Embed Size (px)
Citation preview

Y
Ib
CQ1
a
b
c
d
M
a
ARRA
KRGBB
CR
I
c[trp
UtTQ2
g(
h1
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
ARTICLE IN PRESSG ModelPHRS 2697 1–6
Pharmacological Research xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Pharmacological Research
j ourna l h om epage: w ww.elsev ier .com/ locate /yphrs
s generic rifaximin still a poorly absorbed antibiotic? A comparison ofranded and generic formulations in healthy volunteers
orrado Blandizzia, Giuseppe Claudio Viscomib, Antonio Marzoc, Carmelo Scarpignatod,∗
Division of Pharmacology, Department of Clinical & Experimental Medicine, University of Pisa, Via Roma 55, 56126 Pisa, ItalyResearch and Development Division, Alfa Wassermann Pharmaceuticals, Via Ragazzi del’ 99 5, 40133 Bologna, ItalyInstitute for Pharmacokinetic and Analytical Studies SA, Via Mastri 36, 6853 Ligornetto, SwitzerlandClinical Pharmacology and Digestive Pathophysiology Unit, Department of Clinical and Experimental Medicine, University of Parma, Cattani Pavillon,aggiore University Hospital, Viale Gramsci 14, 43125 Parma, Italy
r t i c l e i n f o
rticle history:eceived 27 March 2014eceived in revised form 2 May 2014ccepted 5 May 2014
eywords:ifaximineneric formulationranded formulationioequivalence
hemical compounds studied in this article:ifaximin (PubChem CID: 6436173)
a b s t r a c t
Rifaximin is an antibiotic, locally acting in the gastrointestinal tract, which may exist in different crystal aswell as amorphous forms. The branded rifaximin formulation contains the polymorph rifaximin-�, whosesystemic bioavailability is very limited. This study was performed to compare the pharmacokinetics of thisformulation with that of a generic product, whose composition in terms of solid state forms of the activepharmaceutical ingredient was found to be different. Two tablets (2 × 200 mg) of branded and genericformulations were given to 24 healthy volunteers of either sex, according to a single-blind, randomized,two-treatment, single-dose, two-period, cross-over design. Plasma and urinary samples were collectedat preset times (for 24 h or 48 h, respectively) after dosing, and assayed for rifaximin concentrations byhigh-performance liquid chromatography–mass spectrometry. Rifaximin plasma and urine concentra-tion–time profiles showed relevant differences when generic and branded rifaximin were compared.Most pharmacokinetic parameters were significantly higher after administration of generic rifaximinthan after rifaximin-�. In particular, the differences for Cmax, AUC and cumulative urinary excretionbetween the generic formulation and the branded product ranged from 165% to 345%. The few adverse
events recorded were not serious and not related to study medications. The results of the present inves-tigation demonstrate different systemic bioavailability of generic and branded formulations of rifaximin.As a consequence, the therapeutic results obtained with rifaximin � should not be translated sic et sim-pliciter to the generic formulations of rifaximin, which do not claim containing only rifaximin � and willdisplay significantly higher systemic absorption in both health and disease.© 2014 Published by Elsevier Ltd.
32
33
34
35
36
37
ntroduction
Generic medicinal products are ‘copies’ of patented drugs andan be marketed following patent expiration of the brand product1]. Accordingly, regulatory authorities have issued guidelines dic-ating the terms and conditions under which generic drugs can be
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
ecognized as therapeutically equivalent to their branded counter-arts [2–4].
∗ Corresponding author at: Clinical Pharmacology and Digestive Pathophysiologynit, Department of Clinical and Experimental Medicine, University of Parma, Cat-
ani Pavillon, Maggiore University Hospital, Viale Gramsci, 43125 Parma, Italy.el.: +39 0521 903863; fax: +1 603 843 5621.
E-mail addresses: [email protected] (C. Blandizzi),[email protected] (G.C. Viscomi), [email protected]. Marzo), [email protected] (C. Scarpignato).
ttp://dx.doi.org/10.1016/j.phrs.2014.05.001043-6618/© 2014 Published by Elsevier Ltd.
38
39
40
41
42
43
44
Bioequivalence studies, consisting of single-dose pharmacoki-netic (PK) evaluations, are required for registration of most genericformulations of systemically acting drugs, including antibacterialcompounds, for which the therapeutic activity depends signifi-cantly on PK parameters [5,6]. For generic formulations of systemicantibiotics, differences in pharmaceutical properties might there-fore result in changes of their PK profiles, with consequentalteration of PK/PD (pharmacodynamic) relationships, leading tovariations in their clinical efficacy, as compared to the brand-namecounterparts.
On the contrary, locally acting antibiotics, such as rifaximin, aremedicinal products, which exert their effect at the site of applica-tion. In this setting, a systemic action, if any, would be considered as
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
an undesirable effect, which could give rise to adverse events [4,7].In these medicinal products, a change in formulation or dosageform may influence – through variations in local and/or systemicbioavailability – their efficacy and/or safety profiles.
45
46
47
48

ING ModelY
2 ogical
ttimeuc
crao[
cpwswtm�dapd
iocntdpts
p(hhb
kcmcnas
cft
M
H
awtC
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
ARTICLEPHRS 2697 1–6
C. Blandizzi et al. / Pharmacol
Besides formulation, the physico-chemical characteristics ofhe active ingredient are also relevant to the local and/or sys-emic bioavailability [8,9]. In this context, crystal polymorphisms extremely important [10–12]. Polymorphism is the ability of a
olecule to assemble into more than one crystal structures. Differ-nt polymorphs display different atom arrangements within thenit cell, and this can have a remarkable impact on the physico-hemical properties of the crystallized compound [11,12].
Different polymorphic forms of a drug can display differenthemical and physical properties, including stability and chemicaleactivity, dissolution rate and solubility, which can affect bioavail-bility, PK and, as a consequence, PD [10,13]. Several examplesf polymorphism impact on bioavailability have been reported14–18].
Rifaximin (4-deoxy-4′-methylpyrido[1′,2′-1,2]imidazo[5,4-]rifamycin SV) is a synthetic product designed to modify thearent compound, rifamycin, in order to achieve low GI absorptionhile retaining good antibacterial activity [19]. Indeed, several
tudies have shown that rifaximin is a non-systemic antibioticith a broad spectrum of antibacterial activity [20,21]. According
o the European Pharmacopeia, rifaximin shows crystal poly-orphism [22] and five distinct crystal forms, namely �, �, �,
and �, have been described [23]. In vitro studies have shownifferent dissolution and solubility rates of these polymorphs,nd in vivo investigations in dogs found significantly different PKatterns amongst the various crystal forms, with the � polymorphisplaying the highest systemic bioavailability [23].
In addition to crystal polymorphs, an amorphous form of rifax-min can be also prepared. The amorphous form of a drug consistsf disordered molecule arrangements and does not display arystalline lattice [24,25]. Because of this peculiarity, there are sig-ificant stability differences between crystalline polymorphs andhe amorphous form of a drug. In vitro dissolution tests on rifaximino suggest for the amorphous form a PK behavior similar to that ofolymorph-�, thus implying a higher systemic bioavailability thanhat of polymorph-� [23]. And indeed, preliminary animal studieshowed that this is the case [26].
A previous study [27] on healthy volunteers showed that the PKrofile of amorphous rifaximin differs from that of polymorph-�the crystal form present in the branded formulation), resulting inigher systemic bioavailability. These findings confirm that also inumans different solid-state forms of rifaximin show a different PKehavior.
Since some generic formulations of rifaximin have been mar-eted, we felt it worthwhile to evaluate their PK profile inomparison to that of the branded product. Indeed, while the sum-ary of product characteristics of the branded rifaximin provides
lear information about its specific crystal structure [28], this wasot the case for the generic products, whose composition and – as
consequence – systemic absorption is unknown. Provided be itignificant, clinical consequences could arise.
The aim of this study was therefore to evaluate the impact of theomposition (in terms of crystalline polymorphs and/or amorphousrom) of the active ingredient present in the generic formulation onhe systemic bioavailability of rifaximin.
ethods
ealthy volunteers
Healthy adult volunteers of either sex (age range: 18–60 years)
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
nd Caucasian origin were invited to participate to the study. Theyere informed of the purpose, methods and potential hazards of
he study, and were requested to sign a written informed consent.linical evaluations, performed to assess the health condition of
PRESS Research xxx (2014) xxx–xxx
volunteers, as well as inclusion and exclusion criteria have beenpreviously described in details [29].
Design of the study
The study was performed in a single center (Institutefor Pharmacokinetic and Analytical Studies S.A., Ligornetto, TI,Switzerland), in accordance with a single-blind, randomized, two-treatment, single-dose, two-period, cross-over design, with awash-out period of 7 days [30]. The study was approved by theEthics Committee of Canton Ticino and Swissmedic (Switzerland),and was conducted in accordance with ICH guidelines for GoodClinical Practice. The study procedures were performed in compli-ance with the Declaration of Helsinki.
Subjects were randomized to receive a 400-mg single-dose(2 × 200-mg tablets) of the generic rifaximin or branded for-mulation (rifaximin polymorph-�; Normix®). The tablets wereadministered with 250 ml of water at 08:00 AM, under fasting con-ditions. About 4, 8 and 12 h after drug intake, a lunch (1200 kcal),a snack (150 kcal) and a dinner (900 kcal) were served. After drugintake, subjects were requested to drink water as follows: 500 mlevery hour of plain mineral water during each of the 4-h intervalsfrom drug administration till 12 h after dosing; then, at will, untilthe end of urine collection (i.e. 48 h post-dosing).
Venous blood samples of 10 ml were collected into tubes (con-taining sodium heparin) kept on ice, at pre-set time intervals of0 (pre-dosing) and 0.5, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 16 and 24 hpost-dosing. Plasma was separated from blood within 20 min bycentrifugation at 2000 × g (10 min at 4 ◦C). Each plasma sample wassplit into two aliquots and stored at −20 ± 5 ◦C. Urine was collectedpre-dosing and at intervals of 0–4, 4–8, 8–12, 12–24, 24–48 h post-dosing into refrigerated flasks. The weight of each urine fractionwas recorded, a sample of approximately 100 mL was split into twoaliquots and frozen.
Study medications
The film-coated tablets (200 mg) of generic rifaximin (San-doz Biopharmaceuticals SpA) and those of branded rifaximin (AlfaWassermann SpA) were from the same batch, which was n. 00307and n. 8278 for generic formulation and NormixTM, respectively.The brand of generic rifaximin was selected amongst the productsavailable in the Italian market at the time of the study. It is notewor-thy that they were all manufactured by the same company (SpecialProduct’s Line SpA, Pomezia, Italy) and contained the same activeingredient (Industrias GMB SA, Barcelona, Spain) [31]. Therefore, nospecific criteria were needed to select a given generic formulation.The compositions of NormixTM and generic rifaximin are displayedin Table 1.
X-ray power diffraction analysis of the generic formulationshowed the presence of both amorphous rifaximin and rifaximin�. Quantitative estimation was not possible, due to interference oftablet excipients in this kind of analysis.
Safety evaluations
Volunteers were enquired about the occurrence of any adverseevent after their admission to the clinical unit, both before theadministration of study drugs and throughout the study until dis-charge. Vital signs were monitored.
Rifaximin assay
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
Rifaximin concentration in plasma and urine samples was mea-sured by liquid chromatography mass spectrometry (LC/MS-MS)as previously described [23], with a lower limit of quantification
166
167
168

ARTICLE IN PRESSG ModelYPHRS 2697 1–6
C. Blandizzi et al. / Pharmacological Research xxx (2014) xxx–xxx 3
Table 1Chemical composition of the rifaximin formulations employed in the presentpharmacokinetic study. The only difference between the branded and generic for-mulations concerns one excipient (highlighted in gray).
Branded rifaximin(Normix®) 200-mgfilm-coated tablet
Generic rifaximin200-mg film-coatedtablet
Active ingredient(crystalline status)
Rifaximin(polymorph �)
Rifaximin(Amorphous form andpolymorph �)
Excipients Sodium starch glycolate Sodium starchglycolate
Glycerol distearate Glycerol monostearateColloidal anhydrous silica Colloidal anhydrous
silicaTalc TalcMicrocrystallinecellulose
Microcrystallinecellulose
Coating components Hypromellose HypromelloseTitanium dioxide Titanium dioxide
(aanait
P
WTncA(cvclorot
S
pnmtp
TD
0-4 0-8 0-12 0-24 0-480
25
50
75
100
125
150
Time (h)
Cum
ulat
ive
Urin
ary
Excr
etio
n ( μ
g)
Branded 400 mgGeneric 400 mg
0 2 4 6 8 10 12 14 16 18 20 22 240
1
2
3
4
5
6
Time (h)
Plas
ma
Con
cent
ratio
n (n
g/m
l)
Branded 400 mgGene ric 400 mg
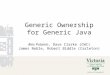
Fig. 1. Mean rifaximin concentration–time (top panel) and cumulative urinary
shown in Fig. 1. The respective values of estimated PK param-eters are reported in Table 3. In most subjects, the first plasmarifaximin concentration could be detected at the first blood sam-pling (i.e. 30 min after dosing) for both rifaximin formulations.
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
Disodium edetate Disodium edetatePropylene glycol Propylene glycolRed iron oxide E172 Red iron oxide E172
LLOQ) of 0.5 ng/mL in both the biological fluids analyzed. The intra-ssay precision (CV%) for all quality control (QC) samples was ≤7.2,nd the mean accuracy (ACC%) ranged from −5.3 to −0.3 of theominal concentration. The inter-assay precision (CV%) was ≤5.1nd the mean accuracy (ACC%) ranged from −1.1 to +2.3 of the nom-nal concentration. No significant interfering peaks were found athe retention times of rifaximin and internal standard.
harmacokinetic evaluations
Non-compartmental PK analysis was carried out withinNonLinTM software (Pharsight, Mountain View, CA, U.S.A.).
he highest concentration achieved in plasma (Cmax), the timeeeded to achieve Cmax (Tmax), the area under the drug plasmaoncentration–time curve from time 0 to infinity (AUC0–∞), theUC from time 0 to the time of last quantifiable drug concentration
AUC0–t), the plasma drug elimination half-life (t1/2), and theumulative urinary excretion (Ae0–48 h) were estimated from indi-idual concentration–time curves. The first order elimination rateonstant was estimated by linear regression of the time versus theog of drug concentration using the terminal (log-linear) portionf the curve. AUC0–t was calculated by the linear trapezoidalule. Extrapolation to infinity for the estimation of AUC0–∞ wasbtained by dividing the last quantifiable drug concentration byhe elimination rate constant and adding this value to AUC0–t [32].
tatistical analysis
Descriptive and summary statistics were used. All results areresented as means ± standard error of the mean (SEM). The sig-
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
ificance of differences between mean values was calculated byeans of Student’s t test for paired data. ANOVA was employed
o evaluate the effect of period, sequence and formulations on PKarameters. p < 0.05 were considered significant. All calculations
able 2emographic characteristics of subjects (n = 24).
Age (years) Height (cm) Weight (kg) BMI (kg/m2)
Mean 36.21 170.25 66.33 22.92SEM 1.82 1.64 1.97 0.37CV% 24.61 4.73 14.55 7.92Min 19.00 156.00 53.00 19.00Max 52.00 181.00 88.00 27.00
excretion (bottom panel) profiles following administration of 400-mg single-dosegeneric or branded (polymorph-�) rifaximin to healthy volunteers. Each point orcolumn represents the mean ± SEM (vertical lines) obtained from 24 subjects.
were performed with the Instat® software (GraphPad Sofware Inc.,La Jolla, CA, USA).
Results
Demographic characteristics of healthy volunteers
Twenty-four subjects met the selection criteria and completedthe experimental procedures. Their overall characteristics are dis-played in Table 2.
Plasma and urinary PK profiles
The mean plasma and urinary excretion profiles of healthyvolunteers, treated with generic rifaximin or rifaximin-�, are
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
Table 3Mean values of plasma and urine pharmacokinetic parameters of rifaximin esti-mated following the administration of generic rifaximin and rifaximin-� at thesingle dose of 400 mg (n = 24).
Parameters 400 mg
Rifaximin-� Generic rifaximin P-value
Cmax (ng/ml) 2.29 ± 0.28 6.89 ± 0.74 <0.00001Tmax (h) 1.78 ± 0.46 1.98 ± 0.30 NSAUC0–t (ng/ml × h) 6.34 ± 0.99 28.26 ± 3.86 <0.00001AUC0–∞(ng/ml × h) 9.80 ± 1.23 32.24 ± 3.98 <0.00001t1/2 (h) 2.8 ± 0.4 4.5 ± 0.4 NSAe0–48h (�g) 45.27 ± 4.61 120.13 ± 14.59 <0.00001

ARTICLE ING ModelYPHRS 2697 1–6
4 C. Blandizzi et al. / Pharmacological
Table 4ANOVA analysis for cross-over design.
Rifaximin Period Sequence Formulation
F p F p F p
Cmax 0.74 0.3975 0.62 0.4378 105.61 <0.00001AUC 1.62 0.2160 0.97 0.3364 206.63 <0.00001
Pwgw
rrdjardu
lrFtti
PiPgfl3
sis1b
S
srs
D
ma[fcaftt
w
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
0–t
AUC0–∞ 3.10 0.0948 0.98 0.3336 162.28 <0.00001Ae0–48 h 1.66 0.2107 2.26 0.1473 83.00 <0.00001
lasma concentrations then increased up to the peak, whichas achieved at 1.98 h (range: 0.50–6.0) in subjects treated with
eneric rifaximin, and 1.78 h (0.5–12.0) in subjects administeredith rifaximin-�.
Plasma concentrations were lower after administration ofifaximin-� than generic rifaximin. Following treatment withifaximin-�, the drug could be detected in plasma up to 8 h fromosing in 3/24 subjects, and up to 10 h from dosing in 2/24 sub-
ects; rifaximin concentrations remained below the LLOQ after 16 hnd 24 h from dosing. Upon administration of the generic product,ifaximin plasma concentrations could be measured up to 12 h fromosing in 6/24 subjects, up to 16 h from dosing in 7/24 subjects, andp to 24 h in 2/24 subjects.
Urine rifaximin concentrations could be detected at all col-ection intervals in all subjects after administration of genericifaximin, and in 21/24 subjects after treatment with rifaximin-�.ollowing the administration of rifaximin-� or generic rifaximin,he highest urine concentration was measured at the first collec-ion interval (0–4 h) in 16/24 subjects, and at the second collectionnterval (4–8 h) in 8/24 subjects.
Rifaximin plasma and urine concentration–time profiles andK parameters showed marked differences when generic rifax-min and rifaximin-� were compared. As shown in Table 3, mostK parameters were significantly higher after administration ofeneric rifaximin than rifaximin-�. In particular, the differencesor Cmax, AUC0–t, AUC0–∞ and Ae0–48 h between the generic formu-ation and the product containing rifaximin-� ranged from 165% to45%.
ANOVA evaluation of all parameters for cross-over designhowed statistically significant differences between the two rifax-min products tested (Table 4). On the contrary, there were notatistically significant differences in relation to the period (period
versus period 2) or the sequence (brand-generic versus generic-rand) of administration of the two formulations.
afety
No serious adverse events occurred throughout the study. Sevenubjects developed 7 adverse events of mild intensity, whichesolved spontaneously and were all judged as not related to thetudy medications.
iscussion
Regulatory Authorities are paying increasing attention to poly-orphism, not only for new drug applications, but also for
bbreviated/abridged new applications, required for generic drugs3,6,32]. Since differences between crystalline and amorphous drugorms might be more relevant than those existing amongst differentrystalline forms, the issue can become very critical from a ther-peutic standpoint when a significant amount of the amorphousorm is administered instead of its crystalline counterpart. Indeed,
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
he systemic bioavailability of the amorphous rifaximin was foundo be significantly higher than that of the polymorph � [27].
In the present study, when generic rifaximin was comparedith the branded formulation (containing the pure polymorph-�),
PRESS Research xxx (2014) xxx–xxx
the findings were unexpected. Indeed, our results show that thePK profile of generic rifaximin differs significantly from that ofbranded rifaximin-�, while – according to regulatory requirementsfor equivalence [3] – the systemic bioavailability of the genericproduct should overlap that of the branded formulation. Indirectcomparisons with data from a previous study [27] suggest thatthe PK of generic formulation also differs from that of the pureamorphous rifaximin. Indeed, since X-ray diffraction patternsshowed that in the generic product both the amorphous formand polymorph � are present, it is conceivable that the systemicbioavailability of rifaximin depends on the composition (in termsof crystalline polymorphs and amorphous form) present in the for-mulation. The observed differences between branded rifaximin-�and its generic formulation cannot be ascribed to variations inthe composition of non-active ingredients, since, as outlined inTable 1, both the excipients and coating components were virtuallythe same. In addition, despite the branded formulation employedin the present investigation belonged to a different batch of theproduct employed in our previous PK study [27], and despite theenrolled subjects were also different, the PK behavior of the activeingredient (polymorph-�) in both studies appears to be consistent,indicating its physico-chemical stability over time.
Drug polymorphs occur during the synthesis and purification ofactive ingredients. The occurrence of a given polymorph dependson the conditions of synthesis and crystallization [12,13]. The wholeproduction process generally leads to the formation of a givenpolymorph rather than the amorphous form of a drug. X-ray diffrac-tion studies revealed that rifaximin polymorphs are hydrates [34]and, since addition or removal of water can lead to changes inpolymorphism, great attention should be paid also to any manip-ulation and storage of the drug (be it a branded or a genericformulation) to ensure stability of the desired crystal structure.Overall, it is possible that – for the generic formulation tested(i.e. a mixture of amorphous and crystalline rifaximin) – manu-facturing and/or storage processes were different from those ofthe original molecule contained in the branded formulation. Beingthe polymorph content related to the manufacturing process, thesame considerations should be applied to those medicinal prod-ucts containing rifaximin, whose origin of the active ingredient isdifferent from that of the molecule contained in the branded formu-lations (Normix®, Xifaxan®, Flonorm® and other brand names). Insome South-American Countries (Argentina, Colombia, Venezuelaand Peru) as well as in Egypt, Turkey, India and China there areindeed branded formulations of rifaximin whose summary of prod-uct characteristics provides no clear information about the specificcrystal structure of the active ingredient.
The increased systemic bioavailability of the generic formula-tion raises some clinically relevant concerns. Indeed, for a poorlyabsorbed antibiotic, whose antimicrobial activity is intended tobe topical (i.e. within the GI tract), systemic absorption mightlead to reduced local bioavailability and potentially to systemicadverse events. In the case of rifaximin, a reduced intraluminalbioavailability might be without clinical consequences since itsfecal concentrations are known to largely exceed the MIC values ofpathogenic enteric bacteria [21]. The risk of adverse events wouldbe expected to correlate with blood levels [35,36]. With the poly-morph-�, contained in the branded formulation, both the short-and long-term tolerability is extremely good [21,37,38], most likelybecause of the lack of systemic absorption. However, after 400-mg single-dose administration of the generic formulation, Cmax
increased by more than 200%. When translating these findings tothe clinical setting, rifaximin blood levels would be expected to
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
increase even more in patients with liver disease, in whom bloodconcentrations of rifaximin-� are already 10–20 times higher,depending on the disease severity (Child–Pugh A–C classes) [38,39].This is of particular concern since rifaximin received approval for
327
328
329
330

ING ModelY
ogical
“p
tTgmsccsmirtfism1oat
srNrtHtaftmodrc
C
gtbwbo
C
ifAfiCW
UQ3
[
[
[
[
[
[
[
[
[
[
[
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
ARTICLEPHRS 2697 1–6
C. Blandizzi et al. / Pharmacol
reduction in risk of overt hepatic encephalopathy recurrence inatients with advanced liver disease” [39].
Rifaximin is the most effective and widely used antibiotic forhe treatment of SIBO (small intestine bacterial overgrowth) [40].he recent discovery of an association between SIBO and functionalut symptoms, albeit controversial, has renewed interest in thisimicry. SIBO represents indeed an umbrella term, under which
ome different functional (e.g. irritable bowel syndrome, chroniconstipation, diarrhea) or organic (e.g. inflammatory bowel disease,eliac disease, diverticular disease, etc.) conditions can be included,ince – in each of them – bacterial proliferation (and consequentinimal inflammation) may, at least in part, trigger similar abdom-
nal symptoms. In all these conditions, especially the organic ones,ifaximin is used long-term to get rid of pathogenic bacteria, reducehe inflammatory response and achieve symptom relief [41,42]. Asor every drug used in the long-term, safety – besides efficacy –s of paramount importance. Rifaximin-� proved to be extremelyafe, even given continuously (at standard therapeutic doses) for 6onths and its minimal, if any, systemic absorption (not exceeding
%) accounts for the adverse event profile, which overlapped thatf placebo [38]. The use of generic rifaximin formulation(s), whosebsorption is higher and often unpredictable, might not guaranteehe excellent tolerability of the branded medication.
A peculiar, potentially serious, adverse event, related toystemic rifaximin exposure, is the development of extra-GI cross-esistance. This is particularly relevant to M. tuberculosis andeisseria meningitides since rifampicin (another member of the
ifamycins’ family) is a pivotal antibiotic for the treatment ofuberculosis [43,44] and prevention of Neisseria meningitis [45–47].owever, a 10-year survey [48] in Italy has shown that mycobac-
erial resistance to rifampicin has remained quite stable over timend a recent Italian study [49] found that all meningococci isolatedrom asymptomatic carriers were susceptible to rifampicin, despitehe large consumption of rifaximin in our Country. The above-
entioned bacterial cross resistances are therefore very unlikely toccur with the polymorph-�, but – taking into account the presentata on systemic bioavailability – it is plausible that the risk ofesistance with the generic formulation of rifaximin might becomelinically relevant.
onclusions
The present results show different systemic bioavailability ofeneric and branded formulations of rifaximin. As a consequence,he therapeutic results obtained with the polymorph-� should note translated sic et simpliciter to generic rifaximin formulations,hich can display significant systemic absorption and can no longer
e included in the class of poorly absorbable (locally acting) antibi-tics.
onflict of interest
Corrado Blandizzi has occasionally been involved, as a speaker,n satellite symposia supported by Alfa Wassermann, the manu-acturer of rifaximin. Giuseppe Claudio Viscomi is an employee oflfa Wassermann. Antonio Marzo is an employee of the Institute
or Pharmacokinetic and Analytical Studies SA, where the clin-cal study was conducted upon contract with Alfa Wassermannarmelo Scarpignato is member of the Speakers’ Bureau of Alfaassermann.
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
ncited reference
[33].
[
[
PRESSResearch xxx (2014) xxx–xxx 5
Acknowledgments
We are indebted to Professor Fabrizia Grepioni (Department ofChemistry “G. Ciamician”, University of Bologna, Italy) for perform-ing and interpreting the XRPD analysis.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.phrs.2014.05.001.
References
[1] Slavik RS, Jewesson PJ, Minghetti P. Regulatory status of medicinal products forhuman beings in the European Union. The role of generic products. PharmacolRes 1996;34:3–7.
[2] EMA The European Agency for the Evaluation of Medicinal Products. Guide-line on the investigation of bioequivalence. CPMP/EWP/QWP/1401/98 Rev. 1;2010. Available at: http://www.ema.europa.eu/docs/en GB/document library/Scientific guideline/2010/01/WC500070039.pdf [accessed 10.03.14].
[3] HHS/FDA Guidance for industry: bioavailability and bioequivalencestudies for orally administered drug products – General consider-ations; 2003. Available at: http://www.fda.gov/downloads/Drugs/Guidance ComplianceRegulatoryInformation/Guidances/ucm070124.pdf[accessed 10.03.14].
[4] World Health Organization. Multisource (generic) pharmaceutical products:guidelines on registration requirements to establish interchangeability. Annex7. WHO Technical Report Series, No. 937; 2006. Available at: http://www.who.int/medicines/services/expertcommittees/pharmprep/QAS04 093Rev4 final.pdf [accessed 10.03.14].
[5] Slavik RS, Jewesson PJ. Selecting antibacterials for outpatient parenteralantimicrobial therapy: pharmacokinetic–pharmacodynamic considerations.Clin Pharmacokinet 2003;42:793–817.
[6] Scaglione F, Paraboni L. Influence of pharmacokinetics/pharmacodynamics ofantibacterials in their dosing regimen selection. Expert Rev Anti Infect Ther2006;4:479–90.
[7] EMA The European Agency for the Evaluation of Medicinal Products.Note for guidance on the clinical requirements for locally applied,locally acting products containing known constituents. CPMP/EWP/239/95;1995. Available at: http://www.ema.europa.eu/docs/en GB/document library/Scientific guideline/2009/09/WC500003687.pdf [accessed 10.03.14].
[8] Thomas VH, Bhattachar S, Hitchingham L, Zocharski P, Naath M, Surendran N,et al. The road map to oral bioavailability: an industrial perspective. ExpertOpin Drug Metab Toxicol 2006;2:591–608.
[9] Hurst S, Loi CM, Brodfuehrer J, El-Kattan A. Impact of physiological, phys-icochemical and biopharmaceutical factors in absorption and metabolismmechanisms on the drug oral bioavailability of rats and humans. Expert OpinDrug Metab Toxicol 2007;3:469–89.
10] Singhal D. Drug polymorphism and dosage form design: a practical perspective.Adv Drug Deliv Rev 2004;56:335–47.
11] Huang LF, Tong WQ. Impact of solid state properties on developability assess-ment of drug candidates. Adv Drug Deliv Rev 2004;56:321–34.
12] Peterson ML, Hickey MB, Zaworotko MJ, Almarsson O. Expanding the scopeof crystal form evaluation in pharmaceutical science. J Pharm Pharm Sci2006;9:317–26.
13] Lee AY, Erdemir D, Myerson AS. Crystal polymorphism in chemical processdevelopment. Annu Rev Chem Biomol Eng 2011;2:259–80.
14] Aguiar AJ, Krc J, Kinkel AW, Samyn JC. Effect of polymorphism on theabsorption of chloramphenicol from chloramphenicol palmitate. J Pharm Sci1967;56:847–53.
15] Pandit JK, Gupta SK, Gode KD, Mishra B. Effect of crystal form on the oralabsorption of phenylbutazone. Int J Pharm 1984;21:129–32.
16] Kato Y, Kohketsu M. Relationship between polymorphism and bioavailabilityof amobarbital in the rabbit. Chem Pharm Bull 1981;29:268–72.
17] Kimura N, Fukui H, Takagaki H, Yonemochi E, Terada K. Characterisationof polymorphs of a novel quinolinone derivative TA-270 (4-hydroxy-1-methyl-3-octyloxy-sinapinoylamino-2(1H)-quinolinone). Chem Pharm Bull2001;49:1321–5.
18] Bauer J, Spanton S, Henry R, Quick J, Dziki W, Porter W, et al. an extraordinaryexample of conformational polymorphism. Pharm Res 2001;18:859–66.
19] Marchi E, Montecchi L, Venturini AP, Mascellani G, Brufani M, Cellai L. 4-Deoxypyrido [1′ ,2′:1,2]imidazo[5,4-c]rifamycin SV derivatives. A new series ofsemisynthetic rifamycins with high antibacterial activity and low gastroentericabsorption. J Med Chem 1985;28:960–3.
20] Scarpignato C, Pelosini I. Rifaximin, a poorly absorbed antibiotic: pharmacology
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
and clinical potential. Chemotherapy 2005;51(Suppl. 1):36–66.21] Scarpignato C, Pelosini I. Experimental and clinical pharmacology of rifaximin,
a gastrointestinal selective antibiotic. Digestion 2006;73(Suppl. 1):13–27.22] European Pharmacopoeia. Rifaximin (Revised Monograph) Suppl.
2011;7.1:2362.
459
460
461
462
463

ING ModelY
6 ogical
[
[
[
[
[
[
[
[[
[
[
[
[
[
[
[
[ Q4
[
[
[
[
[
[
[
[
[
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
ARTICLEPHRS 2697 1–6
C. Blandizzi et al. / Pharmacol
23] Viscomi GC, Campana M, Barbanti M, Grepioni F, Polito M, Confortini D, et al.Crystal forms of rifaximin and their effect on pharmaceutical properties. Crys-tEngComm 2008;10:1074–81.
24] Grant DJW. Theory and origin of polymorphism. In: Brittain HG, editor. Poly-morphism in pharmaceutical solids. New York: Marcel Dekker; 1999. p. 1–34.
25] Rodriguez-Spong B, Price CP, Jayasankar A, Matzger AJ, Rodriguez-Hornedo N.General principles of pharmaceutical solid polymorphism: a supramolecularperspective. Adv Drug Deliv Rev 2004;56:241–74.
26] Viscomi GC, MAffei P, Lauro V, Barbanti M, Confortini D, Braga D. Rifaximinpowder, process for preparing the same and controlled release composi-tions containing said rifaximin useful for obtaining long-lasting effect. WHO2011;1079:70.
27] Marzo A, Ismaili S. A randomised, crossover study to evaluate the safety andthe pharmacokinetic profiles of a single oral dose (400 mg) of amorphous rifax-imin in comparison with a single oral dose (400 mg) of Normix® (rifaximinpolymorph �) in healthy volunteers. Dig Liv Dis 2010;42(Suppl. 2):191–2.
28] Normix® Summary of Product Characteristics (Revision September 1, 2007),Section 5.1.
29] Del Tacca M, Pasqualetti G, Di Paolo A, Virdis A, Massimetti G, Gori G, et al. Lackof pharmacokinetic bioequivalence between generic and branded amoxicillinformulations. A post-marketing clinical study on healthy volunteers. Br J ClinPharmacol 2009;68:34–42.
30] Marzo A. Open questions in bioequivalence. Pharmacol Res 1995;32:237–40.31] Italian Medicines Agency (AIFA). Marketing authorization of generic
rifaximin products. G.U., vol. 263 (Suppl. 247); 2010. Avail-able at: http://www.gazzettaufficiale.it/do/gazzetta/downloadPdf?dataPubblicazioneGazzetta=20101110&numeroGazzetta=263&tipoSerie=SG&tipoSupplemento=SO&numeroSupplemento=247&estensione=pdf&edizione=0 [accessed 10.03.14].
32] Marzo A. Clinical pharmacokinetic registration file for NDA and ANDA proce-dures. Pharmacol Res 1997;36:425–50.
33] Food and Drug Administration (FDA). Guidance for industry. ANDAs:pharmaceutical solid polymorphism. Chemistry, manufacturing andcontrols information. Center for Drug Evaluation and Research(CDER); 2007. Available at: http://www.fda.gov/downloads/Drugs/
Please cite this article in press as: Blandizzi C, et al. Is generic rifaximingeneric formulations in healthy volunteers. Pharmacol Res (2014), htt
GuidanceComplianceRegulatoryInformation/Guidances/ucm072866.pdf[accessed 10.03.14].
34] Braga D, Grepioni F, Chelazzi L, Campana M, Confortini D, Viscomi GC. The struc-ture–property relationship of four crystal forms of rifaximin. CrystEngComm2012;14:6404–11.
[
PRESS Research xxx (2014) xxx–xxx
35] Cohen JS. Avoiding adverse reactions. Effective lower-dose drug therapies forolder patients. Geriatrics 2000;55:54–6.
36] Hickey E. Tools to define the relevance of PK/PD parameters to the efficacy,toxicity and emergence of resistance of antimicrobials. Curr Opin Drug DiscovDev 2007;10:49–52.
37] Ericsson CD. Safety and tolerability of the antibacterial rifaximin in the treat-ment of travellers’ diarrhoea. Drug Saf 2006;29:201–7.
38] Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, et al. Rifaximintreatment in hepatic encephalopathy. N Engl J Med 2010;362:1071–81.
39] Salix Pharmaceuticals Inc XifaxanTM 550 Prescribing Information; 2014. Avail-able at: http://cdn.salix.com/shared/pi/xifaxan550-pi.pdf [accessed 10.03.14][in press].
40] Scarpignato C, Gatta L. Commentary: towards an effective and safe treat-ment of small intestine bacterial overgrowth. Aliment Pharmacol Ther2013;38:1409–10.
41] Scarpignato C, editor. Rifaximin, a poorly absorbed antibiotic. Pharmacologyand clinical use. Basel: Karger AG; 2005. p. 1–132.
42] Scarpignato C, Lanas A, editors. Bacterial flora in digestive disease. Focus onrifaximin. Basel: Karger AG; 2006. p. 1–254.
43] Burman WJ, Gallicano K, Peloquin C. Comparative pharmacokineticsand pharmacodynamics of the rifamycin antibiotics. Clin Pharmacokinet2001;40:327–41.
44] Frieden TR, Sterling TR, Munsiff SS, Watt CJ, Dye C. Tuberculosis. Lancet2003;362:887–99.
45] Girgis N, Sultan Y, Frenck Jr RW, El-Gendy A, Farid Z, Mateczun A. Azithromycincompared with rifampin for eradication of nasopharyngeal colonization byNeisseria meningitidis. Pediatr Infect Dis J 1998;17:816–9.
46] Cuevas LE, Kazembe P, Mughogho GK, Tillotson GS, Hart CA. Eradicationof nasopharyngeal carriage of Neisseria meningitidis in children and adultsin rural Africa: a comparison of ciprofloxacin and rifampicin. J Infect Dis1995;171:728–31.
47] Schwartz B, Al-Tobaiqi A, Al-Ruwais A, Fontaine RE, A’ashi J, Hightower AW,et al. Comparative efficacy of ceftriaxone and rifampicin in eradicating pharyn-geal carriage of group A Neisseria meningitidis. Lancet 1988;1:1239–42.
48] Fietta A, Cascina A, Meloni F, Morosini M, Casali L, Bono L, et al. A 10-year
still a poorly absorbed antibiotic? A comparison of branded andp://dx.doi.org/10.1016/j.phrs.2014.05.001
survey of Mycobacterium tuberculosis isolates in Pavia and their drug resistance:a comparison with other Italian reports. J Chemother 2002;14:33–40.
49] Cresti S, Giordano I, Donati E, Giaccherini R, Barberi A, Cellesi C. Prevalence andchemosusceptibility of Neisseria meningitidis and Haemophilus influenzae in apopulation of central Italy. New Microbiol 2003;26:281–8.
538
539
540
541
542