.

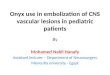
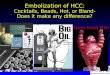
Figure 2. Images from a 38-year-old woman in the large tumor burden group (group 1) with several fibroid tumor–related symptomssuch as menorrhagia, dysmenorrhea, dysfunctional uterine bleeding, palpable mass, urinary frequency, and pelvic heaviness, whowas referred by a gynecologist for UAE. (a) Enhanced T1-weighted sagittal MR image obtained before embolization shows multipleenhancing uterine leiomyomas nearly completely replacing the uterus. The volume of the uterus was measured as 1,560 cm3 on theinitial study. (b) Enhanced T1-weighed sagittal MR image obtained 3 months after UAE shows total necrosis of all uterine tumors; thevolume of the uterus was measured as 1,054 cm3, which represents an approximate 32% volume decrease achieved by UAE.
Table 4 . Complications Associated with Uterine Artery Embolization Procedures
Complication Large Tumor Group (n ¼ 63) Control Group (n ¼ 260) P Value
Total 8 (12.7) 18 (6.9) .193
Major 1 (1.6) 1 (0.4) .353
Minor 7 (11.1) 17 (6.5) .280
Vaginal expulsion of myoma 3 (4.8) 4 (1.5) .137
Fever 4 (6.3) 0 .001
Vaginal discharge 0 4 (1.5) 4.050
Pain 0 5 (1.9) .587
Idiosyncratic reactions* 0 4 (1.5) 4.050
Values in parentheses are percentages.*Idiosyncratic reactions include whole body urticaria, edema, or skin rash.
Choi et al ’ JVIR776 ’ Safety and Effectiveness of UAE in Patients with Large Myomas
after UAE because of a palpable mass and increasing viable
portion within the myoma on follow-up pelvic computed
tomography at 48 months after UAE. Another patient in
group 2 had hysterectomy performed at 6 months after
UAE as result of persistent dysmenorrhea, even though
menorrhagia had improved. In one patient in group 1,
inferior mesenteric artery collateral vessels supplying the
myoma were found during embolization, and these were
not embolized in view of concerns of severe complications
of subsequent bowel necrosis. At 17 months follow-up, this
patient had myomectomy performed as a result of a
palpable mass, abdominal pain, and a viable portion of
subserosal myoma remaining on MR images. Three months
after myomectomy, she underwent hysterectomy as a result
of abdominal pain and a pelvic hematoma. We regarded
this as a case of myomectomy after UAE because the
insufficiently infarcted myoma prompted an initial decision
to perform myomectomy, and the hematoma that formed
postoperatively was the main reason hysterectomy was
performed subsequently. Myomectomy was performed in
five patients as a result of clinical failure, such as persistent
or aggravated symptoms: two patients in group 1 and three
in group 2 at 3–4 months after UAE.
DISCUSSION
UAE is increasingly being offered to women as an
alternative to hysterectomy for symptomatic fibroid
tumors. Previous studies reported that large tumor burden
may be a risk factor for serious complications such as
infection and ischemic uterine injury requiring emergent
hysterectomy, and it is advocated that UAE not be
performed for leiomyomas larger than 10 cm in diameter
or in the setting of large uterine volume (7). A previous
prospective analysis that included 1,278 patients (5) also
indicated that increased tumor size is associated with
a poorer symptomatic score at 36 months follow-up
compared with the baseline score. However, this study
did not include detailed imaging studies such as MR

Volume 24 ’ Number 6 ’ June ’ 2013 777
imaging for the comparison of tumor size before and after
UAE. Although side-by-side comparison with the afore-
mentioned study (5) is difficult, when comparing symptom
scores between patients with a large myoma burden and the
control group in the present study at short-term and
midterm follow-up, there were no significant differences.
Several recent studies (8,10,11) that employed MR imag-
ing for outcome measurements reported somewhat differ-
ent results than the study of Goodwin et al (5). However,
although these studies support the theory that tumor size
maybe not be a key factor in determining whether to
perform UAE, they invariably included a relatively small
number of patients. The present study has a larger study
population and used MR imaging to compare tumor size
before and after UAE between two groups based on tumor
size. We found no statistical differences between the two
groups in several outcomes: average percentage volume
reductions of the dominant tumor and uterus and symptom
scores on short-term follow-up and follow-up of more than
34 months. In addition, the overall rate of procedure-
related complications in the 323 patients was very
low, without a significant difference between the two
groups. Given the rarity of significant complications,
the present study may not have been of sufficient size to
allow the detection of a difference in the rates of adverse
events.
A global leiomyoma infarction rate of greater than 80%
was noted in 96.9% of patients who underwent UAE
mainly with the use of PVA particles, with no statistical
difference between the two groups: 95.2% (60 of 63) in
group 1 and 93.7% (253 of 260) in group 2 (P ¼ .416).
Katsumori et al (8) reported devascularization rates of 72%
in the large tumor group and 90% in the control group with
the use of UAE with gelatin sponge particles; the results
were significantly different between groups (P ¼ .007).
They suggested that the possibly increased collateral
circulation in the large myoma group may have
contributed to these differences and further increased the
potential of regrowth of the tumor (8). However, in the
present study, we found no significant difference between
the two groups in sufficient infarction rate (ie, 4 80%) or
collateral supply when using PVA particles. As reported in
the literature, different embolic materials (ie, gelatin
sponge vs PVA) and cutoff values of infarction rate may
have had an effect on these differences in results (16).
Walker and Pelage (17) reported a 3% hysterectomy rate
in a review of 400 patients who underwent UAE for
symptomatic fibroid tumors during a mean clinical follow-
up of 16.7 months. Three of their patients underwent
emergency hysterectomy for infective complications dur-
ing the postoperative period. Goodwin et al (5) reported a
9.8% hysterectomy rate and a 2.8% myomectomy rate after
UAE in a multicenter study of 2,112 patients. The present
results showed similar or lower rates compared with the
previous studies: the hysterectomy rate was 0.9% and the
myomectomy rate was 3.7% during a mean follow-up
period of 25.3 months. Also, there were no significant
differences between the two groups in hysterectomy or
myomectomy rates.
As in a recent report (18) that concluded that previous
myomectomy may not affect the outcome of UAE, we did
not consider previous treatment such as myomectomy as an
exclusion criterion for UAE in the present study.
Hormone therapy was used in 10 patients in group 1
(15.9%) and five patients in group 2 (1.9%; P o .050).
Preoperative use of gonadotropin-releasing hormone
(GnRH) agonist therapy has been reported to reduce
estimated blood loss and facilitate the surgical approach
by reducing uterine size (19). Recently, Kim et al (20)
reported that pretreatment with GnRH agonists before UAE
of large leiomyomas was safe in patients with large tumors
and did not prevent the performance of UAE. In the present
study, there were 15 patients who received GnRH
treatment before UAE. Our data are insufficient to allow
a determination of whether GnRH before UAE has an
effect on the degree of tumor volume reduction or the
outcome of the embolization procedures. Further studies
will be needed to validate the effectiveness of such
combination treatments.
The present study has several limitations. First, because
this study is retrospective, there may be undetected patient
selection bias, and there may be gaps or inaccuracies in
medical record data. Second, potential confounding factors
such as previous treatment were not controlled. Third, no
definite breakdown of the choice of embolic particle size in
each patient could be obtained; most patients would begin
with UAE with the use of 250-mm PVA particles. A small
portion of patients would not have received these particles
in this size, which may have affected the results.
In conclusion, in the present study, UAE in patients with
large fibroid tumors had outcomes comparable to those in
patients with smaller tumors. Although results from other
studies indicate that larger tumor size may result in
diminished outcomes, our data suggest that these patients
may be treated safely and effectively.
REFERENCES
1. Bradley LD. Uterine fibroid embolization: a viable alternative to hyster-
ectomy. Am J Obstet Gynecol 2009; 201:127–135.
2. Pinto I, Chimeno P, Romo A, et al. Uterine fibroids: uterine artery
embolization versus abdominal hysterectomy for treatment-a prospec-
tive, randomized, and controlled clinical trial. Radiology 2003; 226:
425–431.
3. Mara M, Maskova J, Fucikova Z, Kuzel D, Belsan T, Sosna O. Midterm
clinical and first reproductive results of a randomized controlled trial
comparing uterine fibroid embolization and myomectomy. Cardiovasc
Intervent Radiol 2008; 31:73–85.
4. Al-Fozan H, Tulandi T. Factors affecting early surgical intervention after
uterine artery embolization. Obstet Gynecol Surv 2002; 57:810–815.
5. Goodwin SC, Spies JB, Worthington-Kirsch R, et al. Uterine artery
embolization for treatment of leiomyomata: long-term outcomes from
the FIBROID Registry. Obstet Gynecol 2008; 111:22–33.
6. Vashisht A, Studd J, Carey A, Burn P. Fatal septicaemia after fibroid
embolisation. Lancet 1999; 354:307–308.
7. Pelage JP, Le Dref O, Soyer P, et al. Fibroid-related menorrhagia:
treatment with superselective embolization of the uterine arteries and
midterm follow-up. Radiology 2000; 215:428–431.

Choi et al ’ JVIR778 ’ Safety and Effectiveness of UAE in Patients with Large Myomas
8. Katsumori T, Nakajima K, Mihara T. Is a large fibroid a high-risk factor for
uterine artery embolization? AJR Am J Roentgenol 2003; 181:1309–1314.
9. Parthipun AA, Taylor J, Manyonda I, Belli AM. Does size really matter?
Analysis of the effect of large fibroids and uterine volumes on compli-
cation rates of uterine artery embolisation. Cardiovasc Intervent Radiol
2010; 33:955–959.
10. Firouznia K, Ghanaati H, Sanaati M, et al. Uterine artery embolization in
101 cases of uterine fibroids: do size, location, and number of fibroids
affect therapeutic success and complications? Cardiovasc Intervent
Radiol 2008; 31:521–526.
11. Smeets AJ, Nijenhuis RJ, van Rooij WJ, et al. Uterine artery emboliza-
tion in patients with a large fibroid burden: long-term clinical and MR
follow-up. Cardiovasc Intervent Radiol 2010; 33:943–948.
12. Smith SJ, Sewall LE, Handelsman A. A clinical failure of uterine fibroid
embolization due to adenomyosis. J Vasc Interv Radiol 1999; 10:1171–1174.
13. McLucas B, Adler L, Perrella R. Uterine fibroid embolization: nonsurgical
treatment for symptomatic fibroids. J Am Coll Surg 2001; 192:95–105.
14. Drooz AT, Lewis CA, Allen TE, et al. Quality improvement guidelines for per-
cutaneous transcatheter embolization. J Vasc Interv Radiol 2003; 14:S237–242.
15. Orsini LF, Salardi S, Pilu G, Bovicelli L, Cacciari E. Pelvic organs in
premenarcheal girls: real-time ultrasonography. Radiology 1984; 153:
113–116.
16. Siskin GP, Beck A, Schuster M, Mandato K, Englander M, Herr A.
Leiomyoma infarction after uterine artery embolization: a prospective
randomized study comparing tris-acryl gelatin microspheres versus
polyvinyl alcohol microspheres. J Vasc Interv Radiol 2008; 19:
58–65.
17. Walker WJ, Pelage JP. Uterine artery embolisation for symptomatic
fibroids: clinical results in 400 women with imaging follow up. Br J
Obstet Gynaecol 2002; 109:1262–1272.
18. Huang JY, Kafy S, Dugas A, Valenti D, Tulandi T. Failure of uterine
fibroid embolization. Fertil Steril 2006; 85:30–35.
19. Broekmans FJ. GnRH agonists and uterine leiomyomas. Hum Reprod
1996; 11(suppl 3):3–25.
20. Kim MD, Lee M, Lee MS, et al. Uterine artery embolization of large
fibroids: comparative study of procedure with and without pretreatment
gonadotropin-releasing hormone agonists. AJR Am J Roentgenol 2012;
199:441–446.