Embed Size (px)
Citation preview

Converting absorbed dose to medium to absorbed dose to water for Monte Carlo based
photon beam dose calculations
This article has been downloaded from IOPscience. Please scroll down to see the full text article.
2000 Phys. Med. Biol. 45 983
(http://iopscience.iop.org/0031-9155/45/4/313)
Download details:IP Address: 129.78.32.23The article was downloaded on 10/05/2012 at 17:55
Please note that terms and conditions apply.
View the table of contents for this issue, or go to the journal homepage for more
Home Search Collections Journals About Contact us My IOPscience

Phys. Med. Biol. 45 (2000) 983–995. Printed in the UK PII: S0031-9155(00)09047-3
Converting absorbed dose to medium to absorbed dose towater for Monte Carlo based photon beam dose calculations
J V Siebers†, P J Keall†, A E Nahum‡ and R Mohan†† Department of Radiation Oncology, Medical College of Virginia Hospitals,Virginia Commonwealth University, PO Box 980058, Richmond, VA, USA‡ Joint Department of Physics, Royal Marsden Hospital and Institute of Cancer Research, Sutton,Surrey, UK
E-mail: [email protected]
Received 27 October 1999, in final form 20 January 2000
Abstract. Current clinical experience in radiation therapy is based upon dose computations thatreport the absorbed dose to water, even though the patient is not made of water but of many differenttypes of tissue. While Monte Carlo dose calculation algorithms have the potential for higher doseaccuracy, they usually transport particles in and compute the absorbed dose to the patient mediasuch as soft tissue, lung or bone. Therefore, for dose calculation algorithm comparisons, or toreport dose to water or tissue contained within a bone matrix for example, a method to convertdose to the medium to dose to water is required. This conversion has been developed here byapplying Bragg–Gray cavity theory. The dose ratio for 6 and 18MV photon beams was determinedby computing the average stopping power ratio for the primary electron spectrum in the transportmedia. For soft tissue, the difference between dose to medium and dose to water is approximately1.0%, while for cortical bone the dose difference exceeds 10%. The variation in the dose ratio as afunction of depth and position in the field indicates that for photon beams a single correction factorcan be used for each particular material throughout the field for a given photon beam energy. Theonly exception to this would be for the clinically non-relevant dose to air. Pre-computed energyspectra for 60Co to 24 MV are used to compute the dose ratios for these photon beams and todetermine an effective energy for evaluation of the dose ratio.
1. Introduction
Conventional dose calculations for photon beam radiation therapy typically report the absorbeddose towater (Dw). The reporting ofDw is due partly to the historical development of treatmentplanning algorithms as well as the fact that treatment machines are calibrated in terms of theabsorbed dose to water. The input data used for treatment planning algorithms are generallydose profiles and output factors measured in water phantoms. These data are manipulated invarious ways by the algorithm used, but converting the in-phantom measured dose to waterto dose to medium is not considered. The assumption that the body is water is a good firstapproximation as water makes up the bulk of the volume of cells and body fluid (with a fewexceptions such as bone and tooth enamel) (Tortora and Grabowski 1993).
Monte Carlo (MC) dose calculation algorithms are being introduced into routine treatmentplanning practice (Hartmann-Siantar et al 1994, 1995, Mohan 1997, DeMarco et al 1998,Solberg et al 1998, Wang et al 1998, Fippel 1999, Ma et al 1999). When using Monte Carlo,the absorbed dose is computed to the medium contained in the dose voxel (Dmed). These canbe arbitrary materials, and generally are representative of those found in the body. However,
0031-9155/00/040983+13$30.00 © 2000 IOP Publishing Ltd 983

984 J V Siebers et al
in order to compare MC algorithms with conventional Dw algorithms, the dose comparisonshould be to the same medium. There are several other reasons whyDmed should be convertedto Dw, which will be expanded upon in the discussion section.
The purpose of this paper is to (a) determine the factors required for converting absorbeddose to medium to absorbed dose to water for photon therapy beams, (b) determine if universalconversion factors can be applied throughout the patient volume, (c) determine if conversionfactors depend upon the material density and (d) provide a method for determining conversionfactors for arbitrary patient materials and energies.
2. Background
Absorbed dose Dmed can be converted to Dw for photon beam irradiation using Bragg–Graycavity theory (Bragg 1912, Gray 1936, Attix 1986, Brahme et al 1988). Bragg–Gray cavitytheory and its extension the Spencer–Attix cavity theory (Spencer and Attix 1955) have beensuccessfully applied to ionization chamber dosimetry (AAPM TG-21 1983, ICRU-35 1984,Attix 1986). Bragg–Gray cavity theory is applicable when the cavity material (water in thiscase) does not perturb the fluence of charged particles that would have existed if the cavity werecomposed of the surrounding material. In the case of photons, this requires that the ranges ofthe secondary electrons are much greater than the dimensions of the cavity i.e. that the cavitydoes not ‘perturb’ this electron fluence, which is then entirely characteristic of the surroundingmedium. In practice, for photons at megavoltage energies, the only real dosimeter that fulfillsthis requirement is the gas-filled ionization chamber (Ma and Nahum 1991). The originalBragg–Gray theory requires that delta-ray (secondary electron) equilibrium exists or that theenergy transferred to delta rays is deposited ‘on the spot’; it is evaluated by using the primaryelectron fluence and the unrestricted collision stopping powers (see below). Spencer–Attixtheory (Spencer and Attix 1955, ICRU-35 1984) removed this limitation in an approximatefashion by including delta rays in the fluence of charged particles entering the cavity, and thenusing the stopping power restricted to losses less than 1, where this cutoff energy is relatedto the size of the cavity. For small cavities such as ion chambers 1 is generally set equalto 10 keV (Nahum 1978, ICRU-35 1984). It can be noted that, somewhat paradoxically, thegreatest deviation between the Bragg–Gray and Spencer–Attix values for the stopping-powerratio occur for the smallest values of 1 i.e. for the smallest cavities.
To circumvent the unnecessary issues introduced by the selection of the Spencer–Attix cutoff energy, we consider a hypothetical Bragg–Gray water cavity in which delta-rayequilibrium is established. Thus the conversion can proceed as follows.
Using Bragg–Gray cavity theory, the absorbed dose to water is related to the absorbeddose to medium by
Dw = Dmedsw,med (1)where sw,med is the unrestricted water-to-mediummass collision stopping power ratio averagedover the energy spectra of primary electrons, (8E)m. The so-called primary electrons do notinclude knock-on electrons or �-rays, as their contributions to energy deposition are accountedfor in the unrestricted stopping powers. The stopping power ratio averaged over the primaryelectron spectrum is calculated using
sw,med =Z Emax
0(8E)m(S/⇢)w dE
� Z Emax
0(8E)m(S/⇢)med dE (2)
where (S/⇢)w and (S/⇢)med are the unrestricted mass collision stopping power for the waterand transport medium respectively, andEmax is the maximum energy in the (8E)m distribution(NCRP-27 1961).

Converting absorbed dose to medium to absorbed dose to water 985
To evaluate the Bragg–Gray stopping power ratio for photon beams, knowledge of theelectron fluence in themedia is required. Presently, onlyMC-based dose calculation algorithmsare capable of determining this quantity.
3. Materials and methods
In order to determine sw,med, the Monte Carlo code MCNP (Briesmeister 1997) was usedto transport photons and accompanying electrons through various homogeneous and simpleheterogeneous phantoms. The majority of the calculations used full Monte Carlo simulationsof the treatment head to describe the output beams from the linear accelerator. Details of thetransport through the treatment head are given elsewhere (Siebers et al 1999), and are reviewedhere briefly. Electrons with energy equal to the nominal acceleration potential of the therapyaccelerator were incident upon the accelerator bremsstrahlung target. Photons and electronsexiting the target were transported through the beam-line components (primary collimator,flattening filter and ionization chamber) and had their energy, position and direction stored intoa phase-space description file. These saved particles were then sampled and transported in thisstudy through the beam-defining jaws to a phantom whose surface was at the isocentre planelocation. Particles were transported through a phantom and the primary electron fluence in thephantom medium ((8E)m) was scored (to score only primary fluence, the MCNP parameterRNOK was set to 0). The low energy electron cut-off energy was set to 7.5 keV for the MonteCarlo simulation in this study. Below this energy, the electron fluence was estimated to beequal to the fluence at 7.5 keV and the mean stopping power for these electrons was estimatedto be equal to the residual energy divided by the CSDA range. The uncertainty introduced bythis technique is addressed in the results section.
Monte Carlo simulations were performed for 6 MV and 18 MV photon beams from aVarian 2100C accelerator. The field size was set to 10⇥ 10 cm2 at 100 cm SSD incident upona 50 ⇥ 50 ⇥ 50 cm3 phantom. The electron fluence in each scoring region was determinedusing the track length estimate of the cell flux (which in steady state conditions equals thecell fluence). In each region of the phantom, the electron fluence was used to compute thefluence-averagedmediumandwater stopping power values, and the stopping power ratio (usingequation (2)). Stopping power ratios with respect to water were determined for air (ICRU-441988), lung (ICRU-44 1988), ICRU tissue (ICRU-33 1980), soft bone (spongiosa) (ICRU-441988) and cortical bone (ICRP-23 1975). The densities and compositions of these materialsare listed in table 1. Although air is not a patient material, it is included in this work so resultscan be compared with Andreo and Brahme (1986) who evaluated sw,air using Spencer–Attixtheory for ionization chamber dosimetry as functions of depth and field size.
The variation of the dose ratio as a function of off-axis position and depth was studiedby evaluating sw,med at multiple depths in a pure water phantom both inside and outsidethe 10 ⇥ 10 cm2 field. For the ‘inside the field’ evaluation, (8E)m was evaluated inside a4⇥4 cm2 area centred about the central axis, while the ‘outside the field’ evaluation consistedof evaluating (8E)m for electrons outside a 12 ⇥ 12 cm2 area centred on the central axis.1 ⇥ 108 phase-space particles were transported from the phase-space definition plane in thisportion of the study.
The electron spectra produced in photon interactions will depend upon the material inwhich the transport takes place. To investigate the influence of the differing electron energyspectra produced by various patient-like materials on sw,med, the field-positional tests abovewere repeated with the water phantom replaced with a cortical bone and a lung-tissue phantom.
The stopping power ratio was also evaluated at the interface between lung and bone slabsto investigate if the ratio varies in situations of electronic disequilibrium. Two phantoms were

986 J V Siebers et al
Table 1. The atomic percentage composition by relative mass of the materials used in thesecalculations as well as the physical density, and the density range over which the material is usedin our Monte Carlo dose calculations.
Density[density range]
Material (g cm�3) H C N O Other
Water 1.0 11.2 88.8Air 1.2⇥ 10�3 [0–0.08] 0.0124 75.5 23.2 Ar 1.28(ICRU-44 1988)Lung 0.26 [0.08–0.5] 10.3 10.5 3.1 74.9 Na 0.2, P 0.2, S 0.3, Cl 0.3,(ICRU-44 1988) K 0.2ICRU tissue 1.0 [0.5–1.1] 10.1 11.1 2.6 76.2(ICRU-33 1980)Soft bone 1.18 [1.1–1.4] 8.5 40.4 2.8 36.7 Na 0.1, Mg 0.1, P 3.4, S 0.2,(ICRU-44 1988) Cl 0.2, K 0.1, Ca 7.4, Fe 0.1Cortical bone 1.85 [1.4–2.5] 4.72 14.4 4.20 44.6 Mg 0.22, P 10.5, S 0.315,(ICRP-23 1975) Ca 21.0, Zn 0.01
configured. One consisted of a 5 cm thick semi-infinite lung (⇢ = 0.25 g cm�3) slab followedby a 5 cm thick semi-infinite cortical bone (⇢ = 1.85 g cm�3) slab; the other phantomwas similar, except the bone slab preceded the lung slab. In this case, the electron fluencecrossing the lung–bone interface within 4 cm of the beam central axis was scored and used tocompute the fluence averaged stopping power ratios with respect to water for each material.These simulations were performed for 6 MV and 18 MV photons using 1⇥ 109 phase-spaceparticles.
Additional calculations were performed using pre-computed energy spectra incident onthe phantom to determine sw,air for photon beams commonly used in radiotherapy. The 60Cobeam energy spectrum fromRogers et al (1988) was used, which includes the effect of photonsscattered in the source and by the beam collimators. Energy spectra for 4, 6, 10, 15 and 24MVaccelerators were used from the calculations of Mohan et al (1985). In these cases, a 10 cmdiameter input beamwas normally incident upon the phantom. The track-length average of theprimary electron fluence in the centre 8 cm diameter region was scored as a function of depthin water, lung and bone phantoms. These primary electron fluences were used to compute thewater-to-medium stopping power for each material listed in table 1. The geometric differencesin the beam orientation and the scoring geometry between these calculations and the fullMonteCarlo simulations are expected to be negligible.
Inmost patient treatment planningMonte Carlo dose calculations, data for a givenmaterial(mass-stopping powers and cross-sections) are pre-calculated at a given density, and then usedover a range of material densities. In reality, the stopping power of the material varies withthe material density due to the density effect (Swann 1938, ICRU-37 1984). To study theeffect of material density on stopping power ratio evaluation, stopping power ratio values withrespect to water were evaluated at the minimum, maximum and nominal density values shownin table 1.
In order to extend the concepts listed in this paper to materials and energies not covered inthis paper, an effective energy (Eeff ) for the stopping power ratio look-up is defined as the energyat which the mono-energetic stopping power equals that produced by (8E)m. The effectiveenergy for each pre-computed energy spectra was determine by least squares minimization ofthe difference between the Monte Carlo determined average stopping power ratio and that atthe sample effective energy for each material. A linear fit was then applied to the nominal

Converting absorbed dose to medium to absorbed dose to water 987
acceleration potential versus effective energy results to allow interpolation to different nominalacceleration potentials. Although other beam quality specifiers such as TPR20/10 are betterindicators of the beam quality, use of the nominal accelerating potential is justified here giventhat the dependence of sw,med on beam quality is weak. It can be noted that neither Eeff norTPR20/10 allows accurate simple interpolation of sw,air.
The effect of applying the dose-to-mediumcorrection factors onpatient dose calculations isdemonstrated on a head and neck treatment plan. Here, a Monte Carlo patient dose calculationwas performed using MCV, an in-house developed Monte Carlo dose calculation systemdirectly linked to the ADAC Pinnacle† treatment planning system. Isodose and dose–volumehistograms are given for both dose-to-medium and dose-to-water patient dose calculations.
4. Results
The dependence of sw,med on energy for mono-energetic electrons for typical patient materialsis shown in figure 1. (A similar plot evaluated at the mean energy of primary electrons forelectron beams, but likely applicable to electron energy spectra independent of their source, canbe found in Brahme et al (1988).) Stopping power values were computed using the computercode ESTAR (Berger 1993) which uses the ICRU-37 (1984) formalism and data. From 0.01 to20 MeV, the stopping power ratio for mono-energetic electrons changes substantially (>4%)for air, cortical bone and lung, while for ICRU tissue and soft bone, the ratio varies little.
Figure 1. Water-to-medium mass collision stopping power ratios as a function of electron energy.Materials indicated are as specified in table 1.
In order to determine sw,med for a photon beam, first the primary electron fluence ((8E)m)over which the stopping-power ratio is calculated must be determined. Figure 2 displays(8E)m computed at depths of 1.5 and 45 cm in a water phantom for 6 MV and 18 MV photon
† ADAC Laboratories, Milpitas, CA 95035, USA.

988 J V Siebers et al
Figure 2. Fluence of primary electrons computed at depths of 1.5 cm and 45 cm for 6 MV and18 MV photons.
beams. The depths were chosen for display as they show the maximum deviation in (8E)mfor the depths computed. For each incident photon beam, the electron spectrum shifts tohigher energies as the depth increases. For the instance of the 6 MV photon beam, the meanelectron energy at 1.5 cm depth is 1.00 MeV while at 45 cm depth, the mean electron energyis 1.16 MeV.
The stopping power ratio computed using the 6 MV and 18 MV electron energy as afunction of depth in a water phantom is shown in figure 3. At both energies, the water-to-medium stopping power ratios are nearly constant as a function of depth in the phantom forthe materials of interest. Values at 10 cm depth in the phantom are given in table 2. Thestatistical uncertainties in the sw,med values are less than 0.1%. The systematic uncertainties ofstopping power values and stopping power ratios are discussed in ICRU-37 (1984) and Andreo(1990). The effect of estimating the electron fluence below 7.5 keV as being the same as thatat 7.5 keV had little effect on the calculation as ignoring the electron fluence below 7.5 keVchanged sw,med by only 0.1%.
Evaluation of the stopping power ratio in a cortical bone phantom and lung phantom (usingthe electron energy spectra produced in these materials) revealed results similar to the waterphantom results. Values at 10 cm depth in these phantom materials are summarized in table 2.For typical patient media, sw,med is insensitive to variations in the electron spectra producedby photon transport in that material.
Other locationswhere (8E)m and sw,med might be expected to vary are atmaterial interfacesand outside the treatment field. Table 2 also summarizes results from the evaluation of sw,medoutside the treatment field area and at lung–bone and bone–lung interfaces. For the patientmaterials (neglecting air), sw,med is quite constant for the conditions studied. The maximumdeviation of 1.1% seen for cortical bone is due the fact that the outside the field, the electron

Converting absorbed dose to medium to absorbed dose to water 989
(a)
(b)
Figure 3. Water-to-medium stopping power ratios as a function of depth in the phantom for(a) 6 MV photons and (b) 18 MV photons. The phantom material for this case is water.
energy spectrum is shifted to lower energies due to a predominance of scattered photons. Thebone sw,med changes more than the other patient materials due to its higher effective atomicnumber. These results, combined with the previous results, show that for patient media, sw,med

990 J V Siebers et al
Table 2. Average water-to-medium stopping power ratios calculated for the variety of conditionsand phantoms studied. The incident beam was 10 ⇥ 10 cm2 at the phantom surface. The in-fieldresults evaluate the dose ratio within the central 4⇥ 4 cm2 area of this field while the outside-fieldresults evaluate the ratio outside a 12 ⇥ 12 cm2 area. The in-field and outside-field results areevaluated at a depth of 10 cm depth, while the others are at the depth of the interface.
ICRU Soft CorticalLocation Air Lung tissue bone bone
6 MVIn field (water) 1.117 0.999 1.010 1.035 1.116In field (bone) 1.117 1.000 1.010 1.035 1.117Lung–bone 1.120 1.000 1.010 1.035 1.117Bone–lung 1.118 1.001 1.010 1.035 1.116Outside field 1.132 1.006 1.010 1.035 1.12718 MVIn field (water) 1.085 0.985 1.010 1.035 1.110In field (bone) 1.086 0.986 1.010 1.035 1.111Lung–bone 1.092 0.989 1.010 1.035 1.111Bone–lung 1.086 0.987 1.010 1.035 1.110Outside field 1.117 0.999 1.010 1.035 1.112
Table 3. Calculated water-to-medium stopping power ratios at 10 cm depth for the beam energiesspecified. Also included is the Spencer–Attix (sSAw,air) stopping power ratio computed for each ofthese spectra by Andreo and Brahme (1986).
Air(Andreo) ICRU Soft Cortical
Beam energy (sSAw,air) Air Lung tissue bone bone
60Co 1.133 1.131 1.008 1.010 1.034 1.1194 MV 1.126 1.123 1.003 1.010 1.034 1.1176 MV 1.120 1.117 0.999 1.010 1.035 1.11610 MV 1.108 1.103 0.992 1.010 1.035 1.11315 MV 1.097 1.090 0.988 1.010 1.035 1.11124 MV 1.078 1.071 0.981 1.010 1.035 1.108
is a rather insensitive parameter. Thus, under the assumption that Bragg–Gray cavity theoryis valid, for photon beams a single correction factor can be used for each medium for a givenphoton energy when converting absorbed dose to medium to absorbed dose to water. In otherwords, for photon beams, a voxel-by-voxel evaluation of the dose to medium and dose to wateris not required.
Water-to-medium stopping power ratios evaluated using pre-computed published energyspectra are summarized in table 3. The results at 6MV agree with the values obtained using thefull Monte Carlo simulation (table 2), and the 15 and 24 MV results bracket the 18 MV resultsfrom the full simulation, confirming that the geometric approximationsmade for this simulationare negligible. ICRU tissue and soft-bone sw,med values do not depend upon the photonenergy from 60Co to 24 MV, while lung and cortical bone values decrease by 2.7% and 1.1%respectively. The air sw,med change (from 1.131 to 1.071) is significant, and agrees with theSpencer–Attix stopping power ratios reported by Andreo and Brahme (1986) to within 0.7%.
Evaluations of sw,med at the minimal, nominal and maximum material densities (fromtable 1) for a given material for an 18 MV beam are shown in figure 4. Note that the differencebetween lung and ICRU tissue stopping power ratios is almost entirely due to the materialdensity. The stopping power ratio deviates from that evaluated at the nominal density by up to

Converting absorbed dose to medium to absorbed dose to water 991
Figure 4. The water-to-medium stopping power ratios computed using stopping powers at thephysical material density, and also at the limits of the density ranges shown in table 1, for the18 MV beam.
Table 4. Effective energy for looking up the stopping power ratio for each material at 10 cm depth.Effective energy is defined as the energy at which the mono-energetic stopping power ratio equalsthat obtained using the energy spectra. For each material, the deviation from the MC determinedstopping power ratio is also given.
Nominal ICRU Soft Corticalenergy Eeff Air Lung tissue bone bone60Co 0.098 �0.2% �0.1 0 0.1 04 MV 0.731 0 �0.1 0 �0.3 0.16 MV 0.905 0 0 0 �0.2 010 MV 1.245 �0.3% + 0.3 0 �0.3 015 MV 1.578 �0.4% + 0.6 0 �0.3 024 MV 2.364 �0.3% + 0.9 0 �0.2 0
0.6% for ICRU tissue, 0.3% for lung, 0.2% for soft bone and 0.5% for cortical bone at 6 MV,while at 18 MV the differences are 1.3% for ICRU tissue, 1.0% for lung, 0.4% for soft boneand 0.8% for cortical bone. Thus, for Monte Carlo codes that evaluate the stopping powerat the local density of each voxel, the use of a single sw,med for all densities of the materialintroduces a maximum error of 1.3%. For Monte Carlo codes that use stopping power datafrom a nominal density at all densities of a given medium, sw,med is properly evaluated at thenominal density.
The effective energies (Eeff ) for look-up of sw,med for each pre-computed energy spectraare listed in table 4. Using this table, sw,med values for materials not listed in this paper canbe computed by looking up the mono-energetic sw,med at the Eeff for the nominal accelerationpotentials listed. The maximum error observed using this method to determine sw,med is less

992 J V Siebers et al
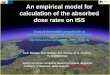
(c)
Figure 5. Results of applying the dose-to-medium to dose-to-water correction for a patient-basedMonte Carlo calculation. The tumour and cord areas are shaded on the CT slice. Only the 1.8and 1.2 Gy isodose lines are shown for clarity. Panel (a) shows dose to medium, (b) shows thedose to water, while (c) shows the dose–volume histograms for dose-to-water (solid line) anddose-to-medium (dashed line) based computations.
than 1%. For nominal acceleration potentials used in this study, a simple linear fit of the datayields
Eeff = 0.081P + 0.41

Converting absorbed dose to medium to absorbed dose to water 993
withP being the nominal acceleration potential. Theweak dependenceEeff onP allows its usein place of more precise beam quality specifiers such as TPR20/10. Using this simple linear fitfor determining Eeff also yields an error of less than 1% in the computed sw,med values; thus,sw,med can also be evaluated for energies not listed here for patient-like materials. This methodshould only be applied to materials with an effective atomic number equal to or less than themaximum investigated here (cortical bone).
Figure 5 shows dose distributions and dose–volume histograms for dose-to-medium- anddose-to-water-based computations for a head and neck plan. Only the 1.8 and 1.6 Gy isodoselines are shown for clarity. The 1.8 Gy isodose line varies substantially between the two dosedistributions. For the dose-to-medium plan, the 1.8 Gy line misses the cord, while for thedose to water plan, the 1.8 Gy line bisects the cord. The 1.8 Gy line covers much more bonyanatomy due to the 11% dose increase in converting from dose to medium to dose to water.Dose–volume histograms, which are widely used in evaluating treatment plans, e.g. as inputto biological models, are shown in figure 5(c). For this plan, converting the dose to mediumto dose to water shifts the resulting DVHs for the target and cord by about 1% as the materialsin these volumes are mainly tissue.
5. Discussion
The conversion between absorbed dose to medium and absorbed dose to water has been shownin this work to be reasonably constant throughout the treatment field and outside the treatmentvolume. The question arises, is it most appropriate to report absorbed dose to medium orabsorbed dose to water?
In dosimetry, such as when an ionization chamber is used, by default one measures thecharge produced in air then converts this response to dose to some material (typically water).Given this, sensible arguments could be made that dosimeter readings (and results from dosecalculation algorithms) should be converted to dose to medium for comparison with MonteCarlo results. Similarly, arguments could be made that since dosimetry calibration protocolsare based upon an absorbed dose-to-water standard (AAPM TG-51 1999), that conversion ofall dose calculation results to this standard is reasonable. Furthermore, since biological indices(NTCP, TCP etc) are given in terms of dose to water, it would be reasonable to always reportthis value. There may be instances when both Dwater and Dmed are desired, for example, doseto water (tumour cells) in bone matrix, and dose to bone in the bone itself. When the dose totarget cells contained within a material is desired, such as osteocytes in a bone matrix, the dosemust be converted. We feel this will be an interesting topic for future debate; however, furtherdiscussion on the merits of each position will not be presented here, as it does not directlypertain to the purpose of this paper. If absorbed dose-to-water values are desired, results fromthis paper can be applied as presented. If absorbed dose-to-medium results are desired, theinverse of the ratios presented here can be applied to convert dose-to-water results to dose tomedium.
6. Conclusions
Monte Carlo based dose calculations typically report absorbed dose to the medium in whichthe particle transport took place. In this paper, we have used Bragg–Gray cavity theory todevelop the conversion factor required to convert this to absorbed dose to water. For a givenphoton beam energy, the same material dependent conversion factor can be used throughoutthe treatment field since the dose-converting stopping power ratio does not depend upon the

994 J V Siebers et al
position in the field. For tissue and soft bone, a single correction factor can be used independentof energy. For lung and cortical bone, sw,med changes by 2.7% and 1.1% respectively from 60Coto 24 MV photons. To account for sw,med changes for these materials, sw,med is well describedby an effective energy. This allows translation of these results to other patient-like materials.Furthermore, since the effective energy is linear with the nominal accelerating potential, theseresults can be applied to determine sw,med for an arbitrary photon energy between 4 MV and24 MV.
Occasional cases may exist in which dose to material is required, such as determiningwhether the dose to the bone matrix is high enough to cause brittleness and potential fracture.In such cases, results fromdose-to-water-based algorithms can use the inverse of the conversionfactors presented here to yield the dose to the material.
Acknowledgment
The MCV authors acknowledge the financial support of NIH grant CA 74158-02.
References
AAPM TG-21 1983 A protocol for the determination of absorbed dose from high-energy photon and electron beamsMed. Phys. 10 741–71
AAPM TG-51 1999 AAPM’s TG-51 protocol for clinical reference dosimetry of high-energy photon and electronbeams Med. Phys. 26 1847–70
Andreo P 1990 Uncertainties in dosimetric data and beam calibration Int. J. Radiat. Oncol. Biol. Phys. 19 1233–47Andreo P and Brahme A 1986 Stopping power data for high-energy photon beams Phys. Med. Biol. 31 839–58Attix F H 1986 Introduction to Radiological Physics and Radiation Dosimetry (New York: Wiley)Berger M J 1993 ESTAR National Institute of Standards and Technology Physics Laboratory Ionizing Radiation
Division Report NISTIR 4999Bragg W H 1912 Studies in Radioactivity (New York: MacMillan)Brahme A, Chavaudra J, Landberg T, McCullough E C, Nusslin F, Rawlinson J A, Svensson G and Svensson H 1988
Accuracy requirements and quality assurance of external beam therapy with photons and electrons Acta Oncol.suppl 1
Briesmeister J F 1997 MCNP—a general Monte Carlo n-particle transport code, version 4B Los Alamos NationalLaboratory Report LA-13181
DeMarco J J, Solberg T D and Smathers J B 1998 A CT-based Monte Carlo simulation tool for dosimetry planningand analysis Med. Phys. 25 1–11
Fippel M 1999 Fast Monte Carlo dose calculation for photon beams based on the VMC electron algorithmMed. Phys.26 1466–75
Gray L H 1936 An ionization method for the absolute measurement of gamma-ray energy Proc. R. Soc. A 156 578Hartmann-Siantar C L, Chandler W P, Chadwick M B, Blann H M, Cox L J, Resler D A, Rathkopf J A, Mackie T R,
Siebers J V, Ross M A, DeLuca P M, Weaver K A and White R M 1995 Dose distributions calculated withPeregrine all particle Monte Carlo code [abstract] Med. Phys. 22 994
Hartmann-Siantar C L, ChandlerW P, ChadwickMB, Cox L J, Rathkopf J A, Resler DA, SvatosMM andWhite RM1994 PEREGRINE: the all-particle Monte Carlo dose calculation code [abstract] Med. Phys. 21 937
ICRP-23 1975 Reference Man: anatomical, physiological and metabolic characteristics International Commission ofRadiation Protection Report 23 (New York: ICRP)
ICRU-33 1980 Radiation quantities and units International Commission on Radiation Units and MeasurementsReport 33 (Bethesda, MD: ICRU)
ICRU-35 1984 Radiation dosimetry: electron beams with energies between 1 and 50 MeV International Commissionon Radiation Units and Measurements Report 35 (Bethesda, MD: ICRU)
ICRU-37 1984 Stopping powers for electrons and positrons International Commission on Radiation Units andMeasurements Report 37 (Bethesda, MD: ICRU)
ICRU-44 1988 Tissue substitutes in radiation dosimetry and measurement International Commission on RadiationUnits and Measurements Report 44 (Bethesda, MD: ICRU)
Ma C M, Mok E, Kapur A, Pawlicki T, Findley D, Brain S, Korster K and Boyer A L 1999 Clinical implementationof a Monte Carlo treatment planning system Med. Phys. 26 2133–43

Converting absorbed dose to medium to absorbed dose to water 995
Ma C-M and Nahum A E 1991 Bragg–Gray theory and ion chamber dosimetry for photon beams Phys. Med. Biol. 36413–28
Mohan R 1997 Why Monte Carlo? 12th Int. Conference on the Use of Computers in Radiotherapy (Salt Lake City,UT)
Mohan R, Chui C and Lidofsky L 1985 Energy and angular distributions of photons from medical linear acceleratorsMed. Phys. 12 592–7
Nahum A E 1978 Water/air mass stopping power ratios for megavoltage photon and electron beams Phys. Med. Biol.23 24–38
NCRP-27 1961 Stopping powers for use with cavity chambers National Bureau of Standards Handbook Report 79National Council on Radiation Protection and Measurements
Rogers D W O, Ewart G M, Bielajew A F and van Dyk G 1988 Calculation of electron contamination in a 60-Cotherapy beam Proc. IAEA Int. Symp. on Dosimetry in Radiotherapy (Vienna)
Siebers J V, Keall P J, Libby B and Mohan R 1999 Comparison of EGS4 and MCNP4b Monte Carlo codes forgeneration of photon phase space distributions for a Varian 2100C Phys. Med. Biol. 44 3009–26
Solberg T D, DeMarco J J, Holly F E, Smathers J B and DeSalles A A F 1998 Monte Carlo treatment planning forstereotactic radiosurgery Radiother. Oncol. 49 73–84
Spencer L V and Attix F H 1955 A theory of cavity ionization Radiat. Res. 3 239Swann W F G 1938 Theory of energy loss of high energy particles J. Franklin Inst. 226 598Tortora T J and Grabowski S R 1993 Principles of Anatomy and Physiology (New York: Harper Collins)Wang L, Chui C-S and Lovelock M 1998 A patient-specific Monte Carlo dose calculation method for photon beams
Med. Phys. 25 867–78