Embed Size (px)
Citation preview

Christopher P. DentonProfessor of Experimental Rheumatology
Royal Free Hospital and UCL Medical School, London, UK
Is stem cell transplant a cure for scleroderma?

No ....
.... perhaps sometimes ....

Overview
Challenges in sclerodermaCurrent treatment with immunosuppressionObservational trials – UK, ESOS, deSScipher
Cyclophosphamide lung studies
Stem cell transplantProcedure
History
Evidence
PerspectivePotentially helpful in some patients
Case selection – “predicting the future”
Current strategies – UK and NHS pathway

Complications of systemic
sclerosis

Timing of the development of internal organ involvement in systemic sclerosis
Diffuse SSc Limited SSc
1995 – 2003 incident SSc cohort at RFH (n=677)
48.8%
16.9%
7.8%
14.4%
Disease duration (months)
n = 276 (40.8%)
Cum
ulat
ive
inci
denc
e (%
)
60
50
40
30
20
10
0
0 60 120 180
24.5%
22.9%
4.0%3.3%
n = 401 (59.2%)
Cum
ulat
ive
inci
denc
e (%
)
60
50
40
30
20
10
0
0 60 120 180Disease duration (months)
Nihtyanova, Denton et al Arthritis Rheumatol (on line, 2014)

SSc
Regular review
Screening for major complications: a cornerstone of global management
ECGEchocardiogramClinical examCardiac MRICardiac catheterisation
Heart involvementPulmonary function testsCXRHRCTClinical examLung biopsy(BAL)
Interstitial lung fibrosis
Clinical exam (BP)eGFRUrinalysis
Renal involvementPulmonary hypertension
ECGEchocardiogramPulmonary function testsClinical examRight heart cath.

dcSSc lcSSc
0 12 24 36 48 6050
60
70
80
90
10093%
91%P=0.534
Disease duration (months)
Surv
ival
(%)
Disease onset
1990 -1993 n=234
2000 -2003 n=286
0 12 24 36 48 60
50
60
70
80
90
100
84%
69%P=0.018
Nihtyanova et al, QJM 2010; 103:109-15
Improving survival in systemic sclerosis: a historical perspective

NSIP
Treatment of skin and lung fibrosis in scleroderma

Potential immunomodulatory strategies Methotrexate
CyclophosphamideAzathioprineMycophenolate mofetilStem cell transplant (autologous/allogeneic)Tacrolimus, rapamycinBiological agents (rituximab, abatacept,
basiliximab)Oral tolerance to type I collagenHyperimmune caprine serum (AIMSPRO®)
Early stage diffuse systemic sclerosis

0
10
20
30
40
50
0
10
20
30
40
50
BaselineYear1 Year2 Year3 BaselineYear1 Year2 Year3 BaselineYear1 Year2 Year3
BaselineYear1 Year2 Year3 BaselineYear1 Year2 Year3
Cyclo then MMF ATG then MMF MMF
No active therapy Other (MTX etc)mR
SS
Skin score over time, by treatment protocol
Skin score change in UK observational study of dcSSc
Herrick et al, J Rheum (2010); 37: 116-24.
Herrick et al, J Rheum (2010); 37: 116-24.
147 patients from 12 centres
– No difference between protocols– Intention to treat analysis– Deterioration usually led to intensified therapy
ESOS – EULAR-ODP funded– MTX, cyclophosphamide, MMF ~300 subjects

1Hoyles et al Arthritis Rheum 2006; 54:3962-70
Cyclophosphamide for lung fibrosis in SSc• Fibrosing alveolitis in scleroderma trial (FAST)1
monthly intravenous cyclophosphamide 600mg/m2 for 6 months followed by (po) azathioprine, or placebo in 45 patients
– Over 12 months improvement/stabilisation FVC in favour of active treatment (p=0.04, BMI corrected – uncorrected p=0.08)
– Magnitude of difference 5.5% (4.8% adjusted) – active arm improved (+2.5 % predicted) – placebo arm worsened (-3.0 % predicted)
FAST primary outcome: FVC
p=0.08
2.44
2.46
2.48
2.50
2.52
2.54
2.56
2.58
2.60
2.62
2.64
baseline 3 months 6 months 9 months 12months
Months since baseline
Abs
olut
e FV
C (m
ean
at e
ach
time
poin
t)
ACTIVE PLACEBO

Oral cyclophosphamide in SSc-PF: the Scleroderma Lung Study (SLS-I)
24 month follow-up data suggest maximum treatment effect on FVC at 18 months then benefit diminishes but improved dyspnoea score remains
cyclophosphamide
1Tashkin et al NEJM 20062Tashkin et al Am J Respir Crit Care Med 2007
• Scleroderma lung study1 (SLS) oral cyclophosphamide (1-2 mg/kg/d) or placebo over 12 months in 158 patients.
• 1° endpoint FVC (change in % predicted) adjusted for baseline severity
2.5% placebo-subtracted difference in favour of cyclophosphamide (p<0.03)
• 2° endpoint %TLC, dyspnoea score, HAQDI, Skin score all p<0.05 in favour of cyclophosphamide

Haemopoetic stem cell transplanation (HSCT) for diffuse cutaneous SSc
• Intensive immunosuppression may lead to long term improvement in outcome for dcSSc
• HSCT allows high dose cyclophosphamide with rapid recovery from myelosuppression
• Prospective controlled trials underway: ASTIS in Europe and SCOT trial in USA. ASSIST results published.
– Compare immunosuppression plus ASCT with monthly cyclophosphamide with time-to-event analysis
– Compatible protocols. SCOT uses TBI (with shielding of lungs and kidneys)

What is an autologous stem cell transplant?
Mobilisation4-6g cyclophosphamide
Conditioning8-16g cyclophosphamide

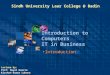
Change in skin score.
Binks M et al. Ann Rheum Dis 2001;60:577-584
©2001 by BMJ Publishing Group Ltd and European League Against Rheumatism

High-dose immunosuppressive therapy for severe systemic sclerosis: initial outcomes.
McSweeney PA, Nash RA, Sullivan KM, Storek J, Crofford LJ, Dansey R, Mayes MD, McDonagh KT, Nelson JL, Gooley TA, Holmberg LA, Chen CS, Wener MH, Ryan K, Sunderhaus J, Russell K, Rambharose J, Storb R, Furst DE. Blood. 2002;100:1602-10.
Skin score
DLco
HAQ-DISevere dcSSc (n=19)
Phase I/II study

Treatment related mortality in major ASCT studies
First author Number of transplants
TRM (%) Study designComments citation
Binks 41 17 Open observational
TRM 10.5% with ASTIS eligible cases
ARD 2001
Farge 57 9 Open observational
Included some cases in Binks et al
ARD 2004
Nash 34 23 Open observational
3 TRM beyond 100 days
Blood 2007
Burt 19 0 Prospective randomised
Highly selected cases
Lancet 2011
van Laar 79 10 Prospective randomised
Full dataset awaited
A&R [abstr] 2012
Burt 90 6 Open observational
Intensive cardiac screening
Lancet 2013

Figure 3 1-year follow-up for patients receiving haemopoetic stem-cell transplantations, monthly cyclophosphamide, or transplantation after failure of cyclophosphamide HSCT=haemopoietic stem-cell transplantation. FVC=forced vital capacity. DLCO=diffusing ...
Richard K Burt , Sanjiv J Shah , Karin Dill , Thomas Grant , Mihai Gheorghiade , James Schroeder , Robert Craig ,...
Autologous non-myeloablative haemopoietic stem-cell transplantation compared with pulse cyclophosphamide once per month for systemic sclerosis (ASSIST): an open-label, randomised phase 2 trial
The Lancet, Volume 378, Issue 9790, 2011, 498 - 506
http://dx.doi.org/10.1016/S0140-6736(11)60982-3

ASTIS outcome dataReported at EULAR and ACR meeting 2012
156 subjects – HSCT [n=79] or iv cyclophosphamide (x12) [n=77]
18 events (death or organ failure) HSCT and 24 in control arm
EFS was significantly better in HSCT group at 84 months (p=0.002)
10% treatment related mortality (TRM, n=8) in HSCT group, no TRM in control arm
Favourable outcomes in mRSS, SHAQ and VC
Worsening of renal function
Van Laar J, Farge D, Tyndall A et al ACR presentation (2012), manuscript submitted.
Clinical variable Transplant (n=67) Control (n=64) P value
↓mRSS 19.7 (10.2) 8.7 (12.1) 0.001
SHAQ ↓ 0.57 (1.14) 0.2 (0.78) 0.03 VC (% predicted) ↑ 4.5 (13.4) 2.2 (13.7) 0.005
↓GFR (ml/min) 11.9 (28.6)* 0.95 (22.9) 0.02 *2 cases of irreversible renal failure excluded

Case selection for ASCT is critical to outcome
Nihtyanova et al, ACR oral presentation 2012
Time to death
Sur
viva
l
95%89%
72%
91%
75%
57%
94%85%
69%
Patients who fulfilled inclusion criteria
Patients who fulfilled inclusion and exclusion criteria
Patients excluded due to severe organ disease
86 80 68 51 Numbers at risk65 61 54 41 Numbers at risk21 19 14 10
398 incident SSc cases with disease onset between 1995 and 1999
• 86 fulfilled ASTIS inclusion
• 21 excluded due to severe organ disease
• 65 fulfilled eligibility criteria
Exclusion criteriaSevere heart, lung or kidney diseaseMalignancy
Inclusion criteriaDiffuse scleroderma with either:
Up to 4 years with skin score at least 15/51 and evidence of significant or worsening heart, lung, kidney disease (PH excluded by Echo)
Up to 2 years with severe skin (at least 20/51) and blood tests suggesting poor outcome (ESR, Hb)

Current statusASTIS trial – soon to be fully publishedOn going treatment programmes
Agreement from UKSSG and EBMT that this should be availableNHS policy being developedPoor prognosis cases
No major heart, lung or renal disease
Failed to respond to 6 months of cyclophosiphamide therapy
2 or 3 centres in UK – London, Sheffield,...
Links to Pulmonary hypertension centres
Strong support at Royal Free and UCL

Overall survival
Time to death
Sur
viva
l
94%85%
69%
ASTIS eligible cases with standard treatment 5 and 10 year survival
in the whole dcSSc cohort
5yr 10yr
86% 72%
86 80 68 51 Numbers at risk65 61 54 41 Numbers at risk21 19 14 10
Nihtyanova et al, ACR oral presentation 2012
ASTISASCT n=67, 16 (18 events) deaths at 33 months = 24% (27%)Control n=64, 24 deaths at 27 months = 37%

Event free survival• Time to death or development of irreversible end stage organ failure
Time to death
Surv
ival
65 61 52 40 Numbers at risk
95%87%
72%66%
Nihtyanova et al, ACR oral presentation 2012
ASTISASCT n=67, 16 (18 events) deaths at 33 months = 24% (27%)Control n=64, 24 deaths at 27 months = 37%

The challenge of severe diffuse systemic sclerosis
2013 RFH clinical database
Died after 5 years SSc – cardiac disease, lung fibrosisTreatment: cyclophosphamideMMFRituximabImmunoglobulinICD
Died after 5 years SSc –renal crisis/gut failure/cardiac diseaseTreatment: MTXcyclophosphamideMMFImmunoglobulinTPNHaemodialysis
16 year follow upAlive – paid employment minimal hospital inputTreatment: MMFCyclophosphamideAutologous stem cell transplant
6 year follow upAlive – workingRenal crisis – no dialysisTreatment: MMF
15 year follow upAlive – severe pain not workingTreated: MMF

Predicting poor outcome in early dcSScEarly diffuse SSc
< 2 years from the first symptom
randomly divided into derivation (n=260) and validation (n=187) cohorts
2 year mortality
Four independent predictors (assigned integer values) comprised the model:
age at first visit (-1, 0, 1),
skin thickness progression rate (0, 1),
gastrointestinal tract severity (0, 1, 2)
anaemia (0, 2).
Derivation and external validation of a prognostic modelComparison of risk class specific 2 year mortality in derivation and validation cohortsRisk class (sum of points)
Pittsburgh derivation cohort (n=252)
Pittsburgh validation cohort(n=126)
p-value Royal Free external validation cohort (n=110)
p-value
Low (≤1)Moderate (1-2)High (≥3)
N6310881
Deceased (%)1.614.849.4
N285048
Deceased (%)0.016.016.6
0.500.850.0002
N336116
Deceased (%)3.08.212.5
0.640.210.006
Domsic R , Nihtyanova S, et al Arthritis Rheumatol. 2014 [Epub ahead of print]

PF incidence in different risk groups in derivation and validation cohorts
Risk score1995-1999 cohort
(n=398)2000-2003 cohort
(n=279)
N PF (%) N PF (%)
<0 96 1 47 20 43 10 39 131 71 20 62 132 58 33 45 313 43 45 35 524 36 61 27 685+ 52 72 24 82
Long term prediction of the development of clinically significant lung fibrosis in SSc
42% of dcSSc and 22% of lcSSc developed csPF (p<0.001).
The variables that predicted csPF development within 10 years
dcSSc, greater age at onset, lower FVC and DLCO, anti-topoisomerase I antibody (ATA)
anti-centromere antibody was protective.
Nihtyanova, Denton et al Arthritis Rheumatol (in press, 2014)

Targeting pathogenic processes in SSc: emerging concepts
Denton, C. P. & Ong, V. H. (2013) Targeted therapies for systemic sclerosisNat. Rev. Rheumatol. doi:10.1038/nrrheum.2013.46

Agent Population Primary endpoint Intervention in active arm Design Phase and status
Sildenafil SSc with ischaemic DUs
Time to healing of ischaemic DUs
20 mg three times per day Double-blind RCT Phase III, recruiting
Autologous SCT;
dcSSc Event-free survival at 48 and 54 months
Autologous SCT and high-dose immunosuppression
RCT Phase II, ongoing
Allogeneic SCT dcSSc Event-free survival at 2 years
Allogeneic SCT and high-dose immunosuppression
Open label Phase I/II, ongoing
Ambrisentan dcSSc mRSS at 12 months 5–10 mg daily Open label Phase II
NAC dcSSc mRSS NAC vs Iloprost RCT Phase II/III, recruiting
Pomalidomide dcSSc and progressive lung fibrosis
Change in mRSS and FVC at week 52
1 mg daily over 52 weeks Double-blind RCT Phase II, recruiting
Rilanocept (IL-1 inhibitor) dcSSc 4 gene biomarker of skin disease and mRSS
320 mg day 0 and 160 mg weekly for 5 weeks, subcutaenously
Double-blind RCT Phase I/II, recruiting
Tadalafil (PDE5 inhibitor) SSc and lung fibrosis
Change in FVC over 6 months
20 mg alternate days over 5 months
Double-blind RCT Phase III, recruiting
Fresolimumab (GC1008)
dcSSc TGFb-regulated gene expression in skin
1 and 5mg/kg intravenously Open label Phase I, recruiting
Rituximab SSc–PAH Change in PVR over 24 weeks
2 infusions, 1000 mg. each, 14 days apart
Double-blind RCT Phase II, recruiting
Macitentan SSc and DUs Reduction of new DUs at 16 weeks
3 mg or 10 mg daily Double-blind RCT Phase III, recruiting
MMF; cyclophosphamide SSc and lung fibrosis.
FVC over 24 months MMF for 2 years or oral cyclophosphamide for 12 months
RCT Phase II, recruiting
Tocilizumab dcSSc mRSS at 6 months 162 mg once per week. subcutaneously
Double-blind RCT Phase II, recruiting
Rituximab dcSSc Death or major organ involvement at 28 weeks
1,000 mg on days 1 and 15 and at week 26
RCT Phase II, ongoing
Current registered clinical trials in systemic sclerosis
Denton, C. P. & Ong, V. H. (2013) Targeted therapies for systemic sclerosisNat. Rev. Rheumatol. doi:10.1038/nrrheum.2013.46

Conclusions• Systemic sclerosis (SSc) outcome is improving
– Systematic investigation is important– Immunosuppression is helpful – Some patients do well with current treatment– Non-lethal complications should be a priority
• Stem cell transplant is feasible but not a cure– Long term outcome may be better than standard treatment in some cases– 1 in 10 patients may die directly from the treatment
• Choosing suitable patients is critical – as in all transplant programmes
• Less toxic and more targeted treatments for SSc are being sought.

Many thanks to ….• Our patients• The “Scleroderma team” at Royal Free• Research Funders• Colleagues in many institutions and organisations• UKSSG colleagues – especially Jaap van Laar• International collaborators – EUSTAR and
FESCA
Arthritis Research Campaign (UK), Raynaud’s and Scleroderma Association (UK), Wellcome Trust (UK), Nuffield Foundation (UK), Scleroderma Society (UK), Rosetrees Trust, Scleroderma Research Foundation (USA), MRC, EULAR, Royal Free Charity